Reichert Ocular Response Analyzer Measures Corneal ... - innova
Reichert Ocular Response Analyzer Measures Corneal ... - innova
Reichert Ocular Response Analyzer Measures Corneal ... - innova
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
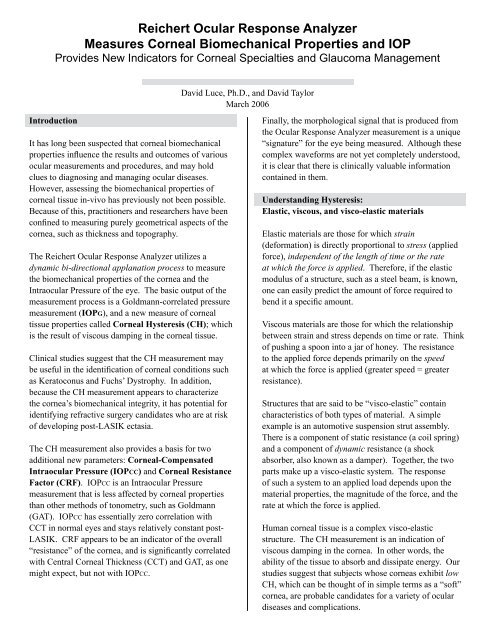
<strong>Reichert</strong> <strong>Ocular</strong> <strong>Response</strong> <strong>Analyzer</strong><strong>Measures</strong> <strong>Corneal</strong> Biomechanical Properties and IOPProvides New Indicators for <strong>Corneal</strong> Specialties and Glaucoma ManagementDavid Luce, Ph.D., and David TaylorMarch 2006IntroductionIt has long been suspected that corneal biomechanicalproperties influence the results and outcomes of variousocular measurements and procedures, and may holdclues to diagnosing and managing ocular diseases.However, assessing the biomechanical properties ofcorneal tissue in-vivo has previously not been possible.Because of this, practitioners and researchers have beenconfined to measuring purely geometrical aspects of thecornea, such as thickness and topography.The <strong>Reichert</strong> <strong>Ocular</strong> <strong>Response</strong> <strong>Analyzer</strong> utilizes adynamic bi-directional applanation process to measurethe biomechanical properties of the cornea and theIntraocular Pressure of the eye. The basic output of themeasurement process is a Goldmann-correlated pressuremeasurement (IOPG), and a new measure of cornealtissue properties called <strong>Corneal</strong> Hysteresis (CH); whichis the result of viscous damping in the corneal tissue.Clinical studies suggest that the CH measurement maybe useful in the identification of corneal conditions suchas Keratoconus and Fuchs’ Dystrophy. In addition,because the CH measurement appears to characterizethe cornea’s biomechanical integrity, it has potential foridentifying refractive surgery candidates who are at riskof developing post-LASIK ectasia.The CH measurement also provides a basis for twoadditional new parameters: <strong>Corneal</strong>-CompensatedIntraocular Pressure (IOPCC) and <strong>Corneal</strong> ResistanceFactor (CRF). IOPCC is an Intraocular Pressuremeasurement that is less affected by corneal propertiesthan other methods of tonometry, such as Goldmann(GAT). IOPCC has essentially zero correlation withCCT in normal eyes and stays relatively constant post-LASIK. CRF appears to be an indicator of the overall“resistance” of the cornea, and is significantly correlatedwith Central <strong>Corneal</strong> Thickness (CCT) and GAT, as onemight expect, but not with IOPCC.Finally, the morphological signal that is produced fromthe <strong>Ocular</strong> <strong>Response</strong> <strong>Analyzer</strong> measurement is a unique“signature” for the eye being measured. Although thesecomplex waveforms are not yet completely understood,it is clear that there is clinically valuable informationcontained in them.Understanding Hysteresis:Elastic, viscous, and visco-elastic materialsElastic materials are those for which strain(deformation) is directly proportional to stress (appliedforce), independent of the length of time or the rateat which the force is applied. Therefore, if the elasticmodulus of a structure, such as a steel beam, is known,one can easily predict the amount of force required tobend it a specific amount.Viscous materials are those for which the relationshipbetween strain and stress depends on time or rate. Thinkof pushing a spoon into a jar of honey. The resistanceto the applied force depends primarily on the speedat which the force is applied (greater speed = greaterresistance).Structures that are said to be “visco-elastic” containcharacteristics of both types of material. A simpleexample is an automotive suspension strut assembly.There is a component of static resistance (a coil spring)and a component of dynamic resistance (a shockabsorber, also known as a damper). Together, the twoparts make up a visco-elastic system. The responseof such a system to an applied load depends upon thematerial properties, the magnitude of the force, and therate at which the force is applied.Human corneal tissue is a complex visco-elasticstructure. The CH measurement is an indication ofviscous damping in the cornea. In other words, theability of the tissue to absorb and dissipate energy. Ourstudies suggest that subjects whose corneas exhibit lowCH, which can be thought of in simple terms as a “soft”cornea, are probable candidates for a variety of oculardiseases and complications.
