Health response to the earthquake in Haiti, January 2010
Health response to the earthquake in Haiti, January 2010
Health response to the earthquake in Haiti, January 2010
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
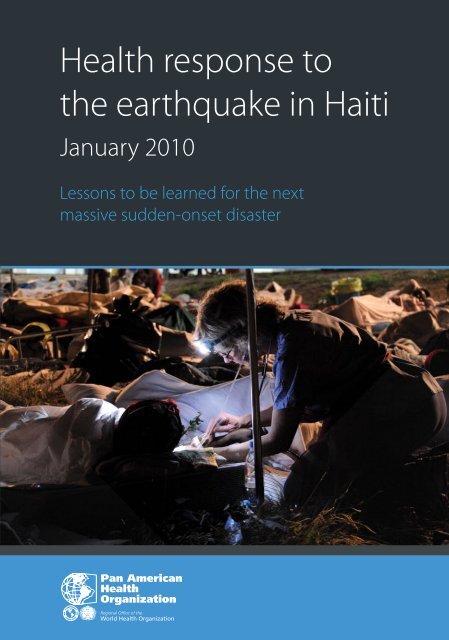
<strong>Health</strong> <strong>response</strong><strong>to</strong> <strong>the</strong> <strong>earthquake</strong><strong>in</strong> <strong>Haiti</strong><strong>January</strong> <strong>2010</strong>Lessons <strong>to</strong> be learnedfor <strong>the</strong> next massivesudden-onset disasterClaude de Ville de GoyetJuan Pablo Sarmien<strong>to</strong>François Grünewald2011
PAHO HQ Library Catalogu<strong>in</strong>g-<strong>in</strong>-Publication DataPan American <strong>Health</strong> Organization<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong>: <strong>January</strong> <strong>2010</strong>Wash<strong>in</strong>g<strong>to</strong>n, D.C.: PAHO, © 2011ISBN: 978-927513252-4I. Title1. EARTHQUAKE2. VULNERABILITY ANALYSIS3. DISASTERS4. PREVENTION AND MITIGATION - methods5. EDUCATION IN DISASTERS - policies6. RISK MANAGEMENT7. HUMAN RESOURCES IN DISASTERS8. HAITINLM WA 295.DH2The Pan American <strong>Health</strong> Organization welcomes requests for permission <strong>to</strong> reproduce or translateits publications, <strong>in</strong> part or <strong>in</strong> full. Applications and <strong>in</strong>quiries should be addressed <strong>to</strong> Edi<strong>to</strong>rialServices, Area of Knowledge Management and Communications (KMC), Pan American <strong>Health</strong>Organization, Wash<strong>in</strong>g<strong>to</strong>n, D.C., U.S.A. The Area on Emergency Preparedness and Disaster Relief;phone (202) 974-3399; email disaster-publications@paho.org will be glad <strong>to</strong> provide <strong>the</strong> latest<strong>in</strong>formation on any changes made <strong>to</strong> <strong>the</strong> text, plans for new editions, and repr<strong>in</strong>ts and translationsalready available.©Pan American <strong>Health</strong> Organization, 2011. All rights reserved.Publications of <strong>the</strong> Pan American <strong>Health</strong> Organization enjoy copyright protection <strong>in</strong> accordancewith <strong>the</strong> provisions of Pro<strong>to</strong>col 2 of <strong>the</strong> Universal Copyright Convention. All rights are reserved.The designations employed and <strong>the</strong> presentation of <strong>the</strong> material <strong>in</strong> this publication do not imply<strong>the</strong> expression of any op<strong>in</strong>ion whatsoever on <strong>the</strong> part of <strong>the</strong> Secretariat of <strong>the</strong> Pan American <strong>Health</strong>Organization concern<strong>in</strong>g <strong>the</strong> status of any country, terri<strong>to</strong>ry, city or area or of its authorities, or concern<strong>in</strong>g<strong>the</strong> delimitation of its frontiers or boundaries.The mention of specific companies or of certa<strong>in</strong> manufacturers’ products does not imply that <strong>the</strong>yare endorsed or recommended by <strong>the</strong> Pan American <strong>Health</strong> Organization <strong>in</strong> preference <strong>to</strong> o<strong>the</strong>rs ofa similar nature that are not mentioned. Errors and omissions excepted, <strong>the</strong> names of proprietaryproducts are dist<strong>in</strong>guished by <strong>in</strong>itial capital letters.All reasonable precautions have been taken by <strong>the</strong> Pan American <strong>Health</strong> Organization <strong>to</strong> verify <strong>the</strong><strong>in</strong>formation conta<strong>in</strong>ed <strong>in</strong> this publication. However, <strong>the</strong> published material is be<strong>in</strong>g distributedwithout warranty of any k<strong>in</strong>d, ei<strong>the</strong>r expressed or implied. The responsibility for <strong>the</strong> <strong>in</strong>terpretationand use of <strong>the</strong> material lies with <strong>the</strong> reader. In no event shall <strong>the</strong> Pan American <strong>Health</strong> Organizationbe liable for damages aris<strong>in</strong>g from its use.The pr<strong>in</strong>t<strong>in</strong>g of this publication was made possible with <strong>the</strong> f<strong>in</strong>ancial support of <strong>the</strong> Canadian InternationalDevelopment Agency (CIDA), <strong>the</strong> Office of U.S. Foreign Disaster Assistance of <strong>the</strong> U.S. Agencyfor International De velopment (OFDA/USAID), <strong>the</strong> Department for International Development of <strong>the</strong>United K<strong>in</strong>gdom (DFID), <strong>the</strong> Spanish Agency for International Development Cooperation (AECID),and <strong>the</strong> European Commission’s department of Humanitarian Aid and Civil Protection (ECHO).Graphic design and cover pho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>
Table ofcontentsForeword...............................................................................................................VAcknowledgments.............................................................................................VIIAbout <strong>the</strong> authors................................................................................................ IXPreface................................................................................................................ XIChapter 1<strong>Haiti</strong> prior <strong>to</strong> <strong>the</strong> <strong>earthquake</strong>.................................................................................. 1Chapter 2The <strong>earthquake</strong>: 12 <strong>January</strong> <strong>2010</strong>........................................................................11Chapter 3The health impact................................................................................................................ 19Chapter 4Who provided assistance?..................................................................................................... 37Chapter 5The life-sav<strong>in</strong>g <strong>response</strong>....................................................................................................... 53Chapter 6Beyond trauma care............................................................................................81
Table ofcontentsChapter 7Information management ..............................................................................111Chapter 8Coord<strong>in</strong>ation ..................................................................................................125Chapter 9Key strategic lessons for <strong>the</strong> next sudden-onset disaster....................................................137Bibliography...................................................................................................144List of acronyms..............................................................................................156Annex 1. Conditions <strong>in</strong> <strong>Haiti</strong> prior <strong>to</strong> <strong>the</strong> <strong>earthquake</strong>........................................159Annex 2. Chronology of events follow<strong>in</strong>g <strong>the</strong> <strong>Haiti</strong> <strong>earthquake</strong>.........................169
ForewordEvery disaster br<strong>in</strong>gs new lessons of general application that we must learn before<strong>the</strong> next sudden-onset disaster strikes. The <strong>Haiti</strong> <strong>earthquake</strong> is no exception.This publication, for practical reasons, focuses on <strong>the</strong> first three months of <strong>the</strong><strong>response</strong>. A similar study might be needed for <strong>the</strong> mid- and long-term recoveryand reconstruction process that occurs after <strong>the</strong> first three months.The key lessons outl<strong>in</strong>ed <strong>in</strong> this publication are not merely <strong>the</strong> views of <strong>the</strong> author,Claude de Ville de Goyet, and co-authors, Juan Pablo Sarmien<strong>to</strong> and FrançoisGrünewald. They reflect <strong>the</strong> collective vision of a large number of partners andexperts. International experts of <strong>the</strong> review group made significant contributions<strong>to</strong> <strong>the</strong> f<strong>in</strong>d<strong>in</strong>gs and conclusions of this important publication.The 12 <strong>January</strong> <strong>2010</strong> <strong>earthquake</strong> could not have occurred <strong>in</strong> a more vulnerableenvironment than <strong>the</strong> capital of <strong>Haiti</strong>. The immediate health impact of <strong>the</strong> <strong>earthquake</strong><strong>in</strong> absolute terms— number of dead and <strong>in</strong>jured—was among <strong>the</strong> highest<strong>in</strong> recent times. When <strong>the</strong> needs are compared <strong>to</strong> <strong>the</strong> national <strong>response</strong> capacity,this disaster was truly unprecedented.The <strong>in</strong>ternational community responded rapidly with an outpour<strong>in</strong>g of generosity.Beyond traditional global donors, relief came from <strong>Haiti</strong>’s immediate neighbors,as well as from every country <strong>in</strong> Lat<strong>in</strong> America and <strong>the</strong> Caribbean. Suchsupport offered an encourag<strong>in</strong>g example of solidarity <strong>in</strong> <strong>the</strong> true spirit of Pan-Americanism.If <strong>the</strong> impact was unprecedented, <strong>the</strong> organization of <strong>the</strong> <strong>response</strong> was not. It followed<strong>the</strong> same chaotic pattern as <strong>in</strong> past disasters. Information was scarce, decisionswere often not evidence-based, and overall sec<strong>to</strong>ral coord<strong>in</strong>ation presentedserious shortcom<strong>in</strong>gs. Management gaps noted <strong>in</strong> past crises were repeated andamplified <strong>in</strong> <strong>Haiti</strong>. The humanitarian community failed <strong>to</strong> put <strong>in</strong> practice <strong>the</strong>lessons learned.The “proliferation of ac<strong>to</strong>rs”, <strong>to</strong> borrow an expression used <strong>in</strong> <strong>the</strong> evaluation of<strong>the</strong> tsunami, ensured a massive offer of services from competent partners. Theoverwhelm<strong>in</strong>g number of people <strong>in</strong> need of immediate assistance ensured thateach m<strong>in</strong>imally prepared and equipped health responder provided valuable healthassistance. However, this proliferation also <strong>in</strong>cluded a number of wholly unpreparedor even <strong>in</strong>competent health ac<strong>to</strong>rs who bypassed <strong>the</strong> overburdened coord<strong>in</strong>ationmechanisms. The WHO <strong>in</strong>itiative <strong>to</strong> launch a global registration processof foreign medical teams and field hospitals is most timely. It should be a first step<strong>to</strong>ward national accreditation of those ac<strong>to</strong>rs.V
Information and coord<strong>in</strong>ation management was a challenge that was not metadequately. One of <strong>the</strong> key lessons <strong>to</strong> be re-learned from <strong>the</strong> <strong>Haiti</strong> <strong>earthquake</strong> isthat coord<strong>in</strong>ation can only be effective if <strong>the</strong> national authorities (civil protection,health, and o<strong>the</strong>r l<strong>in</strong>e m<strong>in</strong>istries) are equipped and truly assume <strong>the</strong> ultimateleadership and authority for coord<strong>in</strong>ation. External coord<strong>in</strong>ation mechanismsare most valuable when <strong>the</strong>y can offer a modicum of order <strong>in</strong> <strong>the</strong> first daysor weeks until <strong>the</strong> authorities recover from <strong>the</strong> impact. But only <strong>the</strong> governmen<strong>to</strong>f an affected country has <strong>the</strong> legitimacy <strong>to</strong> establish and implement relief andrecovery priorities.Disasters are tragedies, but also provide w<strong>in</strong>dows of opportunities. The pr<strong>in</strong>cipleof free access <strong>to</strong> basic health care is now more widely accepted. The <strong>in</strong>ternationalfocus on mental health and psychosocial support shed light on <strong>the</strong> <strong>in</strong>adequacy of<strong>in</strong>stitutionalization as <strong>the</strong> basis for treatment of mental health patients. The highnumber of amputations and o<strong>the</strong>r severe <strong>in</strong>juries result<strong>in</strong>g from <strong>the</strong> <strong>earthquake</strong>prompted a dramatic and positive shift <strong>in</strong> public attitudes <strong>to</strong>ward those with disabilitiesand a strong commitment <strong>to</strong> rehabilitation programs.This publication aims <strong>to</strong> <strong>in</strong>crease <strong>the</strong> technical body of evidence. Many reports, aswell as peer-reviewed articles, have been published on this disaster. This PAHO/WHO publication offers a synopsis from a public health po<strong>in</strong>t of view.In conclusion, we know that o<strong>the</strong>r disasters will affect metropolitan areas <strong>in</strong> develop<strong>in</strong>gcountries. It is not a matter of if, but of when. Only by <strong>in</strong>corporat<strong>in</strong>g thoselessons <strong>in</strong><strong>to</strong> improved risk mitigation and <strong>in</strong> particular health preparedness, willwe avoid repeat<strong>in</strong>g <strong>the</strong> same errors <strong>in</strong> <strong>the</strong> next affected country.The maximum possible reduction of avoidable deaths, disabilities, and suffer<strong>in</strong>grema<strong>in</strong>s our ultimate goal.Mirta Roses PeriagoDirec<strong>to</strong>rPan American <strong>Health</strong> OrganizationVI
AcknowledgmentsThe author and co-authors of this publication express <strong>the</strong>ir gratitude for all thosewho have shared <strong>the</strong>ir experience, <strong>the</strong>ir views, and observations dur<strong>in</strong>g numerousmeet<strong>in</strong>gs and field visits. They helped us <strong>to</strong> appreciate <strong>the</strong> dedication of so manyfac<strong>in</strong>g an <strong>in</strong>surmountable challenge.Our appreciation goes first <strong>to</strong> <strong>the</strong> <strong>Haiti</strong>an health professionals who candidlydescribed <strong>the</strong>ir odyssey <strong>in</strong> <strong>the</strong> first weeks follow<strong>in</strong>g <strong>the</strong> <strong>earthquake</strong>, and <strong>the</strong>irgratitude but also frustration with well-<strong>in</strong>tentioned but sometimes counterproductiveassistance. Among those who have <strong>in</strong>fluenced our th<strong>in</strong>k<strong>in</strong>g are: ArielHenri, Cab<strong>in</strong>et Chief of <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong>; Daniel Henrys, senior consultant;Jean Hughes Henrys, Dean of <strong>the</strong> Medical School, University of NotreDame; Alix Lassegue, Direc<strong>to</strong>r, University Hospital of <strong>Haiti</strong>; Claude Surena,<strong>Haiti</strong>an Medical Association; and Yolene Surena, Direc<strong>to</strong>rate for Civil Protection/WorldBank Project.In <strong>the</strong> <strong>in</strong>ternational community, among <strong>the</strong> many who helped us <strong>to</strong> reconstruct<strong>the</strong> complex patterns of <strong>the</strong> <strong>response</strong>, special recognition is due <strong>to</strong> Edmond Mulet,Special Representative of <strong>the</strong> UN Secretary-General. A remarkable diplomatwith sound judgment on our collective lackluster coord<strong>in</strong>ation, Mr. Mulet reassuredus <strong>in</strong> our quest for additional critical <strong>in</strong>sights. The support and contributionsof UNICEF staff <strong>in</strong> <strong>the</strong> <strong>in</strong>itial <strong>in</strong>terviews but also <strong>in</strong> <strong>the</strong> review process werealso outstand<strong>in</strong>g.There were many colleagues <strong>in</strong> PAHO/WHO who guided us, correct<strong>in</strong>g our <strong>in</strong>terpretationof <strong>the</strong> implications and mid-term consequences of <strong>the</strong> <strong>response</strong>, andstreng<strong>the</strong>n<strong>in</strong>g our grasp of all <strong>the</strong> relevant facts. Among <strong>the</strong>m are <strong>the</strong> two PAHO/WHO representatives who conducted PAHO/WHO <strong>response</strong>, Henriette Chamouilletand Lea Guido; Dana Van Alphen, <strong>the</strong> <strong>Health</strong> Cluster coord<strong>in</strong>a<strong>to</strong>r; andCristian Morales, <strong>Health</strong> Services Advisor. They helped us <strong>to</strong> navigate between<strong>the</strong> two occasionally clash<strong>in</strong>g worlds of <strong>the</strong> life-sav<strong>in</strong>g humanitarian <strong>response</strong> andof <strong>the</strong> long-term, capacity build<strong>in</strong>g of <strong>the</strong> national counterparts.This document would never have come <strong>to</strong> fruition without <strong>the</strong> visionary supportfrom <strong>the</strong> Emergency Preparedness Area at PAHO/WHO Headquarters. Jean-LucPoncelet’s encouragement and ability <strong>to</strong> mobilize resources for <strong>the</strong> preparationand publication of this document, Sam Vigersky and Crist<strong>in</strong>a Estrada’s managementsupport, and Liz S<strong>to</strong>naker’s edi<strong>to</strong>rial contributions were most valuable.VII
In addition we would like <strong>to</strong> acknowledge <strong>the</strong> contributions made by <strong>the</strong> follow<strong>in</strong>gpeople who served on <strong>the</strong> review committee: Ellen Wasserman (Johns Hopk<strong>in</strong>sSchool of Public <strong>Health</strong>); Shannon Stro<strong>the</strong>r (Disaster Resilience Leadership Academy,Tulane University); Alana Officer (WHO); Andre Griekspoor (WHO); JonAndrus (PAHO); Jean Luc Poncelet (PAHO); Sylva<strong>in</strong> Aldighieri (PAHO); CeciliaAcuña (PAHO); Peter Graaff (PAHO); and Nicolas Lagomars<strong>in</strong>o (PAHO).Nam<strong>in</strong>g a few can be an <strong>in</strong>justice for <strong>the</strong> many o<strong>the</strong>rs who helped us. Few of <strong>the</strong>ideas and key f<strong>in</strong>d<strong>in</strong>gs are ours. They all have been revealed <strong>to</strong> us by one colleagueor ano<strong>the</strong>r. Our appreciation and our gratitude go <strong>to</strong> those anonymous th<strong>in</strong>kersfrom NGOs, UN or o<strong>the</strong>r agencies. We hope that <strong>the</strong>se lessons, <strong>the</strong>ir lessons, willbe learned and put <strong>in</strong> practice <strong>in</strong> future disasters.VIII
About <strong>the</strong> authorsClaude de Ville de Goyet, MD MPHClaude de Ville de Goyet graduated from <strong>the</strong> University of Louva<strong>in</strong> (Belgium) <strong>in</strong>1965 and completed a BSc <strong>in</strong> Operational Research at <strong>the</strong> University of SouthAfrica. Follow<strong>in</strong>g six years of public health work <strong>in</strong> Africa, Dr. de Ville de Goyetbecame <strong>the</strong> first Direc<strong>to</strong>r of <strong>the</strong> Disaster Epidemiology Research Center (CRED) at<strong>the</strong> University of Louva<strong>in</strong> <strong>in</strong> Belgium.From 1977 <strong>to</strong> 2002, he was Direc<strong>to</strong>r of <strong>the</strong> Emergency Preparedness and DisasterRelief Coord<strong>in</strong>ation Program of <strong>the</strong> Pan American <strong>Health</strong> Organization, RegionalOffice for <strong>the</strong> Americas of <strong>the</strong> World <strong>Health</strong> Organization (PAHO/WHO). Beg<strong>in</strong>n<strong>in</strong>g<strong>in</strong> 1976, he has travelled frequently <strong>to</strong> <strong>Haiti</strong>.S<strong>in</strong>ce his retirement from PAHO/WHO <strong>in</strong> 2002, Dr. de Ville de Goyet has conducted<strong>in</strong>dependent evaluations after most major disasters, <strong>in</strong>clud<strong>in</strong>g <strong>the</strong> IndianOcean tsunami and <strong>the</strong> Bam and Kashmir <strong>earthquake</strong>s. Dr. de Ville is very familiarwith <strong>the</strong> situation <strong>in</strong> <strong>Haiti</strong>, where he was relief coord<strong>in</strong>a<strong>to</strong>r after <strong>the</strong> 2004Hurricane <strong>in</strong> Gonaives and WHO Representative and Special Advisor <strong>in</strong> early2011 dur<strong>in</strong>g <strong>the</strong> cholera outbreak.Juan Pablo Sarmien<strong>to</strong>, MD MPHJuan Pablo Sarmien<strong>to</strong> graduated from <strong>the</strong> University of Rosario (Colombia) <strong>in</strong>1980, and completed post-graduate studies <strong>in</strong> Disaster Management (UnitedK<strong>in</strong>gdom), Public Adm<strong>in</strong>istration (Colombia), Medical Education (Colombia),Nutrition (United States), and Project Adm<strong>in</strong>istration (Costa Rica).From 1981 <strong>to</strong> 1994, Dr. Sarmien<strong>to</strong> worked for Colombian <strong>in</strong>stitutions <strong>in</strong> a varietyof capacities, <strong>in</strong>clud<strong>in</strong>g: Head of <strong>the</strong> <strong>Health</strong> Unit, Colombian Civil Defense;Chief of Emergency Services, Central Military Hospital; National Disaster Coord<strong>in</strong>a<strong>to</strong>r,M<strong>in</strong>istry of <strong>Health</strong>; Professor, Javeriana University; and National ReliefDirec<strong>to</strong>r, Colombian Red Cross.Between 1994 and 2008, Dr. Sarmien<strong>to</strong> worked for <strong>the</strong> U.S. Agency for InternationalDevelopment, Office for U.S. Foreign Disaster Assistance (USAID/OFDA) as Technical Manager for <strong>the</strong> Lat<strong>in</strong> American and Caribbean RegionalDisaster Program, based <strong>in</strong> Costa Rica.Dr. Sarmien<strong>to</strong> currently works as Research Professor at <strong>the</strong> Lat<strong>in</strong> American andCaribbean Center and at <strong>the</strong> Stempel School of Public <strong>Health</strong>, Florida InternationalUniversity (U.S.A.).IX
François GrünewaldFrançois Grünewald is an agricultural eng<strong>in</strong>eer, specializ<strong>in</strong>g <strong>in</strong> rural economies,and serves as Associate Professor at Paris XII University. He has worked for 30years <strong>in</strong> development, emergency, and post-disaster rehabilitation projects <strong>in</strong> Africa,Asia, Central Europe, and Central and Lat<strong>in</strong> America, serv<strong>in</strong>g with NGOs,UN agencies, and <strong>the</strong> International Committee of <strong>the</strong> Red Cross (ICRC).In 1997, he became chairman of Groupe URD (Urgence-Rehabilitation-Developpement),a French research, evaluation and tra<strong>in</strong><strong>in</strong>g <strong>in</strong>stitute. In that capacityGrünewald has conducted research and evaluation projects for <strong>the</strong> EuropeanUnion, ICRC, <strong>the</strong> UN, and NGOs. He is <strong>the</strong> author of several books and articleson complex emergencies and <strong>the</strong> management of socio-natural disasters.Mr. Grünewald has served as team leader for <strong>the</strong> evaluation of <strong>the</strong> <strong>response</strong> <strong>to</strong><strong>the</strong> Bahr el Ghazal fam<strong>in</strong>e; <strong>the</strong> NGO evaluation of Hurricane Mitch; <strong>the</strong> UnitedK<strong>in</strong>gdom and UNICEF evaluation of <strong>the</strong> Darfur Crisis; evaluation of <strong>the</strong> French<strong>response</strong> <strong>to</strong> <strong>the</strong> Indian Ocean tsunami; IASC evaluation of <strong>in</strong>ternational <strong>response</strong><strong>to</strong> <strong>the</strong> crisis <strong>in</strong> <strong>the</strong> Horn of Africa; and a variety of evaluations follow<strong>in</strong>g <strong>the</strong><strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong>.X
PrefaceThe 12 <strong>January</strong> <strong>2010</strong> <strong>earthquake</strong> was <strong>the</strong> latest and most devastat<strong>in</strong>g of manymajor sudden-impact natural disasters affect<strong>in</strong>g <strong>Haiti</strong> <strong>in</strong> <strong>the</strong> last 10 years. It wasalso one of a series of sudden emergencies that mobilized <strong>the</strong> <strong>in</strong>ternational communityon a global scale.The <strong>response</strong> <strong>to</strong> <strong>Haiti</strong>, especially <strong>in</strong> <strong>the</strong> health sec<strong>to</strong>r, has been generous, evenoverwhelm<strong>in</strong>g. This <strong>in</strong>ternal and external <strong>response</strong> met considerable challengesand problems, some of its own mak<strong>in</strong>g. As was <strong>the</strong> case <strong>in</strong> <strong>the</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong>Indian Ocean tsunami and <strong>the</strong> Pakistan <strong>earthquake</strong>, not all those challenges weremet effectively.The objective of this publication is <strong>to</strong> draw <strong>the</strong> lessons <strong>to</strong> be learned for improv<strong>in</strong>g<strong>the</strong> health <strong>response</strong> <strong>in</strong> future sudden-onset disasters. We know that massive<strong>earthquake</strong>s will occur aga<strong>in</strong> and some will devastate metropolitan areas or even<strong>the</strong> capital city, as was <strong>the</strong> case <strong>in</strong> <strong>Haiti</strong>. <strong>Haiti</strong> is <strong>the</strong> subject of this study, hopefullynot <strong>the</strong> object, as <strong>Haiti</strong> has had her share of catastrophes.The scope of <strong>the</strong> book is limited <strong>to</strong> <strong>the</strong> health <strong>response</strong>, health be<strong>in</strong>g def<strong>in</strong>ed <strong>in</strong> itsbroad sense, not merely medical care or disease control. The review is conf<strong>in</strong>ed <strong>to</strong><strong>the</strong> immediate and early <strong>response</strong> <strong>in</strong> <strong>the</strong> first three months, <strong>the</strong> period dur<strong>in</strong>g whichmost of <strong>the</strong> <strong>in</strong>ternational assistance was mobilized and <strong>in</strong>fluences, for better or worse,rehabilitation and reconstruction.The publication focuses specially but not exclusively on those lessons that are ofgeneral <strong>in</strong>terest, i.e., not specific <strong>to</strong> <strong>the</strong> special case of <strong>Haiti</strong>. The <strong>in</strong>ternationalcommunity has much <strong>to</strong> learn from <strong>the</strong> <strong>response</strong> <strong>in</strong> <strong>Haiti</strong> where it has shown anability <strong>to</strong> repeat its errors and shortcom<strong>in</strong>gs from past disasters.The methodology used for this study is common <strong>to</strong> most evaluations: <strong>in</strong>-depthreview of reports, evaluations, studies, and peer-reviewed scientific publications;over 150 <strong>in</strong>terviews, half of <strong>the</strong>m carried out exclusively for this study and o<strong>the</strong>rsfor similar evaluations carried out by one of <strong>the</strong> three authors; circulation of <strong>the</strong>draft <strong>to</strong> all <strong>in</strong>terviewees for factual validation and comments on <strong>the</strong> authors’ <strong>in</strong>terpretationof <strong>the</strong> f<strong>in</strong>d<strong>in</strong>gs; and, f<strong>in</strong>ally, discussion with a review board convenedby PAHO/WHO.XI
The poorest country <strong>in</strong> <strong>the</strong> WesternHemisphere, <strong>Haiti</strong> has been affected bypolitical violence for most of its recenthis<strong>to</strong>ry. Poverty, corruption, lack ofexport <strong>in</strong>dustries, a large deficit andsevere environmental deterioration anddeforestation, are among <strong>Haiti</strong>’s mostserious disadvantages.Pho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>
Chapter1<strong>Haiti</strong> prior <strong>to</strong><strong>the</strong> <strong>earthquake</strong>This chapter summarizes <strong>the</strong> situation <strong>in</strong> <strong>Haiti</strong> prior <strong>to</strong> <strong>the</strong> <strong>earthquake</strong>. 1 The detailedbackground description can be found <strong>in</strong> Annex 1.Whenever possible, it offers a comparison with <strong>Haiti</strong>’s neighbor, <strong>the</strong> Dom<strong>in</strong>ican Republic(<strong>to</strong> place <strong>the</strong> country <strong>in</strong> a regional context), and with three countries affected<strong>in</strong> <strong>the</strong> last decade by large, sudden-onset natural disasters and recipients of massive<strong>in</strong>ternational assistance: Indonesia and Sri Lanka (Indian Ocean tsunami <strong>in</strong> 2004)and Pakistan (<strong>earthquake</strong> <strong>in</strong> Kashmir <strong>in</strong> 2005).<strong>Haiti</strong>, a French- and Creole-speak<strong>in</strong>g country located <strong>in</strong> <strong>the</strong> middle of <strong>the</strong> Caribbeanbas<strong>in</strong>, has a population estimated at 10 million <strong>in</strong>habitants. 2 It takes up one-third of<strong>the</strong> island of Hispaniola, <strong>the</strong> rest be<strong>in</strong>g occupied by <strong>the</strong> Dom<strong>in</strong>ican Republic, whichhas a comparable population.Half of <strong>the</strong> population lives <strong>in</strong> urban areas, <strong>the</strong> largest be<strong>in</strong>g <strong>the</strong> capital metropolitanarea (Port-au-Pr<strong>in</strong>ce “agglomeration”), with a population estimated at 2.3 million.1 Sources for this chapter <strong>in</strong>clude: Institut <strong>Haiti</strong>en de Statistique et Informatique (IHSI <strong>2010</strong>); World Bank, <strong>Haiti</strong> at aglance (2006); PAHO/WHO, <strong>Health</strong> <strong>in</strong> <strong>the</strong> Americas (2007); WHO, <strong>Haiti</strong> health profile (<strong>2010</strong>); United Nations, Worldpopulation prospects: <strong>the</strong> 2008 revision (2009).2 Estimates <strong>in</strong> official and scientific documents vary from 8 <strong>to</strong> 10 million. The absence of such basic <strong>in</strong>formation as agreedupon census data <strong>in</strong> <strong>Haiti</strong> illustrates <strong>the</strong> lack of reliable or accurate data on many aspects of <strong>the</strong> country’s public life. Forthis reason, figures are rounded <strong>in</strong> this publication.1
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Social, political, and economic determ<strong>in</strong>antsCharacteristics of <strong>Haiti</strong> affect<strong>in</strong>g disaster <strong>response</strong>Disadvantages for <strong>response</strong>:• A small country, among <strong>the</strong> poorest of <strong>the</strong> world, and <strong>the</strong>refore with limited <strong>response</strong>capacity;• Weak <strong>in</strong>stitutions with little control over thousands of donor-supported NGOs;• Lack of governance and a high level of corruption;• The absence of armed forces.Advantages for <strong>response</strong>:• Easy access by land and water;• Presence of peacekeep<strong>in</strong>g forces, UN agencies, and a large number of humanitarian NGOs.In 1991, a military coup paralyzed <strong>the</strong> development of <strong>the</strong> country, lead<strong>in</strong>g <strong>in</strong> 1993<strong>to</strong> an OAS/UN embargo. One of <strong>the</strong> first decisions of <strong>the</strong> newly elected, democraticGovernment <strong>in</strong> 1994, was <strong>to</strong> dismantle <strong>the</strong> army—<strong>the</strong> cause of so many military coups<strong>in</strong> <strong>Haiti</strong>—leav<strong>in</strong>g <strong>the</strong> police force as <strong>the</strong> only national <strong>in</strong>stitution <strong>in</strong> charge of security.Follow<strong>in</strong>g a long series of political upheavals, <strong>the</strong> United Nations Stabilization Mission <strong>in</strong><strong>Haiti</strong> (MINUSTAH) was set up <strong>in</strong> 2004. 3 While <strong>the</strong> <strong>Haiti</strong>an National Police was progressivelyemerg<strong>in</strong>g as a law enforcement body, foreign military forces under MINUSTAH ensuredbasic security both for <strong>the</strong> population, which was <strong>in</strong>creas<strong>in</strong>gly ambivalent <strong>to</strong> this presence, andfor an <strong>in</strong>creas<strong>in</strong>gly large UN humanitarian and development community. MINUSTAH was<strong>the</strong> only entity with significant assets and discipl<strong>in</strong>e for logistic support <strong>to</strong> <strong>the</strong> humanitariancommunity <strong>in</strong> case of sudden-onset disasters. However, this function was not <strong>in</strong>cluded <strong>in</strong> itsmandate. It should be noted that <strong>the</strong> presence of a peacekeep<strong>in</strong>g force <strong>in</strong> absence of civilwar or conflict subjected <strong>the</strong> UN ac<strong>to</strong>rs <strong>to</strong> particularly constra<strong>in</strong><strong>in</strong>g security rules.<strong>Haiti</strong>’s socio-economic situation at <strong>the</strong> time of <strong>the</strong> <strong>earthquake</strong> can be described<strong>in</strong> a nutshell:• One of poorest and smallest countries <strong>in</strong> <strong>the</strong> world and <strong>the</strong> least developed<strong>in</strong> <strong>the</strong> American region;• A high level of corruption, <strong>in</strong>equity, and <strong>in</strong>equality;32FILM• Severe environmental deterioration and deforestation;• Lack of export <strong>in</strong>dustries and a large deficit;• An ongo<strong>in</strong>g bra<strong>in</strong> dra<strong>in</strong>, primarily <strong>to</strong> <strong>the</strong> United States, Canada, and France;32 32APho<strong>to</strong>: UN, Logan Abassi23 MINUSTAH was orig<strong>in</strong>ally established through <strong>the</strong> UN Security Council Resolution 1542 of 30 April 2004, <strong>to</strong> “support<strong>the</strong> Transitional Government <strong>in</strong> ensur<strong>in</strong>g a secure and stable environment; <strong>to</strong> assist <strong>in</strong> moni<strong>to</strong>r<strong>in</strong>g, restructur<strong>in</strong>g andreform<strong>in</strong>g <strong>the</strong> <strong>Haiti</strong>an National Police; <strong>to</strong> help with comprehensive and susta<strong>in</strong>able Disarmament, Demobilization andRe<strong>in</strong>tegration (DDR) programmes; <strong>to</strong> assist with <strong>the</strong> res<strong>to</strong>ration and ma<strong>in</strong>tenance of <strong>the</strong> rule of law, public safety andpublic order <strong>in</strong> <strong>Haiti</strong>; <strong>to</strong> protect United Nations personnel, facilities, <strong>in</strong>stallations and equipment and <strong>to</strong> protect civiliansunder imm<strong>in</strong>ent threat of physical violence; <strong>to</strong> support <strong>the</strong> constitutional and political processes; <strong>to</strong> assist <strong>in</strong> organiz<strong>in</strong>g,moni<strong>to</strong>r<strong>in</strong>g, and carry<strong>in</strong>g out free and fair municipal, parliamentary and presidential elections; <strong>to</strong> support <strong>the</strong> TransitionalGovernment as well as <strong>Haiti</strong>an human rights <strong>in</strong>stitutions and groups <strong>in</strong> <strong>the</strong>ir efforts <strong>to</strong> promote and protect human rights;and <strong>to</strong> moni<strong>to</strong>r and report on <strong>the</strong> human rights situation <strong>in</strong> <strong>the</strong> country. … In extend<strong>in</strong>g <strong>the</strong> mission’s mandate for ano<strong>the</strong>ryear on 13 Oc<strong>to</strong>ber 2009, <strong>the</strong> Security Council, by its resolution 1892, fur<strong>the</strong>r tasked MINUSTAH with provid<strong>in</strong>g logisticaland security assistance for elections anticipated for <strong>2010</strong>” (UN 2011).
HAITI PRIOR TO THE EARTHQUAKE - Chapter 1• Most services delivered by NGOs with <strong>to</strong>ken supervision and consultation from<strong>the</strong> Government. <strong>Haiti</strong> has been called a “Republic of NGOs”.<strong>Haiti</strong> stands <strong>in</strong> stark contrast <strong>to</strong> its neighbor, <strong>the</strong> Dom<strong>in</strong>ican Republic, and <strong>to</strong> o<strong>the</strong>r develop<strong>in</strong>gcountries recently affected by sudden-onset disasters that triggered massive foreign assistance.Comparative data are shown <strong>in</strong> Table 1.1. While <strong>Haiti</strong> can be compared <strong>to</strong> Sri Lanka <strong>in</strong>terms of size, its level of development is far lower. <strong>Haiti</strong>’s development level is comparable <strong>to</strong>that of Pakistan but <strong>the</strong> size of <strong>the</strong> latter country and extent of its resources are very dissimilar.Figure 1.1 shows <strong>the</strong> rank<strong>in</strong>g of <strong>Haiti</strong> <strong>in</strong> <strong>the</strong> Rule of Law Index, compared <strong>to</strong> <strong>the</strong> foursame countries.Table 1.1 Population, <strong>in</strong>come, governance, and security <strong>in</strong>dica<strong>to</strong>rs<strong>in</strong> <strong>Haiti</strong>, Dom<strong>in</strong>ican Republic, Sri Lanka, Pakistan, and IndonesiaIndica<strong>to</strong>r <strong>Haiti</strong> Dom<strong>in</strong>ican Sri Lanka Pakistan IndonesiaRepublicPopulation10 10 20 161 228(millions)GNI per650 4,860 2,290 1,050 2,580(US$; <strong>2010</strong>) acapitaMulti-dimensional0.31 0.05 0.02 0.28 0.1<strong>the</strong> better) bPov-erty Index(<strong>the</strong> lower,CorruptionIndex (rank<strong>in</strong>g<strong>2010</strong>) c 2.2 (146) 3.0 (101) 3.2 (91) 2.3 ( 143) 2.8 (110)Security for<strong>in</strong>ternationalstaffPresence ofmilitaryNGOsNo ongo<strong>in</strong>gcivil conflictbut strictrestriction ofmovementNo nationalmilitary;strong UNpeacekeep<strong>in</strong>gpresenceOne of <strong>the</strong>highestdensitiesof NGOs <strong>in</strong>world; <strong>to</strong>kengovernmen<strong>to</strong>versightGoodsecurityNational militaryactive <strong>in</strong>civil defenseSignificantnumber ofNGOs withmoderategovernmen<strong>to</strong>versightOngo<strong>in</strong>g civilwar; restrictedaccess <strong>to</strong> someareasStrong presenceof nationalmilitary; someareas underrebel controlMany localNGOs, but few<strong>in</strong>ternationalNGOs activebefore tsunami;strong governmen<strong>to</strong>versightGood security;no conflict.Earthquake-affectedprov<strong>in</strong>ceunder militaryauthorityStrong presenceof nationalmilitaryFew <strong>in</strong>ternationalNGOsauthorized <strong>in</strong>Kashmir, butlarge number <strong>in</strong>Pakistan; stronggovernmen<strong>to</strong>versightLow security;civil war ongo<strong>in</strong>g<strong>in</strong> AcehStrong presenceof nationalmilitaryNo <strong>in</strong>ternationalNGOs allowed<strong>in</strong> Aceh prior <strong>to</strong><strong>the</strong> tsunami (UNand ICRC only);strong governmen<strong>to</strong>versightabcGross national <strong>in</strong>come (GNI) per capita (formerly GNP per capita) is <strong>the</strong> gross national <strong>in</strong>come, converted <strong>to</strong> U.S. dollars,divided by <strong>the</strong> midyear population. It comprises <strong>the</strong> value of all products and services generated with<strong>in</strong> a country <strong>in</strong>one year (i.e., its gross domestic product), <strong>to</strong>ge<strong>the</strong>r with its net <strong>in</strong>come received from o<strong>the</strong>r countries (notably <strong>in</strong>terestand dividends). Figures are from World Bank Databank (<strong>2010</strong>).The Multidimensional Poverty Index (Alkire and San<strong>to</strong>s <strong>2010</strong>) uses 10 <strong>in</strong>dica<strong>to</strong>rs <strong>to</strong> measure critical dimensions of povertyat <strong>the</strong> household level. The MPI value summarizes <strong>in</strong>formation on multiple deprivations <strong>in</strong><strong>to</strong> a s<strong>in</strong>gle number.The Corruption Index ranks countries on a scale from 10 (highly clean) <strong>to</strong> 0 (highly corrupt); rank<strong>in</strong>g <strong>in</strong> world is <strong>in</strong>paren<strong>the</strong>ses (Transparency International 2011).3
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Figure 1.1 Rule of law rank<strong>in</strong>gs for <strong>Haiti</strong>, Dom<strong>in</strong>ican Republic,Sri Lanka, Pakistan, and Indonesia (2009)Sri LankaIndonesiaDom<strong>in</strong>ican RepublicPakistan<strong>Haiti</strong>0 255075 100Country’s percentile rank (0-100)Note: The Rule of Law Index is one of six <strong>in</strong>dica<strong>to</strong>rs used <strong>to</strong> assess <strong>the</strong> quality of governance <strong>in</strong> countries. These <strong>in</strong>dica<strong>to</strong>rsaggregate <strong>the</strong> views on <strong>the</strong> quality of governance provided by a large number of enterprise, citizen and expertsurvey respondents <strong>in</strong> <strong>in</strong>dustrialized and develop<strong>in</strong>g countries. Figure compiled from <strong>the</strong> World Bank WorldwideGovernance Indica<strong>to</strong>rs website: http://<strong>in</strong>fo.worldbank.org/governance/wgi/mc_countries.asp.<strong>Health</strong> status 4<strong>Health</strong> characteristics of <strong>Haiti</strong>Negative aspects:• Lack of reliable basel<strong>in</strong>e health statistics;• High level of most communicable diseases;• Only half of <strong>the</strong> population has access <strong>to</strong> poor quality health services, water, orsanitation;• 75% of health services are delivered by NGOs and faith groups, most of which areunwill<strong>in</strong>g <strong>to</strong> follow M<strong>in</strong>istry of <strong>Health</strong> norms and guidel<strong>in</strong>es.Positive aspects:• A strong pharmaceutical and supply system which is <strong>in</strong>ternationally adm<strong>in</strong>istered;• On-site presence of external medical organizations (NGOs or bilateral).A governance review of <strong>the</strong> health sec<strong>to</strong>r carried out by <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong> <strong>in</strong>2007 shows that leadership and regula<strong>to</strong>ry functions <strong>in</strong> <strong>Haiti</strong> were “weak or veryweak” at <strong>the</strong> central, departmental, and periphery levels (MSPP 2007). At <strong>the</strong> crosssec<strong>to</strong>rallevel, donors must share <strong>in</strong> responsibility for a situation that enables NGOs<strong>to</strong> decl<strong>in</strong>e <strong>to</strong> comply with norms and standards or tentative attempts of coord<strong>in</strong>ationfrom <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong>.44 Sources for this section <strong>in</strong>clude: PAHO/WHO, <strong>Health</strong> <strong>in</strong> <strong>the</strong> Americas (2007), PAHO/WHO, <strong>Health</strong> situation <strong>in</strong> <strong>the</strong>Americas, basic <strong>in</strong>dica<strong>to</strong>rs 2009; <strong>Haiti</strong>, PDNA (analytical matrix) (<strong>2010</strong>).
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>NutritionThe levels of global acute malnutrition as well as those of stunt<strong>in</strong>g (chronic malnutrition)are high but markedly under those considered a humanitarian emergency. Thefocus of ongo<strong>in</strong>g projects has not been sufficiently aligned with <strong>Haiti</strong>’s priority nutritionsecurity problems or with <strong>in</strong>ternational best practices. Above all, malnutrition<strong>in</strong> <strong>Haiti</strong> is <strong>the</strong> end result of extreme poverty associated with low education level. Itis primarily an economic and equity issue ra<strong>the</strong>r than a health one.Violence and crim<strong>in</strong>alityThe rate of violence is very high <strong>in</strong> <strong>Haiti</strong>. Reliable figures are unavailable or atbest spotty. Gender-based violence is endemic and underreported. There is littlefollow-up, be it from law enforcement or <strong>the</strong> health services, on reported casesof gender-based violence.32FILMTable 1.2 <strong>Health</strong> statistics for selected countriesIndica<strong>to</strong>r <strong>Haiti</strong> Dom<strong>in</strong>ican Sri Lanka Pakistan IndonesiaRepublicLife expectancy 62 73 69 63 67(years)Under-5 mortality76 24 17 97 34(deaths per1,000 live births)Measles58% 95% 98% 85% 83%immunizationPhysicians per3 19 6 8 110,000Hospital bedsper 10,00013 10 29 10 6Sources: WHO, World <strong>Health</strong> Statistics, 2009 www.who.<strong>in</strong>t/whosis/whostat/EN_WHS09_Table6.pdf; World Bank,<strong>Haiti</strong> at a glance; Dom<strong>in</strong>ican Republic at a glance.32 32APho<strong>to</strong>: PAHO/WHOThe health status of <strong>Haiti</strong> prior <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> is particularly bleak when compared<strong>to</strong> its neighbor or o<strong>the</strong>r countries affected by sudden-onset catastrophes (see Table1.2). The services rema<strong>in</strong> very poor despite considerable <strong>in</strong>vestment by NGOs and<strong>the</strong> higher density of medical doc<strong>to</strong>rs and hospitals beds <strong>in</strong> <strong>the</strong> country compared, for<strong>in</strong>stance, <strong>to</strong> Indonesia.F<strong>in</strong>ally, <strong>the</strong> “s<strong>in</strong>gularity or exceptionality” of <strong>Haiti</strong> <strong>in</strong> <strong>the</strong> Region of <strong>the</strong> Americasshould be noted. It is <strong>the</strong> only <strong>in</strong>dependent, French/Creole-speak<strong>in</strong>g country <strong>in</strong> <strong>the</strong>Caribbean or Lat<strong>in</strong> America. <strong>Haiti</strong> has a social, economic, and political culture comparable<strong>to</strong> no o<strong>the</strong>r. Although it is mak<strong>in</strong>g a consistent effort <strong>to</strong> jo<strong>in</strong> regional <strong>in</strong>stitutions,few if any o<strong>the</strong>r members share <strong>the</strong> same challenges or background, or evenunderstand its culture. <strong>Haiti</strong> is not fully <strong>in</strong>tegrated as an equal member <strong>in</strong> <strong>the</strong> Caribbeanor Lat<strong>in</strong> America. It is an orphan without sibl<strong>in</strong>gs, but with many foster parents.6
HAITI PRIOR TO THE EARTHQUAKE - Chapter 1Disaster vulnerability, risk reduction <strong>in</strong>clud<strong>in</strong>g preparednessVulnerability• <strong>Haiti</strong> is particularly vulnerable <strong>to</strong> disasters. The ma<strong>in</strong> fac<strong>to</strong>rs caus<strong>in</strong>g this vulnerability aresocial and economic.• The focus of preparedness <strong>in</strong> <strong>Haiti</strong> was overwhelm<strong>in</strong>gly on seasonal climaticevents. Rare, but catastrophic events were not contemplated.• The poorest countries are <strong>the</strong> least able and will<strong>in</strong>g <strong>to</strong> <strong>in</strong>vest <strong>in</strong> risk reduction, <strong>in</strong>clud<strong>in</strong>g<strong>in</strong> preparedness. Consider<strong>in</strong>g <strong>the</strong> urgency of every day needs faced by<strong>the</strong>se countries, <strong>the</strong> onus for risk reduction and disaster preparedness should bemore on <strong>the</strong> <strong>in</strong>ternational community.• International agencies and donors should <strong>in</strong>crease <strong>the</strong>ir efforts <strong>to</strong> focus <strong>the</strong> attentionof health authorities on credible scenarios of major sudden-onset disasters.32FILMAmong <strong>the</strong> many fac<strong>to</strong>rs affect<strong>in</strong>g <strong>Haiti</strong>’s vulnerability <strong>to</strong> disasters are <strong>the</strong> concentrationof population (39%) and resources (66% of GDP) <strong>in</strong> and around <strong>the</strong> capital(West Department), deforestation, <strong>the</strong> presence of communities liv<strong>in</strong>g on pla<strong>in</strong>swhich are prone <strong>to</strong> flood<strong>in</strong>g, high urban population density, and a proliferation ofseismically unsafe build<strong>in</strong>gs and <strong>in</strong>frastructure constructed on unstable soils.Environmental vulnerability and social fac<strong>to</strong>rs like poverty, political <strong>in</strong>stability,rapid urbanization, and <strong>the</strong> fragile nature of <strong>the</strong> <strong>Haiti</strong>an State exacerbate <strong>the</strong>damag<strong>in</strong>g effects of natural events.32 32AThese observations have been confirmed by <strong>the</strong> alarm<strong>in</strong>g trend <strong>in</strong> successivedisasters: 56 <strong>in</strong>ternationally recognized disasters, <strong>in</strong>clud<strong>in</strong>g 20 major disasters<strong>in</strong> <strong>the</strong> 20th century and 3 catastrophic hurricane seasons <strong>in</strong> just <strong>the</strong> last decade(see Table 1.3).Pho<strong>to</strong>: UN, Logan AbassiTable 1.3 Summary of recent major disasters <strong>in</strong> <strong>Haiti</strong>EventEffect on Affected DeathsGDP2004: Hurricane Jeanne 7% 300,000 5,0002007: Hurricanes Dean and Noel 2% 194,000 3302008: Tropical s<strong>to</strong>rms Fay and Gustav andHurricane Ike15% 1,000,000 800Compiled from relevant post-disaster needs assessments.7
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Risk reductionAlthough risk reduction <strong>in</strong>cludes preparedness, this aspect will be treated separately.The risk of <strong>earthquake</strong> was not unknown by <strong>the</strong> health sec<strong>to</strong>r and was stressed <strong>in</strong> <strong>the</strong>country health profile developed by PAHO/WHO <strong>in</strong> 2007 (pg 414):“<strong>Haiti</strong> is . . . extremely vulnerable <strong>to</strong> <strong>earthquake</strong>s. The country has eightfault l<strong>in</strong>es; two of <strong>the</strong> most important are located as follows: one <strong>in</strong> <strong>the</strong>far north and <strong>the</strong> o<strong>the</strong>r cross<strong>in</strong>g east <strong>to</strong> west. Seismic activity <strong>in</strong> <strong>Haiti</strong><strong>in</strong> 2003–2005 has revived <strong>the</strong> specter of a possible major <strong>earthquake</strong>(7–8 on <strong>the</strong> Richter scale), which experts have been forecast<strong>in</strong>g for severalyears. The extremely high rate of urbanization that has left <strong>the</strong> metropolitanregion of Port-au-Pr<strong>in</strong>ce with slightly more than two million <strong>in</strong>habitants(10,000–18,000 persons per km2) will worsen <strong>the</strong> damage.”As noted by François Grünewald, <strong>the</strong> <strong>earthquake</strong> “has taken place <strong>in</strong> a context where<strong>the</strong> most frequent problems obscure <strong>the</strong> most serious problems. Though <strong>Haiti</strong> experienced<strong>earthquake</strong>s which destroyed Cap Haïtien <strong>in</strong> 1840 and Port-au-Pr<strong>in</strong>ce <strong>in</strong> 1700,<strong>the</strong>se tragedies of <strong>the</strong> past only had a marg<strong>in</strong>al <strong>in</strong>fluence on <strong>the</strong> national strategy formanag<strong>in</strong>g risks” (<strong>2010</strong>, 2).As often is <strong>the</strong> case, important issues (prepar<strong>in</strong>g for major but rare events 7 ) were overshadowedby more press<strong>in</strong>g immediate priorities (attend<strong>in</strong>g <strong>to</strong> daily and seasonalemergencies). <strong>Haiti</strong>’s Direc<strong>to</strong>rate for Civil Protection (DPC) started <strong>to</strong> work onbuild<strong>in</strong>g standards for critical facilities before <strong>the</strong> <strong>earthquake</strong> and on a disaster riskreduction strategy. They were plann<strong>in</strong>g <strong>to</strong> <strong>in</strong>itiate a build<strong>in</strong>g code project <strong>in</strong> <strong>January</strong><strong>2010</strong>. 8 Reduction of seismic risk through adoption and enforcement of constructionnorms and standards had never been enacted before.32FILMThe easiest and least expensive way <strong>to</strong> protect health (and o<strong>the</strong>r) facilities fromseismic risk is by <strong>in</strong>clud<strong>in</strong>g strict norms <strong>in</strong> new construction. However, few ifany new health facilities had been built <strong>in</strong> <strong>Haiti</strong> <strong>in</strong> recent years. The retrofitt<strong>in</strong>gof exist<strong>in</strong>g facilities is a technically more complicated and more expensiveapproach and was never seriously considered as a feasible and cost-effectivemeasure by <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong> or donor community.No serious attention was given by <strong>the</strong> health sec<strong>to</strong>r <strong>to</strong> <strong>the</strong> possible scenario of a severe<strong>earthquake</strong>. The modest efforts focused on seasonal hurricanes. 9 Admittedly, <strong>Haiti</strong> has<strong>the</strong> highest <strong>in</strong>dex of vulnerability <strong>to</strong> cyclones of all <strong>the</strong> develop<strong>in</strong>g small island states. 10An estimated 96% of <strong>the</strong> population of <strong>Haiti</strong> lives <strong>in</strong> constant danger of two or morerisks. Fur<strong>the</strong>rmore, be<strong>in</strong>g part of an island <strong>in</strong> <strong>the</strong> middle of <strong>the</strong> Caribbean <strong>in</strong>deed<strong>in</strong>creases <strong>the</strong> risks l<strong>in</strong>ked <strong>to</strong> ris<strong>in</strong>g sea level and those related <strong>to</strong> <strong>the</strong> possible impacts ofchang<strong>in</strong>g patterns <strong>in</strong> <strong>the</strong> El Niño/La Niña phenomena (DARA <strong>2010</strong>).32 32APho<strong>to</strong>: PAHO/WHO, Sam Vigersky7 The seismic recurrence <strong>in</strong>terval was estimated at about 150 years.8 At <strong>the</strong> multisec<strong>to</strong>ral level, major donors (World Bank and European donors) provided significant support at <strong>the</strong> end of<strong>the</strong> last decade <strong>to</strong> streng<strong>the</strong>n <strong>the</strong> national Direc<strong>to</strong>rate for Civil Protection. The focus was <strong>in</strong>itially at <strong>the</strong> national level andshifted later <strong>to</strong>ward decentralization and streng<strong>the</strong>n<strong>in</strong>g of <strong>the</strong> department level.9 Cyclones are known as hurricanes <strong>in</strong> <strong>the</strong> Caribbean or typhoons <strong>in</strong> <strong>the</strong> Pacific Ocean.10 Based on <strong>the</strong> estimated number of people killed per year (per million exposed) (World Bank 2005).8
Chapter2The <strong>earthquake</strong>:12 <strong>January</strong> <strong>2010</strong>The impact of <strong>the</strong> <strong>Haiti</strong> <strong>earthquake</strong> was truly unprecedented among recentnatural disasters:• The magnitude of damage and losses <strong>in</strong> absolute terms, but above all compared <strong>to</strong><strong>the</strong> size and poverty of <strong>the</strong> country preclud<strong>in</strong>g any backup capacity;• The destruction of <strong>the</strong> capital and its effect on <strong>the</strong> government apparatus;• The leadership losses <strong>in</strong>curred by <strong>the</strong> UN peacekeep<strong>in</strong>g forces, UN agencies, ando<strong>the</strong>r potential ac<strong>to</strong>rs;• The impact on logistics of severe damage <strong>to</strong> both <strong>the</strong> major airport and seaport.On 12 <strong>January</strong> <strong>2010</strong>, shortly before 5 PM, an <strong>earthquake</strong> with a magnitude of 7.0on <strong>the</strong> MMS scale shook <strong>Haiti</strong> for 35 seconds. 11 It was <strong>the</strong> most powerful <strong>earthquake</strong><strong>to</strong> hit <strong>the</strong> country <strong>in</strong> 200 years. The <strong>earthquake</strong>’s hypocenter was close <strong>to</strong> <strong>the</strong> Earth’ssurface (13 km below) and its epicenter was approximately 25 km southwest of Portau-Pr<strong>in</strong>ce,<strong>the</strong> capital, <strong>in</strong> <strong>the</strong> West Department. Although <strong>the</strong> South-East and NippesDepartments were also affected, only a limited, albeit densely populated, area (45 kmradius) was hit by <strong>the</strong> <strong>earthquake</strong>.11 Initial estimates <strong>in</strong>dicated a magnitude of 7.3 on <strong>the</strong> Richter scale. U.S. Geological Survey and o<strong>the</strong>r sources suggest amagnitude of 7.0. Part of <strong>the</strong> reason for <strong>the</strong> discrepancy is <strong>the</strong> <strong>in</strong>creas<strong>in</strong>g use of <strong>the</strong> Moment Magnitude Scale (MMS)which differs slightly from <strong>the</strong> Richter scale. As with <strong>the</strong> Richter scale, an <strong>in</strong>crease of one step on this logarithmic scalecorresponds <strong>to</strong> a 10 1.5 ≈ 32 times <strong>in</strong>crease <strong>in</strong> <strong>the</strong> amount of energy released, and an <strong>in</strong>crease of two steps corresponds <strong>to</strong> a10 3 (i.e., 1,000 times) <strong>in</strong>crease <strong>in</strong> energy. It should be noted that <strong>the</strong> Richter scale is no<strong>to</strong>riously less accurate <strong>in</strong> measur<strong>in</strong>gsevere <strong>earthquake</strong>s.11
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Accord<strong>in</strong>g <strong>to</strong> a study by <strong>the</strong> U.S. Geological Survey, <strong>the</strong> fault <strong>in</strong>itially thought <strong>to</strong> havetriggered this devastat<strong>in</strong>g <strong>earthquake</strong> is likely still under considerable stra<strong>in</strong> and cont<strong>in</strong>ues<strong>to</strong> pose a significant seismic hazard. 12 This puts <strong>to</strong> rest <strong>the</strong> common misconceptionthat an area affected by a major seismic event is vulnerable <strong>to</strong> milder aftershocksbut protected from more severe <strong>earthquake</strong>s.The Port-au-Pr<strong>in</strong>ce metropolitan area suffered enormous damage. 13 Eighty percent of <strong>the</strong><strong>to</strong>wn of Léogâne (17 km southwest of Port-au-Pr<strong>in</strong>ce) was destroyed.The <strong>earthquake</strong> created an unprecedented situation, amplified by <strong>the</strong> fact that it affected<strong>the</strong> most densely populated area of <strong>the</strong> country and also its economic andadm<strong>in</strong>istrative center. It also severely affected <strong>the</strong> <strong>in</strong>ternational organizations <strong>in</strong> <strong>Haiti</strong>(<strong>in</strong>clud<strong>in</strong>g MINUSTAH, UN agencies, and NGOs).Rural areas <strong>in</strong> <strong>the</strong> West and South-East Departments, <strong>in</strong>clud<strong>in</strong>g <strong>the</strong> mounta<strong>in</strong>ous areaswere also badly affected. Thousands of rural houses <strong>in</strong> remote, hard-<strong>to</strong>-reach areas weredestroyed and <strong>earthquake</strong>-triggered landslides were frequent.The extent of damage and losses reflect <strong>the</strong> particularly high vulnerability of <strong>Haiti</strong>. While<strong>the</strong> U.S. Geological Survey recorded 22 magnitude-7.0 or larger <strong>earthquake</strong>s <strong>in</strong> <strong>2010</strong>, almostall <strong>the</strong> fatalities were produced by <strong>the</strong> 12 <strong>January</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong>. In <strong>2010</strong>, about227,000 people were killed due <strong>to</strong> <strong>earthquake</strong>s, with over 98% from <strong>the</strong> <strong>Haiti</strong> event. 14This large, shallow <strong>earthquake</strong> produced violent shak<strong>in</strong>g that can cause damage even<strong>to</strong> well-built build<strong>in</strong>gs anywhere <strong>in</strong> <strong>the</strong> world. In <strong>Haiti</strong>, this high-<strong>in</strong>tensity shak<strong>in</strong>g<strong>to</strong>ge<strong>the</strong>r with build<strong>in</strong>gs vulnerable <strong>to</strong> <strong>earthquake</strong>s and high population exposure resulted<strong>in</strong> catastrophe.The Post-Disaster Needs Assessment (PDNA)As is systematically done after such an event, <strong>the</strong> <strong>Haiti</strong>an Government and <strong>the</strong> <strong>in</strong>ternationalcommunity launched a Post-Disaster Needs Assessment (PDNA) <strong>in</strong>volv<strong>in</strong>g UNDP, <strong>the</strong> WorldBank, <strong>the</strong> European Commission, and o<strong>the</strong>r donors.“The objectives for <strong>the</strong> PDNA, a cross-sec<strong>to</strong>ral exercise <strong>to</strong> provide a f<strong>in</strong>ancial estimate of <strong>the</strong>damage and needs, were multifold, each ac<strong>to</strong>r stress<strong>in</strong>g a particular one:• “A <strong>to</strong>ol for decision mak<strong>in</strong>g and priority sett<strong>in</strong>g by donors and agencies due <strong>to</strong> meet at <strong>the</strong>Donor Conference <strong>in</strong> New York (31 March <strong>2010</strong>);• “A new vision for <strong>in</strong>-depth reform, mak<strong>in</strong>g use of <strong>the</strong> w<strong>in</strong>dow for opportunities openedbriefly follow<strong>in</strong>g major disasters; however, some questioned whe<strong>the</strong>r an <strong>in</strong>cremental approach<strong>to</strong> ‘build back better’ was not more realistic than a costly new vision;• “A step <strong>to</strong>ward develop<strong>in</strong>g an action plan and strategy for <strong>the</strong> sec<strong>to</strong>rs; this is a result thatwas achieved <strong>in</strong> <strong>the</strong> health sec<strong>to</strong>r, although not fully implemented;• “A necessary statistical record for global comparison and documentation for <strong>the</strong> significant<strong>in</strong>vestment <strong>in</strong> <strong>the</strong> reconstruction process” (Griekspoor <strong>2010</strong>).1212 U.S. Geological Survey geologist Carol Prentice led a team of scientists <strong>to</strong> <strong>Haiti</strong> immediately after <strong>the</strong> <strong>earthquake</strong> <strong>to</strong> searchfor traces of ground rupture. The researchers sought evidence of deformation from <strong>the</strong> <strong>2010</strong> quake and determ<strong>in</strong>ed that <strong>the</strong>ma<strong>in</strong> strand of <strong>the</strong> Enriquillo-Planta<strong>in</strong> Garden (EPG) Fault did not rupture <strong>in</strong> <strong>the</strong> <strong>January</strong> quake, as was <strong>in</strong>itially thought.They also documented evidence of geologically young ground ruptures on <strong>the</strong> EPG Fault, which <strong>the</strong>y believe may haveformed dur<strong>in</strong>g <strong>earthquake</strong>s that struck <strong>Haiti</strong> <strong>in</strong> 1751 and 1770. Because <strong>the</strong> EPG Fault did not rupture <strong>the</strong> surface, little,if any, accumulated stra<strong>in</strong> on that fault was released dur<strong>in</strong>g <strong>the</strong> quake and <strong>the</strong> hazard rema<strong>in</strong>s high ((Koontz <strong>2010</strong>).13 Includ<strong>in</strong>g <strong>the</strong> communes of Port-au-Pr<strong>in</strong>ce, Carrefour, Pétionville, Delmas, Tabarre, Cité Soleil, and Kenscoff.14 A magnitude-8.8 offshore <strong>earthquake</strong> that hit Chile on 27 February was <strong>the</strong> largest recorded <strong>in</strong> <strong>the</strong> world <strong>in</strong> <strong>2010</strong>. Anestimated 577 died; about half of those deaths resulted from an <strong>earthquake</strong>-generated tsunami. The energy released by <strong>the</strong>Chilean <strong>earthquake</strong> was more than 500 times greater than <strong>the</strong> one that hit <strong>Haiti</strong>. However, fatalities were far lower <strong>in</strong> Chiledue <strong>to</strong> that country’s strict build<strong>in</strong>g codes and lower maximum shak<strong>in</strong>g <strong>in</strong>tensities (USGS 2011).
