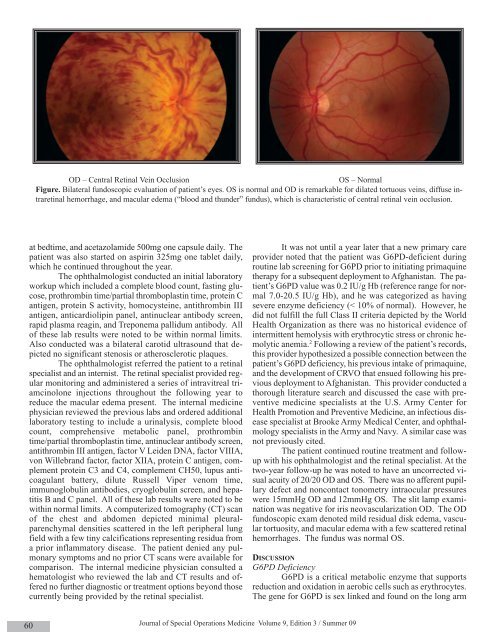
OD – Central Retinal Vein OcclusionOS – NormalFigure. Bilateral fundoscopic evaluation of patient’s eyes. OS is normal and OD is remarkable for dilated tortuous veins, diffuse intraretinalhemorrhage, and macular edema (“blood and thunder” fundus), which is characteristic of central retinal vein occlusion.at bedtime, and acetazolamide 500mg one capsule daily. Thepatient was also started on aspirin 325mg one tablet daily,which he continued throughout the year.The ophthalmologist conducted an initial laboratoryworkup which included a complete blood count, fasting glucose,prothrombin time/partial thromboplastin time, protein Cantigen, protein S activity, homocysteine, antithrombin IIIantigen, anticardiolipin panel, antinuclear antibody screen,rapid plasma reagin, and Treponema pallidum antibody. Allof these lab results were noted to be within normal limits.Also conducted was a bilateral carotid ultrasound that depictedno significant stenosis or atherosclerotic plaques.The ophthalmologist referred the patient to a retinalspecialist and an internist. The retinal specialist provided regularmonitoring and administered a series of intravitreal triamcinoloneinjections throughout the following year toreduce the macular edema present. The internal medicinephysician reviewed the previous labs and ordered additionallaboratory testing to include a urinalysis, complete bloodcount, comprehensive metabolic panel, prothrombintime/partial thromboplastin time, antinuclear antibody screen,antithrombin III antigen, factor V Leiden DNA, factor VIIIA,von Willebrand factor, factor XIIA, protein C antigen, complementprotein C3 and C4, complement CH50, lupus anticoagulantbattery, dilute Russell Viper venom time,immunoglobulin antibodies, cryoglobulin screen, and hepatitisB and C panel. All of these lab results were noted to bewithin normal limits. A computerized tomography (CT) scanof the chest and abdomen depicted minimal pleuralparenchymaldensities scattered in the left peripheral lungfield with a few tiny calcifications representing residua froma prior inflammatory disease. The patient denied any pulmonarysymptoms and no prior CT scans were available forcomparison. The internal medicine physician consulted ahematologist who reviewed the lab and CT results and offeredno further diagnostic or treatment options beyond thosecurrently being provided by the retinal specialist.It was not until a year later that a new primary careprovider noted that the patient was G6PD-deficient duringroutine lab screening for G6PD prior to initiating primaquinetherapy for a subsequent deployment to Afghanistan. The patient’sG6PD value was 0.2 IU/g Hb (reference range for normal7.0-20.5 IU/g Hb), and he was categorized as havingsevere enzyme deficiency (< 10% of normal). However, hedid not fulfill the full Class II criteria depicted by the WorldHealth Organization as there was no historical evidence ofintermittent hemolysis with erythrocytic stress or chronic hemolyticanemia. 2 Following a review of the patient’s records,this provider hypothesized a possible connection between thepatient’s G6PD deficiency, his previous intake of primaquine,and the development of CRVO that ensued following his previousdeployment to Afghanistan. This provider conducted athorough literature search and discussed the case with preventivemedicine specialists at the U.S. Army Center forHealth Promotion and Preventive Medicine, an infectious diseasespecialist at Brooke Army Medical Center, and ophthalmologyspecialists in the Army and Navy. A similar case wasnot previously cited.The patient continued routine treatment and followupwith his