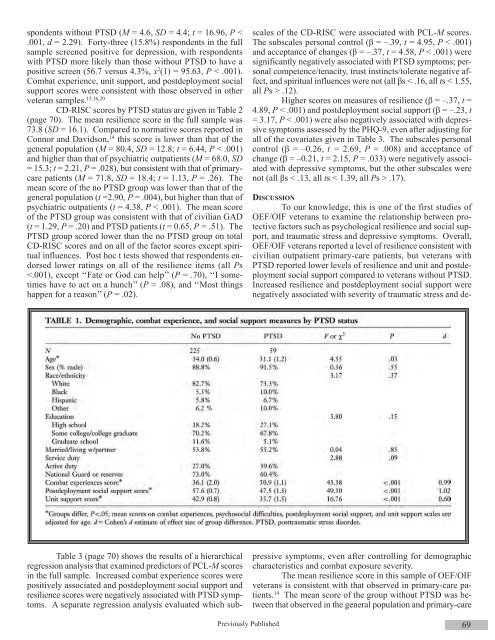
ate). A reminder postcard was sent 1 week after the surveyswere mailed. Respondents were older than nonrespondents inthe sampling frame (33.4 versus 31.3 years, t52.87, P5.004).On average, surveys were completed 26.9 months (standarderror of the mean [SEM] 5.7) following return from deployment.Institutional review boards of the Yale University, theCentral Connecticut State University, and the VA ConnecticutHealthcare System approved the study.ASSESSMENTSThe Connor–Davidson Resilience Scale (CD-RISC 14 )is a 25-item self-report assessment of psychological resilience.Items are scored on a 5-point range: ‘‘0’’ for ‘‘Not true at all,’’‘‘1’’ for ‘‘Rarely true,’’ ‘‘2’’ for ‘‘Sometimes true,’’ ‘‘3’’ for‘‘Often true,’’ and ‘‘4’’ for ‘‘True nearly all of the time.’’ Totalscores, which range from 0 to 100, and five subscales, whichwere generated using exploratory factor analysis in the initialvalidation study of this instrument, 14 are computed: (1) personalcompetence, (2) tolerance of negative affect and stressrelatedgrowth, (3) acceptance of changes, (4) personalcontrol, and (5) spiritual orientation to the future. In this sample,Cronbach’s α on CD-RISC items was .94.The Combat Experiences Scale (CES) is a 15-itemself-report instrument from the Deployment Risk and ResilienceInventory (DRRI, 15,16 available upon request from:http://www.ncptsd.va.gov/ncmain/ assessment/assessmt_request_form.html).It assesses exposure to combat, such as firinga weapon, being fired on by enemy or friendly fire, andwitnessing injury and death. Higher scores represent greatercombat exposure. A previous validation study in OIF veteransfound that CES scores correlated positively with measures ofPTSD and depression symptoms and negatively with mentalhealth functioning. 16 In this sample, Cronbach’s a on CESitems was .93.The Posttraumatic Stress Disorder Checklist—MilitaryVersion (PCLM 17 ) is a 17-item screening instrument basedon diagnostic criteria for PTSD. Respondents who scored >50and who met B, C, and D criteria for PTSD were identified asscreening positive for PTSD. This definition provides a conservativeestimate of the prevalence of PTSD, which correspondsto Diagnostic and Statistical Manual of MentalDisorders—Fourth Edition criteria for PTSD. Cronbach’s αon PCL-M items was .96.The Patient Health Questionnaire—9 (PHQ-9 18 ) is anine-item self-report screening instrument for depression derivedfrom the clinician-administered Primary Care Evaluationof Mental Disorders. Higher scores indicate greaterdepressive symptoms, with scores > 15 indicating a positivescreen for depression. Cronbach’s α on these items was .92.The Unit Support Scale (USS) is a 12-item self-reportinstrument from the DRRI 15,16 that assesses the amount of assistanceand encouragement in the war zone from unit leadersand members, and the military in general. Questions include,‘‘My unit was like a familyto me,’’ ‘‘My superiors made a real attempt to treat me as aperson,’’ and ‘‘I could go to most people in my unit for helpwhen I had a personal problem.’’ A validation study in GulfWar veterans found that scores on the USS correlate negativelywith measures of PTSD, depression, and anxiety. 15 Inthis sample, Cronbach’s α on USS items was .93.The Postdeployment Social Support Scale (PSSS) is a15-item selfreport measure from the DRRI 15,16 that assessespostdeployment emotional support and instrumental assistanceprovided by family, friends, coworkers, employers, and community.Validation studies in OIF and Gulf War veterans foundthat PSSS scores correlated negatively with measures ofPTSD, depression, and physical symptoms and positively withmeasures of physical, mental, and cognitive functioning. 