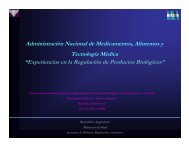
THE EARTHQUAKE: 12 JANUARY <strong>2010</strong> - Chapter 2Overall impact on <strong>in</strong>frastructureThe <strong>earthquake</strong> caused massive <strong>in</strong>frastructure destruction. Accord<strong>in</strong>g <strong>to</strong> <strong>the</strong> surveycarried out by <strong>the</strong> Post-Disaster Needs Assessment (PDNA), 15 (see Box) some 105,000homes were completely destroyed and more than 208,000 damaged. Over 1,300 educationalestablishments and over 50 hospitals and health centers collapsed or were leftunusable. Part of <strong>the</strong> country’s ma<strong>in</strong> port was not operational. Damage <strong>to</strong> <strong>the</strong> airportguidance system limited <strong>the</strong> early arrival of essential <strong>response</strong>, lead<strong>in</strong>g <strong>the</strong> Governmen<strong>to</strong>f <strong>Haiti</strong> <strong>to</strong> delegate authority over its airspace and airport <strong>to</strong> <strong>the</strong> U.S. military.The President’s Palace, Parliament, <strong>the</strong> Law Courts, many o<strong>the</strong>r landmarks of <strong>the</strong> <strong>Haiti</strong>annation, and most of <strong>the</strong> m<strong>in</strong>istry and public adm<strong>in</strong>istration build<strong>in</strong>gs, <strong>in</strong>clud<strong>in</strong>g <strong>the</strong>M<strong>in</strong>istry of <strong>Health</strong>, were destroyed. This damage fur<strong>the</strong>r crippled <strong>the</strong> limited capacity of<strong>the</strong> government <strong>to</strong> lead a forceful <strong>response</strong>.The only natural disaster that came close <strong>to</strong> this level of devastat<strong>in</strong>g governance capacityand adm<strong>in</strong>istrative structures was <strong>the</strong> Managua <strong>earthquake</strong> (Nicaragua, 23 December15 The primary source for this section is: <strong>Haiti</strong> <strong>earthquake</strong> PDNA: assessment of damages, losses, sec<strong>to</strong>ral and general needs, publishedby <strong>the</strong> <strong>Haiti</strong>an Government, March <strong>2010</strong>.M<strong>in</strong>istry of <strong>Health</strong>Presidential PalacePho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>13Pho<strong>to</strong>: UN, Logan Abassi
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>1972). Two-thirds of <strong>the</strong> capital’s population was displaced. However, <strong>the</strong>re were significantdifferences from <strong>the</strong> <strong>Haiti</strong> <strong>earthquake</strong>:• Managua had a population of 325,000 compared <strong>to</strong> <strong>the</strong> 2.5 million <strong>in</strong> Port-au-Pr<strong>in</strong>ce;• Fatalities were relatively few (3,000 <strong>to</strong> 7,000) compared <strong>to</strong> over 200,000 deaths <strong>in</strong><strong>Haiti</strong>;• There was a strong dicta<strong>to</strong>rial government <strong>in</strong> Nicaragua compared <strong>to</strong> a fragile butdemocratic government <strong>in</strong> <strong>Haiti</strong>.Economic impact• The <strong>earthquake</strong> set back <strong>the</strong> economic development of <strong>Haiti</strong> by 10 years;• The economic valuation process of damage and losses does not reflect <strong>the</strong> magnitudeof human losses and suffer<strong>in</strong>g;• When translated <strong>in</strong><strong>to</strong> monetary value, <strong>the</strong> social losses represent only a relatively modesteconomic cost.The health sec<strong>to</strong>r does not operate <strong>in</strong> a vacuum. It is entirely dependent on <strong>the</strong> economichealth of <strong>the</strong> country and its population. An impact of <strong>the</strong> <strong>earthquake</strong> oneconomic well-be<strong>in</strong>g is an impact on public health.The disaster impact on economic performance, employment, and poverty can be assessedfrom two measures:1. The damage: that is, <strong>the</strong> replacement value of physical assets wholly or partiallydestroyed;2. The losses: <strong>the</strong> economic flows result<strong>in</strong>g from <strong>the</strong> temporary absence of damagedassets.Accord<strong>in</strong>g <strong>to</strong> <strong>the</strong> PDNA, <strong>the</strong> <strong>to</strong>tal value of damage and losses caused by <strong>the</strong> <strong>earthquake</strong>on 12 <strong>January</strong> <strong>2010</strong> is estimated at US$ 7.804 billion, surpass<strong>in</strong>g <strong>the</strong> country’sGDP <strong>in</strong> 2009. This is <strong>the</strong> first time <strong>in</strong> 35 years of apply<strong>in</strong>g <strong>the</strong> assessment methodologydeveloped by <strong>the</strong> UN Economic Commission for Lat<strong>in</strong> America and <strong>the</strong>Caribbean 16 for estimat<strong>in</strong>g damage and losses that <strong>the</strong> cost of a disaster is so high <strong>in</strong>economic terms <strong>in</strong> relation <strong>to</strong> a country’s GDP.The private sec<strong>to</strong>r (<strong>in</strong>clud<strong>in</strong>g not-for-profit) susta<strong>in</strong>ed most of <strong>the</strong> damage and losses(US$ 5.722 billion, 73% of <strong>the</strong> <strong>to</strong>tal), whereas <strong>the</strong> public sec<strong>to</strong>r’s share <strong>to</strong>taled US$2.081 billion, or 27%. There are two exceptions: <strong>the</strong> health sec<strong>to</strong>r, where only 40% of<strong>the</strong> health damage/losses were borne by <strong>the</strong> private sec<strong>to</strong>r (i.e., nongovernmental, <strong>in</strong>-16 The Damage and Loss Assessment (DaLA) methodology was <strong>in</strong>itially developed by <strong>the</strong> UN Economic Commission forLat<strong>in</strong> America and <strong>the</strong> Caribbean (UN-ECLAC) <strong>in</strong> 1972. It has s<strong>in</strong>ce been improved through close cooperation of PAHO/WHO, <strong>the</strong> World Bank, Inter-American Development Bank, UNESCO, and ILO <strong>to</strong> capture <strong>the</strong> closest approximation ofdamage and losses due <strong>to</strong> disaster events. It is a flexible <strong>to</strong>ol that can be adapted <strong>to</strong> specific disaster types and governmen<strong>to</strong>wnership requirements. The DaLA methodology bases its assessments on <strong>the</strong> overall economy of <strong>the</strong> affected country.14
THE EARTHQUAKE: 12 JANUARY <strong>2010</strong> - Chapter 2clud<strong>in</strong>g for-profit and not-for-profit) and <strong>the</strong> environment sec<strong>to</strong>r (primarily for wasteand debris disposal) where <strong>the</strong> losses are borne almost entirely by <strong>the</strong> public sec<strong>to</strong>r.The value of material assets destroyed, <strong>in</strong>clud<strong>in</strong>g hous<strong>in</strong>g, schools, hospitals, roads andbridges, ports, and airports, has been estimated at US$ 4.302 billion (55% of <strong>the</strong> <strong>to</strong>tallosses due <strong>to</strong> <strong>the</strong> disaster). The variation <strong>in</strong> economic flows (lost production, fall <strong>in</strong>turnover, job and salary losses, <strong>in</strong>creased production costs, etc.) has reached US$ 3.561billion (equivalent <strong>to</strong> 45% of <strong>the</strong> <strong>to</strong>tal).Hous<strong>in</strong>g is <strong>the</strong> sec<strong>to</strong>r that has been most affected by <strong>the</strong> <strong>earthquake</strong> (damage is US$2.3 billion). Comparatively, <strong>the</strong> economic impact (damage and losses) <strong>in</strong> <strong>the</strong> socialsec<strong>to</strong>r is modest <strong>in</strong> monetary terms. <strong>Health</strong> and education sec<strong>to</strong>rs represent only 6%each of <strong>the</strong> economic impact (see Table 2.1).Table 2.1 Damage and losses from <strong>the</strong> <strong>2010</strong> <strong>Haiti</strong> <strong>earthquake</strong>(rounded <strong>to</strong> millions of US dollars)Sec<strong>to</strong>rs Public Private TotalSocial 352 (23.2%) 1,161 (76.8%) 1,513 (19.4%)Water and sanitation 29 (12.3%) 206 (87.7%) 235 (3%)<strong>Health</strong> 282 (60%) 188 (40%) 470 (6%)Education 40 (8.4%) 437 (91.6%) 477 (6.1%)Food safety and nutrition 0 330 (100%) 330 (4.2%)Infrastructure, <strong>in</strong>clud<strong>in</strong>g hous<strong>in</strong>g 1,402 (31.4%) 3,059 (68.6%) 4,461 (57.2%)Production sec<strong>to</strong>rs 3 1,327 (100%) 1,330 (17%)Environment a 324 (64.3%) 175 (35.7%) 499 (6.4%)TOTAL 2,081 (26.7%) 5,722 (73.3%) 7,803 (100%)Source: Adapted from figures presented <strong>in</strong> Table 2 of <strong>the</strong> PDNA (<strong>Haiti</strong> <strong>2010</strong>, 7).a Damage and losses <strong>to</strong> <strong>the</strong> environment sec<strong>to</strong>r mostly <strong>in</strong>clude solid waste removal (debris, hospital waste, hazardoussubstances, etc.).The PDNA estimated that:• The central government’s overall deficit would likely rise from 4.4% of GDPfor <strong>the</strong> 2008/09 f<strong>in</strong>ancial year 17 <strong>to</strong> 7.1% of GDP dur<strong>in</strong>g <strong>the</strong> f<strong>in</strong>ancial year2009/10, despite a marked <strong>in</strong>crease <strong>in</strong> overall <strong>in</strong>come over <strong>the</strong> years preced<strong>in</strong>g<strong>the</strong> impact date.• The <strong>earthquake</strong> will entail a loss of 8.5% of exist<strong>in</strong>g jobs <strong>in</strong> <strong>the</strong> immediate future.• Poverty <strong>in</strong>dices have returned <strong>to</strong> 2001 levels (71% <strong>in</strong> moderate poverty and 50%<strong>in</strong> extreme poverty), cancel<strong>in</strong>g all modest progress made <strong>in</strong> <strong>the</strong> last decade. 18All <strong>the</strong>se fac<strong>to</strong>rs bear a direct short- and long-term impact on public health.17 The fiscal or f<strong>in</strong>ancial year <strong>in</strong> <strong>Haiti</strong> runs from 1 Oc<strong>to</strong>ber <strong>to</strong> 30 September.18 This projection does not take <strong>in</strong><strong>to</strong> account <strong>the</strong> promis<strong>in</strong>g prospects of <strong>the</strong> reconstruction activities.15
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Impact on <strong>in</strong>ternational and bilateral organizations• The UN and peacekeep<strong>in</strong>g forces lost <strong>the</strong>ir leaders and headquarters.• Many <strong>in</strong>ternational agencies were directly impacted by <strong>the</strong> <strong>earthquake</strong> and unable<strong>to</strong> respond as promptly as expected.The offices of most <strong>in</strong>ternational or bilateral agencies present <strong>in</strong> <strong>Haiti</strong> were located <strong>in</strong>Port-au-Pr<strong>in</strong>ce. Many of <strong>the</strong>m suffered <strong>in</strong>frastructure and staff losses.The UN mission (MINUSTAH) loss was considerable: 102 <strong>in</strong>ternational UN employeeslost <strong>the</strong>ir lives, among whom were <strong>the</strong> Special Representative and <strong>the</strong> Head ofMission, 7 o<strong>the</strong>r <strong>to</strong>p civilian staff, 36 military staff, and 7 UN police officers.Although <strong>the</strong> loss represents less than 1% of <strong>the</strong> entire UN staff <strong>in</strong> <strong>Haiti</strong>, <strong>the</strong> commandstructure of MINUSTAH and operat<strong>in</strong>g capacity of some UN agencies weretemporarily affected. The destruction of <strong>the</strong> Hotel Chris<strong>to</strong>pher which housed <strong>the</strong> MI-NUSTAH Headquarters, resulted <strong>in</strong> <strong>the</strong> loss of most command<strong>in</strong>g officers and left<strong>the</strong> operations <strong>in</strong> chaos. UN Mission search and rescue efforts focused primarily on itsown leaders and staff. Their transportation assets, for <strong>the</strong> most part, rema<strong>in</strong>ed unaffectedby <strong>the</strong> <strong>earthquake</strong>.The offices of many of <strong>the</strong> UN agencies, <strong>in</strong>clud<strong>in</strong>g that of PAHO/WHO, were ei<strong>the</strong>rdamaged or deemed unsecure, while part of <strong>the</strong>ir staff lost <strong>the</strong>ir accommodations.UN Headquarters16Pho<strong>to</strong>: UN, Logan Abassi
THE EARTHQUAKE: 12 JANUARY <strong>2010</strong> - Chapter 2Source: Reproduced from Information Management & M<strong>in</strong>e Action Programs (iMMAP) (<strong>2010</strong>) Earthquake <strong>in</strong> <strong>Haiti</strong>:Estimated Population Exposure. Available from www.immap.org/<strong>in</strong>dex.php?do=map_view&id=56&cat=12.Several bilateral cooperation agencies as well as <strong>in</strong>ternational NGOs suffered materialas well as human losses. The build<strong>in</strong>g of <strong>the</strong> Delegation of <strong>the</strong> European Commission,for <strong>in</strong>stance, became unsuitable and <strong>the</strong> staff was evacuated <strong>to</strong> San<strong>to</strong> Dom<strong>in</strong>go.Losses, material and human, of such a magnitude that affected external agencies contributed<strong>to</strong> mak<strong>in</strong>g <strong>the</strong> rapid organization of an emergency <strong>response</strong> all <strong>the</strong> more precariousand more dependent on headquarters outside of <strong>Haiti</strong>.As noted <strong>in</strong> <strong>the</strong> PDNA, by strik<strong>in</strong>g at <strong>the</strong> very heart of <strong>the</strong> <strong>Haiti</strong>an economy andadm<strong>in</strong>istration, <strong>the</strong> <strong>earthquake</strong> had an acute effect on <strong>the</strong> human and <strong>in</strong>stitutional<strong>response</strong> capacity both of <strong>the</strong> public and <strong>the</strong> private sec<strong>to</strong>rs, of <strong>in</strong>ternational technicaland f<strong>in</strong>ancial partners, and certa<strong>in</strong> NGOs.17
In <strong>the</strong> affected area, 30 out of 49hospitals were damaged or destroyed.<strong>Haiti</strong>’s University and EducationalHospital (HUEH), <strong>the</strong> country’s largesthospital, suffered serious physical as wellas functional losses. The hospital lostseveral staff dur<strong>in</strong>g <strong>the</strong> <strong>earthquake</strong>.Pho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>
Chapter3healthTheimpactMost of <strong>the</strong> health losses were <strong>the</strong> result of an extreme vulnerability <strong>to</strong> disasters, <strong>the</strong>deterioration of <strong>the</strong> medical care system, and dysfunctional public health programs.Accord<strong>in</strong>g <strong>to</strong> <strong>the</strong> Post-Disaster Needs Assessment (PDNA) carried out jo<strong>in</strong>tly by <strong>the</strong><strong>Haiti</strong>an Government and <strong>in</strong>ternational partners <strong>in</strong> February–March <strong>2010</strong>: 19• Some 1.5 million people, represent<strong>in</strong>g 15% of <strong>the</strong> nation’s population, were directlyaffected.• More than 220,000 lost <strong>the</strong>ir lives and more than 300,000 were <strong>in</strong>jured. 20• Some 1.3 million lived <strong>in</strong> temporary shelters <strong>in</strong> <strong>the</strong> Port-au-Pr<strong>in</strong>ce metropolitanarea <strong>in</strong> <strong>the</strong> months follow<strong>in</strong>g <strong>the</strong> impact.• Over 600,000 left <strong>the</strong> disaster zone <strong>to</strong> seek refuge elsewhere <strong>in</strong> <strong>the</strong> country.Problems that already existed <strong>in</strong> terms of access <strong>to</strong> health care, food, and basic serviceswere <strong>the</strong>reby exacerbated nationwide.The health impact <strong>in</strong> <strong>Haiti</strong> was of a much higher order of magnitude than <strong>in</strong> <strong>the</strong>tsunami-affected countries or <strong>in</strong> Pakistan (see Table 3.1).19 It should be noted that all of <strong>the</strong>se statistics have been <strong>in</strong>tensely questioned and rema<strong>in</strong> a matter of debate.20 The tsunami <strong>in</strong> 2004 claimed over 228,000 lives <strong>in</strong> 14 countries (Telford, Cosgrave, Hough<strong>to</strong>n 2006).19
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Table 3.1 Proportion of population killed or <strong>in</strong>jured <strong>in</strong> major disastersPopulation(millions)NumberkilledDeaths/1,000Number<strong>in</strong>juredInjured/1,000Indonesia (tsunami 2004) 228 167,540 a 0.7 25,572 b 0.1Sri Lanka (tsunami 2004) 20 35,322 a 1.8 21,441 c 1.1Pakistan (<strong>earthquake</strong> 2005) 161 73,338 d 0.5 128,309 d 0.8<strong>Haiti</strong> (<strong>earthquake</strong> <strong>2010</strong>) 10 From 65,275<strong>to</strong> 300,000 e 6.5 <strong>to</strong> 30 >300,000 30a Telford, Cosgrave, Hough<strong>to</strong>n 2006.b Doocy et al. 2009.c IFRC 2005.d CRED EM-Data.e See <strong>the</strong> follow<strong>in</strong>g section on mortality.Mortality• The <strong>in</strong>ternational community attaches far <strong>to</strong>o much importance <strong>to</strong> <strong>the</strong> mortality figure.• Donations should not be l<strong>in</strong>ked <strong>to</strong> <strong>the</strong> number of fatalities but ra<strong>the</strong>r <strong>to</strong> <strong>the</strong> numberof survivors and <strong>the</strong> extent of <strong>the</strong>ir needs.• Techniques and methods are available <strong>to</strong> estimate objectively <strong>the</strong> number of personskilled. They must be used when a complete census is not possible.• The endorsement of exaggerated official statistics by <strong>the</strong> humanitarian communityis counterproductive and damag<strong>in</strong>g.If development (health or o<strong>the</strong>rs) statistics are lack<strong>in</strong>g or unreliable <strong>in</strong> normal times,data follow<strong>in</strong>g massive disasters are no<strong>to</strong>riously <strong>in</strong>accurate. Initial estimates of numberof deaths or <strong>in</strong>juries rarely result from <strong>in</strong>dividual body counts, detailed list<strong>in</strong>gs fromfacilities or humanitarian organizations, or censuses or surveys conducted at a later stage.In <strong>the</strong> aftermath of most disasters, <strong>the</strong> number of deaths is a much-sought statisticby <strong>the</strong> mass media and <strong>the</strong> public. It is <strong>the</strong> most powerful figure <strong>to</strong> elicit emotionsand generosity. The usefulness of mortality statistics <strong>to</strong> gauge <strong>the</strong> magnitude of <strong>the</strong>needs (of survivors) is overstated.32FILMAfter <strong>earthquake</strong>s, an <strong>in</strong>itial rough estimate is usually announced <strong>in</strong> <strong>the</strong> first fewdays. Then, reported numbers rapidly <strong>in</strong>crease day after day, occasionally suddenlysoar<strong>in</strong>g <strong>to</strong> accommodate higher and conflict<strong>in</strong>g estimates advanced byhumanitarian organizations (for example, <strong>the</strong> Red Cross societies) or a publicstatement from higher authorities.In <strong>Haiti</strong>, <strong>the</strong> report<strong>in</strong>g of estimated numbers of deaths by <strong>the</strong> Direc<strong>to</strong>ratefor Civil Protection (and endorsed, de fac<strong>to</strong>, by <strong>the</strong> UN Office for <strong>the</strong> Coord<strong>in</strong>ationof Humanitarian Affairs [OCHA] and <strong>the</strong> <strong>in</strong>ternational community)followed <strong>the</strong> same pattern. An <strong>in</strong>itial rough estimate of 75,000 killed was providedafter one week, progressively <strong>in</strong>creas<strong>in</strong>g <strong>to</strong> 112,392 on Day 13. No fur<strong>the</strong>r officialrevisions were offered for ano<strong>the</strong>r 10 days. On 4 February, Day 24 of <strong>the</strong> disaster, <strong>the</strong>Prime M<strong>in</strong>ister made a public statement that “<strong>the</strong> number of killed could be as high as200,000 and that of <strong>in</strong>jured above 300,000.” The tally was <strong>in</strong>creased <strong>to</strong> 212,000 and<strong>the</strong> counter started ris<strong>in</strong>g aga<strong>in</strong> <strong>to</strong> reach 222,570 deaths (see Figure 3.1).32 32APho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>20
THE HEALTH IMPACT - Chapter 3Figure 3.1 Reported deaths by days s<strong>in</strong>ce <strong>earthquake</strong> impact250,000Fatalities reported200,000150,000100,00050,00008 10 12 13 26* 35 38 47Number of days s<strong>in</strong>ce impact*Prime M<strong>in</strong>ister made a statement <strong>in</strong>creas<strong>in</strong>g <strong>the</strong> death <strong>to</strong>ll <strong>to</strong> over 200,000 on 4 February <strong>2010</strong> (Day 24).Do estimated mortality figures reflect reality?Scientists rout<strong>in</strong>ely question <strong>the</strong> accuracy of estimates of deaths follow<strong>in</strong>g major disasters.Divergence <strong>in</strong> op<strong>in</strong>ion is usually on a reasonable order and does not question<strong>the</strong> credibility of <strong>the</strong> whole process.In <strong>the</strong> Indian Ocean tsunami, <strong>in</strong>itial estimates <strong>in</strong> Indonesia and Sri Lanka calculatedbodies recovered and miss<strong>in</strong>g persons separately. The latter figure was exceptionallyhigh due <strong>to</strong> <strong>the</strong> number washed away by <strong>the</strong> waves or buried under <strong>to</strong>ns of mud anddebris. As bodies were recovered days and weeks later, <strong>the</strong> first number (dead bodies)<strong>in</strong>creased rapidly while <strong>the</strong> number of miss<strong>in</strong>g rema<strong>in</strong>ed unchanged, because no identificationwas attempted <strong>in</strong> ei<strong>the</strong>r country. Mass media and agencies rapidly comb<strong>in</strong>edboth figures <strong>in</strong><strong>to</strong> one. The f<strong>in</strong>al statistics clearly <strong>in</strong>cluded significant double count<strong>in</strong>g.In <strong>the</strong> case of <strong>the</strong> Pakistan <strong>earthquake</strong> <strong>in</strong> 2005, <strong>the</strong> remoteness of most affected areasresulted <strong>in</strong> a very approximate figure probably reflect<strong>in</strong>g <strong>the</strong> death <strong>to</strong>ll with<strong>in</strong> reasonablemarg<strong>in</strong>s. There was limited opportunity for surveys or controversy.The Bam <strong>earthquake</strong> <strong>in</strong> Islamic Republic of Iran <strong>in</strong> 2003, which was a shallow, localized<strong>earthquake</strong> of manageable size, offers us an illustration of a correct approach. Asusual, <strong>in</strong>itial estimates overstated <strong>the</strong> number of casualties: For months <strong>the</strong> officialmortality figure was above 41,000 killed. Follow<strong>in</strong>g a special census, <strong>the</strong> authoritiesformally corrected <strong>the</strong> earlier estimate down <strong>to</strong> 26,271 out of a <strong>to</strong>tal of 142,376people <strong>in</strong> <strong>the</strong> affected areas. No o<strong>the</strong>r example of correction is reported.In <strong>Haiti</strong>, it is accepted that <strong>the</strong> number of deaths (and miss<strong>in</strong>g) caused by <strong>the</strong> <strong>earthquake</strong>was extraord<strong>in</strong>arily high. How high rema<strong>in</strong>s an issue.21
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>It was not until <strong>the</strong> publication of several studies carried out months after <strong>the</strong> impactthat <strong>the</strong> official process of report<strong>in</strong>g mortality figures was thrown <strong>in</strong><strong>to</strong> controversy, question<strong>in</strong>gits <strong>in</strong>tegrity and credibility. A survey by <strong>the</strong> University of Michigan and later astudy commissioned by USAID/<strong>Haiti</strong> suggested lower but statistically more credibleestimates of <strong>the</strong> number killed: 149,095 (University of Michigan) 21 or 65,575 (USAIDstudy) (see Box). It is unclear whe<strong>the</strong>r and when <strong>the</strong> relief authorities were <strong>in</strong>formed of<strong>the</strong> results of this survey published only n<strong>in</strong>e months after <strong>the</strong> impact. The Governmen<strong>to</strong>f <strong>Haiti</strong> unexpectedly raised fur<strong>the</strong>r <strong>the</strong> official figure <strong>to</strong> over 300,000 when commemorat<strong>in</strong>g<strong>the</strong> first anniversary of <strong>the</strong> <strong>earthquake</strong>, almost five times <strong>the</strong> lowest scientific estimate(see Table 3.2). Despite <strong>the</strong> methodological differences of <strong>the</strong> two studies, <strong>the</strong>yoffer significantly lower figures than those officially issued by national authorities.<strong>Haiti</strong>an fatalities: two surveys dispute official <strong>to</strong>llsUSAID studyThe death <strong>to</strong>ll was determ<strong>in</strong>ed based on two sources of <strong>in</strong>formation: 1) The color-codedbuild<strong>in</strong>g assessment carried out by <strong>Haiti</strong>’s M<strong>in</strong>istry of Public Works, Transport, Communication(MTPTC) through an <strong>in</strong>ternational entity 22 and 2) <strong>the</strong> Build<strong>in</strong>g Assessments and RubbleRemoval (BARR) survey <strong>in</strong> which people were asked how many of <strong>the</strong> residents <strong>in</strong> each of <strong>the</strong>houses assessed died, among o<strong>the</strong>r questions. The group calculated <strong>the</strong> deaths per residenceby us<strong>in</strong>g average occupancy per house (5.2) and average death rate by yellow, green, and redhouses. The study concludes that <strong>the</strong> number of people killed <strong>in</strong> <strong>the</strong> <strong>earthquake</strong> was 65,575(<strong>the</strong> range of <strong>the</strong> estimate at p < .01 is 46,190 <strong>to</strong> 84,961 dead) (Schwartz, Pierre, Calpas 2011).University of Michigan studyThe mortality rate is established compar<strong>in</strong>g two surveys: 1) a 2009 survey (pre-<strong>earthquake</strong>) carriedout by <strong>the</strong> University of Michigan, sampl<strong>in</strong>g 1,800 households <strong>in</strong> <strong>the</strong> Port-au-Pr<strong>in</strong>ce area;and 2) a post-<strong>earthquake</strong> survey conducted <strong>in</strong> <strong>2010</strong>, <strong>in</strong> which 1,732 (93.1%) of <strong>the</strong> 2009 sampledhousehold members were located. Us<strong>in</strong>g population estimates for <strong>the</strong> greater area of Port-Au-Pr<strong>in</strong>ce of 2,713,599 and an average of 5.7 persons per household, <strong>the</strong>y calculated 158,679 deaths:111,794 died dur<strong>in</strong>g or immediately after <strong>the</strong> <strong>earthquake</strong>, 37,301 died as result of <strong>the</strong> <strong>in</strong>juries,and 9,583 died of an illness <strong>in</strong> a period of six weeks follow<strong>in</strong>g <strong>the</strong> impact (Kolbe et al. <strong>2010</strong>).Table 3.2 Mortality estimates for <strong>Haiti</strong> <strong>earthquake</strong>SourceNumber killedGovernment (<strong>2010</strong>) 222,570Government (Jan 2011) 300,000Univ. of Michigan study 149,095USAID study 65,575It is important <strong>to</strong> note that <strong>the</strong> absence of data disaggregated by age and gender <strong>in</strong>official statistics had some impact on both <strong>the</strong> understand<strong>in</strong>g of <strong>the</strong> quake and its effects,as well as on programm<strong>in</strong>g <strong>the</strong> relief efforts <strong>in</strong> <strong>Haiti</strong>. 232221 This figure does not <strong>in</strong>clude <strong>the</strong> estimated number of deaths from illness unrelated <strong>to</strong> <strong>the</strong> <strong>earthquake</strong>.22 Miyamota International tra<strong>in</strong>ed 270 <strong>Haiti</strong>an eng<strong>in</strong>eers <strong>in</strong> build<strong>in</strong>g assessment techniques, us<strong>in</strong>g a color-coded system:Green = safe; Yellow = <strong>in</strong>habit after repairs; and Red = unsafe for occupancy. From February <strong>2010</strong> <strong>to</strong> <strong>January</strong> 2011 <strong>the</strong>team evaluated 382,256 Port-au-Pr<strong>in</strong>ce build<strong>in</strong>gs with <strong>the</strong> follow<strong>in</strong>g results: 205,539 green (54%), 99,043 yellow (26%),and 77,674 red (20%). This <strong>in</strong>itiative was endorsed by <strong>the</strong> M<strong>in</strong>istry of Public Works, Transport, and Communication, UNOffice for Project Services (UNOPS) and <strong>the</strong> Pan American Development Foundation (PADF).23 Very partial data <strong>in</strong> Indonesia suggest that mortality among women result<strong>in</strong>g from <strong>the</strong> tsunami was significantly higher <strong>in</strong>some fish<strong>in</strong>g villages.
THE HEALTH IMPACT - Chapter 3The ma<strong>in</strong> lesson for future disasters is not what <strong>the</strong> best estimate <strong>in</strong> <strong>Haiti</strong> was, it is <strong>the</strong>need for a transparent methodology <strong>to</strong> produce <strong>the</strong> official statistics. The credibility of<strong>the</strong> <strong>in</strong>ternational humanitarian community is also at stake: Although many <strong>in</strong>ternationalstaff privately questioned <strong>the</strong> credibility of <strong>the</strong> figures, all agencies and <strong>the</strong> massmedia welcomed <strong>the</strong> highest figures possible for <strong>the</strong>ir own purposes (for fund rais<strong>in</strong>g,readership, or o<strong>the</strong>r motives).In many catastrophes, <strong>the</strong> management of death figures, a difficult technical task underany circumstances, is handled politically. What is new <strong>in</strong> <strong>the</strong> case of <strong>Haiti</strong> is <strong>the</strong>significant and ris<strong>in</strong>g discrepancy between <strong>the</strong> official figures and <strong>the</strong> scientific estimates.This has led, more than a year after <strong>the</strong> event, <strong>to</strong> a public controversy, s<strong>in</strong>ce <strong>the</strong>amount of fund<strong>in</strong>g that a disaster deserves is closely l<strong>in</strong>ked <strong>in</strong> <strong>the</strong> public’s eyes <strong>to</strong> <strong>the</strong>number of persons killed. 24 It is <strong>in</strong>deed <strong>the</strong> recognition of this l<strong>in</strong>kage which <strong>in</strong>citesgovernments and agencies <strong>to</strong> opt for <strong>the</strong> highest figures possible.This perception needs <strong>to</strong> be changed: <strong>the</strong> ma<strong>in</strong> criteria for assistance should be <strong>the</strong>number of people <strong>in</strong> need (<strong>the</strong> dead are not <strong>in</strong> need of assistance) and <strong>the</strong> urgency andmagnitude of <strong>the</strong>ir need.Regardless of <strong>the</strong> controversy, <strong>the</strong> mortality rate was very high (almost 10% of <strong>the</strong>population <strong>in</strong> <strong>the</strong> metropolitan capital area if <strong>the</strong> official figure of 220,000 is accepted).The question is: why?The Richter scale read<strong>in</strong>g alone of an <strong>earthquake</strong> is a poor predic<strong>to</strong>r of <strong>the</strong> expectedmorbidity/mortality. Everyth<strong>in</strong>g is a matter of geological context (type of soil, epicenter,and hypocenter) and physical and socio-economic vulnerability. The trigger<strong>in</strong>gevent is natural, <strong>the</strong> disaster itself is not natural.All estimates are fairly illustrative of <strong>the</strong> gravity of <strong>the</strong> tragedy, as well as suitable for purposesof public <strong>in</strong>formation and fund rais<strong>in</strong>g. Whe<strong>the</strong>r fewer than 100,000 casualtiesor surpass<strong>in</strong>g 300,000, <strong>the</strong> impact is an immense tragedy for a poor country <strong>the</strong> size of<strong>Haiti</strong> (6.5 <strong>to</strong> 30 deaths per 1,000 <strong>in</strong>habitants accord<strong>in</strong>g <strong>to</strong> <strong>the</strong> figure selected). Comparatively,<strong>the</strong> mortality of <strong>the</strong> Indian Ocean tsunami was 1.8/1,000 <strong>in</strong> Sri Lanka and0.7/1,000 <strong>in</strong> Indonesia (see Table 3.1). Few families or <strong>in</strong>stitutions <strong>in</strong> Port-au-Pr<strong>in</strong>cewere spared fatalities.First, such a high mortality rate is not uncommon for a shallow <strong>earthquake</strong> directlyunder a densely populated area. In <strong>the</strong> Bam, Iran, <strong>earthquake</strong> <strong>in</strong> 2003, 18% of <strong>the</strong>population was killed.O<strong>the</strong>r fac<strong>to</strong>rs affect<strong>in</strong>g vulnerability are mentioned <strong>in</strong> a study by Mompelat (<strong>2010</strong>):• Extreme vulnerability of constructions;• High occupation density of dwell<strong>in</strong>gs;• Highly <strong>in</strong>stable soil (slopes);24 See, for example, <strong>the</strong> article “U.S. Reduces Estimates of Homeless <strong>in</strong> <strong>Haiti</strong> Quake”, New York Times, 31 May 2011.23
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>• Severe damage <strong>to</strong> facilities with high occupancy (schools, universities, adm<strong>in</strong>istration);• Mortality <strong>in</strong> <strong>the</strong> narrow streets;• Lack of access <strong>to</strong> medical care.Most of those fac<strong>to</strong>rs could have been m<strong>in</strong>imized by <strong>the</strong> adoption of a risk-reductionapproach <strong>in</strong>clud<strong>in</strong>g land use management and construction norms.On <strong>the</strong> positive side, <strong>the</strong> tim<strong>in</strong>g (4:53 PM) contributed <strong>to</strong> m<strong>in</strong>imize <strong>the</strong> impact. Manyadults and children were <strong>in</strong> <strong>the</strong> streets. One hour earlier, public offices and schoolswould have been occupied; a few hours later, most <strong>Haiti</strong>ans would have been at home.Immediate morbidity• The number of <strong>in</strong>juries by type and gravity is a critical statistic lack<strong>in</strong>g <strong>in</strong> most disasters.• A very simple list detail<strong>in</strong>g <strong>the</strong> type of <strong>in</strong>juries <strong>to</strong> be reported <strong>in</strong> <strong>the</strong> aftermath ofdisasters needs <strong>to</strong> be developed urgently at <strong>the</strong> global level.This section reviews <strong>the</strong> immediate impact on health, that is, primarily <strong>in</strong> terms of<strong>in</strong>juries and traumas. Delayed impact such as on disease transmission, mental health,violence, and nutrition is discussed <strong>in</strong> Chapter 6.Estimates of <strong>the</strong> number of persons <strong>in</strong>jured are also no<strong>to</strong>riously <strong>in</strong>accurate <strong>in</strong> most severedisasters <strong>in</strong> less developed countries. They offer at best a reasonable guess of <strong>the</strong> magnitudeof <strong>the</strong> problem. In <strong>Haiti</strong>, offer<strong>in</strong>g a scientific estimate on <strong>the</strong> number of <strong>in</strong>juries was almostimpossible. There was no registry of patients and no <strong>in</strong>formation system <strong>in</strong> most of <strong>the</strong>facilities. The situation can best be illustrated by <strong>the</strong> observation of a team arriv<strong>in</strong>g <strong>in</strong> Portau-Pr<strong>in</strong>ce10 days after <strong>the</strong> <strong>earthquake</strong> with <strong>the</strong> mission <strong>to</strong> res<strong>to</strong>re surgical services <strong>to</strong> <strong>the</strong>University Hospital (Peranteau et al. <strong>2010</strong>):“No patient identifiers were present and <strong>the</strong>re were no physical reportsaccompany<strong>in</strong>g patients <strong>to</strong> <strong>in</strong>dicate <strong>the</strong>ir diagnoses, operations or careplan . . . At first we used scraps of papers or cardboard taped <strong>to</strong> <strong>the</strong>patient <strong>in</strong>dicat<strong>in</strong>g name and <strong>in</strong>jury . . . as paper became available, as<strong>in</strong>gle sheet became <strong>the</strong> makeshift chart taped <strong>to</strong> <strong>the</strong> edge of <strong>the</strong> stretcher.”If such a situation prevailed after two weeks <strong>in</strong> <strong>the</strong> country’s largest hospital, it is notsurpris<strong>in</strong>g that, with <strong>the</strong> exception of self-susta<strong>in</strong>ed military facilities, no compileddata were available for overall management or report<strong>in</strong>g.Although <strong>the</strong> number of <strong>in</strong>jured is a critical <strong>in</strong>dica<strong>to</strong>r of <strong>the</strong> need for assistance, <strong>the</strong>external pressure for updated figures was far less than for mortality data. Consequently,those statistics were less frequently released by <strong>Haiti</strong>’s Direc<strong>to</strong>rate for Civil Protection.As was true for mortality, <strong>the</strong> morbidity figure evolved over time, start<strong>in</strong>g with a roughestimate of more than 200,000 <strong>in</strong>jured on Day 9 (20 <strong>January</strong>) <strong>to</strong> be readjusted down<strong>to</strong> 194,000 on Day 15, and <strong>in</strong>creased <strong>to</strong> 196,501 <strong>the</strong> next day. On 4 February, an24
THE HEALTH IMPACT - Chapter 3estimate of “over 300,000 <strong>in</strong>jured” was announced publicly by <strong>the</strong> Prime M<strong>in</strong>isterand adopted officially by <strong>the</strong> Direc<strong>to</strong>rate for Civil Protection effective on 6 February(Day 26). These figures must be considered with caution and are only <strong>in</strong>dicative of <strong>the</strong>magnitude of <strong>the</strong> impact.The challenge of estimat<strong>in</strong>g <strong>the</strong> numbers and types of <strong>in</strong>juries rema<strong>in</strong>:• What def<strong>in</strong>es an <strong>in</strong>jured person, and <strong>the</strong> methodology used <strong>to</strong> calculate <strong>the</strong> figuresare unknown.• There was no systematic collection of data from <strong>the</strong> many medical teams attend<strong>in</strong>g<strong>to</strong> <strong>the</strong> <strong>in</strong>jured.Disaggregation by age, sex, or type of <strong>in</strong>juries was only available from some of <strong>the</strong> bes<strong>to</strong>rganizedforeign medical teams or hospitals. Their patients represent a very small andbiased sample. Often, <strong>the</strong>se data were analyzed retrospectively after <strong>the</strong> <strong>in</strong>terventionand <strong>the</strong> f<strong>in</strong>d<strong>in</strong>gs could be shared only after be<strong>in</strong>g published <strong>in</strong> peer-reviewed journals.Table 3.3 shows <strong>the</strong> distribution of patients by type of <strong>in</strong>jury for <strong>the</strong> patients admitted<strong>to</strong> <strong>the</strong> University of Miami Global Institute/Project Medishare field hospital <strong>in</strong>Port-au-Pr<strong>in</strong>ce over a three-month period (CDC 2011b, 1675). This field hospitalalso served as a referral treatment center and <strong>the</strong> data presented may not be fullyrepresentative of <strong>the</strong> overall pathology. In particular, <strong>the</strong> most severe diagnosis groups(head/sp<strong>in</strong>e, crush syndrome) are probably over-represented among <strong>the</strong> patients. Therate of 5.6% crush syndrome cannot be generalized <strong>to</strong> <strong>the</strong> entire <strong>in</strong>jured populationalthough <strong>the</strong>re is evidence that <strong>the</strong> <strong>in</strong>cidence of crush syndrome can reach 2% <strong>to</strong> 5%overall among disaster victims (Sheng 1987).Field HospitalPho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>25
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Table 3.3 Distribution of patients by type of <strong>in</strong>jury admitted<strong>to</strong> a field hospital, 21 <strong>January</strong>–28 May <strong>2010</strong>Injury diagnosis groups Number admitted %Head/Sp<strong>in</strong>e 142 16.6Fracture: Extremity 188 21.9Burn 40 4.7Penetrat<strong>in</strong>g <strong>in</strong>jury 27 3.1Fracture: Non-extremity 43 5.0Crush/Compartment syndrome 48 5.6Spra<strong>in</strong>/Stra<strong>in</strong>/Contusion 18 2.1Wound <strong>in</strong>fection/Abscess 158 18.4Abrasion/Laceration/Cut 133 15.5Traumatic avulsion/Amputation 22 2.6O<strong>the</strong>r 38 4.4Total 857 100Source: CDC 2011b, 1675.The health authorities established a National Sent<strong>in</strong>el Surveillance Site (NSSS) system<strong>to</strong> complement <strong>the</strong> rout<strong>in</strong>e sent<strong>in</strong>el surveillance system (COSE) <strong>to</strong> address specificpost-<strong>earthquake</strong> conditions. The NSSS was set up with support from PAHO/WHOand CDC. From 25 <strong>January</strong> (almost two weeks after impact) 51 surveillance siteswith<strong>in</strong> and outside <strong>the</strong> affected area reported new admissions segregated by ma<strong>in</strong>cause, diseases as well as <strong>in</strong>juries. Both NSSS and COSE cont<strong>in</strong>ue <strong>to</strong> function. Thedata from NSSS are presented <strong>in</strong> Table 3.4.Table 3.4 Reported post-<strong>earthquake</strong> <strong>in</strong>juries by age group,25 <strong>January</strong> –24 April <strong>2010</strong>Type of <strong>in</strong>jury Age group (years) Total< 5 years > 5 years UnknownTrauma 141 947 60 1,148 (22.7%)Fracture 61 321 85 467 (9.2%)Head <strong>in</strong>jury 2 23 2 27 (0.5%)Weapon or dagger <strong>in</strong>jury 4 96 11 111 (2.2%)Burns 37 99 13 149 (2.9%)Infected wounds 195 2,691 175 3,061 (60.4%)Crush syndrome 5 78 5 88 (1.7%)Amputations 3 11 0 14 (0.2%)Total 448 4,266 351 5,065Source: Adapted from Magloire et al. <strong>2010</strong>.26
THE HEALTH IMPACT - Chapter 3As reported by Magloire et al. (<strong>2010</strong>) <strong>the</strong> surveillance system could not describe <strong>the</strong> immediatetrauma effects of <strong>the</strong> <strong>earthquake</strong> as many victims died or were treated before <strong>the</strong> report<strong>in</strong>gmechanism was established. It is important <strong>to</strong> note that <strong>the</strong> 51 report<strong>in</strong>g sites were selectedfrom among exist<strong>in</strong>g facilities associated with <strong>the</strong> U.S. President’s Emergency Plan for AIDSRelief (PEPFAR). They offered general care for a fee but were not equipped for emergencytrauma care. Specialized field hospitals and teams were not <strong>in</strong>cluded among report<strong>in</strong>g sites.F<strong>in</strong>ally, <strong>the</strong> data <strong>in</strong>clude all <strong>in</strong>juries whe<strong>the</strong>r or not related <strong>to</strong> <strong>the</strong> <strong>earthquake</strong>. It should benoted that traffic accidents and violence are major sources of daily <strong>in</strong>juries <strong>in</strong> <strong>Haiti</strong>.First, <strong>the</strong> 5,065 cases of trauma reported represented only 12% of <strong>the</strong> <strong>to</strong>tal of new patientswith reportable conditions (16 additional <strong>in</strong>fectious and non-<strong>in</strong>fectious conditionswere <strong>in</strong>cluded). As noted by Magloire et al., <strong>in</strong> <strong>the</strong> two departments near <strong>the</strong> epicenter,<strong>in</strong>juries accounted for 9.2%, while <strong>in</strong> <strong>the</strong> eight departments fur<strong>the</strong>r from <strong>the</strong>epicenter, <strong>the</strong>y accounted for 15.2%. The migration of <strong>the</strong> population, <strong>the</strong> compet<strong>in</strong>gpresence of trauma teams and hospitals <strong>in</strong> <strong>the</strong> affected departments, and <strong>the</strong> generallypoor public attendance at <strong>the</strong> report<strong>in</strong>g sites may expla<strong>in</strong> this surpris<strong>in</strong>g result.Never<strong>the</strong>less, <strong>the</strong> data are valuable for guidance of foreign teams arriv<strong>in</strong>g two weeksor more after an <strong>earthquake</strong>:• Infected wounds are <strong>the</strong> ma<strong>in</strong> condition past <strong>the</strong> immediate emergency;• Fractures rema<strong>in</strong> a serious burden even two weeks after <strong>the</strong> impact;• Demand for rout<strong>in</strong>e normal pathology rapidly exceeds that for treatment of <strong>earthquake</strong>-relatedtrauma.Ano<strong>the</strong>r source of data is <strong>the</strong> consolidated survey by Handicap International (Calvotand Shivji, forthcom<strong>in</strong>g). It provides <strong>the</strong> best picture of <strong>the</strong> situation based on visits<strong>to</strong> 17 hospitals with <strong>in</strong>terviews and review of almost 2,600 patients. As with any o<strong>the</strong>rpartial data, <strong>the</strong>y are not fully representative. Among <strong>the</strong>ir observations (Table 3.5) is<strong>the</strong> relatively higher <strong>in</strong>cidence of <strong>in</strong>juries among <strong>the</strong> work<strong>in</strong>g age group (18–59 yearsold). In this group, women were particularly vulnerable (57% women versus 43% men).Table 3.5 Sample of persons with <strong>in</strong>juries visited <strong>in</strong> hospitals <strong>in</strong> <strong>Haiti</strong>,by age group and sex, <strong>January</strong> <strong>2010</strong>Age group Male Female Total Percentageby age groupDistribution of age group<strong>in</strong> <strong>to</strong>tal population< 5 80 52 132 5% 12%5 <strong>to</strong> 17 188 207 395 15% 32%18 <strong>to</strong> 59 741 1,039 1,780 69% 49%> 60 94 193 287 11% 7%Total 1103 1,491 2,594 100% 100%Population 43% 57%with <strong>in</strong>juriesTotalPopulation48% 52%Note: These figures are based on persons with <strong>in</strong>juries visited by Handicap International teams <strong>in</strong> hospitals between 15 and 29<strong>January</strong> <strong>2010</strong>. The team focused on persons with <strong>in</strong>juries requir<strong>in</strong>g urgent post-<strong>in</strong>jury or post-operative rehabilitation care,so <strong>the</strong> data cannot be <strong>in</strong>terpreted as represent<strong>in</strong>g all <strong>in</strong>juries susta<strong>in</strong>ed <strong>in</strong> <strong>the</strong> <strong>earthquake</strong>. Reproduced with permission of <strong>the</strong>authors (Calvot and Shivji, forthcom<strong>in</strong>g).27
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>The same study describes <strong>the</strong> distribution by type of <strong>in</strong>jury. As shown <strong>in</strong> Table 3.6,approximately half were fractures and 16% were amputations.Table 3.6 Type of <strong>in</strong>jury <strong>in</strong> persons visited <strong>in</strong> hospitals <strong>in</strong> <strong>Haiti</strong>,<strong>January</strong> <strong>2010</strong>Type of <strong>in</strong>jury Number PercentageFractures 1,233 48%Amputations 407 16%Sp<strong>in</strong>al cord and traumatic bra<strong>in</strong> <strong>in</strong>juries 41 2%Burns 27 1%Eye <strong>in</strong>juries 20 1%O<strong>the</strong>r, unspecified 866 33%Total 2,594 100%Note: See note for Table 3.5; reproduced with permission of <strong>the</strong> authors (Calvot and Shivji, forthcom<strong>in</strong>g).Compil<strong>in</strong>g <strong>the</strong> statistics from medical teams, if and when available, is fur<strong>the</strong>r complicated by<strong>the</strong> absence of standard nomenclature and def<strong>in</strong>itions of type of <strong>in</strong>juries.Crush syndromeCrush syndrome cont<strong>in</strong>ues <strong>to</strong> be underreported <strong>in</strong> most disasters worldwide.Crush syndrome is a condition caused by prolonged compression of skeletal muscles lead<strong>in</strong>g<strong>to</strong> renal failure. There is no consolidated s<strong>in</strong>gle source on <strong>the</strong> <strong>in</strong>cidence of this conditionafter <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong>. In addition <strong>to</strong> <strong>the</strong> 48 cases referred <strong>to</strong> <strong>the</strong> Miami Universityfield hospital and <strong>the</strong> 88 reported by <strong>the</strong> surveillance system, 25 <strong>the</strong> Renal Disaster ReliefTask Force of <strong>the</strong> International Society of Nephrology work<strong>in</strong>g through Médec<strong>in</strong>s SansFrontières (MSF) tallied 51 cases of acute kidney <strong>in</strong>jury (AKI) (Vanholder et al. <strong>2010</strong>).Whe<strong>the</strong>r those cases are dist<strong>in</strong>ct from those reported elsewhere is unknown.When compar<strong>in</strong>g <strong>the</strong> 51 acute kidney <strong>in</strong>jury patients with crush <strong>in</strong>juries <strong>in</strong> <strong>the</strong> <strong>Haiti</strong>event with <strong>in</strong>jury <strong>in</strong> o<strong>the</strong>r disasters, <strong>the</strong> specialized Renal Task Force found that prevalenceof AKI was low <strong>in</strong> <strong>Haiti</strong>. In assess<strong>in</strong>g <strong>the</strong>se results, <strong>the</strong> Task Force (Vanholder etal. 2011) observed:“. . . several fac<strong>to</strong>rs may have <strong>in</strong>fluenced this, such as: <strong>the</strong> fact that it occurreddur<strong>in</strong>g <strong>the</strong> day, when people are up and about, favor<strong>in</strong>g head and chest traumaand decreas<strong>in</strong>g <strong>the</strong> compression trauma <strong>to</strong> muscles; <strong>the</strong> presence of many build<strong>in</strong>gswhich were not sturdy enough <strong>to</strong> cause severe muscle trauma; difficultiesencountered with early rescue; <strong>the</strong> extrication of most victims by neighbors orfamily members result<strong>in</strong>g <strong>in</strong> a selection of less heavily wounded people, anda lack of immediate medical help for <strong>the</strong> occasional severely affected victim.”2825 While surgical trauma hospitals or specialized teams can be entrusted <strong>in</strong> this difficult diagnosis, <strong>the</strong> surveillance system’ssent<strong>in</strong>el sites are general care facilities provid<strong>in</strong>g AIDS treatment and may not be fully familiar with this condition. Thisleaves some doubt about <strong>the</strong> 88 cases reported by <strong>the</strong> surveillance system several weeks after <strong>the</strong> impact.
THE HEALTH IMPACT - Chapter 3Ano<strong>the</strong>r plausible explanation may be high mortality associated with severe underreport<strong>in</strong>gdue <strong>to</strong> <strong>the</strong> absence of centralized data collection <strong>in</strong> <strong>the</strong> first two weeks.Sp<strong>in</strong>al cord <strong>in</strong>juriesThere is scarce <strong>in</strong>formation on <strong>the</strong> number of sp<strong>in</strong>al cord <strong>in</strong>jury (SCI) patients whosurvived <strong>the</strong> first days after <strong>the</strong> <strong>earthquake</strong>. A survey by Handicap International(Calvot and Shavji, forthcom<strong>in</strong>g) estimated <strong>the</strong> number <strong>to</strong> be above 100, later revisedcloser <strong>to</strong> 150. Information <strong>in</strong> <strong>the</strong> <strong>Haiti</strong> SCI database 26 <strong>in</strong> mid-2011 <strong>in</strong>dicatesover 200 beneficiaries, of which 135 susta<strong>in</strong>ed a SCI directly as a result of <strong>the</strong> <strong>earthquake</strong>;<strong>the</strong> majority of patients presented complete paraplegia. Statistics cont<strong>in</strong>ue<strong>to</strong> be collected and this number will <strong>in</strong>crease. The death <strong>to</strong>ll amongst this grouprema<strong>in</strong>s unknown.Most of <strong>the</strong> severe cases (cervical lesions or multi-trauma) probably did not survive <strong>the</strong>rough handl<strong>in</strong>g by bystanders and <strong>the</strong> <strong>in</strong>itial lack of medical care (Burns et al. <strong>2010</strong>).It is important <strong>to</strong> recall <strong>the</strong> fact that many <strong>in</strong>jured were not sent <strong>to</strong> health facilities <strong>in</strong>time because of <strong>the</strong> difficulties of mov<strong>in</strong>g <strong>in</strong> <strong>the</strong> destroyed city dur<strong>in</strong>g <strong>the</strong> first night(electricity was cut <strong>in</strong> most areas). Many may have died <strong>in</strong> <strong>the</strong> street despite <strong>the</strong> factthat neighbors and relatives removed <strong>the</strong>m from <strong>the</strong> rubble. The very low level of “firstaid” culture <strong>in</strong>creased <strong>the</strong> on-site mortality as most simple, life-sav<strong>in</strong>g acts were by andlarge unknown.Impact on health servicesImpact on health <strong>in</strong>frastructure• The immediate impact on <strong>the</strong> capacity of <strong>the</strong> health services has been dramatic,both <strong>in</strong> terms of <strong>in</strong>frastructure and health workers.• The capacity of <strong>the</strong> public and private sec<strong>to</strong>r <strong>to</strong> offer immediate medical assistancewas considerably reduced at a time when it was most needed.32FILMWith<strong>in</strong> <strong>the</strong> affected departments, 30 out of 49 hospitals were damaged or destroyed.The ability of <strong>the</strong> health care system <strong>to</strong> respond has been permanentlyaffected by <strong>the</strong> destruction, and delivery of service is disorganized. The M<strong>in</strong>istryof <strong>Health</strong> was unable <strong>to</strong> fulfill its leadership role, primarily because its ma<strong>in</strong>build<strong>in</strong>g was completely destroyed.The damage predom<strong>in</strong>antly affected <strong>the</strong> secondary and tertiary facilities, while90% of primary health care centers <strong>in</strong> <strong>the</strong> affected departments rema<strong>in</strong>ed <strong>in</strong>tac<strong>to</strong>r suffered only light damage (see Table 3.7).Pho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>32 32A26 The confidential <strong>Haiti</strong> SCI Database was created <strong>in</strong> March <strong>2010</strong> and cont<strong>in</strong>ues <strong>to</strong> be adm<strong>in</strong>istered by Heal<strong>in</strong>g Hands for<strong>Haiti</strong>/<strong>Haiti</strong> Hospital Appeal.29
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Specialized facilities were also affected:• Before <strong>the</strong> <strong>earthquake</strong>, <strong>the</strong>re were at least four hemodialysis units across <strong>Haiti</strong>,treat<strong>in</strong>g approximately 100 chronic patients. One unit was lost dur<strong>in</strong>g <strong>the</strong> <strong>earthquake</strong>.• The <strong>earthquake</strong> destroyed <strong>the</strong> build<strong>in</strong>gs hous<strong>in</strong>g <strong>the</strong> National Center for Transfusionsand <strong>the</strong> National Blood Safety Program. For <strong>the</strong> first eight days after <strong>the</strong><strong>earthquake</strong>, no <strong>Haiti</strong>an blood was available for transfusion.• The sole hospital for chronic mental disease was seriously damaged <strong>in</strong> <strong>the</strong> <strong>earthquake</strong>.Most of <strong>the</strong> 76 patients slept on <strong>the</strong> hospital grounds with no protectionfor a susta<strong>in</strong>ed period of time.Table 3.7 Damage susta<strong>in</strong>ed by type of health structureLevel of damageby type of structureNo damageor very littledamageLightdamageSeveredamageCompletelydestroyedTotalSecondary and tertiary14 5 22 8 49hospitals<strong>Health</strong> centers and cl<strong>in</strong>ics 215 38 12 9 274M<strong>in</strong>istry of <strong>Health</strong> and4 8 1 10 23o<strong>the</strong>r adm<strong>in</strong>istrativebuild<strong>in</strong>gsUniversity and tra<strong>in</strong><strong>in</strong>g23 2 3 19 47<strong>in</strong>stitutesTotal 256 53 38 46 393Total as a percentage (%) 65 14 10 12 100Source: <strong>Haiti</strong>, PDNA <strong>2010</strong>, Table 16.In several facilities, personnel refused <strong>to</strong> re-enter premises <strong>the</strong>y deemed unsafe <strong>in</strong> spiteof structurally m<strong>in</strong>or or cosmetic damages and reassurance from eng<strong>in</strong>eers. This is notuncommon. The same reluctance <strong>to</strong> reoccupy facilities that were emptied <strong>to</strong>o hastilywas observed after <strong>the</strong> <strong>earthquake</strong>s <strong>in</strong> Mexico City (1985) and El Salvador (2001). It isfar easier <strong>to</strong> take <strong>the</strong> decision <strong>to</strong> evacuate a hospital than <strong>to</strong> reoccupy it. The long-termsolution is <strong>to</strong> carry out risk reduction prior <strong>to</strong> an <strong>earthquake</strong> through a careful structuraland nonstructural assessment of critical facilities <strong>to</strong> determ<strong>in</strong>e which are at risk and mayneed evacuation. Those considered resilient <strong>to</strong> <strong>earthquake</strong>s should not be evacuated at<strong>the</strong> first sign of seismic activity. Few facilities <strong>in</strong> Port-au-Pr<strong>in</strong>ce would fit <strong>in</strong> this category.NGOs are major stakeholders <strong>in</strong> <strong>the</strong> provision of medical care <strong>in</strong> <strong>Haiti</strong>. They have notbeen spared by <strong>the</strong> impact. All MSF structures (except one emergency facility) wereseverely damaged, some with patients and staff members trapped <strong>in</strong>side.<strong>Haiti</strong>’s University and Educational Hospital (HUEH—also known as General Hospital),<strong>the</strong> country’s largest, suffered serious physical as well as functional losses(Table 3.8).30
THE HEALTH IMPACT - Chapter 3Table 3.8 Earthquake damage <strong>to</strong> <strong>the</strong> <strong>Haiti</strong> University Hospital (HUEH)Build<strong>in</strong>gs entirely unsafeDepartment of SurgeryOutpatient consultationPediatric departmentBuild<strong>in</strong>gs safe and usableAdm<strong>in</strong>istrationMost of <strong>in</strong>ternal medic<strong>in</strong>eMost of emergency servicesMaternityNew facilities (urology and derma<strong>to</strong>logy)RadiologyThe HUEH eng<strong>in</strong>eers ordered immediate evacuation of all premises <strong>in</strong> case of aftershock.This recommendation was reportedly confirmed later by separate assessmentsby USAID, U.S. Army Corps of Eng<strong>in</strong>eers, PAHO/WHO, and Spa<strong>in</strong>’s Fire Brigadeexperts. After <strong>the</strong> second aftershock, <strong>the</strong> use of emergency services was reduced. After<strong>the</strong> third aftershock, <strong>the</strong> patients refused <strong>to</strong> re-enter <strong>the</strong> build<strong>in</strong>gs and <strong>the</strong> medicalpersonnel expressed fear about work<strong>in</strong>g <strong>in</strong> <strong>the</strong> oldest build<strong>in</strong>gs. Consequently, <strong>the</strong>decision was made <strong>to</strong> place all patients and most of <strong>the</strong> operat<strong>in</strong>g rooms under tents. 27This reaction was not limited <strong>to</strong> public facilities run by <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong>. MostMSF hospitals were damaged and unusable, and where still <strong>in</strong>tact, patients and staffwere <strong>to</strong>o frightened <strong>to</strong> enter, so all MSF services and hospitals were placed <strong>in</strong> tents.27 Abstracted and translated from a report from <strong>the</strong> HUEH direc<strong>to</strong>r <strong>to</strong> <strong>the</strong> M<strong>in</strong>ister of <strong>Health</strong>.<strong>Haiti</strong>’s University and Educational Hospital31www. maps.google.com
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>PROMESS, <strong>the</strong> central pharmaceutical warehouse, rema<strong>in</strong>ed mostly <strong>in</strong>tact. Fortunately,its s<strong>to</strong>ck had been replenished at <strong>the</strong> end of 2009.Impact on health personnelThe <strong>earthquake</strong> did not spare M<strong>in</strong>istry of <strong>Health</strong> personnel. Very high but unconfirmedestimates of losses were circulated and occasionally published. These figureswere shown <strong>to</strong> be <strong>in</strong>accurate by a retrospective survey on <strong>the</strong> impact of <strong>the</strong> <strong>earthquake</strong>on <strong>the</strong> health staff carried out two months after <strong>the</strong> impact by <strong>the</strong> Human ServicesDirec<strong>to</strong>rate of <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong> (MSPP <strong>2010</strong>a).In this survey, a census was conducted <strong>in</strong> <strong>the</strong> three affected departments. Of 6,812 employees,5,879 health workers (86%) were identified based on questionnaires sent <strong>to</strong>all M<strong>in</strong>istry of <strong>Health</strong> <strong>in</strong>stitutions. Of <strong>the</strong> 5,879, 61 were reported killed; 59 of <strong>the</strong>sewere <strong>in</strong> West Department, where <strong>the</strong> capital is located. These figures <strong>in</strong>clude M<strong>in</strong>istryemployees only. They do not cover students (medical or nurs<strong>in</strong>g), whose mortality waspresumably higher due <strong>to</strong> <strong>the</strong> collapse of <strong>the</strong> nurs<strong>in</strong>g school, among o<strong>the</strong>r causes. 28The reasons for <strong>the</strong> relatively low mortality figure are simple: as mentioned earlier, at<strong>the</strong> time of <strong>the</strong> <strong>earthquake</strong>, office workers had ma<strong>in</strong>ly left <strong>the</strong>ir workplaces and wereon <strong>the</strong>ir way home.Most practic<strong>in</strong>g doc<strong>to</strong>rs divide <strong>the</strong>ir work<strong>in</strong>g time between official duties <strong>in</strong> a publicfacility and private practice. This is a life necessity given <strong>the</strong> meager and irregular28 The nurs<strong>in</strong>g school at Lumière University—one of three official nurs<strong>in</strong>g schools <strong>in</strong> <strong>the</strong> country—was reduced <strong>to</strong> rubble,kill<strong>in</strong>g an estimated 150 students (UNFPA <strong>2010</strong>).Local nurs<strong>in</strong>g staff at field hospital32Pho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>
THE HEALTH IMPACT - Chapter 3salaries paid by <strong>the</strong> Government. Relatively few physicians were present <strong>in</strong> <strong>the</strong> healthfacilities at <strong>the</strong> time of <strong>the</strong> impact. For <strong>in</strong>stance, <strong>in</strong> <strong>the</strong> ma<strong>in</strong> tertiary level facility, <strong>the</strong>University Hospital, only <strong>the</strong> night shift was present.In addition, <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong> survey found that 245 (2.2%) of M<strong>in</strong>istry stafflost a member of <strong>the</strong>ir immediate family (spouse or children) and 3,955 (67%) weretechnically homeless (30% of <strong>the</strong>ir houses were destroyed and 37% were damagedand potentially unsecure). The fact that many M<strong>in</strong>istry staff were reported absent forsome time is largely attributed <strong>to</strong> <strong>the</strong> fact that <strong>the</strong>y had <strong>to</strong> f<strong>in</strong>d relatives and organizefor <strong>the</strong>ir survival before report<strong>in</strong>g <strong>to</strong> <strong>the</strong>ir duty stations.It was estimated that 50% of <strong>the</strong> health workers were liv<strong>in</strong>g under tents for a susta<strong>in</strong>edperiod of time.Impact on population displacement• Reasonable estimates on size and place of displacements are essential for plann<strong>in</strong>g<strong>the</strong> delivery of health, water, and sanitation services.• Statistics on displacement tend <strong>to</strong> be on <strong>the</strong> high side <strong>in</strong>itially and are contestedlater.• The health effects of displacement are not limited <strong>to</strong> areas physically affected by<strong>the</strong> <strong>earthquake</strong>.The level of destruction and loss of employment and homes led many people <strong>to</strong> seekshelter <strong>in</strong> temporary settlements. The concentration of displaced families <strong>in</strong> thousandsof small camps and settlements presented a health risk <strong>in</strong> itself and a challenge for <strong>the</strong>provision of health services because it caused a massive redistribution of catchment areas.The situation was quite dist<strong>in</strong>ct from that observed <strong>in</strong> o<strong>the</strong>r countries where spaceallowed for organized, medium-scale settlements (10,000 persons or more). There wasno vacant land <strong>in</strong> Port-au-Pr<strong>in</strong>ce itself and all small public spaces were overcrowded, <strong>in</strong>itiallyleav<strong>in</strong>g only 2 or 3 square meters per person. Common facilities (water, electricity,waste disposal) were non-existent and would compete for space.Moni<strong>to</strong>r<strong>in</strong>g <strong>the</strong> constant flux of displaced households under <strong>the</strong> conditions <strong>in</strong> <strong>Haiti</strong>was particularly prone <strong>to</strong> <strong>in</strong>accuracy. The number of camps was close <strong>to</strong> 1,200, somehous<strong>in</strong>g only a few hundred persons. Families (or some of <strong>the</strong>ir members) shiftedfrom place <strong>to</strong> place accord<strong>in</strong>g <strong>to</strong> <strong>the</strong> benefits (aid) <strong>to</strong> be expected. A detailed descriptionof <strong>the</strong> registration strategy used by <strong>the</strong> Camp Coord<strong>in</strong>ation and Camp Management“Cluster” was circulated by <strong>the</strong> International Organization for Migration(IOM) <strong>in</strong> April <strong>2010</strong>.An official number of <strong>in</strong>ternally displaced after <strong>the</strong> <strong>earthquake</strong> (1.5 million <strong>in</strong> temporarycamps) was released by IOM and accepted <strong>in</strong>itially by all partners, only <strong>to</strong>be questioned one year later by scientists (and mass media). Discrepancies betweensources as well as <strong>in</strong>ternal <strong>in</strong>consistencies <strong>in</strong> <strong>the</strong> figures are illustrated <strong>in</strong> Table 3.9.33
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Table 3.9 Numbers of persons liv<strong>in</strong>g <strong>in</strong> temporary shelters<strong>in</strong> <strong>Haiti</strong> after <strong>earthquake</strong>, by sourceSourcePDNA (March <strong>2010</strong>)IOM Registration Strategy (April<strong>2010</strong>)IOM Press Brief<strong>in</strong>g Note (Dec <strong>2010</strong>)USAID survey (Schwartz et al. 2011)Data1.5 M persons directly affectedAround 1.3 M liv<strong>in</strong>g <strong>in</strong> temporary shelters <strong>in</strong> <strong>the</strong> metropolitanPort-au-Pr<strong>in</strong>ce area; 500,000 moved <strong>in</strong><strong>to</strong> <strong>the</strong> res<strong>to</strong>f <strong>the</strong> country450,000 households liv<strong>in</strong>g <strong>in</strong> shelters a (i.e., at least 2 Mpersons)Peak figure <strong>in</strong> <strong>the</strong> camps was 1.5 MEstimated number of people who went <strong>to</strong> camps <strong>in</strong><strong>January</strong> is 866,412 <strong>to</strong> 894,588 ( p < .01)By April <strong>2010</strong>, approximately half of those who had gone<strong>to</strong> camps or <strong>the</strong> countryside had returned homea Accord<strong>in</strong>g <strong>to</strong> <strong>the</strong> IOM, household size is estimated between 5.2 and 5.7 persons.The lesson is that any statistic, not only mortality data, can only be a rough estimatelikely <strong>to</strong> be subject <strong>to</strong> question<strong>in</strong>g. The key aga<strong>in</strong> is <strong>to</strong> resist <strong>the</strong> temptation <strong>to</strong> errsystematically <strong>to</strong> <strong>the</strong> higher side and <strong>to</strong> share <strong>the</strong> methodology adopted as was done<strong>in</strong> this case. There is no real benefit for <strong>the</strong> affected population <strong>to</strong> adopt <strong>the</strong> higherend of all measurements. A middle road approach will more likely make divergencebetween experts a matter of scientific debate ra<strong>the</strong>r than a public crisis affect<strong>in</strong>g <strong>the</strong>credibility of an agency.Faced with <strong>the</strong> situation <strong>in</strong> Port-au-Pr<strong>in</strong>ce, <strong>the</strong> Government encouraged migration <strong>to</strong> nonaffecteddepartments, and buses were rapidly made ready <strong>to</strong> transport people. S<strong>in</strong>ce roads<strong>in</strong> <strong>the</strong> affected area were impassable, buses were located at <strong>the</strong> periphery. Movements ofpeople away from <strong>the</strong> capital started spontaneously, dur<strong>in</strong>g <strong>the</strong> night of 12 <strong>January</strong>; <strong>the</strong>first arrivals of <strong>the</strong> <strong>in</strong>jured were reported <strong>in</strong> <strong>the</strong> early morn<strong>in</strong>g of 13 <strong>January</strong> at Sa<strong>in</strong>t Marsand Gonaïves hospitals. The flow of “evacuated <strong>in</strong>jured people” cont<strong>in</strong>ued for a few days,rapidly overstretch<strong>in</strong>g <strong>the</strong> <strong>response</strong> capacities of <strong>the</strong>se facilities. <strong>Health</strong> services <strong>in</strong> <strong>the</strong> receiv<strong>in</strong>gareas, which were already <strong>in</strong>sufficient <strong>to</strong> meet <strong>the</strong> most basic needs of <strong>the</strong> localpopulation, had <strong>to</strong> attend <strong>to</strong> a flux of reportedly between 500,000 and 600,000 disasteraffected<strong>in</strong>dividuals, many with <strong>in</strong>juries and emergency treatment needs. These healthfacilities normally charged for services, habitually saw only a few patients daily, and had nos<strong>to</strong>cks of supplies <strong>to</strong> serve <strong>the</strong> <strong>in</strong>crease <strong>in</strong> patients. How long <strong>the</strong> extra medical burden onnon-affected departments lasted is unclear.If efforts were made by <strong>the</strong> Government <strong>to</strong> encourage and moni<strong>to</strong>r <strong>the</strong> <strong>in</strong>itial movemen<strong>to</strong>ut of Port-au-Pr<strong>in</strong>ce, few data were sought by or provided <strong>to</strong> <strong>the</strong> humanitariancommunity on <strong>the</strong> return of those displaced.The Rapid Initial Needs Assessment for <strong>Haiti</strong> (RINAH) is one of <strong>the</strong> few studies thatexplored this issue <strong>in</strong> some depth. 29 Ano<strong>the</strong>r survey commissioned by UNFPA confirmsthat more than a quarter of <strong>the</strong> population of <strong>the</strong> metropolitan area left after <strong>the</strong>12 <strong>January</strong> <strong>earthquake</strong> (<strong>Haiti</strong> Data Services <strong>2010</strong>). Half migrated <strong>in</strong><strong>to</strong> urban areas of29 See: Assessment Capacities (ACAPS), <strong>2010</strong>, Rapid <strong>in</strong>itial needs assessment for <strong>Haiti</strong> (RINAH).34
THE HEALTH IMPACT - Chapter 3unaffected departments (Figure 3.3). However, <strong>the</strong> study went fur<strong>the</strong>r and enquiredon <strong>the</strong> duration of this displacement: “The data show that those who left after 12<strong>January</strong> have returned soon after. Around one out of three (27.7%) have been awayless than one month and 55% between one and three months. In conclusion, less than20% stayed more than three months outside <strong>the</strong> metropolitan area.” 30The massive <strong>in</strong>ternational distribution of goods and services <strong>in</strong> <strong>the</strong> metropolitan area<strong>in</strong>fluenced or determ<strong>in</strong>ed this reflux. Material assistance <strong>in</strong>deed became much more accessible<strong>in</strong> Port-au-Pr<strong>in</strong>ce, <strong>in</strong>cit<strong>in</strong>g <strong>the</strong> return of displaced populations. As distributionswere organized <strong>in</strong> temporary settlements, some of <strong>the</strong> beneficiaries were not those affectedby <strong>the</strong> <strong>earthquake</strong> but actually <strong>the</strong> economically vulnerable seek<strong>in</strong>g better opportunities(shelter, food, water, health, and education opportunities). What is not knownis <strong>the</strong> importance of this fac<strong>to</strong>r.It is ra<strong>the</strong>r enlighten<strong>in</strong>g <strong>to</strong> note ano<strong>the</strong>r f<strong>in</strong>d<strong>in</strong>g of <strong>the</strong> UNFPA survey: The municipalityof Cité Soleil, <strong>the</strong> poorest area of <strong>the</strong> city but one of <strong>the</strong> less affected by <strong>the</strong> impact,received <strong>the</strong> smallest proportion of displaced from o<strong>the</strong>r municipalities (2.9%)but has <strong>the</strong> highest rate of displacement. More than 20% of <strong>the</strong> residents migrated<strong>in</strong><strong>to</strong> o<strong>the</strong>r (more affected) municipalities.Figure 3.3 Internal migration follow<strong>in</strong>g <strong>the</strong> <strong>Haiti</strong> <strong>earthquake</strong>,by departmentTotal 604,215100,00050,000NORTHWESTNORTHNORTHEASTARTIBONITE162,509CENTERGRANDE-ANSENIPPESSOUTHSOUTHEASTWESTSource: National System for Risk and Disaster Management (Système national de gestion des risques et des désastres—SNGRD) Report No 15, February <strong>2010</strong>.30 This is supported by <strong>the</strong> study conducted for USAID by Schwartz, Pierre, and Calpas (2011).35
Lorem Local health ipsum personnel, doler sit <strong>Haiti</strong>ans ameliv<strong>in</strong>g abroad (<strong>the</strong> ‘diaspora’)and neighbor<strong>in</strong>g countries played a significant role <strong>in</strong> <strong>the</strong><strong>response</strong>. Humanitarian ac<strong>to</strong>rs already work<strong>in</strong>g <strong>in</strong> <strong>Haiti</strong>, as wellRum et quate volorio volorestibus quidessimusas foreign aut untem medical et eaque teams, rectibea also became prae Git a et valuable asset dur<strong>in</strong>glandanti ulliquat et offictem. Et etus, untiur<strong>the</strong> atiusant relief vellect operation. orest, omniet volupta tquae.Nam, es nim sequi cuptaturi berati velibus asexerspera is necusci debisqu oditem eos<strong>to</strong>officiust vel ipsundaerum eatquunt ute iumeatat.
