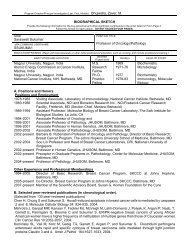
440 YOUSEMTable 2. MULTIPLE ENDOCRINE NEOPLASTA (MEN) SyNDROMESFeature MEN I MEN IIA MEN IIBEponymParathyroid abnormalityThyroid lesionPituitary lesionsPheochromocytomaOther manifestationsChromosomalinkageWermerHyperparathyroidism (90%)due to hyperplasia morecommonly than adenomaGoiter, adenomas,thyroiditis are rareAdenomas (20-30"/.)NoPancreatic islet celladenomas (insulinoma orgastrinoma) 30-35%Adrenal codex adenomasor carctnomasRarely glucagonomas,VlPomas, carcinoidZollinger-Ellison syndromeA-D chromosome 11SippleParathyroid hyperplasia in20-300/0Medullary thyroid carcinomaNoYesA-D chromosome 10Mucosal neuroma syndromeVery rareMedullary thyroid carcinomaNoYesMucocutaneous neuromasMarfanoid faciesCafe au lait spotsA-D. chromosome 10perplasia accounts lor 727o to 75% of patients withhyperparathyroidism.CT is- Leported to have a sensitivity rate of 457oto 88%s'! ultrasonography, 307o to 697o20,21,35,58,n.and MR imaging, 40Vo to 63Va58'76 for detecting hyperplasticglands. Parathyroid hyperplasia is detectedin43%to 657o of cases with thallium subtractionand 55% to 75% with ee-Tc sestamibi.20,21,53, s8' e3The added accuracy in identifying hyperplasticglands has led to a growing consensus in supportof the use of ee^Tc sestamibi as the optimal agentfor p-alathyroid adenoma and hyperplasia localization.53,5480Parathyroid CarcinomaOf all patients with hyperparathyroidism, the incidenceof parathyroid carcinoma (Fig. 5) is onlyFigure 5. MR image of parathyroid carcinoma. A large softtissue mass (arrows) is seen anterolateral to the tracheaon the left side. The mass seems to be invading the inferiorplatysma-sternocleidomastoid musculature and invades ajugular vein (J). Histopathologically, this was a parathyroidcarcinoma.7% to 2%, although parathyroid carcinoma causeshyperparathyroidism in 85Va to 90Vo of cases.3e,aoMetastases to lymph nodes occur in one third ofcases, and distant metastases in27Vo to287a ofpatients.Men and women are affected eouallv.Edmonson and colleagues noted thai a paratnyroidcarcinoma may have the same sonographic appearanceas a benign large adenoma (hypoechoicwith or without heterogeneity); only the presenceof local invasion into the thyroid gland, muscles orvessels, or nodal metastases would suggest this diagnosis.l3Parathyroid carcinomas have been reported toaccumula te oo'Tc sestamibi.L alReoperation for HyperparathyroidismDuring reoperation of previously operated cases,307o to 75% of abnormal parathyroid glands arefound in a perithyroidal location, presumablyoverlooked or missed during the initial operation.12'4s'46'61Parathyroid adenomas in patients whohave failed initial operation are located in the anteriormediastinum in 20Vo to 38V0, in a paraesophagealor deep cervical location in approxim ately 20Va,intrathyroidal in 8Vo, and parathymic in 2Vo.45' 46' 61Supernumerary adenomatous glands are present in15% of cases. Of those located in the chest, posteriormediastinal ectopic adenomas are one-fifth as commonas anterior ones.sThe risks associated with reoperation outweighthe cost of preoperative imaging. In those patientswho are reoperated, the risk of vocal-cord injurybecause of damage to the recurrent laryngeal nerv-eor vagus nerve is approximately 77o compared withthe initial operating room risk of 1..3%.a6 When imagingis not performed prior to reoperation for hyperparathyroidism,surgery is approximately 60Voto707o successful; when imaging is performed prior
<strong>PARA<strong>THYROID</strong></strong> <strong>AND</strong> <strong>THYROID</strong> <strong>IMAGING</strong> 441to reoperation, the success rate increases to 80%to 90%.58 In reoperated cases, the sensitivities ofultrasonography (36-7 6V"),'n'45' 58' 77scintigr aphy (26-g0 vo), z+, +s,so, sa cT (45_ 63%),24,4s,s8, 77 and MR imaging(50-91Vo)'n'"'n5'56's8 have ranged widely. In a reviewof the literature, Price concluded that MR imagingwas the best cross-sectional imaging study to performin this scenario, and nuclear scintigraphy thebest functional examination.s8 The latest figures onsestamibi scintigraphy have shown sensitivities inthe range of 80% to90Vo.a1'e2Parathyroid hyperplasiais the most difficult diagnosis to make and accountsfor most false-negative studies.al e2 Nonetheless,Majors and colleagues found that sestamibi scanningidentified parathyroid tissue in all nine previouslyoperated patients, including one with parathyroidcancer.