How it works:Operation of the <strong>Ocular</strong> <strong>Response</strong> <strong>Analyzer</strong>The <strong>Ocular</strong> <strong>Response</strong> <strong>Analyzer</strong> utilizes a rapid airimpulse to apply force to the cornea, and an advancedelectro-optical system to monitor its deformation.Alignment to the patient’s eye is fully automated.A precisely-metered collimated-air-pulse causes thecornea to move inwards, past applanation, and into aslight concavity. Milliseconds after applanation, the airpump shuts off and the pressure declines in a smoothfashion. As the pressure decreases, the cornea begins toreturn to its normal configuration.Background on <strong>Corneal</strong> Hysteresis:What are we really measuring?It was observed that CH measurements were repeatableon individual eyes but differed significantly from personto person. The distribution of CH values for a normalpopulation (N=246 eyes) is shown below in Figure 2.It was also observed that these subject’s right and lefteye CH values are strongly correlated (R 2 0.60) furtherdemonstrating that corneal hysteresis is a biologicalmetric.In the process, it once again passes through anapplanated state. The applanation detection systemmonitors the cornea throughout the entire process, andtwo independent pressure values are derived from theINWARD and OUTWARD applanation events.One might expect these two pressure values to be thesame. However, due to the dynamic nature of the airpulse, the viscous damping in the cornea causes delaysin the inward and outward applanation events, resultingin two different pressure values.The average of these two pressure values provides arepeatable, Goldmann-correlated IOP value (IOPG).The difference between these two pressure values is<strong>Corneal</strong> Hysteresis (CH). (See Figure 1). The abilityto measure this effect is the key to the understandingthe biomechanical properties of the cornea and theirinfluence on the IOP measurement process.Figure 2 – Typical CH distribution of a normal populationIn order to explain CH, attempts were made to correlateit with corneal radius, astigmatism, visual acuity, andaxial length. No correlations of notable significancewere discovered, causing the investigators to believethat they were indeed measuring a new ocular parameter.Perhaps the most obvious relationship to examine is thatof the new CH measurement vs. traditional GoldmannIOP values.<strong>Corneal</strong> Hysteresis and Intraocular PressureTo investigate the relationship between CH and IOP,thirty-two normal eyes were measured at 3 differentpressure levels using both a Goldmann tonometerand the <strong>Ocular</strong> <strong>Response</strong> <strong>Analyzer</strong> (see Figure 3).Measurements were made within minutes of each otherto minimize diurnal effects.Figure 1 - The difference between the “inward” applanation and the“outward” applanation is called <strong>Corneal</strong> HysteresisInitial IOP measurements were made on the eyes in theirnormal state and then at two artificially elevated pressurelevels induced by a modified ophthalmodynamometer.The resulting inward and outward applanation datafor each set of measurements were plotted againstGoldmann IOP.