Chapter4providedWhoassistance?• While <strong>the</strong> impact of <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> was unprecedented, <strong>the</strong> short-term <strong>response</strong>had all <strong>the</strong> strengths and weaknesses noted <strong>in</strong> evaluations of earlier disasters.• Lessons from <strong>the</strong> past have not been learned.The logistical challenges faced by <strong>the</strong> responders were overwhelm<strong>in</strong>g:• International access: The airport facility, briefly closed, was reopened thanks <strong>to</strong>U.S. military <strong>in</strong>tervention. However, its use was <strong>in</strong>itially reserved for U.S. militarytroop movement and selected bilateral relief assistance or evacuations. The harborwas severely damaged.• Land transportation: The lack of vehicles, especially consider<strong>in</strong>g <strong>the</strong> unavailabilityof <strong>the</strong> MINUSTAH fleet for 7 days, 31 was compounded by chaotic traffic conditions.It often <strong>to</strong>ok several hours <strong>to</strong> move from one meet<strong>in</strong>g place <strong>to</strong> <strong>the</strong> nextwith<strong>in</strong> Port-au-Pr<strong>in</strong>ce.• Power: Modern relief is dependent on a reliable source of electricity, a conditionrarely met even months after <strong>the</strong> impact <strong>in</strong> <strong>Haiti</strong>.31 As noted <strong>in</strong> Chapter 1, <strong>the</strong> MINUSTAH mandate did not consider logistic support <strong>to</strong> <strong>the</strong> humanitarian agencies.37
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>• Communications: Fixed telephone l<strong>in</strong>es, that were unreliable <strong>in</strong> normal times, weresuspended; mobile phone l<strong>in</strong>es were unavailable most of <strong>the</strong> time, satellite telephonecircuits were overloaded, and <strong>in</strong>ternet access was limited.• Language: The language barrier was a significant obstacle for some foreign teamsthat found <strong>the</strong>mselves unable <strong>to</strong> communicate properly <strong>in</strong> French or Creole with<strong>the</strong>ir local partners and beneficiaries.• Adm<strong>in</strong>istrative obstacles: A cumbersome process for both cus<strong>to</strong>ms clearance <strong>in</strong> <strong>Haiti</strong>and approval of movement and arrangement for escort, when required by UNsecurity rules, caus<strong>in</strong>g difficulties and delays.Substantially <strong>in</strong>creas<strong>in</strong>g <strong>the</strong> number of personnel, <strong>to</strong> coord<strong>in</strong>ate and manage <strong>the</strong>health sec<strong>to</strong>r <strong>response</strong> without <strong>in</strong>creas<strong>in</strong>g logistical support, would not have resulted<strong>in</strong> a more effective <strong>response</strong>.The humanitarian ac<strong>to</strong>rs• If <strong>the</strong> impact of <strong>the</strong> <strong>earthquake</strong> was unprecedented, <strong>the</strong> <strong>response</strong> was not. It followed<strong>the</strong> trend observed <strong>in</strong> past disasters.• National professionals and neighbor<strong>in</strong>g countries played a significant role. The foreign<strong>response</strong> was extremely generous.The earliest and <strong>the</strong>refore most effective responders were those already <strong>in</strong> <strong>Haiti</strong> and especially<strong>in</strong> Port-au-Pr<strong>in</strong>ce: relatives and neighbors, local health services, and <strong>the</strong> manyhumanitarian agencies already on site. How many lives, for <strong>in</strong>stance, neighbors andrelatives have saved will never be known. The local contribution was <strong>in</strong>valuable bu<strong>to</strong>vershadowed by <strong>in</strong>ternational ac<strong>to</strong>rs better skilled <strong>in</strong> public relations.The <strong>Haiti</strong>an ac<strong>to</strong>rsAccord<strong>in</strong>g <strong>to</strong> most accounts, <strong>the</strong> solidarity among <strong>the</strong> <strong>Haiti</strong>ans was massive, with peoplehelp<strong>in</strong>g each o<strong>the</strong>r <strong>in</strong> <strong>the</strong> ru<strong>in</strong>s, shar<strong>in</strong>g <strong>the</strong> little <strong>the</strong>y had, and try<strong>in</strong>g <strong>to</strong> get as many peopleas <strong>the</strong>y could out of <strong>the</strong> debris. Despite a few unruly <strong>in</strong>cidents dur<strong>in</strong>g supply distribution,which were overblown by <strong>the</strong> media, <strong>the</strong> many s<strong>to</strong>ries of solidarity confirm once more thatrampant social disorder and violence after natural disasters is, <strong>in</strong>deed, just a myth.Local health personnelIn all disasters, local health services play a key role, especially <strong>the</strong> first few days beforeassistance can arrive. <strong>Haiti</strong> was no exception.A much debated issue is <strong>the</strong> conflict <strong>in</strong> roles for health workers between car<strong>in</strong>g for <strong>the</strong>irown families and <strong>the</strong>ir professional obligations. How did that play out <strong>in</strong> <strong>Haiti</strong>?38
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>support <strong>to</strong> serve <strong>the</strong> population for a given period of time, <strong>the</strong> practice does weakennational <strong>in</strong>stitutions and may hamper recovery. 36The key po<strong>in</strong>t is that reduced staff<strong>in</strong>g <strong>in</strong> public facilities does not necessarily mean that<strong>the</strong> miss<strong>in</strong>g doc<strong>to</strong>rs and health workers were not help<strong>in</strong>g <strong>the</strong>ir population.In <strong>the</strong> private, non-profit sec<strong>to</strong>r (NGO and faith-based organizations), absenteeismwas not an issue as illustrated by one agency comment: “Despite <strong>the</strong> tremendouspersonal losses susta<strong>in</strong>ed by many national staff members, and despite <strong>the</strong> chaos thatfollowed <strong>the</strong> <strong>earthquake</strong>, <strong>the</strong> majority of MSF’s surviv<strong>in</strong>g <strong>Haiti</strong>an staff immediatelyset <strong>to</strong> work help<strong>in</strong>g <strong>the</strong>ir countrymen and cont<strong>in</strong>ued <strong>to</strong> do so throughout this difficultperiod” (MSF 2011, 7).More surpris<strong>in</strong>gly <strong>in</strong> <strong>the</strong> harsh economic context of <strong>Haiti</strong>, <strong>the</strong> for-profit sec<strong>to</strong>r didnot lag far beh<strong>in</strong>d <strong>in</strong> generosity. Private, for-profit hospitals and cl<strong>in</strong>ics opened <strong>the</strong>irdoors, offered <strong>the</strong>ir services, and shared <strong>the</strong>ir supplies from <strong>the</strong> time of <strong>the</strong> impact.The staff of several cl<strong>in</strong>ics immediately provided care at no cost and acted as fieldhospitals. 37<strong>Haiti</strong>ans from abroadAssociations of expatriated health personnel can play a major role. However, <strong>the</strong>yshould plan ahead and take <strong>the</strong> lead <strong>in</strong> coord<strong>in</strong>at<strong>in</strong>g and facilitat<strong>in</strong>g <strong>the</strong> efforts of<strong>the</strong>ir members.The importance of <strong>the</strong> presence of <strong>Haiti</strong>an expatriates (<strong>the</strong> so-called “diaspora”) dur<strong>in</strong>g<strong>the</strong> post-disaster period has been well documented. Their knowledge of <strong>Haiti</strong>anculture, language, and cus<strong>to</strong>ms, coupled with <strong>the</strong>ir wide range of technical and professionalskills, gave <strong>the</strong>m a unique advantage over o<strong>the</strong>r groups dur<strong>in</strong>g <strong>the</strong> health<strong>response</strong>.Though <strong>the</strong> <strong>in</strong>ternational teams deployed <strong>to</strong> <strong>Haiti</strong> made numerous references <strong>to</strong> <strong>the</strong> workof national and expatriate <strong>Haiti</strong>ans, it is rare <strong>to</strong> f<strong>in</strong>d numbers or precise descriptions of<strong>the</strong>ir contribution. For example, <strong>the</strong> University of Miami Global Institute/Project Medishare(UMGI/PM), which has a 15-year relationship with <strong>Haiti</strong>an physicians, observedthat one of <strong>the</strong> key characteristics of this operation was <strong>the</strong> participation of <strong>Haiti</strong>an professionalsand technicians both liv<strong>in</strong>g <strong>in</strong> <strong>Haiti</strong> and abroad. However, <strong>the</strong>re are no specificfigures regard<strong>in</strong>g this phenomenon.Table 4.1 summarizes <strong>the</strong> few data available <strong>to</strong> <strong>the</strong> authors on <strong>the</strong> participation of nationalstaff and expatriate <strong>Haiti</strong>ans with selected groups <strong>in</strong>volved <strong>in</strong> <strong>the</strong> post-disasterhealth operation. 3836 The M<strong>in</strong>istry of <strong>Health</strong> developed guidel<strong>in</strong>es for <strong>the</strong> payment of <strong>Haiti</strong>an public staff by <strong>in</strong>ternational ac<strong>to</strong>rs. Agencies foundit difficult <strong>to</strong> change <strong>the</strong>ir salary scales, creat<strong>in</strong>g discrepancies with<strong>in</strong> <strong>the</strong>ir local staff (based on whe<strong>the</strong>r <strong>the</strong> date of a contractwas before or after <strong>the</strong> guidel<strong>in</strong>es were issued) and were reluctant <strong>to</strong> fur<strong>the</strong>r complicate <strong>the</strong>ir competitive search for scarcelocal skills. For <strong>the</strong> most part <strong>the</strong> guidel<strong>in</strong>es were ignored.37 The Alliance for International Medical Action (ALIMA), an <strong>in</strong>ternational NGO arriv<strong>in</strong>g a few days after <strong>the</strong> disaster, hadpre-<strong>earthquake</strong> contact with <strong>the</strong> private Cl<strong>in</strong>ique Lambert and decided <strong>to</strong> support it. The <strong>in</strong>ternational staff <strong>in</strong>volved <strong>in</strong>this operation was impressed by <strong>the</strong> sense of dedication of <strong>the</strong> cl<strong>in</strong>ic’s <strong>Haiti</strong>an staff, who worked 24 hours/day, 7days/week<strong>in</strong> very difficult conditions.38 Although <strong>the</strong> expertise and contribution of expatriate <strong>Haiti</strong>ans were appreciated by <strong>the</strong> employ<strong>in</strong>g agencies, compet<strong>in</strong>glocal <strong>in</strong>terests (family, social, or political) did occasionally complicate <strong>the</strong>ir <strong>in</strong>tegration <strong>in</strong> <strong>the</strong> team.40
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>be done overnight by technical or coord<strong>in</strong>at<strong>in</strong>g agencies that were deprived of officesand communication. 39The direct impact on agencies that normally lead <strong>the</strong> <strong>in</strong>ternational <strong>response</strong> was specific<strong>to</strong> <strong>the</strong> <strong>Haiti</strong>an disaster. In o<strong>the</strong>r countries affected by sudden disasters, <strong>the</strong> UN capacity<strong>to</strong> assist, respond, and coord<strong>in</strong>ate was not affected. However, plann<strong>in</strong>g for future scenariosof urban disaster should <strong>in</strong>clude this aspect.Bilateral agencies confronted <strong>the</strong> same challenges. They faced an additional and compet<strong>in</strong>gpriority from <strong>the</strong>ir obligation <strong>to</strong> care for <strong>the</strong>ir nationals (resident or visi<strong>to</strong>rs)who were miss<strong>in</strong>g or <strong>in</strong>jured. 40 This legitimate concern <strong>in</strong>fluenced greatly <strong>the</strong> prioritiesof <strong>the</strong>ir strategic and operational <strong>in</strong>volvement (transport, air traffic control, searchand rescue, medical care, etc.). Many dispatched SAR and medical teams, fundedo<strong>the</strong>r ac<strong>to</strong>rs, and provided supplies.External ac<strong>to</strong>rsThe Tsunami Evaluation Coalition (TEC) assessment of <strong>the</strong> <strong>in</strong>ternational <strong>response</strong>(Telford, Cosgrave, Hough<strong>to</strong>n 2006, 55) rema<strong>in</strong>s valid for <strong>Haiti</strong>:“The number of <strong>in</strong>ternational agencies <strong>in</strong>volved <strong>in</strong> <strong>the</strong> <strong>response</strong> grewunabated. Well-resourced agencies and very small ones, competent and<strong>in</strong>competent, well-prepared and unprepared, secular and faith-based,reputable and disreputable, household names and unknown, ambitiousand humble, opportunistic and committed, governmental and nongovernmental,national and <strong>in</strong>ternational, bilateral and multilateral, wellestablishedand just-formed—<strong>the</strong>y all turned up.”Foreign teams arriv<strong>in</strong>g <strong>in</strong> <strong>the</strong> country <strong>to</strong> provide health assistance <strong>in</strong> <strong>the</strong> aftermath of<strong>the</strong> <strong>earthquake</strong> belonged <strong>to</strong> one of <strong>the</strong> follow<strong>in</strong>g groups:• Medical components of urban search and rescue (USAR) teams. More than 30 countriessent USAR teams, many of <strong>the</strong>m with some health equipment (from verybasic stabilization boxes <strong>to</strong> full-fledged emergency field hospitals). This represented<strong>the</strong> first <strong>response</strong> of many bilateral government agencies (<strong>the</strong> traditional humanitariandonors but also Caribbean and Lat<strong>in</strong> American countries and many o<strong>the</strong>rsfrom around <strong>the</strong> world).• Bilateral government medical teams. These arrived from many countries, <strong>in</strong>clud<strong>in</strong>gfrom <strong>the</strong> Caribbean. Often more than one <strong>in</strong>stitution from a country was present.For example, United States assistance <strong>in</strong>cluded <strong>the</strong> Office for Foreign Disaster Assistance(State Department), <strong>the</strong> military (Department of Defense), and teams from<strong>the</strong> U.S. <strong>Health</strong> and Human Services Department, <strong>to</strong> name only a few;39 As mentioned earlier, land-l<strong>in</strong>e telephone service was suspended, mobile systems were mostly unavailable, satellite phoneswere rapidly overloaded (”no circuit”). Only hand-held radios provided some support <strong>in</strong> most locations. Internet and Skypeservices were <strong>in</strong>termittently available.40 By 19 February, an estimated 27,199 American citizens had returned <strong>to</strong> <strong>the</strong> U.S., most with <strong>the</strong> logistical assistance of <strong>the</strong> U.S.Government.42
WHO PROVIDED ASSISTANCE? - Chapter 4• UN or UN related agencies, <strong>in</strong>clud<strong>in</strong>g PAHO/WHO, UNICEF, UN PopulationFund (UNFPA), World Food Programme (WFP), and <strong>the</strong> International Organizationfor Migration (IOM);• Red Cross system (IFRC, ICRC and many participat<strong>in</strong>g national societies). The RedCross system mobilized its six health Emergency Response Units (ERU) whichconsist of “health services <strong>in</strong> a box” <strong>to</strong> be dispatched <strong>in</strong> less than 24 hours withspecialized and support (logistics) staff;• International NGOs (from <strong>the</strong> most established and experienced <strong>to</strong> <strong>the</strong> small or lessknown);• Bilateral, non-State <strong>in</strong>stitutions (hospitals or universities, for example), many withongo<strong>in</strong>g activities and established <strong>Haiti</strong>an counterparts;• Teams from social or religious associations. This category <strong>in</strong>cluded many small ac<strong>to</strong>rsbut with <strong>the</strong> advantage of hav<strong>in</strong>g exist<strong>in</strong>g, one-<strong>to</strong>-one relationships at <strong>the</strong> locallevel;• Ad hoc <strong>in</strong>itiatives by <strong>in</strong>dividuals or groups set up only for <strong>the</strong> event (<strong>the</strong> “mushroom”NGOs that pop up overnight after each major crisis).Over <strong>the</strong> last decade, <strong>the</strong> number of those ac<strong>to</strong>rs has grown rapidly and without a strategyor master plan, lead<strong>in</strong>g <strong>the</strong> World Disaster Report of <strong>the</strong> IFRC (2004) <strong>to</strong> call <strong>the</strong>humanitarian community <strong>the</strong> “largest unregulated <strong>in</strong>dustry.” Mass media play an importantrole <strong>in</strong> this wild expansion. If <strong>the</strong> far-reach<strong>in</strong>g mass media contribute <strong>to</strong> generat<strong>in</strong>gglobal generosity and compassion on behalf of <strong>the</strong> affected population, <strong>the</strong>y also representan almost irresistible <strong>in</strong>centive for politicization of <strong>the</strong> process or its exploitationfor <strong>the</strong> sake of publicity (or even proselytism by some faith groups, as occurred <strong>in</strong> <strong>Haiti</strong>).Effectiveness is a matter of contextThe results of <strong>the</strong> proliferation of health responders were atypical <strong>in</strong> <strong>Haiti</strong> compared<strong>to</strong> o<strong>the</strong>r past (and probably most future) disasters:• In <strong>Haiti</strong>, <strong>the</strong> magnitude of <strong>the</strong> needs, <strong>the</strong> poor state of services prior <strong>to</strong> <strong>the</strong> impact,and <strong>the</strong> absence of national back-up capacity after <strong>the</strong> event resulted <strong>in</strong> many ofthose ac<strong>to</strong>rs provid<strong>in</strong>g significant assistance <strong>to</strong> <strong>the</strong> population.• In o<strong>the</strong>r disasters (Indian Ocean tsunami, <strong>earthquake</strong>s <strong>in</strong> Iran or Pakistan), most ofthose teams were more a burden than assistance.This proliferation of <strong>in</strong>ternational organizations is far from new (as already noted <strong>in</strong><strong>the</strong> tsunami evaluation), suggest<strong>in</strong>g that not much has been learned.The number of small, short-duration medical missions <strong>in</strong> <strong>Haiti</strong> is unknown but likely<strong>to</strong> be high due <strong>to</strong> <strong>the</strong> visibility of <strong>the</strong> <strong>earthquake</strong> and proximity <strong>to</strong> North America. Inan assessment of volunteerism <strong>in</strong> <strong>Haiti</strong>, Kathleen Jobe (2011) spelled out <strong>the</strong> conditionsfor those teams <strong>to</strong> be effective: “Short-term medical missions should be familiar with <strong>the</strong>broader public health messages that are determ<strong>in</strong>ed by <strong>in</strong>-country public health officialsand established <strong>in</strong>-country NGOs”. In <strong>the</strong> same ve<strong>in</strong>, C. Bajkiewicz (2009) observes:43
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>“Volunteers are well served by evaluat<strong>in</strong>g not only <strong>the</strong> personal benefit <strong>the</strong>y derive fromparticipat<strong>in</strong>g <strong>in</strong> <strong>the</strong> mission, but also <strong>the</strong> overall impact of <strong>the</strong> mission on local healthcare and public health priorities.”The close neighborsThe traditional bilateral humanitarian ac<strong>to</strong>rs played a major role <strong>in</strong> <strong>the</strong> health <strong>response</strong>.Among <strong>the</strong>m was <strong>the</strong> United States Department of <strong>Health</strong> and Human Services(HHS), an agency provid<strong>in</strong>g a large array of services, <strong>in</strong>clud<strong>in</strong>g <strong>the</strong> National DisasterMedical System (NDMS) and <strong>the</strong> Centers for Disease Control and Prevention(CDC), both of which were activated <strong>in</strong> <strong>Haiti</strong>. As noted <strong>in</strong> <strong>the</strong> box, <strong>the</strong> variety andextent of services was unusual compared <strong>to</strong> past disasters <strong>in</strong> <strong>the</strong> world.Examples of support from <strong>the</strong> U.S. Department of <strong>Health</strong> and Human ServicesMedical care: Deployed <strong>the</strong> medical assets of <strong>the</strong> NDMS, consist<strong>in</strong>g of almost 1,000 health respondersover <strong>the</strong> 42-day mission;Evacuation: Assisted return<strong>in</strong>g U.S. citizens and arranged for referral of <strong>in</strong>jured <strong>Haiti</strong>ans <strong>to</strong> tertiarycare <strong>in</strong>stitutions <strong>in</strong> <strong>the</strong> United States;Disease surveillance: Provided assistance for epidemiological surveillance and labora<strong>to</strong>ry support;Dead bodies: S<strong>to</strong>rage, identification, and repatriation of bodies of U.S. citizens.Many Lat<strong>in</strong> American or Caribbean countries provided substantial assistance. Of <strong>the</strong>latter, two countries were particularly well placed <strong>to</strong> play an important health role dur<strong>in</strong>g<strong>the</strong> first days: Cuba and <strong>the</strong> Dom<strong>in</strong>ican Republic, due <strong>to</strong> <strong>the</strong>ir medical presenceor geographic proximity.CubaCuba has ma<strong>in</strong>ta<strong>in</strong>ed a strong medical presence <strong>in</strong> <strong>Haiti</strong> s<strong>in</strong>ce 1998. Over this period,more than 6,000 health personnel have served <strong>in</strong> <strong>the</strong> country, often <strong>in</strong> difficult ruralenvironments. At <strong>the</strong> time of <strong>the</strong> impact, <strong>the</strong> Cuban Medical Brigades had morethan 330 primary health care professionals <strong>in</strong> <strong>the</strong> country. Those experts provided animmediate source of medical personnel familiar with <strong>the</strong> conditions of <strong>the</strong> country.They reported see<strong>in</strong>g <strong>the</strong>ir first patients less than 90 m<strong>in</strong>utes after <strong>the</strong> impact andcompleted 1,000 emergency consultations with<strong>in</strong> <strong>the</strong> first 24 hours. At <strong>the</strong> end, morethan 1,500 personnel contributed <strong>to</strong> <strong>the</strong> <strong>response</strong>. A summary of <strong>the</strong> reported activities<strong>in</strong> <strong>the</strong> first 10 days is presented <strong>in</strong> Table 4.2.Table 4.2 Cuban medical assistance <strong>in</strong> <strong>Haiti</strong>, 12–22 <strong>January</strong> <strong>2010</strong>Affected area NumberSurgeryDeathsof casesM<strong>in</strong>or Major Total Children Adults TotalPort-au-Pr<strong>in</strong>ce 11,354 113 622 735 19 49 68Suburban areas 3,553 63 80 143 37 28 65O<strong>the</strong>rs 5,188 896 180 1,076 1 14 15Total 20,095 1,072 882 1,954 57 91 148Source: Report provided <strong>to</strong> PAHO/WHO by <strong>the</strong> Cuban Medical Brigade, 22 February 2011.44
WHO PROVIDED ASSISTANCE? - Chapter 4Dom<strong>in</strong>ican RepublicThe Dom<strong>in</strong>ican Republic, a country with occasionally tense relations with its poorerneighbor, has played several roles:• First, <strong>the</strong> Dom<strong>in</strong>ican Republic received tens of thousands of refugees, many seek<strong>in</strong>gurgent surgical care. The country provided health assistance at all major bordercross<strong>in</strong>g po<strong>in</strong>ts (especially Jimaní).• It rapidly deployed a civil protection team <strong>to</strong> Port-au-Pr<strong>in</strong>ce <strong>in</strong> order <strong>to</strong> provideassistance and expertise at <strong>the</strong> site of <strong>the</strong> disaster.• For <strong>the</strong> first few weeks, <strong>the</strong> Dom<strong>in</strong>ican Republic was a vital lifel<strong>in</strong>e for <strong>the</strong> relief operations<strong>in</strong> <strong>Haiti</strong>. San<strong>to</strong> Dom<strong>in</strong>go became a major hub for most of <strong>the</strong> foreign assistanceas <strong>the</strong> access <strong>to</strong> Port-au-Pr<strong>in</strong>ce airport was constra<strong>in</strong>ed by <strong>the</strong> deployment of<strong>the</strong> U.S. military, Civil Protection, and consular operations (evacuations). There werefew exceptions and those that were allowed <strong>to</strong> land <strong>in</strong> Port-au-Pr<strong>in</strong>ce had <strong>to</strong> undergoa complex clearance process. In addition, <strong>the</strong> Port-au-Pr<strong>in</strong>ce sea port rema<strong>in</strong>ed <strong>in</strong>accessibledue <strong>to</strong> severe damage and after repairs were made it was congested. Land<strong>in</strong>g<strong>in</strong> San<strong>to</strong> Dom<strong>in</strong>go and mov<strong>in</strong>g overland <strong>to</strong> <strong>Haiti</strong> border cross<strong>in</strong>gs became <strong>the</strong> normalprocedure. The Dom<strong>in</strong>ican Republic facilitated or waived cus<strong>to</strong>ms and immigrationprocedures at both <strong>the</strong> San<strong>to</strong> Dom<strong>in</strong>go airport and at <strong>the</strong> Jimaní border cross<strong>in</strong>g.45
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>The number of people seek<strong>in</strong>g shelter and medical care <strong>in</strong> <strong>the</strong> Dom<strong>in</strong>ican Republicwas overwhelm<strong>in</strong>g and required <strong>the</strong> support of <strong>the</strong> entire Dom<strong>in</strong>ican health system.It is a few hours’ drive <strong>in</strong> normal circumstances from <strong>the</strong> <strong>Haiti</strong>an capital (62 km) <strong>to</strong>Jimaní, a primary border <strong>to</strong>wn on <strong>the</strong> Dom<strong>in</strong>ican side (see map). For <strong>the</strong> Dom<strong>in</strong>icanRepublic, it was not a m<strong>in</strong>or, localized emergency but a major mass casualty event thatexceeded its normal <strong>response</strong> capacity. It was a local disaster that <strong>to</strong>ok place <strong>in</strong> parallel<strong>to</strong> <strong>the</strong> larger one <strong>in</strong> Port-au-Pr<strong>in</strong>ce. There could be no guidance or support from <strong>the</strong>authorities of <strong>the</strong> affected country. The Dom<strong>in</strong>ican Republic did handle it on its own.As we will see, <strong>the</strong> disaster <strong>in</strong> <strong>Haiti</strong> followed a now well-known pattern of shift<strong>in</strong>gpriorities from life-sav<strong>in</strong>g trauma care <strong>to</strong> post-operative concerns and welfare. The<strong>response</strong> <strong>to</strong> <strong>the</strong> “border disaster” followed a similar pattern but was greatly accelerated.The tim<strong>in</strong>g was closer <strong>to</strong> that observed <strong>in</strong> o<strong>the</strong>r disasters when a whole country standsbeh<strong>in</strong>d <strong>the</strong> assistance <strong>to</strong> a small part of its population. For <strong>in</strong>stance, epidemiologicalsurveillance and o<strong>the</strong>r communicable disease measures were already adopted at <strong>the</strong>Dom<strong>in</strong>ican Republic’s central level on Day 3, an early warn<strong>in</strong>g system was activatedon Day 4, and field visits of epidemiologists were made <strong>to</strong> temporary settlements onDay 5 (PAHO/WHO <strong>2010</strong>b). In <strong>Haiti</strong>, two weeks passed before <strong>the</strong> first systems forsurveillance and control of communicable disease could actually be set up.Clearly, <strong>the</strong> scale of needs was far greater <strong>in</strong> Port-au-Pr<strong>in</strong>ce than <strong>in</strong> Jimaní. Never<strong>the</strong>less,<strong>the</strong> magnitude of <strong>the</strong> task faced by <strong>the</strong> Dom<strong>in</strong>ican health services and CivilDefense cannot be underestimated. From 18 <strong>to</strong> 23 <strong>January</strong>, reports <strong>in</strong>dicate a severeoverload of <strong>the</strong> health services <strong>in</strong> all border prov<strong>in</strong>ces <strong>in</strong> <strong>the</strong> Dom<strong>in</strong>ican Republic. For10 days, key staff rema<strong>in</strong>ed on duty without relief and on Day 15, <strong>the</strong> hospitals <strong>in</strong> <strong>the</strong>border departments still had more <strong>Haiti</strong>an patients than local ones.The exodus of affected families and people <strong>to</strong>ward <strong>the</strong> Dom<strong>in</strong>ican Republic slowed after 10days, and <strong>the</strong> number of new patients started <strong>to</strong> decl<strong>in</strong>e. Dur<strong>in</strong>g <strong>January</strong>, <strong>the</strong> Dom<strong>in</strong>icanhealth services attended <strong>to</strong> 1,985 patients, performed a high number of amputations (212),immobilized 121 fractures, and registered 15 deaths <strong>in</strong> hospitals (PAHO/WHO <strong>2010</strong>b).The credit for <strong>the</strong> achievements <strong>in</strong> Jimaní should be shared with <strong>the</strong> countries andNGOs back<strong>in</strong>g up <strong>the</strong> Dom<strong>in</strong>ican Republic with teams at <strong>the</strong> border. Little outsidesupport was received from <strong>the</strong> donors.O<strong>the</strong>r countries from <strong>the</strong> region• Many Lat<strong>in</strong> American or Caribbean countries did not report <strong>the</strong>ir assistance <strong>to</strong> <strong>the</strong>OCHA F<strong>in</strong>ancial Track<strong>in</strong>g System. They lost an opportunity for a permanent record of<strong>the</strong> nature and value of <strong>the</strong>ir <strong>in</strong>-k<strong>in</strong>d contributions.• Some of <strong>the</strong> countries new <strong>to</strong> <strong>in</strong>ternational medical relief would benefit from organiz<strong>in</strong>g<strong>the</strong>ir own “lessons learned” exercise and <strong>in</strong>creas<strong>in</strong>g <strong>the</strong>ir preparedness and tra<strong>in</strong><strong>in</strong>g.In addition <strong>to</strong> <strong>the</strong> special roles played by Cuba and <strong>the</strong> Dom<strong>in</strong>ican Republic, <strong>the</strong>rewas probably not one country <strong>in</strong> Lat<strong>in</strong> America and <strong>the</strong> Caribbean that did not contribute<strong>in</strong> one way or ano<strong>the</strong>r <strong>to</strong> sav<strong>in</strong>g lives and provid<strong>in</strong>g care <strong>to</strong> <strong>the</strong> affected population<strong>in</strong> <strong>Haiti</strong>. The contributions <strong>to</strong>ok diverse forms: from <strong>the</strong> deployment of searchand rescue teams, <strong>the</strong> deployment of field or ship hospitals, <strong>the</strong> dispatch of medical46
WHO PROVIDED ASSISTANCE? - Chapter 4teams, or <strong>the</strong> secondment of <strong>in</strong>dividual volunteers for <strong>the</strong> management of <strong>in</strong>com<strong>in</strong>gsupplies or experts <strong>to</strong> assist one of <strong>the</strong> humanitarian organizations. The <strong>response</strong> <strong>to</strong> <strong>the</strong><strong>Haiti</strong> <strong>earthquake</strong> was global, but it was also truly regional.Information on <strong>the</strong> regional medical <strong>response</strong> comes primarily from <strong>in</strong>terviews and<strong>to</strong> a lesser extent from media reports. There is a serious lack of adm<strong>in</strong>istrative <strong>in</strong>formation(report<strong>in</strong>g of <strong>in</strong>-k<strong>in</strong>d donations <strong>to</strong> <strong>the</strong> UN/OCHA on-l<strong>in</strong>e f<strong>in</strong>ancial track<strong>in</strong>gsystem, technical documentation, or scientific analysis) on <strong>the</strong>se activities. Of <strong>the</strong> 280peer-reviewed articles listed <strong>in</strong> Medl<strong>in</strong>e, 41 none addressed lessons learned or activitiesof Lat<strong>in</strong> American or Caribbean medical teams. 42 This needs <strong>to</strong> be addressed bothfrom an educational and public relations po<strong>in</strong>t of view.Regional organizationsThe supportive role at <strong>the</strong> operational level of <strong>the</strong> regional organizations <strong>to</strong> which<strong>Haiti</strong> belongs should be noted. With<strong>in</strong> 24 hours, <strong>the</strong> Caribbean Disaster EmergencyManagement Agency (CDEMA) supported <strong>the</strong> Government of Jamaica <strong>to</strong> mobilizeits medical personnel. Jamaica became a stag<strong>in</strong>g area for fur<strong>the</strong>r Caribbean assistance.As early as 14 <strong>January</strong> (Day 3), <strong>the</strong> Caribbean Community (CARICOM) identified<strong>the</strong> health sec<strong>to</strong>r as <strong>the</strong> agreed area of focus for <strong>the</strong> coord<strong>in</strong>ated regional <strong>in</strong>tervention.The modest Caribbean resources were complemented by Australia, which channeledAUS$ 1 million <strong>to</strong> CDEMA (i.e., 10% of <strong>the</strong> <strong>in</strong>itial pledge from this country).How much more effective would <strong>the</strong> <strong>response</strong> of <strong>the</strong> Dom<strong>in</strong>ican Republic and o<strong>the</strong>rCaribbean countries have been had o<strong>the</strong>r donors followed this example?41 A literature review was conducted of articles <strong>in</strong> <strong>the</strong> U.S. National Library of Medic<strong>in</strong>e’s MEDLINE database on 7 August2011.42 An edi<strong>to</strong>rial on lessons learned <strong>in</strong> <strong>Haiti</strong> was published <strong>in</strong> <strong>the</strong> West Indian Medical Journal (Vaughan <strong>2010</strong>).El Buen Samaritano HospitalFlags from <strong>the</strong> countries provid<strong>in</strong>g medicalteams at <strong>the</strong> <strong>Haiti</strong>-Dom<strong>in</strong>ican border.Pho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>47
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Institutional bilateral assistance• Prior experience <strong>in</strong> <strong>the</strong> affected country or close partnership with an established, onsiteNGO is essential.• A significant commitment should be susta<strong>in</strong>ed both on <strong>the</strong> humanitarian but above allon <strong>the</strong> adm<strong>in</strong>istrative, f<strong>in</strong>ancial, and logistical sides.• A mid-term view is critical. Improvised, overnight operations are not likely <strong>to</strong> be productive,regardless of <strong>the</strong> scientific credentials of <strong>the</strong> <strong>in</strong>stitution. Be<strong>in</strong>g a world-classacademic or cl<strong>in</strong>ical center is not sufficient <strong>to</strong> become a major humanitarian ac<strong>to</strong>r.The magnitude of <strong>the</strong> disaster and <strong>the</strong> proximity of <strong>Haiti</strong> <strong>to</strong> North America, amongo<strong>the</strong>r fac<strong>to</strong>rs, <strong>in</strong>duced a very strong <strong>response</strong> by private (nongovernmental) health<strong>in</strong>stitutions, particularly from <strong>the</strong> U.S. Some but not all of <strong>the</strong>se <strong>in</strong>stitutions hadongo<strong>in</strong>g health projects <strong>in</strong> <strong>the</strong> country. A similar <strong>response</strong> was not observed after <strong>the</strong>Indian Ocean tsunami or <strong>the</strong> Pakistan (Kashmir) <strong>earthquake</strong>.Three of <strong>the</strong> largest and best documented <strong>response</strong>s from academic <strong>in</strong>stitutions <strong>in</strong> <strong>the</strong>United States were organized by medical centers <strong>in</strong> Chicago, hospitals affiliated with HarvardUniversity, and <strong>the</strong> University of Miami Project Medishare (see box).These <strong>in</strong>itiativesshared many features that were critical for <strong>the</strong>ir success:Medical care at <strong>the</strong> <strong>Haiti</strong>/Dom<strong>in</strong>ican border48Pho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>
WHO PROVIDED ASSISTANCE? - Chapter 4• The participation of various global health <strong>in</strong>itiatives or <strong>in</strong>ternational emergencymedic<strong>in</strong>e programs at <strong>the</strong>se <strong>in</strong>stitutions;• Preexist<strong>in</strong>g partnership with large NGOs through which <strong>the</strong> medical staff was deployed<strong>in</strong> <strong>Haiti</strong> (Chicago) or pre-exist<strong>in</strong>g stand<strong>in</strong>g projects <strong>in</strong> <strong>the</strong> country;• A mid-term view (several months);• Strong adm<strong>in</strong>istrative, logistics, and communication support; 43• A systematic debrief<strong>in</strong>g (lessons learned) process for all volunteers;• The participation of a large number of <strong>Haiti</strong>ans (local or expatriate);• Geographical proximity of <strong>Haiti</strong> (an important albeit not critical fac<strong>to</strong>r).Examples of <strong>response</strong> from teach<strong>in</strong>g <strong>in</strong>stitutionsChicago Medical ResponseThis <strong>in</strong>itiative was formed by six academic medical centers from <strong>the</strong> city of Chicago. As of 1April it had deployed 158 medical volunteers <strong>to</strong> work with established NGOs <strong>in</strong> <strong>Haiti</strong>. The m<strong>in</strong>imumduration of deployment required was two weeks. The <strong>in</strong>itiative supported <strong>the</strong> UniversityHospital (HUEH), staffed several mobile cl<strong>in</strong>ics, and collaborated with <strong>the</strong> post-operative station<strong>in</strong> Fond Parisien near <strong>the</strong> Dom<strong>in</strong>ican border.Harvard Humanitarian ProgramPartners <strong>in</strong> <strong>Health</strong> (PIH), a not-for-profit Harvard affiliate with an established presence <strong>in</strong> <strong>Haiti</strong><strong>to</strong>ok <strong>the</strong> lead <strong>in</strong> university-related medical assistance. The group operated n<strong>in</strong>e medical sites <strong>in</strong><strong>Haiti</strong>. By 19 June, 50 medical and surgical personnel had been deployed <strong>in</strong> <strong>Haiti</strong> from Harvardaffiliatedhospitals. Harvard teach<strong>in</strong>g hospitals sent planeloads of medical supplies, <strong>in</strong>clud<strong>in</strong>gsurgical and anes<strong>the</strong>sia equipment.The University of Miami Global Institute/Project Medishare (UMGI/PM)Dur<strong>in</strong>g <strong>the</strong> first n<strong>in</strong>e days after <strong>the</strong> <strong>earthquake</strong> <strong>the</strong> Project Medishare hospital functioned <strong>in</strong>side<strong>the</strong> United Nations compound with 250 beds, 12 staff, and no critical-care units or organizedoperat<strong>in</strong>g rooms. Sanitation and o<strong>the</strong>r work<strong>in</strong>g conditions <strong>in</strong> <strong>the</strong> first few days were dire.The hospital was later set up at <strong>the</strong> Port-au-Pr<strong>in</strong>ce airport <strong>in</strong> a four-tent facility, with three fullyorganized operat<strong>in</strong>g rooms and 17 critical-care beds. It was staffed by 220 volunteers from <strong>the</strong>United States and Canada who served <strong>in</strong> 7-day rotations. There was strong adm<strong>in</strong>istrative andlogistics support <strong>in</strong> <strong>Haiti</strong> as well as <strong>in</strong> Miami. The group coord<strong>in</strong>ated flights <strong>to</strong> transport medicalstaff, supplies, equipment, and victims between <strong>Haiti</strong> and <strong>the</strong> United States. This support<strong>in</strong>cluded tele-medic<strong>in</strong>e consultations and communications (see G<strong>in</strong>zburg et al. <strong>2010</strong>).A proliferation of <strong>in</strong>ternational organizationsIn Banda Aceh, Indonesia, approximately 180 agencies (represent<strong>in</strong>g all sec<strong>to</strong>rs) registeredwith <strong>the</strong> UN follow<strong>in</strong>g <strong>the</strong> tsunami. In addition, <strong>the</strong> TEC estimated that “<strong>the</strong>remay have been as many as 200 small <strong>in</strong>ternational agencies that stayed only a fewweeks” (Telford, Cosgrave, Hough<strong>to</strong>n 2006, 55).43 It is estimated that Chicago <strong>in</strong>stitutions dedicated 1500 hours of faculty and adm<strong>in</strong>istrative time <strong>to</strong> <strong>the</strong>ir operations <strong>in</strong><strong>Haiti</strong>.49
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>In Port-au-Pr<strong>in</strong>ce, <strong>the</strong> proliferation of <strong>in</strong>ternational organizations was far greater than<strong>in</strong> Banda Aceh. In <strong>the</strong> health sec<strong>to</strong>r alone, 390 agencies, mostly <strong>in</strong>ternational, registeredwith <strong>the</strong> external coord<strong>in</strong>at<strong>in</strong>g mechanism (<strong>Health</strong> Cluster) (see Figure 4.2).Many more health ac<strong>to</strong>rs did not register.Figure 4.2 Number of <strong>in</strong>ternational agencies registered with <strong>the</strong><strong>Health</strong> Cluster follow<strong>in</strong>g <strong>the</strong> <strong>Haiti</strong> <strong>earthquake</strong>450Number of registered agencies4003503002502001501005000 4 7 12 15 35 79Days after impactNote: Figures were compiled from situation reports and <strong>Health</strong> Cluster Bullet<strong>in</strong>s.Missionaries of Charity50Pho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>
WHO PROVIDED ASSISTANCE? - Chapter 4The <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>Haiti</strong> <strong>earthquake</strong> was not an anomaly, an “unprecedented” glitch<strong>in</strong> an o<strong>the</strong>rwise rational <strong>response</strong>. It was, ra<strong>the</strong>r, a confirmation and acceleration of aglobal humanitarian trend observed <strong>in</strong> recent sudden-onset disasters (<strong>the</strong> <strong>earthquake</strong> <strong>in</strong>Pakistan and <strong>the</strong> Indian Ocean tsunami). In <strong>the</strong> last decade, <strong>the</strong> only countries sparedthis chaotic situation were those with sufficient resources <strong>to</strong> meet most urgent needsor those able <strong>to</strong> moni<strong>to</strong>r and regulate <strong>the</strong> flow of outside assistance and ensure that itcomplemented local efforts.The follow<strong>in</strong>g chart differentiates <strong>the</strong>se f<strong>in</strong>d<strong>in</strong>gs accord<strong>in</strong>g <strong>to</strong> <strong>the</strong>ir specificity <strong>to</strong> <strong>Haiti</strong>.Lessons new or specific <strong>to</strong> <strong>Haiti</strong>• A demand for medical care far exceed<strong>in</strong>g <strong>the</strong> offer <strong>in</strong> <strong>the</strong> first few weeks.• Rapid <strong>response</strong> of medical <strong>in</strong>ternational NGOs and o<strong>the</strong>r humanitarian ac<strong>to</strong>rs present prior<strong>to</strong> impact.• Rapid arrival due <strong>to</strong> proximity (18 hours <strong>in</strong>stead of 3 days).• Large medical diaspora abroad respond as <strong>in</strong>dividuals.• Lack of national military assets but massive U.S. military and UN peacekeep<strong>in</strong>g <strong>in</strong>terventionor presence.• Strong and susta<strong>in</strong>ed health <strong>in</strong>itiatives from major U.S. university hospitals.Lessons noted <strong>in</strong> past disasters• Very generous <strong>response</strong> lead<strong>in</strong>g <strong>to</strong> exponential <strong>in</strong>crease <strong>in</strong> <strong>the</strong> number of health “partners”.• Significant number of unqualified or unprepared ac<strong>to</strong>rs.• External coord<strong>in</strong>ation mechanisms (Clusters) do not reflect local mandate of l<strong>in</strong>e m<strong>in</strong>istries.• Failure <strong>to</strong> <strong>in</strong>volve and streng<strong>the</strong>n local government for timely transfer of responsibilities/authority.• Too much emphasis on coord<strong>in</strong>ation (meet<strong>in</strong>gs) ra<strong>the</strong>r than on <strong>in</strong>telligence ga<strong>the</strong>r<strong>in</strong>g andstrategic guidance.• Increas<strong>in</strong>g priority on “build back better” (l<strong>in</strong>kage between relief, rehabilitation, anddevelopment).51
Lorem ipsum doler sit ameRum et quate volorio volorestibus quidessimusaut untem et eaque rectibea prae Git etlandanti ulliquat et offictem. Et etus, untiuratiusant vellect orest, omniet volupta tquae.Nam, es nim sequi cuptaturi berati velibus asexerspera is necusci debisqu oditem eos<strong>to</strong>officiust vel ipsundaerum eatquunt ute iumeatat.In <strong>the</strong> Buen Samaritano hospital on <strong>the</strong> Dom<strong>in</strong>icanRepublic border, relief priorities shifted day by day,Pho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>although <strong>the</strong> disproportion between needs andresources was not as extreme as <strong>in</strong> Port-au-Pr<strong>in</strong>ce.
Chapter5life-sav<strong>in</strong>gThe<strong>response</strong>The <strong>response</strong> phasesThe traditional disaster management cycle, from preparedness <strong>to</strong> reconstruction, asshown <strong>in</strong> Figure 5.1, has become <strong>to</strong>o simplistic <strong>to</strong> describe modern humanitarian<strong>response</strong>. The respective boundaries between relief, early recovery, and reconstructionare becom<strong>in</strong>g <strong>in</strong>creas<strong>in</strong>gly blurred. The emergency relief phase tends <strong>to</strong> l<strong>in</strong>ger as longas humanitarian fund<strong>in</strong>g is available. This is especially true <strong>in</strong> situations like <strong>Haiti</strong>,where crises succeed each o<strong>the</strong>r (when not overlapp<strong>in</strong>g), and where long-term developmentseems so elusive.53
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Figure 5.1 The disaster management cycleDisaster relief changes considerably over time. Relief priorities shift day by day: fromsearch and rescue and life-sav<strong>in</strong>g medical <strong>in</strong>terventions <strong>to</strong> water, food, temporary shelters,resumption of rout<strong>in</strong>e programs, and meet<strong>in</strong>g needs of specific groups. Prioritiesand <strong>the</strong>ir tim<strong>in</strong>g vary from event <strong>to</strong> event.In smaller and less overwhelm<strong>in</strong>g disasters <strong>the</strong>se changes are accelerated, as was seen <strong>in</strong>Jimaní, <strong>the</strong> border city <strong>in</strong> <strong>the</strong> Dom<strong>in</strong>ican Republic. The imbalance between needs andresources was not as extreme <strong>in</strong> Jimaní as <strong>in</strong> Port-au-Pr<strong>in</strong>ce: more orderly plann<strong>in</strong>g waspossible, changes could be anticipated, and a calendar was rapidly agreed upon among <strong>the</strong>ma<strong>in</strong> ac<strong>to</strong>rs. In <strong>Haiti</strong>, <strong>the</strong> magnitude of <strong>the</strong> impact and of <strong>the</strong> needs ensured that, withfew exceptions, sav<strong>in</strong>g lives, provision of food, water, and shelter, and o<strong>the</strong>r priorities overlappedand competed for time and attention for a much longer period than usual.We can identify two periods <strong>in</strong> <strong>the</strong> relief phase after <strong>the</strong> <strong>earthquake</strong>:• An “immediate” life-sav<strong>in</strong>g phase, which, <strong>in</strong> <strong>Haiti</strong>, lasted approximately two weeks(16 days). The crucial activities were search and rescue (10 days) and emergencytrauma care. O<strong>the</strong>r concerns, although present, were secondary.• A second phase—of still undef<strong>in</strong>ed duration—began when <strong>the</strong> focus shifted predom<strong>in</strong>antly<strong>to</strong> pos<strong>to</strong>perative care, rehabilitation, primary health care for displacedpopulations, resumption of key programs, and <strong>the</strong> welfare priorities of food, water,and shelter (<strong>in</strong>clud<strong>in</strong>g camp management), among o<strong>the</strong>rs. Cross-cutt<strong>in</strong>g priorities54
THE LIFE-SAVING RESPONSE - Chapter 5such as gender issues and protection of human rights were raised <strong>in</strong> <strong>the</strong> first daysafter <strong>the</strong> <strong>earthquake</strong> by <strong>the</strong> relevant agencies or NGOs and progressively received <strong>the</strong>attention <strong>the</strong>y deserved.The turn<strong>in</strong>g po<strong>in</strong>t between <strong>the</strong> two phases seems <strong>to</strong> be on 28 <strong>January</strong> (Day 17) 44when, accord<strong>in</strong>g <strong>to</strong> <strong>the</strong> <strong>Haiti</strong> <strong>Health</strong> Cluster Bullet<strong>in</strong> (No. 9):• “Reports <strong>in</strong>dicate almost all people with <strong>in</strong>juries have received medical attention;however, some still require surgical care. 45• “The current priorities of <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong> <strong>in</strong>clude post-operative careand rehabilitation of disabled people, primary care at <strong>in</strong>ternally displaced personssites, and provision of medical services outside of Port-au-Pr<strong>in</strong>ce.”There was <strong>in</strong>creas<strong>in</strong>g overlap between activities and priorities. Most of <strong>the</strong> welfareneeds listed under <strong>the</strong> second phase were urgent and required attention <strong>in</strong> <strong>the</strong> first fewdays after <strong>the</strong> event. Even <strong>in</strong> <strong>the</strong> immediate phase, all agencies carried out <strong>the</strong>ir activities(whe<strong>the</strong>r <strong>the</strong>y were critical or even relevant at that time), compet<strong>in</strong>g for resourcesand facilities. The lack of a coord<strong>in</strong>at<strong>in</strong>g body that was able and empowered <strong>to</strong> set andenforce clear priorities allowed every ac<strong>to</strong>r <strong>to</strong> determ<strong>in</strong>e its own agenda.The “immediate” life-sav<strong>in</strong>g <strong>response</strong>As is always true, <strong>the</strong> first <strong>response</strong> <strong>in</strong> <strong>Haiti</strong> was from <strong>the</strong> local population and healthworkers (nationals or expatriate <strong>Haiti</strong>ans present <strong>in</strong> <strong>the</strong> country).Several health priorities dom<strong>in</strong>ated this first phase: search and rescue, trauma care, anddisposal of bodies. Many o<strong>the</strong>r concerns and activities were concomitant: water, food,and shelter. These issues shifted <strong>to</strong> <strong>the</strong> <strong>to</strong>p of <strong>the</strong> priority list once <strong>the</strong> life-sav<strong>in</strong>g activitiesended. All those priorities shared <strong>the</strong> same requirements (or constra<strong>in</strong>ts) such asavailability of data from rapid assessment, efficient logistics, and supply management.Urban Search and Rescue (USAR): its impact on health• The impact of <strong>in</strong>ternational USAR <strong>in</strong> terms of lives saved is relatively low compared<strong>to</strong> o<strong>the</strong>r measures. Streng<strong>the</strong>n<strong>in</strong>g local SAR capacity should be a priorityfor future disasters.• There are, however, o<strong>the</strong>r compell<strong>in</strong>g human and <strong>in</strong>stitutional benefits and objectives<strong>in</strong> provid<strong>in</strong>g this costly form of assistance.Search and rescue activities are not part of <strong>the</strong> health sec<strong>to</strong>r responsibility. They arehowever a life-sav<strong>in</strong>g activity with medical components. In addition, at <strong>the</strong> <strong>in</strong>ternationallevel this “sec<strong>to</strong>r” has been systematically organized and streng<strong>the</strong>ned, whichoffers potential lessons for improv<strong>in</strong>g <strong>the</strong> management of <strong>the</strong> health <strong>response</strong>.44 The pattern of shift<strong>in</strong>g priorities (from trauma <strong>to</strong> communicable diseases and primary health care) is common <strong>to</strong> many<strong>earthquake</strong>s. However, <strong>the</strong> phases are typically much shorter. The sheer number of <strong>in</strong>jured and <strong>the</strong> poor local capacity <strong>in</strong><strong>Haiti</strong> extended <strong>the</strong> surgical phase <strong>to</strong> more than two weeks <strong>in</strong>stead of a few days, as is cus<strong>to</strong>mary.45 A decrease <strong>in</strong> <strong>the</strong> number of urgent surgical <strong>in</strong>terventions was already noted on Day 10 (<strong>Health</strong> Cluster Bullet<strong>in</strong> No. 3, 22<strong>January</strong>).55
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>SAR contributions <strong>to</strong> sav<strong>in</strong>g livesInternational USAR started with<strong>in</strong> 24 hours of impact and ended on 22 <strong>January</strong>,when <strong>the</strong> Government declared <strong>the</strong> search and rescue phase over. No live rescues hadbeen reported <strong>in</strong> <strong>the</strong> preced<strong>in</strong>g days. Call<strong>in</strong>g off search and rescue activities is alwaysa difficult political decision. Survivors are known <strong>to</strong> have been rescued weeks after <strong>the</strong>impact. The fac<strong>to</strong>rs <strong>in</strong>fluenc<strong>in</strong>g <strong>the</strong> duration of survival are many, but <strong>the</strong> most criticaldur<strong>in</strong>g structural collapse is <strong>the</strong> “formation of a viable void space (i.e., a ‘pocket’or ‘survival space’ so <strong>the</strong> survivor escapes fatal <strong>in</strong>jury as <strong>the</strong> rubble settles). This voidspace is most likely <strong>to</strong> occur <strong>in</strong> concrete re<strong>in</strong>forced build<strong>in</strong>gs and <strong>the</strong> least probable <strong>in</strong>adobe constructions” (Mac<strong>in</strong>tyre, Barbera, Pet<strong>in</strong>aux 2011).There were 132 live rescues reported by <strong>in</strong>ternational USAR teams. This is <strong>the</strong> secondhighest number ever saved by <strong>in</strong>ternational teams. 46 This outcome was <strong>the</strong> result of<strong>the</strong> work of over 60 USAR teams from 30 nations respond<strong>in</strong>g with more than 1,800rescuers (UN/OCHA <strong>2010</strong>).The logistics challenges were formidable and <strong>the</strong> economic cost very high. 47 Cost-effectivenessmay be a controversial issue <strong>in</strong> humanitarian <strong>response</strong> where “no cost should be spared<strong>to</strong> save one life.” However, resources are limited and funds used for one relief activity maynot be available for ano<strong>the</strong>r. The expected outcome for <strong>the</strong> beneficiaries of each alternative<strong>in</strong>tervention should play a greater role <strong>in</strong> decid<strong>in</strong>g which type of assistance <strong>to</strong> provide.One country, a very strong promoter of <strong>the</strong> International Search and Rescue AdvisoryGroup (INSARAG), decided not <strong>to</strong> send its USAR team, which had beenplaced on standby at <strong>the</strong> depart<strong>in</strong>g airport. The ma<strong>in</strong> fac<strong>to</strong>r <strong>in</strong> this decision wasthat <strong>the</strong> expected delay <strong>in</strong> deployment was projected <strong>to</strong> be over 50 hours. Thecountry chose <strong>in</strong>stead <strong>to</strong> shift its resources <strong>to</strong> deploy a medical team specializ<strong>in</strong>g<strong>in</strong> pediatrics and obstetrics. 48 This pragmatic decision is credited <strong>in</strong> hav<strong>in</strong>gsaved <strong>the</strong> lives of 150 <strong>to</strong> 200 patients, many more than could have been rescuedby <strong>the</strong> USAR team.Cost-effectiveness does matter <strong>in</strong> relief activities but <strong>the</strong>re are many importantand legitimate considerations o<strong>the</strong>r than <strong>the</strong> number of lives saved <strong>in</strong>decid<strong>in</strong>g whe<strong>the</strong>r or not <strong>to</strong> send a USAR team (SDC 2011).3232 32AFILMPho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>Search and rescue is a time-sensitive activity (Mac<strong>in</strong>tyre et al. 2011). Its effectivenessdecl<strong>in</strong>es rapidly hours and days after <strong>the</strong> impact. This expla<strong>in</strong>s why <strong>the</strong> two local teamsfrom <strong>the</strong> <strong>Haiti</strong>an Direc<strong>to</strong>rate for Civil Protection saved 78 persons <strong>in</strong> spite of <strong>the</strong>irlimited skills and lack of equipment. 49 That statistic is not mentioned <strong>in</strong> reports onUSAR performance <strong>in</strong> <strong>Haiti</strong>.USAR performance <strong>in</strong>dica<strong>to</strong>rs (“live rescue”) provoke some questions:• Most of <strong>the</strong> foreign USAR teams concentrated <strong>the</strong>ir efforts on <strong>in</strong>stitutional venues,hotel facilities, and residential build<strong>in</strong>gs. Many of <strong>the</strong>se structures were built withre<strong>in</strong>forced concrete, where <strong>the</strong>re is a higher chance of survival for those trapped.46 More persons were rescued alive <strong>in</strong> <strong>the</strong> Turkey <strong>earthquake</strong> <strong>in</strong> 1999.47 The U.S. search and rescue teams saved 34 persons at a cost over US$ 40 million.48 It should be noted that public op<strong>in</strong>ion <strong>in</strong> this donor country was <strong>in</strong>itially aga<strong>in</strong>st <strong>the</strong> decision not <strong>to</strong> send USAR teams..49 This figure was cited <strong>in</strong> a presentation by <strong>the</strong> Direc<strong>to</strong>r of <strong>the</strong> <strong>Haiti</strong>an Direc<strong>to</strong>rate for Civil Protection at <strong>the</strong> INSARAG<strong>2010</strong> Global Meet<strong>in</strong>g, Kobe, Japan, 14–16 September <strong>2010</strong>. In addition <strong>to</strong> those 78 persons, a larger number were rescuedby relatives and neighbors, although <strong>the</strong> numbers and outcomes are unknown.56
THE LIFE-SAVING RESPONSE - Chapter 5The USAR teams do have an obligation <strong>to</strong> search for <strong>the</strong>ir own countrymen, and<strong>the</strong> occupants of <strong>the</strong>se build<strong>in</strong>gs were largely foreigners. No compiled <strong>in</strong>formationwas made available regard<strong>in</strong>g <strong>the</strong> nationality of <strong>the</strong> people rescued, but many local<strong>in</strong>terlocu<strong>to</strong>rs believed that <strong>the</strong>y were predom<strong>in</strong>antly foreigners.• Extricat<strong>in</strong>g someone alive is no guarantee that he or she will survive. Indeed, <strong>the</strong>medical capacity of <strong>the</strong> SAR teams was limited <strong>to</strong> <strong>in</strong>itial care and stabilizationand medical teams were overwhelmed with car<strong>in</strong>g for acute patients. A few teamstracked <strong>the</strong> outcome of those survivors days or weeks later. How many of <strong>the</strong> liverescues may have succumbed <strong>to</strong> <strong>the</strong>ir <strong>in</strong>juries shortly after rescue is not known,but it should be kept <strong>in</strong> m<strong>in</strong>d that many of <strong>the</strong> rescued are believed <strong>to</strong> have beenforeigners who were rapidly evacuated by air <strong>to</strong> sophisticated medical facilities.The most important health lesson from <strong>the</strong> <strong>in</strong>ternational USAR process is that <strong>the</strong>remust be a susta<strong>in</strong>ed effort <strong>to</strong> improve quality and coord<strong>in</strong>ation. Mechanisms usedby INSARAG <strong>to</strong> address coord<strong>in</strong>ation challenges are described below. 50• INSARAG is a network of disaster-prone and disaster-respond<strong>in</strong>g countries andorganizations dedicated <strong>to</strong> urban search and rescue (USAR) and operational fieldcoord<strong>in</strong>ation. It works <strong>to</strong> develop and promote <strong>in</strong>ternationally accepted proceduresand systems for susta<strong>in</strong>ed cooperation between national USAR teams operat<strong>in</strong>gon <strong>the</strong> <strong>in</strong>ternational scene.• A voluntary, <strong>in</strong>dependent peer-review process of <strong>in</strong>ternational USAR teams (<strong>the</strong> IN-SARAG External Classification—IEC), is a feature that does not exist but is neededfor foreign medical teams. IEC is seen as a capacity-build<strong>in</strong>g <strong>to</strong>ol and a means ofensur<strong>in</strong>g that <strong>in</strong>ternational m<strong>in</strong>imum standards are recognized by USAR teams. Itis also a work <strong>in</strong> progress: of <strong>the</strong> 60 <strong>to</strong> 70 USAR <strong>in</strong>ternational teams <strong>in</strong> <strong>Haiti</strong>, only8 were IEC classified while 8 were <strong>in</strong> <strong>the</strong> IEC queue for classification (UN/OCHA<strong>2010</strong>, 25).• An On-Site Operations Coord<strong>in</strong>ation Center (OSOCC) based on a concept orig<strong>in</strong>allydeveloped by UNDAC as part of <strong>the</strong> INSARAG methodology was activated<strong>in</strong> <strong>Haiti</strong>. Its objective is <strong>to</strong> assist affected countries <strong>to</strong> coord<strong>in</strong>ate <strong>in</strong>ternationalsearch-and-rescue efforts follow<strong>in</strong>g an <strong>earthquake</strong>.• A “virtual” OSOCC, a component of <strong>the</strong> OSOCC, was also established by UN-DAC and activated with <strong>the</strong> first alert <strong>in</strong> <strong>Haiti</strong>. It facilitated <strong>the</strong> registration of“who, what, and when” (i.e, who had what resources, who was ready <strong>to</strong> go, andwhen <strong>the</strong>y reached <strong>the</strong> disaster site). The virtual OSOCC attempts <strong>to</strong> registerall <strong>in</strong>com<strong>in</strong>g USAR groups while <strong>the</strong> OSOCC itself is deployed with receptionunits at <strong>the</strong> entry po<strong>in</strong>ts of <strong>the</strong> disaster-affected country (pr<strong>in</strong>cipally airports orsea ports).• A systematic attempt <strong>to</strong> evaluate <strong>the</strong>se mechanisms takes place at After-ActionReviews (AAR). Results and recommendations from <strong>the</strong> review feed <strong>in</strong><strong>to</strong> <strong>the</strong> IN-SARAG guidel<strong>in</strong>es.50 See <strong>the</strong> UN OCHA website for a full description of INSARAG activities: www.unocha.org/what-we-do/coord<strong>in</strong>ation-<strong>to</strong>ols/osocc-rdc/overview.57
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>The review undertaken by UNDAC at <strong>the</strong> After-Action Review Meet<strong>in</strong>g reached thisencourag<strong>in</strong>g conclusion: “The IEC-classified teams <strong>in</strong> <strong>Haiti</strong> demonstrated professionalism,followed <strong>the</strong> INSARAG Guidel<strong>in</strong>es throughout <strong>the</strong>ir deployment and madea genu<strong>in</strong>e difference dur<strong>in</strong>g <strong>the</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong>. The meet<strong>in</strong>g suggestedactions <strong>to</strong> be taken <strong>to</strong> ensure that priority was given <strong>to</strong> IEC classified teams by <strong>the</strong>affected countries dur<strong>in</strong>g an <strong>earthquake</strong> <strong>response</strong>” (UN/OCHA <strong>2010</strong>, 28). How effective<strong>the</strong>se mechanisms were <strong>in</strong> filter<strong>in</strong>g out sub-standard teams <strong>in</strong> <strong>the</strong> very difficultcontext of <strong>the</strong> first week <strong>in</strong> <strong>Haiti</strong> is, however, not documented.The health sec<strong>to</strong>r would benefit from review<strong>in</strong>g and, where appropriate, emulat<strong>in</strong>gthis process of quality control.Trauma careIn this section, several issues will be discussed: <strong>the</strong> role and contribution of foreignmedical teams (FMT) and foreign field hospitals (FFH, land- or sea-based), <strong>the</strong> applicationof triage techniques, surgical challenges, post-operative treatment, patientreferral, and evacuation issues.Earthquakes are unique among o<strong>the</strong>r disasters <strong>in</strong> that <strong>the</strong>y can produce an enormousnumber of <strong>in</strong>juries <strong>in</strong> <strong>the</strong> matter of a few seconds or m<strong>in</strong>utes. In tsunamis, relativelyfew survivors require medical care: most <strong>in</strong> <strong>the</strong> path of <strong>the</strong> wave are killed. The challenge<strong>to</strong> <strong>the</strong> health system posed by an <strong>earthquake</strong> is significantly different from conflictsituations where casualties are often announced or predictable and spread overdays or weeks. In <strong>earthquake</strong>s, <strong>the</strong> emergency services are taken by surprise (whatever<strong>the</strong>ir level of preparedness) and may suffer <strong>the</strong>mselves from <strong>the</strong> impact.Before <strong>the</strong> <strong>2010</strong> <strong>earthquake</strong>, emergency medical services <strong>in</strong> <strong>the</strong> non-profit system(State or NGOs) <strong>in</strong> <strong>Haiti</strong> were ill-equipped and understaffed <strong>to</strong> respond even <strong>to</strong>a small-scale event with mass casualties. In spite of tra<strong>in</strong><strong>in</strong>g courses on mass casualtymanagement and o<strong>the</strong>r <strong>in</strong>ternational cooperation <strong>in</strong>itiatives for preparedness,<strong>the</strong>y were unprepared <strong>to</strong> face large emergencies. The private for-profit sec<strong>to</strong>rwas nearly as poorly equipped <strong>to</strong> treat more than a few patients with severeconditions. The direct impact of <strong>the</strong> <strong>earthquake</strong> fur<strong>the</strong>r reduced this capacity.Emergency trauma care rema<strong>in</strong>ed <strong>the</strong> priority for over two weeks <strong>in</strong> <strong>Haiti</strong>until all patients received medical care supplied first by local personnel, followedby assistance from an <strong>in</strong>creas<strong>in</strong>g number of external partners.3232 32AFILMPho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>The discrepancy between <strong>the</strong> number of <strong>in</strong>jured persons (estimated at 300,000) and<strong>the</strong> data on <strong>the</strong> number of people treated (up <strong>to</strong> 173,000 “consultations” <strong>in</strong> 24 hospitalsover <strong>the</strong> first four months) (W<strong>in</strong>ter 2011), 51 suggests that dur<strong>in</strong>g <strong>the</strong> first daysmany people may have died from <strong>the</strong> lack of immediate medical attention and laterfrom secondary <strong>in</strong>fections. The University of Michigan survey provides an order ofmagnitude for this delayed mortality: For an estimated 111,794 killed on impact, anadditional 37,301 would not have survived <strong>the</strong>ir <strong>in</strong>juries <strong>in</strong> <strong>the</strong> next six weeks. That is12% of <strong>the</strong> estimated number of <strong>in</strong>juries (over 300,000) and one of four of <strong>the</strong> deathsattributable <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> (Kolbe et al. <strong>2010</strong>).51 This figure is approximate and only illustrative of <strong>the</strong> fact that many may not have received medical attention.58
THE LIFE-SAVING RESPONSE - Chapter 5For <strong>the</strong> first 24 hours: <strong>Haiti</strong> was on its own. The immediate <strong>response</strong>, for which <strong>the</strong>reare no quantified data, came from <strong>the</strong> nationals and o<strong>the</strong>r ac<strong>to</strong>rs already present <strong>in</strong>Port-au-Pr<strong>in</strong>ce. Those ac<strong>to</strong>rs experienced <strong>the</strong> <strong>in</strong>credible stress of a major <strong>earthquake</strong>;some had personal losses.Ambulances, barely available <strong>to</strong> <strong>the</strong> general population before <strong>the</strong> impact, were not anoption. Families ga<strong>the</strong>red <strong>the</strong>ir <strong>in</strong>jured relatives and delivered <strong>the</strong>m <strong>to</strong> <strong>the</strong> nearest healthfacility or its location if it was destroyed. Some opted <strong>to</strong> travel <strong>to</strong> <strong>the</strong> border with <strong>the</strong>Dom<strong>in</strong>ican Republic where <strong>in</strong>tact and better-equipped facilities could be expected.The first report from <strong>the</strong> University Hospital is illustrative of <strong>the</strong> difficult conditionsof work <strong>in</strong> <strong>the</strong> rema<strong>in</strong><strong>in</strong>g facilities:“At <strong>the</strong> time of <strong>the</strong> <strong>earthquake</strong>, <strong>the</strong>re were nearly 600 patients <strong>in</strong> <strong>the</strong>hospital. With<strong>in</strong> 30 m<strong>in</strong>utes of <strong>the</strong> impact, approximately 800 personsentered <strong>the</strong> premises; most were <strong>in</strong>jured, and 95% were trauma cases. Allpatients were on <strong>the</strong> grounds of <strong>the</strong> hospital as <strong>in</strong>structions were given <strong>to</strong>immediately evacuate <strong>the</strong> build<strong>in</strong>gs. Fifteen hundred patients <strong>in</strong>itiallyrequired care. At 5 PM, only night duty staff was present.“With <strong>the</strong> arrival of <strong>the</strong> Direc<strong>to</strong>r General of <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong> itwas possible for <strong>the</strong> medical staff <strong>to</strong> overcome <strong>the</strong>ir fear and reluctanceand enter <strong>the</strong> build<strong>in</strong>gs, where s<strong>to</strong>cks of medic<strong>in</strong>es and consumable supplies(alcohol, gauze, dress<strong>in</strong>gs, dis<strong>in</strong>fectant, cot<strong>to</strong>n, etc.) could be found.The entire s<strong>to</strong>ck was used dur<strong>in</strong>g <strong>the</strong> night. The pharmaceutical s<strong>to</strong>cks of<strong>the</strong> emergency services, surgery and <strong>in</strong>ternal medic<strong>in</strong>e departments, aswell as <strong>the</strong> warehouse of <strong>the</strong> central pharmacy were emptied”. 52This situation repeated itself <strong>in</strong> many public or NGO health facilities. With night fall<strong>in</strong>g,many of <strong>the</strong> most severely <strong>in</strong>jured were wait<strong>in</strong>g <strong>to</strong> be attended or died. Many of <strong>the</strong> <strong>Haiti</strong>andoc<strong>to</strong>rs, who at <strong>the</strong> time of impact were at <strong>the</strong>ir private practice or at home, attended<strong>to</strong> <strong>the</strong>ir neighbors. As noted earlier, report<strong>in</strong>g <strong>to</strong> <strong>the</strong>ir hospitals was not feasible: roads wereblocked, power was down, communications (<strong>in</strong>clud<strong>in</strong>g mobile phones) were unavailable,and <strong>the</strong> demand for <strong>the</strong>ir skills <strong>in</strong> <strong>the</strong>ir own neighborhoods was urgent and press<strong>in</strong>g.Humanitarian organizations, after a rapid <strong>in</strong>ven<strong>to</strong>ry of <strong>the</strong> health of <strong>the</strong>ir staff and <strong>the</strong>condition of <strong>the</strong>ir own facilities, were cop<strong>in</strong>g with ris<strong>in</strong>g numbers of casualties show<strong>in</strong>gup at <strong>the</strong>ir doors. 53Admittedly, <strong>Haiti</strong> was not prepared for any type of mass casualties. But no country orsystem could have had an orderly <strong>response</strong> <strong>to</strong> a disaster of this magnitude that affected<strong>the</strong> political, adm<strong>in</strong>istrative, and economic center of <strong>the</strong> country.After <strong>the</strong> <strong>in</strong>itial 24 hours, external assistance started <strong>to</strong> arrive while a flow of patientsand affected population was build<strong>in</strong>g up at <strong>the</strong> Dom<strong>in</strong>ican Republic border and <strong>in</strong>non-affected departments.52 Dr. Alex Larsen (HUEH), (nd), Rapport au M<strong>in</strong>istre de la Sante publique et de la Population. [Translated from <strong>the</strong> French.]53 By <strong>the</strong> end of <strong>the</strong> first week, MSF estimated it had treated more than 3,000 wounded people <strong>in</strong> <strong>the</strong> <strong>Haiti</strong>an capital andperformed more than 400 surgeries. Ultimately, MSF was one of <strong>the</strong> major ac<strong>to</strong>rs <strong>in</strong> emergency surgical care among <strong>the</strong>30 foreign field hospitals deployed dur<strong>in</strong>g this first three-month emergency phase. MSF surgeons performed 5,707 majorsurgical procedures, 150 of which <strong>in</strong>volved amputations (MSF 2011).59
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>The testimony of a Handicap International expert familiar with <strong>Haiti</strong> summarizes <strong>the</strong>situation <strong>in</strong> Port-au-Pr<strong>in</strong>ce:“We spent approximately two weeks <strong>in</strong> some 17 different hospitals, cl<strong>in</strong>ics,and field hospitals evaluat<strong>in</strong>g <strong>the</strong> numbers/types of catastrophic <strong>in</strong>juries,<strong>the</strong> acute needs (for personnel and equipment/supplies), and assist<strong>in</strong>g<strong>in</strong> plann<strong>in</strong>g longer term rehabilitation and care needs.“The capacity of each location serv<strong>in</strong>g trauma patients varied tremendously—somesites had multiple teams on <strong>the</strong> premises, o<strong>the</strong>r sites hadone provider only. . . Most of <strong>the</strong> hospital structures <strong>in</strong> <strong>the</strong> greater Portau-Pr<strong>in</strong>cearea had a mixture of local staff (doc<strong>to</strong>rs, nurses), <strong>in</strong>ternationalaid organizations (for example: Red Cross, MSF, Merl<strong>in</strong>) andsmall, <strong>in</strong>dependent groups or <strong>in</strong>dividuals who arrived with or without<strong>in</strong>vitation <strong>to</strong> assist (hospital groups, church-based, etc.).“There was—by all appearances and experience—little coord<strong>in</strong>ation betweenany of <strong>the</strong> sites. . . More often than not, an <strong>in</strong>dividual hospital hadlittle idea what o<strong>the</strong>r facilities <strong>in</strong> <strong>the</strong> Port-au-Pr<strong>in</strong>ce area could offer <strong>in</strong>terms of surgical services, how <strong>the</strong>y could f<strong>in</strong>d out that <strong>in</strong>formation, orhow <strong>to</strong> transport a patient <strong>to</strong> ano<strong>the</strong>r site. At each hospital where multipleorganizations were ‘on <strong>the</strong> ground,’ <strong>the</strong>re was at times little communicationeven between those groups.“By <strong>the</strong> second week, many of <strong>the</strong> hospitals had established patient track<strong>in</strong>gsystems; each patient rema<strong>in</strong><strong>in</strong>g was <strong>in</strong> a data-base. However, it appearedthat this was not coord<strong>in</strong>ated nationally—each hospital did its own th<strong>in</strong>g.Each organization seemed <strong>to</strong> have its own patient <strong>in</strong>formation form.“One of <strong>the</strong> issues I could see was that many responders had never been <strong>to</strong> <strong>Haiti</strong>,had no local cell phone, had no way <strong>to</strong> communicate with local authorities,and did not appear <strong>to</strong> know ‘who was <strong>in</strong> charge’.” 54Incom<strong>in</strong>g foreign medical teams and hospitals• The number of foreign medical teams or field hospitals is <strong>in</strong>creas<strong>in</strong>g <strong>in</strong> every disaster asis <strong>the</strong> diversity of <strong>the</strong>ir place of orig<strong>in</strong>.• In <strong>Haiti</strong>, <strong>the</strong>y arrived much earlier than <strong>in</strong> Indonesia or <strong>in</strong> Pakistan. Their effectivenesswas also higher consider<strong>in</strong>g <strong>the</strong> exceptional gap between <strong>the</strong> needs and localmedical resources.• PAHO/WHO guidel<strong>in</strong>es were not generally applied. A different approach <strong>to</strong>ward qualitycontrol of <strong>the</strong>se resources is required.54 Personal communication with Dr. Colleen O’Connell, MD, PMR, 31 <strong>January</strong> 2011.60
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong><strong>Haiti</strong> may have seen <strong>the</strong> highest number of field hospitals (land-based or on ship) provid<strong>in</strong>gassistance. Unlike <strong>the</strong> situation <strong>in</strong> <strong>the</strong> aftermath of almost all o<strong>the</strong>r disasters where those externalfacilities were under-utilized, hospital ships were work<strong>in</strong>g at near full capacity <strong>in</strong> <strong>Haiti</strong>and provid<strong>in</strong>g a most valuable, albeit short-term, replacement for secondary and tertiary levelfacilities lost <strong>in</strong> <strong>the</strong> impact (or that were lack<strong>in</strong>g prior <strong>to</strong> <strong>the</strong> disaster). Due <strong>to</strong> <strong>the</strong> collapse of<strong>the</strong> <strong>Haiti</strong>an health <strong>in</strong>frastructure, <strong>the</strong> USNS Comfort became <strong>the</strong> ma<strong>in</strong> tertiary level facility.Specifications for hospital ships for which data are available are shown <strong>in</strong> Table 5.2.Table 5.2 Hospital ships serv<strong>in</strong>g <strong>in</strong> <strong>Haiti</strong> after <strong>the</strong> <strong>earthquake</strong>Colombia a France b Mexico c Spa<strong>in</strong> d U.S.A. eShipCartagena de Sirico Huasteco Castilla USNS ComfortIndiasArrival date 22 Jan (Day 10) 24 Jan (Day 12) 20 Jan (Day 8) 4 Feb ( Day 23) 20 Jan (Day 8)Departure date 14 Feb 6 Feb n/a 4 May 10 MarchStay (no. of days) 23 10 n/a 64 36Capacity Multipurpose 50 beds Multipurpose /25 beds70 beds 50 trauma-beds;400 <strong>in</strong>termediatecarebeds, 500m<strong>in</strong>imal-care bedsOperat<strong>in</strong>g rooms 1 2 1 2 10-12ICU No No n/a 8 beds 30 bedsRx n/a n/a Yes No YesLabora<strong>to</strong>ry n/a n/a n/a Yes YesNo. of people attended 200 n/a n/a 7,568 869No. of surgical procedures 27 45 n/a 104 821Comments8 doc<strong>to</strong>rs from<strong>the</strong> CartagenaNavy HospitalMexican Navymedical professionalsFrench Navy<strong>in</strong> partnershipwith a fieldhospital andan advancedmedical unitA mobile healthunit <strong>in</strong> Petit Goaveprovided PHC andreferred selectedpatients <strong>to</strong> <strong>the</strong>ship, expla<strong>in</strong><strong>in</strong>g<strong>the</strong> high numberattendedNote: Only ships for which reports or sources of <strong>in</strong>formation are available have been <strong>in</strong>cluded. “n/a”= <strong>in</strong>formationnot available.a Radio Santa Fe Interview with Guillermo Barrera.b Website for Sirico vessel: http://tcd.siroco.free.fr/actualites<strong>2010</strong>haiti.htm.c Website for U.S. Navy: http://www.navy.mil/search/display.asp?s<strong>to</strong>ry_id=50975.d Revista Española de Defensa (<strong>2010</strong>).e Galeckas (2011).U.S. Navy coord<strong>in</strong>atedpatienttransfers with <strong>Haiti</strong>an,<strong>in</strong>ternational,and NGO healthfacilitiesSome observations can be made regard<strong>in</strong>g those ships:1. All arrived a week or more after <strong>the</strong> <strong>earthquake</strong>;2. The USNS Comfort was by far <strong>the</strong> most technically sophisticated;3. Two ships stayed beyond 30 days.62
