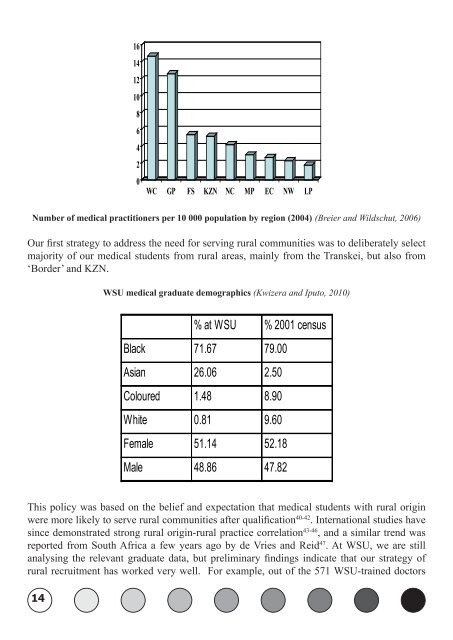
14 16 14 12 10 8 6 4 2 0 WC GP FS KZn nC MP EC nW LP Number <strong>of</strong> medical practitioners per 10 000 popul<strong>at</strong>ion by region (2004) (Breier and Wildschut, 2006) Our first str<strong>at</strong>egy to address the need for serving rural communities was to deliber<strong>at</strong>ely select majority <strong>of</strong> our medical students from rural areas, mainly from the Transkei, but also from ‘Border’ and KZN. <strong>WSU</strong> medical gradu<strong>at</strong>e demographics (Kwizera and Iputo, 2010) % <strong>at</strong> W SU % 2001 census Black 71.67 79.00 Asian 26.06 2.50 Coloured 1.48 8.90 W hite 0.81 9.60 Female 51.14 52.18 Male 48.86 47.82 This policy was based on the belief and expect<strong>at</strong>ion th<strong>at</strong> medical students with rural origin were more likely to serve rural communities after qualific<strong>at</strong>ion 40-42 . Intern<strong>at</strong>ional studies have since demonstr<strong>at</strong>ed strong rural origin-rural practice correl<strong>at</strong>ion 43-46 , and a similar trend was reported from South Africa a few <strong>years</strong> ago by de Vries and Reid 47 . At <strong>WSU</strong>, we are still analysing the relevant gradu<strong>at</strong>e d<strong>at</strong>a, but preliminary findings indic<strong>at</strong>e th<strong>at</strong> our str<strong>at</strong>egy <strong>of</strong> rural recruitment has worked very well. For example, out <strong>of</strong> the 571 <strong>WSU</strong>-trained <strong>doctors</strong>
who, as <strong>of</strong> 2009 were in independent practice (i.e. were neither in Community Service nor in Internship) 242 (42.38%) were practicing in the Eastern Cape. At least a third <strong>of</strong> these were in rural areas and the majority <strong>of</strong> those in or near large urban areas had their practices in the townships 48 . This preliminary finding not only s<strong>how</strong>s th<strong>at</strong> we are meeting a cardinal UNITRA Council Guideline, but it also vindic<strong>at</strong>es us on our policy <strong>of</strong> deliber<strong>at</strong>e rural recruitment. More excitingly, I am almost certain th<strong>at</strong> once the d<strong>at</strong>a has been fully analysed, we are going to report one the highest provincial and n<strong>at</strong>ional gradu<strong>at</strong>e retention r<strong>at</strong>es by medical schools in this country. Another curriculum factor th<strong>at</strong> has been propounded as promoting medical gradu<strong>at</strong>es’ choice <strong>of</strong> rural careers is their rural exposure during undergradu<strong>at</strong>e <strong>training</strong> 49-53 . In our settings, we are a rural institution, and our <strong>training</strong> is therefore, intrinsically a continuous rural exposure 28 . We <strong>how</strong>ever, did not want to complacently make this assumption, and we deliber<strong>at</strong>ely incorpor<strong>at</strong>ed a significant (rural) community-based component into our undergradu<strong>at</strong>e curriculum; which has been amply described in various public<strong>at</strong>ions from this institution 54-58 . Unlike the strong correl<strong>at</strong>ion between rural origin-rural career choices, <strong>how</strong>ever, the impact <strong>of</strong> rural placement or exposure per se is less prominent and more variable, partly because the practice is rel<strong>at</strong>ively recent and there is no standardised implement<strong>at</strong>ion among