ophthalmologist and the retinal specialist. At thetwo-year follow-up he was noted to have an uncorrected visualacuity of 20/20 OD and OS. There was no afferent pupillarydefect and noncontact tonometry intraocular pressureswere 15mmHg OD and 12mmHg OS. The slit lamp examinationwas negative for iris neovascularization OD. The ODfundoscopic exam denoted mild residual disk edema, vasculartortuosity, and macular edema with a few scattered retinalhemorrhages. The fundus was normal OS.DISCUSSIONG6PD DeficiencyG6PD is a critical metabolic enzyme that supportsreduction and oxidation in aerobic cells such as erythrocytes.The gene for G6PD is sex linked and found on the long arm60Journal of <strong>Special</strong> <strong>Operations</strong> Medicine Volume 9, Edition 3 / <strong>Summer</strong> 09
of the X chromosome. Notable is that more than 400 millionpeople carry a G6PD-deficient gene. 1,2,3 Although dispersedworldwide, G6PD deficiency occurs with increased frequencythroughout Africa, Asia, the Middle East, and the Mediterraneanregion. While G6PD deficiency may provide a biologicaladvantage through relative resistance to Plasmodiumfalciparum malaria, it has over 440 known genetic variantsthat result in varying degrees of enzymopathy and a wide spectrumof clinical outcomes ranging from asymptomatic to severehemolytic reactions resulting in transfusion or death. 1,2G6PD deficiency has conventionally been the archetype of enzymopathyhemolytic anemias and is a leading model of hemolyticanemia resulting from intracorpuscular andextracorpuscular interaction, as most of these hemolytic casesare triggered by an exogenous agent. These exogenous triggersinclude infections, toxins, foodstuffs (ie, fava beans), andmedications (ie, antimicrobials).Although the antimicrobial primaquine prompted thediscovery of G6PD deficiency over 50 years ago, 1 primaquinecontinues to be an important adjunct used routinely for antimalarialtherapy. As a response to frequent deployments ofnumerous Army personnel to malaria-endemic regions includingAfghanistan, the Department of the Army directed thatall deploying U.S. Army personnel would undergo G6PD deficiencyscreening in order to safeguard against hemolytic reactionsresulting from primaquine therapy. 6 In this case report,it is uncertain how the individual described did not receivescreening for G6PD deficiency prior to the initiation of primaquinetherapy.By itself, primaquine is a cause of increased levels ofmethemoglobin in many patients who take it, but the levelsachieved seldom cause symptoms. However, pathologicmethemoglobinemia and hemolytic anemia do routinely occurin G6PD-deficient individuals who consume primaquine. Primaquineis known to be associated with visual accommodationcomplaints, although a review of the literature does notreveal documentation of other visual disorders to includeCRVO. However, the finding of increased erythrocyte aggregationand erythrocyte-endothelium interaction observed inhemolytic disease states may contribute to diffuse microvascularthrombosis in various organ systems to include the eye. 7Central Retinal Vein OcclusionRetinal vein occlusion includes branch retinal vein occlusionand central retinal vein occlusion. Following diabeticretinopathy, retinal vein occlusion is the second most commonsight-threatening retinal vascular disorder. The prevalence ofCRVO in the <strong>United</strong> <strong>States</strong> has been reported to be 1 per 1000and is slightly more common in men than in women. 