THE LIFE-SAVING RESPONSE - Chapter 5All ships developed <strong>the</strong>ir own system of referral; often through one s<strong>in</strong>gle <strong>in</strong>stitution(e.g., HUEH for <strong>the</strong> USNS Comfort, <strong>the</strong> French Lyceum for <strong>the</strong> French vessel Sirico).Teams at o<strong>the</strong>r facilities did not necessarily know <strong>the</strong> criteria used by <strong>the</strong> hospital shipsfor accept<strong>in</strong>g patients.In addition <strong>to</strong> <strong>the</strong> self-conta<strong>in</strong>ed field hospitals, many foreign medical teams (FMT)built <strong>the</strong>ir own capacity nearly emulat<strong>in</strong>g that of <strong>the</strong> FFH, <strong>the</strong> only difference be<strong>in</strong>gthat services were delivered <strong>in</strong> local facilities that were conceded or commandeered.International claims and local reports or <strong>in</strong>terviews about <strong>the</strong> numbers of FMT could notbe easily reconciled. Track<strong>in</strong>g all FMTs was not feasible, but reconstruct<strong>in</strong>g what happened<strong>in</strong> <strong>the</strong> University Hospital, for <strong>in</strong>stance, illustrates <strong>the</strong> situation <strong>in</strong> many places.A report from HUEH clearly states that “<strong>the</strong> important and welcome assistance from<strong>the</strong> foreign humanitarians arrived <strong>the</strong> even<strong>in</strong>g of 14 <strong>January</strong> with two emergency physicians,<strong>the</strong>n three more arrived on 15 <strong>January</strong> but without material or medic<strong>in</strong>es”. 58Interviews with <strong>in</strong>ternational responders and national officials do not always offer<strong>the</strong> same timel<strong>in</strong>e of events, differ<strong>in</strong>g some times by only 24 hours. However, those24 hours may mean <strong>the</strong> difference between life and death for some patients. Thesedifferences are important <strong>to</strong> local counterparts: <strong>the</strong>y resent <strong>the</strong> exaggerated claims offoreign teams while perceiv<strong>in</strong>g <strong>the</strong>ir own efforts and contributions as be<strong>in</strong>g m<strong>in</strong>imizedor overlooked. This is representative of a serious communication problem.Assertions that field hospitals were not operational as early as needed, by no meanssuggests a deferred or leisurely <strong>response</strong>. Consider<strong>in</strong>g all <strong>the</strong> logistical, operational, andpolitical constra<strong>in</strong>ts, <strong>the</strong> deployment was massive and remarkably fast. This occurred <strong>in</strong>spite of problems caused by <strong>the</strong> restrictive military management of airport access.Integration of foreign assets with local authoritiesThe pace of FMT and FFH arrival rapidly accelerated. Follow<strong>in</strong>g aga<strong>in</strong> with <strong>the</strong>HUEH as example:“Support from <strong>the</strong> Emergency Unit of <strong>the</strong> Association of <strong>Haiti</strong>an Doc<strong>to</strong>rsAbroad (AMHE) arrived on 16 <strong>January</strong> (Day 4) with 60 persons. . .[This association] will set up <strong>the</strong> first section of post-traumatic emergencycare at <strong>the</strong> University Hospital. . . This team br<strong>in</strong>gs material, equipmentand medic<strong>in</strong>es as required. . . Ten o<strong>the</strong>r NGOs with a <strong>to</strong>tal of 200foreigners will succeed each o<strong>the</strong>r <strong>in</strong> shifts of one or two weeks until <strong>the</strong>end of March”. 59Accord<strong>in</strong>g <strong>to</strong> <strong>in</strong>terviews conducted with hospital authorities and <strong>in</strong>ternational ac<strong>to</strong>rs,some of <strong>the</strong> non-<strong>Haiti</strong>an teams operat<strong>in</strong>g <strong>in</strong> <strong>the</strong> first week <strong>in</strong> <strong>the</strong> HUEH reportedlycommandeered part of <strong>the</strong> premises, recruited personnel from outside <strong>the</strong> hospital,and denied <strong>the</strong> HUEH staff <strong>the</strong> roles <strong>the</strong>y considered as <strong>the</strong>ir own. Instead of assist<strong>in</strong>glocal authorities, <strong>the</strong>y displaced <strong>the</strong>m and <strong>to</strong>ok over. The same situation was reported58 Dr. Alex Larsen (HUEH), (nd), Rapport au M<strong>in</strong>istre de la Sante publique et de la Population. [Translated from <strong>the</strong>French.] Underl<strong>in</strong>ed text appeared <strong>in</strong> <strong>the</strong> orig<strong>in</strong>al.59 Under this head<strong>in</strong>g of NGO, <strong>the</strong> report <strong>in</strong>cluded bilateral governmental teams such as <strong>the</strong> Swiss Development Cooperation.Dr. Alex Larsen (HUEH), (nd), Rapport au M<strong>in</strong>istre de la Sante publique et de la Population. [Translated from <strong>the</strong>French.]63
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong><strong>in</strong> o<strong>the</strong>r facilities <strong>in</strong> <strong>Haiti</strong>. Interviews and reports on <strong>the</strong> Indian Ocean tsunami and<strong>the</strong> Pakistan <strong>earthquake</strong> <strong>in</strong>dicate that <strong>the</strong> problem is common <strong>in</strong> <strong>the</strong> humanitariancommunity. However, it is less of an issue <strong>in</strong> larger countries where <strong>the</strong>re is a stronggovernment and <strong>in</strong>stitutions have not been directly affected by <strong>the</strong> event.The issue of <strong>in</strong>tegrat<strong>in</strong>g national staff <strong>in</strong> foreign teams is complex. In fully equippedand well-established military type field hospitals, mak<strong>in</strong>g room <strong>in</strong> a tra<strong>in</strong>ed and homogenousteam for local health personnel may cause problems. However, <strong>in</strong>tegrat<strong>in</strong>glocal staff of <strong>the</strong> host<strong>in</strong>g facility should be less difficult for teams that are assembled fora specific event or those already work<strong>in</strong>g <strong>in</strong> <strong>the</strong> country before <strong>the</strong> event. Most agenciesfound it easier <strong>to</strong> recruit local personnel under <strong>the</strong>ir direct authority than <strong>to</strong> sharemanagement with local counterparts.The duration of <strong>the</strong> presence of <strong>the</strong> teams and hospitals varied widely: One highlyspecialized military field hospital was rapidly operational, triaged and treated patientswith <strong>the</strong> fastest possible turnover, and left after 10 days. Some, like <strong>the</strong> hospital ships,arrived later, specialized <strong>in</strong> <strong>the</strong> most difficult cases, and stayed longer. O<strong>the</strong>rs, suchas <strong>the</strong> Red Cross hospital, may stay <strong>in</strong>def<strong>in</strong>itely and be adm<strong>in</strong>istered by <strong>the</strong> local authorities.This is true <strong>in</strong> <strong>the</strong> case of some temporary emergency facilities that are builteven better than exist<strong>in</strong>g government facilities that were <strong>in</strong>tended <strong>to</strong> last for years (forexample, <strong>the</strong> MSF “conta<strong>in</strong>er” hospital <strong>in</strong> Léogâne). This is a matter of choice and <strong>the</strong>strategic decision of <strong>the</strong> donor, but that does not always co<strong>in</strong>cide with <strong>the</strong> M<strong>in</strong>istryof <strong>Health</strong> plan.There is benefit <strong>in</strong> this diversity as long as, like <strong>in</strong> an orchestra, <strong>the</strong>re is a score or masterplan that all follow. This was not <strong>the</strong> case <strong>in</strong> <strong>Haiti</strong>. Each “musician” played his/her <strong>in</strong>strumentas well as possible with <strong>the</strong> selected score. There is no surprise that <strong>the</strong> resultwas “cacophony” (<strong>the</strong> term used by Zanotti, <strong>2010</strong>).Quality controlThe quality and professionalism of <strong>the</strong> medico-surgical assistance appeared <strong>to</strong> be,<strong>in</strong> <strong>the</strong> op<strong>in</strong>ion of most <strong>in</strong>terlocu<strong>to</strong>rs, relatively satisfac<strong>to</strong>ry given <strong>the</strong> circumstances.There were, of course, noticeable exceptions and examples of possible unethical behavior.But <strong>the</strong>y were by far <strong>the</strong> exception. As noted by <strong>the</strong> Handicap International expertwho visited 17 hospitals <strong>in</strong> two weeks:“The care be<strong>in</strong>g adm<strong>in</strong>istered <strong>to</strong> patients <strong>in</strong> most <strong>in</strong>stances appeared appropriatefor <strong>the</strong> resources available. Stumps from amputations were be<strong>in</strong>gwrapped; patients were be<strong>in</strong>g fed and receiv<strong>in</strong>g water; fractures were be<strong>in</strong>gei<strong>the</strong>r treated by external fixa<strong>to</strong>rs (until fixa<strong>to</strong>rs were <strong>in</strong> short supply) or byimmobilization <strong>in</strong> casts” . 60The issue is that <strong>the</strong>re is no accepted standard or mechanism <strong>to</strong> moni<strong>to</strong>r and assess <strong>the</strong>quality of <strong>the</strong> trauma care. Op<strong>in</strong>ions are made based on occasional observation andconversation with colleagues. Reprehensive or dubious practices were not discouragedor penalized. 61 Relief assistance rema<strong>in</strong>s <strong>the</strong> “wild west” of medic<strong>in</strong>e where only <strong>the</strong>60 Personal communication, Colleen O’Connell, MD, <strong>in</strong> an e-mail of her f<strong>in</strong>d<strong>in</strong>gs while work<strong>in</strong>g with Handicap International.61 Reports of a foreign religious group approach<strong>in</strong>g patients <strong>in</strong> hospitals <strong>to</strong> conv<strong>in</strong>ce <strong>the</strong>m <strong>to</strong> seek cure through ritualsra<strong>the</strong>r than medical treatment was nei<strong>the</strong>r <strong>in</strong>vestigated nor acted on.64
THE LIFE-SAVING RESPONSE - Chapter 5most experienced and professionalized groups (military, Red Cross, MSF, among o<strong>the</strong>rs)have developed <strong>the</strong>ir own guidel<strong>in</strong>es, standards, and procedures. This situation isnot specific <strong>to</strong> <strong>Haiti</strong> but is generic <strong>in</strong> all crises where assistance is on a massive scale.Changes are overdue, as eloquently expressed <strong>in</strong> an article by several MSF experts(Chu et al. 2001):“As an <strong>in</strong>creas<strong>in</strong>g number of ac<strong>to</strong>rs are becom<strong>in</strong>g <strong>in</strong>volved <strong>in</strong> <strong>the</strong> delivery ofhumanitarian surgery, <strong>the</strong> need <strong>to</strong> establish a framework for quality surgicaldelivery is more press<strong>in</strong>g. The quality of surgical care may be regulatedthrough a comb<strong>in</strong>ation of structural, process, and output measures that could<strong>in</strong>clude m<strong>in</strong>imum standards for safe surgery, <strong>the</strong> deployment of appropriatelytra<strong>in</strong>ed surgeons and anes<strong>the</strong>siologists for <strong>the</strong>se contexts, pro<strong>to</strong>cols for preoperativeevaluation, <strong>in</strong>traoperative management and pos<strong>to</strong>perative care,and standardized databases <strong>to</strong> record pos<strong>to</strong>perative <strong>in</strong>fection and mortalityrates. A simple checklist for each patient can be utilized <strong>to</strong> ensure compliance.Standardiz<strong>in</strong>g data collection can help <strong>to</strong> evaluate surgical delivery”.As <strong>the</strong> authors noted <strong>in</strong> <strong>the</strong>ir article, <strong>the</strong>re may be resistance <strong>to</strong> such measures.Triage of mass casualties• Some form of triage was used by most of <strong>the</strong> foreign medical teams. Unlike o<strong>the</strong>r disasters,<strong>the</strong>re was no alternative <strong>in</strong> <strong>Haiti</strong> as <strong>the</strong> number of casualties wait<strong>in</strong>g on <strong>the</strong> frontsteps of <strong>the</strong> cl<strong>in</strong>ics or hospitals far exceeded <strong>the</strong> available resources.• Criteria for triage varied widely. The purpose was <strong>to</strong> maximize <strong>the</strong> use of <strong>the</strong> resourcesand capacity of each health care provider.The concept of triage orig<strong>in</strong>ated <strong>in</strong> France dur<strong>in</strong>g <strong>the</strong> late eighteenth century. 62 It focusedprimarily on mass casualty situations where a systematic sort<strong>in</strong>g process sought <strong>to</strong> assignpriorities <strong>in</strong> care <strong>in</strong> order <strong>to</strong> save as many lives as possible.Triage is not just one concept. Today <strong>the</strong>re are at least two different scenarios dur<strong>in</strong>gwhich triage is applied: 1) at <strong>the</strong> scene of <strong>the</strong> mass casualty event, also called prehospitalcare, and 2) <strong>in</strong> health care facilities.In <strong>the</strong> former, <strong>the</strong> first responder community selects those <strong>in</strong>jured who will be givenpriority for primary stabilization and transportation <strong>to</strong> health facilities. Initial medicalcare might be provided at an advanced health post at <strong>the</strong> site of <strong>the</strong> emergency. This isonly applicable <strong>in</strong> localized mass casualty <strong>in</strong>cidents where a medical command centercan be established. Its effectiveness lies <strong>in</strong> <strong>the</strong> limited number of patients and controlof transportation/dispatch by receiv<strong>in</strong>g <strong>in</strong>stitutions. The dilemma is who is treatedfirst or last.62 Robertson-Steel (2006) states that Baron Dom<strong>in</strong>ique Jean Larrey, Surgeon-<strong>in</strong>-Chief <strong>to</strong> Napoleon’s Imperial Guard, was <strong>the</strong>first <strong>to</strong> apply a process of sort<strong>in</strong>g around 1792.65
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>In health care facilities, <strong>in</strong>jured persons have reached hospitals and health facilities (or<strong>the</strong> facility’s location if it has been destroyed). They are often accompanied by relativeswho are vocal <strong>in</strong> demand<strong>in</strong>g attention. Contrary <strong>to</strong> what happens dur<strong>in</strong>g normal situations,<strong>in</strong> which <strong>the</strong> severity of a patient’s condition determ<strong>in</strong>es <strong>the</strong> priority of attention,<strong>in</strong> <strong>the</strong> event of a disaster, <strong>the</strong> imbalance between <strong>the</strong> demand and <strong>the</strong> available resourcesrequires care providers <strong>to</strong> consider not only <strong>the</strong> severity of <strong>the</strong> patient’s condition, bu<strong>to</strong><strong>the</strong>r criteria such as <strong>the</strong> prognosis and <strong>the</strong> benefit that <strong>the</strong> action taken (care and/ortransportation accord<strong>in</strong>g <strong>to</strong> available capabilities) will afford <strong>the</strong> patient. Those with apoor prognosis (likely <strong>to</strong> die, <strong>in</strong> most <strong>in</strong>stances) or those who will not suffer irreversibledamage if care is delayed, are placed on hold or denied access <strong>to</strong> <strong>the</strong> facility.Therefore, triage must be more rigorous and selective <strong>to</strong> <strong>the</strong> extent that <strong>the</strong> magnitudeof <strong>the</strong> disaster <strong>in</strong>creases and <strong>the</strong> disparity between needs and capabilities andresources becomes greater. The dilemma under this scenario rema<strong>in</strong>s: Who is go<strong>in</strong>g<strong>to</strong> be treated? This is someth<strong>in</strong>g not easily unders<strong>to</strong>od and accepted by patients and<strong>the</strong>ir relatives.For more than 72 hours <strong>in</strong> <strong>Haiti</strong>, <strong>the</strong> process of transport<strong>in</strong>g <strong>in</strong>jured persons was massive,spontaneous, and chaotic. Hospitals and health centers were surrounded by <strong>in</strong>juredpersons and corpses taken <strong>the</strong>re by <strong>the</strong> population. While local health facilities were notprepared for <strong>the</strong> systematic use of triage, most of <strong>the</strong> foreign teams and hospitals hadsome criteria for screen<strong>in</strong>g patients <strong>the</strong>y would accept. Table 5.3 illustrates this po<strong>in</strong>twith f<strong>in</strong>d<strong>in</strong>gs from three hospitals.Transport<strong>in</strong>g <strong>the</strong> <strong>in</strong>jured66Pho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>
THE LIFE-SAVING RESPONSE - Chapter 5Table 5.3 Triage experiences <strong>in</strong> selected health facilitiesfollow<strong>in</strong>g <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong>Local health facilities supportedby MSFOperative <strong>in</strong> <strong>Haiti</strong> before <strong>the</strong><strong>earthquake</strong> and cont<strong>in</strong>ues <strong>to</strong> bepresent <strong>in</strong> <strong>Haiti</strong> a“In <strong>the</strong> immediate aftermath . . .it was not possible. . . <strong>to</strong> carry outsystematic triage due <strong>to</strong> <strong>the</strong> massivenumbers of wounded peopleflood<strong>in</strong>g hospital grounds”(MSF 2011) bField hospital (Israeli DefenseForces)Started on Day 4 and cont<strong>in</strong>uedfor 10 daysHospital ship (USNS Comfort)Period ofperformanceStarted on Day 8 and cont<strong>in</strong>uedfor 40 daysCriteria foraccept<strong>in</strong>gpatientsPatients with severe <strong>in</strong>juries(<strong>in</strong>clud<strong>in</strong>g open and <strong>in</strong>fectedwounds); patients with antici–pated short-term treatment (up<strong>to</strong> 24–48 hours); and patientswho had just been rescued byUSAR (Mer<strong>in</strong> et al. <strong>2010</strong>) cPatients with bra<strong>in</strong> <strong>in</strong>juries;paraplegia secondary <strong>to</strong> sp<strong>in</strong>al<strong>in</strong>juries; low score <strong>in</strong> <strong>the</strong> Glasgowcoma score. Attention <strong>to</strong> patientswith crush <strong>in</strong>juries was <strong>in</strong>itiallydenied, but this criterionchanged one week later whendialysis equipment was availableOnly patients with <strong>earthquake</strong>related<strong>in</strong>juries (e.g., complicatedextremity <strong>in</strong>juries, obstetriccases, and maxillofacial <strong>in</strong>juries)(Etienne et al. <strong>2010</strong>; Auerbach etal. <strong>2010</strong>)Criteria fordeny<strong>in</strong>g careNo patients were rejected. Somepatients were referred <strong>to</strong> San<strong>to</strong>Dom<strong>in</strong>go for advanced treatmentand some severe burn<strong>in</strong>juries were referred <strong>to</strong> <strong>the</strong> USNSComfortLess severely <strong>in</strong>jured patientswho could be attended <strong>in</strong> o<strong>the</strong>rhealth facilities <strong>in</strong> Port-au-Pr<strong>in</strong>ceCases not accepted <strong>in</strong>cluded: pelvicfractures, closed head <strong>in</strong>juries,complete sp<strong>in</strong>al cord lesions, andcases requir<strong>in</strong>g assisted ventilation(Auerbach et al. <strong>2010</strong>)821 surgical procedures on 446patients (Ray et al. <strong>2010</strong>)Patientstreated5,707 major surgical procedures(first month: 2,386; secondmonth: 1,902; third month: 1,419)1,100 treated patients242 surgical procedures underanes<strong>the</strong>sia were performed on205 patientsa Two of <strong>the</strong> three secondary level health care structures that Médec<strong>in</strong>s Sans Frontières operated <strong>in</strong> Port-au-Pr<strong>in</strong>cewere destroyed; only one emergency facility was still functional.b With<strong>in</strong> a few hours of <strong>the</strong> <strong>earthquake</strong>, more than 400 critically <strong>in</strong>jured and dy<strong>in</strong>g patients arrived at once. Personnelfocused primarily on m<strong>in</strong>or wound dress<strong>in</strong>gs of <strong>in</strong>jured persons, try<strong>in</strong>g <strong>to</strong> organize triage, and provid<strong>in</strong>g immediatelife-sav<strong>in</strong>g surgery and end-of-life-care.c Patients with mild <strong>in</strong>juries (ambula<strong>to</strong>ry patients) and pregnant women were referred <strong>in</strong>ternally <strong>to</strong> different areas.Given <strong>the</strong> shortcom<strong>in</strong>gs <strong>in</strong> <strong>in</strong>formation management, it is impossible <strong>to</strong> establish <strong>the</strong>number of <strong>in</strong>jured, <strong>the</strong> number accepted, and <strong>the</strong> number rejected for <strong>in</strong>juries classifiedas <strong>to</strong>o severe, much less <strong>to</strong> estimate <strong>the</strong> subsequent morbidity and mortality.Under this scenario, it is <strong>the</strong>refore very difficult <strong>to</strong> determ<strong>in</strong>e <strong>the</strong> effectiveness of <strong>the</strong>implemented triage techniques <strong>in</strong> <strong>the</strong> number of lives saved.What <strong>the</strong> triage clearly achieved is a better use of <strong>the</strong> very scarce operat<strong>in</strong>g facilities.Theaters and surgeons’ time were optimized <strong>in</strong> most cases. It should be emphasizedthat surgery is only one critical step <strong>in</strong> <strong>the</strong> treatment process.Independent teams have improved <strong>the</strong>ir own performance, but <strong>the</strong>se are <strong>in</strong>itial andfacility-centered achievements. 63 The success of one team could imply <strong>the</strong> failure ofo<strong>the</strong>r teams not equipped <strong>to</strong> provide post-operative care or referral with <strong>the</strong> consequent<strong>in</strong>crease <strong>in</strong> morbidity and mortality. The impact of triage should also be seenwith<strong>in</strong> a health care network that shares <strong>in</strong>formation, resources, and capabilities.In <strong>Haiti</strong>, a holistic view of <strong>the</strong> flow of casualties was miss<strong>in</strong>g.63 Government of Israel (<strong>2010</strong>), “Triage <strong>in</strong> mass causality events—tak<strong>in</strong>g s<strong>to</strong>ck of <strong>the</strong> <strong>Haiti</strong>an experience” [unpublished].67
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Surgical approaches and issuesThe 12 <strong>January</strong> <strong>earthquake</strong> generated many scientific peer-reviewed articles. 64 A significantnumber address <strong>the</strong> suitability of various techniques for anes<strong>the</strong>sia or surgery,subjects which are not part of <strong>the</strong> scope of this publication. O<strong>the</strong>r <strong>to</strong>pics <strong>in</strong>clude advancesmade <strong>in</strong> electronic management of medical files and patient registration underemergency conditions, <strong>the</strong> use of advanced labora<strong>to</strong>ries, po<strong>in</strong>t-of-care technology fordiagnosis, <strong>the</strong> application of portable diagnostic devices (ultrasound for <strong>in</strong>stance). 65The potential for robust, field-tested technologies is important for <strong>the</strong> future of disastermedic<strong>in</strong>e <strong>in</strong> poor countries.Several papers have been published that disaggregate cases by condition, but few offerdetails on <strong>the</strong> type of procedures or treatment. Figures 5.2 and 5.3, show<strong>in</strong>g surgicaland orthopedic <strong>in</strong>terventions at <strong>the</strong> University Hospital and at MSF facilities, illustratewhat appears <strong>to</strong> be a common pattern <strong>in</strong> <strong>the</strong> first weeks after <strong>the</strong> <strong>earthquake</strong>.Figure 5.2 Features of trauma <strong>in</strong>terventions performed at HUEH,<strong>Haiti</strong>, <strong>January</strong>–February <strong>2010</strong>Plasc surgery, 10;1%Suture, 2;0.3%Tracon/Extension, 14;2%Dress<strong>in</strong>g, 393;62%Debridement, 119;19%Delayed primary closure, 7;1%Fracture, 98;16%Amputaon, 7;1%Cast, 61;10%External fixa<strong>to</strong>rs, 23;4%Source: Adapted from official data provided from <strong>the</strong> Swiss Development Corporation. Reproduced with permission.64 As of August 2011, a Medl<strong>in</strong>e search on <strong>the</strong> <strong>Haiti</strong> <strong>earthquake</strong> produced 280 titles.65 The use of health technology <strong>in</strong> humanitarian <strong>response</strong> was <strong>the</strong> subject of a one-day summit between civilan and militaryexperts and NGOs. Baltimore, Maryland, 29 September <strong>2010</strong>.68
THE LIFE-SAVING RESPONSE - Chapter 5Figure 5.3 Surgical and orthopedic proceduresperformed <strong>in</strong> MSF facilitiesNumber of <strong>in</strong>terventions, by type,13 <strong>January</strong> <strong>to</strong> 12 February <strong>2010</strong>, <strong>Haiti</strong>1000900800Number of <strong>in</strong>terventions7006005004003002001000WoundsurgeryOrthopedicsM<strong>in</strong>orsurgeryGynecologyandObstetricsVisceralsurgerySpecializedsurgery400Number of orthopedic procedures, by type,13 <strong>January</strong> <strong>to</strong> 12 February <strong>2010</strong>, <strong>Haiti</strong>350Number of <strong>in</strong>terventions300250200150100500Reduction offractures &luxationsAmputationof a limbFixa<strong>to</strong>r External Osteosyn<strong>the</strong>sis OrthopedicsvariousSource: Axelle Ronsse, Médic<strong>in</strong>s sans Frontières, “Surgical <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>2010</strong> <strong>Haiti</strong> <strong>earthquake</strong>” (powerpo<strong>in</strong>t presentation).Used with permission.69
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Four medical conditions call for special attention: crush syndrome with its lethal renalfailure, sp<strong>in</strong>al cord <strong>in</strong>jury (SCI), amputations, and, more generally, fractures. Interest<strong>in</strong>gly,<strong>the</strong> general proliferation of humanitarian agencies has also resulted <strong>in</strong> <strong>the</strong> emergenceof new or <strong>in</strong>creas<strong>in</strong>gly proactive partners offer<strong>in</strong>g highly specialized expertiseand assistance for some of those conditions.The “renal disaster”The expression “renal disaster” used <strong>in</strong> a scientific article on crush syndrome (Sever,Lameire, Vanholder 2009) illustrates <strong>the</strong> potential for loss of lives due <strong>to</strong> shortcom<strong>in</strong>gs<strong>in</strong> diagnos<strong>in</strong>g and treat<strong>in</strong>g severe cases of crush syndrome. As noted by <strong>the</strong> sameauthors: “Although many crush patients can survive with<strong>in</strong> <strong>the</strong> first hours or even daysuntil rescue, death will be <strong>in</strong>evitable for most of <strong>the</strong>m after extrication if emergencymeasures for <strong>the</strong> prevention of [acute kidney <strong>in</strong>jury] AKI… are not taken.”Crush syndrome patients and, by extension, <strong>the</strong> renal victims are usually overlookedor neglected. “Accord<strong>in</strong>g <strong>to</strong> <strong>the</strong> general perception, <strong>the</strong>y constitute a relatively m<strong>in</strong>orgroup requir<strong>in</strong>g complex and labor-<strong>in</strong>tensive <strong>the</strong>rapeutic measures and are rarely<strong>in</strong>cluded <strong>in</strong> governmental or local disaster plans” (Sever, Lameire, Vanholder 2009).Informal and empirical enquiries by PAHO/WHO <strong>in</strong> past disasters <strong>in</strong> Lat<strong>in</strong> Americahave shown a lack of awareness of this condition. Ei<strong>the</strong>r Lat<strong>in</strong> American <strong>earthquake</strong>sdid not produce many crush syndromes or <strong>the</strong> condition was under-diagnosed.The Renal Disaster Relief Task Force (RDRTF) of <strong>the</strong> International Society of Nephrologywas established <strong>to</strong> provide specialized care (<strong>in</strong>clud<strong>in</strong>g dialysis) for this specialgroup of patients. Strong on expertise but weak on logistics and operational skills, <strong>the</strong>group partnered with MSF.A dialysis center with eight units was operational <strong>in</strong> <strong>Haiti</strong> on Day 5, <strong>in</strong> time <strong>to</strong> preventfatalities (which generally occur between 4 and 10 days after <strong>the</strong> trauma). 66 Efforts by<strong>the</strong> task force <strong>to</strong> publicize <strong>the</strong>ir availability and expertise <strong>to</strong> o<strong>the</strong>r medical partners <strong>in</strong>Port-au-Pr<strong>in</strong>ce were limited. In particular, <strong>the</strong>y did not rout<strong>in</strong>ely participate <strong>in</strong> <strong>the</strong>coord<strong>in</strong>ation meet<strong>in</strong>gs, and as a consequence, did not receive a large number of referrals<strong>to</strong> <strong>the</strong>ir facilities (only 19). Among <strong>the</strong> many important announcements of availableservices published <strong>in</strong> <strong>the</strong> <strong>Health</strong> Cluster Bullet<strong>in</strong>, no mention was made of crushsyndrome and <strong>the</strong> exist<strong>in</strong>g resources for diagnosis (<strong>in</strong>clud<strong>in</strong>g po<strong>in</strong>t-of-care labora<strong>to</strong>rydevices) and treatment. The lack of participation of <strong>the</strong> task force <strong>in</strong> <strong>the</strong> cluster meet<strong>in</strong>gsresulted <strong>in</strong> a facility that could accommodate up <strong>to</strong> 200 patients a day runn<strong>in</strong>gat 20% of its capacity. 67As expressed <strong>in</strong> a letter <strong>to</strong> <strong>the</strong> edi<strong>to</strong>r of Lancet by <strong>the</strong> Task Force, one of <strong>the</strong> majorlessons it learned from <strong>the</strong> <strong>Haiti</strong> disaster is <strong>the</strong> need for better <strong>in</strong>teragency communication(Vanholder et al. <strong>2010</strong>). In this particular case, <strong>the</strong> full-time assignmen<strong>to</strong>f a liaison officer/technician <strong>to</strong> participate <strong>in</strong> <strong>the</strong> numerous meet<strong>in</strong>gs would havebeen cost-effective. This is one example where it can be demonstrated that participation<strong>in</strong> coord<strong>in</strong>ation meet<strong>in</strong>gs would have saved more lives.66 Immediate deaths follow<strong>in</strong>g release from entrapment are caused by hyperkalemia.67 There are no data on <strong>the</strong> number of untreated crush syndromes <strong>in</strong> <strong>Haiti</strong>, but it is estimated <strong>to</strong> be several times more than<strong>the</strong> 200-patient capacity of <strong>the</strong> dialysis center.70
THE LIFE-SAVING RESPONSE - Chapter 5Ano<strong>the</strong>r observation is <strong>the</strong> need for special tagg<strong>in</strong>g and medical supervision of patientsundertak<strong>in</strong>g periodic dialysis. When mixed with o<strong>the</strong>r patients, treat<strong>in</strong>g doc<strong>to</strong>rsand even visit<strong>in</strong>g medical volunteers from o<strong>the</strong>r groups were prescrib<strong>in</strong>g treatment<strong>in</strong>compatible with dialysis or even select<strong>in</strong>g <strong>the</strong> patient for immediate transfer <strong>to</strong> o<strong>the</strong>rfacilities. 68Sp<strong>in</strong>al cord <strong>in</strong>jury (SCI)Prior <strong>to</strong> <strong>the</strong> <strong>earthquake</strong>, <strong>the</strong> mid-term survival rate of <strong>Haiti</strong>an patients with SCI wasbelieved <strong>to</strong> be almost nil. In <strong>the</strong> aftermath of this disaster, over 150 such cases reachedmedical facilities, pass<strong>in</strong>g through or bypass<strong>in</strong>g <strong>the</strong> triage system designed <strong>to</strong> selectthose patients with more chance of survival at <strong>the</strong> lowest cost <strong>in</strong> medical resources, acriterion SCI does not meet. In past disasters, <strong>in</strong> medically under-developed countries,<strong>the</strong> prognosis of those patients would have been grim.In <strong>Haiti</strong>, early advocacy for action was published <strong>in</strong> lead<strong>in</strong>g professional publications(edi<strong>to</strong>rials, <strong>in</strong>vited comments, and forums). Appeals for specialists andphysio<strong>the</strong>rapists were launched and heard. Several groups dedicated special resources<strong>to</strong> those cases. Among <strong>the</strong>m were <strong>the</strong> Project Medishare of <strong>the</strong> Universityof Miami, which <strong>in</strong>cluded a sp<strong>in</strong>al care unit <strong>in</strong> <strong>the</strong> tent hospital (G<strong>in</strong>zburg et al.<strong>2010</strong>; Wang <strong>2010</strong>); <strong>the</strong> <strong>Haiti</strong> Hospital Appeal, 69 a small NGO that transformed<strong>the</strong>ir soon-<strong>to</strong>-be-opened pediatric facility <strong>in</strong><strong>to</strong> an adult rehabilitation center forup <strong>to</strong> 22 SCI (Landry et al. <strong>2010</strong>a; Stephenson 2011); Heal<strong>in</strong>g Hands for <strong>Haiti</strong>International, a well-established rehabilitation NGO; and f<strong>in</strong>ally, <strong>the</strong> U.S. Navyhospital ship, <strong>the</strong> USNS Comfort (Landry et al. <strong>2010</strong>a; Burns et al. <strong>2010</strong>). Later,o<strong>the</strong>r organizations such as <strong>the</strong> Toron<strong>to</strong> Rehabilitation Institute assisted with specialistSCI <strong>in</strong>put.While a sp<strong>in</strong>al cord <strong>in</strong>jury once practically condemned <strong>the</strong> patient <strong>to</strong> death with<strong>in</strong> afew years, patients <strong>in</strong> <strong>Haiti</strong> are now receiv<strong>in</strong>g more appropriate care. It is an area where<strong>the</strong> disaster has triggered a permanent improvement of <strong>the</strong> health services.Treatment of fracturesAs noted by physicians work<strong>in</strong>g with Handicap International (O’Connell et al. <strong>2010</strong>, 8),fractures were <strong>the</strong> most common diagnosis:“All modes of fracture management have been reported, <strong>in</strong>clud<strong>in</strong>g: traction,closed reduction, open reduction, <strong>in</strong>ternal fixation, external fixa<strong>to</strong>r,slab cast and spl<strong>in</strong>t, and complete circumferential cast<strong>in</strong>g. Lack of imag<strong>in</strong>gcapacity <strong>in</strong> many facilities limited diagnostic abilities, and doc<strong>to</strong>rs notedthat some fractures had <strong>to</strong> be diagnosed by palpation only. O<strong>the</strong>r centersran out of film and process<strong>in</strong>g agents, result<strong>in</strong>g <strong>in</strong> similar limitations”.68 In <strong>the</strong> first weeks, it was not uncommon for foreign physicians <strong>to</strong> repeatedly visit a health facility <strong>to</strong> exam<strong>in</strong>e a particularpatient and leave <strong>in</strong>structions for <strong>the</strong> facility’s local nurs<strong>in</strong>g personnel.69 See www.haitihospitalappeal.org.71
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>The result of this situation is that months after <strong>the</strong> <strong>earthquake</strong>, many of <strong>the</strong> fracturesrequired a second operation for realignment of <strong>the</strong> bones.One issue still debated among emergency professionals is <strong>the</strong> use of external versus <strong>in</strong>ternalfixa<strong>to</strong>rs, <strong>the</strong> latter requir<strong>in</strong>g sterile operat<strong>in</strong>g conditions rarely found <strong>in</strong> disasterconditions (Lebel et al. 2011).AmputationsAmputations may save lives, but <strong>the</strong>y also threaten <strong>the</strong> social life and economic survivalof <strong>the</strong> patients. It is a procedure that should not be taken lightly. Rehabilitation andsupport services are below standard <strong>in</strong> <strong>Haiti</strong>, as <strong>in</strong> many countries. Disabled persons,whatever <strong>the</strong> cause of <strong>the</strong>ir disability and <strong>the</strong>ir prior status, are rejected by society. Theyare considered as “punished by god for <strong>the</strong>ir s<strong>in</strong>s” and are hidden at home. 70 Undertak<strong>in</strong>gan amputation has a very high social and human cost.After <strong>the</strong> Pakistan <strong>earthquake</strong> <strong>in</strong> 2005, unpublished concern regard<strong>in</strong>g possibly unnecessaryamputations had already emerged. In on-site <strong>in</strong>terviews, some medical teams wereseem<strong>in</strong>gly present<strong>in</strong>g <strong>the</strong> high number of amputations made under difficult field conditionsas <strong>in</strong>dicative of <strong>the</strong> heroism of <strong>the</strong>ir <strong>in</strong>tervention.In <strong>Haiti</strong>, this issue became publicized follow<strong>in</strong>g <strong>the</strong> prelim<strong>in</strong>ary report from HandicapInternational project<strong>in</strong>g <strong>the</strong> number of amputees <strong>to</strong> be over 2,000 and possibly up <strong>to</strong>70 “In a country where 10 percent of <strong>the</strong> population is disabled, you could spend a week here and never see any [disabledpersons],” said Josue Joseph, a spokesperson for <strong>the</strong> <strong>Haiti</strong>an Secretariat for Integration. Accessed at: www.terradaily.com/afp/100609015616.nv60byyh.html, June <strong>2010</strong>.Post-operative care72Pho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>
THE LIFE-SAVING RESPONSE - Chapter 5Patient with external fixa<strong>to</strong>rs4,000 (O’Connell et al. <strong>2010</strong>). Later this figurewas adjusted <strong>to</strong> 1,200–1,500. For <strong>the</strong> purposeof illustration, MSF, <strong>the</strong> largest provider ofemergency surgical care <strong>in</strong> <strong>the</strong> first weeks, reportedhav<strong>in</strong>g performed 173 amputations ona <strong>to</strong>tal of 147 patients (16 of <strong>the</strong>se patients underwentmultiple <strong>in</strong>terventions, possibly <strong>in</strong>volv<strong>in</strong>gtwo separate limbs). Medical teams at <strong>the</strong>border with <strong>the</strong> Dom<strong>in</strong>ican Republic reported217 amputations.As noted <strong>in</strong> <strong>the</strong> prelim<strong>in</strong>ary survey by HandicapInternational (O’Connell et al. <strong>2010</strong>),<strong>the</strong>re are many reasons why amputations areperformed, <strong>in</strong>clud<strong>in</strong>g: as primary <strong>in</strong>terventionfor complex severe wounds and fractures mak<strong>in</strong>g<strong>the</strong> limb unviable or as “secondary treatment for <strong>in</strong>fected wounds, compartmentsyndromes, and poorly treated fractures”.Pho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>Techniques for amputations were also questioned. Use of <strong>the</strong> so-called guillot<strong>in</strong>e techniqueguarantees <strong>the</strong> need for repeated, corrective <strong>in</strong>terventions on <strong>the</strong> stump <strong>to</strong> accommodatepros<strong>the</strong>sis. This technique is much more rapid (m<strong>in</strong>utes <strong>in</strong>stead of hours) and does notrequire much skill or <strong>in</strong>strumentation. Conservative treatment of severe <strong>in</strong>fection requirestime-consum<strong>in</strong>g and susta<strong>in</strong>ed nurs<strong>in</strong>g care (a profession under-represented <strong>in</strong> <strong>the</strong> humanitarian<strong>response</strong>), and its success is far from certa<strong>in</strong>. Most of <strong>the</strong> <strong>in</strong>terlocu<strong>to</strong>rs recognizedthat under <strong>the</strong> extreme workload and lack of adequate facilities, often <strong>the</strong>re wereno better options than <strong>to</strong> amputate a limb that could have been saved <strong>in</strong> better equippedfacilities (follow<strong>in</strong>g <strong>the</strong> pr<strong>in</strong>ciple of triage <strong>to</strong> maximize <strong>the</strong> benefits).The level of amputation is paramount for <strong>in</strong>dications for pros<strong>the</strong>sis. In 107 cases reviewedby Handicap International, above <strong>the</strong> knee amputations represented <strong>the</strong> largestproportion of lower limb amputations (63%) versus 37% for amputations below <strong>the</strong>knee (see Table 5.4). There are <strong>in</strong>sufficient data for comparison with o<strong>the</strong>r disasters.Table 5.4 Level of amputation <strong>in</strong> patients <strong>in</strong>jured <strong>in</strong> <strong>Haiti</strong> <strong>earthquake</strong>Level of amputation No. Percentage of amputeesBelow knee 27 25%Above knee 46 43%Upper limb 17 16%Unspecified 17 16%Total 107 100%Note: Data from Handicap International (O’Connell et al. <strong>2010</strong>).Publicity about this issue had some benefits for <strong>the</strong> population and offered some lessons:1. First, it is crucial <strong>to</strong> centrally register <strong>the</strong> number of amputations, moni<strong>to</strong>r <strong>the</strong> useof this procedure, and review <strong>the</strong>ir <strong>in</strong>dications.73
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>2. A key step <strong>in</strong> develop<strong>in</strong>g local health systems is <strong>the</strong> establishment of surgical outcomesmoni<strong>to</strong>r<strong>in</strong>g. Such moni<strong>to</strong>r<strong>in</strong>g can optimize patient follow-up and fosterprofessional accountability for <strong>the</strong> treatment of amputation patients <strong>in</strong> disastersett<strong>in</strong>gs and humanitarian emergencies (Knowl<strong>to</strong>n et al. 2011).3. The number of amputees is not <strong>the</strong> same as <strong>the</strong> number of those want<strong>in</strong>g or requir<strong>in</strong>gpros<strong>the</strong>ses. Indeed, some amputations may not be suitable for pros<strong>the</strong>sisand some amputees might prefer <strong>to</strong> capitalize on <strong>the</strong>ir disability. In <strong>2010</strong>, Heal<strong>in</strong>gHands for <strong>Haiti</strong> partnered with Handicap International <strong>to</strong> provide some 500pros<strong>the</strong>ses. About half of <strong>the</strong> recipients had undergone amputations prior <strong>to</strong> <strong>the</strong>impact.4. This <strong>in</strong>tervention should require second medical op<strong>in</strong>ions and, when possible, <strong>in</strong>formedconsent of <strong>the</strong> patient. That was standard procedure for many, but not all<strong>the</strong> medical teams <strong>in</strong> <strong>Haiti</strong>.5. F<strong>in</strong>ally, rehabilitation specialists must be <strong>in</strong>volved early <strong>in</strong> treatment, ideally beforeamputation, and should educate <strong>the</strong> surgical team <strong>in</strong> pros<strong>the</strong>tic considerations.Mental health specialists must be <strong>in</strong>cluded <strong>to</strong> help <strong>the</strong> patient with communityre<strong>in</strong>tegration.Reconstructive surgeryThe surgical reconstruction of major <strong>in</strong>juries is only rarely addressed <strong>in</strong> <strong>the</strong> early<strong>response</strong> phase of <strong>earthquake</strong>s. In <strong>Haiti</strong>, this specialized service was made availablebut rema<strong>in</strong>ed <strong>in</strong> short supply despite <strong>the</strong> massive level of resources deployedfor this event. Ra<strong>the</strong>r remarkable is <strong>the</strong> contribution made <strong>to</strong> treat survivors withcraniofacial <strong>in</strong>juries who required complex and multiple procedures <strong>to</strong> achieveoptimal results. Thanks <strong>to</strong> <strong>the</strong> modern facilities on <strong>the</strong> USNS Comfort, some34 cases were improved, requir<strong>in</strong>g 93 craniofacial surgical procedures. Averagepatient hospitalization time was 17 days (rang<strong>in</strong>g from 5 <strong>to</strong> 38 days) (Ray etal. 2011). These surgeries were also performed at a Brazilian field hospital.Proximity <strong>to</strong> North America and French terri<strong>to</strong>ries, <strong>the</strong> presence of MINUSTAHfacilities, and <strong>the</strong> very rapid mobilization of some o<strong>the</strong>r military facilities were keyfac<strong>to</strong>rs lead<strong>in</strong>g <strong>to</strong> a quality of orthopedic and reconstructive care that cannot usuallybe expected <strong>in</strong> emergency <strong>response</strong>. It is a performance that has rarely been seen <strong>in</strong>disasters <strong>in</strong> more remote places.3232 32AFILMPho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>Post-operative care, referral, and foreign medical evacuations• In most disasters, <strong>the</strong>re is much more assistance for surgical care than for follow-upcare of surgical patients: <strong>to</strong>o many doc<strong>to</strong>rs and not enough nurses.• Referral of patients <strong>to</strong> different levels of care was h<strong>in</strong>dered by logistical constra<strong>in</strong>ts butabove all by a lack of <strong>in</strong>formation on specialty services and space available as well as<strong>the</strong> procedures and criteria for patients’ referral.74Post-operative care was an issue from <strong>the</strong> first few days of <strong>the</strong> <strong>response</strong> until late dur<strong>in</strong>g<strong>the</strong> recovery. With<strong>in</strong> a week, it was upgraded <strong>to</strong> one of <strong>the</strong> <strong>to</strong>p priorities. Not all foreignfield hospitals and medical teams addressed this issue <strong>in</strong> <strong>the</strong> same manner. One of <strong>the</strong>
THE LIFE-SAVING RESPONSE - Chapter 5most active field hospitals strictly applied <strong>the</strong> triage pr<strong>in</strong>ciple <strong>to</strong> take full advantage of<strong>the</strong>ir surgical resources. Turnover was maximized and patients were triaged <strong>to</strong> achieve<strong>the</strong> most efficient use of operat<strong>in</strong>g <strong>the</strong>aters. Patients who underwent surgery were discharged,on average, with<strong>in</strong> 39 hours of <strong>the</strong> procedure. 71 No provision was made forpost-operative care, which was not considered a function of this facility.Field hospitals concentrated on what <strong>the</strong>y do best and what <strong>the</strong>y are equipped for:provid<strong>in</strong>g immediate or delayed surgical care. Follow-up and time consum<strong>in</strong>g pos<strong>to</strong>perativecare were <strong>to</strong> be provided by less sophisticated teams or facilities. Unfortunately,those facilities were ei<strong>the</strong>r not available or overburdened. Although <strong>the</strong>reare no data on <strong>the</strong> impact of this situation on <strong>the</strong> outcome of patients, <strong>the</strong>re weredoubts about this approach under conditions prevail<strong>in</strong>g <strong>in</strong> <strong>Haiti</strong>: that is, no effectivecoord<strong>in</strong>ation among ac<strong>to</strong>rs, and local health authorities who were not <strong>in</strong> a position <strong>to</strong>assume strong leadership. Most components of <strong>the</strong> medical <strong>response</strong> system workedefficiently but <strong>in</strong>dependently of each o<strong>the</strong>r, ensur<strong>in</strong>g serious problems <strong>in</strong> <strong>the</strong> overallcha<strong>in</strong> for complete care. There were many examples of excellence, but <strong>the</strong>y were unl<strong>in</strong>ked,“bubbles” of excellence (see box).Post-operative care is a time-consum<strong>in</strong>g activity requir<strong>in</strong>g a significant number ofauxiliary personnel, nurses <strong>in</strong> particular. There is no lack of <strong>in</strong>terest and dedicationon <strong>the</strong> part of this profession, as was evident <strong>in</strong> <strong>Haiti</strong>. 72 Follow<strong>in</strong>g <strong>the</strong> <strong>earthquake</strong><strong>in</strong> Pakistan and <strong>the</strong> Indian Ocean tsunami <strong>the</strong>re was also an <strong>in</strong>sufficient number ofnurses compared <strong>to</strong> <strong>the</strong> number of doc<strong>to</strong>rs volunteer<strong>in</strong>g <strong>the</strong>ir services. There is oftena chronic shortage of nurses <strong>in</strong> donor countries and <strong>in</strong>stitutions provid<strong>in</strong>g volunteers.A successful partnership delivers post-operative careOne success s<strong>to</strong>ry was <strong>the</strong> partnership developed between a hospital <strong>in</strong> Jimaní (Hospital BuenSamaritano), an NGO <strong>in</strong> <strong>Haiti</strong> (Love a Child), and PAHO/WHO. It provides a model for plann<strong>in</strong>gfollow-up of patients.• From Day 3, <strong>the</strong> pressure on Dom<strong>in</strong>ican medical facilities clearly po<strong>in</strong>ted <strong>to</strong> <strong>the</strong> need for arrangementsfor post-surgery care, preferably <strong>in</strong> <strong>Haiti</strong>.• On Day 4, <strong>the</strong> Dom<strong>in</strong>ican M<strong>in</strong>istry of <strong>Health</strong> and PAHO/WHO approached NGOs established<strong>in</strong> Fond Parisien, on <strong>the</strong> <strong>Haiti</strong>an side of <strong>the</strong> border, about develop<strong>in</strong>g a facility for dischargedsurgical patients and <strong>the</strong>ir families. A school designed for 400 students and managed byLove a Child was identified as a first-l<strong>in</strong>e facility for post-operative treatment of patientsdischarged from local and Dom<strong>in</strong>ican facilities.• Over <strong>the</strong> follow<strong>in</strong>g days, equipment, mattresses, and o<strong>the</strong>r supplies were provided by <strong>the</strong>Dom<strong>in</strong>ican M<strong>in</strong>istry of <strong>Health</strong> and PAHO/WHO.• On Day 8, <strong>the</strong> facility received <strong>the</strong> first 65 patients.• On Day 9, <strong>the</strong> Hospital Eau de Vie <strong>in</strong> Fond Parisien was evaluated and streng<strong>the</strong>ned <strong>to</strong> serveas a back-up facility, should <strong>the</strong> 400 beds of <strong>the</strong> converted school be <strong>in</strong>sufficient.To transform an idea <strong>in</strong><strong>to</strong> a concrete achievement <strong>in</strong> <strong>the</strong> space of one week is a noteworthyaccomplishment, made possible by <strong>in</strong>formal partnership between a government, an NGO, anda UN organization, unh<strong>in</strong>dered by bureaucratic obstacles.71 Government of Israel, <strong>2010</strong> (unpublished).72 Of <strong>the</strong> 280 articles registered <strong>in</strong> <strong>the</strong> U.S. National Library of Medic<strong>in</strong>e’s Medl<strong>in</strong>e database (searched by <strong>the</strong> author us<strong>in</strong>g <strong>the</strong>keywords “<strong>Haiti</strong> <strong>earthquake</strong>” on 7 August 2011), 43 were ei<strong>the</strong>r on nurs<strong>in</strong>g support <strong>to</strong> <strong>Haiti</strong> or were published <strong>in</strong> a nurs<strong>in</strong>gjournal.75
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Patient flow: evacuation, referral, post-operative carePatient referralPost-operative care is only one aspect of <strong>the</strong> broader issue of referral of patients betweenfacilities.The flow of patients between levels of care was particularly problematic <strong>in</strong> <strong>Haiti</strong>. Problemsranged from lack of transportation <strong>to</strong> lack of knowledge about options.Medical teams provid<strong>in</strong>g primary or secondary care often did not know of <strong>the</strong> potentialcapacity of more sophisticated facilities. Extraord<strong>in</strong>ary work pressure considerably limited<strong>the</strong> communication between medical teams and hospitals. Few could spare staff <strong>to</strong>participate <strong>in</strong> <strong>the</strong> numerous coord<strong>in</strong>ation meet<strong>in</strong>gs. The underutilization of <strong>the</strong> dialysiscapacity mentioned earlier is only one example.A testimony from a trauma expert is reveal<strong>in</strong>g:“The most challeng<strong>in</strong>g aspect was a clear plan conveyed <strong>to</strong> all <strong>the</strong> responders/groups,as <strong>to</strong> who was able <strong>to</strong> manage what, and how <strong>to</strong> get <strong>the</strong>patients referred and transferred. A good example is sp<strong>in</strong>al cord <strong>in</strong>jury. Itwas my experience that at many sites where SCI patients were identified(often ly<strong>in</strong>g on mattresses <strong>in</strong> <strong>the</strong> street/park<strong>in</strong>g lots, or even on sheets of76
THE LIFE-SAVING RESPONSE - Chapter 5plywood), <strong>the</strong> doc<strong>to</strong>rs/nurses car<strong>in</strong>g for <strong>the</strong>m did not know where <strong>to</strong> send<strong>the</strong>m. Hav<strong>in</strong>g been at many of <strong>the</strong> sites, I knew which centers were accept<strong>in</strong>gSCI patients, and was able <strong>to</strong> assist <strong>in</strong> triage, referral and transpor<strong>to</strong>rganization when I ‘found’ SCI patients at o<strong>the</strong>r sites. This was avery one-off type of approach, and even at centers accept<strong>in</strong>g SCI patients,if <strong>the</strong> ‘wrong’ person was at triage when <strong>the</strong> SCI patient arrived, <strong>the</strong>ycould have been turned away.” 73It was not until four weeks after <strong>the</strong> impact that a one-page list<strong>in</strong>g of resources for referralwas made available. This list offered names and sometimes addresses of specializedservices such as burn treatment, pediatric surgery, dialysis, neurosurgery, ophthalmology,cranio-facial surgery, medical evacuations, or simply obstetrics, a need often overlooked <strong>in</strong>a trauma-focused environment. In future disasters, dissem<strong>in</strong>at<strong>in</strong>g a list<strong>in</strong>g of referral facilitiesshould be one of <strong>the</strong> first priorities.Problems were not limited <strong>to</strong> referral from lower level <strong>to</strong> tertiary level but also <strong>in</strong> <strong>the</strong>reverse. The USNS Comfort hospital ship found it difficult <strong>to</strong> identify receiv<strong>in</strong>g <strong>in</strong>stitutionsfor <strong>the</strong>ir patients requir<strong>in</strong>g less acute but longer term follow-up care.73 Personal communication with Dr. Colleen O’Connell, MD, PMR, 31 <strong>January</strong> 2011.Flow of patients/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>Pho<strong>to</strong>s: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>77
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Foreign medical evacuationsEvacuation abroad should be an option of last resort <strong>to</strong> be adopted cautiously and understrict oversight of <strong>the</strong> national health services. Preference should be given <strong>in</strong>stead<strong>to</strong> streng<strong>the</strong>n<strong>in</strong>g <strong>the</strong> capacity of local counterparts.Unlike <strong>the</strong> disasters <strong>in</strong> Indonesia, Sri Lanka, Pakistan, and Iran (Bam <strong>earthquake</strong>), <strong>the</strong>rewas no back-up facility <strong>in</strong>side <strong>Haiti</strong> where patients could be evacuated. Evacuat<strong>in</strong>g patients<strong>in</strong><strong>to</strong> foreign facilities is entirely dist<strong>in</strong>ct from redistribut<strong>in</strong>g patients with<strong>in</strong> nationalhealth services as was done massively <strong>in</strong> Iran (15,000 evacuated <strong>in</strong> <strong>the</strong> matter of acouple of days) 74 and <strong>in</strong> Sri Lanka. 75Transfer of <strong>Haiti</strong>an patients <strong>to</strong> foreign facilities (mostly <strong>in</strong> <strong>the</strong> Dom<strong>in</strong>ican Republic,United States, and French terri<strong>to</strong>ries) was done extensively <strong>in</strong> <strong>the</strong> first few days. Quantifieddata, as for many o<strong>the</strong>r aspects of <strong>the</strong> relief operations, are not easily available.Recipient countries and hospitals often used medical evacuation as a back-up alternativeor support for <strong>the</strong>ir medical facilities <strong>in</strong> <strong>the</strong> field. Criteria for selection, if articulatedat all, were not broadly publicized or known.Selective evacuations of sp<strong>in</strong>al cord <strong>in</strong>jury cases <strong>to</strong> foreign countries <strong>to</strong>ok placeearly after <strong>the</strong> impact, but <strong>the</strong>y were soon curtailed (<strong>in</strong> part due <strong>to</strong> <strong>the</strong> realizationthat those patients would be occupy<strong>in</strong>g expensive beds for an open-ended periodof time). Return<strong>in</strong>g those chronic patients <strong>to</strong> <strong>Haiti</strong> where a suitable receiv<strong>in</strong>gfacility could not be found was ethically impossible. Economic considerations,especially for <strong>in</strong>stitutions car<strong>in</strong>g for patients requir<strong>in</strong>g expensive, long-termcare, should be considered at an early stage. 76In several <strong>in</strong>stances, relatives did not have <strong>in</strong>formation on <strong>the</strong> whereaboutsof <strong>in</strong>jured family members who were evacuated. There were also <strong>the</strong> issuesof immigration and subsistence for <strong>the</strong> patient’s family <strong>in</strong> <strong>the</strong> host country.Foreign medical evacuation of <strong>the</strong> <strong>in</strong>jured is an expression of solidarity with<strong>the</strong> affected population but it often causes more problems than anticipated.As experienced <strong>in</strong> receiv<strong>in</strong>g countries/terri<strong>to</strong>ries such as Mart<strong>in</strong>ique, accept<strong>in</strong>ga patient requir<strong>in</strong>g long-term care is <strong>the</strong> easiest part, decid<strong>in</strong>g <strong>to</strong> returnhim/her raises ethical issues.National authorities of <strong>the</strong> affected country or an agency <strong>the</strong>y designate shouldplay a moni<strong>to</strong>r<strong>in</strong>g/track<strong>in</strong>g role, if not an approval role, <strong>in</strong> this process. It isan approach that should not be left entirely <strong>to</strong> <strong>the</strong> <strong>in</strong>itiative and criteria of foreignteams. Recipient <strong>in</strong>stitutions should rema<strong>in</strong> accountable <strong>to</strong> both families and healthauthorities of <strong>the</strong> affected countries and be unambiguous regard<strong>in</strong>g <strong>the</strong> duration of<strong>the</strong>ir commitment.41 FILM32 32APho<strong>to</strong>s: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>74 Almost all <strong>in</strong>jured <strong>in</strong> <strong>the</strong> Bam <strong>earthquake</strong> were evacuated before <strong>the</strong> first foreign field hospitals arrived.75 All nationals <strong>in</strong>jured <strong>in</strong> <strong>the</strong> tsunami were treated and referred <strong>to</strong> third level care <strong>in</strong> departmental facilities. None needed <strong>to</strong>be evacuated <strong>to</strong> <strong>the</strong> 2,000-bed General Hospital <strong>in</strong> <strong>the</strong> capital city, Colombo.76 In <strong>the</strong> U.S., <strong>the</strong> Government concluded a formal agreement with receiv<strong>in</strong>g <strong>in</strong>stitutions <strong>to</strong> reimburse 110% of Medicarerates for approved <strong>Haiti</strong>an patients.78
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>fear that uncontrollable epidemics were <strong>the</strong> unavoidable result of decay<strong>in</strong>g bodies.Mass burials, cremation, or o<strong>the</strong>r “dis<strong>in</strong>fection” techniques are not justified froma health po<strong>in</strong>t of view. It is remarkable that, after an <strong>earthquake</strong> produc<strong>in</strong>g such alarge number of bodies left unattended for days, no similar unfounded announcementwas made locally by senior health or humanitarian officials. This should becredited <strong>to</strong> <strong>the</strong> early formal announcements by WHO that dead bodies are not asource of large epidemics. Never<strong>the</strong>less, this myth was still proliferated <strong>in</strong> mass media<strong>in</strong> Europe and Lat<strong>in</strong> America.<strong>Haiti</strong>ans hold <strong>the</strong>ir deceased family members <strong>in</strong> high regard and perform elaborate,costly, and extended funeral rituals <strong>to</strong> assure <strong>the</strong> goodwill of <strong>the</strong> deceased. Deceasedfamily members are still considered <strong>to</strong> be part of <strong>the</strong> family. As stated <strong>in</strong> <strong>the</strong> WHOpublication Culture and Mental <strong>Health</strong> <strong>in</strong> <strong>Haiti</strong> (<strong>2010</strong>a, 20), “The issue of proper deathrites and burial is particularly important <strong>in</strong> <strong>the</strong> wake of <strong>the</strong> <strong>earthquake</strong>. Many peoplehave not had <strong>the</strong> opportunity <strong>to</strong> f<strong>in</strong>d and bury <strong>the</strong>ir lost loved ones or had <strong>to</strong> abandon<strong>the</strong>m, or see <strong>the</strong>m buried <strong>in</strong> a mass grave with no ceremonies. As a result, <strong>the</strong>re may bean <strong>in</strong>crease <strong>in</strong> ambiguity and uncerta<strong>in</strong>ty over <strong>the</strong> fate of <strong>the</strong> dead…”.PAHO/WHO guidel<strong>in</strong>es (2004) recommend that bodies be s<strong>to</strong>red, identified andreturned <strong>to</strong> <strong>the</strong> family <strong>to</strong> allow for griev<strong>in</strong>g and ritual burial. Given <strong>the</strong> magnitude of<strong>the</strong> losses and <strong>the</strong> urgency of o<strong>the</strong>r life sav<strong>in</strong>g measures, this was not a practical option<strong>in</strong> <strong>Haiti</strong>. Nor was it follow<strong>in</strong>g <strong>the</strong> disasters <strong>in</strong> Pakistan, Indonesia, and Sri Lanka.Thailand, however, was an exception. 77The morgue <strong>in</strong> <strong>the</strong> University Hospital which was designed <strong>to</strong> handle around 30 cadaversrapidly exceeded its capacity and was overwhelmed, accord<strong>in</strong>g <strong>to</strong> <strong>the</strong> report ofits Direc<strong>to</strong>r, “by up <strong>to</strong> 10,000 bodies”. At <strong>the</strong> same time, MINUSTAH reported onDay 3 that it had collected and buried more than 13,000 bodies <strong>in</strong> mass graves. Howaccurate those figures are consider<strong>in</strong>g <strong>the</strong> chaotic and emotional conditions rema<strong>in</strong>s<strong>to</strong> be seen. They are never<strong>the</strong>less illustrative of <strong>the</strong> overwhelm<strong>in</strong>g task that lay ahead.Municipal and state authorities mobilized a fleet of private trucks and worked day andnight fill<strong>in</strong>g improvised mass burial sites outside <strong>the</strong> city.No statistics and sparse documentary evidence (pho<strong>to</strong>s or documents) were collected<strong>to</strong> allow for delayed identification of <strong>the</strong> rema<strong>in</strong>s. The seem<strong>in</strong>g acceptance of thishasty process by <strong>Haiti</strong>’s deeply religious people was remarkable and reflects <strong>the</strong> senseof shock and <strong>the</strong> population’s focus on <strong>the</strong> survival challenges ahead. Long-term psychologicalimpacts are unknown.77 In Thailand, almost 5,400 bodies were recovered after <strong>the</strong> tsunami. Special efforts, last<strong>in</strong>g over one year, were made <strong>to</strong>identify <strong>the</strong> deceased, <strong>in</strong>clud<strong>in</strong>g by pho<strong>to</strong>s, f<strong>in</strong>ger pr<strong>in</strong>t<strong>in</strong>g, and DNA analysis. One fac<strong>to</strong>r <strong>in</strong>fluenc<strong>in</strong>g <strong>the</strong>se efforts was <strong>the</strong>presence of almost 2,000 foreigners among <strong>the</strong> victims (Sribanditmongkol et al. 2005).80
Chapter6Beyondtrauma careThe delayed <strong>response</strong> (up <strong>to</strong> 3 months)Dur<strong>in</strong>g <strong>the</strong> first two weeks after <strong>the</strong> <strong>earthquake</strong>, <strong>the</strong>re were many more health relatedactivities than just rescu<strong>in</strong>g trapped victims and provid<strong>in</strong>g trauma care. Water andsanitation, food and shelter, and access <strong>to</strong> primary health care were among <strong>the</strong> manyneeds of <strong>the</strong> affected population. They became <strong>the</strong> <strong>to</strong>p priorities of humanitarianagencies once <strong>the</strong> life-sav<strong>in</strong>g <strong>in</strong>terventions were completed, <strong>to</strong>ge<strong>the</strong>r with surveillanceof communicable diseases, rehabilitation, and many-cross cutt<strong>in</strong>g issues.This publication cannot review or analyze <strong>in</strong> detail <strong>the</strong> many challenges faced andsolutions found for those broad social issues. This chapter addresses selected <strong>to</strong>pics ofparticular public health <strong>in</strong>terest for future mass-scale disasters.Cl<strong>in</strong>ics and mobile <strong>in</strong>tervention teams <strong>in</strong> settlementsThe terms “cl<strong>in</strong>ics” and “mobile teams” covered a large range of services: from <strong>the</strong> wellestablishedand fully staffed temporary or fixed facility <strong>in</strong> a large camp <strong>to</strong> <strong>the</strong> smalltent where a nurse or a doc<strong>to</strong>r occasionally provided m<strong>in</strong>imal care <strong>to</strong> patients.The M<strong>in</strong>istry of <strong>Health</strong> of <strong>Haiti</strong>, itself recover<strong>in</strong>g from <strong>the</strong> impact, realized that it had<strong>in</strong> fact very little <strong>in</strong>fluence on <strong>the</strong> immediate trauma care process, which, as shown <strong>in</strong>Chapter 5, had its own dynamics and rules. Very early on, <strong>the</strong> M<strong>in</strong>istry centered its81
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>attention on <strong>the</strong> establishment of “mobile cl<strong>in</strong>ics” <strong>to</strong> provide primary health care <strong>to</strong> <strong>the</strong>displaced populations or <strong>to</strong> provide a temporary substitute for <strong>the</strong> facilities destroyedby <strong>the</strong> <strong>earthquake</strong>. A chronology of <strong>the</strong> M<strong>in</strong>istry’s statements regard<strong>in</strong>g <strong>the</strong> establishmen<strong>to</strong>f primary health care cl<strong>in</strong>ics after <strong>the</strong> <strong>earthquake</strong> is <strong>in</strong>cluded <strong>in</strong> <strong>the</strong> Box.M<strong>in</strong>istry of <strong>Health</strong> targets for primary health care follow<strong>in</strong>g <strong>the</strong> <strong>earthquake</strong>With<strong>in</strong> a few days of <strong>the</strong> <strong>earthquake</strong>, <strong>the</strong> President of <strong>Haiti</strong> established a National Commissionfor <strong>the</strong> Management of <strong>the</strong> Crisis, which <strong>in</strong>cluded <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong>. The M<strong>in</strong>istry’s nationalpriorities <strong>in</strong>cluded “establish<strong>in</strong>g mobile cl<strong>in</strong>ics <strong>in</strong> all <strong>the</strong> spontaneous camps that have beencreated, ensur<strong>in</strong>g obstetric care and delivery kits as close <strong>to</strong> <strong>the</strong> population concentrations aspossible and ensur<strong>in</strong>g that <strong>the</strong> delivery of health care services is properly coord<strong>in</strong>ated.”• On 21 <strong>January</strong> (Day 10), <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong> fur<strong>the</strong>r asserted its leadership and distributedguidel<strong>in</strong>es on what should be available at primary and secondary level cl<strong>in</strong>ics. NGOsand organizations were asked <strong>to</strong> provide <strong>the</strong>ir comments on <strong>the</strong> basic package proposedby <strong>the</strong> M<strong>in</strong>istry. A special work<strong>in</strong>g group on primary care/mobile cl<strong>in</strong>ics was meet<strong>in</strong>g twicea week <strong>in</strong> <strong>the</strong> M<strong>in</strong>istry.• On 25 <strong>January</strong> (Day 14), <strong>the</strong> M<strong>in</strong>istry requested partners <strong>to</strong> focus <strong>the</strong>ir attention on primaryhealth care, health centers, and hospitals. The <strong>in</strong>itial life-sav<strong>in</strong>g phase was end<strong>in</strong>g. All healthpartners <strong>in</strong> <strong>Haiti</strong> supported this strategy, at least <strong>in</strong> pr<strong>in</strong>ciple. In practice, <strong>the</strong> decision <strong>to</strong> locatethose services on <strong>the</strong> premises of exist<strong>in</strong>g health facilities was ignored by many NGOs.• On 2 February (Day 22), <strong>the</strong> M<strong>in</strong>istry clarified its vision of post-<strong>earthquake</strong> care, def<strong>in</strong><strong>in</strong>g <strong>the</strong>services and human resources required at <strong>the</strong> three levels of care (see Table 6.1).• On 8 February, <strong>the</strong> <strong>Health</strong> Cluster reported: “mobile cl<strong>in</strong>ics are be<strong>in</strong>g deployed <strong>in</strong> 250 spontaneoussettlements as identified by <strong>the</strong> Government.”Source: <strong>Health</strong> Cluster Bullet<strong>in</strong>s, <strong>January</strong>–February 2011.The focus on primary health care was not limited <strong>to</strong> <strong>the</strong> area directly affected by <strong>the</strong><strong>earthquake</strong> but also addressed <strong>the</strong> needs of <strong>the</strong> many people who were displaced <strong>in</strong><strong>to</strong>o<strong>the</strong>r departments. On 25 <strong>January</strong> <strong>the</strong> M<strong>in</strong>istry made this statement: “health facilities<strong>in</strong> <strong>the</strong> departments outside of <strong>the</strong> capital are overwhelmed due <strong>to</strong> <strong>in</strong>ternally displacedpersons and <strong>the</strong>y do not have <strong>the</strong> capacity <strong>to</strong> treat <strong>the</strong> number of people arriv<strong>in</strong>g”. Thenext day, <strong>the</strong> M<strong>in</strong>istry reiterated its message <strong>to</strong> partners: “encourag<strong>in</strong>g <strong>Health</strong> Clusterpartners <strong>to</strong> move outside <strong>the</strong> capital area <strong>to</strong> provide needed services as well as mid- andlong-term commitments for health activities” (<strong>Health</strong> Cluster Bullet<strong>in</strong> No. 7). Thiswas an important contribution <strong>to</strong> <strong>the</strong> l<strong>in</strong>kage of relief with development.There was no shortage of plans and strategic documents <strong>in</strong> <strong>the</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong>,but <strong>the</strong>y were not always followed by action. Was this concept of mobile cl<strong>in</strong>icsimplemented and put <strong>in</strong><strong>to</strong> practice?The M<strong>in</strong>istry def<strong>in</strong>ed <strong>the</strong> m<strong>in</strong>imum package of services it considered necessary at<strong>the</strong> primary care level (see Table 6.1). To determ<strong>in</strong>e <strong>the</strong> effectiveness of <strong>the</strong> mobilecl<strong>in</strong>ic strategy, PAHO/WHO and <strong>the</strong> International Rescue Committee (IRC) commissionedManagement Science for <strong>Health</strong> (MSH) <strong>in</strong> March <strong>2010</strong> <strong>to</strong> identify siteswhere <strong>the</strong>re was still a need for mobile cl<strong>in</strong>ics.82
BEYOND TRAUMA CARE - Chapter 6Table 6.1 M<strong>in</strong>imum package of services for first level cl<strong>in</strong>ics(mobile or fixed)Components of care• Treatment of m<strong>in</strong>or wounds• Prenatal care, normal deliveries, and postpartumcare• Contraception• Treatment of childhood illness (diarrheaand dehydration, fever and nutritionalsurveillance)• Vacc<strong>in</strong>ation program• Treatment of malnutrition• Treatment for acute and chronic illness (e.g.,asthma, hypertension)• Reception and immediate transfer of rapevictims; record cases with allegations ofviolence• Regular treatment for HIV and distributionof ARVsHuman resourcesA multidiscipl<strong>in</strong>ary team, <strong>in</strong>clud<strong>in</strong>g:• Medical doc<strong>to</strong>r (optional)• Nurses• Students complet<strong>in</strong>g tra<strong>in</strong><strong>in</strong>g <strong>in</strong> <strong>the</strong> healthsciences• Social worker• Psychologist/Social motiva<strong>to</strong>rNote: Translated and adapted from Provision des services dans les camps/zones de regroupement de la population (MSPP<strong>2010</strong>e).Pho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>32FILM32 32AA survey of 206 of <strong>the</strong> largest temporary settlements (out of a list of 400 campsprovided by IOM) was carried out from 18 <strong>to</strong> 29 March <strong>to</strong> determ<strong>in</strong>e <strong>the</strong> exist<strong>in</strong>gcoverage and delivery of a m<strong>in</strong>imum package of services (Table 6.2). However, itbecame clear that none of <strong>the</strong> cl<strong>in</strong>ics (fixed or mobile) serv<strong>in</strong>g <strong>the</strong> camps was offer<strong>in</strong>g<strong>the</strong> full set of services. For <strong>the</strong> purpose of <strong>the</strong> survey, <strong>the</strong> m<strong>in</strong>imum packagewas redef<strong>in</strong>ed <strong>to</strong> <strong>in</strong>clude six services: (1) general consultation, (2) prenatalconsultation, (3) pediatric consultation, (4) neonatal care, (5) family plann<strong>in</strong>g,(6) vacc<strong>in</strong>ation.The survey results were mixed. Out of <strong>the</strong> 206 settlements host<strong>in</strong>g 163,000families, only 72 had local access <strong>to</strong> health care, i.e., 35% coverage. Of <strong>the</strong> 79health posts, 46% of <strong>the</strong> structures were mobile cl<strong>in</strong>ics. 78 Only 10% offered <strong>the</strong> fullm<strong>in</strong>imum package (for all six services as redef<strong>in</strong>ed for <strong>the</strong> survey). The distribution ofservices is shown <strong>in</strong> Table 6.2.78 Some of <strong>the</strong> larger settlements had two health centers/cl<strong>in</strong>ics.83
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Table 6.2 Primary health services offered at 79 health postssurveyed <strong>in</strong> <strong>Haiti</strong>, March <strong>2010</strong>Services provided Po<strong>in</strong>t of health service delivery (%)General consultations 96Pediatric consultations 94Prenatal consultations 87Neonatal care 71Immunizations 43Family plann<strong>in</strong>g 39Source: Management Science for <strong>Health</strong> (MSH) (<strong>2010</strong>).Official targets may not have been reached, but <strong>the</strong>re is a consensus that <strong>the</strong> level,quality, and proximity of primary health care offered were generally superior <strong>to</strong> thatavailable <strong>to</strong> most of <strong>the</strong> affected population prior <strong>to</strong> <strong>the</strong> disaster. There were exceptions:Antenatal care was mostly done without any lab test<strong>in</strong>g; 79 <strong>to</strong>o many cl<strong>in</strong>icsused donated drugs not <strong>in</strong> <strong>the</strong> essential drug list; and foreign health workers at cl<strong>in</strong>icsworked with transla<strong>to</strong>rs and did not properly understand <strong>the</strong> compla<strong>in</strong>ts of <strong>the</strong> patients.Much more important, mobile cl<strong>in</strong>ics were often not l<strong>in</strong>ked <strong>to</strong> exist<strong>in</strong>g healthfacilities. This situation hampered <strong>the</strong> ability <strong>to</strong> rebuild <strong>the</strong> health system and <strong>to</strong> providecare <strong>to</strong> people closer <strong>to</strong> <strong>the</strong>ir communities.How susta<strong>in</strong>ed this effort was is ano<strong>the</strong>r issue. A survey commissioned by <strong>the</strong> M<strong>in</strong>istryof <strong>Health</strong> <strong>in</strong> July <strong>2010</strong> found that out of 286 <strong>in</strong>stitutions/mobile cl<strong>in</strong>ics consideredfor <strong>the</strong> survey sampl<strong>in</strong>g, only 171 could be found or were operational at <strong>the</strong> time fielddata were collected (MSPP <strong>2010</strong>b).Free care policyProvision of care and medic<strong>in</strong>es was free of charge for <strong>the</strong> duration of <strong>the</strong> emergency. 80This was an important departure from <strong>the</strong> government policy of fee-based care, whichis promoted by <strong>in</strong>ternational f<strong>in</strong>ancial <strong>in</strong>stitutions. This policy of free care has beenextended de fac<strong>to</strong> for several months, although no official policy document was issuedby <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong>.Promulgat<strong>in</strong>g a free care policy had its down side. The fees were used by public healthfacilities <strong>to</strong> recruit additional staff and subsidize some of <strong>the</strong>ir services. Without thiscompensat<strong>in</strong>g mechanism, <strong>the</strong> free care policy was detrimental <strong>to</strong> government facilitiesthat did not have free drugs and fund<strong>in</strong>g for basic supplies and services (clean<strong>in</strong>gmaterial, paper, Internet and telephone fees). The power genera<strong>to</strong>rs <strong>in</strong> facilities werealso often paid for with <strong>the</strong>se fees. This worsened <strong>the</strong> situation of public facilities.Communal health offices that received 5% of benefits were <strong>in</strong> a difficult position.The long-term implication of free basic services is addressed later <strong>in</strong> <strong>the</strong> section on <strong>the</strong>l<strong>in</strong>kage between relief, rehabilitation, and development (LRRD).8479 Before <strong>the</strong> <strong>earthquake</strong>, hemoglob<strong>in</strong> and ur<strong>in</strong>e tests, and tests for HIV and syphilis were free of charge <strong>in</strong> many dispensaries.80 Interviews suggested that <strong>the</strong> free availability of medic<strong>in</strong>es did not have an economic effect on <strong>the</strong> private pharmacies, manyof which were impacted directly by <strong>the</strong> <strong>earthquake</strong>. Most of <strong>the</strong> <strong>in</strong>come of private pharmacies comes from <strong>the</strong> wealthiersegment of <strong>the</strong> population. Some even believe that free access <strong>to</strong> essential drugs for <strong>the</strong> poorest sec<strong>to</strong>r of <strong>the</strong> population maycreate awareness of <strong>the</strong> value of modern drugs and, <strong>the</strong>refore, a new market.
