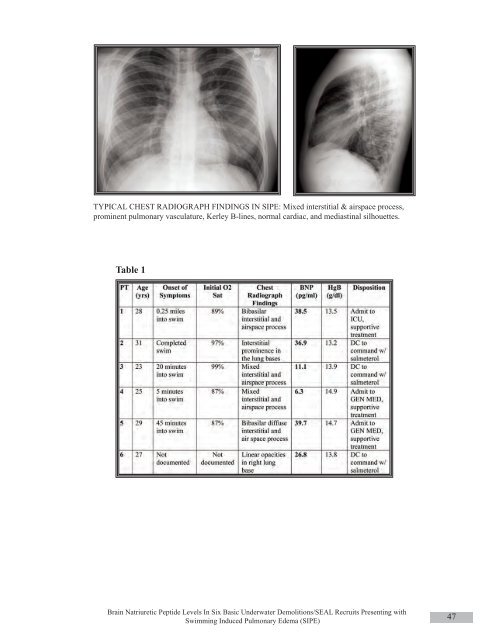
overall accuracy of 80% for cardiac dyspnea. 4 Additionally,brain natriuretic peptide has a sensitivity of82% and specificity of 92% for identification of cardiaccauses of syncope, when a cut-off value of40pg/ml is used. 25It is of note, that resting BNP concentrationsare not elevated in physiologically hypertrophiedhearts of endurance athletes. 26CLINICAL CONSIDERATIONSTypical symptoms of SIPE include dyspnea,cough which may be productive of pink or white frothysputum, chest pain or tightness, and hemoptysis. Uponinitial symptom onset, patients may exhibit confusionsecondary to hypoxemia. Typical signs include laboredbreathing, tachypnea, and hypoxemia.SIPE can be confidently diagnosed in any patientpresenting with the above noted signs and symptomsoccurring during or immediately after aswimming event, in association with a demonstrablechest radiograph abnormality. The treatment of SIPEis primarily supportive. It is imperative to deliver supplementaloxygen to the patient, titrated to maintainnormal oxygen saturation. In the military setting,Corpsmen or First Responders covering training evolutionswith an inherent risk for the development ofSIPE, should be equipped with pulse oximetry, supplementaloxygen, and inhaled beta agonists. Theyshould be trained in Basic Life Support (BLS/CPR).Prompt evaluation by a physician with access to radiography,Advanced Cardiac Life Support (ACLS) capability,and laboratory support is important formoderate to severe cases of SIPE. However, there is noevidence in the literature that ACLS has been necessaryin the treatment of SIPE.Clinical experience has shown long acting inhaledbeta agonists, such as salmeterol, to be of utility.This agent accelerates resolution via improved alveolarfluid clearance and also provides symptomatic reliefto the patient. 16 Diuretics generally are not necessaryin the treatment of SIPE. 27Occasionally patients with SIPE will requireinpatient admission, though frequently patients can bedischarged directly from the emergency departmentafter a period of treatment and observation, once oxygensaturation has returned to baseline on room air.A hallmark of SIPE is rapid resolution. Frequently,symptoms resolve within 12 to 24 hours withchest radiographs demonstrating resolution within 24to 48 hours. Frequently, patients can be returned to fullduty within 72 hours.Historically, there is no evidence that individualswho suffer from an episode of SIPE are predisposedto have additional occurrences. Typically,BUDS candidates who suffer from SIPE have graduationrates commensurate with their fellow students whohave not had a SIPE event. In fact, testing in dry conditionsof individuals previously diagnosed with SIPErevealed that they do not have abnormal pulmonaryfunction tests, abnormal exercise capacity, or abnormalpulmonary arterial pressure response to hypoxemia. 10There are no definite predisposing factors forSIPE. However, Shupak et al. did demonstrate thatbaseline FVC, FEV1, and FEF were 25 to 75% lowerin twenty-one individuals diagnosed with SIPE. Thuslower initial lung volumes and flows may be predictiveof vulnerability to SIPE. 28METHODSSix BUD/S recruits presented to the ED withpulmonary complaints after a surface bay swim. Thediagnosis of SIPE was made on all six individualsbased on presenting complaint, chest radiograph findings,and physical examination. BNP levels weredrawn on these individuals as part of the clinical evaluationof dyspnea, cough, and pulmonary edema in theemergency department setting. Transport time to theED was approximately thirty to forty-five minutes fromsymptom onset. Labs were drawn within two hours ofswim termination.The case definition of SIPE for the purposes ofthis report is hypoxemia occurring during or immediatelyafter a swimming event, a demonstrable chest radiographabnormality, improvement or resolution ofsaid abnormality in less than 48 hours, absence of evidenceof pulmonary infection, and absence of a historyof breathing against a closed glottis or aspiration ofwater.RESULTS AND PATIENT DATASee Table 1 on page 47ResultsBNP levels ranged from 6.3pg/ml to39.7pg/ml. The average was 26.55pg/ml. All valuesfell within the NMCSD laboratory range of normal, 1-100pg/ml. All six individuals demonstrated abnormalchest radiographs with both interstitial and airspaceprocesses. The cardiac and mediastinal silhouetteswere normal in all cases. Three patients were admittedto the internal medicine service. One patient was admittedto the ICU. Two patients were discharged totheir command. The patients admitted to the hospitalstayed an average of twenty-four hours. Their treatmentconsisted of supplemental oxygen and beta-agonists(alveolar fluid clearance). All were returned tofull duty within seventy-two hours. Two of the six individualswent on to complete BUD/S training and becameSEALs. This graduation rate of 33% is consistentwith normal rates in individuals attending BUD/S.This likely indicates that a single episode of SIPE doesnot cause long-term decrements in physical performancefrom a cardiovascular standpoint.46Journal of <strong>Special</strong> <strong>Operations</strong> Medicine Volume 9, Edition 3 / <strong>Summer</strong> 09