5The majority of people diagnosed with CRVO areover the age of 50. The most common symptom of CRVO isacute and persistent monocular visual loss. Patients characteristicallypresent with an abrupt, painless, unilateral loss ofvision of variable severity. CRVO is generally categorized asischemic or nonischemic. The hallmark fundus finding ofCRVO is four-quadrant retinal hemorrhage. The more commonnonischemic form has good perfusion to the retina andrelatively good visual acuity on presentation. Vision may returnto normal if not decreased by persistent macular edema.Nonischemic CRVO can progress to ischemic CRVO, withone-third of nonischemic cases progressing to ischemic withina year. Frequent follow-up is needed to monitor for thischange. Patients can also have ischemic CRVO on initial presentationwith visual acuity typically 20/400 or worse. IschemicCRVO typically presents with more extensive retinal hemorrhage,cotton wool spots, disc edema, and often an afferentpupillary defect. Intravenous fluorescein angiogram is commonlyused to help define the level of retinal non-perfusion inCRVO. Vision loss in ischemic CRVO may result from ganglioncell ischemia, macular edema, or neovascular complicationswith secondary glaucoma.Although CRVO can occur without a known underlyingcause, it is often associated with systemic disease (atherosclerosis,autoimmune disease, diabetes, hypertension,intravenous drug abuse, renal insufficiency, tobacco use, vasculitis)or local pathology (ocular trauma, orbital abscess, orbitaltumor, glaucoma). 5,8 When CRVO occurs in youngerpatients it is often associated with blood dyscrasias such as coagulationdisorders and hyperviscosity syndromes.Sickle cell disease has been associated with a hypercoagulablestate. 7 Given the hyperviscosity and vaso-occlusivetendencies of individuals with sickle cell crisis, 9 it isinteresting that only one case of CRVO in a sickle cell patienthas been reported in the literature. 10 Additionally, it is notablethat in this sickle cell case report, a comorbid protein S deficiencymay have contributed to the ultimate CRVO pathogenesis.Furthermore, an extensive review of the medicalliterature also detected only one article describing CRVO incidencein G6PD-deficient patients. 4 However, this article postulatedprotection against CRVO in Sardinian G6PD-deficientpatients with the Mediterranean variant. The investigators inthis study cited a 3.55% incidence of CRVO in their G6PDdeficientpopulation versus a 10-15% incidence of CRVO intheir general population. Not stated in this article was the riskof CRVO development in a G6PD-deficient individual with anactive oxidative stressor.Treatment of CRVO has historically been directed towardthe management of the contributing or associated systemicmedical problem, as few treatments have had provenefficacy in the treatment of CRVO. Treatment options includeaspirin, non-steroidal anti-inflammatory drugs, plasmapheresis,anticoagulation, fibrinolytics, and systemic corticosteroids.Anti-platelet agents are frequently prescribed; however, theirefficacy is controversial. Panretinal photocoagulation is usedfor patients experiencing neovascular complications to reduceor reverse angiogenesis and avoid the development of neovascularglaucoma.Additional treatment options with improved efficacyhave recently become available. Intravitreal triamcinolone hasproven effective in reducing edema and improving vision forpatients with macular edema, 11,12 and is more likely to be efficaciousin patients without ischemic CRVO or diabetes. However,these patients sometimes have rebound symptoms andrequire continued treatment.A new approach to treating CRVO is the use of intravitrealbevacizumab. 13 Elevated levels of vascular endothelialgrowth factor (VEGF) have been found in CRVO andhave been positively correlated with the onset and progressionPreviously Published 61
