Golniški simpozij 2011 Zbornik povzetkov
Golniški simpozij 2011 Zbornik povzetkov
Golniški simpozij 2011 Zbornik povzetkov

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Comprehensive medication history:<br />
the need for the implementation<br />
of medication reconciliation processes<br />
Lea Knez 1 , Renata Reæonja 1,2 , Stanislav Øuøkoviœ 1 , Mitja Koønik 1 , Aleø Mrhar 2<br />
1<br />
Faculty of Pharmacy, University of Ljubljana<br />
2<br />
University Clinic of Respiratory and Allergic Diseases, Golnik<br />
Background<br />
Comprehensive medication history (CMH) is of outmost importance for patient evaluation and prescription<br />
of drug treatment upon hospital admission. The aim of this study was to assess the need<br />
for the implementation of medication reconciliation processes into clinical practice.<br />
Method<br />
Patients admitted to a teaching hospital in Slovenia were randomly selected and included in the<br />
study. For every patient a CMH was obtained by a research pharmacist using different sources of information.<br />
Next, medication history in the hospital medical record was reviewed. Prescription of medicines<br />
was assessed for completeness of information and discrepancies between both medication<br />
histories were recorded and classified.<br />
Results<br />
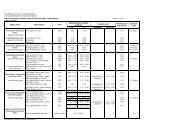
Overall, 108 patients with a median age of 73 years were included. The research pharmacist recorded<br />
the use of 651 medicines, of which 94.9% provided all relevant details for drug identification and administration.<br />
Less medicines (464) were recorded in the hospital medical record as compared to the<br />
CMH (paired t-test, p>0.001) and only 42.0% of these medicines were evaluated as complete. When<br />
comparing the medication history in the medical record with the CMH, at least one discrepancy was<br />
detected in 72.4% of medicines and was often present in the medication order on the drug chart<br />
(76.2%) and in the discharge letter (69.9%). Discrepancies often arose due to medicine’s omission<br />
(20.9%) and medicine’s commission (6.5%).<br />
Conclusions<br />
The high rate of discrepancies between the recorded drug history and CMH reported in our study<br />
shows the need for implementation of medication reconciliation practices. Pharmacists’ participation<br />
in admission reconciliation, as described in this study, led to more complete and accurate drug<br />
histories. In the study hospital, pharmacist-led CMH have been introduced in a research framework<br />
within which the benefits of this service for the reduction of medication errors and adverse drug<br />
events are being studied against routine practice in a randomised trial.<br />
24