Figure 3 – Plotting the inward and outward applanation events vs.GAT on the same corneas at 3 pressure levelsThe data clearly show that the average <strong>Corneal</strong>Hysteresis remains relatively constant, for the sameset of corneas, over a wide range of pressuresdemonstratingthat <strong>Corneal</strong> Hysteresis is essentiallyindependent of pressure in normal eyes.Figure 4 below shows the <strong>Corneal</strong> Hysteresis parameterplotted against IOPG (traditional Goldmann-correlated)for a population of normal subjects (N=182 eyes),further demonstrating that CH is independent of pressurein normal eyes.Figure 4 – Typical relationship between Goldmann-correlatedIOPG and <strong>Corneal</strong> Hysteresis in normalsWhat About Central <strong>Corneal</strong> Thickness (CCT)?To determine if hysteresis is related to central cornealthickness (CCT), the CCT of 182 normal eyes wasmeasured with a 20 Mhz ultrasound pachymeter. TheCCT data were plotted against the <strong>Corneal</strong> Hysteresismeasurement for the same eyes. The correlation isstatistically significant, but weak, having an R 2 value of0.19 (Figure 5).Figure 5 – CH vs. CCT in a normal population N=182 eyesCH, CRF, and IOPCC: New <strong>Ocular</strong> ParametersClinical studies have shown that corneal biomechanicalproperties, as identified by the CH measurement,are not an artifact of any other variable and are ofconsiderable interest in the assessment of various ocularmeasurements and conditions.The CH measurement has been shown to be significantand useful in its own right, but in addition, the dynamicbi-directional applanation process can be used toderive other valuable information; namely <strong>Corneal</strong>-Compensated IOP (IOPCC) and <strong>Corneal</strong> ResistanceFactor (CRF). Both of these parameters are the resultof large-scale clinical data analysis and are derivedfrom specific combinations of the inward and outwardapplanation values using proprietary algorithms.<strong>Corneal</strong> Hysteresis is a phenomenon that results fromthe dynamic nature of the air pulse and the viscousdamping inherent in the cornea. CRF, is also derivedfrom this response. CRF is a measurement of thecumulative effects of both the viscous and elasticresistance encountered by the air jet while deforming thecorneal surface. CRF exhibits the expected property ofincreasing at significantly elevated pressures. ThoughCH and CRF are, on average, the same for a normalpopulation, they differ from person to person, providingus with distinct corneal information..<strong>Corneal</strong>-Compensated IOP (IOPCC) is a pressuremeasurement that utilizes the new information providedby the <strong>Corneal</strong> Hysteresis measurement to provide anIOP value that is less affected by corneal properties.While we cannot yet claim to be measuring “truepressure”, early investigations have demonstratedthat IOPCC is a better indicator of the real IntraocularPressure than GAT.
These new metrics have applications in a variety ofimportant areas including, but not limited to, refractivesurgery, corneal disease classification, accurateIOP measurement, and in glaucoma diagnosis andmanagement.We have now defined and briefly introduced the threenew parameters provided by the <strong>Ocular</strong> <strong>Response</strong><strong>Analyzer</strong>. Clinical evidence supporting the value of thesenew metrics is presented and discussed in the remainingportion of this paper.