*tBy combining ultrasonography, CT, and scintigraphy,one can increase the sensitivity rate to 78%,but at a high cost.as Although more invasive studieshave a greater yield, they are more demanding.Miller and colleagues' study found parathyroid venoussampling (80Vo), intraoperative ultrasonography(787"), and arteriography (49-60Vo) Io havehigher sensitivity rates than the noninvasive imagingstudies.aa The expense and technical difficultyin performing these invasive examinations precludestheir routine use, but they may be held inabeyance for cases with equivocal or nonrevealing,noninvasive sfudies.In the patient who has failed prior surgery for aparathyroid adenoma, both imaging and surgerymust contend with scar tissue in and around thethyroid glands, a loss of tissue planes, postoperativeinflammation, lymphadenopathy simulating parathyroidadenomas, and distortion of landmarks.False-negative scans (caused by obscured anatomy)tend to occur in the perithymic or perithyroidaloperative beds. The incidence of false-positive examinations(usually caused by lymphadenopathy)is lowest with nuclear medicine studies, followedby MR imaging, ultrasonography, and CT accordingto Miller and colleagues.asTherefore, which study should one perform in thepreviously operated patient? Two camps of opinionhave formed. Sestamibi scintigraphy is probably themost accurate and affordable studv currentlv availableto identify parathyroid adenomas; its disadvantageis that the surrounding anatomy is not visualizedfor surgical orientation. It alone or combinedwith ultrasonography or CT is an effective option.Alternatively, the most accurate (and most expensive)cross-sectional imaging technique is MR imaging,which provides good anatomic detail, althoughit has the small risk of mistaking a lymphnode for an adenoma. Because re-reoperation is ananathema to the surgeon, multiple studies are notuncommonly performed if one is not definitive. Theidea of using a morphologic test (CT, ultrasonography,or MR imaging) and a functional test (ee-Tcsestamibi) is appealing. Use of this algorithm in-creases the reoperation success rate by more than30%.16Secondary and TertiaryHyperparathyroidismThe evaluation of patients with secondary ortertiary hyperparathyroidism is rarely centeredaround the parathyroid glands because the kidneysare the source ofabnormality in these diseases. Parathyroidglandular hyperplasia usually occurs in associationwith chronic renal failure and renal osteodystrophy.e-Tc sestamibi has been able to identifybilateral uptake in hyperplastic glands and residualparathyroid tissue in those individuals treated surgicallyin the neck for secondary hyperparathyroidism.e3Therapeutic TechniquesEthanol ablation of parathyroid adenomas hasbeen performed under ultrasound guidance by percutaneousinjection of absolute ethanol.sl' 71' 8e Thistechnique may be used in patients with primary orsecondary hyperparathyroidism who are not surgicalcandidates because of medical illnesses. Approximately0.5 mL to 1 mL of ethanol (95Vo) may beinjected at multiple sites within an adenoma witha22-gauge needle. The success of this technique ismonitored by following serial serum calcium levels;the technique may be repeated until normocalcemiais achieved.Parathyroid CystsCysts of the parathyroid glands are more commonin women than in men and mav be presentin the neck (Fig. 6) or anterior mediastinum. Atpresentation, they may be very large in size, andthe differential diagnosis may include thyroid cysts,thymic cysts, and necrotic lymph nodes. They usuallyarise in the region of the inferior pole of thethyroid gland. They are virtually never found inchildren; most cases present in the fourth and fifthdecade of life.a0 They are usually unilocular, large,and may have hyperproteinaceous contents yieldinghigh intensity on Tl-weighted MR scans. Theetiology may be congenital because of remnants ofpharyngeal pouches, or cysts may develop fromdegenerated parathyroid adenomas.HypoparathyroidismThe most common cause of hypoparathyroidismis iatrogenic removal of all functioning parathyroidtissue during surgery for hyperparathyroidism orthyroid disease. Primary idiopathic hypoparathy-