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>3. The donations from <strong>the</strong> public or donor agencies must be appropriate for localconditions. Electric wheelchairs, of great assistance <strong>in</strong> developed countries, are unsuitablefor Port-au-Pr<strong>in</strong>ce where many urban roads require four-wheel drive <strong>in</strong>normal times and are unfavorable for pedestrians, especially for <strong>the</strong> disabled.4. International medical and allied professionals need <strong>to</strong> be prepared <strong>to</strong> provide cont<strong>in</strong>uityand consistency and rapidly educate local staff (especially <strong>in</strong> <strong>the</strong> newly recognizedspecialty of sp<strong>in</strong>al cord <strong>in</strong>jury). It is also imperative that educa<strong>to</strong>rs speak<strong>the</strong> local language <strong>to</strong> reduce mis<strong>in</strong>terpretation and mis<strong>in</strong>formation.Communicable diseases control<strong>Health</strong> officials, humanitarian agencies, and mass media used <strong>to</strong> overemphasize <strong>the</strong>risk of outbreaks follow<strong>in</strong>g sudden-onset disasters. Massive outbreaks predicted <strong>in</strong> <strong>the</strong>aftermath of past <strong>earthquake</strong>s have failed <strong>to</strong> materialize <strong>in</strong> <strong>the</strong> last 40 years. Declarationson <strong>the</strong> <strong>in</strong>evitability of devastat<strong>in</strong>g epidemics often result from ignorance of pasthis<strong>to</strong>ry, but <strong>the</strong>re are cases when calculated mis<strong>in</strong>formation has been used <strong>to</strong> mobilizeresources for health activities (this occurred <strong>in</strong> <strong>the</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> tsunami <strong>in</strong> 2004).Unnecessarily alarm<strong>in</strong>g an already traumatized public is counterproductive, and whendeliberate, it is unethical.Over <strong>the</strong> last two decades, PAHO/WHO and o<strong>the</strong>r agencies have conducted an educationalcampaign <strong>to</strong> demystify <strong>the</strong> <strong>to</strong>pic of disease outbreaks after disaster and <strong>to</strong>stimulate a more objective and balanced approach <strong>to</strong> prevent<strong>in</strong>g <strong>the</strong>m. On one side,epidemics rema<strong>in</strong> a strong possibility <strong>in</strong> <strong>the</strong> absence of any preventive measures. Riskfac<strong>to</strong>rs <strong>in</strong>clude displacement of populations, contam<strong>in</strong>ation of water, overcrowd<strong>in</strong>g <strong>in</strong>settlements, and deteriorat<strong>in</strong>g sanitation. Dead bodies are not one of those fac<strong>to</strong>rs (Watsonet al. 2007). On <strong>the</strong> o<strong>the</strong>r side, public health measures are implemented more effectivelyand efficiently because both <strong>the</strong> public and authorities have a deep-seated fearof epidemics even when <strong>the</strong>se fears are not exacerbated by humanitarian ac<strong>to</strong>rs.Emergency surveillance and early warn<strong>in</strong>g systems are <strong>the</strong> first l<strong>in</strong>e of defense aga<strong>in</strong>stcommunicable diseases and must be carried out flexibly and rapidly after <strong>the</strong> impact.Emergency post-<strong>earthquake</strong> surveillanceAn emergency surveillance system must:• Start with<strong>in</strong> <strong>the</strong> first few days of <strong>the</strong> event;• Include sent<strong>in</strong>el stations among medical humanitarian ac<strong>to</strong>rs;• Be simple, by focus<strong>in</strong>g on a very limited number of <strong>the</strong> most critical conditions(syndromes).A surveillance system should be complemented by an alert system where all partnerscan directly report abnormal health situations.No major outbreak was detected after <strong>the</strong> <strong>earthquake</strong>s <strong>in</strong> <strong>Haiti</strong> and Pakistan or after<strong>the</strong> tsunami <strong>in</strong> Indonesia and Sri Lanka.86
BEYOND TRAUMA CARE - Chapter 6Before <strong>the</strong> 12 <strong>January</strong> <strong>earthquake</strong>, <strong>the</strong> surveillance system <strong>in</strong> <strong>Haiti</strong> focused on sixnotifiable diseases: acute hemorrhagic fever, suspected men<strong>in</strong>gococcal men<strong>in</strong>gitis, suspecteddiph<strong>the</strong>ria, suspected acute flaccid paralysis, suspected measles, and bites byanimals suspected of hav<strong>in</strong>g rabies.An improved system was required for <strong>the</strong> emergency. It had <strong>to</strong> be better adapted <strong>to</strong> <strong>the</strong>needs and concerns <strong>in</strong> disaster situations, more flexible, and capable of be<strong>in</strong>g rapidlyanalyzed and dissem<strong>in</strong>ated.It <strong>to</strong>ok 13 days <strong>to</strong> launch this system: Interviews with PAHO/WHO epidemiologistspresent dur<strong>in</strong>g <strong>the</strong> impact permit a reconstruction of <strong>the</strong> steps for establish<strong>in</strong>g anemergency surveillance system (Table 6.3). 84Table 6.3 Chronology of actions establish<strong>in</strong>g emergencysurveillance system, <strong>January</strong> <strong>2010</strong>Day of emergencyDay 1, 12 <strong>January</strong>(6PM)Day 2Day 3Day 4Day 5Day 7Day 12Day 13ActionsEvacuation of PAHO/WHO offices and recovery of key materials andcommunication equipment.No <strong>in</strong>formation; confirm welfare of staff (account<strong>in</strong>g for staff, food, accommodation).Decision <strong>to</strong> move PAHO office <strong>to</strong> PROMESS warehouse.All staff (national and <strong>in</strong>ternational) accounted for (no casualties).Attempted visit <strong>to</strong> <strong>the</strong> National Labora<strong>to</strong>ry (Epidemiology headquarters)– all roads blocked.Contact with public health authorities at PROMESS.Visit <strong>to</strong> <strong>the</strong> National Labora<strong>to</strong>ry; found <strong>to</strong> be <strong>in</strong>tact but no personnelpresent.National Labora<strong>to</strong>ry premises occupied by two foreign field hospitals.Meet<strong>in</strong>g with National Labora<strong>to</strong>ry Direc<strong>to</strong>r and U.S. Centers for DiseaseControl and Prevention (CDC).Formal start of an ad-hoc work<strong>in</strong>g group <strong>to</strong> plan a surveillance system,<strong>in</strong>clud<strong>in</strong>g M<strong>in</strong>istry of <strong>Health</strong>, PAHO/WHO, CDC, MSF (Epicentre), Cuban,Ch<strong>in</strong>ese, and Taiwanese epidemiologists, etc.Formal launch of National Surveillance System.Set up surveillance work<strong>in</strong>g group with<strong>in</strong> <strong>the</strong> <strong>Health</strong> Cluster structure(40 participants <strong>in</strong> daily meet<strong>in</strong>gs).An ad-hoc <strong>in</strong>ternational work<strong>in</strong>g group agreed on <strong>the</strong> 25 conditions for which newoccurrences must be reported nationwide (see Table 6.4). It is now recognized that<strong>the</strong> number was <strong>to</strong>o high and <strong>in</strong>cluded conditions of <strong>in</strong>creas<strong>in</strong>gly marg<strong>in</strong>al relevanceas time elapsed (for <strong>in</strong>stance, new amputations or crush syndromes). This isa common result of decisions taken by consensus <strong>in</strong> committees.84 The Dom<strong>in</strong>ican Republic established its own surveillance and early warn<strong>in</strong>g system <strong>in</strong> Jimaní and neighbor<strong>in</strong>g prov<strong>in</strong>ces.With<strong>in</strong> a few days, <strong>the</strong> system was <strong>in</strong> place. The Dom<strong>in</strong>ican Republic benefited from a more manageable localized emergencyand <strong>the</strong> full back<strong>in</strong>g of its government, which was unaffected by <strong>the</strong> <strong>earthquake</strong>.87
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Countrywide, 51 sent<strong>in</strong>el stations were selected from <strong>the</strong> 94 pre-exist<strong>in</strong>g health facilitiesaffiliated with <strong>the</strong> U.S. President’s Emergency Plan for AIDS Relief (PEPFAR).The selected sites were due <strong>to</strong> report daily by e-mail or telephone on new occurrencesof <strong>the</strong> 25 specified reportable conditions. The level of report<strong>in</strong>g was variable but generallywas low. Daily report<strong>in</strong>g was <strong>to</strong>o demand<strong>in</strong>g even for facilities not primarily<strong>in</strong>volved <strong>in</strong> humanitarian <strong>response</strong>.Table 6.4 Post-<strong>earthquake</strong> reportable conditions; <strong>Haiti</strong>Infectious diseases• Fever of unknown cause• Suspected malaria• Suspected dengue fever• Acute hemorrhagic feversyndrome• Acute watery diarrhea• Acute bloody diarrhea• Suspected typhoid fever• Acute respira<strong>to</strong>ry <strong>in</strong>fections• Suspected measles (feverand rash)• Tuberculosis• TetanusNon-<strong>in</strong>fectious diseasesNon-traumaTrauma related• Acute malnutrition• Trauma• Sk<strong>in</strong> disorder• Fracture• Renal failure• Cerebral concussionfrom head <strong>in</strong>jury• Pregnancy complications or 3rdtrimester without previous care• Mental health or psychologicalhealth• Chronic diseases not accountedfor <strong>in</strong> o<strong>the</strong>r conditions• O<strong>the</strong>r, not specified• Laceration from weaponor dagger <strong>in</strong>jury• Burns• Infected wounds• Crush <strong>in</strong>jury syndrome• Amputation• O<strong>the</strong>r, not specifiedOn 24 April (over three months after <strong>the</strong> impact), <strong>the</strong> U.S. Centers for Disease Controland Prevention (CDC) assumed responsibility for analysis of data (Magliore etal. <strong>2010</strong>).Consider<strong>in</strong>g <strong>the</strong> difficult conditions of its <strong>in</strong>ception, <strong>the</strong> system <strong>in</strong>evitably had seriousdefects such as a late start, chronic underreport<strong>in</strong>g, unclear def<strong>in</strong>itions, and limited labora<strong>to</strong>rysupport or field supervision for quality control. More important, foreign medicalteams and facilities that were provid<strong>in</strong>g most of <strong>the</strong> <strong>earthquake</strong> related services were not<strong>in</strong>cluded <strong>in</strong> <strong>the</strong> report<strong>in</strong>g system, which was based on pre-exist<strong>in</strong>g, primary level <strong>in</strong>stitutionsactive <strong>in</strong> AIDS programs.Never<strong>the</strong>less, <strong>the</strong> network did provide some basis <strong>to</strong> rule out any unexpected <strong>in</strong>crease of<strong>the</strong> notifiable conditions, especially <strong>in</strong>fectious syndromes. Day after day, <strong>the</strong> system reportedthat no unexpected or abnormal <strong>in</strong>crease <strong>in</strong> diseases was detected. With <strong>the</strong> l<strong>in</strong>ger<strong>in</strong>gconcern shared by most ac<strong>to</strong>rs of possible epidemics and a higher density of medicalpersonnel ever seen by <strong>Haiti</strong>, <strong>the</strong> absence of any significant outbreak is worth not<strong>in</strong>g. 8585 A major cholera epidemic started <strong>in</strong> Oc<strong>to</strong>ber <strong>2010</strong>. It was unrelated <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> disaster as it started <strong>in</strong> a departmentnot directly affected by <strong>the</strong> event. Fur<strong>the</strong>rmore, <strong>the</strong> morbidity/mortality of cholera was lower among <strong>the</strong> displaced populationsattended by humanitarian organizations than <strong>in</strong> groups not affected by <strong>the</strong> <strong>earthquake</strong>. Had <strong>the</strong> emergence of thisunrelated cholera epidemic co<strong>in</strong>cided <strong>in</strong> time and place with <strong>the</strong> <strong>earthquake</strong> <strong>response</strong>, <strong>the</strong> myth of <strong>in</strong>evitable post-disasterepidemics would have been considerably more difficult <strong>to</strong> dispel.88
BEYOND TRAUMA CARE - Chapter 6The three most reported conditions for <strong>the</strong> period 25 <strong>January</strong> <strong>to</strong> 24 April were: acuterespira<strong>to</strong>ry diseases (16.3%), suspected malaria (10.3%), and fever of unknown cause(10%) (Magliore et al. <strong>2010</strong>). These are common f<strong>in</strong>d<strong>in</strong>gs <strong>in</strong> develop<strong>in</strong>g countries.Labora<strong>to</strong>ry supportStreng<strong>the</strong>n<strong>in</strong>g <strong>the</strong> labora<strong>to</strong>ry was a major success <strong>in</strong> <strong>Haiti</strong>.The limited capacity <strong>in</strong> public health and cl<strong>in</strong>ical labora<strong>to</strong>ry service was severely reducedby <strong>the</strong> impact. Several agencies partnered with <strong>the</strong> <strong>Haiti</strong>an Government <strong>to</strong> res<strong>to</strong>recapacity of <strong>the</strong> <strong>Haiti</strong> National Public <strong>Health</strong> Labora<strong>to</strong>ry. Among <strong>the</strong>m, CDC <strong>in</strong>collaboration with USAID began send<strong>in</strong>g labora<strong>to</strong>ry supplies <strong>in</strong>clud<strong>in</strong>g microscopes,rapid diagnostic tests, and o<strong>the</strong>r critical equipment and reagents by <strong>the</strong> end of <strong>January</strong>.Subject matter experts were also provided for <strong>the</strong> post-disaster disease surveillance(malaria, typhoid, measles, cholera, dengue, etc.).Tra<strong>in</strong><strong>in</strong>g of <strong>the</strong> labora<strong>to</strong>ry staff began on 8 February and <strong>the</strong> National Labora<strong>to</strong>ry tested<strong>the</strong> first dengue sample on 10 February, less than a month after <strong>the</strong> <strong>earthquake</strong> hit.Two months after <strong>the</strong> impact, <strong>the</strong> National Labora<strong>to</strong>ry began send<strong>in</strong>g consolidatedreports <strong>to</strong> <strong>the</strong> <strong>Haiti</strong>an M<strong>in</strong>istry of <strong>Health</strong>.Immunization programs• In <strong>Haiti</strong>, <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong> refra<strong>in</strong>ed from endors<strong>in</strong>g improvised or <strong>in</strong>discrim<strong>in</strong>atemass immunization campaigns as had occurred follow<strong>in</strong>g some o<strong>the</strong>r disasters.• Instead, <strong>the</strong> M<strong>in</strong>istry recommended targeted vacc<strong>in</strong>ations of vulnerable groups <strong>to</strong>meet specific risks. Private ac<strong>to</strong>rs did not consistently follow <strong>the</strong>se guidel<strong>in</strong>es.32FILMBecause a widespread, lethal outbreak is not a reasonable scenario, improvised emergencyimmunizations programs generally have no place <strong>in</strong> <strong>the</strong> immediate aftermathof <strong>the</strong> disaster. This does not, however, preclude <strong>the</strong> need for specific and carefullyplanned immunizations <strong>to</strong> respond <strong>to</strong> a specific threat or <strong>to</strong> take advantage of populationdisplacement <strong>to</strong> improve rout<strong>in</strong>e immunization coverage.Specific fac<strong>to</strong>rs required attention <strong>in</strong> <strong>Haiti</strong>:• An <strong>in</strong>creased <strong>in</strong>cidence of tetanus was anticipated due <strong>to</strong> <strong>the</strong> high number of<strong>in</strong>juries (many wounds had not been cleaned and were becom<strong>in</strong>g <strong>in</strong>fected);• A DPT immunization campaign had been planned for <strong>the</strong> week of <strong>the</strong> <strong>earthquake</strong><strong>in</strong> <strong>response</strong> <strong>to</strong> an ongo<strong>in</strong>g diph<strong>the</strong>ria outbreak <strong>in</strong> Port-au-Pr<strong>in</strong>ce;32 32A• F<strong>in</strong>ally, <strong>the</strong> opportunity (and risks) of a large population with very low rout<strong>in</strong>eimmunization coverage (<strong>the</strong> lowest <strong>in</strong> <strong>the</strong> Region of <strong>the</strong> Americas) liv<strong>in</strong>g<strong>in</strong> temporary settlements served by NGOs or donors.Pho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>89
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>TetanusThere are no reliable estimates of <strong>the</strong> number of post-<strong>in</strong>jury tetanus cases <strong>in</strong> <strong>Haiti</strong>. Asof 8 February <strong>2010</strong>, 16 cases were reported by <strong>the</strong> surveillance system. Cuban andDom<strong>in</strong>ican medical teams also periodically reported cases.Tetanus vacc<strong>in</strong>e and serum were available <strong>in</strong> sufficient amounts <strong>in</strong> PROMESS, <strong>the</strong>pharmaceutical warehouse adm<strong>in</strong>istered by PAHO/WHO. Surpris<strong>in</strong>gly, many foreignmedical teams arriv<strong>in</strong>g <strong>to</strong> treat <strong>the</strong> <strong>in</strong>jured did not have those essential productsavailable. A campaign was <strong>in</strong>itiated <strong>to</strong> <strong>in</strong>form all teams of <strong>the</strong> need for and availabilityof vacc<strong>in</strong>e and serum.Dip<strong>the</strong>ria, pertussis, and tetanus (DPT)In most countries, DPT is part of <strong>the</strong> rout<strong>in</strong>e child immunization program. In <strong>Haiti</strong>,it was estimated that 50%-60% of <strong>the</strong> new cohort (under one year old) was not coveredat <strong>the</strong> time of <strong>the</strong> <strong>earthquake</strong>.Hav<strong>in</strong>g passed <strong>the</strong> acute emergency, <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong> decided <strong>to</strong> plan a campaignat <strong>the</strong> end of February (6 weeks after impact) for DPT and measles, mumps, and rubella(MMR). Some major NGOs opposed this move and absta<strong>in</strong>ed from collaborat<strong>in</strong>g.In addition, logistical problems appeared rapidly <strong>in</strong> <strong>the</strong> first cycle (maps of temporarysettlements pr<strong>in</strong>ted <strong>in</strong> English) followed by vacc<strong>in</strong>e fatigue <strong>in</strong> <strong>the</strong> second cycle. 86MeaslesAlthough <strong>the</strong>re had been no confirmed cases of measles s<strong>in</strong>ce 2001, <strong>the</strong> risk of outbreaksrema<strong>in</strong>ed present due <strong>to</strong> low immunization coverage. In 2007 coverage wasestimated at only 58% <strong>in</strong> children under one year old. New cohorts of children werepotentially at risk.In a brief<strong>in</strong>g document prepared for <strong>Haiti</strong> responders, WHO recommended that all displacedpersons between six months and 35 years old who were liv<strong>in</strong>g <strong>in</strong> an overcrowdedcamp be vacc<strong>in</strong>ated aga<strong>in</strong>st rubella and measles (WHO <strong>2010</strong>b). As <strong>in</strong>dicated earlier, anational strategy <strong>to</strong> improve <strong>the</strong> coverage <strong>in</strong> <strong>the</strong> camps was adopted <strong>in</strong> February but wasnot supported by some of <strong>the</strong> largest NGOs.No case of measles has been reported s<strong>in</strong>ce <strong>the</strong> <strong>earthquake</strong>.Water, sanitation, and hygiene (WASH)• Water and sanitation are rapidly emerg<strong>in</strong>g as a major public health priority <strong>in</strong> all disasterswhere <strong>the</strong>re are massive displacements of population.• The M<strong>in</strong>istry of <strong>Health</strong>, although often not responsible for <strong>the</strong> delivery of services,should assume quality control of water and sanitation.86 All houses <strong>in</strong> <strong>the</strong> metropolitan area were GPS-referenced prior <strong>to</strong> <strong>the</strong> <strong>earthquake</strong>. With <strong>the</strong> massive displacement of populationafter <strong>the</strong> <strong>earthquake</strong>, this technical prowess was of little use for immunization campaigns.90
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>The impact of <strong>the</strong> 12 <strong>January</strong> <strong>earthquake</strong> on water supply <strong>in</strong> Port-au-Pr<strong>in</strong>ce wasra<strong>the</strong>r atypical. In urban <strong>earthquake</strong>s, attention normally focuses on <strong>the</strong> damage <strong>to</strong>water and sewage pipe systems result<strong>in</strong>g <strong>in</strong> a shortage of water and <strong>the</strong> risk of crosscontam<strong>in</strong>ationbetween both networks. Reports of people break<strong>in</strong>g <strong>in</strong><strong>to</strong> pipes <strong>to</strong>access water have been common <strong>in</strong> past disasters.These were not major issues <strong>in</strong> <strong>Haiti</strong> where dr<strong>in</strong>k<strong>in</strong>g water distribution was largely basedon three systems: an extensive commercial distribution network of high quality water(reverse osmosis and o<strong>the</strong>r techniques); <strong>the</strong> establishment of networks deliver<strong>in</strong>g waterat collective delivery po<strong>in</strong>ts (bornes et fonta<strong>in</strong>es) managed by local committees (Comitésde l’eau); and water delivered at <strong>the</strong> house level by networks function<strong>in</strong>g under <strong>the</strong> municipalcompany (CAMEP).The challenge was <strong>the</strong>refore <strong>to</strong> res<strong>to</strong>re <strong>the</strong>se three networks and ensure <strong>the</strong> availabilityof dr<strong>in</strong>k<strong>in</strong>g water at no cost <strong>to</strong> <strong>the</strong> beneficiaries. Four days after <strong>the</strong> impact it was estimatedthat <strong>the</strong> commercial sec<strong>to</strong>r was <strong>in</strong> <strong>the</strong> position <strong>to</strong> produce 1 million gallons ofwater per day. The challenge was how <strong>to</strong> distribute it. The commercial sec<strong>to</strong>r played amajor role <strong>in</strong> this distribution, first spontaneously <strong>the</strong>n later as contrac<strong>to</strong>rs who werefunded or subsidized by DINEPA and many humanitarian organizations.On <strong>the</strong> operational level, <strong>the</strong> water <strong>response</strong> was pragmatic with <strong>the</strong> objective of provid<strong>in</strong>gas many people as possible with a bare m<strong>in</strong>imum of water. Although all <strong>in</strong>terviewees<strong>in</strong> <strong>Haiti</strong> were aware of <strong>the</strong> “m<strong>in</strong>imum humanitarian standards” established by <strong>the</strong> SphereProject (2011) (for example, 15 liters/person/day), none spontaneously mentioned <strong>the</strong>m<strong>in</strong> our <strong>in</strong>terviews. Instead, <strong>the</strong>y focused on slowly rais<strong>in</strong>g <strong>the</strong> <strong>in</strong>itial amount of dr<strong>in</strong>k<strong>in</strong>gwater <strong>to</strong> be made available <strong>to</strong> all (from 3 liters <strong>to</strong> 5 liters of dr<strong>in</strong>k<strong>in</strong>g water) over a matterof weeks and months.This approach is a considerable improvement on <strong>the</strong> frequent misuse of Sphere standardsby donors as compulsory, quantified goals <strong>to</strong> be achieved under risk of penalty.This was observed <strong>in</strong> o<strong>the</strong>r disasters (natural or human-caused) where agencies opted<strong>to</strong> limit <strong>the</strong> number of <strong>the</strong>ir beneficiaries receiv<strong>in</strong>g an unrealistically high “m<strong>in</strong>imum”standard or requirement <strong>in</strong> order <strong>to</strong> avoid criticism by evalua<strong>to</strong>rs or donors for notbe<strong>in</strong>g <strong>in</strong> compliance. This was <strong>in</strong> fact exactly <strong>the</strong> contrary of <strong>the</strong> triage pr<strong>in</strong>ciple: <strong>the</strong>best benefit for <strong>the</strong> greatest number.As reported <strong>in</strong> <strong>the</strong> <strong>Health</strong> Cluster Bullet<strong>in</strong> (No. 20) nearly five weeks after <strong>the</strong>impact:32FILM“The WASH Cluster cont<strong>in</strong>ues <strong>to</strong> provide safe dr<strong>in</strong>k<strong>in</strong>g water (5 liters perperson per day) <strong>to</strong> over 780,000 people through water tankers and watertreatment plants at 300 sites across Port-au-Pr<strong>in</strong>ce, Léogâne , and Jacmel.The Cluster aims <strong>to</strong> scale up provision of safe dr<strong>in</strong>k<strong>in</strong>g water <strong>to</strong> a <strong>to</strong>tal of1.1 million persons per day. Approximately 2.1 million liters of water aredelivered per day <strong>to</strong> about 500,000 displaced persons <strong>in</strong> 184 sites.”Twelve months after <strong>the</strong> <strong>earthquake</strong>, <strong>the</strong>re was still a large amount of water be<strong>in</strong>g delivered<strong>to</strong> camps and sites with dozens of bladders be<strong>in</strong>g used every day, underl<strong>in</strong><strong>in</strong>g<strong>the</strong> difficulties of f<strong>in</strong>d<strong>in</strong>g solutions “beyond water trucks”. Provision of safe water <strong>in</strong><strong>Haiti</strong> is a never-end<strong>in</strong>g humanitarian task.32 32APho<strong>to</strong>: PAHO/WHO, Sam Vigersky92
BEYOND TRAUMA CARE - Chapter 6Environmental health <strong>in</strong> temporary settlementsNew approaches are needed for excreta and waste management <strong>in</strong> temporary settlements<strong>in</strong> dense urban areas.Pho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>32FILM32 32ASanitation and hygiene (waste disposal, human excreta, etc.) often fall outside <strong>the</strong>responsibility of <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong>, but are never<strong>the</strong>less critical for public health.On 28 <strong>January</strong> (Day 17), <strong>the</strong> WASH Cluster shifted its priority from water <strong>to</strong> sanitation:a change reflect<strong>in</strong>g <strong>the</strong> relative progress <strong>in</strong> provision of water and <strong>the</strong> l<strong>in</strong>ger<strong>in</strong>gfear of possible outbreaks <strong>in</strong> overcrowded settlements without even rudimentary sanitation.Rapidly, <strong>the</strong> provision of latr<strong>in</strong>es ra<strong>the</strong>r than <strong>the</strong> distribution of water became<strong>the</strong> preem<strong>in</strong>ent priority and challenge.Sanitation conditions <strong>in</strong> <strong>Haiti</strong> <strong>in</strong>clud<strong>in</strong>g <strong>in</strong> <strong>the</strong> capital were very poor prior <strong>to</strong> <strong>the</strong><strong>earthquake</strong>. Normal overcrowd<strong>in</strong>g <strong>in</strong> Port-au-Pr<strong>in</strong>ce is such that few open spaces(parks, squares, green spaces, etc.) exist. After <strong>the</strong> quake <strong>the</strong>y were quickly packedwith displaced populations. In an urban environment, <strong>in</strong>stall<strong>in</strong>g traditionallatr<strong>in</strong>es (trenches, for <strong>in</strong>stance) at a safe distance from tents and shelters wasnot possible. Dur<strong>in</strong>g <strong>the</strong> first three months, more than 3,000 portable latr<strong>in</strong>es(chemical or not) were <strong>in</strong>stalled by NGOs <strong>in</strong> targeted camps <strong>in</strong> metropolitanareas. The major challenges were <strong>to</strong> f<strong>in</strong>d unoccupied spaces where <strong>the</strong>y could bepositioned, and <strong>to</strong> organize an ongo<strong>in</strong>g system of collection and disposal of urbanexcreta. This was not solved dur<strong>in</strong>g <strong>the</strong> period under review (Grünewald,B<strong>in</strong>der, Georges <strong>2010</strong>).The objective of waste disposal has largely benefitted <strong>the</strong> commercial sec<strong>to</strong>r. It wasonly partially met <strong>in</strong> part due <strong>to</strong> lengthy difficulties with cus<strong>to</strong>ms clearance and <strong>the</strong>registration of UNICEF trucks.Despite efforts <strong>to</strong> <strong>in</strong>stall latr<strong>in</strong>es, progress was slow 30 days after impact:“Sanitation cont<strong>in</strong>ues <strong>to</strong> be a major challenge of utmost concern. It iscurrently estimated that less than 5% of <strong>the</strong> needs for latr<strong>in</strong>es is be<strong>in</strong>gmet (one latr<strong>in</strong>e per 50 people). This poses huge challenges for publichealth <strong>in</strong> temporary settlement sites.” 89This challenge was, however, alleviated by a progressive reduction <strong>in</strong> <strong>the</strong> numberof families <strong>in</strong> temporary settlements. However, for many of those <strong>in</strong>terviewed, itappears that <strong>the</strong> services provided by <strong>the</strong> <strong>in</strong>ternational community were ultimatelybetter than those available <strong>to</strong> <strong>the</strong> general population, although far short of <strong>the</strong> “m<strong>in</strong>imum”standard of one latr<strong>in</strong>e for 20 people as set <strong>in</strong>ternationally. 9089 Reported <strong>in</strong> <strong>the</strong> <strong>Health</strong> Cluster Bullet<strong>in</strong> No. 18. The figure of one latr<strong>in</strong>e for 50 persons was seen as <strong>to</strong>o optimistic by some<strong>in</strong>terviewees who believed that <strong>the</strong> number of users actually was around 200 per latr<strong>in</strong>e for at least three months.90 See <strong>the</strong> Sphere Project standards for excreta disposal at: www.sphereproject.org/content/view/43/83/lang,english.93
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Environmental health <strong>in</strong> medical facilitiesMedical and hospital waste is a major problem <strong>in</strong> all disasters. It is a costly issue thatmust be addressed early on.The need for safe water <strong>in</strong> hospitals (exist<strong>in</strong>g or new facilities) was brought <strong>to</strong> <strong>the</strong> attentionof decision makers at a very early stage. Coord<strong>in</strong>ation between DINEPA and<strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong> as well as quality control by PAHO/WHO-tra<strong>in</strong>ed personnelensured that this problem was addressed beg<strong>in</strong>n<strong>in</strong>g one week after <strong>the</strong> impact.The provision of medical care by thousands of health professionals or volunteers createda significant need for safe disposal of human as well as medical waste (dress<strong>in</strong>gs, syr<strong>in</strong>ges,needles, expired drugs, etc.). The Swedish Civil Cont<strong>in</strong>gency Agency (March <strong>2010</strong>)estimated that 15%–20% of health care waste was hazardous or <strong>in</strong>fectious (<strong>in</strong>clud<strong>in</strong>gdiscarded human tissues or limbs).The need for “a clear strategy for deal<strong>in</strong>g with health care waste” was identified as apriority from Day 6 and rema<strong>in</strong>ed so for weeks. On Day 13, a system was launched<strong>to</strong> collect medical wastes and dispose of <strong>the</strong>m <strong>in</strong> a landfill. Progress was noted <strong>in</strong><strong>the</strong> ma<strong>in</strong> hospitals but <strong>the</strong> issue l<strong>in</strong>gered due <strong>to</strong> <strong>the</strong> carelessness of some <strong>in</strong>dependentteams or facilities.Lack of prior plann<strong>in</strong>g for safe disposal of medical waste is a recurrent problem<strong>in</strong> disasters and need not be rediscovered by humanitarian organizations <strong>in</strong>each emergency situation.Food and nutrition32 32AFILM32Pho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>No widespread malnutrition was noted <strong>in</strong> <strong>Haiti</strong> or <strong>in</strong> o<strong>the</strong>r disaster-affected countries.This may be due <strong>in</strong> part <strong>to</strong> <strong>the</strong> massive food distribution and streng<strong>the</strong>n<strong>in</strong>g of nutritionalactivities but also <strong>to</strong> <strong>the</strong> fact that <strong>earthquake</strong>s do not affect food availability at<strong>the</strong> national level. The issue was one of lost <strong>in</strong>come that might be addressed by directf<strong>in</strong>ancial assistance <strong>to</strong> households.Prior publications from PAHO/WHO on natural disasters outl<strong>in</strong>ed that <strong>the</strong> impac<strong>to</strong>f <strong>earthquake</strong>s on food supply and malnutrition is dist<strong>in</strong>ct from that of hydrologicaldisasters such as floods, hurricanes, or drought. Earthquakes do not directly affect cropsor food s<strong>to</strong>cks at <strong>the</strong> national level. They may have an <strong>in</strong>direct and delayed impact onnutritional levels by reduc<strong>in</strong>g <strong>the</strong> access of some of <strong>the</strong> affected population <strong>to</strong> exist<strong>in</strong>gs<strong>to</strong>cks because of lost <strong>in</strong>come or logistical problems.<strong>Haiti</strong> was not an exception. Food s<strong>to</strong>res and markets were closed only temporarily(1–2 weeks at most). Food and basic supplies were rapidly available provided onecould afford <strong>the</strong>m. Prices <strong>in</strong>creased but not <strong>to</strong> <strong>the</strong> po<strong>in</strong>t of affect<strong>in</strong>g those luckyenough <strong>to</strong> have ma<strong>in</strong>ta<strong>in</strong>ed <strong>the</strong>ir bus<strong>in</strong>ess and <strong>in</strong>come. The destruction of <strong>the</strong> harbor<strong>in</strong> Port-au-Pr<strong>in</strong>ce and o<strong>the</strong>r logistical challenges (blocked roads) were only temporary,aggravat<strong>in</strong>g problems affect<strong>in</strong>g both <strong>the</strong> humanitarian and commercial flow of goods.94
BEYOND TRAUMA CARE - Chapter 6Pho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>32FILM32 32AThe most important impact from a nutritional po<strong>in</strong>t of view is <strong>the</strong> fact that an already<strong>in</strong>adequate access <strong>to</strong> a proper diet for those economically most vulnerable was drasticallyreduced by <strong>the</strong> loss of <strong>the</strong>ir means of survival. Loss of meager livelihoods wasonly partially compensated by <strong>the</strong> sharp <strong>in</strong>crease <strong>in</strong> remittances from abroad, and89% of <strong>the</strong> recipients used those remittances before <strong>the</strong> <strong>earthquake</strong> <strong>to</strong> procure food.Some donors and experts suggested early after <strong>the</strong> impact that if <strong>the</strong> primary cause wasa loss of <strong>in</strong>come, cash assistance should partly replace <strong>the</strong> importation and distributionof food after <strong>the</strong> <strong>in</strong>itial emergency <strong>response</strong> (WFP <strong>2010</strong>).Prior <strong>to</strong> <strong>the</strong> <strong>earthquake</strong>, <strong>the</strong> “cluster” structure was seen as very peculiar (B<strong>in</strong>derand Grünewald <strong>2010</strong>): nutrition, food aid, and food security after sudden-onsetdisasters were considered dist<strong>in</strong>ct, albeit related, issues that are coord<strong>in</strong>ated separately.The Nutrition Cluster under UNICEF, <strong>the</strong> Food Aid Cluster under WFP,and Food Security Cluster under FAO were three different and disconnectedentities. Yet prevention of acute malnutrition <strong>in</strong> <strong>the</strong> aftermath of a geologicaldisaster, <strong>the</strong> end result of food <strong>in</strong>security, is mostly beyond <strong>the</strong> responsibilityof <strong>the</strong> health sec<strong>to</strong>r.The re-activation of <strong>the</strong> Nutrition Cluster offered UNICEF an opportunity <strong>to</strong>streng<strong>the</strong>n <strong>the</strong> capacity of its counterpart <strong>in</strong> <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong> by provid<strong>in</strong>g an<strong>in</strong>strument <strong>to</strong> exercise leadership over humanitarian ac<strong>to</strong>rs. The priorities as establishedby <strong>the</strong> Nutrition Cluster, which convened on 20 <strong>January</strong> (Day 9), <strong>in</strong>cluded:• Protection and support for women who are breastfeed<strong>in</strong>g;• Moni<strong>to</strong>r<strong>in</strong>g breast-milk substitutes and o<strong>the</strong>r milk products com<strong>in</strong>g <strong>in</strong><strong>to</strong> <strong>the</strong>country;• Moni<strong>to</strong>r<strong>in</strong>g <strong>the</strong> provision of breast-milk substitutes and o<strong>the</strong>r milk products;• Complementary feed<strong>in</strong>g of children above six months old;• Treatment of global acute malnutrition.Between 40 and 50 agencies participated <strong>in</strong> <strong>the</strong> meet<strong>in</strong>gs of <strong>the</strong> Nutrition Cluster.Only 25 of <strong>the</strong>m had professional nutritional expertise while some 15 were regardedas “amateurs, without any idea of <strong>the</strong> nutritional value of food.” Rapidly, <strong>the</strong> nutritionaloffers and requests were critically reviewed and filtered, ultimately focus<strong>in</strong>gmore on <strong>the</strong>rapeutic products. The department of <strong>the</strong> M<strong>in</strong>istry deal<strong>in</strong>g with nutritionwas <strong>the</strong> only one that had updated guidel<strong>in</strong>es <strong>in</strong> an electronic version, which weregenerally respected by all partners. However, specific guidel<strong>in</strong>es on breast milk substituteswere often violated.The Food Aid Cluster, led by <strong>the</strong> World Food Programme, focused <strong>in</strong> February onsupplementary feed<strong>in</strong>g of children (6–59 months) and pregnant or lactat<strong>in</strong>g women<strong>in</strong> temporary shelters <strong>in</strong> Port-au-Pr<strong>in</strong>ce. The program was based on distribution ofhigh-energy biscuits or ready-<strong>to</strong>-use foods <strong>to</strong> 88,000 beneficiaries. In March <strong>2010</strong>,<strong>the</strong> supplementary feed<strong>in</strong>g program was extended <strong>to</strong> <strong>the</strong> same vulnerable groups <strong>in</strong>departmental urban areas hav<strong>in</strong>g received large numbers of <strong>in</strong>ternally displaced. At<strong>the</strong> same time, <strong>the</strong> biscuits and ready-<strong>to</strong>-use food were progressively and partly substitutedwith <strong>the</strong> usual WFP supplementary ration made of corn-soya blend (CSB), oil,and sugar (WFP <strong>2010</strong>).95
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>The normal activities of prevention and treatment of acute malnutrition with<strong>in</strong> <strong>the</strong>M<strong>in</strong>istry of <strong>Health</strong> with UNICEF, which were <strong>in</strong>adequate prior <strong>to</strong> <strong>the</strong> impact, wereresumed <strong>in</strong> March (6 weeks after impact).General food distribution was of a much greater scope than targeted nutritional programs.At <strong>the</strong> peak of activity, food was reportedly distributed <strong>to</strong> over 4 million beneficiaries.It should be noted that <strong>the</strong> PDNA estimated <strong>the</strong> affected population at 1.5million. Accord<strong>in</strong>g <strong>to</strong> a WFP external evaluation, “political fac<strong>to</strong>rs <strong>in</strong>fluenced <strong>the</strong><strong>in</strong>put and stance <strong>the</strong> <strong>Haiti</strong>an government <strong>to</strong>ok with respect <strong>to</strong> program implementation,<strong>in</strong>clud<strong>in</strong>g <strong>the</strong> phas<strong>in</strong>g out of general food distribution <strong>to</strong> more targeted safetynet activities” (WFP 2011).O<strong>the</strong>r experts are of <strong>the</strong> view that <strong>the</strong> large-scale food aid was largely a <strong>response</strong> pushedby some governments, and by and large term<strong>in</strong>ated on time <strong>in</strong> order <strong>to</strong> avoid negativeeffects. Some donors <strong>in</strong>terviewed also mentioned <strong>the</strong>ir only partly successful efforts<strong>to</strong> promote greater cash-based programs (not merely <strong>the</strong> traditional cash- or voucherfor-workbut also direct, un-earmarked cash allocations). Yet, as recommended bysome studies, 91 many aid ac<strong>to</strong>rs f<strong>in</strong>ally moved away from food-based and engaged <strong>in</strong>cash-based relief activities, especially cash-for-work programs (e.g., remov<strong>in</strong>g debrisand improv<strong>in</strong>g <strong>the</strong> urban environment and sanitation).The provision of milk products was also a po<strong>in</strong>t of <strong>in</strong>terest. The unsupervised donationof powdered milk is strongly discouraged <strong>in</strong> <strong>the</strong> aftermath of sudden-impactdisasters. Its use outside well-managed programs is often unsanitary and a potentialcause of diarrhea. The quality of water be<strong>in</strong>g a special concern <strong>in</strong> <strong>Haiti</strong>, it wasnecessary <strong>to</strong> repeatedly rem<strong>in</strong>d NGOs and health care providers not <strong>to</strong> distributepowdered milk. 92 Success was only partial.32FILMIn conclusion, fur<strong>the</strong>r surveys <strong>in</strong>dicated that malnutrition did not <strong>in</strong>creaseas a result of <strong>the</strong> <strong>earthquake</strong>. Consider<strong>in</strong>g <strong>the</strong> scale of food distribution andsupplementary feed<strong>in</strong>g, this outcome was <strong>to</strong> be expected. More than that, <strong>the</strong>flow of remittances from <strong>the</strong> diaspora <strong>in</strong>creased significantly thus <strong>in</strong>creas<strong>in</strong>g<strong>the</strong> purchas<strong>in</strong>g power of <strong>the</strong> affected populations and <strong>the</strong>ir access <strong>to</strong>food. Food markets became very active <strong>in</strong> a few weeks time and <strong>the</strong> flow ofproducts from rural areas <strong>to</strong> affected urban zones <strong>in</strong>creased rapidly. Thereare no data available regard<strong>in</strong>g <strong>the</strong> cost-effectiveness or <strong>the</strong> possible negativeimpacts (for example, on local food production and markets, dependency, etc.) of<strong>the</strong> massive distribution of food compared <strong>to</strong> o<strong>the</strong>r measures. Whe<strong>the</strong>r f<strong>in</strong>ancial assistance<strong>to</strong> households would not have been more effective from <strong>the</strong> po<strong>in</strong>t of viewof nutrition and well-be<strong>in</strong>g has not been sufficiently debated <strong>in</strong> <strong>the</strong> case of <strong>Haiti</strong>. Itdef<strong>in</strong>itely would have helped <strong>to</strong> ma<strong>in</strong>ta<strong>in</strong> <strong>the</strong> sense of dignity and pride that is soimportant <strong>to</strong> <strong>Haiti</strong>an culture.32 32APho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>91 See, for example, ALNAP/ProVention (2009), “Respond<strong>in</strong>g <strong>to</strong> Urban Disasters: learn<strong>in</strong>g from previous relief and recoveryoperations.” Available at: www.alnap.org/pool/files/alnap-provention-lessons-urban.pdf .92 Instead, ready-<strong>to</strong>-dr<strong>in</strong>k t<strong>in</strong>s were provided, contribut<strong>in</strong>g <strong>to</strong> <strong>the</strong> <strong>to</strong>ns of waste produced daily and clogg<strong>in</strong>g most of <strong>the</strong> dra<strong>in</strong>agesystem <strong>in</strong> Port-au-Pr<strong>in</strong>ce.96
BEYOND TRAUMA CARE - Chapter 6Mental health and psychosocial assistance32FILM• Needs for psychosocial assistance should not be overlooked on <strong>the</strong> assumptionthat poor communities are more resilient.• The psychosocial field is currently attract<strong>in</strong>g <strong>to</strong>o many emergency ac<strong>to</strong>rs who maynot have <strong>the</strong> necessary expertise and resources.• Specialized programs <strong>in</strong> <strong>the</strong> aftermath of sudden-onset disasters should serve as<strong>the</strong> po<strong>in</strong>t of entry for <strong>the</strong> provision of mental health services at primary health careand community levels.In past sudden-onset disasters, <strong>the</strong> mental health impact on <strong>the</strong> affected populationhas been <strong>the</strong> subject of debate, lead<strong>in</strong>g <strong>to</strong> diverse <strong>in</strong>terventions. 93 These range from<strong>the</strong> dispatch of unprepared young social workers from Western urban areas <strong>in</strong><strong>to</strong> <strong>the</strong>conservative Islamic, rural environment of Bam (Iran) <strong>to</strong> <strong>the</strong> excessive medicalizationof an o<strong>the</strong>rwise common reaction <strong>in</strong> <strong>the</strong> aftermath of a sudden disaster. 94Pho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>32 32AThe different perspectives beh<strong>in</strong>d mental health <strong>in</strong>tervention and psychosocialsupport are well articulated <strong>in</strong> WHO/IASC guidel<strong>in</strong>es and are summarized below(WHO/IASC 2007):• Aid agencies outside <strong>the</strong> health sec<strong>to</strong>r tend <strong>to</strong> speak of “support<strong>in</strong>g psychosocialwell-be<strong>in</strong>g”. <strong>Health</strong> sec<strong>to</strong>r agencies tend <strong>to</strong> speak of “mental health”. Exact def<strong>in</strong>itionsof <strong>the</strong>se terms vary between and with<strong>in</strong> aid organizations, discipl<strong>in</strong>es andcountries.• Mental health and psychosocial problems <strong>in</strong> emergencies are highly <strong>in</strong>terconnectedyet may be predom<strong>in</strong>antly social or psychological <strong>in</strong> nature (ra<strong>the</strong>r than medical).• Significant problems of a predom<strong>in</strong>antly social nature <strong>in</strong>clude:• Pre-exist<strong>in</strong>g (pre-emergency) social problems (e.g., extreme poverty);• Emergency-<strong>in</strong>duced social problems (e.g., family separation; disruption ofsocial networks; destruction of community structures, resources, and trust;<strong>in</strong>creased gender-based violence); and• Aid-<strong>in</strong>duced social problems (e.g., underm<strong>in</strong><strong>in</strong>g of community structures ortraditional support mechanisms).• Similarly, problems of a predom<strong>in</strong>antly psychological nature <strong>in</strong>clude:• Pre-exist<strong>in</strong>g problems (e.g., severe mental disorder; alcohol abuse);• Emergency-<strong>in</strong>duced problems (e.g., grief, non-pathological distress, depressionand anxiety disorders, <strong>in</strong>clud<strong>in</strong>g post-traumatic stress disorder [PTSD]); and• Aid-related problems (e.g., anxiety due <strong>to</strong> a lack of <strong>in</strong>formation).93 Psychosocial support <strong>to</strong> relief workers, an important <strong>to</strong>pic, is not addressed <strong>in</strong> this section.94 A survey conducted six months after <strong>the</strong> tsunami <strong>in</strong> Sri Lanka found that 56% of <strong>the</strong> <strong>in</strong>ternally displaced populationsuffered from post-traumatic stress disorder (PTSD). In o<strong>the</strong>r words, more than half of <strong>the</strong> population was suffer<strong>in</strong>gfrom a pathological disorder (Wickrama 2008).97
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>The key po<strong>in</strong>t of <strong>the</strong> WHO/IASC guidel<strong>in</strong>es is that “mental health and psychosocialproblems <strong>in</strong> emergencies encompass far more than <strong>the</strong> experience of PTSD.” Thispo<strong>in</strong>t was well unders<strong>to</strong>od by <strong>the</strong> Sri Lankan authorities who recommended “listen<strong>in</strong>g<strong>to</strong> victims [of <strong>the</strong> tsunami] without offer<strong>in</strong>g op<strong>in</strong>ions and not diagnos<strong>in</strong>g or label<strong>in</strong>gpeople as suffer<strong>in</strong>g from post-traumatic stress disorder” (Mahoney et al. 2006).Disasters are highly emotional events. The State of M<strong>in</strong>nesota handbook on disaster recoveryoffers a layman’s description of <strong>the</strong> various phases <strong>in</strong> <strong>the</strong> affected population’s reaction <strong>to</strong>disasters (Table 6.5). It is noteworthy that this scenario can be applicable <strong>to</strong> most cultures.Table 6.5 Four phases of disaster <strong>response</strong>Phase Usual length of time Actions EmotionsHeroic phase Prior <strong>to</strong> impact andup <strong>to</strong> a week afterwardsStruggle <strong>to</strong> prevent lossof lives and m<strong>in</strong>imizeproperty damageFear, anxiety, stunnedHoneymoonphaseDisillusionmentphaseReconstructionphaseTwo weeks <strong>to</strong> twomonthsSeveral months <strong>to</strong>over a yearSeveral yearsRelief efforts lift spirits ofsurvivors; hopes of quickrecovery run high; optimismis often short-livedThe realities of bureaucraticpaperwork andrecovery delays set <strong>in</strong>;outside help leaves; survivorsrealize <strong>the</strong>y havelots <strong>to</strong> do <strong>the</strong>mselves and<strong>the</strong>ir lives many never be<strong>the</strong> sameNormal function<strong>in</strong>g isgradually reestablishedSource: M<strong>in</strong>nesota Department of Public Safety (n.d.) Recovery from disaster handbook (Chapter 1).Euphoria at be<strong>in</strong>g alive,grateful, grief, disbeliefFrustration, depression,self-doubt, loss/grief,isolationSatisfaction with progress;emotions appropriate<strong>to</strong> current events32Mental health <strong>in</strong>terventions <strong>in</strong> <strong>Haiti</strong> 95FILMThere is a lack of quantified or objective <strong>in</strong>formation regard<strong>in</strong>g <strong>the</strong> importanceof <strong>the</strong> mental health impact on <strong>the</strong> affected <strong>Haiti</strong>an population. This was alsoobserved <strong>in</strong> <strong>the</strong> disasters <strong>in</strong> Indonesia, Sri Lanka, and Pakistan.PAHO/WHO estimated that at one po<strong>in</strong>t over 110 different organizationswere provid<strong>in</strong>g mental health and/or psychosocial services, or conduct<strong>in</strong>gtra<strong>in</strong><strong>in</strong>g <strong>to</strong> health and mental health professionals (PAHO/WHO 2011a). Asobserved after <strong>the</strong> Indian Ocean tsunami and Pakistan <strong>earthquake</strong>, psychosocialassistance takes many forms, <strong>in</strong>clud<strong>in</strong>g activities as simple as enterta<strong>in</strong><strong>in</strong>g children.Mental health was not an orphan <strong>to</strong>pic <strong>in</strong> <strong>the</strong> <strong>Haiti</strong> <strong>earthquake</strong> <strong>response</strong>; it had severalparents. Immediately after <strong>the</strong> <strong>earthquake</strong>, meet<strong>in</strong>gs of a Cross-Cluster Work<strong>in</strong>g32 32APho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>95 Z. Abaakouk provided <strong>in</strong>sight <strong>in</strong><strong>to</strong> mental health care services available prior <strong>to</strong> and follow<strong>in</strong>g impact <strong>in</strong> <strong>Haiti</strong>. See Abaakouk,“Mental health <strong>in</strong> <strong>Haiti</strong> <strong>in</strong> <strong>2010</strong>: a public health need, an added value with<strong>in</strong> health care practice and a corners<strong>to</strong>nefor reconstruction” <strong>in</strong> PAHO/WHO, Mental health and psychosocial support <strong>in</strong> emergencies <strong>in</strong> <strong>the</strong> Caribbean (forthcom<strong>in</strong>g).98
BEYOND TRAUMA CARE - Chapter 6Group on Mental <strong>Health</strong> and Psychosocial Support were convened first by UNICEFand later by IOM <strong>to</strong> assist <strong>in</strong> coord<strong>in</strong>at<strong>in</strong>g <strong>the</strong> many organizations present <strong>in</strong> <strong>the</strong>field. The M<strong>in</strong>istry of <strong>Health</strong>, with WHO support, also led a Mental <strong>Health</strong> Work<strong>in</strong>gGroup with selected ac<strong>to</strong>rs (ma<strong>in</strong>ly psychological and psychiatric service providers)that focused on specific strategic issues related <strong>to</strong> <strong>the</strong> mental health model for <strong>in</strong>terventionat <strong>the</strong> national level. This <strong>in</strong>cluded: essential psychotropic drug list, mentalhealth pro<strong>to</strong>cols, mental health data collection, draft<strong>in</strong>g a plan for tra<strong>in</strong><strong>in</strong>g health andmental health professionals, etc.In order <strong>to</strong> guide <strong>the</strong> <strong>in</strong>itial <strong>response</strong>, WHO provided some tentative projections orestimates of what might be expected <strong>in</strong> <strong>the</strong> aftermath of disasters:• “The percentage of people with a severe mental disorder (e.g., psychosis and severelydisabl<strong>in</strong>g presentations of mood and anxiety disorders) <strong>in</strong>creases by 1 percent over and above an estimated basel<strong>in</strong>e of 2–3 per cent.• “In addition, <strong>the</strong> percentage of people with mild or moderate mental disorders, <strong>in</strong>clud<strong>in</strong>gmost presentations of mood and anxiety disorders (such as post-traumaticstress disorder, or PTSD), may <strong>in</strong>crease by 5–10 per cent above an estimated basel<strong>in</strong>eof 10 per cent.• “In most situations natural recovery over time (i.e., heal<strong>in</strong>g without outside <strong>in</strong>tervention)will occur for many—but not all—survivors with mild and moderatedisorders” (WHO/IASC 2007,123).No attempt was apparently made <strong>to</strong> validate those figures <strong>in</strong> <strong>the</strong> context of <strong>Haiti</strong>, acountry show<strong>in</strong>g extraord<strong>in</strong>ary resilience over <strong>the</strong> years but also submitted <strong>to</strong> a considerableshock (<strong>the</strong> <strong>earthquake</strong>, <strong>the</strong> mass casualties, <strong>the</strong> amputations, <strong>the</strong> management ofdead bodies, and <strong>the</strong> side effects of an <strong>in</strong>ternational <strong>response</strong> not always address<strong>in</strong>g <strong>the</strong>perceived priorities). Resiliency, a survival trait, does not reduce <strong>the</strong> emotional stress andneed for psychosocial support.The extent of <strong>the</strong> mental health <strong>response</strong> is better documented. In addition <strong>to</strong> local humanresources, additional assistance poured <strong>in</strong><strong>to</strong> <strong>Haiti</strong>. Among <strong>the</strong>m were 10 psychiatrists, 4psychologists, professionals from <strong>the</strong> Cuban Medical Brigade work<strong>in</strong>g at <strong>the</strong> communitylevel, three mental health tra<strong>in</strong>ers from International Medical Corps, experts and cl<strong>in</strong>icalpractitioners from <strong>the</strong> major medical NGOs (MSF, Médec<strong>in</strong>s du Monde) as well as frommany Red Cross societies. 96Yves Lecomte (<strong>2010</strong>) gave <strong>the</strong> follow<strong>in</strong>g account:“Accord<strong>in</strong>g <strong>to</strong> a census conducted by <strong>the</strong> Work<strong>in</strong>g Group of <strong>the</strong> M<strong>in</strong>istryof <strong>Health</strong>, <strong>the</strong>re would be 100 NGOs work<strong>in</strong>g <strong>in</strong> mental health, or 1% of<strong>the</strong> NGOs currently active. Seventeen <strong>in</strong>tervention methods are available,[<strong>in</strong>clud<strong>in</strong>g]: psychological as <strong>in</strong>dividual counsel<strong>in</strong>g, group psycho<strong>the</strong>rapy,medication, social issues advocacy, skills development, vocational tra<strong>in</strong><strong>in</strong>g,social support, etc.” 9796 Basauri, V. Rapport de Mission: La Santé mentale et le soutien psycho-social <strong>in</strong> Haïti [PAHO/WHO Mission Report, 3-6 Feb.<strong>2010</strong>].97 Quotations from <strong>the</strong> article by Yves Lecomte (<strong>2010</strong>) were translated from <strong>the</strong> French.99
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Such a proliferation of ac<strong>to</strong>rs is not always <strong>in</strong> <strong>the</strong> best <strong>in</strong>terest of <strong>the</strong> affected population.Not all responders were as professional or effective as should be expected. The first priority<strong>in</strong> humanitarian assistance is “do no harm.” External mental health and psychosocialsupport is an important means of help<strong>in</strong>g people affected by emergencies but has <strong>the</strong>potential <strong>to</strong> cause harm because it deals with highly sensitive, cultural issues.Lecomte expressed reservations regard<strong>in</strong>g <strong>the</strong> nature of some of this assistance:“Despite <strong>the</strong> fact that s<strong>in</strong>ce <strong>the</strong> seventies, it is said that mental health is nota priority of <strong>the</strong> State and that ‘<strong>Haiti</strong> does not support <strong>the</strong> mentally ill,’ everybodyhas been do<strong>in</strong>g mental health s<strong>in</strong>ce 12 <strong>January</strong> <strong>2010</strong>. In fact, somesay, ‘<strong>Haiti</strong> was <strong>in</strong>vaded by a disparate variety of mental health experts whoare nei<strong>the</strong>r doc<strong>to</strong>rs, psychiatrists, nor psychologists.’. . . Many do not speakFrench or Creole. Suddenly, mental health <strong>in</strong> <strong>Haiti</strong> has become a coveteditem <strong>in</strong>ternationally.”On <strong>the</strong> positive side, <strong>the</strong> same author noted that “many <strong>in</strong>ternational organizations <strong>in</strong>tervened<strong>in</strong> <strong>the</strong> camps and hospitals and provided tra<strong>in</strong><strong>in</strong>g for mental health practitioners.”Those mixed f<strong>in</strong>d<strong>in</strong>gs were also observed <strong>in</strong> <strong>the</strong> aftermath of major disasters attract<strong>in</strong>gconsiderable assistance and fund<strong>in</strong>g (<strong>earthquake</strong>s <strong>in</strong> Bam, Iran, <strong>in</strong> 2003, Pakistan <strong>in</strong>2005, and <strong>the</strong> Indian Ocean tsunami <strong>in</strong> 2004).In spite of those occasional excesses, <strong>the</strong> <strong>response</strong> has produced significant changes <strong>in</strong><strong>Haiti</strong>’s approach <strong>to</strong> mental health. Its effectiveness can be assessed subjectively by us<strong>in</strong>g<strong>the</strong> WHO/IASC list of “Dos and Don’ts” (2007, 123). The most relevant for <strong>the</strong><strong>Haiti</strong> <strong>response</strong> can be found <strong>in</strong> Table 6.6.More than 110 organizationsprovided mental health services100Pho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>
BEYOND TRAUMA CARE - Chapter 6Table 6.6 Recommended ”dos and don’ts” and mental healthand psychosocial support activities after <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong>DoEstablish one overall coord<strong>in</strong>ationgroup on mental healthand psychosocial supportPay attention <strong>to</strong> gender differencesLearn about local culturalpractices and use a mix of localand external methods as appropriateBuild government capacitiesand <strong>in</strong>tegrate mental healthcare for survivors <strong>in</strong> generalhealth servicesIntegrate psychosocial considerations<strong>in</strong><strong>to</strong> all sec<strong>to</strong>rs ofhumanitarian assistanceResponse <strong>in</strong> <strong>Haiti</strong>Two parallel processes: one managed by <strong>the</strong> UN and one by<strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong>. Priority should have been given <strong>to</strong>streng<strong>the</strong>n <strong>the</strong> leadership of <strong>the</strong> M<strong>in</strong>istry.Appears <strong>to</strong> be a concern attended by most <strong>the</strong> ac<strong>to</strong>rs.WHO published a literature review on this <strong>to</strong>pic early on. aA genu<strong>in</strong>e local approach and strategy was a priority of <strong>the</strong>work<strong>in</strong>g group established by <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong>. bInternational NGOs and ac<strong>to</strong>rs stressed capacity build<strong>in</strong>gand tra<strong>in</strong><strong>in</strong>g. The strategy developed by <strong>the</strong> M<strong>in</strong>istryof <strong>Health</strong> work<strong>in</strong>g group focuses on decentralization and<strong>in</strong>tegration of mental health <strong>in</strong> health services (away fromspecialized psychiatric hospitals). Mass media gave visibility<strong>to</strong> this approach. cThe meet<strong>in</strong>gs organized by UNICEF and later by IOM <strong>in</strong>cluded<strong>the</strong>matic sessions on education, children, religion, etc.Don’tDo not conduct duplicate assessmentsor accept prelim<strong>in</strong>arydata <strong>in</strong> an uncritical mannerDo not assume that everyoneis traumatized, or that peoplewho appear resilient need nosupportDo not use a charity model thattreats people <strong>in</strong> <strong>the</strong> communityma<strong>in</strong>ly as beneficiaries ofservicesDo not provide psychotropicmedication without tra<strong>in</strong><strong>in</strong>gand supervisionDo not <strong>in</strong>stitutionalize peopleunless <strong>in</strong>stitutionalization is atemporary and <strong>in</strong>disputably lastresortResponse <strong>in</strong> <strong>Haiti</strong>A weak po<strong>in</strong>t as no quantified and objective assessmentwas available. Lack of clear criteria on <strong>the</strong> mental healthneeds and more press<strong>in</strong>g, compet<strong>in</strong>g issues may expla<strong>in</strong>this shortcom<strong>in</strong>g.The services of many seasoned agencies appeared <strong>to</strong> betailor-made for <strong>the</strong> needs of <strong>the</strong> population. No excessivemedicalization and use of PTSD def<strong>in</strong>itions were noted.Emphasis was on psychosocial assistance and communityapproaches.From <strong>in</strong>terviews, <strong>the</strong> <strong>response</strong> has contributed <strong>to</strong> problemsof dependency and frustration among “beneficiaries.” Theself-centered <strong>in</strong>stitutional focus of many ac<strong>to</strong>rs is claimed<strong>to</strong> have contributed negatively.Except for occasional unconfirmed or undocumentedobservations, use of medication was limited and believed <strong>to</strong>be under supervision.A major achievement was <strong>the</strong> shift from an <strong>in</strong>stitutionalization-basedapproach prior <strong>to</strong> <strong>the</strong> disaster <strong>to</strong> a communityand health services focus.Source: WHO/IASC 2007.a See WHO (<strong>2010</strong>a).b Observations on <strong>the</strong> strategy and local approach <strong>to</strong> mental health support were published <strong>in</strong> D. Henrys. Réflexionssur une politique de santé mentale en Haïti. Revue haïtienne de santé mentale. Vol 2; 217-219.c An article published <strong>in</strong> <strong>the</strong> New York Times (19 March <strong>2010</strong>) stated: “Ultimately, <strong>in</strong>ternational experts are encourag<strong>in</strong>g<strong>the</strong> <strong>Haiti</strong>an <strong>Health</strong> M<strong>in</strong>istry, which <strong>the</strong>y say is receptive and eager for help, <strong>to</strong> <strong>in</strong>corporate mental health care<strong>in</strong><strong>to</strong> <strong>the</strong> primary health care system and <strong>to</strong> make it available throughout <strong>the</strong> country.”101
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>All <strong>in</strong>formation clearly po<strong>in</strong>ts <strong>to</strong>ward a significant improvement <strong>in</strong> <strong>the</strong> approach andpriority given by <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong> <strong>to</strong> a long neglected issue <strong>in</strong> <strong>Haiti</strong>. A w<strong>in</strong>dowof opportunity has been used.Reproductive health /gender-based violenceReproductive health emergencies should be attended from <strong>the</strong> early days of <strong>response</strong>.While trauma care may be <strong>the</strong> dom<strong>in</strong>ant and most visible concern <strong>in</strong> <strong>the</strong> immediateaftermath of an <strong>earthquake</strong>, deliveries and obstetrical emergencies cont<strong>in</strong>ue <strong>to</strong> occurand require un<strong>in</strong>terrupted attention <strong>to</strong> save lives. Increases <strong>in</strong> gender-based violence arealso rout<strong>in</strong>ely reported <strong>in</strong> <strong>the</strong> aftermath of most disasters. Attention <strong>to</strong> <strong>the</strong>se particularlyvulnerable groups is critical.Reproductive health careThe rate of deliveries often <strong>in</strong>creases temporarily <strong>in</strong> <strong>the</strong> first days and weeks aftera sudden-impact disaster (one might speculate that this is <strong>the</strong> result of stress).Although no data are available on <strong>the</strong> number of deliveries, <strong>in</strong>formal reports tend<strong>to</strong> confirm this observation <strong>in</strong> <strong>Haiti</strong>. Similarly, <strong>the</strong> number of pregnancies after<strong>the</strong> impact often <strong>in</strong>creases. This was noted <strong>in</strong> a survey <strong>in</strong> temporary settlementsconducted by <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong>.32FILMThe reported rate of pregnancy <strong>in</strong> a post-<strong>earthquake</strong> study was 12%. 98 Prior <strong>to</strong><strong>the</strong> <strong>earthquake</strong>, this rate was 6% nationally (4% <strong>in</strong> urban areas and 8% <strong>in</strong> ruralareas) (MSPP 2006). The very high rate observed <strong>in</strong> <strong>the</strong> camps may reflect<strong>in</strong>creased promiscuity <strong>in</strong> <strong>the</strong>se settlements, <strong>in</strong>creased <strong>in</strong>cidence of unprotectedsex <strong>in</strong> a context of disruption, and/or <strong>in</strong>adequate supply of family plann<strong>in</strong>g services.The desire for pregnancy or hav<strong>in</strong>g a child could also be expla<strong>in</strong>ed by psychologicalreasons, as is often observed after major disasters (MSPP <strong>2010</strong>b).With<strong>in</strong> days after <strong>the</strong> impact, <strong>the</strong> groups specializ<strong>in</strong>g <strong>in</strong> reproductive health <strong>in</strong>tensified<strong>the</strong>ir efforts <strong>to</strong> ensure proper attention was given <strong>to</strong> women’s health. This was <strong>in</strong>a context dom<strong>in</strong>ated by <strong>the</strong> dispatch of military trauma field hospitals or polemics onamputations and crush syndromes.With<strong>in</strong> one week, <strong>the</strong> Reproductive <strong>Health</strong> Response <strong>in</strong> Crises Consortium (RHRC)urged responders “<strong>to</strong> establish services <strong>to</strong> treat pregnancy complications, <strong>in</strong>clud<strong>in</strong>gemergency C-section, <strong>to</strong> provide immediate access <strong>to</strong> cl<strong>in</strong>ical care for survivors ofsexual violence, <strong>to</strong> resume HIV prevention, as well as <strong>to</strong> reestablish <strong>the</strong> usual familyplann<strong>in</strong>g methods.” 99A reproductive health work<strong>in</strong>g group was set up <strong>in</strong> Port-au-Pr<strong>in</strong>ce <strong>to</strong> address <strong>the</strong>seissues and a M<strong>in</strong>imum Initial Service Package for Reproductive <strong>Health</strong> was promotedthrough <strong>the</strong> timely distribution of emergency kits by UNFPA.32 32APho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>10298 A sample size of 2,391 women, 15 <strong>to</strong> 49 years old was used <strong>in</strong> this study.99 The Reproductive <strong>Health</strong> Response <strong>in</strong> Crises (RHRC) Consortium consists of seven members: American Refugee Committee(ARC), CARE, Columbia University, International Rescue Committee (IRC), John Snow Research and Tra<strong>in</strong><strong>in</strong>gInstitute (JSI), Marie S<strong>to</strong>pes International (MSI) and Women’s Refugee Commission.