<strong>Corneal</strong> Pathologies and CH/CRFIdentifying and classifying corneal conditionsMeasuring biomechanical properties of the cornea withthe <strong>Ocular</strong> <strong>Response</strong> <strong>Analyzer</strong> gives us the potential, forthe first time, to identify various corneal conditions bymeans of a measurable and repeatable metric.A comparison of CH values obtained from eyeswith known corneal conditions with normal-subjectmeasurement values reveals significant differences. Acomparison of the CH and CRF values of three uniquepopulations is shown in Table 1. A CH histogram for thethree populations is shown in Figure 6.It is easy to see that the <strong>Corneal</strong> Hysteresis and CRFmeasurements in the eyes with corneal disorders are, onaverage, significantly lower than in normal eyes.NeyesAvemmHgRangemmHgSt DevmmHgCHNormals 246 11.19 7.24 - 15.80 1.63Keratoconics 62 8.74 4.80 - 12.39 1.17Fuchs’ 24 8.41 3.60 - 10.37 1.73Figure 6 – Comparison of <strong>Corneal</strong> Hysteresis distribution ofnormal, keratoconic, and Fuchs’ subjectsLow CH demonstrates that these corneas are less capableof absorbing (damping) the energy of the air pulse. LowCRF indicates that the overall rigidity (resistance) ofthese corneas is less than normals. The low CRF inthese eyes could explain why many Keratoconic andFuchs’ subjects measure unusually low IOP on GAT.Similar CH and CRF results have been observed invarious studies. Clearly these low values are typical ofa compromised cornea. With this in mind, some expertstheorize that normal eyes exhibiting significantly lowerthan average CH or CRF may be at risk of developingcorneal conditions in the future.In addition to simple differences in the CH values,significant differences are observable in the morphologyof the measurement-signal waveforms. Examples oftypical waveforms for each of the three populations areshown in Figures 7-9.CRFNormals 246 10.46 5.37 – 15.74 1.75Keratoconics 62 7.12 2.21 – 11.58 2.11Fuchs’ 24 7.83 4.76 – 10.59 1.23Table 1 – CH and CRF of normal, keratoconic, and Fuchs’ subjectsFigure 7 – Typical signal from a normal eye. <strong>Corneal</strong> Hysteresisvalue of 12.5 mmHg
The easily identifiable differences in CH and CRFbetween normal and compromised corneas suggest howthese metrics provide a more complete characterizationof the biomechanical state of the cornea than CCT. Thisobservation, coupled with the fact that CH and CRF areonly weakly correlated with CCT, leads us to believe thatthe corneal hysteresis measurement will be a useful toolfor eliminating potential LASIK patients who are at riskof developing post-LASIK ectasia. Studies investigatingthis issue are currently proceeding.Figure 8 – Typical signal from a keratoconic eye. <strong>Corneal</strong>Hysteresis value of 6.4 mmHgCH and CRF also have potential uses in post-LASIKfollow up. Clinical trials show significant post-LASIKchanges in CH (Figures 10 and 11).Figure 9 – Typical signal from a Fuchs’ Dystrophy eye. <strong>Corneal</strong>Hysteresis value of 7.3 mmHgFigure 10 – Typical signal from a normal subject’s eye pre-LASIK.<strong>Corneal</strong> Hysteresis value is 11.4 mmHgThough we are currently only utilizing the in and outapplanation pressure values to determine the CH andCRF measurements, in the future we may be able toextract additional information from the shape of thepressure/applanation signal waveform.<strong>Corneal</strong> Hysteresis and CRF in LASIKPotential clinical applications of the CH and CRFmeasurements in the area of refractive surgery areobvious. Currently, Central <strong>Corneal</strong> Thickness (CCT)is a primary factor used for screening candidates forrefractive surgery. Patients with thinner corneas areconsidered to be at higher risk of developing post-LASIK corneal ectasia. While rare, this complication isnot confined to patients with thin corneas and is a majorconcern for both doctors and patients. When it occurs itmay result in life-long complications for the patient andlitigation against the surgeon.Figure 11 – Signal from the same subject’s eye one weekpost-LASIK. <strong>Corneal</strong> Hysteresis value is 8.4 mmHgClinical data from several studies show a universalreduction in post-LASIK CH and CRF. Pre and postLASIK CH data are presented in Figure 12. Someexperts hypothesize that reduced post-LASIK CH/CRFis not primarily a function of corneal thinning, but rathera result of weakening of the structure related to thecreation of the flap.
