Health Bulletin 2009
Health Bulletin 2009
Health Bulletin 2009

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
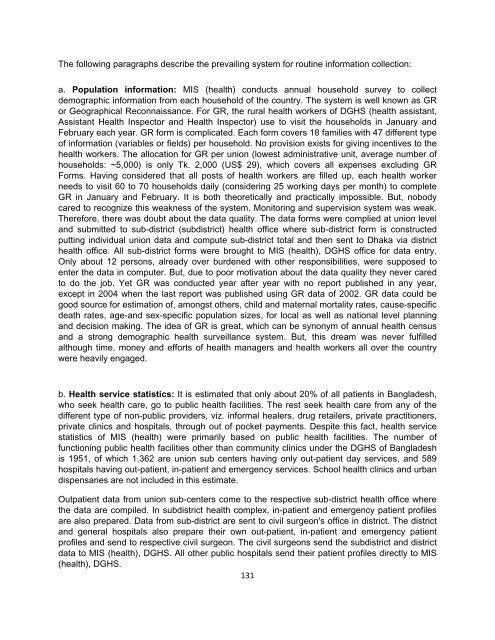
The following paragraphs describe the prevailing system for routine information collection:<br />
a. Population information: MIS (health) conducts annual household survey to collect<br />
demographic information from each household of the country. The system is well known as GR<br />
or Geographical Reconnaissance. For GR, the rural health workers of DGHS (health assistant,<br />
Assistant <strong>Health</strong> Inspector and <strong>Health</strong> Inspector) use to visit the households in January and<br />
February each year. GR form is complicated. Each form covers 18 families with 47 different type<br />
of information (variables or fields) per household. No provision exists for giving incentives to the<br />
health workers. The allocation for GR per union (lowest administrative unit, average number of<br />
households: ~5,000) is only Tk. 2,000 (US$ 29), which covers all expenses excluding GR<br />
Forms. Having considered that all posts of health workers are filled up, each health worker<br />
needs to visit 60 to 70 households daily (considering 25 working days per month) to complete<br />
GR in January and February. It is both theoretically and practically impossible. But, nobody<br />
cared to recognize this weakness of the system. Monitoring and supervision system was weak.<br />
Therefore, there was doubt about the data quality. The data forms were complied at union level<br />
and submitted to sub-district (subdistrict) health office where sub-district form is constructed<br />
putting individual union data and compute sub-district total and then sent to Dhaka via district<br />
health office. All sub-district forms were brought to MIS (health), DGHS office for data entry.<br />
Only about 12 persons, already over burdened with other responsibilities, were supposed to<br />
enter the data in computer. But, due to poor motivation about the data quality they never cared<br />
to do the job. Yet GR was conducted year after year with no report published in any year,<br />
except in 2004 when the last report was published using GR data of 2002. GR data could be<br />
good source for estimation of, amongst others, child and maternal mortality rates, cause-specific<br />
death rates, age-and sex-specific population sizes, for local as well as national level planning<br />
and decision making. The idea of GR is great, which can be synonym of annual health census<br />
and a strong demographic health surveillance system. But, this dream was never fulfilled<br />
although time, money and efforts of health managers and health workers all over the country<br />
were heavily engaged.<br />
b. <strong>Health</strong> service statistics: It is estimated that only about 20% of all patients in Bangladesh,<br />
who seek health care, go to public health facilities. The rest seek health care from any of the<br />
different type of non-public providers, viz. informal healers, drug retailers, private practitioners,<br />
private clinics and hospitals, through out of pocket payments. Despite this fact, health service<br />
statistics of MIS (health) were primarily based on public health facilities. The number of<br />
functioning public health facilities other than community clinics under the DGHS of Bangladesh<br />
is 1951, of which 1,362 are union sub centers having only out-patient day services, and 589<br />
hospitals having out-patient, in-patient and emergency services. School health clinics and urban<br />
dispensaries are not included in this estimate.<br />
Outpatient data from union sub-centers come to the respective sub-district health office where<br />
the data are compiled. In subdistrict health complex, in-patient and emergency patient profiles<br />
are also prepared. Data from sub-district are sent to civil surgeon's office in district. The district<br />
and general hospitals also prepare their own out-patient, in-patient and emergency patient<br />
profiles and send to respective civil surgeon. The civil surgeons send the subdistrict and district<br />
data to MIS (health), DGHS. All other public hospitals send their patient profiles directly to MIS<br />
(health), DGHS.<br />
131





![Bangladesh Demographic and Health Survey 2007 [FR207]](https://img.yumpu.com/38440445/1/190x257/bangladesh-demographic-and-health-survey-2007-fr207.jpg?quality=85)