TYPICAL CHEST RADIOGRAPH FINDINGS IN SIPE: Mixed interstitial & airspace process,prominent pulmonary vasculature, Kerley B-lines, normal cardiac, and mediastinal silhouettes.Table 1Brain Natriuretic Peptide Levels In Six Basic Underwater Demolitions/SEAL Recruits Presenting withSwimming Induced Pulmonary Edema (SIPE)47
- Page 1 and 2: Volume 9, Edition 3 / Summer 09 Jou
- Page 3 and 4: An 18D deworms a camel during a “
- Page 5 and 6: Field Evaluation and Management of
- Page 7 and 8: The circumferential anchoring strip
- Page 9 and 10: In doing so, all the skin is closed
- Page 11 and 12: NATO SOF Transformation and theDeve
- Page 13 and 14: current and future operations, thes
- Page 15 and 16: sion of a physician, and limited pr
- Page 17 and 18: REFERENCES1. James L. Jones, “A b
- Page 19 and 20: This article is the first of two me
- Page 21 and 22: Figure 4 : A Special Forces medic c
- Page 23 and 24: exposure. Conversely, the customary
- Page 25 and 26: 7. Ted Westmoreland. (2006). Attrib
- Page 27 and 28: first three days of injury, althoug
- Page 29 and 30: 9. Markgraf CG, Clifton GL, Moody M
- Page 31 and 32: the only sign of OCS may be elevate
- Page 33 and 34: E. The canthotomy allows for additi
- Page 35 and 36: 33. Rosdeutscher, J.D. and Stradelm
- Page 37 and 38: Tinnitus, a Military Epidemic:Is Hy
- Page 39 and 40: The development of chronic NIHL pro
- Page 41 and 42: supplied by diffusion. During expos
- Page 43 and 44: similar to those of other authors,
- Page 45 and 46: promising effect on tinnitus. Howev
- Page 47 and 48: ADDITIONAL REFERENCESHoffmann, G; B
- Page 49: et al. demonstrated that both right
- Page 53 and 54: 11. Norsk P, Bonde-Petersen F, Warb
- Page 55 and 56: ABSTRACTS FROM CURRENT LITERATUREMa
- Page 57 and 58: tourniquet times are less than 6 ho
- Page 59 and 60: tal from July 1999 to June 2002. In
- Page 61 and 62: Operation Sadbhavana: Winning Heart
- Page 63 and 64: CENTRAL RETINAL VEIN OCCLUSION IN A
- Page 65 and 66: of the X chromosome. Notable is tha
- Page 67 and 68: AUTHORS*75th Ranger Regiment6420 Da
- Page 69 and 70: Casualties presenting in overt shoc
- Page 71 and 72: PSYCHOLOGICAL RESILIENCE AND POSTDE
- Page 73 and 74: spondents without PTSD (M = 4.6, SD
- Page 75 and 76: patients, whereas the mean score of
- Page 77 and 78: 29. Whealin JM, Ruzek JI, Southwick
- Page 79 and 80: average, time between return from d
- Page 81 and 82: ing functioning in both PTSD (Zatzi
- Page 83 and 84: Editorial Comment on “Psychologic
- Page 85 and 86: Blackburn’s HeadhuntersPhilip Har
- Page 87 and 88: The Battle of Mogadishu:Firsthand A
- Page 89 and 90: Task Force Ranger encountered enemy
- Page 91 and 92: Peter J. Benson, MDCOL, USACommand
- Page 93 and 94: Numerous military and civilian gove
- Page 95 and 96: Anthony M. Griffay, MDCAPT, USNComm
- Page 97 and 98: This is a great read that speaks di
- Page 99 and 100: and twenty-eight. Rabies immune glo
- Page 101 and 102:
Rhett Wallace MD FAAFPLTC MC SFS DM
- Page 103 and 104:
LTC Craig A. Myatt, Ph.D., HQ USSOC
- Page 105 and 106:
LTC Bill Bosworth, DVM, USSOCOM Vet
- Page 107 and 108:
Europe, Mideast, Africa and SWAU.S.
- Page 109 and 110:
SOF and SOF Medicine Book ListWe ha
- Page 111 and 112:
TITLE AUTHOR ISBNCohesion, the Key
- Page 113 and 114:
TITLE AUTHOR ISBNI Acted from Princ
- Page 115 and 116:
TITLE AUTHOR ISBNRats, Lice, & Hist
- Page 117 and 118:
TITLE AUTHOR ISBNThe Healer’s Roa
- Page 119 and 120:
TITLE AUTHOR ISBNGuerilla warfare N
- Page 121 and 122:
TITLEAUTHORBlack Eagles(Fiction)Bla
- Page 123 and 124:
TITLE(Good section on Merrill’s M
- Page 125 and 126:
GENERAL REFERENCESALERTS & THREATSB
- Page 127 and 128:
Aviation Medicine Resources: http:/
- Page 129 and 130:
LABORATORYClinical Lab Science Reso
- Page 131 and 132:
A 11 year old boy whose tibia conti
- Page 133 and 134:
Meet Your JSOM StaffEXECUTIVE EDITO
- Page 135 and 136:
Special Forces Aidman's PledgeAs a