different institutions 59 , and partly due to the presence many confounding variables, some <strong>of</strong> which can not be easily controlled for 53, 59 . Nonetheless our experience from Exit Surveys <strong>of</strong> final year students in 2001, 2002 and in 2005, 2006 (6 and 5 year programmes, respectively), is th<strong>at</strong> 37.7% reported th<strong>at</strong> communitybased clinical <strong>training</strong> was better than in other settings (e.g. tertiary teaching hospitals), 18.4% thought it was somewh<strong>at</strong> better, 30.6% felt it was about the same as other settings, and 4.1% and 2.0% said it was somewh<strong>at</strong> worse, and worse, respectively 24 . Regarding the equipping our medical undergradu<strong>at</strong>es with “the necessary scientific and pr<strong>of</strong>essional knowledge, skills and <strong>at</strong>titudes”, we were the first medical school in sub-Saharan Africa to implement an innov<strong>at</strong>ive curriculum based on the ‘SPICES’ model 60 –i.e. Student-centred, using Problembased learning (PBL), Integr<strong>at</strong>ed, Community-based, with provision for Electives and planned so as to be System<strong>at</strong>ic. When developing this curriculum, we drew different aspects from different medical schools in Australia, Middle East, Europe, and North America which were already practitioners <strong>of</strong> innov<strong>at</strong>ive curricula, and we adapted these aspects to suit and serve our settings and needs, respectively. In the process, we also forged useful and lasting partnerships with some <strong>of</strong> these institutions, e.g. the <strong>University</strong> <strong>of</strong> Newcastle in Australia and Bowman Grey <strong>University</strong> in USA. Our PBL curriculum has been extensively described 4, 7, 61-64 , monitored 8, 10-12, 65 , reviewed 66 and evalu<strong>at</strong>ed 9, 11, 24, 29, 65, 67-71 ; the l<strong>at</strong>ter including rigorous accredit<strong>at</strong>ion visits by the Health Pr<strong>of</strong>essions Council <strong>of</strong> South Africa (HPCSA) 71, 72 . In addition, we have followed-up all our gradu<strong>at</strong>es meticulously 9, 48 , and the clear picture th<strong>at</strong> has emerged from these processes is th<strong>at</strong>, notwithstanding our considerable constraints, we have produced, and we are producing well-trained, holistic, competent, and confident <strong>doctors</strong>, who have made a big contribution to healthcare in this region, province, and country <strong>at</strong> large. 15
- Page 1: Walter Sisulu University PROFESSORI
- Page 5 and 6: The Vice-Chancellor of Walter Sisul
- Page 7 and 8: it is for some today, my parents di
- Page 9 and 10: every evening! Then there were my
- Page 11 and 12: “It is therefore unreasonable to
- Page 13: fallen short of those Guidelines /
- Page 17 and 18: had 5.8% of our graduates, while Fr
- Page 19 and 20: us refine our fulfilment of the abo
- Page 21 and 22: how this is done. I am sure that ev
- Page 23 and 24: in this regard the two gender group
- Page 25 and 26: My grumbling aside, Mr VC Sir, I th
- Page 27 and 28: Medicine, and say: “To those of y
- Page 29 and 30: Bagumah, Dan Ncayiyana, Khaya Mfeny
- Page 31 and 32: REFEREnCES 1. JAMES C. Unreliable M
- Page 33 and 34: 25. KWIZERA EN, NGANWA-BAGUMAH AB,
- Page 35 and 36: 53. KAYE DK, MWANIKA A, SEWANKAMBO
- Page 37: 88. STROBEL J, van BARNEVELD A. Whe
- Page 40 and 41: In 1985, Dr Kwizera was offered a C
- Page 48: 48 Design: Mthatha Health Resource