BEYOND TRAUMA CARE - Chapter 6A survey of 171 cl<strong>in</strong>ics 100 serv<strong>in</strong>g temporary settlements <strong>in</strong> July <strong>2010</strong> suggests thatfive months after <strong>the</strong> impact, <strong>the</strong>re were still significant deficits <strong>in</strong> terms of <strong>the</strong> rangeof services (m<strong>in</strong>imum package) provided. Accord<strong>in</strong>g <strong>to</strong> <strong>the</strong> authors of <strong>the</strong> survey, <strong>the</strong>deficits observed were probably related <strong>to</strong> <strong>the</strong> disorganization of health care servicesand non-adherence <strong>to</strong> standards set by <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong> regard<strong>in</strong>g <strong>the</strong> m<strong>in</strong>imumpackage of services. In addition, <strong>the</strong> survey authors note that lack of availability ofcerta<strong>in</strong> services for obstetric and neonatal emergencies and sexual health may be due<strong>to</strong> <strong>the</strong> specialized nature of <strong>the</strong>se <strong>in</strong>terventions (MSPP <strong>2010</strong>b).The same survey confirmed that access <strong>to</strong> reproductive health care although not yetmeet<strong>in</strong>g m<strong>in</strong>imum standards had improved considerably <strong>in</strong> <strong>the</strong> temporary settlementscompared <strong>to</strong> <strong>the</strong> situation prior <strong>to</strong> <strong>the</strong> <strong>earthquake</strong>.Gender-based violence• Increased gender-based violence is rout<strong>in</strong>ely reported after most disasters. Although<strong>the</strong> problem was better documented after <strong>the</strong> <strong>Haiti</strong> <strong>earthquake</strong>, <strong>the</strong> lack ofquantified evidence about this issue should be addressed.• A cross-sec<strong>to</strong>ral strategy <strong>to</strong> address this chronically overlooked issue must be developedand implemented under <strong>the</strong> leadership of <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong>.In addition <strong>to</strong> <strong>the</strong> need for urgent res<strong>to</strong>ration of normal reproductive health services, an“epidemic of gender-based violence” was reported <strong>in</strong> <strong>the</strong> media and <strong>in</strong> technical reports.How significant and evidence-based this post-<strong>earthquake</strong> outbreak of gender-based violencewas is unclear. 101 Amnesty International (<strong>2010</strong>) observed: “Protection mechanismsfor women and girl victims of sexual violence were deficient before <strong>the</strong> <strong>earthquake</strong>, now<strong>the</strong>y are <strong>to</strong>tally absent. This is a major cause for under-report<strong>in</strong>g.” The report providesnumerous observations of tragic cases, but it lacks quantified evidence.Sexual violence is a much more difficult or elusive issue <strong>to</strong> document than amputationsor communicable diseases, but lack of statistics is no reason for <strong>in</strong>action. In<strong>Haiti</strong>, <strong>the</strong> magnitude of <strong>the</strong> problem before and after <strong>the</strong> <strong>earthquake</strong> prompted a largearray of <strong>in</strong>itiatives from provision of specialized medical care, <strong>in</strong>creased polic<strong>in</strong>g of <strong>the</strong>camps by <strong>the</strong> UN and National Police, <strong>to</strong> <strong>the</strong> adoption of protective measures such as<strong>the</strong> <strong>in</strong>stallation of 200 durable streetlights <strong>in</strong> 40 of <strong>the</strong> camps.In March <strong>2010</strong>, <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong> launched a national program for attention<strong>to</strong> <strong>the</strong> victims of sexual violence. Accord<strong>in</strong>g <strong>to</strong> <strong>in</strong>terviews, <strong>the</strong> pro<strong>to</strong>col proposed by<strong>the</strong> M<strong>in</strong>istry met with resistance from some NGOs who were unwill<strong>in</strong>g <strong>to</strong> change<strong>the</strong>ir own pro<strong>to</strong>col and <strong>response</strong> kits, <strong>in</strong>sist<strong>in</strong>g <strong>in</strong>stead that <strong>the</strong> national program beamended <strong>to</strong> adopt <strong>the</strong>ir approach.100 In <strong>the</strong> survey conducted by <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong> (MSPP <strong>2010</strong>b), 171 <strong>in</strong>stitutions were visited <strong>in</strong> <strong>the</strong> 12 municipalitiesaffected by <strong>the</strong> <strong>earthquake</strong> <strong>to</strong> assess <strong>the</strong> provision of care and services. Of <strong>the</strong>se, 86 were function<strong>in</strong>g <strong>in</strong>side <strong>the</strong> temporarysettlements and 85 outside. The facilities were provid<strong>in</strong>g general health care, and not exclusively reproductive health.101 The household survey carried out by <strong>the</strong> University of Michigan (Kolbe et al. <strong>2010</strong>) estimated that “<strong>in</strong> <strong>the</strong> six weeks after <strong>the</strong><strong>earthquake</strong>, 10,813 people (95% confidence <strong>in</strong>terval, 6,726–14,900) were sexually assaulted, <strong>the</strong> vast majority of whom werefemale. In <strong>the</strong> same period 4,645 <strong>in</strong>dividuals (95% confidence <strong>in</strong>terval 1,943–7,347) were physically assaulted.”103
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>There are valuable lessons <strong>to</strong> be learned from <strong>the</strong> efforts <strong>to</strong> respond <strong>to</strong> or preventsexual violence <strong>in</strong> <strong>the</strong> aftermath of <strong>the</strong> <strong>earthquake</strong>.• As noted after <strong>the</strong> tsunami, it is impossible <strong>to</strong> f<strong>in</strong>d out whe<strong>the</strong>r gender-based violencehas actually <strong>in</strong>creased (Felten-Biermann 2006). It does not, however, meanthat it does not exist.• A national strategy, whe<strong>the</strong>r for gender-based violence or o<strong>the</strong>r public health priorities,cannot be implemented unless all health ac<strong>to</strong>rs, foreign or national, accept<strong>the</strong> technical leadership of <strong>the</strong> health authorities.As is <strong>the</strong> case for o<strong>the</strong>r neglected problems, <strong>the</strong> high visibility of <strong>the</strong> <strong>response</strong> andfund<strong>in</strong>g available has shed light on ongo<strong>in</strong>g deficiencies and put <strong>in</strong><strong>to</strong> motion areform process. This reform most likely will benefit future victims of gender-basedviolence <strong>in</strong> <strong>Haiti</strong>.Supplies• Inappropriate health donations is a serious issue <strong>in</strong> all large disasters; however, thisoccurred <strong>to</strong> a lesser extent <strong>in</strong> <strong>the</strong> case of <strong>Haiti</strong>.• The existence of a central pharmaceutical warehouse managed by PAHO/WHO hasbeen an asset unmatched <strong>in</strong> o<strong>the</strong>r disaster-affected countries.How did <strong>the</strong> <strong>Haiti</strong> <strong>response</strong> compare <strong>to</strong> recent global disasters <strong>in</strong> terms of <strong>in</strong>com<strong>in</strong>ghealth supplies and procurement capacity?<strong>Haiti</strong> <strong>response</strong> faced logistics problems similar <strong>to</strong> those <strong>in</strong> o<strong>the</strong>r major humanitariandeployments <strong>in</strong> <strong>the</strong> past:• The amount of <strong>in</strong>com<strong>in</strong>g supplies (and personnel) <strong>in</strong>creased rapidly over <strong>the</strong> firstweeks.• Transport <strong>in</strong><strong>to</strong> <strong>Haiti</strong> was a major limit<strong>in</strong>g fac<strong>to</strong>r. The management of <strong>the</strong> airport <strong>in</strong>Port-au-Pr<strong>in</strong>ce and <strong>the</strong> control of <strong>Haiti</strong>an air space were rapidly assumed by <strong>the</strong> U.S.military which had its own set of security and bilateral priorities, dist<strong>in</strong>ct from thoseof <strong>the</strong> humanitarian civilian community. Critically needed medical equipment, <strong>in</strong>clud<strong>in</strong>gsome field hospitals and health teams, were rerouted through San<strong>to</strong> Dom<strong>in</strong>go<strong>in</strong> <strong>the</strong> Dom<strong>in</strong>ican Republic.• Transport with<strong>in</strong> <strong>Haiti</strong> was complicated by <strong>the</strong> destruction, rubble <strong>in</strong> <strong>the</strong> roads, and<strong>the</strong> lack of vehicles <strong>to</strong> accommodate <strong>the</strong> surge of experts and o<strong>the</strong>r personnel arriv<strong>in</strong>g<strong>in</strong> <strong>in</strong>creas<strong>in</strong>g numbers. The considerable transport assets of MINUSTAH werenot made available <strong>to</strong> <strong>the</strong> humanitarian community or even <strong>to</strong> UN agencies until<strong>the</strong> Security Council adopted a resolution mandat<strong>in</strong>g MINUSTAH <strong>to</strong> assist <strong>in</strong> thisregard (Day 7). 102102 UN Security Council Resolution 1908 was adopted on 19 <strong>January</strong> <strong>2010</strong> <strong>to</strong> “<strong>in</strong>crease <strong>the</strong> overall force levels of MINUS-TAH <strong>to</strong> support <strong>the</strong> immediate recovery, reconstruction and stability efforts”.104
BEYOND TRAUMA CARE - Chapter 6The lack of medical supplies rapidly became a major obstacle <strong>in</strong> <strong>the</strong> treatment of <strong>the</strong><strong>in</strong>jured. The items miss<strong>in</strong>g were <strong>the</strong> same reported <strong>in</strong> short supply <strong>in</strong> any <strong>earthquake</strong>:dress<strong>in</strong>gs, gauze, dis<strong>in</strong>fectant, suture material, cast<strong>in</strong>g supplies, and X-ray film. Standardemergency kits (<strong>in</strong>clud<strong>in</strong>g trauma kits) were rapidly made available, but accord<strong>in</strong>g<strong>to</strong> several <strong>in</strong>terlocu<strong>to</strong>rs <strong>the</strong>y did not adequately satisfy <strong>the</strong> most common shortages<strong>in</strong> <strong>the</strong> aftermath of a massive <strong>earthquake</strong>.One item <strong>in</strong> short supply not often mentioned <strong>in</strong> o<strong>the</strong>r disasters was external bonefixa<strong>to</strong>rs. The demand for this orthopedic equipment was unexpectedly high as conditionsfor <strong>the</strong> use of <strong>the</strong> <strong>in</strong>ternal fixa<strong>to</strong>rs (surgical skills and sterile environment) wererarely met <strong>in</strong> <strong>the</strong> first weeks. PROMESS (see below) could not meet demand for thisunusual item (unusual <strong>in</strong> <strong>the</strong> sense that it is not part of <strong>the</strong> “normal” list of essentialarticles). 103 S<strong>to</strong>ckpil<strong>in</strong>g this item globally seems <strong>to</strong> be <strong>the</strong> only practical approach.PROMESSPROMESS, <strong>the</strong> central health procurement system managed by PAHO/WHO, wasan unusual but <strong>in</strong>valuable <strong>in</strong>ternational asset <strong>in</strong> <strong>the</strong> first weeks. PROMESS facilitieshad not suffered critical damage. Its s<strong>to</strong>ck had just been replenished at <strong>the</strong> end of 2009and its personnel were serv<strong>in</strong>g not only <strong>in</strong> public <strong>in</strong>stitutions but also <strong>in</strong> eligible nonprofitfacilities or organizations. This efficient and well-tuned mechanism was <strong>in</strong> placefor support <strong>to</strong> all humanitarian health ac<strong>to</strong>rs. However, local public health offices thatwere runn<strong>in</strong>g out of s<strong>to</strong>cks were not universally aware of this service.103 With <strong>the</strong> urgent and large demand for external fixa<strong>to</strong>rs, PROMESS placed an order for 2,000 units. The amount was not excessiveconsider<strong>in</strong>g <strong>the</strong> number of fractures. However, <strong>the</strong> procurement system (centralized <strong>in</strong> PAHO/WHO HQ) was unfamiliar withsources for this specialized item, which is not rout<strong>in</strong>ely <strong>in</strong> s<strong>to</strong>ck at <strong>the</strong> usual suppliers. Ultimately, 50 units were delivered but <strong>the</strong>yarrived far <strong>to</strong>o late.PROMESS distributed essential medic<strong>in</strong>es and supplies<strong>to</strong> hospitals and <strong>in</strong>ternational and local NGOs.Pho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>105
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>In <strong>the</strong> immediate aftermath of <strong>the</strong> <strong>earthquake</strong>, PROMESS saw an average of 30 clientsper day, such as public hospitals and <strong>in</strong>ternational and local NGOs. Dur<strong>in</strong>g <strong>the</strong> first45 days, PROMESS distributed more than 345,000 boxes of essential medic<strong>in</strong>es andsupplies, <strong>in</strong>clud<strong>in</strong>g antibiotics, vacc<strong>in</strong>es, drugs for mental health conditions, drugsfor treatment of TB, diabetes and malaria, and anes<strong>the</strong>tics. In March, 100 mobilecl<strong>in</strong>ic kits were distributed <strong>in</strong> all priority areas. In early April, <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong>extended free access <strong>to</strong> medic<strong>in</strong>es until 12 July <strong>2010</strong> and PROMESS cont<strong>in</strong>ued <strong>to</strong>partner with <strong>the</strong> M<strong>in</strong>istry for <strong>the</strong> distribution of health packages <strong>to</strong> most mobile cl<strong>in</strong>ics,public hospitals, and NGOs.Several fac<strong>to</strong>rs limit<strong>in</strong>g <strong>the</strong> effectiveness of PROMESS were addressed with <strong>the</strong> suppor<strong>to</strong>f <strong>the</strong> U.S. Government:• Repair of walls surround<strong>in</strong>g <strong>the</strong> facility and improved security;• Updat<strong>in</strong>g <strong>the</strong> <strong>in</strong>ven<strong>to</strong>ry of supplies;• Organiz<strong>in</strong>g <strong>the</strong> cha<strong>in</strong> of distribution <strong>to</strong> accommodate <strong>the</strong> <strong>in</strong>creased number ofclients and <strong>the</strong> urgency of <strong>the</strong> deliveries;• Creat<strong>in</strong>g access <strong>to</strong> and space for s<strong>to</strong>rage areas by clear<strong>in</strong>g rubble.Drug donationsAccord<strong>in</strong>g <strong>to</strong> <strong>response</strong>s <strong>to</strong> specific questions dur<strong>in</strong>g <strong>in</strong>terviews and <strong>the</strong> review of technicalreports, <strong>the</strong>re is general consensus that <strong>the</strong> quality of drug donations has improved.WHO guidel<strong>in</strong>es on donations of pharmaceuticals (WHO 1999) appear <strong>to</strong>have been followed more systematically than <strong>in</strong> past disasters or <strong>in</strong> o<strong>the</strong>r regions.Progress, however, does not mean satisfac<strong>to</strong>ry performance. On Day 15, as noted <strong>in</strong><strong>the</strong> <strong>Health</strong> Cluster Bullet<strong>in</strong> (No. 8), “The majority of medic<strong>in</strong>es arriv<strong>in</strong>g <strong>in</strong><strong>to</strong> <strong>Haiti</strong>are well classified; however, <strong>the</strong>re are still a lot of medic<strong>in</strong>es without labels, expired orarriv<strong>in</strong>g as assortments, thus hamper<strong>in</strong>g distribution.”Although PROMESS required detailed <strong>in</strong>formation (list<strong>in</strong>g, expiration date, analysiscertificate) before accept<strong>in</strong>g donations, rejected supplies usually found ano<strong>the</strong>r po<strong>in</strong><strong>to</strong>f entry. The department for regula<strong>to</strong>ry authority of pharmaceuticals <strong>in</strong> <strong>the</strong> M<strong>in</strong>istryof <strong>Health</strong> rema<strong>in</strong>ed <strong>to</strong>o weak <strong>to</strong> ve<strong>to</strong> unsolicited and <strong>in</strong>appropriate donations. Thisoffice did not receive support from <strong>the</strong> <strong>in</strong>ternational community.Inappropriate donations were usually from new humanitarian ac<strong>to</strong>rs (groups with noprior experience) or new donor countries, <strong>in</strong>clud<strong>in</strong>g from <strong>the</strong> Americas. Overall, traditionaldonors and established bilateral agencies seem <strong>to</strong> have exercised stronger leadership<strong>in</strong> controll<strong>in</strong>g <strong>the</strong> quality of donations from <strong>the</strong>ir countries and constituents.L<strong>in</strong>kage with early recovery and development• It is never <strong>to</strong>o early <strong>to</strong> <strong>in</strong>itiate recovery and “build back better” <strong>in</strong> <strong>the</strong> health sec<strong>to</strong>r.• Disasters offer opportunities for change, however <strong>in</strong>cremental <strong>the</strong>y may be. Someare be<strong>in</strong>g used <strong>in</strong> <strong>Haiti</strong>.106
BEYOND TRAUMA CARE - Chapter 6In this section, <strong>the</strong> outlook will project beyond <strong>the</strong> <strong>in</strong>itial three-month period. It willattempt <strong>to</strong> determ<strong>in</strong>e <strong>the</strong> impact of <strong>the</strong> early <strong>response</strong> on <strong>the</strong> recovery and reconstructionprocess <strong>in</strong> <strong>Haiti</strong>.Initial relief activities have a justification and dynamic of <strong>the</strong>ir own. Designed <strong>to</strong>save lives, <strong>the</strong>y can truly do so or also evolve <strong>in</strong><strong>to</strong> development-like activities. Theymay be carried out <strong>in</strong> a manner that ei<strong>the</strong>r prepares <strong>the</strong> ground for, and blends <strong>in</strong><strong>to</strong>recovery and reconstruction processes, or that complicates that process.Early recovery represents <strong>the</strong> undef<strong>in</strong>ed border or transition between emergency reliefand reconstruction. Whe<strong>the</strong>r it is an extended humanitarian function or an <strong>in</strong>itial step<strong>to</strong>ward post-impact development is a matter both of perspective and orig<strong>in</strong> of fund<strong>in</strong>g:that is, humanitarian/emergency or development (World Bank 2008, 31–32).Over <strong>the</strong> last decade, development ac<strong>to</strong>rs have become more proactive and rapid <strong>in</strong> trigger<strong>in</strong>g<strong>the</strong> reconstruction process, overlapp<strong>in</strong>g <strong>in</strong> time with <strong>the</strong> immediate <strong>response</strong>. The economicvaluation of damage developed by <strong>the</strong> Economic Commission for Lat<strong>in</strong> Americaand <strong>the</strong> Caribbean (ECLAC) used <strong>to</strong> be launched more than a month after impact; it isnow promoted with<strong>in</strong> a few weeks. In Indonesia, <strong>the</strong> <strong>in</strong>ternational f<strong>in</strong>ancial <strong>in</strong>stitutions<strong>in</strong>itiated economic assessment with<strong>in</strong> three weeks, <strong>in</strong>volv<strong>in</strong>g a large number of expertssupported by recent local graduates. There were more experts compil<strong>in</strong>g, scrut<strong>in</strong>iz<strong>in</strong>g, andvalidat<strong>in</strong>g f<strong>in</strong>ancial and cost data from all sources than were employed <strong>to</strong> ga<strong>the</strong>r and compile<strong>response</strong> <strong>in</strong>telligence. A similar effort was launched <strong>in</strong> Sri Lanka and Pakistan.In <strong>Haiti</strong>, <strong>the</strong> same approach resulted <strong>in</strong> early plann<strong>in</strong>g for a Post-Disaster Needs Assessment(PDNA). Twenty years ago, early recovery and reconstruction were an afterthough<strong>to</strong>nce relief was near completion; <strong>in</strong> <strong>Haiti</strong> it was pushed <strong>to</strong> early <strong>in</strong> <strong>the</strong> agenda.On 19 <strong>January</strong> (Day 7) <strong>the</strong> Early Recovery Cluster was activated <strong>in</strong> <strong>Haiti</strong>.The two processes (<strong>response</strong> and reconstruction) may run <strong>in</strong>dependently or be closelyl<strong>in</strong>ked <strong>to</strong>ge<strong>the</strong>r. The l<strong>in</strong>kage between relief, rehabilitation, and development (LRRD)was a feature present <strong>in</strong> this emergency. This l<strong>in</strong>kage is an asset for agencies with botha strong development mandate and an emergency <strong>response</strong> capacity.There were strengths as well as shortcom<strong>in</strong>gs <strong>in</strong> this l<strong>in</strong>kage.Success s<strong>to</strong>ries <strong>in</strong> LRRDReconstruction, which is development, is meet<strong>in</strong>g considerable obstacles <strong>in</strong> <strong>Haiti</strong>. Themost brilliant schemes cannot succeed without some modicum of efficient governmentwith authority regard<strong>in</strong>g its partners.While most “ambitious new ideas” articulated by <strong>the</strong> PDNA process have not beenimplemented, <strong>the</strong> seeds of many <strong>in</strong>cremental <strong>the</strong>matic changes have been planted <strong>in</strong><strong>Haiti</strong>. Preexist<strong>in</strong>g but dormant <strong>in</strong>itiatives for change were reactivated, promoted, and<strong>in</strong> some cases funded. Progress <strong>in</strong> some <strong>in</strong>itiatives may not last but o<strong>the</strong>rs will changepublic health <strong>in</strong> <strong>Haiti</strong>. The <strong>in</strong>itial successes are listed below. Most have been discussedearlier. None is revolutionary, but development is always <strong>in</strong>cremental.• Free access <strong>to</strong> primary health care— <strong>the</strong> SIG and <strong>the</strong> SOG: Before <strong>the</strong> impact of <strong>the</strong><strong>earthquake</strong>, modest efforts were under way by WHO <strong>to</strong> conclude compensation107
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>agreements with <strong>in</strong>dividual non-profit <strong>in</strong>stitutions will<strong>in</strong>g <strong>to</strong> provide free obstetriccare (So<strong>in</strong>s Obstétricaux Gratuits, or SOG) (WHO <strong>2010</strong>d). It was a strong departurefrom a rigidly enforced, albeit poorly controlled user-fee policy on whichlocal health facilities became dependent for most of <strong>the</strong>ir operations. The SOGprogram was made operational aga<strong>in</strong> after February <strong>2010</strong> with a simplified activityreport<strong>in</strong>g mechanism. It not only cont<strong>in</strong>ued <strong>to</strong> provide free-of-charge obstetriccare <strong>to</strong> pregnant women right after <strong>the</strong> <strong>earthquake</strong>, but dur<strong>in</strong>g <strong>2010</strong> it expanded<strong>the</strong> content of <strong>the</strong> health package, becom<strong>in</strong>g <strong>the</strong> SOG-2 <strong>in</strong> July <strong>2010</strong>. Sixty-threehealth <strong>in</strong>stitutions are currently provid<strong>in</strong>g services under <strong>the</strong> program all over <strong>the</strong>country. As a result, <strong>the</strong> number of <strong>in</strong>stitutional deliveries has <strong>in</strong>creased from anaverage of 2,953 per month <strong>in</strong> 2007 <strong>to</strong> an estimated 6,828 per month <strong>in</strong> <strong>2010</strong> <strong>in</strong>participat<strong>in</strong>g <strong>in</strong>stitutions (PAHO/WHO 2011a). 104The SIG program (So<strong>in</strong>s Infantiles Gratuits) provides free care for children underage 5 thanks <strong>to</strong> a f<strong>in</strong>ancial agreement with public and private hospitals similar <strong>to</strong>that of <strong>the</strong> SOG. It was launched and implemented after <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> order<strong>to</strong> ease <strong>the</strong> f<strong>in</strong>ancial difficulties be<strong>in</strong>g experienced by both <strong>the</strong> general populationand <strong>the</strong> health facilities. Twenty-seven of <strong>the</strong> largest hospitals <strong>in</strong> <strong>the</strong> countryengaged <strong>in</strong> SIG between July and November <strong>2010</strong>. Dur<strong>in</strong>g this time more than15,000 children beyond <strong>the</strong> base l<strong>in</strong>e numbers had <strong>the</strong> opportunity <strong>to</strong> access qualitycare with dignity.The temporary support for <strong>the</strong>se programs from humanitarian fund<strong>in</strong>g was substitutedby a development grant ensur<strong>in</strong>g <strong>the</strong> susta<strong>in</strong>ability of free access <strong>to</strong> care forthose groups. 105• Mental health: As discussed above, a new community-based approach is complement<strong>in</strong>g<strong>the</strong> traditional third level hospital-based care of mental health. This represents achange of attitude and approach which is likely <strong>to</strong> last.• Rehabilitation and acceptance of disabilities: The <strong>earthquake</strong> also <strong>in</strong>duced a significantchange of perception and policies regard<strong>in</strong>g disabilities <strong>in</strong> <strong>Haiti</strong>. It is a profoundand permanent modification of public behavior. Institutional changes willfollow.• Awareness of gender-based violence: The emergency provided an opportunity for<strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong> <strong>to</strong> develop a strategy, albeit still under debate, <strong>to</strong> providestandardized care for victims of gender-based violence. It has shed light on thislong-stand<strong>in</strong>g problem that has largely been overlooked.• Communicable diseases surveillance and control: The establishment of a surveillancesystem based on 51 sent<strong>in</strong>el stations is a first for <strong>Haiti</strong>. Although late and fraughtwith serious quality issues, this experience has re<strong>in</strong>forced <strong>the</strong> Epidemiology Departmen<strong>to</strong>f <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong>. The importance of fur<strong>the</strong>r streng<strong>the</strong>n<strong>in</strong>g thisdepartment was demonstrated <strong>in</strong> <strong>the</strong> cholera outbreak late <strong>in</strong> <strong>2010</strong>.104 Some NGOs, as a matter of <strong>in</strong>ternal policy, were deliver<strong>in</strong>g free care without formally adher<strong>in</strong>g <strong>to</strong> <strong>the</strong> SOG.105 On a more <strong>in</strong>ternational scale, <strong>the</strong> SIG and SOG programs contributed <strong>to</strong> <strong>the</strong> IASC Global <strong>Health</strong> Cluster position recommend<strong>in</strong>gremoval of user fees for primary health care dur<strong>in</strong>g humanitarian crises. See IASC (<strong>2010</strong>b).108
BEYOND TRAUMA CARE - Chapter 6• Water services: DINEPA, a relatively strong <strong>in</strong>stitution responsible for water distribution<strong>in</strong> <strong>Haiti</strong>, has emerged stronger from <strong>the</strong> disaster <strong>response</strong>. The qualityof services offered <strong>to</strong> <strong>in</strong>ternally displaced populations (IDPs) by <strong>in</strong>ternationalpartners exceeded that available <strong>in</strong> non-affected areas. The long-term benefit hasbeen shown aga<strong>in</strong> dur<strong>in</strong>g <strong>the</strong> subsequent cholera outbreak. Morbidity and mortalityrates <strong>in</strong> temporary settlements were considerably lower <strong>in</strong> <strong>the</strong> IDP settlements.• Nutrition: Accord<strong>in</strong>g <strong>to</strong> UNICEF, <strong>the</strong> emergency gave nutrition issues higher priorityat <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong> and provided opportunities <strong>to</strong> streng<strong>the</strong>n programsat <strong>the</strong> department level.• Decentralization of management and services: The <strong>response</strong> <strong>to</strong> <strong>the</strong> emergency contributed<strong>to</strong> revitaliz<strong>in</strong>g <strong>the</strong> trend <strong>to</strong>ward decentralization of services <strong>to</strong> departmentsand <strong>the</strong> community level. The central level may have been weakened by <strong>the</strong><strong>in</strong>ternational <strong>response</strong>, but <strong>the</strong> local level has probably benefitted <strong>in</strong> terms of visibilityand direct access <strong>to</strong> <strong>the</strong> <strong>in</strong>ternational community. This has led <strong>to</strong> a renewalof <strong>the</strong> debate at <strong>the</strong> national level.• Reduction of vulnerability <strong>to</strong> <strong>earthquake</strong>s: As is common after major <strong>earthquake</strong>s,awareness and commitment <strong>to</strong> disaster risk reduction <strong>in</strong>creased considerably. Thenew health facilities (repaired or reconstructed) will comply with safety norms <strong>in</strong><strong>the</strong> process of review. A jo<strong>in</strong>t World Bank and PAHO/WHO project will promoteand moni<strong>to</strong>r <strong>the</strong> development of guidel<strong>in</strong>es and <strong>the</strong> implementation of <strong>the</strong> concep<strong>to</strong>f safe hospitals as part of <strong>the</strong> reconstruction process.In <strong>Haiti</strong>, <strong>the</strong> tragedy offered an impetus for <strong>in</strong>cremental change <strong>in</strong> <strong>the</strong> medium-term.Shortcom<strong>in</strong>gs <strong>in</strong> LRRDSeveral aspects of <strong>the</strong> <strong>response</strong> <strong>in</strong> <strong>the</strong> first months were not supportive of a successfuland rapid recovery. The most noticeable were <strong>the</strong> lack of NGO support <strong>to</strong> M<strong>in</strong>istryof <strong>Health</strong> strategic and policy <strong>in</strong>itiatives, <strong>the</strong> practice of “poach<strong>in</strong>g” human resources,<strong>the</strong> closure of a private for-profit hospital, and <strong>the</strong> weaken<strong>in</strong>g of <strong>the</strong> role and potentialleadership of national <strong>in</strong>stitutions.• The M<strong>in</strong>istry of <strong>Health</strong> had little leverage over <strong>the</strong> immediate <strong>response</strong> by NGOsand o<strong>the</strong>r ac<strong>to</strong>rs. It focused pragmatically on recovery plann<strong>in</strong>g. Strategies andnorms were developed only <strong>to</strong> be ignored or <strong>in</strong> some <strong>in</strong>stances contradicted byNGOs that were supposed <strong>to</strong> be implementers. While reconstruction and developmentcannot be dictated by overly detailed plann<strong>in</strong>g at <strong>the</strong> central level, nei<strong>the</strong>rcan it come about when <strong>the</strong>re is systematic disregard of <strong>the</strong> technical norms andstandards provided by l<strong>in</strong>e m<strong>in</strong>istries.• The practice of recruit<strong>in</strong>g national health professionals from local health services,or “poach<strong>in</strong>g,” is common <strong>in</strong> all major natural disasters or conflicts. In <strong>the</strong> medium-term,as <strong>in</strong>dicated earlier, this practice seriously weakens <strong>the</strong> recovery capacityof <strong>the</strong> country.Attempts by <strong>the</strong> M<strong>in</strong>istry and <strong>the</strong> <strong>Health</strong> Cluster <strong>to</strong> agree upon a standard approachregard<strong>in</strong>g this recruitment and salaries were never seriously considered by <strong>the</strong> majormedical NGOs that were compet<strong>in</strong>g among <strong>the</strong>mselves (and with <strong>the</strong> UN) for <strong>the</strong>109
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>services of <strong>the</strong> few local health professionals available. It was a market where <strong>the</strong> demandfar exceeded <strong>the</strong> local offer. Qualified personnel were recruited not only from<strong>the</strong> public sec<strong>to</strong>r but also from <strong>the</strong> dedicated local NGOs unable <strong>to</strong> match salariesoffered by <strong>in</strong>ternational NGOs. There is no easy solution when <strong>the</strong> humanitarian<strong>in</strong>dustry operates <strong>in</strong> an unregulated, free market mode.• The bankruptcy of a major private facility has ended an era of open<strong>in</strong>g <strong>the</strong> forprofitsec<strong>to</strong>r <strong>to</strong> poor patients. The Centre de diagnostic et traitement <strong>in</strong>tégré (CDTI)closed on 1 April, a situation <strong>in</strong> which everyone loses. S<strong>in</strong>ce <strong>the</strong> first hours after <strong>the</strong>impact, this hospital offered free emergency care <strong>to</strong> <strong>the</strong> affected population. CDTIreported treat<strong>in</strong>g 10,500 patients and perform<strong>in</strong>g some 2,000 surgical <strong>in</strong>terventions<strong>in</strong> 10 weeks. 106In an <strong>in</strong>terview with <strong>the</strong> Nouvelliste, <strong>the</strong> ma<strong>in</strong> newspaper <strong>in</strong> <strong>Haiti</strong>, <strong>the</strong> CDTI direc<strong>to</strong>rclaimed “We did not receive any emergency funds dur<strong>in</strong>g <strong>the</strong> three monthsof services that we offered.” 107 However, this <strong>in</strong>stitution did receive an importantamount of assistance <strong>in</strong> <strong>the</strong> form of essential medical supplies, equipment, and humanresources. In fact, CDTI experienced severe economic difficulties long before<strong>the</strong> <strong>earthquake</strong>. The issue is not one hospital’s fate but <strong>the</strong> fact that <strong>the</strong> <strong>in</strong>ternationalcommunity is ill-equipped <strong>to</strong> deal with <strong>the</strong> issue of monetary compensation for<strong>the</strong> care provided at no cost by <strong>the</strong> for-profit sec<strong>to</strong>r. This issue should be addressedespecially <strong>in</strong> situations where <strong>the</strong> role of a particular facility is critical.• The weaken<strong>in</strong>g of health <strong>in</strong>stitutions will be discussed <strong>in</strong> more detail <strong>in</strong> <strong>the</strong> sectionon national coord<strong>in</strong>ation <strong>in</strong> Chapter 8.106 Interest<strong>in</strong>gly, some NGO <strong>in</strong>terlocu<strong>to</strong>rs praised <strong>the</strong> quality of care and noted that it was one of <strong>the</strong> few facilities with aproper balance <strong>in</strong> <strong>the</strong> number of doc<strong>to</strong>rs and nurses.107 The Nouvelliste. 6 April <strong>2010</strong>.110
Chapter7Informationmanagement• Information management, <strong>in</strong>clud<strong>in</strong>g <strong>in</strong> <strong>the</strong> health sec<strong>to</strong>r, appears <strong>to</strong> be one of <strong>the</strong>weakest po<strong>in</strong>ts of <strong>response</strong> <strong>in</strong> past disasters. The situation is compounded by <strong>the</strong>proliferation of general ac<strong>to</strong>rs as well as agencies address<strong>in</strong>g highly specific needs.• Considerably more human resources should be dedicated <strong>to</strong> <strong>in</strong>telligence ga<strong>the</strong>r<strong>in</strong>g:<strong>the</strong> one who is best <strong>in</strong>formed is <strong>the</strong> one with <strong>the</strong> moral authority <strong>to</strong> coord<strong>in</strong>ate.• Coord<strong>in</strong>ation cannot be effective <strong>in</strong> <strong>the</strong> absence of actionable <strong>in</strong>formation.Disaster management is essentially <strong>in</strong>formation management. The ma<strong>in</strong> difference betweendecision mak<strong>in</strong>g <strong>in</strong> crises versus <strong>in</strong> normal situations is not so much <strong>the</strong> humanitarianconsequences but <strong>the</strong> higher levels of uncerta<strong>in</strong>ty. Decisions <strong>in</strong> sudden-onsetdisasters need <strong>to</strong> be made with limited or no accurate factual <strong>in</strong>formation. Therefore,emotions, <strong>in</strong>stitutional <strong>in</strong>terests, or political considerations often prevail.The Global <strong>Health</strong> Cluster led by WHO developed a list of suggested core health<strong>in</strong>dica<strong>to</strong>rs. 108 Few of <strong>the</strong>m were collected and moni<strong>to</strong>red before <strong>the</strong> impact, least of allunder <strong>the</strong> chaotic conditions and extreme pressure for immediate action.108 See IASC, Global <strong>Health</strong> Cluster (2009), “Global health cluster suggested set of core <strong>in</strong>dica<strong>to</strong>rs and benchmarks by category.”111
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Information needsInformation needs are not limited <strong>to</strong> <strong>the</strong> traditional <strong>in</strong>dica<strong>to</strong>rs of number of dead (afigure of no practical immediate value), <strong>the</strong> number of <strong>in</strong>jured (when compiled, itis often <strong>to</strong>o late for action), <strong>the</strong> number of homeless or IDPs (elusive but actionabledata), and <strong>the</strong> number of damaged build<strong>in</strong>gs/houses. What is needed is relativelyspecific <strong>in</strong>formation on <strong>the</strong> extent of additional and critical human needs caused by<strong>the</strong> disaster, and <strong>the</strong> amount of resources already on site or <strong>in</strong> <strong>the</strong> pipel<strong>in</strong>e <strong>to</strong> address<strong>the</strong>m. Too often, <strong>the</strong> assumption is that local capacity is overwhelmed or non-existent.This perception was unfortunately more accurate <strong>in</strong> <strong>the</strong> case of <strong>the</strong> 12 <strong>January</strong> <strong>earthquake</strong><strong>in</strong> <strong>Haiti</strong> than for <strong>the</strong> disasters <strong>in</strong> Indonesia, Pakistan, and Sri Lanka, where localresources and solidarity were severely underestimated or discounted by <strong>the</strong> <strong>in</strong>ternationalcommunity.What matters are not <strong>the</strong> needs per se, but those needs that cannot be met with exist<strong>in</strong>gresources.The <strong>in</strong>itial rapid assessment• In <strong>the</strong> <strong>in</strong>itial “rapid” assessment, speed should prevail over perfection.• Democratic consensus on all <strong>in</strong>dica<strong>to</strong>rs and <strong>in</strong>clusiveness are <strong>in</strong>compatible with speed.Leave well enough alone.• Assessments must lead <strong>to</strong> decision-mak<strong>in</strong>g by compar<strong>in</strong>g observed needs wi<strong>the</strong>xist<strong>in</strong>g capacity <strong>in</strong> light of practical constra<strong>in</strong>ts.In catastrophic disasters such as <strong>the</strong> Indian Ocean tsunami or <strong>the</strong> <strong>earthquake</strong>s <strong>in</strong> Pakistanand <strong>Haiti</strong>, humanitarian partners will immediately deploy <strong>the</strong>ir assistance, beforeany data can be compiled and validated.Needs can take many forms and change rapidly over time and place. Response (localor <strong>in</strong>ternational) may rapidly meet some of <strong>the</strong> needs, render<strong>in</strong>g fur<strong>the</strong>r <strong>in</strong>terventionoff target or counterproductive; some life-sav<strong>in</strong>g needs or vulnerable groups may beoverlooked. An <strong>in</strong>tersec<strong>to</strong>ral (<strong>in</strong>teragency) <strong>in</strong>itial rapid assessment (IRA) should be<strong>the</strong> first step before more decisive and specific action is taken. It is potentially a critical<strong>to</strong>ol for sett<strong>in</strong>g up broad priority areas <strong>to</strong> guide <strong>the</strong> global humanitarian <strong>response</strong>.Speed is more important than comprehensiveness or high accuracy. Information from a“quick and dirty survey,” <strong>to</strong> borrow an epidemiological term, should be available beforedonors and agencies have made all <strong>the</strong>ir decisions. It is better <strong>to</strong> have 60% confidence <strong>in</strong>data before <strong>the</strong> decision, than <strong>to</strong> wait two weeks for 95% statistical probability.The IRAs <strong>in</strong> <strong>Haiti</strong> and <strong>in</strong> <strong>the</strong> tsunami-affected countries present both extremes. In <strong>the</strong>case of <strong>the</strong> tsunami, <strong>the</strong> <strong>in</strong>itial assessment was rapid but so sketchy (a few pages) as <strong>to</strong>be of little use. In <strong>Haiti</strong>, <strong>the</strong> pursuit of technical perfection resulted <strong>in</strong> data that were<strong>to</strong>o complex and <strong>to</strong>o late <strong>to</strong> assist partners with operational decision mak<strong>in</strong>g.In <strong>Haiti</strong>, a specific IRA, called <strong>the</strong> Rapid Initial Needs Assessment for <strong>Haiti</strong> (RI-NAH), was launched on 23 <strong>January</strong>. To speed up <strong>the</strong> process, pre-agreed <strong>in</strong>ternational112
INFORMATION MANAGEMENT- Chapter 7templates for IRAs were developed—and not used. Attempts <strong>to</strong> achieve consensuson areas of concern and priorities of all key ac<strong>to</strong>rs led <strong>to</strong> lengthy negotiations amongpartners. As often is <strong>the</strong> case, <strong>the</strong> large number of parties <strong>in</strong> <strong>the</strong> discussion resulted <strong>in</strong>an <strong>in</strong>flated questionnaire <strong>in</strong>clud<strong>in</strong>g someth<strong>in</strong>g for every agency’s concern regardless ofits relevance (<strong>in</strong> terms of importance or tim<strong>in</strong>g) for <strong>the</strong> beneficiaries.Committee-driven design is particularly slow, as can be seen from <strong>the</strong> sequence below:• Day 12 (23 <strong>January</strong>): The actual fieldwork for <strong>the</strong> assessment began; it concludedon 6 February.• Day 29 (9 February): The <strong>Health</strong> Cluster reported: “<strong>the</strong> Rapid Initial Needs Assessmentfor <strong>Haiti</strong> (RINAH) 109 evaluated several sec<strong>to</strong>rs <strong>in</strong>clud<strong>in</strong>g water, hygiene,security, and sanitation, visit<strong>in</strong>g 108 locations with<strong>in</strong> Port-au-Pr<strong>in</strong>ce and 98 locationsoutside of Port-au-Pr<strong>in</strong>ce. Data are still be<strong>in</strong>g assimilated and analyzed andwill be made available soon.” 110• Day 39 (19 February): Announcements were made that a Revised Flash Appeal(<strong>the</strong> jo<strong>in</strong>t process for emergency fund rais<strong>in</strong>g) had been issued. 111 It would be assumedthat <strong>the</strong> prelim<strong>in</strong>ary results of RINAH, although not officially released,were used <strong>in</strong> this process. At <strong>the</strong> same time three o<strong>the</strong>r assessments of <strong>in</strong>terest <strong>to</strong><strong>the</strong> health sec<strong>to</strong>r were completed or launched:• Key health partners who ma<strong>in</strong>ta<strong>in</strong> networks of service providers <strong>in</strong> <strong>Haiti</strong> conductedan assessment of <strong>the</strong> impact of <strong>the</strong> <strong>earthquake</strong> on <strong>the</strong>ir service delivery;• A rapid assessment was carried out by <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong> with supportfrom UNAIDS on <strong>the</strong> delivery of services for prevention of mo<strong>the</strong>r-<strong>to</strong>-childtransmission of AIDS <strong>in</strong> West Department;• The Post-Disaster Needs Assessment (PDNA) was be<strong>in</strong>g organized by <strong>the</strong><strong>Haiti</strong> government <strong>to</strong> guide recovery.• On Day 45 (25 February), results of <strong>the</strong> RINAH (data with hundreds of tablesand graphs) were released <strong>to</strong> all partners. Meanwhile, at <strong>the</strong> request of <strong>the</strong> M<strong>in</strong>istryof <strong>Health</strong>, an “emergency health <strong>in</strong>formation cell” was meet<strong>in</strong>g with<strong>in</strong> <strong>the</strong> <strong>Health</strong>Cluster <strong>to</strong> “assemble clearer <strong>in</strong>formation on <strong>the</strong> health situation <strong>in</strong> <strong>the</strong> country.”The methodology suffered from some design flaws: a questionnaire unsuitable for <strong>the</strong><strong>Haiti</strong>an context and language; a list of questions that were far <strong>to</strong>o long (<strong>in</strong>terviewslasted three hours); and some confusion between an assessment of <strong>the</strong> impact of <strong>the</strong><strong>earthquake</strong> or of <strong>the</strong> ongo<strong>in</strong>g poverty (CDC <strong>2010</strong>a). The “severe security restrictionsimposed by <strong>the</strong> UN.” were also seen as an important fac<strong>to</strong>r delay<strong>in</strong>g this and o<strong>the</strong>rrapid assessments (ACAPS <strong>2010</strong>, Grünewald and Renaud<strong>in</strong> <strong>2010</strong>).The f<strong>in</strong>ancial costs (estimated at US$ 3 million) and <strong>the</strong> resources required (128 workers,18 evalua<strong>to</strong>rs, 23 helicopters, and 51 vehicles) were disproportionate <strong>in</strong> view of109 Assessment Capacities Project (ACAPS), Rapid <strong>in</strong>itial needs assessment for <strong>Haiti</strong> (RINAH). Conducted 23 <strong>January</strong>-6February <strong>2010</strong>.110 <strong>Health</strong> Cluster Bullet<strong>in</strong> No. 19, 11 February <strong>2010</strong>.111 The revised flash appeal did not make mention of <strong>the</strong> RINHA but expected more <strong>in</strong>formation on longer term needs <strong>to</strong> be<strong>in</strong>cluded <strong>in</strong> <strong>the</strong> Post Disaster Needs Assessment (PDNA), which had not yet been launched.113
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong><strong>the</strong> lack of use of <strong>the</strong> results. The RINAH was only <strong>the</strong> first of 10 cross-sec<strong>to</strong>r surveys.But more serious is <strong>the</strong> fact that <strong>the</strong>se exercises systematically forget that needs assessmentis not enough: Capacity assessment (exist<strong>in</strong>g resources and those <strong>in</strong> <strong>the</strong> pipel<strong>in</strong>e) andproper analysis of constra<strong>in</strong>ts are essential components if <strong>the</strong> <strong>in</strong>itial assessments are <strong>to</strong> beof any value <strong>to</strong> decision makers. These two elements were mostly miss<strong>in</strong>g <strong>in</strong> <strong>in</strong>itial assessmentscarried out <strong>in</strong> <strong>the</strong> disasters under review.These issues and problems were not specific <strong>to</strong> <strong>Haiti</strong>. After <strong>the</strong> Indian Ocean tsunami,<strong>the</strong> evalua<strong>to</strong>rs for <strong>the</strong> Tsunami Evaluation Commission (TEC) found that most of <strong>the</strong><strong>in</strong>teragency assessments failed <strong>to</strong> <strong>in</strong>fluence decision makers and donors. It should be notedthat <strong>in</strong> past disasters <strong>in</strong>vestments <strong>in</strong> time and resources for <strong>the</strong> rapid assessment have beenfar more modest. Add<strong>in</strong>g resources and funds did not contribute <strong>to</strong> better <strong>in</strong>formation orbenefit <strong>the</strong> <strong>response</strong> <strong>in</strong> <strong>Haiti</strong>.The Post-Disaster Needs Assessment (PDNA)• Government ownership is essential: The PDNA is a valuable exercise <strong>to</strong> <strong>the</strong> extentthat it builds on <strong>the</strong> capacity of <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong> and focuses <strong>the</strong> Governmentand its partners on health sec<strong>to</strong>r reconstruction early on. It should determ<strong>in</strong>e <strong>the</strong>shape of <strong>the</strong> health system that will emerge after <strong>the</strong> disaster.• Broad participation of <strong>the</strong> health sec<strong>to</strong>r <strong>in</strong> <strong>the</strong> cross-sec<strong>to</strong>ral recovery process iscritical <strong>to</strong> ensure that basic health needs and priorities receive adequate attention<strong>in</strong> <strong>the</strong> rehabilitation and recovery process.The PDNA process is comprehensive and <strong>the</strong>refore also time-consum<strong>in</strong>g. 112 It pulls<strong>to</strong>ge<strong>the</strong>r <strong>in</strong>formation on <strong>the</strong> physical impacts of a disaster, <strong>the</strong> economic value of <strong>the</strong>damage (replacement cost) and losses (<strong>in</strong>come or services), and <strong>the</strong> human impacts asexperienced by <strong>the</strong> affected population.One of <strong>the</strong> assets of <strong>the</strong> PDNA is its ownership by <strong>the</strong> government of <strong>the</strong> affectedcountry. Although promoted and supported by <strong>the</strong> <strong>in</strong>ternational community (UN,<strong>the</strong> World Bank, regional f<strong>in</strong>ancial <strong>in</strong>stitutions, <strong>the</strong> EC, and o<strong>the</strong>rs), <strong>the</strong> PDNAshould be requested and led by <strong>the</strong> government.In <strong>Haiti</strong>, as early as on Day 7 <strong>in</strong>itial approaches were made for a scop<strong>in</strong>g mission before<strong>the</strong> end of <strong>January</strong>. 113 However, <strong>the</strong> formal request was delayed until 16 Februaryas <strong>the</strong> Government required changes <strong>in</strong> <strong>the</strong> Terms of Reference <strong>in</strong> order <strong>to</strong> assumetrue ownership.As is often <strong>the</strong> case, balance shifted excessively <strong>to</strong>wards <strong>in</strong>frastructure when many of<strong>the</strong> challenges were <strong>in</strong> <strong>the</strong> development of human resources and <strong>in</strong>stitutional build<strong>in</strong>g.The PDNA was also <strong>in</strong>fluenced (some said “carried away”) by <strong>the</strong> anticipationof pledges, which, as seen from past disasters, do not fully materialize. The effec-112 In <strong>Haiti</strong>, <strong>the</strong> <strong>in</strong>itial draft of <strong>the</strong> health section required <strong>the</strong> full time efforts of several experts from UNICEF, UNFPA,<strong>the</strong> Interim <strong>Haiti</strong> Recovery Commission (IHRC), <strong>the</strong> Cl<strong>in</strong><strong>to</strong>n Foundation, and CIDA as well as three professionals fromWHO for up <strong>to</strong> four weeks. Over 15 professionals from <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong> were <strong>in</strong>volved on a daily basis, one almostfull-time.113 At least twice earlier than <strong>in</strong> <strong>the</strong> aftermath of o<strong>the</strong>r disasters (Pakistan <strong>earthquake</strong> and Indian Ocean tsunami).114
INFORMATION MANAGEMENT- Chapter 7tiveness of <strong>the</strong> document itself (ra<strong>the</strong>r than <strong>the</strong> process) <strong>in</strong> guid<strong>in</strong>g and <strong>in</strong>fluenc<strong>in</strong>gdonors is seen as limited. Key donors participated proactively <strong>in</strong> <strong>the</strong> process, butmost had probably already established <strong>the</strong>ir own priorities.Accord<strong>in</strong>g <strong>to</strong> some <strong>in</strong>terlocu<strong>to</strong>rs, <strong>the</strong> product was an “<strong>in</strong>spirational document withambitious new ideas and horizons.” However, most of <strong>the</strong>se “new” ideas were alreadypiloted somewhere <strong>in</strong> <strong>Haiti</strong>. In <strong>the</strong> health sec<strong>to</strong>r, an effort was made not <strong>to</strong> <strong>in</strong>troducepolicy directions that were completely alien.Success s<strong>to</strong>ries <strong>in</strong> recovery (LRRD) such as decentralization of services, provision ofsome health services at no cost (obstetric and pediatric), and o<strong>the</strong>rs were advocated<strong>in</strong> <strong>the</strong> PDNA and <strong>the</strong>refore facilitated. A positive result of this exercise was reach<strong>in</strong>gconsensus <strong>in</strong> <strong>the</strong> health sec<strong>to</strong>r on <strong>the</strong> <strong>in</strong>terim (six-month) health plan developed by<strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong>. 114The experience ga<strong>in</strong>ed <strong>in</strong> <strong>Haiti</strong> will be valuable <strong>to</strong> guide <strong>the</strong> health recovery process <strong>in</strong>future disasters (WHO <strong>2010</strong>c).Specific assessments• Consolidated <strong>in</strong>formation management should be <strong>the</strong> utmost priority <strong>in</strong> future disasters.• Considerable human resources are required <strong>to</strong> transform <strong>the</strong> numerous surveysand assessments <strong>in</strong><strong>to</strong> collective strategic plann<strong>in</strong>g.In <strong>Haiti</strong>, as <strong>in</strong> countries affected by o<strong>the</strong>r major disasters, <strong>the</strong>re was a proliferation ofspecific surveys and assessments, almost as many as <strong>the</strong>re were ac<strong>to</strong>rs or problems <strong>to</strong>be addressed. The challenge of compil<strong>in</strong>g and <strong>in</strong>terpret<strong>in</strong>g <strong>the</strong> results was overwhelm<strong>in</strong>g.A work<strong>in</strong>g group on <strong>in</strong>formation management was established with<strong>in</strong> <strong>the</strong> <strong>Health</strong>Cluster, a Google group on assessment was led by OCHA <strong>to</strong> set up and update a“Survey of Surveys,” 115 while as noted before, an “emergency health <strong>in</strong>formation cell”was established by <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong>.The need for timely <strong>in</strong>formation was <strong>in</strong>satiable: Who is do<strong>in</strong>g what, where (3Ws)? Are<strong>the</strong> exist<strong>in</strong>g health facilities operational? Which key supplies are needed? What donationshave been received and are potentially available? Where are <strong>the</strong> field hospitalsand what are <strong>the</strong>ir capabilities? How many temporary settlements and with how manypeople (when new ones were spontaneously created every day)? How many peoplemigrated <strong>to</strong>ward departments and what is <strong>the</strong> absorption capacity of <strong>the</strong>ir services?What is <strong>the</strong> impact on food s<strong>to</strong>cks, <strong>in</strong>come, and availability and needs? What is <strong>the</strong>water availability and quality <strong>in</strong> camps and hospitals?The list of queries fluctuated and expanded day-by-day. Agencies and clusters attempted<strong>to</strong> respond separately <strong>to</strong> many of those questions. Those m<strong>in</strong>i-assessments may not114 <strong>Haiti</strong>, M<strong>in</strong>istry of <strong>Health</strong> (<strong>2010</strong>), Plan <strong>in</strong>térimaire du secteur santé: Mars <strong>2010</strong> - Septembre 2011.115 As noted <strong>in</strong> <strong>the</strong> <strong>Health</strong> Cluster Bullet<strong>in</strong> No. 22 (22 February <strong>2010</strong>).115
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>have provided <strong>the</strong> comprehensive view required for strategic orientation at <strong>the</strong> macrolevel, but <strong>in</strong> most <strong>in</strong>stances <strong>the</strong>y met <strong>the</strong> needs of <strong>the</strong> agency carry<strong>in</strong>g out <strong>the</strong> survey.It rema<strong>in</strong>s a question as <strong>to</strong> how often <strong>the</strong> better-targeted and specific assessment reportsand <strong>the</strong> <strong>in</strong>formation compiled were timely and conv<strong>in</strong>c<strong>in</strong>g enough <strong>to</strong> <strong>in</strong>fluence operationaldecisions of o<strong>the</strong>r partners <strong>in</strong> <strong>the</strong> humanitarian community.Information on <strong>in</strong>com<strong>in</strong>g assistance and ac<strong>to</strong>rsInformation on <strong>in</strong>com<strong>in</strong>g human resources (<strong>the</strong> responders)• Information on available (or soon <strong>to</strong> be) resources is essential <strong>to</strong> determ<strong>in</strong>e unmetneeds.• The capacity <strong>to</strong> moni<strong>to</strong>r <strong>the</strong> arrival and potential contribution of <strong>in</strong>com<strong>in</strong>g healthteams (lack<strong>in</strong>g <strong>in</strong> past disasters) was fur<strong>the</strong>r weakened by <strong>the</strong> proliferation of organizations<strong>in</strong> <strong>Haiti</strong>.As shown <strong>in</strong> Chapter 4, an unusually high number of <strong>in</strong>dividuals, teams, fieldhospitals, and organizations flooded <strong>the</strong> affected areas. Efforts made at <strong>the</strong> <strong>in</strong>ternationallevel <strong>to</strong> moni<strong>to</strong>r, if not <strong>in</strong>fluence, this flow were far from effective.As a first measure, <strong>in</strong>com<strong>in</strong>g ac<strong>to</strong>rs were required <strong>to</strong> register. This o<strong>the</strong>rwisesensible approach was complicated by a duplication of efforts and processesrequired by national <strong>in</strong>stitutions. <strong>Health</strong> organizations had <strong>to</strong> register, <strong>in</strong> pr<strong>in</strong>ciple,with <strong>the</strong> M<strong>in</strong>istry of Plann<strong>in</strong>g, <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong>, <strong>the</strong> <strong>Health</strong> Commissionestablished by <strong>the</strong> President, and f<strong>in</strong>ally <strong>the</strong> <strong>Health</strong> Cluster. When <strong>the</strong> <strong>Health</strong>Cluster was report<strong>in</strong>g over 200 agencies registered, <strong>the</strong> number comply<strong>in</strong>g withregistration at <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong> was only 46. A much larger but unknownnumber of (smaller) ac<strong>to</strong>rs were not registered with any <strong>in</strong>stitution. 11632 26AFILM261414 14AA valuable <strong>in</strong>formation product is <strong>the</strong> so-called 3W list: “Who is do<strong>in</strong>g What andWhere” (or <strong>in</strong> <strong>the</strong> 4W version: “When” and for how long). Compil<strong>in</strong>g this list is timeconsum<strong>in</strong>g,and depends on <strong>the</strong> collaboration and transparency of ac<strong>to</strong>rs (<strong>in</strong> absenceof pro-active surveys or systematic visits). It is <strong>in</strong> constant need of updat<strong>in</strong>g so as not<strong>to</strong> quickly become obsolete. For months, only very rough 3W maps were available.The compilation of <strong>the</strong>se lists, however <strong>in</strong>complete, was an appreciated achievement<strong>in</strong> <strong>Haiti</strong>, although no evaluation of <strong>the</strong> actual use made of <strong>the</strong> <strong>in</strong>formation (or its effectiveness)is available.The same can be said of <strong>the</strong> numerous maps developed for <strong>the</strong> health sec<strong>to</strong>r with <strong>the</strong>support of WFP and OCHA. <strong>Health</strong> ac<strong>to</strong>rs frequently cited difficulties due <strong>to</strong> <strong>the</strong> lackof precise mapp<strong>in</strong>g of health services present <strong>in</strong> <strong>the</strong> camps and temporary settlements. 117Quality assurance is <strong>in</strong>dispensable for proper <strong>response</strong> management, especially <strong>in</strong><strong>the</strong> health field. Information provided at registration or <strong>in</strong> 3W lists is based almost54 54AFILMPho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>FILM54116116 Many of <strong>the</strong> NGOs registered with <strong>the</strong> Presidential <strong>Health</strong> Commission (or <strong>the</strong> Cluster) believed that <strong>the</strong>y were au<strong>to</strong>maticallyregistered with <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong>. This was not <strong>the</strong> case, which reflects <strong>the</strong> tension between adm<strong>in</strong>istrative and politicalbranches of <strong>the</strong> sec<strong>to</strong>r.117 This was <strong>the</strong> responsibility of <strong>the</strong> agency <strong>in</strong> charge of Camps Coord<strong>in</strong>ation and Camp Management, not of <strong>the</strong> health sec<strong>to</strong>r.It is ano<strong>the</strong>r result of <strong>the</strong> piecemeal <strong>in</strong>ternational approach <strong>in</strong> <strong>the</strong> health sec<strong>to</strong>r.
