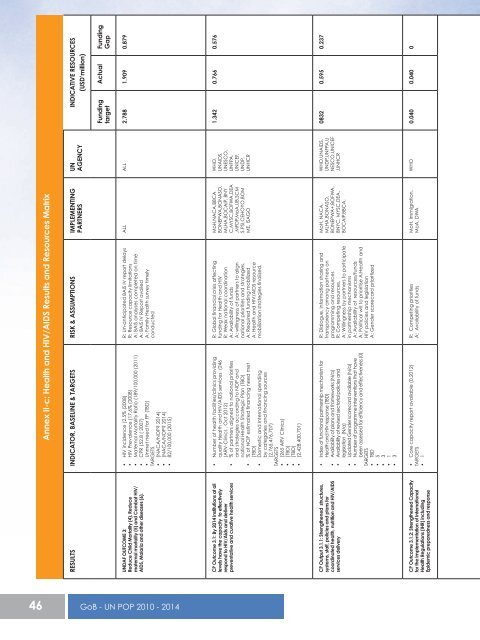
Annex II-c: Health and HIV/AIDS Results and Resources MatrixRESULTS INDICATOR, BASELINE & TARGETS RISK & ASSUMPTIONS IMPLEMENTINGPARTNERS<strong>UN</strong>AGENCYINDICATIVE RESOURCES(USD’million)FundingtargetActual FundingGap<strong>UN</strong>DAF OUTCOME 3:Reduce Child Mortality (4), Reducematernal mortality (5) and Combat HIV/AIDS, Malaria and other diseases (6).• HIV incidence (2.5% (2008)• HIV Prevalence (17.6% (2008)• Maternal Mortality Ratio (189/100,000 (2011)• CPR (52.8 ( 2007)• Unmet need for FP (TBD)TARGETS• (NACA/NOP? <strong>2014</strong>)• (NACA/NOP? <strong>2014</strong>)• 82/100,000 (2015)R: Un-anticipated BAIS IV report delaysR: Resource capacity limitationsA: BAIS analyses completed on timeA: BAIS IV Report availedA: Family Health survey timelyconductedALL ALL 2.788 1.909 0.879CP Outcome 3.1: By <strong>2014</strong> institutions at alllevels have the capacity to effectivelyrespond to HIV/Aids and deliverpreventative and curative health services• Number of health facilities/clinics providingquality Health and HIV/AIDS services (246(ARV-Clinics , Oct 2012)• % of partners aligned to national prioritiesand strategies according to NOP andnational Health Strategic Plan (TBD)• % of NOP estimated financing need met(TBD)• Domestic and International spendingby categories and financing sources(2,765,476,707)TARGETS• (265 ARV Clinics)• (TBD)• (TBD)• (2,428,400,701)R: Global financial crisis affectingfunding for Health and HIVR: Weak national coordinationA: Availability of fundsA: willingness of partners to alignnational priorities and strategies.A: Required funding mobilizedA: Health and HIV/AIDS resourcemobilization strategies finalized.MoH,NACA,BBCABONEPWA,BONASO,MLHA,BOCAIP, BNYC,MYSC,BOFWA,DEA,MFDP,MoA,UB,SCMS,PSI,CEHOYO,BOMME, ISAGOWHO,<strong>UN</strong>AIDS,<strong>UN</strong>ESCO,<strong>UN</strong>FPA,<strong>UN</strong>ICEF,<strong>UN</strong>DP,<strong>UN</strong>HCR1.342 0.766 0.576CP Output 3.1.1: Strengthened structures,systems, staff, policies and plans forcoordinated health, nutrition and HIV/AIDSservices delivery• Index of functional partnership mechanism forHealth and HIV response (TBD)• Availability of plans and frameworks (N/a)• Availability of revised sectorial policies andlegislation (N/a)• Updated Gender scorecard available (N/a)• Number of programme interventions that havebeen assessed for efficiency and effectiveness (0)TARGETS• TBD• 5• 3• 1• 3R: Dialogue, information sharing andtransparency among partners onprogramming and resourcesR: Competing resources.A: Willingness by partners to participatein partnership mechanismsA: Availability of resources/fundsA: Political will to prioritise A:Health andHIV policies and legislationA: Gender scorecard prioritizedMoH, NACA,MLHA,BONASO,BONEPWA+,BOFWA,BNYC, MYSC,DEA,BOCAIP,BBCA,WHO,<strong>UN</strong>AIDS,<strong>UN</strong>DP,<strong>UN</strong>FPA,<strong>UN</strong>ESCO,<strong>UN</strong>ICEF,<strong>UN</strong>HCR0832 0.595 0.237CP Outcome 3.1.2: Strengthened Capacityfor the implementation of InternationalHealth Regulations (IHR) includingEpidemic preparedness and response• Core capacity report available (0,2012)TARGETS• 1R: Competing prioritiesA: Availability of fundsMoH, Immigration,MoA, DWAWHO 0.040 0.040 046 <strong>GoB</strong> - <strong>UN</strong> <strong>POP</strong> <strong>2010</strong> - <strong>2014</strong>