15,16In this sample, Cronbach’s α on these items was .82.DATA ANALYSISLogarithmic base 10 transformations were used totransform nonnormally distributed continuous variables (e.g.,PCL-M scores) prior to analysis. Demographic characteristicswere compared using independent-samples t tests and x 2 tests.Scores on each of the CDRISC items by PTSD status werecompared using univarate analyses of covariance (two-tailed,α 5.05) with demographic variables that differed between thegroups entered as covariates. Cohen’s d values ([Meangroup1_ Mean group2 ]/pooled standard deviation) were computedto estimate effect sizes of group differences. 19 Post hoc t testswere used to compare total CD-RISC scores to norms reportedin Connor and Davidson 14 and to examine group differenceson individual CD-RISC items, with P < .01 considered significantin the latter analyses.Hierarchical regression analyses were conducted toexamine predictors of traumatic stress and depressive symptomseverity. All respondents, including those with and withoutPTSD and with and without positive screens fordepression, were included in these analyses. Continuousscores on the PCL-M and PHQ-9 were entered as dependentvariables in separate analyses. Variables hypothesized to berelated to PTSD and depressive symptoms were entered as independentvariables. Step 1 included demographic variables(age, sex, race/ethnicity, education, relationship status, dutytype: active versus reserve), Step 2 included a measure of combatexposure (CES), and Step 3 included potentially protectivefactors (USS, PSSS, CDRISC). Complete data were availablefor 255 respondents.RESULTSDEMOGRAPHIC CHARACTERISTICS, COMBAT EXPERIENCESEVERITY, AND PSYCHOSOCIAL MEASURESIn the full sample, mean age was 34.9 (SE = .4), 89.4%were white, 82.4% completed at least some college education,27.8% were active duty, and 72.2% were in the National Guardor Reserves: 87.4% were in the Army, 9.1% Marines, 2.2% AirForce, and 1.3% multiple branches. Demographic characteristicsand scores on combat experience and psychosocial measuresby PTSD status are given in Table 1. The PTSD groupwas younger than the no PTSD group, but did not differ bysex, race/ethnicity, education, relationship status, and servicetype. They scored higher on the CES (large effect size), andlower on the postdeployment social support (large effect size)and unit support (medium effect size) measures.Mean PCL-M scores were 35.9 (SD = 18.0) for the fullsample, 64.3 (SD = 10.2) for respondents with PTSD, and 27.8(SD = 9.7) for respondents without PTSD. Mean PHQ-9scores were 7.3 (SD = 6.9) for the full sample, with respondentswith PTSD (M = 16.5, SD = 5.9) scoring higher than re-68Journal of <strong>Special</strong> <strong>Operations</strong> Medicine Volume 9, Edition 3 / <strong>Summer</strong> 09
spondents without PTSD (M = 4.6, SD = 4.4; t = 16.96, P .17).DISCUSSIONTo our knowledge, this is one of the first studies ofOEF/OIF veterans to examine the relationship between protectivefactors such as psychological resilience and social support,and traumatic stress and depressive symptoms. Overall,OEF/OIF veterans reported a level of resilience consistent withcivilian outpatient primary-care patients, but veterans withPTSD reported lower levels of resilience and unit and postdeploymentsocial support compared to veterans without PTSD.Increased resilience and postdeployment social support werenegatively associated with severity of traumatic stress and depressivesymptoms, even after controlling for demographiccharacteristics and combat exposure severity.The mean resilience score in this sample of OEF/OIFveterans is consistent with that observed in primary-care patients.14 The mean score of the group without PTSD was betweenthat observed in the general population and primary-carePreviously Published 69
