Chronic Kidney Disease Pathway Document Description Presented ...
Chronic Kidney Disease Pathway Document Description Presented ...
Chronic Kidney Disease Pathway Document Description Presented ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
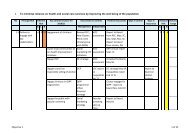
Appendix 1<br />
The Dudley Group of Hospitals<br />
NHS Trust<br />
<strong>Pathway</strong> for the Management of Calcium and Phosphate balance in<br />
<strong>Chronic</strong> <strong>Kidney</strong> <strong>Disease</strong> within Dudley Health Economy<br />
Rationale: Hyperphosphataemia (elevated serum phosphate) is recognised as an important risk factor for many adverse outcomes in dialysis<br />
patients, including vascular calcification, calciphylaxis, secondary hyperparathyroidism and mortality. Retention of phosphate occurs much earlier in<br />
the course of CKD. Serum phosphate concentration increases when eGFR falls below 30 mls/minute (CKD 4).<br />
Aim: To maintain phosphate levels between 0.9-1.5 mmol/L (1) and between 1.1 and 1.8 mmol/L in dialysis patients.<br />
Dietary Modification: Patients with CKD may need to follow a reduced phosphate diet. Phosphate rich foods include chocolate, nuts, dairy, eggs,<br />
meat and fish. This needs to be balanced carefully and so referral to a specialist dietitian is essential.<br />
If phosphate or intact PTH levels cannot be controlled within target range despite dietary phosphate restriction then prescribe a phosphate binder.<br />
Calcium containing phosphate binders<br />
1 st Line Choice:<br />
Calcium Carbonate (Calcichew®) 1.25g<br />
(Contains 500mg elemental calcium per tablet)<br />
Dose: To be titrated starting at 1 bd up to 2 tds<br />
with meals<br />
S/E: diarrhoea, hypercalcaemia<br />
Alternatives: Adcal ® 1.5g<br />
(Contains 600mg elemental calcium per tablet)<br />
or add D3 in those at risk of Osteoporosis with<br />
CKD stages 1-3<br />
2 nd Line Choice:<br />
Calcium Acetate (Phosex®) 1000mg<br />
Indication – hyperphosphataemia and<br />
intolerance to calcium carbonate or contraindicated.<br />
NB - contains less elemental calcium<br />
compared to calcium carbonate for the same<br />
phosphate binding capacity; this is also<br />
affected less by gastric pH.<br />
Dose: 1g tds with meals titrated according to<br />
serum phosphate levels, max 12 daily.<br />
S/E: nausea and vomiting, constipation.<br />
NB - Prescribing should be in line with an<br />
effective shared care agreement (ESCA)<br />
Calcium Acetate.doc<br />
* MONITORING<br />
Parameter<br />
Serum<br />
Phosphorous<br />
concentration<br />
Serum<br />
calcium<br />
concentration<br />
Frequency<br />
of<br />
Monitoring<br />
Every 2-4<br />
weeks until<br />
stable levels<br />
are reached<br />
and then 1-3<br />
months as<br />
directed by<br />
the clinician<br />
Target (KDOQI,<br />
Renal Association,<br />
recommendations<br />
for stages of CKD)<br />
CKD Stage 3/4 0.9 –<br />
1.5 mmol/l<br />
Dialysis 1.1 – 1.8<br />
mmol/l<br />
1-2 monthly CKD Stage 3/4 2.1 -<br />
2.6 mmol/l<br />
Dialysis 2.2 – 2.5<br />
mmol/l<br />
Ca x P CKD Stage 3/4 2.6 mmols/l<br />
SEVELAMER (RENAGEL®) 800mg<br />
Indication: hyperphosphataemia as monotherapy<br />
or in combination with calcium containing<br />
phosphate binder. May also decrease total and<br />
LDL cholesterol.<br />
Dose: 1 tds with meals, titrate dose according to<br />
calcium and phosphate balance, max 5 per<br />
meal.<br />
SE’s/CI: CI in hypersensitivity,<br />
hypophosphataemia, bowel obstruction, young<br />
children, gastroparesis, swallowing disorders.<br />
NB – Prescribing should be in line with an ESCA<br />
Sevelamer.doc<br />
OR<br />
LANTHANUM (FOSRENOL®)<br />
Indication: hyperphosphataemia<br />
NB – May be beneficial in those who are<br />
intolerant to sevelamer or where it is desirable to<br />
reduce the pill burden.<br />
Dose: 500mg, 750mg or 1000mg with meals<br />
titrated to 1500mg or 3000mg daily.<br />
S/E’s: Abdominal pain, constipation, diarrhoea,<br />
nausea and vomiting.<br />
NB – Prescribing should be in line with an ESCA<br />
Lanthanum.doc<br />
PRESCRIBING COSTS:- / DRUG<br />
INFORMATION<br />
Phosphate binders<br />
Calcichew 2tds £15.67<br />
Phosex 2tds £18.47<br />
Sevelamer 3tds £171.86<br />
Lanthanum 1tds 750mg £142.03<br />
Cost of 28 days<br />
treatment (BNF 56)<br />
63