Figure 12 – <strong>Corneal</strong> hysteresis of 15 eyes pre- and post-LASIKIn addition to the possible uses already discussed, someexperts believe that the CH measurement will be usefulin customizing ablation algorithms in order to betterpredict and control LASIK outcomes. While this ispurely hypothetical at the present time, studies are beingpursued to explore this possibility.NeyesAvemmHgRangemmHgSt DevmmHgIOPGNormals 246 15.10 7.03 – 24.92 3.22POAG 289 15.97 4.01 – 55.00 5.26NTG 24 16.07 12.05 – 21.32 2.30CHNormals 246 11.19 7.24 - 15.80 1.63POAG 289 10.08 2.07 - 19.96 2.32NTG 24 8.82 6.80 – 11.59 1.39CRFNormals 246 10.46 5.37 - 15.74 1.75POAG 289 9.30 1.70 – 24.18 2.26NTG 24 8.67 6.35 – 12.60 1.50Table 3 – CH and CRF of normal, keratoconic, and Fuchs’ subjects<strong>Corneal</strong> Hysteresis and CRF in GlaucomaRecently, the <strong>Ocular</strong> Hypertension Treatment Study(OHTS), and other studies on the subject, have broughtto light the importance of Central <strong>Corneal</strong> Thickness(CCT) in diagnosing and managing glaucoma. Thesestudies have suggested that low CCT (thin cornea)may be an independent risk factor for the developmentand progression of the disease. Many experts believethat corneal parameters other than CCT may provideclues that will aid in the diagnosis and management ofglaucoma. Recent studies suggest that pathology in thelamina cribrosa may be reflected in detectable changes ofcorneal properties. Clinical studies utilizing the <strong>Ocular</strong><strong>Response</strong> <strong>Analyzer</strong> support this hypothesis.Compared to normals, glaucomatous subjects have asignificantly lower than average <strong>Corneal</strong> Hysteresis anda much wider range. A comparison of IOP, CH, and CRFvalues for normal, Primary Open Angled Glaucoma(POAG), and “Normal Tension Glaucoma” (NTG)populations is shown in Table 3. A histogram of CH forthe three populations is shown in Figure 13.An interesting observation is that lower-than-average CHis also observed in patients who have been identified asNTG subjects. Currently individuals who have NTG areoften missed during routine IOP screening. Obviouslyit would be a tremendous breakthrough if <strong>Corneal</strong>Hysteresis is proven to be a reliable indicator of thisdisease condition.Figure 13 – Comparing the corneal hysteresis distributionof normal and glaucomatous subjectsAlso noteworthy is the fact that signals obtained fromeyes of NTG subjects looks similar to the signalsobtained from keratoconus, Fuchs’, and post-LASIKpatients, reinforcing the theory that glaucomatousdamage, in some manner, presents itself via the cornea.The signal from a NTG subject’s eye is shown inFigure 14.Figure 14 – Signal obtained from the eye of an NTG subject
As previously mentioned, in a normal population, thereis essentially no correlation between CH and IOPG(Page 3, Figure 5). However, in a typical glaucomatouspopulation there is a negative correlation between thetwo parameters (Figure 15). The eyes with severelyelevated pressures have much lower than averageCH. Conversely, these same eyes have higher CRFmeasurements. Investigators theorize that low CHis a result of “corneal remodeling” in response toglaucomatous damage and that high CRF is indicative ofstiffening of the cornea due to the elevated pressure.Figure 16 – Typical relationship between CCT and IOPGin a normal population N=182 eyes.The scatter present in this plot demonstrates that CCTcannot be used to adjust individual measured IOP values.Analysis of this and other IOP vs. CCT data has shownthat adjusting IOP based on CCT could lead not only toerrors in the magnitude of the adjustment, but also in thedirection of the adjustment.Figure 15 – IOPG vs. CH and CRF in a glaucomatous population of289 eyesIOPCC: Eliminating the <strong>Corneal</strong> EffectBy now nearly everyone recognizes that the currentgold standard for measuring pressure, the Goldmanntonometer, has considerable flaws. The GAT, andtonometers calibrated to “read like” a GAT, are affectedby corneal properties including rigidity, thickness,hydration, curvature, and perhaps other factors not yetidentified. Dr. Goldmann designed his tonometer toprovide accurate measurements in eyes with “average”corneas. But we now know that many corneas varymore significantly from average than previously thought.In theory, thicker corneas overstate IOP values andthinner corneas understate IOP values. Many attemptshave been made to establish a CCT-based correctionalgorithm to adjust Goldmann-obtained IOP values.However, the magnitude of the CCT/IOP relationshipidentified by the various studies is inconsistent. Thisvariation has resulted in numerous algorithms that differsignificantly from one another. A typical IOP vs. CCTplot for a population of 182 normal eyes is shown inFigure 16.Evidence in the literature continues to mount leadingexperts to question whether the Goldmann tonometeris sensitive and specific enough to be used for thecritical purpose of measuring IOP in the diagnosis andmanagement of Glaucoma. Refractive surgery, perhapsmore than anything else, has exposed how seriouslythe Goldmann Tonometer is compromised by cornealproperties.It is well-documented that there is an apparent, butartificial, reduction in post-LASIK GAT-measuredIOP. However, this anomaly cannot be explained by, orcorrected for, using CCT data or any currently knownparameter. This is because the LASIK procedure notonly thins the cornea, it induces complex biomechanicalchanges that are not measurable by any previouslyavailable device.Clearly, we need a new method of measuringIntraocular Pressure that takes corneal biomechanicsinto consideration. Only the <strong>Ocular</strong> <strong>Response</strong> <strong>Analyzer</strong>is capable of measuring these properties. IOPCCtakes corneal biomechanical properties into account,enabling the <strong>Ocular</strong> <strong>Response</strong> <strong>Analyzer</strong> to providepressure measurements that are less affected by cornealproperties. As evidence, a plot of IOPCC vs. CCT for a182-eye normal population is shown inFigure 17.