- Page 1 and 2:
Volume 9, Edition 3 / Summer 09 Jou
- Page 3 and 4:
An 18D deworms a camel during a “
- Page 5 and 6:
Field Evaluation and Management of
- Page 7 and 8:
The circumferential anchoring strip
- Page 9 and 10:
In doing so, all the skin is closed
- Page 11 and 12:
NATO SOF Transformation and theDeve
- Page 13 and 14:
current and future operations, thes
- Page 15 and 16:
sion of a physician, and limited pr
- Page 17 and 18:
REFERENCES1. James L. Jones, “A b
- Page 19 and 20:
This article is the first of two me
- Page 21 and 22: Figure 4 : A Special Forces medic c
- Page 23 and 24: exposure. Conversely, the customary
- Page 25 and 26: 7. Ted Westmoreland. (2006). Attrib
- Page 27 and 28: first three days of injury, althoug
- Page 29 and 30: 9. Markgraf CG, Clifton GL, Moody M
- Page 31 and 32: the only sign of OCS may be elevate
- Page 33 and 34: E. The canthotomy allows for additi
- Page 35 and 36: 33. Rosdeutscher, J.D. and Stradelm
- Page 37 and 38: Tinnitus, a Military Epidemic:Is Hy
- Page 39 and 40: The development of chronic NIHL pro
- Page 41 and 42: supplied by diffusion. During expos
- Page 43 and 44: similar to those of other authors,
- Page 45 and 46: promising effect on tinnitus. Howev
- Page 47 and 48: ADDITIONAL REFERENCESHoffmann, G; B
- Page 49 and 50: et al. demonstrated that both right
- Page 51 and 52: TYPICAL CHEST RADIOGRAPH FINDINGS I
- Page 53 and 54: 11. Norsk P, Bonde-Petersen F, Warb
- Page 55 and 56: ABSTRACTS FROM CURRENT LITERATUREMa
- Page 57 and 58: tourniquet times are less than 6 ho
- Page 59 and 60: tal from July 1999 to June 2002. In
- Page 61 and 62: Operation Sadbhavana: Winning Heart
- Page 63 and 64: CENTRAL RETINAL VEIN OCCLUSION IN A
- Page 65 and 66: of the X chromosome. Notable is tha
- Page 67 and 68: AUTHORS*75th Ranger Regiment6420 Da
- Page 69 and 70: Casualties presenting in overt shoc
- Page 71: PSYCHOLOGICAL RESILIENCE AND POSTDE
- Page 75 and 76: patients, whereas the mean score of
- Page 77 and 78: 29. Whealin JM, Ruzek JI, Southwick
- Page 79 and 80: average, time between return from d
- Page 81 and 82: ing functioning in both PTSD (Zatzi
- Page 83 and 84: Editorial Comment on “Psychologic
- Page 85 and 86: Blackburn’s HeadhuntersPhilip Har
- Page 87 and 88: The Battle of Mogadishu:Firsthand A
- Page 89 and 90: Task Force Ranger encountered enemy
- Page 91 and 92: Peter J. Benson, MDCOL, USACommand
- Page 93 and 94: Numerous military and civilian gove
- Page 95 and 96: Anthony M. Griffay, MDCAPT, USNComm
- Page 97 and 98: This is a great read that speaks di
- Page 99 and 100: and twenty-eight. Rabies immune glo
- Page 101 and 102: Rhett Wallace MD FAAFPLTC MC SFS DM
- Page 103 and 104: LTC Craig A. Myatt, Ph.D., HQ USSOC
- Page 105 and 106: LTC Bill Bosworth, DVM, USSOCOM Vet
- Page 107 and 108: Europe, Mideast, Africa and SWAU.S.
- Page 109 and 110: SOF and SOF Medicine Book ListWe ha
- Page 111 and 112: TITLE AUTHOR ISBNCohesion, the Key
- Page 113 and 114: TITLE AUTHOR ISBNI Acted from Princ
- Page 115 and 116: TITLE AUTHOR ISBNRats, Lice, & Hist
- Page 117 and 118: TITLE AUTHOR ISBNThe Healer’s Roa
- Page 119 and 120: TITLE AUTHOR ISBNGuerilla warfare N
- Page 121 and 122: TITLEAUTHORBlack Eagles(Fiction)Bla
- Page 123 and 124:
TITLE(Good section on Merrill’s M
- Page 125 and 126:
GENERAL REFERENCESALERTS & THREATSB
- Page 127 and 128:
Aviation Medicine Resources: http:/
- Page 129 and 130:
LABORATORYClinical Lab Science Reso
- Page 131 and 132:
A 11 year old boy whose tibia conti
- Page 133 and 134:
Meet Your JSOM StaffEXECUTIVE EDITO
- Page 135 and 136:
Special Forces Aidman's PledgeAs a