PARATHYROID AND THYROID IMAGING - Neuroradiology
PARATHYROID AND THYROID IMAGING - Neuroradiology
PARATHYROID AND THYROID IMAGING - Neuroradiology
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
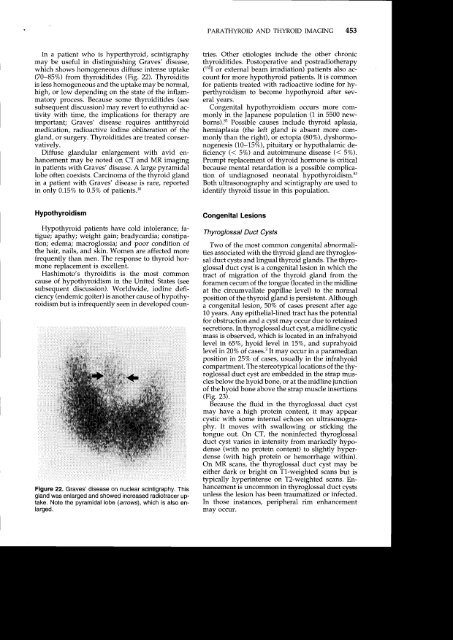
<strong>PARA<strong>THYROID</strong></strong> <strong>AND</strong> <strong>THYROID</strong> <strong>IMAGING</strong> 453In a patient who is hyperthyroid, scintigraphymay be useful in distinguishing Graves' disease,which shows homogeneous diffuse intense uptake(70-85%) from thyroidltides (FiB. 22). Thyroiditisis less homogeneous and the uptake may be normal,high, or low depending on the state of the inflammatoryprocess. Because some thyroiditides (seesubsequent discussion) may revert to euthyroid activitywith time, the implications for theiapy areimportant; Graves' disease requires antithyroidmedication, radioactive iodine obliteration of thegland, or surgery. Thyroiditides are treated conservatively.Diffuse glandular enlargement with avid enhancementmay be noted on CT and MR imagingin patients with Graves' disease. A large pyramidallobe often coexists. Carcinoma of the thyroid glandin a patient with Graves' disease is rare, reportedin only 0.157o to 0.5Vo of patients.l0tries. Other etiologies include the other chronicthyroiditides. Postoperative and postradiotherapy(131I or external beam irradiation) patients also accountfor more hypothyroid patients. It is commonfor patients treated with radioactive iodine for hyperthyroidismto become hypothyroid after severaryears.Congenital hypothyroidism occurs more commonlyin the Japanese population (1 in 5500 newborns).83Possible causes include thyroid aplasia,hemiaplasia (the left gland is absent more commonlythan the right), or ectopia (80%), dyshormonogenesis(10-1,5%), pituitary or hypothalamic deficiency(< 5%) and autoimmune disease (< SVo).Prompt replacement of thyroid hormone is criticalbecause mental retardation is a possible complicationof undiagnosed neonatal hypothyroidism.83Both ultrasonography and scintigraphy are used toidentify thyroid tissue in this population.HypothyroidismHypothyroid patients have cold intolerance; fatigue;apathy; weight gain; bradycardia; constipation;edema; macroglossia; and poor condition ofthe hair, nails, and skin. Women are affected morefrequently than men. The response to thyroid hormonereplacement is excellent.Hashimoto's thyroiditis is the most commoncause of hypothyroidism in the United States (seesubsequent discussion). Worldwide, iodine deficiency(endemic goiter) is another cause of hypothyroidismbut is infrequently seen in developed coun-Figure 22. Graves' disease on nuclear scintigraphy. Thisgland was enlarged and showed increased radiotracer uptake.Note the pyramidalobe (arrows), which is also enlarged.Congenital LesionsThyroglossal Duct CystsTwo of the most common congenital abnormalitiesassociated with the thyroid gland are thyroglossalduct cysts and lingual thyroid glands. The thyroglossalduct cyst is a congenital lesion in which thetract of migration of the thyroid gland from theforamen cecum of the tongue (located in the midlineat the circumvallate papillae level) to the normalposition of the thyroid gland is persistent. Althougha congenital lesion, 50% of cases present after age10 years. Any epithelial-lined tract has the potentialfor obstruction and a cyst may occur due to retainedsecretions. In thyroglossal duct cyst, a midline cysticmass is observed, which is located in an infrahyoidlevel in 65V", hyoid level in 1,5%, and suprahyoidlevel in 20Vo of cases.3 It mav occur in a paramedianposition in 25Vo of cases, usually in the infrahyoidcompartment. The stereotypical locations of the thyroglossalduct cyst are embedded in the strap musclesbelow the hyoid bone, or at the midline junctionof the hyoid bone above the strap muscle insertions(Fig. 23).Because the fluid in the thyroglossal duct cystmay have a high protein content, it may appearcystic with some internal echoes on ultrasonography.It moves with swallowing or sticking thetongue out. On CT, the noninfected thyroglossalduct cyst varies in intensity from markedly hypodense(with no protein content) to slightly hyperdense(with high protein or hemorrhage within).On MR scans, the thyroglossal duct cyst may beeither dark or bright on Tl-weighted scans but istypically hyperintense on T2-weighted scans. Enhancementis uncommon in thyroglossal duct cystsunless the lesion has been traumatized or infected.In those instances, peripheral rim enhancementmay occur.