INFORMATION MANAGEMENT- Chapter 7entirely on what <strong>the</strong> ac<strong>to</strong>rs say <strong>the</strong>y do (or <strong>in</strong>tend <strong>to</strong> do). It does not cover <strong>in</strong>formationon <strong>the</strong>ir operational capacity or professional competence. S<strong>in</strong>ce <strong>the</strong>re were no provisionsor resources for quality control of <strong>the</strong> <strong>in</strong>com<strong>in</strong>g ac<strong>to</strong>rs, <strong>the</strong> <strong>in</strong>formation providedby ac<strong>to</strong>rs could not be validated. This has been a serious issue <strong>in</strong> all recent disasters,only made worse <strong>in</strong> <strong>Haiti</strong> with <strong>the</strong> explod<strong>in</strong>g number of partners. 118Information on <strong>in</strong>com<strong>in</strong>g suppliesThe Logistics Support System (LSS/SUMA) has proven its value as a management <strong>to</strong>olof humanitarian supplies <strong>in</strong> recent disasters. In <strong>Haiti</strong>, it was one of <strong>the</strong> few <strong>in</strong>ternational<strong>in</strong>struments directly managed by national authorities.In most disaster situations, <strong>the</strong> management of <strong>in</strong>com<strong>in</strong>g supplies is one of <strong>the</strong> majorbottlenecks <strong>in</strong> <strong>the</strong> humanitarian system. In <strong>the</strong> health sec<strong>to</strong>r, large amounts of unsolicitedand <strong>in</strong>appropriate supplies (expired medic<strong>in</strong>es, used and unsuitable equipment,etc.) compete for scarce s<strong>to</strong>rage and transportation facilities. In past conflicts or naturaldisasters <strong>in</strong> <strong>Haiti</strong> and elsewhere, safely discard<strong>in</strong>g unwanted medical supplies hasbeen done at significant expense.The ma<strong>in</strong> challenge is not only deal<strong>in</strong>g physically with those <strong>in</strong>appropriate donations,but <strong>to</strong> know what has arrived where, and for whom. In major disasters it is common foragencies and authorities <strong>to</strong> make public appeals for urgent donations of medical itemsthat are already available <strong>in</strong> large amounts <strong>in</strong> warehouses at an airport or at governmen<strong>to</strong>r NGO facilities. The cross-sec<strong>to</strong>ral coord<strong>in</strong>ation agency (Direc<strong>to</strong>rate for Civil Protection)and M<strong>in</strong>istry of <strong>Health</strong> had no general decision-mak<strong>in</strong>g authority on <strong>the</strong> flow ofdonations <strong>in</strong> <strong>Haiti</strong>.PAHO/WHO developed and rout<strong>in</strong>ely implemented SUMA, a cross-sec<strong>to</strong>ral <strong>in</strong>itiativefor <strong>in</strong>ven<strong>to</strong>ry and management of humanitarian supplies. It has been used for over 20 years<strong>in</strong> all disasters <strong>in</strong> <strong>the</strong> Americas and <strong>in</strong> many emergencies <strong>in</strong> o<strong>the</strong>r regions of <strong>the</strong> world.More recently, PAHO/WHO jo<strong>in</strong>ed forces with o<strong>the</strong>r UN ac<strong>to</strong>rs (among <strong>the</strong>m WFP,<strong>the</strong> lead agency for <strong>the</strong> Logistics Cluster) <strong>to</strong> move SUMA <strong>to</strong> <strong>the</strong> more powerful LogisticsSupport System (LSS).LSS/SUMA offers two different services: consolidated <strong>in</strong>ven<strong>to</strong>ry at entry po<strong>in</strong>ts and support<strong>to</strong> warehouse management. It is dedicated <strong>to</strong> <strong>the</strong> management of <strong>in</strong>formation not of <strong>the</strong> supplies<strong>the</strong>mselves, which is <strong>the</strong> responsibility of <strong>the</strong> Logistics Cluster.LSS/SUMA was activated very early <strong>in</strong> <strong>the</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>Haiti</strong> <strong>earthquake</strong> (see Table 7.1).Based both <strong>in</strong> Port-au-Pr<strong>in</strong>ce and San<strong>to</strong> Dom<strong>in</strong>go, it provided decision makers (<strong>in</strong> <strong>the</strong> Direc<strong>to</strong>ratefor Civil Protection) with cross-sec<strong>to</strong>r data so that <strong>the</strong>y could better moni<strong>to</strong>r andcoord<strong>in</strong>ate <strong>the</strong> entry of supplies <strong>in</strong><strong>to</strong> <strong>the</strong>ir own country. In <strong>the</strong> Dom<strong>in</strong>ican Republic, LSS/SUMA supported <strong>the</strong> management of warehouses.118 Many <strong>in</strong>terlocu<strong>to</strong>rs had anecdotal horror s<strong>to</strong>ries of unethical or <strong>in</strong>competent behavior, rang<strong>in</strong>g from disaster “<strong>to</strong>urism” <strong>to</strong><strong>the</strong> unannounced closure of one organization’s project and office <strong>in</strong> Port-au-Pr<strong>in</strong>ce, leav<strong>in</strong>g field staff stranded <strong>in</strong> departmentswithout <strong>in</strong>formation or support.117
32 32A<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Table 7.1 Timel<strong>in</strong>e of LSS/SUMA activities <strong>in</strong> <strong>Haiti</strong>;<strong>January</strong>–March <strong>2010</strong>12 <strong>January</strong> Impact of <strong>the</strong> <strong>earthquake</strong>15 <strong>January</strong> Arrival of <strong>the</strong> advance team (<strong>Haiti</strong> and <strong>the</strong> Dom<strong>in</strong>ican Republic)16 <strong>January</strong> Beg<strong>in</strong> activities <strong>in</strong> <strong>Haiti</strong> and San<strong>to</strong> Dom<strong>in</strong>go; coord<strong>in</strong>ate with Logistics Clusterand OCHA23 <strong>January</strong> Open a warehouse <strong>in</strong> Jimaní (Dom<strong>in</strong>ican Republic) for medical supplies<strong>in</strong> transit1 February Support from <strong>the</strong> White Helmets (Argent<strong>in</strong>a); cooperation with IOM10 February Inven<strong>to</strong>ry starts at Port-au-Pr<strong>in</strong>ce port facilities (recently reopened)17 March Meet<strong>in</strong>g with Direc<strong>to</strong>rate for Civil Protection about lessons learned; developmentproject <strong>in</strong>itiatedOngo<strong>in</strong>g Project <strong>to</strong> support capacity of <strong>the</strong> <strong>Haiti</strong>an Direc<strong>to</strong>rate for Civil ProtectionAn important feature is that LSS/SUMA counterparts were primarily <strong>in</strong> <strong>the</strong> <strong>Haiti</strong>anDirec<strong>to</strong>rate for Civil Protection. 119 The Government of <strong>Haiti</strong> owned and managed <strong>the</strong><strong>in</strong>formation ra<strong>the</strong>r than <strong>the</strong> UN or ano<strong>the</strong>r external agency. Hav<strong>in</strong>g some post fac<strong>to</strong><strong>in</strong>formation on <strong>the</strong> supplies already on site was, however, not sufficient <strong>to</strong> <strong>in</strong>fluenceand filter <strong>the</strong> donations <strong>the</strong>mselves. The Direc<strong>to</strong>rate for Civil Protection played <strong>the</strong>lead role <strong>in</strong> activat<strong>in</strong>g and <strong>in</strong>stall<strong>in</strong>g LSS/SUMA at two entry po<strong>in</strong>ts (<strong>the</strong> airport andlater <strong>the</strong> seaport); it was one of <strong>the</strong> very few <strong>in</strong>ternational <strong>in</strong>itiatives directly managedby this <strong>Haiti</strong>an <strong>in</strong>stitution. The organization of LSS/SUMA <strong>in</strong> <strong>Haiti</strong> and categories ofsupplies <strong>in</strong>ven<strong>to</strong>ried are shown <strong>in</strong> Figures 7.1, 7.3.In <strong>the</strong> health sec<strong>to</strong>r, LSS/SUMA supported PROMESS, <strong>the</strong> ma<strong>in</strong> channel for distributionof medical supplies on behalf of <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong>.LSS/SUMA operates dur<strong>in</strong>g emergencies by mobiliz<strong>in</strong>g dedicated volunteers fromneighbor<strong>in</strong>g countries (<strong>in</strong> this case from <strong>the</strong> Dom<strong>in</strong>ican Republic, Nicaragua, andArgent<strong>in</strong>a). Its deployment capacity is impressive due <strong>to</strong> <strong>the</strong> thousands of volunteerstra<strong>in</strong>ed <strong>in</strong> Lat<strong>in</strong> America and <strong>the</strong> Caribbean (as well as outside <strong>the</strong> Americas). It is atrue example of regional solidarity <strong>in</strong> action.21FILM32FILM21 21A4242 42APho<strong>to</strong>s: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>118119 Counterparts and local experts are tra<strong>in</strong>ed <strong>in</strong> all countries of <strong>the</strong> Americas, <strong>Haiti</strong> <strong>in</strong>cluded. As often occurs <strong>in</strong> major disasters,tra<strong>in</strong>ed nationals faced compet<strong>in</strong>g demands and few were immediately available for what was perceived a less critical(not life-sav<strong>in</strong>g) activity.
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Figure 7.3 Weight of supplies by categoryarriv<strong>in</strong>g at Port-au-Pr<strong>in</strong>ce harborNon food12,762Personal needs/educaon846Logiscs/<strong>to</strong>ols54Medical1,080Unclassified items1,188Food43,956Water4,680Category Weight <strong>in</strong> TonsSource: Adapted from figures provided by V. Mart<strong>in</strong>ez and J. Venegas, PAHO/WHO, SUMA.Dissem<strong>in</strong>ation of <strong>in</strong>formation• Information should be available for on-site decision mak<strong>in</strong>g as well as for <strong>in</strong>stitutionalmemory for future disasters.• A common service <strong>in</strong>formation center, as was deployed after <strong>the</strong> tsunami, waslack<strong>in</strong>g <strong>in</strong> <strong>Haiti</strong>.Collect<strong>in</strong>g and <strong>in</strong>terpret<strong>in</strong>g mean<strong>in</strong>gful and timely <strong>in</strong>formation can be an almost impossiblechallenge <strong>in</strong> disasters. This has been noted <strong>in</strong> <strong>the</strong> aftermath of all disasters<strong>in</strong>volv<strong>in</strong>g large numbers of ac<strong>to</strong>rs. To <strong>in</strong>fluence decision mak<strong>in</strong>g and effect changes,<strong>in</strong>formation must be available <strong>in</strong> <strong>the</strong> format that meets <strong>the</strong> specific requests and needsof <strong>the</strong> <strong>in</strong>tended users.Follow<strong>in</strong>g <strong>the</strong> Indian Ocean tsunami, UN/OCHA established <strong>the</strong> HumanitarianInformation Center (HIC), a common service <strong>in</strong>formation desk where newcomerscould register, receive copies of exist<strong>in</strong>g <strong>in</strong>formation and maps, as well as file <strong>the</strong>ir ownreports for dissem<strong>in</strong>ation.In <strong>Haiti</strong>, <strong>the</strong> HIC was not formally activated <strong>in</strong> spite of <strong>the</strong> much greater flow ofvisi<strong>to</strong>rs and general enquiries. 120 Sec<strong>to</strong>rs were basically left with <strong>the</strong> task of brief<strong>in</strong>g all<strong>in</strong>com<strong>in</strong>g visi<strong>to</strong>rs regardless of <strong>the</strong>ir potential <strong>to</strong> contribute positively. This distracted120 The map center set up by OCHA did provide pr<strong>in</strong>ted and soft format maps.120
INFORMATION MANAGEMENT- Chapter 7health experts from more serious and productive tasks. Ano<strong>the</strong>r significant source ofdistraction was <strong>the</strong> constant demand on <strong>the</strong> time of coord<strong>in</strong>a<strong>to</strong>rs and field staff <strong>to</strong>repackage <strong>the</strong> same <strong>in</strong>formation (or lack of) <strong>in</strong> dist<strong>in</strong>ct formats and styles accord<strong>in</strong>g<strong>to</strong> <strong>the</strong> specific purpose of <strong>the</strong> request (adm<strong>in</strong>istrative, <strong>in</strong>formation for <strong>the</strong> agency’sexecutive management, fund rais<strong>in</strong>g, public relations, or merely <strong>to</strong> justify a requestfor support).While efforts were made <strong>to</strong> improve <strong>the</strong> immediate dissem<strong>in</strong>ation of <strong>in</strong>formation <strong>to</strong> operationalpartners, 121 less attention has been given <strong>to</strong> preserv<strong>in</strong>g this perishable data forfuture use. Dur<strong>in</strong>g <strong>the</strong> tsunami <strong>response</strong>, <strong>the</strong> HIC played <strong>the</strong> role of deposi<strong>to</strong>ry. Therewas no s<strong>in</strong>gle po<strong>in</strong>t when key documents produced <strong>in</strong> <strong>the</strong> first few months <strong>in</strong> <strong>Haiti</strong> weresystematically saved <strong>in</strong> electronic format for public or academic access. 122 Of particular<strong>in</strong>terest would be access <strong>to</strong> <strong>the</strong> e-mail “<strong>in</strong>box” and “sent box” of <strong>the</strong> clusters so as <strong>to</strong>appreciate <strong>the</strong> chang<strong>in</strong>g patterns and flow of requests and action. Early cluster e-mailexchanges were not available for research purposes (lost or corrupted files for <strong>the</strong> healthsec<strong>to</strong>r and access not granted for o<strong>the</strong>rs). As a matter of transparency and for <strong>the</strong> sake ofcollective memory, cluster files and archives should be <strong>in</strong> <strong>the</strong> public doma<strong>in</strong>.To address this lack of <strong>in</strong>stitutional memory, several data rescue projects have beenlaunched, almost as an afterthought. 123 Those projects are no substitute for a policy ofsystematic, long-term preservation and shar<strong>in</strong>g of files as <strong>in</strong>itiated by <strong>the</strong> HIC <strong>in</strong> <strong>the</strong>aftermath of <strong>the</strong> tsunami.Mass media and social media• <strong>Haiti</strong> <strong>response</strong> confirmed <strong>the</strong> preem<strong>in</strong>ent role of <strong>the</strong> mass media. In light of <strong>the</strong>ir<strong>in</strong>fluence on <strong>the</strong> flow and nature of assistance, <strong>the</strong> health sec<strong>to</strong>r would benefit by<strong>in</strong>volv<strong>in</strong>g <strong>the</strong>m more closely <strong>in</strong> its <strong>in</strong>formation management activities.• For <strong>the</strong> first time, social media played a large role <strong>in</strong> <strong>in</strong>formation dissem<strong>in</strong>ation. Its potentialshould be explored and, if possible, harnessed before <strong>the</strong> next disaster.Both traditional mass media and new social media played a critical role <strong>in</strong> encourag<strong>in</strong>ggenerous support for <strong>Haiti</strong>. It was a double-edged sword: it was positive when it motivated<strong>the</strong> public and governments <strong>to</strong> provide f<strong>in</strong>ancial and operational support, but negativewhen it <strong>in</strong>cited a deluge of well-<strong>in</strong>tentioned but unsuitable supplies or personnel.121 This became <strong>the</strong> ma<strong>in</strong> raison d’être of <strong>the</strong> numerous meet<strong>in</strong>gs.122 The Emergency Operations Center (EOC) of PAHO/WHO was close <strong>to</strong> fill<strong>in</strong>g this role <strong>in</strong>ternally. It has a remarkable collectionof documents, situation reports, and documentation related <strong>to</strong> health. Its function, however, is not for documentpreservation and access.123 The U.S. National Library of Medic<strong>in</strong>e and PAHO/WHO are collaborat<strong>in</strong>g on <strong>the</strong> “Project for collect<strong>in</strong>g, preserv<strong>in</strong>g anddissem<strong>in</strong>at<strong>in</strong>g health and disaster <strong>in</strong>formation after <strong>the</strong> <strong>January</strong> <strong>2010</strong> <strong>earthquake</strong>.” The University of <strong>Haiti</strong> (UEH) and TulaneUniversity Disaster Resilience Leadership Academy (DRLA) have conducted a review of over 500 documents related <strong>to</strong> <strong>the</strong><strong>earthquake</strong>, 94 of which have been classified <strong>in</strong> a database (available at www.drlatulane.org).124 Dur<strong>in</strong>g <strong>the</strong> first two months after <strong>the</strong> <strong>earthquake</strong> <strong>the</strong>re was no local coverage by traditional news media <strong>in</strong> <strong>Haiti</strong> (nationaltelevision news or newspapers) due <strong>to</strong> <strong>the</strong> extensive damage <strong>to</strong> communications and transport <strong>in</strong>frastructure and seriousdeficiencies <strong>in</strong> utilities services. Foreign outlets <strong>in</strong>cluded, among o<strong>the</strong>rs, CNN, <strong>the</strong> New York Times, and Los Angeles Times.121
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Mass mediaIn past humanitarian crises foreign news outlets carried extensive coverage from <strong>the</strong> firstday of impact. 124 Their capacity <strong>to</strong> react quickly and obta<strong>in</strong> <strong>in</strong>formation is impressive.Their ability <strong>to</strong> deploy resources is far superior <strong>to</strong> that of most humanitarian agencies.It is difficult <strong>to</strong> gauge <strong>to</strong> what extent official allocations of fund<strong>in</strong>g and deploymentwere <strong>in</strong>fluenced by <strong>the</strong> public perceptions shaped by <strong>the</strong> rapid media coverage ra<strong>the</strong>rthan by formal assessments from UN and o<strong>the</strong>r humanitarian agencies. Interviews <strong>in</strong><strong>Haiti</strong> and similar studies of past disasters suggest that <strong>the</strong> media play <strong>the</strong> major role<strong>in</strong> this regard, although not always with <strong>the</strong> most reliable or objective <strong>in</strong>formation. 125In all major disasters, <strong>the</strong> accuracy of <strong>the</strong> <strong>in</strong>formation <strong>in</strong> <strong>the</strong> mass media may bedeterm<strong>in</strong>ed by <strong>the</strong> need <strong>to</strong> oversimplify complex situations. The perception is that<strong>the</strong> public prefers black and white s<strong>to</strong>ries. Accuracy is also <strong>in</strong>fluenced by <strong>the</strong> qualityof brief<strong>in</strong>gs provided by partners and stakeholders. Pacify<strong>in</strong>g comments such as <strong>the</strong>“situation is under control” are generally poorly received. Alarm<strong>in</strong>g <strong>in</strong>formation evenif <strong>in</strong>tended <strong>to</strong> generate support for a special group or issue usually f<strong>in</strong>ds a more receptiveaudience. The responsibility <strong>to</strong> improve <strong>the</strong> quality of media coverage lies with <strong>the</strong>humanitarian ac<strong>to</strong>rs who should give higher priority <strong>to</strong> <strong>in</strong>form<strong>in</strong>g <strong>the</strong> public abouteffective <strong>response</strong> than <strong>to</strong> secur<strong>in</strong>g favorable coverage for <strong>the</strong>ir activities.When <strong>the</strong> objective of media brief<strong>in</strong>gs is <strong>to</strong> <strong>in</strong>form <strong>the</strong> public on health impacts oreducate it, for example, on <strong>the</strong> need for sanitation or <strong>the</strong> absence of risk caused bydead bodies, <strong>the</strong> message is generally unders<strong>to</strong>od.In <strong>Haiti</strong>, relations between health ac<strong>to</strong>rs and <strong>the</strong> media appeared predom<strong>in</strong>antly directed<strong>to</strong>ward <strong>the</strong> impact on public relations (<strong>the</strong> agency image) ra<strong>the</strong>r than on apartnership <strong>to</strong> better <strong>in</strong>form and educate <strong>the</strong> public on what actions were likely <strong>to</strong> beeffective. Greater benefit for <strong>the</strong> affected population would result from improved collaborationbetween humanitarian agencies and <strong>the</strong> media, for <strong>in</strong>stance by embedd<strong>in</strong>gselected journalists <strong>in</strong> <strong>in</strong>itial assessment missions. 126Social mediaOn 22 <strong>January</strong> a reporter for <strong>the</strong> BBC (MacLeod <strong>2010</strong>) commented:“New and emerg<strong>in</strong>g media played a key role <strong>in</strong> break<strong>in</strong>g news <strong>to</strong> <strong>the</strong>outside world of <strong>the</strong> <strong>Haiti</strong> <strong>earthquake</strong>. Citizens turned <strong>to</strong> a range ofnetwork<strong>in</strong>g <strong>to</strong>ols <strong>in</strong> a bid <strong>to</strong> share <strong>the</strong> news and personal s<strong>to</strong>ries frommicroblogg<strong>in</strong>g on Twitter and video-shar<strong>in</strong>g on YouTube <strong>to</strong> <strong>the</strong> <strong>in</strong>ternettelephone application Skype, and <strong>the</strong> social media site Facebook. Forover 24 hours after <strong>the</strong> quake, countless reports and images came no<strong>to</strong>nly from big, established news organisations but from ord<strong>in</strong>ary peopleon <strong>the</strong> spot. …122125 Authors of an evaluation of <strong>the</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> Indian Ocean tsunami make this observation: “The mass media, not <strong>the</strong> UNor ano<strong>the</strong>r humanitarian body, was able <strong>to</strong> provide early and ‘conv<strong>in</strong>c<strong>in</strong>g’ comprehensive formal assessment of immediateneeds” <strong>in</strong> <strong>the</strong> aftermath of <strong>the</strong> tsunami. “The quality of this <strong>in</strong>formation, and especially <strong>the</strong> tendency <strong>to</strong> pick up <strong>the</strong> mostnegative, frighten<strong>in</strong>g or outrageous statements from any unqualified source, has long been a matter of legitimate compla<strong>in</strong>tfrom responsible and professional disaster managers” (de Ville de Goyet and Mor<strong>in</strong>ière 2006; 14, 58).126 This was a recommendation of <strong>the</strong> Tsunami Evaluation Coalition (recommendation No. 11) (de Ville de Goyet andMor<strong>in</strong>ière 2006).
INFORMATION MANAGEMENT- Chapter 7“However, aid agencies, charities and o<strong>the</strong>rs po<strong>in</strong>ted out that while news wasbe<strong>in</strong>g broken and gett<strong>in</strong>g out of <strong>the</strong> country via new and emerg<strong>in</strong>g media,such platforms were often unable <strong>to</strong> provide practical assistance <strong>to</strong> victims.”32FILMIt is <strong>to</strong>o early <strong>to</strong> conclude what may be <strong>the</strong> role of social media <strong>in</strong> <strong>the</strong> management offuture disasters. As noted <strong>in</strong> regard <strong>to</strong> <strong>Haiti</strong>, social media were “call<strong>in</strong>g <strong>in</strong><strong>to</strong> question<strong>the</strong> <strong>in</strong>gra<strong>in</strong>ed view of unidirectional, official-<strong>to</strong>-public <strong>in</strong>formation broadcasts. Socialmedia may also offer potential psychological benefit for vulnerable populations ga<strong>in</strong>edthrough participation as stakeholders <strong>in</strong> <strong>the</strong> <strong>response</strong>” (Keim and Noji 2011).However, this new form of peer-<strong>to</strong>-peer <strong>in</strong>formation collection and shar<strong>in</strong>g played asignificant role <strong>in</strong> identify<strong>in</strong>g needs. Web-based platforms such as Ushahidi 127 became<strong>in</strong>formation providers l<strong>in</strong>ked <strong>to</strong> geographic <strong>in</strong>formation systems, and produced <strong>in</strong>teractivemaps through Google maps. There may be caveats for <strong>the</strong>se emerg<strong>in</strong>g systems,but <strong>the</strong>y proved very useful at <strong>the</strong> time <strong>to</strong> direct ambulances <strong>to</strong> <strong>the</strong> <strong>in</strong>jured or sick and<strong>to</strong> allocate relief.Official reports from <strong>the</strong> government and humanitarian organizations are unlikely<strong>to</strong> rema<strong>in</strong> <strong>the</strong> only source of <strong>in</strong>formation (apart from <strong>the</strong> mass media) and may be<strong>in</strong>creas<strong>in</strong>gly challenged <strong>in</strong> <strong>the</strong> future by a “bot<strong>to</strong>m-up” flow of <strong>in</strong>formation.The shortcom<strong>in</strong>gs noted do not reflect a lack of dedication or concern on <strong>the</strong> part of<strong>the</strong> coord<strong>in</strong>a<strong>to</strong>rs and managers, but ra<strong>the</strong>r <strong>the</strong> complexity of fast evolv<strong>in</strong>g, multifacetedneeds and <strong>response</strong> unmatched by correspond<strong>in</strong>g <strong>in</strong>stitutional <strong>in</strong>vestment.The <strong>Health</strong> Cluster Coord<strong>in</strong>a<strong>to</strong>r <strong>in</strong> her one-month report clearly identifies <strong>in</strong>formationmanagement as one of two pillars for future activities. It was def<strong>in</strong>ed as:“The construction of an <strong>in</strong>formation management system/situation room thatallows for decisions on actions via a clear presentation about <strong>the</strong> <strong>in</strong>itial needs,trends, service provision, epidemiologic alerts, status of <strong>the</strong> national health system(facilities, staff) and <strong>in</strong>ternational cooperation, so as <strong>to</strong> see where are <strong>the</strong>priorities and gaps, <strong>to</strong> def<strong>in</strong>e actions, <strong>to</strong> moni<strong>to</strong>r implementation, and <strong>to</strong> evaluateresults” (Van Alphen <strong>2010</strong>).Pho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>32 32A127 Ushahidi (which means “testimony” <strong>in</strong> Swahili) is a data-mapp<strong>in</strong>g platform that was first used <strong>in</strong> 2007 <strong>in</strong> Kenya. Thedevelopers used it “<strong>to</strong> collate and locate reports of unrest sent <strong>in</strong> by <strong>the</strong> public via text message, e mail and social media. . . Ushahidi quickly became <strong>the</strong> world’s default platform for mapp<strong>in</strong>g crises, disasters and political upheaval. [By May of2011] Ushahidi, which is free <strong>to</strong> download, had been used 14,000 times <strong>in</strong> 128 countries <strong>to</strong> map everyth<strong>in</strong>g from last year’s<strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>to</strong> this year’s Japanese tsunami. . . . ”(Perry 2011).123
One of <strong>the</strong> biggest challenges faced by Dr. Alex Larsen, <strong>the</strong>n M<strong>in</strong>isterLorem ipsum doler sit ameof <strong>Health</strong> (middle), dur<strong>in</strong>g <strong>the</strong> first months of <strong>the</strong> <strong>response</strong> waskeep<strong>in</strong>g track of all <strong>the</strong> different organizations that were <strong>in</strong> <strong>Haiti</strong>:by Rum mid et April, quate 396 volorio <strong>in</strong>ternational volorestibus agencies quidessimusaut untem et eaque rectibea prae Git etregistered with <strong>the</strong> <strong>Health</strong>Cluster, landanti 50 ulliquat of those et were offictem. registered Et etus, with untiur <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong>.atiusant vellect orest, omniet volupta tquae.Seventy-six Nam, es nim agencies sequi cuptaturi left <strong>the</strong> berati country velibus two as weeks after <strong>the</strong> <strong>earthquake</strong>.exerspera is necusci debisqu oditem eos<strong>to</strong>officiust vel ipsundaerum eatquunt ute iumeatat.Pho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>
Chapter8Coord<strong>in</strong>ation• The primary responsibility for coord<strong>in</strong>ation lies with national authorities.• Although direct external coord<strong>in</strong>ation may be required for a short period after asudden-onset natural disaster, it cannot exercise <strong>the</strong> same authority over humanitarianpartners that a legitimate government can.• A mechanism and set date for transfer of responsibility were lack<strong>in</strong>g <strong>in</strong> all recentdisasters.Coord<strong>in</strong>ation has been discussed <strong>in</strong> several places <strong>in</strong> this publication. Overall, <strong>the</strong>reis a strong consensus that <strong>the</strong> <strong>response</strong> from all sec<strong>to</strong>rs was chaotic and poorly coord<strong>in</strong>ated<strong>in</strong> <strong>Haiti</strong>.The same was said for <strong>the</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> tsunami and <strong>to</strong> <strong>the</strong> Pakistan <strong>earthquake</strong>.However, <strong>in</strong> <strong>the</strong> aftermath of <strong>Haiti</strong>, several edi<strong>to</strong>rials and articles <strong>in</strong> professional journalsraised serious and fundamental issues regard<strong>in</strong>g <strong>the</strong> current status of <strong>in</strong>ternational<strong>response</strong>. Abstracts of titles are illustrative of <strong>the</strong> malaise: “Growth of aid and <strong>the</strong> decl<strong>in</strong>eof humanitarianism,” “Un<strong>in</strong>tended consequences of humanitarian volunteerism,” and“Cacophonies of aid.” 128 The fact that <strong>the</strong>se critiques were published <strong>in</strong> peer-reviewedscientific publications and not only <strong>in</strong> <strong>the</strong> mass media is significant.This chapter will summarize <strong>the</strong> health sec<strong>to</strong>r f<strong>in</strong>d<strong>in</strong>gs from many <strong>in</strong>terviews and reviewof extensive bibliography. The alternatives and way forward will be discussed <strong>in</strong><strong>the</strong> next chapter on key lessons.128 See: “Edi<strong>to</strong>rial: Growth of aid and <strong>the</strong> decl<strong>in</strong>e of humanitarianism” Lancet (<strong>2010</strong>), 375(9711):253; Jobe K., “Disaster relief<strong>in</strong> post-<strong>earthquake</strong> <strong>Haiti</strong>: un<strong>in</strong>tended consequences of humanitarian volunteerism” Travel Med Infect Dis (2011), 9(1):1–-5; and Zanotti L., “Cacophonies of aid, failed state build<strong>in</strong>g and NGOs <strong>in</strong> <strong>Haiti</strong>: sett<strong>in</strong>g <strong>the</strong> stage for disaster, envision<strong>in</strong>g<strong>the</strong> future” Third World Q (<strong>2010</strong>), 31(5):755–71.125
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>What is coord<strong>in</strong>ation and who is responsible?Coord<strong>in</strong>ation has a dist<strong>in</strong>ct mean<strong>in</strong>g for every ac<strong>to</strong>r. Some see coord<strong>in</strong>ation merely asa forum <strong>to</strong> learn what o<strong>the</strong>rs are do<strong>in</strong>g, while for o<strong>the</strong>rs it is <strong>the</strong> authoritative sett<strong>in</strong>g ofpriorities by <strong>the</strong> coord<strong>in</strong>at<strong>in</strong>g body, with resources be<strong>in</strong>g allocated and activities permittedaccord<strong>in</strong>gly. For many, it is also a mechanism of quality control whereby <strong>the</strong> “mushroom”opera<strong>to</strong>rs (popp<strong>in</strong>g up overnight) without experience and resources are weeded out.All profess <strong>to</strong> be will<strong>in</strong>g <strong>to</strong> coord<strong>in</strong>ate with o<strong>the</strong>rs. Few accept be<strong>in</strong>g coord<strong>in</strong>ated.Many operational partners, while decry<strong>in</strong>g <strong>the</strong> vacuum of authority as a major impediment<strong>to</strong> effective relief, <strong>in</strong> fact see it as convenient.There is not always a clear understand<strong>in</strong>g about who has <strong>the</strong> authority <strong>to</strong> coord<strong>in</strong>ate<strong>the</strong> health <strong>response</strong>. That should not be <strong>the</strong> case: <strong>the</strong> UN General Assembly Resolution46/182 acknowledges clearly that <strong>the</strong> Government has primary responsibility <strong>in</strong>organiz<strong>in</strong>g humanitarian assistance <strong>in</strong> a disaster. In <strong>the</strong> aftermath of a natural disaster<strong>in</strong> a country with a recognized government, <strong>the</strong> authority for all health issues shouldrema<strong>in</strong> with <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong> of <strong>the</strong> affected country, not with <strong>in</strong>ternational, adhoc structures. The issue may be blurred or debatable <strong>in</strong> conflict situations or <strong>in</strong> failedstates. The latter situation was not <strong>the</strong> case <strong>in</strong> <strong>Haiti</strong>.Whe<strong>the</strong>r a weak <strong>in</strong>stitution <strong>in</strong> a country so severely crippled by a disaster could coord<strong>in</strong>ate<strong>the</strong> highly complex web of agencies and ac<strong>to</strong>rs alone is ano<strong>the</strong>r matter. Specialized UN agenciesand mechanisms play a key role <strong>in</strong> assist<strong>in</strong>g <strong>the</strong> health authorities and <strong>in</strong> some <strong>in</strong>stancestemporarily accept <strong>the</strong> burden of de fac<strong>to</strong> coord<strong>in</strong>at<strong>in</strong>g <strong>the</strong> <strong>response</strong>. In <strong>the</strong> same way that <strong>the</strong>Government of <strong>Haiti</strong> formally delegated its authority over airport operations and <strong>Haiti</strong>anairspace <strong>to</strong> <strong>the</strong> United States, it implicitly delegated overall or sec<strong>to</strong>ral coord<strong>in</strong>ation of <strong>the</strong>external <strong>response</strong> <strong>to</strong> <strong>the</strong> UN. As was <strong>the</strong> case <strong>in</strong> Pakistan, <strong>the</strong> authorities <strong>in</strong>itially welcomed<strong>the</strong> establishment of <strong>the</strong> UN Clusters on <strong>the</strong> understand<strong>in</strong>g that <strong>the</strong>y would streng<strong>the</strong>n <strong>the</strong>capacity of l<strong>in</strong>e m<strong>in</strong>istries while <strong>the</strong>y readied <strong>the</strong>mselves <strong>to</strong> assume leadership.National coord<strong>in</strong>ationCross-sec<strong>to</strong>ral national coord<strong>in</strong>ation• Weak and poorly perform<strong>in</strong>g national organizations tend <strong>to</strong> be marg<strong>in</strong>alized andfur<strong>the</strong>r debilitated by <strong>the</strong> <strong>in</strong>ternational <strong>response</strong> while <strong>the</strong> stronger ones mayemerge streng<strong>the</strong>ned.• In <strong>the</strong> same way that <strong>the</strong> most vulnerable <strong>in</strong>dividuals among <strong>the</strong> affected populationshould receive special attention from <strong>the</strong> humanitarian responders, <strong>the</strong> weak or “vulnerable”national <strong>in</strong>stitutions should benefit early from special support from <strong>the</strong> <strong>in</strong>ternationalcommunity and donors. This is particularly important when <strong>the</strong> mandate of those <strong>in</strong>stitutionsis critical for survival and recovery, as <strong>in</strong> <strong>the</strong> case of <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong>.The coord<strong>in</strong>ation mechanisms for deal<strong>in</strong>g with disasters are relatively complex <strong>in</strong> <strong>Haiti</strong>.129 The operational arm of <strong>the</strong> system is <strong>the</strong> Direc<strong>to</strong>rate for Civil Protection (DPC).DPC presence at <strong>the</strong> prov<strong>in</strong>cial and municipal levels is uneven.126129 In 1999, <strong>the</strong> National System for <strong>the</strong> Management of Risk and Disasters (SNGRD) was established. The SNGRDconsists of 26 governmental and nongovernmental <strong>in</strong>stitutions <strong>in</strong>volved <strong>in</strong> disaster preparedness and <strong>response</strong>. TheDirec<strong>to</strong>rate for Civil Protection (DPC) is a central direc<strong>to</strong>rate of <strong>the</strong> M<strong>in</strong>istry of Interior and is <strong>the</strong> executive arm of <strong>the</strong>SNGRD.
COORDINATION - Chapter 8In emergencies, <strong>the</strong> Government activates <strong>the</strong> Emergency Operations Center (Centred’Opération d’Urgence—COU), which br<strong>in</strong>gs <strong>to</strong>ge<strong>the</strong>r <strong>the</strong> relevant <strong>in</strong>stitutions. Surpris<strong>in</strong>gly,this center was not activated after <strong>the</strong> <strong>earthquake</strong>. This had consequences,as many of <strong>the</strong> national <strong>in</strong>stitutions felt relatively lost <strong>in</strong> this “<strong>in</strong>stitutional vacuum.”In <strong>the</strong> first months, external fund<strong>in</strong>g and logistics support for overall coord<strong>in</strong>ationkept flow<strong>in</strong>g <strong>to</strong> <strong>the</strong> UN and <strong>in</strong>ternational agencies, bypass<strong>in</strong>g <strong>the</strong> DPC coord<strong>in</strong>a<strong>to</strong>rs.DPC staff were left almost without personal or professional means while young, <strong>in</strong>experienced,foreign volunteers had transport facilities, <strong>in</strong>ternet and communicationaccess, food, and accommodation.The adoption of English as <strong>the</strong> work<strong>in</strong>g language of all coord<strong>in</strong>ation and brief<strong>in</strong>gmeet<strong>in</strong>gs, <strong>the</strong> location of those meet<strong>in</strong>gs <strong>in</strong> <strong>the</strong> MINUSTAH base (“Logbase”) withrestricted access for <strong>Haiti</strong>an nationals, and <strong>the</strong> sheer imbalance <strong>in</strong> number of attendees(“one <strong>Haiti</strong>an official versus 150 <strong>in</strong>ternationals” as said by an <strong>in</strong>terviewee) made itextremely difficult for <strong>the</strong> DPC <strong>to</strong> reclaim leadership and assume its coord<strong>in</strong>ation role.For affected populations <strong>the</strong> benefit of <strong>in</strong>ternational agencies assum<strong>in</strong>g <strong>the</strong> lead <strong>in</strong> <strong>the</strong> firstweeks is not questioned. Those agencies have had greater experience and have <strong>the</strong> skills forthis task. 130 Their leadership was necessary <strong>in</strong> <strong>the</strong> immediate <strong>response</strong> when speed meantlives saved. However, <strong>the</strong> fact that <strong>the</strong>ir control persisted throughout <strong>the</strong> recovery and rehabilitationprocess with only <strong>to</strong>ken participation of <strong>the</strong> DPC is of concern. 131The Presidential CommissionsAn ad hoc mechanism was established a few days after <strong>the</strong> <strong>earthquake</strong> <strong>to</strong> assert <strong>Haiti</strong>anState leadership <strong>in</strong> <strong>the</strong> <strong>response</strong>: <strong>the</strong> Presidential Commissions. Directly l<strong>in</strong>ked <strong>to</strong> <strong>the</strong>President and perceived as “double pouvoir” by some l<strong>in</strong>e m<strong>in</strong>istries who felt deprived of<strong>the</strong>ir adm<strong>in</strong>istrative responsibilities, <strong>the</strong>se commissions contributed <strong>to</strong> blurr<strong>in</strong>g l<strong>in</strong>es andweaken<strong>in</strong>g tested l<strong>in</strong>ks of <strong>the</strong> normal mechanisms.In <strong>the</strong> health sec<strong>to</strong>r, one of <strong>the</strong> added values of <strong>the</strong> Presidential <strong>Health</strong> Commission was<strong>the</strong> participation of academic and o<strong>the</strong>r national health ac<strong>to</strong>rs <strong>in</strong> addition <strong>to</strong> <strong>the</strong> M<strong>in</strong>istrystaff. The first location of its office <strong>in</strong> <strong>the</strong> vic<strong>in</strong>ity of <strong>the</strong> airport (<strong>the</strong> de fac<strong>to</strong> center ofall humanitarian coord<strong>in</strong>ation activities and temporary headquarters of most UN agencies)132 greatly facilitated closer contact. Op<strong>in</strong>ions vary regard<strong>in</strong>g <strong>the</strong> value of sett<strong>in</strong>g upthis <strong>Health</strong> Commission <strong>in</strong> an atmosphere of protracted tensions between political decisionmakers and adm<strong>in</strong>istra<strong>to</strong>rs with<strong>in</strong> <strong>the</strong> health m<strong>in</strong>istry, a problem mentioned by severalkey <strong>in</strong>terlocu<strong>to</strong>rs. Some see this <strong>in</strong>itiative as alleviat<strong>in</strong>g <strong>the</strong> problem while o<strong>the</strong>rs see athird stakeholder as a complicat<strong>in</strong>g fac<strong>to</strong>r.M<strong>in</strong>istry of <strong>Health</strong>Be<strong>in</strong>g a l<strong>in</strong>e M<strong>in</strong>istry <strong>in</strong> a very specialized and regulated area (ra<strong>the</strong>r than a centraldirec<strong>to</strong>rate, as <strong>the</strong> DPC), one would expect that <strong>the</strong> M<strong>in</strong>istry’s authority would be lesschallenged. It was not challenged—it was mostly ignored.130 The caliber, seniority and experience of <strong>in</strong>ter-Cluster coord<strong>in</strong>a<strong>to</strong>rs, as well as <strong>the</strong> speed of <strong>the</strong>ir arrival were questioned <strong>in</strong><strong>in</strong>terviews and external evaluation reports.131 The situation is reportedly similar 18 months after impact.132 Be<strong>in</strong>g part of <strong>the</strong> military peacekeep<strong>in</strong>g headquarters, access <strong>to</strong> Logbase was first denied and later merely difficult for <strong>Haiti</strong>answho were not employees of <strong>in</strong>ternational agencies, <strong>in</strong>clud<strong>in</strong>g officials of <strong>the</strong> government.127
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Over 70% of <strong>the</strong> health budget is externally funded. Most of <strong>the</strong> health resources (facilities,staff, and budget) are not under <strong>the</strong> control and management of <strong>the</strong> State bu<strong>to</strong>f donors and NGOs, who are often critical of <strong>the</strong> lack of leadership and governance<strong>in</strong> <strong>the</strong> sec<strong>to</strong>r. A vicious circle is susta<strong>in</strong>ed as key decisions are ultimately taken outside<strong>the</strong> M<strong>in</strong>istry.The M<strong>in</strong>istry of <strong>Health</strong> had not <strong>in</strong>vested seriously <strong>in</strong> its preparedness for major emergencies.The Disaster Preparedness Unit rema<strong>in</strong>ed grossly understaffed and was <strong>in</strong>effectiveand marg<strong>in</strong>alized <strong>in</strong> this mega-crisis. With <strong>the</strong> loss of its ma<strong>in</strong> build<strong>in</strong>g with staff,files and equipment, <strong>the</strong> M<strong>in</strong>istry was ill-equipped <strong>to</strong> exercise leadership over an unrulyhumanitarian community. A weak <strong>in</strong>stitution fur<strong>the</strong>r weakened by <strong>the</strong> impact was nomatch for f<strong>in</strong>ancially <strong>in</strong>dependent NGOs that felt <strong>the</strong>y had <strong>the</strong> back<strong>in</strong>g of <strong>the</strong> UN,<strong>the</strong> donors (cooperation agencies and/or public op<strong>in</strong>ion), and <strong>the</strong>ir own constituencies.NGOs could and regularly did opt out from any policy or strategy set by <strong>the</strong> M<strong>in</strong>istry.This marg<strong>in</strong>alization persisted throughout <strong>the</strong> year <strong>in</strong> spite of UNICEF and WHOsupport <strong>to</strong> <strong>the</strong> M<strong>in</strong>istry. 133 Streng<strong>the</strong>n<strong>in</strong>g <strong>the</strong> M<strong>in</strong>istry’s ability for strategic plann<strong>in</strong>gand its capacity <strong>to</strong> deliver, areas of greatest weakness <strong>in</strong> <strong>the</strong> eyes of <strong>the</strong> partners, wasnot a priority for <strong>the</strong> <strong>in</strong>ternational humanitarian community. 134 This situation was farfrom unique <strong>to</strong> <strong>Haiti</strong>. It was noted <strong>in</strong> Indonesia and Sri Lanka (although <strong>the</strong> Clusterapproach had not yet been adopted <strong>in</strong> 2004) and <strong>in</strong> Pakistan. However, <strong>in</strong> thosecountries dependence on external assistance was m<strong>in</strong>imal and <strong>in</strong>stitutions were able <strong>to</strong>reassert <strong>the</strong>ir authority <strong>to</strong> a considerable extent. This was due <strong>to</strong> <strong>the</strong> efforts of nationalauthorities, not as a planned strategy by <strong>in</strong>ternational ac<strong>to</strong>rs.A success s<strong>to</strong>ry: <strong>the</strong> water and sanitation agencyAs noted <strong>in</strong> Chapter 6, DINEPA, <strong>the</strong> water and sanitation <strong>in</strong>stitution <strong>in</strong> <strong>Haiti</strong>, offeredan example of how a national entity could reclaim and assume its leadershipand successfully coord<strong>in</strong>ate <strong>the</strong> partners <strong>in</strong> its area of competence.How easily this could have been duplicated <strong>in</strong> o<strong>the</strong>r sec<strong>to</strong>rs—<strong>in</strong> health <strong>in</strong> particular—is debatable. Water and sanitation is far less emotional and visible (andconsequently less political <strong>in</strong>ternationally) than medical care. DINEPA, a relativelywell organized and efficient <strong>in</strong>stitution prior <strong>to</strong> <strong>the</strong> <strong>earthquake</strong>, was alreadyreceiv<strong>in</strong>g direct fund<strong>in</strong>g from major donors and it did not suffer significantlyfrom <strong>the</strong> impact of <strong>the</strong> <strong>earthquake</strong>.To conclude, a comment published on 3 February (three weeks after impact) by anNGO work<strong>in</strong>g <strong>in</strong> <strong>Haiti</strong> says it best (Ivers and Cullen <strong>2010</strong>):32FILM32 32APho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>“[T]he <strong>in</strong>ternational community needs <strong>to</strong> prioritize medium- andlong-term <strong>in</strong>vestment <strong>in</strong> <strong>the</strong> health care system of <strong>Haiti</strong>, which wasweak before <strong>the</strong> <strong>earthquake</strong>. Support must be susta<strong>in</strong>ed and promiseskept if <strong>Haiti</strong> is <strong>to</strong> be rebuilt not only with stronger build<strong>in</strong>gs,but also with a greatly streng<strong>the</strong>ned m<strong>in</strong>istry of health that sets <strong>the</strong>priorities. NGOs must <strong>the</strong>n adopt <strong>the</strong>se priorities and work <strong>in</strong> part-128133 In fact, WHO experience dur<strong>in</strong>g <strong>the</strong> crisis has been one of a much closer association and more open dialogue with <strong>the</strong> highestauthorities than ever before.134 A common critique is <strong>the</strong> proliferation of strategic official documents or plans that are never implemented by <strong>the</strong> M<strong>in</strong>istry of<strong>Health</strong>. However, resources and means for implementation were often not <strong>in</strong> <strong>the</strong> control of <strong>the</strong> M<strong>in</strong>istry but of its <strong>in</strong>dependentm<strong>in</strong>ded partners.
COORDINATION - Chapter 8nership with <strong>the</strong> <strong>Haiti</strong>an government <strong>to</strong> achieve <strong>the</strong>m. We at Partners<strong>in</strong> <strong>Health</strong>—which has worked <strong>in</strong> <strong>Haiti</strong> for 20 years—cont<strong>in</strong>ue<strong>to</strong> believe that <strong>the</strong> <strong>Haiti</strong>an people can be empowered <strong>to</strong> take careof one ano<strong>the</strong>r if <strong>the</strong>y are given monetary support and solidarity.”International coord<strong>in</strong>ationHumanitarian Reform and <strong>the</strong> health sec<strong>to</strong>rThe Inter-Agency Stand<strong>in</strong>g Committee (IASC) is <strong>the</strong> <strong>in</strong>ter-agency forum for coord<strong>in</strong>ation,policy development, and decision mak<strong>in</strong>g <strong>in</strong>volv<strong>in</strong>g <strong>the</strong> key external UN andnon-UN humanitarian partners. It was established <strong>in</strong> June 1992 <strong>in</strong> <strong>response</strong> <strong>to</strong> UnitedNations General Assembly Resolution 46/182 on <strong>the</strong> streng<strong>the</strong>n<strong>in</strong>g of humanitarianassistance. General Assembly Resolution 48/57 affirmed its role as <strong>the</strong> primary mechanismfor <strong>in</strong>ter-agency coord<strong>in</strong>ation of humanitarian assistance.Members are <strong>the</strong> UN operational agencies and selected non-UN humanitarianagencies are stand<strong>in</strong>g <strong>in</strong>vitees. 135 There is no representation or <strong>in</strong>put from disasteraffectedcountries.In 2005, <strong>the</strong> IASC adopted an ambitious Humanitarian Reform cover<strong>in</strong>g severalareas: f<strong>in</strong>anc<strong>in</strong>g of assistance, streng<strong>the</strong>n<strong>in</strong>g <strong>the</strong> function of <strong>the</strong> Humanitarian Coord<strong>in</strong>a<strong>to</strong>r<strong>in</strong> <strong>the</strong> UN, and more systematic and predictable attention <strong>to</strong> all ma<strong>in</strong>sec<strong>to</strong>rs of <strong>response</strong> (“<strong>the</strong> Cluster Approach”) (Holmes 2007). The cluster approachis of more direct concern <strong>to</strong> <strong>the</strong> health m<strong>in</strong>istries <strong>in</strong> affected countries.The cluster approach <strong>in</strong>tends <strong>to</strong> <strong>in</strong>troduce a system of sec<strong>to</strong>ral coord<strong>in</strong>ation agreed uponamong external humanitarian ac<strong>to</strong>rs. It is <strong>in</strong>tended as a mechanism that can help <strong>to</strong>address identified gaps <strong>in</strong> <strong>response</strong> and enhance <strong>the</strong> quality of humanitarian action. 136In September 2005 <strong>the</strong> IASC agreed <strong>to</strong> designate global “cluster leads” <strong>in</strong> n<strong>in</strong>e sec<strong>to</strong>rs orareas of activity. These global sec<strong>to</strong>rs (clusters) as def<strong>in</strong>ed by <strong>the</strong> IASC closely reflect <strong>the</strong>distribution of mandates among ma<strong>in</strong> UN agencies:Technical areas:1. Nutrition2. <strong>Health</strong>3. Water/Sanitation4. Emergency Shelter135 International Committee of <strong>the</strong> Red Cross (ICRC) and International Federation of Red Cross and Red Crescent Societies(IFRC) are stand<strong>in</strong>g <strong>in</strong>vitees. NGOs are represented by <strong>the</strong> International Council of Voluntary Agencies (ICVA) orInterAction which are associations of NGOs.136 Summarized from <strong>the</strong> IASC Guidance Note on Us<strong>in</strong>g <strong>the</strong> Cluster Approach <strong>to</strong> Streng<strong>the</strong>n Humanitarian Response (24 November2006).129
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Cross-cutt<strong>in</strong>g areas:5. Camp Coord<strong>in</strong>ation/Management6. Protection7. Early RecoveryCommon service areas:8. Logistics9. Emergency Telecommunications<strong>Health</strong>, which is an all-<strong>in</strong>clusive concept, 137 was <strong>the</strong>reby split <strong>in</strong><strong>to</strong> three technical areas(nutrition, health, and water and sanitation).The IASC pr<strong>in</strong>cipals (<strong>the</strong> head of agencies) agreed that at country level <strong>the</strong> cluster approachshould be applied, with some flexibility, <strong>in</strong> all new emergencies.The nature of <strong>the</strong> l<strong>in</strong>ks between clusters and <strong>the</strong> host government “will depend on <strong>the</strong>situation <strong>in</strong> each country and on <strong>the</strong> will<strong>in</strong>gness and capacity of each of <strong>the</strong>se ac<strong>to</strong>rs <strong>to</strong>lead or participate <strong>in</strong> humanitarian activities.” 138 Accord<strong>in</strong>g <strong>to</strong> <strong>the</strong> procedures for fieldactivation of <strong>the</strong> clusters, <strong>the</strong> UN Resident Coord<strong>in</strong>a<strong>to</strong>r, follow<strong>in</strong>g consultations with<strong>the</strong> Humanitarian Country Team, submits <strong>the</strong> decision for approval by <strong>the</strong> UN Under-Secretary-General and Emergency Relief Coord<strong>in</strong>a<strong>to</strong>r. The host Government and allo<strong>the</strong>r partners are <strong>the</strong>n <strong>in</strong>formed of <strong>the</strong> decision taken.Global, regional and local coord<strong>in</strong>ation• Disasters trigger<strong>in</strong>g a global <strong>response</strong> call for global coord<strong>in</strong>ation.• Priority sett<strong>in</strong>g and actual coord<strong>in</strong>ation must take place <strong>in</strong> <strong>the</strong> affected country <strong>to</strong>ensure that <strong>the</strong> <strong>response</strong> is relevant <strong>to</strong> <strong>the</strong> unique local context.International coord<strong>in</strong>ation must be done where <strong>the</strong> action is tak<strong>in</strong>g place and whereall humanitarian partners are: at national and sub-national levels.Regional and global levels should be <strong>in</strong> a support mode. Country offices of developmentagencies are designed for long-term cooperation and are not always particularly suitedfor manag<strong>in</strong>g emergency <strong>in</strong>formation and coord<strong>in</strong>at<strong>in</strong>g a massive <strong>response</strong> of “new ac<strong>to</strong>rs”<strong>in</strong> <strong>the</strong> aftermath of a sudden-onset disaster. The national office, regardless of itssec<strong>to</strong>ral mandate, should be offered and accept strong re<strong>in</strong>forcement of managementstaff with humanitarian experience. 139In <strong>Haiti</strong>, <strong>the</strong> magnitude of <strong>the</strong> disaster and <strong>the</strong> global nature of <strong>the</strong> <strong>response</strong> calledfor strong participation of global coord<strong>in</strong>ation mechanisms. In spite of <strong>the</strong>ir efforts<strong>to</strong> play a lead role, regional organizations (political or technical), did not have <strong>the</strong>130137 The WHO constitution def<strong>in</strong>es health as “a state of complete physical, mental and social well be<strong>in</strong>g and not merely <strong>the</strong> absenceof disease or <strong>in</strong>firmity.”138 See <strong>the</strong> One Response web site: http://one<strong>response</strong>.<strong>in</strong>fo/Coord<strong>in</strong>ation/ClusterApproach/Pages/Global%20Cluster%20Leads.aspx.139 Send<strong>in</strong>g additional staff <strong>to</strong> <strong>Haiti</strong> caused some resistance <strong>in</strong> development agencies both <strong>in</strong> terms of f<strong>in</strong>d<strong>in</strong>g <strong>the</strong> appropriatepeople at an agency’s headquarters, and accept<strong>in</strong>g <strong>the</strong> additional expertise <strong>in</strong> <strong>the</strong> country office.
