SOP for Post Entry Quarantine Inspection - Plant quarantine India
SOP for Post Entry Quarantine Inspection - Plant quarantine India
SOP for Post Entry Quarantine Inspection - Plant quarantine India

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
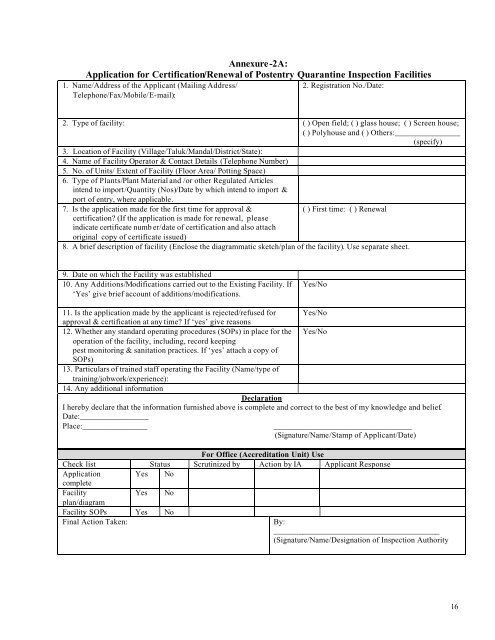
Annexure-2A:Application <strong>for</strong> Certification/Renewal of <strong>Post</strong>entry <strong>Quarantine</strong> <strong>Inspection</strong> Facilities1. Name/Address of the Applicant (Mailing Address/Telephone/Fax/Mobile/E-mail):2. Registration No./Date:2. Type of facility: ( ) Open field; ( ) glass house; ( ) Screen house;( ) Polyhouse and ( ) Others:________________(specify)3. Location of Facility (Village/Taluk/Mandal/District/State):4. Name of Facility Operator & Contact Details (Telephone Number)5. No. of Units/ Extent of Facility (Floor Area/ Potting Space)6. Type of <strong>Plant</strong>s/<strong>Plant</strong> Material and /or other Regulated Articlesintend to import/Quantity (Nos)/Date by which intend to import &port of entry, where applicable.7. Is the application made <strong>for</strong> the first time <strong>for</strong> approval &( ) First time: ( ) Renewalcertification? (If the application is made <strong>for</strong> renewal, pleaseindicate certificate numb er/date of certification and also attachoriginal copy of certificate issued)8. A brief description of facility (Enclose the diagrammatic sketch/plan of the facility). Use separate sheet.9. Date on which the Facility was established10. Any Additions/Modifications carried out to the Existing Facility. If‘Yes’ give brief account of additions/modifications.Yes/No11. Is the application made by the applicant is rejected/refused <strong>for</strong> Yes/Noapproval & certification at any time? If ‘yes’ give reasons12. Whether any standard operating procedures (<strong>SOP</strong>s) in place <strong>for</strong> the Yes/Nooperation of the facility, including, record keepingpest monitoring & sanitation practices. If ‘yes’ attach a copy of<strong>SOP</strong>s)13. Particulars of trained staff operating the Facility (Name/type oftraining/jobwork/experience):14. Any additional in<strong>for</strong>mationDeclarationI hereby declare that the in<strong>for</strong>mation furnished above is complete and correct to the best of my knowledge and belief.Date:_________________Place:__________________________________________________(Signature/Name/Stamp of Applicant/Date)For Office (Accreditation Unit) UseCheck list Status Scrutinized by Action by IA Applicant ResponseApplication Yes NocompleteFacilityYes Noplan/diagramFacility <strong>SOP</strong>s Yes NoFinal Action Taken:By:_________________________________________(Signature/Name/Designation of <strong>Inspection</strong> Authority16