Figure 17 – IOPCC vs. CCT for a populationof normal eyes N = 182In addition to providing pressure measurements that areuninfluenced by CCT, the <strong>Ocular</strong> <strong>Response</strong> <strong>Analyzer</strong>facilitates post-LASIK IOP measurements that appearto remain consistent with pre-LASIK measurements.IOPCC values for 14 eyes pre and post LASIK are shownin Figure 18. Whereas Goldmann-measured IOP valuesare known to drop between 2-6 mmHg post LASIK, theaverage post-LASIK IOPCC reduction in this populationis less than 1 mmHg.SummaryFigure 19 – IOPCC and IOPG in 24 NTG eyesThe dynamic bi-directional applanation processemployed in the <strong>Reichert</strong> <strong>Ocular</strong> <strong>Response</strong> <strong>Analyzer</strong>facilitates the measurement of <strong>Corneal</strong> Hysteresis (CH).The CH phenomenon is observable due to viscousdamping in the cornea and permits the calculation of<strong>Corneal</strong> Resistance Factor (CRF) which appears toreflect the overall resistance of the cornea. Both metricsare new measurements of the biomechanical propertiesof the cornea.The ability of the device to characterize thebiomechanical properties of the cornea enables thecalculation of IOPCC, a measure of Intraocular Pressurethat is less influenced by corneal properties thanGoldmann or other currently available tonometers.IOPCC is unaffected by corneal properties such as CCTand remains essentially unchanged after LASIK.Observing the IOPCC of a population of Normal TensionGlaucoma (NTG) subjects, reveals that the pressure inthese eyes is significantly higher than indicated by thetraditional Goldmann-correlated IOP measurement. Inthis population, IOPCC is , on average, more than 2.25mmHg higher than IOPG (Figure 19).This chart also demonstrates the <strong>Ocular</strong> <strong>Response</strong><strong>Analyzer</strong>’s unique ability to simultaneously providea Goldmann-correlated IOP measurement (IOPG) aswell as the IOPCC value. With this feature clinicianscan observe the difference between the two values forreference purposes.Figure 18 –IOPCC pre and post LASIK in 14 eyesPublished and preliminary results from clinical studies inprocess worldwide suggest these new parameters may beclinically useful in a number of different areas including,but not limited to: Identification of corneal diseasessuch as keratoconus and Fuchs’ Dystrophy, Glaucomadiagnosis and management, screening potential LASIKcandidates, and accurate IOP measurement.<strong>Reichert</strong> would like to acknowledge the following individuals forproviding clinical data cited in this paper: Dr. Clifford Scott, OD;Mr. Sunil Shah, MD; Dr. James Brandt, MD, Dr. David Castellano,MD; Dr. Jay Pepose, MD; and Dr. Mitsugu Shimmyo, MD.<strong>Reichert</strong>, Inc.3374 Walden Avenue, Depew, NY 14043Toll Free: 888-849-8955 | Tel: (716) 686-4500Fax: (716) 686-4545 | www.reichert.com


![OCT Setting: CORNEA RADIAL 6( 6.0mm[1024] ) - innova](https://img.yumpu.com/48127738/1/190x146/oct-setting-cornea-radial-6-60mm1024-innova.jpg?quality=85)