CP Outcome 3.1.3: Strengthened capacityfor MOH, NACA and MLG &RD andcivil society to undertake routine datacollection, research, studies and surveys.CP Output 3.1.4: A responsive to demandsupply chain for health, nutrition and HIV/AIDS commodities in placeCP OUTCOME 3.2: Increased availabilityand demand for quality services forcommunicable and non-communicablediseases by 2016CP Output 3.2.1: Government institutionsincluding formal and non-formaleducations institutions , civil society, privatesector media and community basedorganisations have capacity to undertakepublic awareness, health promotion,management and monitoring andEvaluation of communicable and noncommunicablediseasesCP Output 3.2.2: Strengthened capacityfor Health sector to plan, implementand monitor Maternal and Child Healthprograms.CP Output 3.2.3: Access to both curativeand palliative care at cancer treatmentcenter by Cancer patients• Integrated District Health Information Systemfunctional (0)• Market research on condom access andutilization (0)TARGETS• 1• 1• Average No. of stock out days per yearfor RHCS, HIV test kits, ARVs at central anddistrict level (TBD)TARGETS• TBD• % population in malaria endemic districtsusing LLINS (49%, 2012)• % children under five sleeping under LLINS(12%, 2007).• % population protected by Indoor ResidualSpraying (IRS) (46%,2012).• STEPS III survey report available (0)• Mental Health programme review reportavailable (0)TARGETS• 90%• 90%• 90%• 1• 1• Proportion of confirmed malaria casesinvestigated (51%)• % of districts reporting cases to national levelwithin 24hrs (0)• MTR report of the Malaria strategic (MSP)plan undertaken (0)• Availability of a signed national joint planof action to implement the Librevilledeclaration (0)• Number of health facilities providingintegrated SRH and HIV information andservices (0, 2012).• GBV and HIV/AIDS linkages study(0,2008).TARGETS• 100%• 1• 1• 9• 1• Non-polio AFP rate (0/100,000)• Number of health personnel trained in EmOCper hospitals (1 health care worker per healthfacility,2012).• IMCI coverage (40% of trained personnel inhealth facilities)TARGETS• 2/100,000 yearly• 2 health providers per health facility• 60%• Number of new cases treatedTARGETS• About 1000 patients of the annual 1400 newcancer cases treated withthe potential of curing a significant proportion,especially cervical cancersR: Capacity for management ofStrategic Information at district level.A: Availability of TA /fundsA: Database developed in time.A: All partners willing to use singlereporting system.A: Approval by HR Developmentcommittee.R: Budget constraintsR: Declining external fundingA: Reliable supply chain managementsystemR: Non-acceptance by community ofIndoor Residual Spraying (IRS).R:A: Availability of fundsA: Adequate LLINS procured anddistributed to target population.R: Political will to implement theLibreville declaration.R: Uncertaininty of sectorialinvestments.R: Resource constraints.A: SRH/HIV integration strategydisseminated and implemented.A: Districts have capacity to implementnational malaria elimination plan.A: Development of joint plan of actionprioritized.A: Availability of funds and TAA: Availability of testing kits.R: District capacity to implement theIMCI training.R: Inappropriate deployment ofpersonnel release of health workers fortraining.A: Availability of funds.A: Capacity availabilityA: Availability of funds to completeconstruction and governmentcommitmentA: Availability of expert and equipmentin the marketBONEPWANACAMOHBONELABOFWACEYOHOBOMME ISAGO,MFDP-CSOUBWHO,<strong>UN</strong>AIDS,<strong>UN</strong>ICEF,<strong>UN</strong>DP,<strong>UN</strong>FPA0. 247 0. 107 0. 140MOH, PSISCMS<strong>UN</strong>FPA,WHO,<strong>UN</strong>AIDS0. 223 0. 024 0. 199MoH,NACA,BONELA,BOCAIP,BONEPWA,MoESD,MoLG & RD,MEWT,BRCS,Skills Share.WHO,<strong>UN</strong>DP,<strong>UN</strong>ESCO,<strong>UN</strong>AIDS,<strong>UN</strong>HCR,<strong>UN</strong>ICEF,<strong>UN</strong>FPA4765 0. 249 2275MoH,MoESD,MoLG&RD,MEWTWHO,<strong>UN</strong>ESCO,<strong>UN</strong>DP,<strong>UN</strong>HCR0. 070 0. 040 0. 030MoH,MoESD,BRCS & Skills share.WHO,<strong>UN</strong>FPA,<strong>UN</strong>ICEF,0. 4065 0. 209 0.1975MoH - Public Health IAEA 0.4690 0.4690 0<strong>GoB</strong> - <strong>UN</strong> <strong>POP</strong> <strong>2010</strong> - <strong>2014</strong> 47