- Page 1 and 2:
Volume 9, Edition 3 / Summer 09 Jou
- Page 3 and 4:
An 18D deworms a camel during a “
- Page 5 and 6:
Field Evaluation and Management of
- Page 7 and 8:
The circumferential anchoring strip
- Page 9 and 10:
In doing so, all the skin is closed
- Page 11 and 12:
NATO SOF Transformation and theDeve
- Page 13 and 14: current and future operations, thes
- Page 15 and 16: sion of a physician, and limited pr
- Page 17 and 18: REFERENCES1. James L. Jones, “A b
- Page 19 and 20: This article is the first of two me
- Page 21 and 22: Figure 4 : A Special Forces medic c
- Page 23 and 24: exposure. Conversely, the customary
- Page 25 and 26: 7. Ted Westmoreland. (2006). Attrib
- Page 27 and 28: first three days of injury, althoug
- Page 29 and 30: 9. Markgraf CG, Clifton GL, Moody M
- Page 31 and 32: the only sign of OCS may be elevate
- Page 33 and 34: E. The canthotomy allows for additi
- Page 35 and 36: 33. Rosdeutscher, J.D. and Stradelm
- Page 37 and 38: Tinnitus, a Military Epidemic:Is Hy
- Page 39 and 40: The development of chronic NIHL pro
- Page 41 and 42: supplied by diffusion. During expos
- Page 43 and 44: similar to those of other authors,
- Page 45 and 46: promising effect on tinnitus. Howev
- Page 47 and 48: ADDITIONAL REFERENCESHoffmann, G; B
- Page 49 and 50: et al. demonstrated that both right
- Page 51 and 52: TYPICAL CHEST RADIOGRAPH FINDINGS I
- Page 53 and 54: 11. Norsk P, Bonde-Petersen F, Warb
- Page 55 and 56: ABSTRACTS FROM CURRENT LITERATUREMa
- Page 57 and 58: tourniquet times are less than 6 ho
- Page 59 and 60: tal from July 1999 to June 2002. In
- Page 61 and 62: Operation Sadbhavana: Winning Heart
- Page 63: CENTRAL RETINAL VEIN OCCLUSION IN A
- Page 67 and 68: AUTHORS*75th Ranger Regiment6420 Da
- Page 69 and 70: Casualties presenting in overt shoc
- Page 71 and 72: PSYCHOLOGICAL RESILIENCE AND POSTDE
- Page 73 and 74: spondents without PTSD (M = 4.6, SD
- Page 75 and 76: patients, whereas the mean score of
- Page 77 and 78: 29. Whealin JM, Ruzek JI, Southwick
- Page 79 and 80: average, time between return from d
- Page 81 and 82: ing functioning in both PTSD (Zatzi
- Page 83 and 84: Editorial Comment on “Psychologic
- Page 85 and 86: Blackburn’s HeadhuntersPhilip Har
- Page 87 and 88: The Battle of Mogadishu:Firsthand A
- Page 89 and 90: Task Force Ranger encountered enemy
- Page 91 and 92: Peter J. Benson, MDCOL, USACommand
- Page 93 and 94: Numerous military and civilian gove
- Page 95 and 96: Anthony M. Griffay, MDCAPT, USNComm
- Page 97 and 98: This is a great read that speaks di
- Page 99 and 100: and twenty-eight. Rabies immune glo
- Page 101 and 102: Rhett Wallace MD FAAFPLTC MC SFS DM
- Page 103 and 104: LTC Craig A. Myatt, Ph.D., HQ USSOC
- Page 105 and 106: LTC Bill Bosworth, DVM, USSOCOM Vet
- Page 107 and 108: Europe, Mideast, Africa and SWAU.S.
- Page 109 and 110: SOF and SOF Medicine Book ListWe ha
- Page 111 and 112: TITLE AUTHOR ISBNCohesion, the Key
- Page 113 and 114: TITLE AUTHOR ISBNI Acted from Princ
- Page 115 and 116:
TITLE AUTHOR ISBNRats, Lice, & Hist
- Page 117 and 118:
TITLE AUTHOR ISBNThe Healer’s Roa
- Page 119 and 120:
TITLE AUTHOR ISBNGuerilla warfare N
- Page 121 and 122:
TITLEAUTHORBlack Eagles(Fiction)Bla
- Page 123 and 124:
TITLE(Good section on Merrill’s M
- Page 125 and 126:
GENERAL REFERENCESALERTS & THREATSB
- Page 127 and 128:
Aviation Medicine Resources: http:/
- Page 129 and 130:
LABORATORYClinical Lab Science Reso
- Page 131 and 132:
A 11 year old boy whose tibia conti
- Page 133 and 134:
Meet Your JSOM StaffEXECUTIVE EDITO
- Page 135 and 136:
Special Forces Aidman's PledgeAs a