COORDINATION - Chapter 8critical mass <strong>to</strong> assume this leadership. The contributions of OAS, CARICOM, andCDEMA, among o<strong>the</strong>rs, were most valuable but were dwarfed by <strong>the</strong> sheer volume of<strong>the</strong> <strong>in</strong>ternational assistance. 140 PAHO/WHO, as a regional health body, did not have<strong>the</strong> capacity <strong>to</strong> quickly mobilize a sufficient number of experts, especially given <strong>the</strong> desirabilityof French language skills and familiarity with <strong>Haiti</strong>, which is uncharacteristicof o<strong>the</strong>r countries <strong>in</strong> <strong>the</strong> region.The most valuable asset of a regional office rema<strong>in</strong>s its closeness <strong>to</strong> <strong>the</strong> health authorities,<strong>the</strong> health services, and <strong>the</strong> health conditions. This familiarity with <strong>the</strong> local contextis an important asset <strong>to</strong> ensure that future coord<strong>in</strong>ation streng<strong>the</strong>ns ra<strong>the</strong>r thanhampers <strong>the</strong> capacity of <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong>.Cluster application and health implications <strong>in</strong> <strong>Haiti</strong>• Clusters <strong>in</strong> a given country should reflect <strong>the</strong> mandate of <strong>the</strong> l<strong>in</strong>e m<strong>in</strong>istries.• When necessary, participation should be limited <strong>to</strong> those <strong>in</strong> a position <strong>to</strong> offer a significantcontribution.• At <strong>the</strong> early stage, a small executive committee and technical work groups should be establishedunder <strong>the</strong> leadership of <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong>.At <strong>the</strong> global level, <strong>the</strong> normative work of <strong>the</strong> Global Clusters resulted <strong>in</strong> an array of technicalguidel<strong>in</strong>es that facilitated and guided <strong>the</strong> field work (for <strong>in</strong>stance, on user fees <strong>in</strong> emergencysituations, mental health and psychosocial assistance, gender-based violence, etc.).At <strong>the</strong> country level, <strong>Haiti</strong> already had experience work<strong>in</strong>g with clusters dur<strong>in</strong>g <strong>the</strong><strong>response</strong> <strong>to</strong> <strong>the</strong> tropical s<strong>to</strong>rms and hurricanes that hit <strong>the</strong> country <strong>in</strong> August and September2008. Many of <strong>the</strong> f<strong>in</strong>d<strong>in</strong>gs and recommendations <strong>in</strong> <strong>the</strong> Cluster Evaluationfor <strong>Haiti</strong> (B<strong>in</strong>der and Grünewald <strong>2010</strong>), which was carried out before <strong>the</strong> <strong>earthquake</strong>,rema<strong>in</strong> pert<strong>in</strong>ent. Some of <strong>the</strong> most relevant are:• “Underm<strong>in</strong><strong>in</strong>g of local ownership due <strong>to</strong> a <strong>to</strong>p-down approach and a membershipexclud<strong>in</strong>g local NGOs and government or donors;• “Lack of clear criteria for activation and deactivation;• “Improved identification of exist<strong>in</strong>g gaps but no evidence of those gaps be<strong>in</strong>g betterfilled;• “Improved <strong>in</strong>formation shar<strong>in</strong>g but poor <strong>in</strong>formation management (lost or untimely<strong>in</strong>formation);• “Weak <strong>in</strong>ter-cluster (cross-sec<strong>to</strong>rial) coord<strong>in</strong>ation…”In <strong>the</strong> case of <strong>the</strong> 12 <strong>January</strong> <strong>earthquake</strong>, <strong>the</strong> devastat<strong>in</strong>g impact on <strong>the</strong> weak capacityof <strong>the</strong> <strong>Haiti</strong>an Government made activat<strong>in</strong>g <strong>the</strong> clusters <strong>the</strong> most promis<strong>in</strong>g approachfor some measure of coord<strong>in</strong>ation at least dur<strong>in</strong>g <strong>the</strong> first few weeks of <strong>the</strong> <strong>response</strong>.140 An orig<strong>in</strong>al and much appreciated <strong>in</strong>itiative from CDEMA has been <strong>to</strong> sponsor short periods of rest <strong>in</strong> Jamaica for key staffof <strong>Haiti</strong>’s M<strong>in</strong>istry of <strong>Health</strong>. The <strong>in</strong>itiative was very similar <strong>to</strong> <strong>the</strong> statu<strong>to</strong>ry “Rest and Recuperation” (RR) leave with full paygranted <strong>to</strong> <strong>in</strong>ternational UN staff who were required <strong>to</strong> work for extended periods at <strong>the</strong> duty stations under hazardous, stressfuland difficult conditions.131
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>The number of sec<strong>to</strong>rs/clusters activated <strong>in</strong> <strong>Haiti</strong> exceed <strong>the</strong> number <strong>in</strong>itially envisagedby <strong>the</strong> Humanitarian Reform: agriculture, camp coord<strong>in</strong>ation/management,early recovery, education, emergency telecommunications, food distribution, health,logistics, nutrition, protection (which <strong>in</strong>cluded two sub-clusters: child protection andgender-based violence), shelters, non-food items, and f<strong>in</strong>ally water, sanitation, andhygiene–a <strong>to</strong>tal of 12 clusters and two subsec<strong>to</strong>rs. All clusters were led by an <strong>in</strong>ternationalagency with <strong>the</strong> exception of <strong>the</strong> water, sanitation, and hygiene cluster, <strong>in</strong>itiallyassigned <strong>to</strong> UNICEF but actually led by DINEPA at its own request.The structure adopted did not seek <strong>to</strong> match <strong>the</strong> structure of <strong>the</strong> <strong>Haiti</strong>an State that<strong>the</strong> system was designed <strong>to</strong> assist. For <strong>in</strong>stance, <strong>the</strong> responsibilities of <strong>the</strong> M<strong>in</strong>istry of<strong>Health</strong> were distributed <strong>to</strong> <strong>the</strong> three clusters but also <strong>to</strong> a higher number of work<strong>in</strong>ggroups, several under additional clusters (camp management, protection, etc.). Thisshould be avoided <strong>in</strong> future disasters by match<strong>in</strong>g <strong>the</strong> clusters structure <strong>to</strong> <strong>the</strong> scopeof mandate of <strong>the</strong> l<strong>in</strong>e m<strong>in</strong>istries.The section below focuses on <strong>the</strong> <strong>Health</strong> Cluster. It was responsible for everyth<strong>in</strong>ghealth related for which ano<strong>the</strong>r cluster had not been set up.The <strong>in</strong>itial implementation of <strong>the</strong> <strong>Health</strong> Cluster met considerable challenges and hada slow learn<strong>in</strong>g curve. The challenges <strong>in</strong>cluded:• Severe logistics limitations, among which were security restrictions. As noted by<strong>the</strong> UN Humanitarian Coord<strong>in</strong>a<strong>to</strong>r <strong>in</strong> May <strong>2010</strong>, “<strong>the</strong>re has been ongo<strong>in</strong>g discussionof protect<strong>in</strong>g ‘humanitarian space’. Yet <strong>Haiti</strong> is not <strong>the</strong> [Democratic Republicof <strong>the</strong> Congo]; <strong>the</strong> humanitarian <strong>response</strong> is not tak<strong>in</strong>g place <strong>in</strong> a war zone, <strong>in</strong> anenvironment of civil conflict between warr<strong>in</strong>g factions.” This statement is supportedby evidence that “between 2007 and 2009 collective violence had dramaticallydecl<strong>in</strong>ed even if o<strong>the</strong>r forms of violence—that is, sexual and gender-based—began<strong>to</strong> appear more visible” (Muggah <strong>2010</strong>).• A randomized household survey (n=2,940) <strong>in</strong> <strong>the</strong> months after <strong>the</strong> <strong>earthquake</strong><strong>in</strong>dicated that crime and victimization rates were lower than announced <strong>in</strong> <strong>the</strong>global media. “Contrary <strong>to</strong> media claims of widespread loot<strong>in</strong>g and organised<strong>the</strong>ft, <strong>the</strong> vast majority of Port-au-Pr<strong>in</strong>ce residents reported that nei<strong>the</strong>r <strong>the</strong>y norany members of <strong>the</strong>ir household had had property s<strong>to</strong>len from <strong>the</strong>m or <strong>in</strong>tentionallydestroyed by o<strong>the</strong>rs s<strong>in</strong>ce <strong>the</strong> <strong>earthquake</strong>”(Muggah <strong>2010</strong>). Only 20% of <strong>the</strong>respondents considered <strong>in</strong>security/crime a very serious or serious problem after <strong>the</strong><strong>earthquake</strong> compared <strong>to</strong> 62.9% prior <strong>to</strong> <strong>the</strong> <strong>earthquake</strong>. (Kolbe 2009, Kolbe andMuggah <strong>2010</strong>).These f<strong>in</strong>d<strong>in</strong>gs are supported by <strong>the</strong> lower number of gunshot wounds treated byMSF <strong>in</strong> <strong>the</strong> first month after <strong>the</strong> <strong>earthquake</strong> (see Figure 8.1). As noted by MSF,<strong>in</strong>terventions for gunshot wounds are part of every day life <strong>in</strong> <strong>Haiti</strong>, but <strong>the</strong>y wereless frequent <strong>in</strong> <strong>the</strong> first month follow<strong>in</strong>g <strong>the</strong> <strong>earthquake</strong>.132
COORDINATION - Chapter 8Figure 8.1 Number of operations for gunshot wounds performed<strong>in</strong> MSF facilities, 13 <strong>January</strong> <strong>to</strong> 12 April <strong>2010</strong>, <strong>Haiti</strong>1009080Number of <strong>in</strong>terventions7060504030<strong>2010</strong>01st month 2nd month 3rd monthSource: Axelle Ronsse, Médic<strong>in</strong>s sans Frontières, Surgical <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>2010</strong> <strong>Haiti</strong> <strong>earthquake</strong> (powerpo<strong>in</strong>t presentation).Used with permission.32FILM• The dist<strong>in</strong>ct perception at <strong>in</strong>ternational level and <strong>the</strong> result<strong>in</strong>g restrictions,which were perhaps due <strong>to</strong> unrealisitically alarmist scenarios and extraneousconsiderations, fur<strong>the</strong>r alienated <strong>the</strong> UN ac<strong>to</strong>rs from <strong>the</strong>ir counterparts and <strong>the</strong>population. 141 A new UN Security Management System was <strong>in</strong>tended <strong>to</strong> movedecision-mak<strong>in</strong>g away from “go/no-go” <strong>to</strong> balanc<strong>in</strong>g risk and opportunity. 142 Itsapplication was not felt yet <strong>in</strong> <strong>Haiti</strong>.• A large number of organizations performed far above expectations but a significantnumber were m<strong>in</strong>or ac<strong>to</strong>rs without significant experience or resources and <strong>the</strong>reforeunable <strong>to</strong> offer added value. The <strong>Health</strong> Cluster meet<strong>in</strong>gs became an opportunity<strong>to</strong> claim visibility (flag wav<strong>in</strong>g) or for newcomers <strong>to</strong> collect basic <strong>in</strong>formationon what <strong>to</strong> do and where <strong>to</strong> go. The strategic coord<strong>in</strong>ation objective was lost. Tokeep clusters from collaps<strong>in</strong>g under <strong>the</strong>ir own weight <strong>in</strong> future disasters, filter<strong>in</strong>gor “triage” of participants may be required. Cluster support should be directed<strong>to</strong> those agencies and ac<strong>to</strong>rs most likely <strong>to</strong> provide significant benefits for <strong>the</strong>health of <strong>the</strong> affected population.Pho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>32 32A141 The early and excellent decision of PAHO/WHO <strong>to</strong> move <strong>in</strong><strong>to</strong> PROMESS facilities ra<strong>the</strong>r than <strong>to</strong> <strong>the</strong> MINUSTAHbase (“LogBase”)—as <strong>in</strong>structed by UN security—had a positive impact on its future activities, offsett<strong>in</strong>g <strong>the</strong> disadvantagesof be<strong>in</strong>g relatively far from <strong>the</strong> clusters’ meet<strong>in</strong>g place.142 This shift from risk aversion <strong>to</strong> risk management represents <strong>the</strong> culm<strong>in</strong>ation of <strong>the</strong> past decade’s evolution <strong>in</strong> th<strong>in</strong>k<strong>in</strong>gand methodology for programm<strong>in</strong>g <strong>in</strong> <strong>in</strong>secure conditions. Key <strong>to</strong> this shift is <strong>the</strong> concept of <strong>the</strong> enabl<strong>in</strong>g security approach,i.e., an approach that focuses on “how <strong>to</strong> provide services” as opposed <strong>to</strong> “when <strong>to</strong> be grounded”. Under thisnew approach, <strong>the</strong> use of military or armed escorts for humanitarian agencies is purely a security risk mitigation measure<strong>to</strong> reduce security risks from one acceptable risk level <strong>to</strong> ano<strong>the</strong>r (ra<strong>the</strong>r than reduc<strong>in</strong>g risk from an unacceptable <strong>to</strong> anacceptable level as rema<strong>in</strong>ed mostly <strong>the</strong> case <strong>in</strong> <strong>the</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong>).133
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>A slow learn<strong>in</strong>g curve resulted from <strong>the</strong> extreme pressure on <strong>the</strong> few senior staff <strong>in</strong>volved<strong>in</strong> <strong>the</strong> cluster process. Respond<strong>in</strong>g <strong>to</strong> urgent needs delayed important decisions.Among <strong>the</strong> positive measures taken belatedly were:• Sett<strong>in</strong>g up a select group of agencies work<strong>in</strong>g <strong>in</strong> <strong>Haiti</strong> before, dur<strong>in</strong>g, and after <strong>the</strong><strong>earthquake</strong> <strong>to</strong> agree upon strategic options and collectively guide <strong>the</strong> process: Thecluster was <strong>in</strong>itially conceived precisely <strong>to</strong> provide this guidance. Democratic consensus-build<strong>in</strong>gamong all participants proves not <strong>to</strong> be effective <strong>in</strong> acute <strong>response</strong>management. After several weeks this “small committee,” where keys options anddecisions were debated, was quietly set up among 19 larger agencies that have along-term commitment <strong>in</strong> <strong>Haiti</strong>. 143• Organiz<strong>in</strong>g technical work<strong>in</strong>g groups where specific <strong>the</strong>matic <strong>to</strong>pics could be discussedat <strong>the</strong> level of practical details: Ultimately those work<strong>in</strong>g groups <strong>in</strong>cluded<strong>the</strong> follow<strong>in</strong>g <strong>to</strong>pics: hospitals, mobile cl<strong>in</strong>ics, mental health and psychosocial support,vec<strong>to</strong>r control, epidemiology, disabilities, and <strong>in</strong>formation. Experience hasshown <strong>in</strong> <strong>the</strong> disasters <strong>in</strong> <strong>Haiti</strong>, Indonesia, Sri Lanka, Pakistan, and o<strong>the</strong>rs that <strong>the</strong>work <strong>in</strong> <strong>the</strong>matic sub-groups was far more concrete and productive than <strong>in</strong> <strong>the</strong>large forum. In future disasters, establish<strong>in</strong>g some or all of those groups from <strong>the</strong>early stage of <strong>the</strong> emergency should be considered.• Decentraliz<strong>in</strong>g <strong>the</strong> <strong>Health</strong> Cluster <strong>to</strong> departments (away from <strong>the</strong> capital): a veryefficient measure that should be planned earlier <strong>in</strong> future large disasters.In addition <strong>to</strong> coord<strong>in</strong>at<strong>in</strong>g <strong>the</strong> outcome from all those sub-groups, <strong>the</strong> health sec<strong>to</strong>r wasalso attempt<strong>in</strong>g <strong>to</strong> ma<strong>in</strong>ta<strong>in</strong> coherence <strong>in</strong> public health activities that were be<strong>in</strong>g coord<strong>in</strong>atedby o<strong>the</strong>r clusters (nutrition, hygiene and community health education, reproductive health,HIV/AIDS, and gender-based violence, among o<strong>the</strong>rs).As noted <strong>in</strong> <strong>the</strong> 2009 evaluation of clusters <strong>in</strong> six country studies (<strong>in</strong>clud<strong>in</strong>g <strong>Haiti</strong>,Hurricane 2008), <strong>in</strong>ter-cluster coord<strong>in</strong>ation was <strong>in</strong>effective <strong>in</strong> most cases and did notlead <strong>to</strong> <strong>in</strong>tegration of cross-cutt<strong>in</strong>g issues (IASC <strong>2010</strong>a, 6). This observation was stillaccurate <strong>in</strong> <strong>2010</strong>.In spite of <strong>the</strong> serious shortcom<strong>in</strong>gs <strong>in</strong> terms of national ownership, this donor-supportedapproach has considerable value <strong>in</strong> <strong>the</strong> first weeks especially when those nationalcoord<strong>in</strong>at<strong>in</strong>g bodies which are severely affected are still under <strong>the</strong> shock of <strong>the</strong> impact.If coord<strong>in</strong>ation was difficult <strong>to</strong> achieve, it is due <strong>to</strong> <strong>the</strong> absence of legal or formalauthority over <strong>the</strong> “partners,” normally <strong>the</strong> exclusive prerogative of <strong>the</strong> State, and<strong>the</strong> chaotic and exponential escalation of humanitarian assistance ra<strong>the</strong>r than <strong>to</strong> <strong>the</strong>faulty design of this gap-fill<strong>in</strong>g coord<strong>in</strong>ation model. It must be said, however, that <strong>in</strong>disasters of <strong>the</strong> scale of <strong>Haiti</strong>’s, effective coord<strong>in</strong>ation is almost impossible <strong>to</strong> achieve.The clusters rapidly outlived <strong>the</strong>ir usefulness—and <strong>the</strong>ir welcome—with <strong>Haiti</strong>an counterparts.The failure of <strong>the</strong> humanitarian community <strong>to</strong> implement an early albeit progressiveand moni<strong>to</strong>red transfer of leadership and responsibility <strong>to</strong> <strong>the</strong> national Direc<strong>to</strong>rate forCivil Protection, <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong> and o<strong>the</strong>r l<strong>in</strong>e m<strong>in</strong>istries rapidly eroded <strong>the</strong> tenuouslegitimacy of <strong>the</strong> clusters <strong>in</strong> a country with an established and recognized government.The result has been a weaken<strong>in</strong>g of <strong>the</strong> <strong>in</strong>stitutions: The pr<strong>in</strong>ciple of “First, do no Harm”143 Unfortunately <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong> was not systematically <strong>in</strong>vited <strong>to</strong> participate <strong>in</strong> <strong>the</strong> “small committee” meet<strong>in</strong>gs.134
COORDINATION - Chapter 8has been overlooked. Unfortunately, <strong>the</strong> situation after <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> was noexception. This has been observed and reported <strong>in</strong> past major disasters.The argument of <strong>the</strong> <strong>in</strong>herent <strong>in</strong>ability of <strong>the</strong> <strong>Haiti</strong>an authorities <strong>to</strong> manage such a crisishas been proven fallacious <strong>in</strong> view of <strong>the</strong> role played by DINEPA. It demonstratedthat such a transition or shar<strong>in</strong>g of power was <strong>in</strong>deed possible even <strong>in</strong> <strong>the</strong> difficultenvironment of <strong>Haiti</strong>.The coord<strong>in</strong>ation by lead agencies, mostly UN agencies, left room for considerable improvement.However, challenges and obstacles <strong>to</strong> coord<strong>in</strong>ation were not limited <strong>to</strong> <strong>the</strong><strong>in</strong>ternational system. The <strong>response</strong> taxed <strong>the</strong> coord<strong>in</strong>ation mechanisms of <strong>the</strong> largestdonors as well. In <strong>the</strong> health sec<strong>to</strong>r, <strong>the</strong> U.S. Department of <strong>Health</strong> and Human Services(HHS) worked <strong>in</strong> an environment <strong>in</strong> which <strong>the</strong> Department of State served as <strong>the</strong> leadfor <strong>the</strong> fatality management mission, USAID served as <strong>the</strong> lead for public health andmedical care <strong>to</strong> <strong>the</strong> <strong>Haiti</strong>an population, <strong>the</strong> Department of Homeland Security was<strong>the</strong> lead for repatriation of U.S. citizens, and <strong>the</strong> Department of State with <strong>the</strong> FederalEmergency Management Agency (FEMA) coord<strong>in</strong>ated patient movements. That wasjust for <strong>Health</strong> and Human Services’ own activities. In addition, health assistance wasprovided by <strong>the</strong> Department of Defense and Department of State agencies.If achiev<strong>in</strong>g effective communication and coord<strong>in</strong>ation <strong>in</strong> <strong>the</strong> <strong>response</strong> from onecountry was difficult, <strong>the</strong> task of coord<strong>in</strong>at<strong>in</strong>g all ac<strong>to</strong>rs was far more complex andambitious.135
The health sec<strong>to</strong>r’s ultimate goal dur<strong>in</strong>ga disaster rema<strong>in</strong>s reduc<strong>in</strong>g all possibleavoidable deaths, disabilities and suffer<strong>in</strong>g.(Picture taken at <strong>the</strong> pediatric ward of <strong>the</strong>HUEH hospital).Pho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>
Chapter9Key strategiclessonsnextfor <strong>the</strong>sudden-onsetdisasterIn this chapter, <strong>the</strong> focus is on strategic lessons of global use. Among sudden-onset disasters,<strong>earthquake</strong>s pose a particularly difficult challenge <strong>to</strong> <strong>the</strong> <strong>in</strong>ternational community.Speed and professionalism dur<strong>in</strong>g <strong>the</strong> <strong>response</strong> are critical. Among <strong>earthquake</strong>s,<strong>Haiti</strong> was an exceptional situation. Consequently, not all <strong>the</strong> lessons from <strong>Haiti</strong> willbe relevant <strong>to</strong> <strong>the</strong> next catastrophic <strong>earthquake</strong>.The magnitude of <strong>in</strong>ternational <strong>response</strong> has <strong>in</strong>creased dramatically from one disaster<strong>to</strong> <strong>the</strong> next. This growth has many positive aspects:• First, many develop<strong>in</strong>g countries, neighbors or not, are now jo<strong>in</strong><strong>in</strong>g <strong>the</strong> more traditionalhumanitarian donors <strong>to</strong> respond <strong>to</strong> disasters. A number of specialized137
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>agencies are fill<strong>in</strong>g small niches neglected <strong>in</strong> <strong>the</strong> past and new NGOs are provid<strong>in</strong>gcollective services <strong>to</strong> o<strong>the</strong>r partners (communications, <strong>in</strong>formation, logistics, etc.).There are now numerous organizations active <strong>in</strong> a variety of health discipl<strong>in</strong>es,creat<strong>in</strong>g <strong>the</strong> potential for great diversity and coverage of services.• This rapid growth has come with a lot of pa<strong>in</strong> and changes. In <strong>the</strong> health sec<strong>to</strong>r,a two-fold process is emerg<strong>in</strong>g: On one side, <strong>the</strong> established humanitarian organizationsare becom<strong>in</strong>g more professional by develop<strong>in</strong>g <strong>the</strong>ir own standards andnorms and tra<strong>in</strong><strong>in</strong>g <strong>the</strong>ir staff. On <strong>the</strong> o<strong>the</strong>r side, <strong>the</strong> number of <strong>in</strong>experiencednewcomers (NGOs, universities, countries, and o<strong>the</strong>rs) is ris<strong>in</strong>g rapidly. Some of<strong>the</strong>se new ac<strong>to</strong>rs plan <strong>to</strong> rema<strong>in</strong> <strong>in</strong> <strong>the</strong> humanitarian field, which justifies <strong>the</strong> <strong>in</strong>vestmentmade by more established agencies <strong>in</strong> guid<strong>in</strong>g <strong>the</strong>ir first steps. In <strong>the</strong> verydist<strong>in</strong>ctive health vacuum of <strong>Haiti</strong>, <strong>the</strong>y did contribute positively and will improve<strong>the</strong>ir performance. However, a ris<strong>in</strong>g m<strong>in</strong>ority of new ac<strong>to</strong>rs, with doubtful healthcompetence or with questionable motives, were def<strong>in</strong>itely more a h<strong>in</strong>drance thanhelp. They should be filtered out by <strong>the</strong> health authorities.Few of <strong>the</strong> lessons from <strong>the</strong> health <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>Haiti</strong> <strong>earthquake</strong> are new or groundbreak<strong>in</strong>g.Most have been “learned” <strong>in</strong> a variety of regional workshops and published<strong>in</strong> formal evaluations. Consider <strong>the</strong> regional workshop follow<strong>in</strong>g <strong>the</strong> Indian Oceantsunami (UN 2005), <strong>the</strong> analysis of <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>Haiti</strong> <strong>earthquake</strong> published byALNAP (<strong>2010</strong>), an evaluation of <strong>the</strong> health sec<strong>to</strong>r <strong>in</strong> <strong>Haiti</strong> one year after <strong>the</strong> <strong>earthquake</strong>(Merl<strong>in</strong> 2011), or <strong>the</strong> notes on prelim<strong>in</strong>ary lessons learned from <strong>Haiti</strong> (Fisher<strong>2010</strong>).The humanitarian community seems <strong>to</strong> have little <strong>in</strong>stitutional memory or capacity<strong>to</strong> change.Is a better organized <strong>response</strong> possible?Lack of <strong>in</strong>formation shar<strong>in</strong>g and coord<strong>in</strong>ation (two <strong>in</strong>tertw<strong>in</strong>ed concepts) is <strong>the</strong> mostcommon criticism <strong>in</strong> <strong>the</strong> aftermath of disasters. It is easily documented by externalevalua<strong>to</strong>rs, eagerly conveyed by mass media, and conveniently used by lead agencies<strong>to</strong> call for more resources and staff.There are two relevant questions: 1) Is it possible <strong>to</strong> significantly improve <strong>the</strong> <strong>in</strong>formation?2) Is it possible <strong>to</strong> effectively coord<strong>in</strong>ate such an unruly world of humanitarianorganizations?Is it possible <strong>to</strong> significantly improve <strong>the</strong> <strong>in</strong>formation? In <strong>the</strong> health field, <strong>the</strong> <strong>response</strong> isa def<strong>in</strong>ite “yes.”The first step is <strong>to</strong> identify (conservatively and pragmatically) what must be known<strong>to</strong> improve relief and what can be collected <strong>in</strong> time for this <strong>in</strong>formation <strong>to</strong> have <strong>the</strong>proper impact (not what we would love <strong>to</strong> know). In matters of immediate traumacare, which is a rapidly chang<strong>in</strong>g field, perhaps not much can be known and dissem<strong>in</strong>atedbefore it becomes obsolete.138
KEY STRATEGIC LESSONS FOR THE NEXT SUDDEN-ONSET DISASTER - Chapter 9The second step is <strong>to</strong> deploy qualified human resources <strong>in</strong> time. This implies <strong>in</strong>teragencyagreements and <strong>the</strong> capacity <strong>to</strong> share rosters of experts. It supposes a significant<strong>in</strong>vestment <strong>in</strong> deployment of human resources and logistic support at <strong>the</strong> time of <strong>the</strong>crisis and a shift of lead agencies’ priorities from visible delivery of “hard” services <strong>to</strong>“soft” <strong>in</strong>formation management.Is it possible <strong>to</strong> effectively coord<strong>in</strong>ate such an unruly world of organizations? In <strong>the</strong> healthfield, <strong>the</strong> <strong>response</strong> is a more qualified “yes.”More human and f<strong>in</strong>ancial resources and def<strong>in</strong>itely more meet<strong>in</strong>gs are not necessarily <strong>the</strong>solution. Coord<strong>in</strong>ation should not be an end <strong>in</strong> itself. Some level of chaos is an <strong>in</strong>tegralpart of <strong>the</strong> <strong>in</strong>itial <strong>response</strong> <strong>to</strong> large disasters. To what extent “more” coord<strong>in</strong>ation will improve<strong>the</strong> fate of <strong>the</strong> affected population deserves scrut<strong>in</strong>y. A high-level UN official <strong>in</strong> <strong>Haiti</strong>concluded privately that <strong>the</strong> lack of coord<strong>in</strong>ation <strong>in</strong> <strong>the</strong> first two months may have <strong>in</strong> factpermitted mean<strong>in</strong>gful, community-level contributions from <strong>the</strong> many small or marg<strong>in</strong>alac<strong>to</strong>rs. The same ac<strong>to</strong>rs were seen as a major burden <strong>in</strong> past disasters <strong>in</strong> countries with morenational capacity. Response and coord<strong>in</strong>ation must be determ<strong>in</strong>ed by <strong>the</strong> context.A particular area that may benefit from quality control and improved coord<strong>in</strong>ation isthat of foreign medical care assistance. The next disaster may require a substantial andrapid mobilization of senior managers and <strong>the</strong>matic experts, with significant logisticalsupport, which is very problematic <strong>in</strong> <strong>the</strong> first days when needed most. WHO andits regional offices need <strong>to</strong> seek partnerships with bilateral and o<strong>the</strong>r <strong>in</strong>stitutions <strong>to</strong>develop a roster of experts and considerably <strong>in</strong>crease <strong>the</strong>ir surge capacity <strong>to</strong> coord<strong>in</strong>ate<strong>the</strong> <strong>in</strong>com<strong>in</strong>g flow of medical responders. The Global Outbreak Alert and ResponseNetwork (GOARN) may serve as a useful model. Many bilateral groups and NGOshave demonstrated a high level of technical competence and critical analysis. Theirsupport and participation will be most valuable.The efforts of INSARAG <strong>to</strong> improve search and rescue assistance may provide someadditional clues <strong>to</strong> <strong>the</strong> way forward <strong>in</strong> <strong>the</strong> health sec<strong>to</strong>r. An <strong>in</strong>dependent review ofits impact <strong>in</strong> <strong>Haiti</strong> is, however, still lack<strong>in</strong>g (i.e., “What would have happened if thissusta<strong>in</strong>ed <strong>in</strong>vestment had not been made by INSARAG?”).In o<strong>the</strong>r words, we need <strong>to</strong> shift from outcome <strong>in</strong>dica<strong>to</strong>rs (“more coord<strong>in</strong>ation isbetter”) <strong>to</strong> impact appraisal by demonstrat<strong>in</strong>g that divert<strong>in</strong>g funds from relief activities<strong>to</strong>ward coord<strong>in</strong>ation and quality control actually does save more lives.Ownership of <strong>the</strong> disasterMobiliz<strong>in</strong>g more external coord<strong>in</strong>a<strong>to</strong>rs will not, <strong>in</strong> itself, improve coord<strong>in</strong>ation. Coord<strong>in</strong>ationwithout mean<strong>in</strong>gful participation and leadership of <strong>the</strong> national healthauthorities is ultimately doomed <strong>to</strong> fail.One of <strong>the</strong> key f<strong>in</strong>d<strong>in</strong>gs of <strong>the</strong> self-evaluation of <strong>the</strong> UN Country HumanitarianTeam <strong>in</strong> <strong>Haiti</strong> was <strong>the</strong> need <strong>to</strong> ensure national ownership of <strong>the</strong> disaster <strong>response</strong>.“Government, however weak, has <strong>to</strong> play a central role <strong>in</strong> humanitarian leadership139
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>and coord<strong>in</strong>ation of post-natural disaster. We as humanitarian leaders and ac<strong>to</strong>rs have<strong>to</strong> accept and facilitate this.”To follow up on those f<strong>in</strong>d<strong>in</strong>gs, <strong>the</strong> IASC recommended that:• “Wherever possible, <strong>in</strong>ternational humanitarian ac<strong>to</strong>rs should <strong>the</strong>n organize <strong>the</strong>mselves<strong>to</strong> support or complement exist<strong>in</strong>g national <strong>response</strong> mechanisms ra<strong>the</strong>rthan create parallel ones which may actually weaken or underm<strong>in</strong>e national efforts.• “Where appropriate and practical, government leads should be actively encouraged<strong>to</strong> co-chair cluster meet<strong>in</strong>gs with <strong>the</strong>ir Cluster Lead Agency counterparts. Aswith all co-chair arrangements, respective responsibilities should be clearly def<strong>in</strong>edfrom <strong>the</strong> outset” (IASC 2011).Sudden-onset disasters are creat<strong>in</strong>g a wave of generosity (and <strong>the</strong>refore a high numberof volunteers who are <strong>in</strong> need of coord<strong>in</strong>ation, and strong competition for fund<strong>in</strong>gand visibility among ac<strong>to</strong>rs which is <strong>in</strong> need of arbitration). In such disasters, <strong>the</strong> clusterapproach must be implemented differently <strong>to</strong> ensure national ownership.Assert<strong>in</strong>g <strong>the</strong> national government’s primary role <strong>in</strong> coord<strong>in</strong>at<strong>in</strong>g and selectively filter<strong>in</strong>gexternal assistance is not an easy matter for national authorities even when localhealth resources have <strong>the</strong> capacity <strong>to</strong> respond effectively. 144 The perception held by <strong>the</strong>public that <strong>the</strong> <strong>in</strong>ternational community is better suited <strong>to</strong> coord<strong>in</strong>ate <strong>response</strong> guaranteesthat weaker national <strong>in</strong>stitutions will cont<strong>in</strong>ue <strong>to</strong> be marg<strong>in</strong>alized, and fur<strong>the</strong>rweakened. Coord<strong>in</strong>ation should be a key feature of national disaster preparedness.A formal agreement on <strong>the</strong> cluster approach with governments prior <strong>to</strong> <strong>the</strong> disaster is an<strong>in</strong>dispensable prelim<strong>in</strong>ary step.As part of jo<strong>in</strong>t preparedness efforts, a formal agreement for sec<strong>to</strong>ral coord<strong>in</strong>ation(cluster approach) should be discussed with those countries most vulnerable <strong>to</strong> largescale,sudden-onset natural disasters. Many potential worst-case, urban <strong>earthquake</strong>scenarios have already been identified and those countries are receiv<strong>in</strong>g technical cooperation<strong>in</strong> preparedness from <strong>the</strong> UN and bilateral agencies. Under this agreement:• The Government will determ<strong>in</strong>e <strong>the</strong> number and scope of responsibility of <strong>the</strong> sec<strong>to</strong>rs/clustersat <strong>the</strong> national level <strong>in</strong> order <strong>to</strong> better reflect <strong>the</strong> organization of <strong>the</strong>government and respective mandate of <strong>the</strong> l<strong>in</strong>e m<strong>in</strong>istries. Adjust<strong>in</strong>g <strong>the</strong> clusters<strong>to</strong> national structure is a requirement <strong>to</strong> facilitate <strong>the</strong> early and smooth transferof responsibility <strong>to</strong> <strong>the</strong> government. The sec<strong>to</strong>r/cluster structure at national levelwill vary from country <strong>to</strong> country (<strong>in</strong> l<strong>in</strong>e with <strong>the</strong> flexibility recommended <strong>in</strong> <strong>the</strong>2006 IASC guidel<strong>in</strong>es recogniz<strong>in</strong>g that “one size does not fit all”).• The Government, <strong>in</strong> consultation with <strong>the</strong> UN Humanitarian Country Team, willdesignate <strong>in</strong> advance one or more (co-lead) agencies <strong>to</strong> assist <strong>the</strong> national <strong>in</strong>stitution(l<strong>in</strong>e m<strong>in</strong>istry) responsible for each sec<strong>to</strong>r. Those lead agencies may or maynot be <strong>the</strong> same as those at global level (ano<strong>the</strong>r recommendation of <strong>the</strong> IASC140144 Follow<strong>in</strong>g <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> Mexico City (1985), hospital bed occupancy never exceeded 95% and <strong>the</strong> ample resources ofthis large country were mobilized. The Government <strong>in</strong>itially decl<strong>in</strong>ed external medical assistance. With<strong>in</strong> one day, however,a campaign launched by <strong>the</strong> <strong>in</strong>ternational media forced <strong>the</strong> Government <strong>to</strong> withdraw its decision and open its borders <strong>to</strong>foreign medical teams.
KEY STRATEGIC LESSONS FOR THE NEXT SUDDEN-ONSET DISASTER - Chapter 9guidel<strong>in</strong>es). It would not affect <strong>the</strong> role of <strong>the</strong> cluster lead agency at global level. Itis also unders<strong>to</strong>od that <strong>in</strong> <strong>the</strong> immediate life-sav<strong>in</strong>g phase, <strong>the</strong> co-lead UN agenciesmay have <strong>to</strong> actually manage and coord<strong>in</strong>ate <strong>the</strong> entire <strong>response</strong> <strong>in</strong> exceptionalsituations such as <strong>in</strong> <strong>Haiti</strong>.• The agreement will endorse <strong>the</strong> exist<strong>in</strong>g 24-hour activation mechanism for <strong>the</strong>clusters but ensure explicit participation of <strong>the</strong> government <strong>in</strong> <strong>the</strong> UN decisionmak<strong>in</strong>gprocess (beyond merely <strong>in</strong>form<strong>in</strong>g authorities).• F<strong>in</strong>ally, a clear end-date (for example, three weeks) will be set for ei<strong>the</strong>r transfer ofresponsibility <strong>to</strong> <strong>the</strong> national <strong>in</strong>stitution or a formal request for extension of <strong>the</strong>lead role of <strong>the</strong> <strong>in</strong>ternational agencies for a specified period, should <strong>the</strong> nationalauthorities deem that necessary.In brief, <strong>the</strong> humanitarian community must acknowledge that <strong>in</strong> order <strong>to</strong> streng<strong>the</strong>n<strong>the</strong> capacity of national authorities it is worth tak<strong>in</strong>g <strong>the</strong> risk, <strong>in</strong> <strong>the</strong> short-term, ofhav<strong>in</strong>g less “efficient” or “experienced” coord<strong>in</strong>ation. Indeed, <strong>the</strong> risk of additionalchaos might be less than anticipated consider<strong>in</strong>g <strong>the</strong> poor performance of externalcoord<strong>in</strong>ation <strong>in</strong> <strong>the</strong> first few months <strong>in</strong> <strong>Haiti</strong> and o<strong>the</strong>r disasters. Instead of manag<strong>in</strong>g<strong>the</strong> crisis <strong>the</strong>mselves, <strong>in</strong>ternational partners should accompany and build <strong>the</strong> capacityof <strong>the</strong>ir counterparts—admittedly a more demand<strong>in</strong>g and difficult task.The Port-au-Pr<strong>in</strong>ce metropolitan area was severely affected.Eighty percent of <strong>the</strong> <strong>to</strong>wn of Léogâne (17 km southwes<strong>to</strong>f Port-au-Pr<strong>in</strong>ce) was destroyed.Pho<strong>to</strong>: PAHO/WHO, Vic<strong>to</strong>r Arisca<strong>in</strong>141
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Quality control <strong>in</strong> <strong>the</strong> medical sec<strong>to</strong>rMany agencies that regularly provide medical teams and field hospitals are dedicat<strong>in</strong>gconsiderable effort <strong>to</strong> improve <strong>the</strong> quality of <strong>the</strong>ir performance by carry<strong>in</strong>g outsystematic evaluations and tra<strong>in</strong><strong>in</strong>g. Some have gone a step fur<strong>the</strong>r <strong>to</strong> analyze <strong>the</strong> costeffectivenessof <strong>the</strong>ir <strong>in</strong>terventions <strong>in</strong> terms of development and relief. 145 However, notall groups have a high standard of quality assurance.Medical care is one of <strong>the</strong> most regulated service sec<strong>to</strong>rs <strong>in</strong> all countries, even <strong>in</strong> lessdeveloped ones. Accredit<strong>in</strong>g medical doc<strong>to</strong>rs, paramedical technicians, and pharmacistsor licensed facilities is one of <strong>the</strong> key functions of a m<strong>in</strong>istry of health <strong>in</strong> “normal”times. In <strong>the</strong> aftermath of a disaster, any medical team or <strong>in</strong>dividual can claim (accuratelyor not) competence and <strong>the</strong> qualifications <strong>to</strong> amputate limbs or undertakemajor surgery. The medical humanitarian bus<strong>in</strong>ess has grown <strong>to</strong>o much not <strong>to</strong> be betterregulated. There must be a balance between <strong>the</strong> current laissez-faire approach andrigid accreditation. Regulations must be adapted <strong>to</strong> fit <strong>the</strong> magnitude and urgency ofneeds that cannot be met nationally.Some def<strong>in</strong>itions are useful at this stage:• Registration is merely a process of fil<strong>in</strong>g <strong>in</strong>formation <strong>in</strong><strong>to</strong> a register or database. Itdoes not validate <strong>the</strong> competence of <strong>the</strong> entity registered.• Certification <strong>in</strong>volves a technical evaluation of compliance with pre-established requirementsor criteria. An <strong>in</strong>dependent third party normally does this evaluation.In light of <strong>the</strong> potential liability for <strong>the</strong> certify<strong>in</strong>g agency, INSARAG has adopted<strong>the</strong> term “external classification.”• Accreditation is “a formal process by which a recognized body recognizes that ahealth care organization meets applicable, pre-determ<strong>in</strong>ed, and published standards.”In normal, non-crisis situations, “An accreditation decision about a specifichealth care organization is made follow<strong>in</strong>g a periodic on-site evaluation bya team of peer reviewers, typically conducted every two <strong>to</strong> three years. Accreditationis often a voluntary process <strong>in</strong> which organizations choose <strong>to</strong> participate,ra<strong>the</strong>r than one required by law and regulation” (Rooney and van Ostenberg1999).• Licensure is a process by which a government authority grants permission <strong>to</strong> an <strong>in</strong>dividualpractitioner or health care organization <strong>to</strong> operate. In normal situations,organizational licensure is granted follow<strong>in</strong>g an on-site <strong>in</strong>spection <strong>to</strong> determ<strong>in</strong>e ifm<strong>in</strong>imum health and safety standards have been met.At this stage, registration is <strong>the</strong> only process that can be realistically considered <strong>in</strong> <strong>the</strong>medical sec<strong>to</strong>r.145 Accord<strong>in</strong>g <strong>to</strong> one analysis (Gossel<strong>in</strong> et al. 2011), <strong>the</strong> costs saved per disability-adjusted life year (DALY) <strong>in</strong> short surgicalmissions for elective surgery and those <strong>in</strong> post-<strong>earthquake</strong> relief missions <strong>in</strong> <strong>the</strong> same country were unexpectedlyvery similar.142
KEY STRATEGIC LESSONS FOR THE NEXT SUDDEN-ONSET DISASTER - Chapter 9As endorsed by <strong>the</strong> Global <strong>Health</strong> Cluster, sett<strong>in</strong>g up a worldwide registry of providersof such services and develop<strong>in</strong>g predeterm<strong>in</strong>ed and published norms and standards fordeployment of medical teams and hospitals are <strong>the</strong> <strong>in</strong>itial steps <strong>to</strong>ward improved qualitycontrol of <strong>the</strong> health <strong>response</strong>.The m<strong>in</strong>istry of health must be provided with this basic <strong>in</strong>formation about <strong>the</strong> capacityof foreign medical teams and field hospitals prior <strong>to</strong> <strong>the</strong> occurrence of a disaster.Learn<strong>in</strong>g from <strong>the</strong> pastThere were many evaluations of <strong>the</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong>; more thana few <strong>in</strong>terlocu<strong>to</strong>rs said that <strong>the</strong>re were <strong>to</strong>o many. Never<strong>the</strong>less, it is hard <strong>to</strong> note asignificant improvement or change of attitude <strong>in</strong> <strong>the</strong> <strong>response</strong>. One of <strong>the</strong> ma<strong>in</strong> shortcom<strong>in</strong>gsis, perhaps, <strong>the</strong> scope of those evaluations: How efficiently and effectively are<strong>the</strong> objectives and policies pursued? How did we mobilize our resources and coord<strong>in</strong>atewhat we set out <strong>to</strong> accomplish?Whe<strong>the</strong>r <strong>the</strong> objectives pursued were desirable and achievable, or if <strong>the</strong> policies were<strong>in</strong> <strong>the</strong> best long-term <strong>in</strong>terest of <strong>the</strong> beneficiaries were beyond <strong>the</strong> scope of <strong>the</strong> termsof reference of most evaluations.Some of those strategic and policy <strong>to</strong>pics are best left <strong>to</strong> researchers ra<strong>the</strong>r than hiredevalua<strong>to</strong>rs. However, <strong>to</strong> do proper research, scientists would benefit from greater access<strong>to</strong> documents and <strong>in</strong>ternal reports (<strong>in</strong>clud<strong>in</strong>g electronic mail) than is allowed by<strong>the</strong> current level of transparency of ma<strong>in</strong> ac<strong>to</strong>rs.F<strong>in</strong>ally, <strong>to</strong> paraphrase Nigel Fisher, <strong>the</strong> Humanitarian Coord<strong>in</strong>a<strong>to</strong>r <strong>in</strong> <strong>Haiti</strong>, <strong>the</strong> “lessonslearned tend <strong>to</strong> focus on resolv<strong>in</strong>g what did not work so well. But aga<strong>in</strong>, weshould not forget <strong>the</strong> many considerable achievements of <strong>the</strong> humanitarian community.”In <strong>Haiti</strong>, many lives were saved, people were fed and sheltered, and <strong>the</strong>y receivedmuch better care than before. The disaster brought significant positive changes <strong>in</strong>mentality, behavior, and attitude. It is up <strong>to</strong> <strong>the</strong> <strong>Haiti</strong>ans and <strong>the</strong> <strong>in</strong>ternational community<strong>to</strong> ensure that those changes endure.143
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>BibliographyAbaakouk Z. (forthcom<strong>in</strong>g). Mental health <strong>in</strong> <strong>Haiti</strong> <strong>in</strong> <strong>2010</strong>: a public health need, an added value with<strong>in</strong>health care practice and a corners<strong>to</strong>ne for reconstruction. In PAHO/WHO, Mental health and psychosocialsupport <strong>in</strong> emergencies <strong>in</strong> <strong>the</strong> Caribbean. Wash<strong>in</strong>g<strong>to</strong>n, D.C.: PAHO/WHO.Active Learn<strong>in</strong>g Network for Accountability and Performance <strong>in</strong> Humanitarian Action (ALNAP)/ProVention.2009. Respond<strong>in</strong>g <strong>to</strong> urban disasters: learn<strong>in</strong>g from previous relief and recovery operations. Available at:www.alnap.org/pool/files/alnap-provention-lessons-urban.pdf.———. <strong>2010</strong>. <strong>Haiti</strong> <strong>earthquake</strong> <strong>response</strong>: context analysis. Available at: www.alnap.org/pool/files/haiti-context-analysis-f<strong>in</strong>al.pdf.Adams P. <strong>2010</strong>. Ra<strong>in</strong>y season could hamper <strong>Haiti</strong>’s recovery. Lancet 375(9720):1067–9.Afshar, M., M. Raju, D. Ansell, T. P. Bleck. 2011. Narrative review: tetanus—a health threat after naturaldisasters <strong>in</strong> develop<strong>in</strong>g countries. Ann Intern Med 154(5):329–35.Alkire, S., M. E. San<strong>to</strong>s. <strong>2010</strong>. Multidimensional Poverty Index: <strong>2010</strong> Data. Oxford Poverty and HumanDevelopment Initiative. Available at: www.ophi.org.uk/policy/multidimensional-poverty-<strong>in</strong>dex.American Medical Association. <strong>2010</strong>. Medical and public health responders: prepar<strong>in</strong>g for <strong>the</strong> <strong>Haiti</strong>an <strong>earthquake</strong>disaster relief efforts. [Web-based tra<strong>in</strong><strong>in</strong>g program.] Available at: www.ama-assn.org/ama/pub/news/news/haiti-<strong>earthquake</strong>-<strong>response</strong>.page.American Red Cross. 2011. <strong>Haiti</strong> <strong>earthquake</strong> relief, one-year report. Available at: www.redcross.org/wwwfiles/Documents/pdf/<strong>in</strong>ternational/<strong>Haiti</strong>/<strong>Haiti</strong>Earthquake_OneYearReport.pdf.Amnesty International. <strong>2010</strong>. <strong>Haiti</strong>: after <strong>the</strong> <strong>earthquake</strong>: <strong>in</strong>itial mission f<strong>in</strong>d<strong>in</strong>gs, March <strong>2010</strong>. London: AmnestyInternational Publications. Available from: www.amnesty.org/en/library/<strong>in</strong>fo/AMR36/004/<strong>2010</strong>.Anderson, A. J., C. L. Powell. 2011. “The role of humanitarian efforts: lessons from <strong>Haiti</strong>.” Lecture, 45th AnnualUniformed Services Pediatric Sem<strong>in</strong>ar, American Academy of Pediatrics. Wash<strong>in</strong>g<strong>to</strong>n, D.C., 12–15March.Archibold, R.C. 2011. U.S. reduces estimates of homeless <strong>in</strong> <strong>Haiti</strong> quake. New York Times, 31 May.Assessment Capacities Project (ACAPS). <strong>2010</strong>. Rapid <strong>in</strong>itial needs assessment for <strong>Haiti</strong> (RINAH). Conducted23 <strong>January</strong>–6 February <strong>2010</strong>, Port-au-Pr<strong>in</strong>ce. Available at: www.acaps.org/img/documents/r<strong>in</strong>ahreport-f<strong>in</strong>al-r<strong>in</strong>ah-report-feb<strong>2010</strong>.pdf.Association of Schools of Public <strong>Health</strong>. <strong>Haiti</strong>an <strong>earthquake</strong> relief: schools of public health respond. Accessed20 July 2011. www.asph.org/document.cfm?page=1141.Auerbach, P. S., R. L. Norris, A. S. Menon, et al. <strong>2010</strong>. Civil–military collaboration <strong>in</strong> <strong>the</strong> <strong>in</strong>itial medical<strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong>. N Engl J Med 362(10):e32.144
BIBLIOGRAPHYBabcock, C., C. Baer, C. Bayram, et al. <strong>2010</strong>. Chicago medical <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>2010</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong>:translat<strong>in</strong>g academic collaboration <strong>in</strong><strong>to</strong> direct humanitarian <strong>response</strong>. Disaster Med Public <strong>Health</strong> Prep4(2):169–73.Bajkiewicz, C. 2009. Evaluat<strong>in</strong>g short-term missions: How can we improve? J Christ Nurs 26(2):110–4.Bar-On, E. E. Lebel, Y. Kreiss, et al. 2011. Orthopaedic management <strong>in</strong> a mega mass casualty situation:<strong>the</strong> Israel Defense Forces Field Hospital <strong>in</strong> <strong>Haiti</strong> follow<strong>in</strong>g <strong>the</strong> <strong>January</strong> <strong>2010</strong> <strong>earthquake</strong>. Injury, Apr 18.[Epub ahead of pr<strong>in</strong>t].Barrera, G. <strong>2010</strong>. Regreso al país del buque ARC Cartegena de Indias procedente de <strong>Haiti</strong> [Radio Santa Febroadcast, <strong>in</strong>terview with Commander Guillermo Barrera, Colombian National Navy]. Accessed 20May 2011. www.radiosantafe.com/<strong>2010</strong>/02/10/regreso-al-pais-el-buque-arc-cartagena-de-<strong>in</strong>dias-procedente-de-haiti.Basauri, V. <strong>2010</strong>. Rapport de Mission: La Santé mentale et le soutien psycho-social <strong>in</strong> Haïti (PAHO/WHOMission Report, 3–6 February <strong>2010</strong>). Unpublished.Bassett, L. <strong>2010</strong>, Nutrition security <strong>in</strong> <strong>Haiti</strong>: pre- and post-<strong>earthquake</strong> conditions and <strong>the</strong> way forward. WorldBank En Breve Series No. 157 ( June <strong>2010</strong>). Available at: www.worldbank.org/enbreve.Bennett, J., W. Bertrand, C. Hark<strong>in</strong>, et al. 2006. Coord<strong>in</strong>ation of <strong>in</strong>ternational humanitarian assistance <strong>in</strong>tsunami-affected countries. London: Tsunami Evaluation Coalition.B<strong>in</strong>der, A., F. Grünewald. <strong>2010</strong>. IASC Cluster approach evaluation, 2nd phase. Country study: <strong>Haiti</strong>. GroupeURD (April <strong>2010</strong>). Available at: www.gppi.net/fileadm<strong>in</strong>/gppi/GPPi-URD_Cluster_II_Evaluation_HAITI_e.pdf.Born, C.T., T.R. Cullison, J.A. Dean, et al. 2011. Partnered disaster preparedness: lessons learned from<strong>in</strong>ternational events. J Am Acad Orthop Surg 19 (suppl 1): S44–S48.Burns, A. S., C. O’Connell, M.D. Landry. <strong>2010</strong>. Sp<strong>in</strong>al cord <strong>in</strong>jury <strong>in</strong> post-<strong>earthquake</strong> <strong>Haiti</strong>: lessonslearned and future needs. PM&R Vol. 2, 695–7.Calvot, T., A. Shivji. (Forthcom<strong>in</strong>g). <strong>Haiti</strong>, du Traumatisme au Relèvement, Quelles Perspectives? In Conoir,Y. (ed.). Laval, Canada: Presses de l’Université Laval.CdeBaca, L. <strong>2010</strong>. Best practices: human traffick<strong>in</strong>g <strong>in</strong> disaster zones. Keynote remarks <strong>to</strong> <strong>the</strong> Harvard KennedySchool’s Ash Center for Democratic Governance and Innovation, Wash<strong>in</strong>g<strong>to</strong>n, D.C., May 24,<strong>2010</strong>. Available at: www.reliefweb.<strong>in</strong>t/node/355692.Centre for Research on <strong>the</strong> Epidemiology of Disasters (CRED). Emergency Events Database (EM-DAT).Available at: www.emdat.be.Chu, K. M., M. Trelles, N. P. Ford. 2011. Quality of care <strong>in</strong> humanitarian surgery. World J Surg 35(6):1169–72.Cochran, J. <strong>2010</strong>. Statistics without Borders assists with <strong>Haiti</strong>an data collection project. Statistics WithoutBorders/Amstat News, <strong>2010</strong>. Accessed 1 <strong>January</strong> 2011. www.magaz<strong>in</strong>e.amstat.org/blog/<strong>2010</strong>/05/13/swb5_10.Cosgrave, J. 2007. Syn<strong>the</strong>sis report: expanded summary. Jo<strong>in</strong>t evaluation of <strong>the</strong> <strong>in</strong>ternational <strong>response</strong> <strong>to</strong> <strong>the</strong>Indian Ocean tsunami. London: Tsunami Evaluation Coalition. Available at: www.alnap.org/pool/files/Syn_Report_Sum.pdf.145
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>DARA. <strong>2010</strong>. Climate vulnerability moni<strong>to</strong>r. Report. Available from http://dara<strong>in</strong>t.org/climate-vulnerability-moni<strong>to</strong>r/climate-vulnerability-moni<strong>to</strong>r-<strong>2010</strong>.de Ville de Goyet, C., L. Mor<strong>in</strong>ière. 2006. The role of needs assessment <strong>in</strong> <strong>the</strong> tsunami <strong>response</strong>. Tsunami EvaluationCoalition. Available at: www.alnap.org/<strong>in</strong>itiatives/tec/<strong>the</strong>matic/needs.aspx.Doocy C., C. Rob<strong>in</strong>son, C. Moodie, G. Burnham. 2009. Tsunami-related <strong>in</strong>jury <strong>in</strong> Aceh Prov<strong>in</strong>ce, Indonesia.Global Public <strong>Health</strong> 4(2):205–14.Dowell, S. F., J.W. Tappero, T.R. Frieden. 2011. Public health <strong>in</strong> <strong>Haiti</strong>: challenges and progress. N Engl JMed 364(4):300–1.Eckes-Roper, J. <strong>2010</strong>. Operation <strong>Haiti</strong> relief: South Florida health/medical <strong>response</strong>. Philadelphia Public<strong>Health</strong> Forum: Current Issues <strong>in</strong> Public <strong>Health</strong> and Preparedness.Etienne M., C. Powell, B. Faux. <strong>2010</strong>. Disaster relief <strong>in</strong> <strong>Haiti</strong>: a perspective from <strong>the</strong> neurologists on <strong>the</strong>USNS Comfort. Lancet Neurology 9(5): 461–3.Farfel A., A. Assa, I. Amir, et al. 2011. <strong>Haiti</strong> <strong>earthquake</strong> <strong>2010</strong>: a field hospital pediatric perspective. Eur JPediatr 170(4):519–25.Farmer, P. 2011. <strong>Haiti</strong> after <strong>the</strong> <strong>earthquake</strong>. New York: Public Affairs.Felten-Biermann, C. 2006. Gender and natural disaster: sexualized violence and <strong>the</strong> tsunami. Development49(3):82–6.Ferris, D. <strong>2010</strong>. Pharmacist’s assistance after <strong>Haiti</strong> <strong>earthquake</strong>. Am J <strong>Health</strong> Syst Pharm 67:1138–41.Fisher, N. <strong>2010</strong>. Notes on prelim<strong>in</strong>ary lessons learnt from <strong>Haiti</strong>. Address <strong>to</strong> IASC Pr<strong>in</strong>cipals Meet<strong>in</strong>g, 6 May<strong>2010</strong>, New York. Unpublished.Florida Department of <strong>Health</strong>. <strong>2010</strong>. Recommendations/guidel<strong>in</strong>es for <strong>in</strong>itial <strong>in</strong>fection control, medical screen<strong>in</strong>gsand vacc<strong>in</strong>ations of <strong>Haiti</strong>an <strong>earthquake</strong> evacuees. February 3, <strong>2010</strong>.Florida Hospital Association. National Disaster Medical System Overview and Contact Information, Feb. 5,<strong>2010</strong>. www.fha.org/Article.html?ArtID=8774.Food and Agriculture Organization and World Food Programme. <strong>2010</strong>. Evaluation de la Récolte et de lasécurité alimentaire en Haïti. [Special Mission Report, 21 September <strong>2010</strong>]. Available at: www.fao.org/docrep/012/ak353f/ak353f00.htm.France. Embassy of France <strong>in</strong> <strong>the</strong> United States. <strong>2010</strong>. Earthquake <strong>in</strong> <strong>Haiti</strong>—update on French effort(02/04/10). Accessed 20 May 2011. http://ambafrance-us.org/spip.php?article1504.Galeckas, K. 2011. Derma<strong>to</strong>logy aboard <strong>the</strong> USNS Comfort: disaster relief operations <strong>in</strong> <strong>Haiti</strong> after <strong>the</strong><strong>2010</strong> <strong>earthquake</strong>. Derma<strong>to</strong>logic cl<strong>in</strong>ics 29(1):15–9.Gerd<strong>in</strong> M. and J. Von Schreeb. 2011. Presentation at <strong>the</strong> 17th World Congress on Disaster and Emergencymedic<strong>in</strong>e <strong>in</strong> Beij<strong>in</strong>g, May 2011.G<strong>in</strong>zburg E., W.W. O’Neill, P. J. Goldschmidt-Clermont, et al. <strong>2010</strong>. Rapid medical relief—Project Medishareand <strong>the</strong> <strong>Haiti</strong>an <strong>earthquake</strong>. N Engl J Med 362(10):e31.Goodman A. <strong>2010</strong>. M<strong>in</strong>istry of <strong>to</strong>uch—reflections on disaster work after <strong>the</strong> <strong>Haiti</strong>an <strong>earthquake</strong>. N EnglJ Med 362(11):e37.146
BIBLIOGRAPHYGossel<strong>in</strong> R. A., G. Gialamas, D. M. Atk<strong>in</strong>. 2011. Compar<strong>in</strong>g <strong>the</strong> cost-effectiveness of short orthopedic missions<strong>in</strong> elective and relief situations <strong>in</strong> develop<strong>in</strong>g countries. World J Surg 35(5):951–5.Griekspoor, A. <strong>2010</strong>. Key issues from <strong>the</strong> <strong>Haiti</strong> PDNA. Geneva: World <strong>Health</strong> Organization.Growth of aid and <strong>the</strong> decl<strong>in</strong>e of humanitarianism. [Edi<strong>to</strong>rial]. <strong>2010</strong> Lancet 375(9711):253.Grünewald, F. <strong>2010</strong>. The health <strong>response</strong> <strong>in</strong> <strong>Haiti</strong> after <strong>the</strong> <strong>earthquake</strong>: some food for thought. Groupe UrgenceRéhabilitation Développement (URD): 9 June. Available at: www.urd.org/IMG/pdf/The_health_<strong>response</strong>_<strong>in</strong>_<strong>Haiti</strong>_after_<strong>the</strong>_<strong>earthquake</strong>_Some_food_for_thought.pdf.Grünewald, F., A. B<strong>in</strong>der, Y. Georges. <strong>2010</strong>. Inter-agency real-time evaluation <strong>in</strong> <strong>Haiti</strong>: 3 months after <strong>the</strong><strong>earthquake</strong>. Groupe Urgence Réhabilitation Développement; Global Public Policy Institute.Grünewald, F., B. Renaud<strong>in</strong>. <strong>2010</strong>. Etude en temps réel de la gestion de la crise en Haïti après le séisme du 12janvier <strong>2010</strong>: Mission du 9 au 23 février <strong>2010</strong>. [Real-time evaluation <strong>in</strong> <strong>Haiti</strong> follow<strong>in</strong>g <strong>the</strong> 12 <strong>January</strong><strong>2010</strong> <strong>earthquake</strong>. Report for mission conducted 9 <strong>to</strong> 23 February for <strong>the</strong> Strategic Affairs Delegation of<strong>the</strong> M<strong>in</strong>istry of Defence, France; 4 April <strong>2010</strong>.]<strong>Haiti</strong>. M<strong>in</strong>istère de la Santé Publique et de la Population (MSPP) [M<strong>in</strong>istry of <strong>Health</strong>]. 2006. Enquêtemortalité, morbidité et utilisation des services EMMUS IV 2005–2006 [Survey of mortality, morbidity,and utilization of services]. Port-au-Pr<strong>in</strong>ce. Available at : www.paho.org/english/d/csu/haiprelreportemmus-iv.pdf.———. 2007. Bilan vision et gouvernance. Forum nationale pour le realignement de la reforme du secteur sante(FRRSS) [Governance report: forum for <strong>the</strong> realignment of health sec<strong>to</strong>r reform]. Port-au-Pr<strong>in</strong>ce.———. <strong>2010</strong>a. Analyse des résultats du recensement des ressources huma<strong>in</strong>es post-séisme [Census of humanresources follow<strong>in</strong>g <strong>the</strong> <strong>earthquake</strong>]. 16 March <strong>2010</strong>. Port-au-Pr<strong>in</strong>ce.———. <strong>2010</strong>b. Goudougoudou - Timoun boum Enquête sur la santé dans les sites d’hébergement-Haïti [<strong>Health</strong>survey <strong>in</strong> temporary settlements <strong>in</strong> <strong>Haiti</strong>]. Port-au-Pr<strong>in</strong>ce.———. <strong>2010</strong>c. Plan <strong>in</strong>térimaire du secteur santé: Mars 201–Septembre 2011 [Interim plan of <strong>the</strong> healthsec<strong>to</strong>r: March <strong>2010</strong>–September 2011]. Port-au-Pr<strong>in</strong>ce.———. <strong>2010</strong>d. Pro<strong>to</strong>cole national de prise en charge de la malnutrition aiguë globale en Haïti–Version révisée,Mai <strong>2010</strong> [National pro<strong>to</strong>col for management of global acute malnutrition <strong>in</strong> <strong>Haiti</strong>–Revised, May<strong>2010</strong>]. Port-au-Pr<strong>in</strong>ce.———. <strong>2010</strong>e. Provision des services dans les camps / zones de regroupement de la population [Service delivery<strong>in</strong> camps, temporary population settlements]. Port-au-Pr<strong>in</strong>ce.<strong>Haiti</strong>, Office of <strong>the</strong> Prime M<strong>in</strong>ister. <strong>2010</strong>. <strong>Haiti</strong> <strong>earthquake</strong> PDNA: Assessment of damages losses, general andsec<strong>to</strong>ral needs. Annex <strong>to</strong> <strong>the</strong> Action Plan for National Recovery and Development of <strong>Haiti</strong>. Port-au-Pr<strong>in</strong>ce.Handicap International. <strong>2010</strong>. Jo<strong>in</strong>t study <strong>to</strong> analyze outcomes of surgical and rehabilitation <strong>in</strong>tervention<strong>in</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>Haiti</strong> <strong>earthquake</strong> <strong>in</strong> <strong>January</strong> <strong>2010</strong> (2 pages). Port-au-Pr<strong>in</strong>ce.Henry J. Kaiser Family Foundation, U.S. Global <strong>Health</strong> Policy. <strong>2010</strong>. <strong>Health</strong> <strong>in</strong> <strong>Haiti</strong> and <strong>the</strong> U.S. Government<strong>in</strong>volvement. Fact Sheet February <strong>2010</strong>. Available at: www.kff.org/globalhealth/upload/8053.pdf.Henrys D. Réflexions sur une politique de santé mentale en Haïti. Revue haïtienne de santé mentale. Vol 2;217–219.147
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Holmes, J. 2007. Humanitarian action: a Western dom<strong>in</strong>ated enterprise <strong>in</strong> need of change. Forced MigrationReview 29: 4–5.Huerta-Alardín, A.L, J. Varon, and P. E. Marik. 2005. Review: Bench-<strong>to</strong>-bedside review: Rhabdomyolysis– an overview for cl<strong>in</strong>icians. Critical Care 9(2):158–69.Hussey S.M., P. J. Dukette, S. H. Dunn, et al. 2011. The <strong>2010</strong> <strong>Haiti</strong> <strong>earthquake</strong>: a pathology perspectiveaboard <strong>the</strong> USNS Comfort. Arch Pathol Lab Med 135(4):417-21.Information Management & M<strong>in</strong>e Action Programs (iMMAP). <strong>2010</strong>. Earthquake <strong>in</strong> <strong>Haiti</strong>: estimated populationexposure [Map]. Available from www.immap.org/<strong>in</strong>dex.php?do=map_view&id=56&cat=12.InterAction. <strong>2010</strong>. “InterAction members respond <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong>.” Accessed 24 December<strong>2010</strong>. www.<strong>in</strong>teraction.org/pr<strong>in</strong>t/3063.Inter-Agency Stand<strong>in</strong>g Committee (IASC), Global <strong>Health</strong> Cluster. 2009. Global health cluster suggested set of core<strong>in</strong>dica<strong>to</strong>rs and benchmarks by category. Available at www.iawg.net/resources/core_<strong>in</strong>dica<strong>to</strong>rs_31jul09.pdf.Inter-Agency Stand<strong>in</strong>g Committee (IASC). <strong>2010</strong>a. Cluster approach evaluation 2nd phase: Executive Summary[6 April <strong>2010</strong>].Inter-Agency Stand<strong>in</strong>g Commmittee (IASC)/Global <strong>Health</strong> Cluster. <strong>2010</strong>b. Position Paper: Remov<strong>in</strong>g userfees for primary health care services dur<strong>in</strong>g humanitarian crises (24 March <strong>2010</strong>). Prehosp Disaster Med25(4): 374–6.Inter-Agency Stand<strong>in</strong>g Committee. 2011. Operational guidance for Cluster lead agencies on work<strong>in</strong>g withnational authorities (endorsed 1 July 2011).Interim <strong>Haiti</strong> Recovery Commission. 2011. <strong>Haiti</strong> one year later: <strong>the</strong> progress <strong>to</strong> date and <strong>the</strong> path forward:a report from <strong>the</strong> Interim <strong>Haiti</strong> Recovery Commission, <strong>January</strong> 12, 2011. Accessed 20 July 2011. http://en.cirh.ht/files/pdf/ihrc_oneyear_en_20110112.pdf.International Federation of Red Cross and Red Crescent Societies. 2004. World disaster report. Geneva:IFRC.———. 2005. Tsunami two-year progress report. Accessed 20 July 2011. www.ifrc.org/Docs/Appeals/04/2804srilankapr.pdf.International Organization for Migration (IOM). <strong>2010</strong>. Significant drop <strong>in</strong> numbers of <strong>in</strong>ternally displaced<strong>in</strong> camps <strong>in</strong> <strong>Haiti</strong>. Press brief<strong>in</strong>g (10 December <strong>2010</strong>). Accessed at: www.iom.<strong>in</strong>t/jahia/Jahia/media/press-brief<strong>in</strong>g-notes/pbnAM/cache/offonce?entryId=28848.International Rescue Committee. 2011. The <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong>: <strong>the</strong> IRC responds. Available from: www.rescue.org/sites/default/files/...file/IRC_Report_<strong>Haiti</strong>Anniversary.pdf.Ireland C. <strong>2010</strong>. Medical workers ga<strong>in</strong> momentum. Harvard Gazette, 19 <strong>January</strong>.Israel Government. <strong>2010</strong>. Triage <strong>in</strong> mass causality events—tak<strong>in</strong>g s<strong>to</strong>ck of <strong>the</strong> <strong>Haiti</strong>an experience. Unpublishedpaper, 17 pages.Ivers, L.C., K. Cullen. <strong>2010</strong>. Coord<strong>in</strong>at<strong>in</strong>g and prioritiz<strong>in</strong>g aid <strong>in</strong> <strong>Haiti</strong>. N Engl J Med 362(7):e21.Jobe, K. 2011. Disaster relief <strong>in</strong> post-<strong>earthquake</strong> <strong>Haiti</strong>: un<strong>in</strong>tended consequences of humanitarian volunteerism.Travel Med Infect Dis 9(1):1–5.148
BIBLIOGRAPHYKaufmann, D., A. Kraay, M. Mastruzzi. <strong>2010</strong>. The worldwide governance <strong>in</strong>dica<strong>to</strong>rs: methodology and analyticalissues. World Bank Policy Research Work<strong>in</strong>g Paper No. 5430. Available at: http://ssrn.com/abstract=1682130.Keim, M.E., E. Noji. 2011. Emergent use of social media: a new age of opportunity for disaster resilience.Am J Disaster Med 6(1):47–54.Knowl<strong>to</strong>n, L.M., J. E. Gosney Jr, S. Chackungal, et al. 2011. Report of <strong>the</strong> 2011 Humanitarian ActionSummit Surgical Work<strong>in</strong>g Group on Amputations Follow<strong>in</strong>g Disasters or Conflict. Consensus Statements Regard<strong>in</strong>g<strong>the</strong> Multidiscipl<strong>in</strong>ary Care of Limb Amputation Patients <strong>in</strong> Disasters or Humanitarian Emergencies[forthcom<strong>in</strong>g].Koenig, S., L.C. Ivers, S. Pace, et al. <strong>2010</strong>. Successes and challenges of HIV treatment programs <strong>in</strong> <strong>Haiti</strong>:aftermath of <strong>the</strong> <strong>earthquake</strong>. HIV Ther 4(2):145–60.Kolbe A.R., R.A.Hutson, H. Shannon, et al. <strong>2010</strong>. Mortality, crime and access <strong>to</strong> basic needs before andafter <strong>the</strong> <strong>Haiti</strong> <strong>earthquake</strong>: a random survey of Port-au-Pr<strong>in</strong>ce households. Journal of Medic<strong>in</strong>e, Conflictand Survival 26(4):281–97.Kolbe, A. 2009. Household survey of <strong>in</strong>security <strong>in</strong> Port-au-Pr<strong>in</strong>ce: prelim<strong>in</strong>ary f<strong>in</strong>d<strong>in</strong>gs. Small arms survey. AnnArbor: University of Michigan.Kolbe, A., R. Muggah. <strong>2010</strong>. Assess<strong>in</strong>g needs after <strong>the</strong> quake: prelim<strong>in</strong>ary f<strong>in</strong>d<strong>in</strong>gs from a randomized survey ofPort-au-Pr<strong>in</strong>ce residents. Geneva: UNDP and Ottawa: Development Research Centre.Kolbe, A. R., R.A. Hutson. 2006. Human rights abuse and o<strong>the</strong>r crim<strong>in</strong>al violations <strong>in</strong> Port-au-Pr<strong>in</strong>ce.Lancet 368(9538):864–73.Koontz, H. <strong>2010</strong>. <strong>Haiti</strong> quake risk may still be high. United States Geological Survey Newsroom. Accessed12 September 2011. Available at: www.usgs.gov/newsroom/article.asp?ID=2627.Kopp, J.B., L. K. Ball, A. Cohen, et al., 2007. Kidney patient care <strong>in</strong> disasters: lessons from <strong>the</strong> hurricanesand <strong>earthquake</strong> of 2005. Cl<strong>in</strong>ical Journal Am Soc Nephrol 2(4):814–24.Landry, M.D., C.S. S<strong>in</strong>gh, L. Carnie. <strong>2010</strong>a. Sp<strong>in</strong>al cord <strong>in</strong>jury rehabilitation <strong>in</strong> post-<strong>earthquake</strong> <strong>Haiti</strong>: <strong>the</strong>critical role for non-governmental organizations. [Edi<strong>to</strong>rial] Physio<strong>the</strong>rapy 96 (4):267–8.Landry, M.D., M. McGlynn, E. Ng, et al. <strong>2010</strong>b. Humanitarian <strong>response</strong> follow<strong>in</strong>g <strong>the</strong> <strong>earthquake</strong> <strong>in</strong><strong>Haiti</strong>: reflections on unprecedented need for rehabilitation. World <strong>Health</strong> Popul 12(1):18–22.Lebel E., N. Blumberg, A. Gill, et al. 2011. External fixa<strong>to</strong>r frames as <strong>in</strong>terim damage control for limb <strong>in</strong>juries:experience <strong>in</strong> <strong>the</strong> <strong>2010</strong> <strong>Haiti</strong> <strong>earthquake</strong>. J Trauma. Apr 15 [Epub ahead of pr<strong>in</strong>t].Lecomte Y. <strong>2010</strong>. La santé mentale en Haïti : le nouvel Eldorado? Revue haïtienne de santé mentale Vol 2.pp 9–12.Mac<strong>in</strong>tyre, A. G., J. A. Barbera, B. P. Pet<strong>in</strong>aux. 2011. Survival <strong>in</strong>terval <strong>in</strong> <strong>earthquake</strong> entrapments: researchf<strong>in</strong>d<strong>in</strong>gs re<strong>in</strong>forced dur<strong>in</strong>g <strong>the</strong> <strong>2010</strong> <strong>Haiti</strong> <strong>earthquake</strong> <strong>response</strong>. Disaster Med Public <strong>Health</strong> Prep5(1):13–22.MacLeod, L. <strong>2010</strong>. New media vital <strong>in</strong> break<strong>in</strong>g <strong>Haiti</strong> <strong>earthquake</strong> s<strong>to</strong>ry. BBC World Service.www.bbc.co.uk/worldservice/worldagenda/<strong>2010</strong>/01/100122_worldagenda_haiti_moni<strong>to</strong>r<strong>in</strong>g.shtml.149
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Magloire, R., K. Mung, S. Harris, et al. <strong>2010</strong>. Launch<strong>in</strong>g a national surveillance system after an <strong>earthquake</strong>—<strong>Haiti</strong>.MMWR 59:933–8.Mahoney J., V. Chandra, H. Gambheera, et al. 2006. Respond<strong>in</strong>g <strong>to</strong> <strong>the</strong> mental health and psychologicalsupport needs of <strong>the</strong> people of Sri Lanka <strong>in</strong> disasters. Int Rev Psychiatry. 18(6):593–7.Management Sciences for <strong>Health</strong> (MSH). <strong>2010</strong>. F<strong>in</strong>al report: L’accès aux services de santé primaires dans 206camps de déplacés de la zone métropolita<strong>in</strong>e de Port-au-Pr<strong>in</strong>ce, Haïti. Port-au-Pr<strong>in</strong>ce.Médec<strong>in</strong>s Sans Frontières (MSF). 2011. <strong>Haiti</strong> one year after: a review of Médec<strong>in</strong>s Sans Frontières’ humanitarianaid operations. www.msf.org.au/uploads/media/Medec<strong>in</strong>s_Sans_Frontieres_<strong>Haiti</strong>-one-year-report.pdf.Mer<strong>in</strong> O., N. Ash, G. Levy, et al. <strong>2010</strong>. The Israeli field hospital <strong>in</strong> <strong>Haiti</strong>—ethical dilemmas <strong>in</strong> early disaster<strong>response</strong>. N Engl J Med 362(11):e38.Merl<strong>in</strong>. 2011. Is <strong>Haiti</strong>’s health system any better? A report call<strong>in</strong>g for a more coord<strong>in</strong>ated, collaborative approach<strong>to</strong> disaster <strong>response</strong>. www.merl<strong>in</strong>usa.org/wp-content/uploads/2011/01/Merl<strong>in</strong>USA_Is-<strong>Haiti</strong>-health-system-any-better1.pdf.Misk<strong>in</strong> I.N., R. Nir-Paz, C. Block, et al. <strong>2010</strong>. Antimicrobial <strong>the</strong>rapy for wound <strong>in</strong>fections after catastrophic<strong>earthquake</strong>s. N Engl J Med 363(26):2571–3.Mompelat, J.M. <strong>2010</strong>. Mission d’expertise post-sismique du BRGM en <strong>Haiti</strong>. Bureau de Recherches Géologiqueset M<strong>in</strong>ières (BRGM). [Mission report <strong>to</strong> <strong>Haiti</strong>, 4 March <strong>2010</strong>]. (France) Available at: www.planseisme.fr/IMG/pdf/haiti_brgm.pdf.Muggah, R. <strong>2010</strong>. The effects of stabilisation on humanitarian action <strong>in</strong> <strong>Haiti</strong>. Disasters 34(S3):S444–63.National Human Rights Defense Network (RNDDH). <strong>2010</strong>. Second report on <strong>the</strong> overall situation<strong>in</strong> <strong>the</strong> country after <strong>the</strong> <strong>earthquake</strong> of <strong>January</strong> 12, <strong>2010</strong>–March 2, <strong>2010</strong>. Port au Pr<strong>in</strong>ce. Available at:www.rnddh.org/IMG/pdf/RNDDH_Earthquake_<strong>January</strong>_12_<strong>2010</strong>.pdf.Nemeroff, C.B., P.J. Goldschmidt-Clermont. 2011. In <strong>the</strong> aftermath of tragedy: medical and psychiatricconsequences. Academic Psychiatry 35(1):4–7.O’Connell. C. A. Shivji, T. Calvot. <strong>2010</strong>. Handicap International. Prelim<strong>in</strong>ary f<strong>in</strong>d<strong>in</strong>gs about persons with<strong>in</strong>juries. Port-au-Pr<strong>in</strong>ce, 15–26 <strong>January</strong>. http://reliefweb.<strong>in</strong>t/node/343807.Organization of American States (OAS). Inter-American Commission on Human Rights. nd. The right ofwomen <strong>in</strong> <strong>Haiti</strong> <strong>to</strong> be free from violence and discrim<strong>in</strong>ation. Available from: www.cidh.org/countryrep/<strong>Haiti</strong>mujer2009eng/<strong>Haiti</strong>Women09.Intro.Chap.IandII.htm#II.Pan American <strong>Health</strong> Organization (PAHO/WHO). 2003. Guidel<strong>in</strong>es for <strong>the</strong> use of foreign field hospitals <strong>in</strong><strong>the</strong> aftermath of sudden-impact disasters.Wash<strong>in</strong>g<strong>to</strong>n, D.C: PAHO/ WHO.———. 2004. Management of dead bodies <strong>in</strong> disaster situations. (PAHO/WHO Disaster Manuals andGuidel<strong>in</strong>es Series, No. 5). Available at: www.paho.org/english/dd/ped/deadbodiesbook.pdf.———. 2007. <strong>Health</strong> <strong>in</strong> <strong>the</strong> Americas, 2007. Vol. II. Wash<strong>in</strong>g<strong>to</strong>n, D.C.:PAHO/WHO.———. 2009. <strong>Health</strong> situation <strong>in</strong> <strong>the</strong> Americas, basic <strong>in</strong>dica<strong>to</strong>rs, 2009. Wash<strong>in</strong>g<strong>to</strong>n, D.C.: PAHO/WHO.150
BIBLIOGRAPHY———. <strong>2010</strong>a. Edi<strong>to</strong>rial: Field hospitals and medical teams <strong>in</strong> <strong>the</strong> aftermath of <strong>earthquake</strong>s. Disasters: Preparednessand Mitigation <strong>in</strong> <strong>the</strong> Americas (No. 114). Accessed 25 <strong>January</strong> <strong>2010</strong>. http://new.paho.org/disasters/newsletter/<strong>in</strong>dex.php?option=com_content&view=article&id=429&Itemid=266&lang=en.———. <strong>2010</strong>b. Edi<strong>to</strong>rial: What can we really learn from <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong>? Disasters: Preparednessand Mitigation <strong>in</strong> <strong>the</strong> Americas (No. 113). Accessed 25 December <strong>2010</strong>. http://new.paho.org/...e&id=99%3Awhat-can-we-really-learn-from-<strong>the</strong>-<strong>earthquake</strong>-<strong>in</strong>-haiti&catid=79%3Aissue-113-may-<strong>2010</strong>-edi<strong>to</strong>rial&Itemid=123&lang=en.———. <strong>2010</strong>c. <strong>Haiti</strong> <strong>Health</strong> Cluster Bullet<strong>in</strong>s—Earthquake, <strong>January</strong>–March <strong>2010</strong>, Nos. 1–25. Available at:http://new.paho.org/disasters/<strong>in</strong>dex.php?option=com_content&task=view&id=1108&Itemid=1.———. <strong>2010</strong>d. Special report: update on <strong>the</strong> health <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> (16 February <strong>2010</strong>).Wash<strong>in</strong>g<strong>to</strong>n, D.C.: PAHO/WHO.———. 2011a. Earthquake <strong>in</strong> <strong>Haiti</strong>—One Year Later: PAHO/WHO Report on <strong>the</strong> <strong>Health</strong> Situation. Wash<strong>in</strong>g<strong>to</strong>n,D.C.: PAHO/WHO. Available from: http://new.paho.org/disasters/<strong>in</strong>dex.php?option=com_content&task=view&id=1475&Itemid=1.———. 2011b. A Year of <strong>Health</strong> Challenges for <strong>Haiti</strong>. Office of <strong>the</strong> Direc<strong>to</strong>r. Newsletter <strong>January</strong> 2011.Available at http://new.paho.org/hq/<strong>in</strong>dex.php?option=com_content&task=view&id=4609&Itemid=1926&lang=en.Peranteau W.H., J.M. Havens, S. Harr<strong>in</strong>g<strong>to</strong>n, et al. <strong>2010</strong>. Re-establish<strong>in</strong>g surgical care at Port-au-Pr<strong>in</strong>ceGeneral Hospital, <strong>Haiti</strong>. J Am Coll Surg 211(1):126–30.Perry, A. <strong>2010</strong>. Silicon savanna: mobile phones transform Africa. Time Magaz<strong>in</strong>e, 30 June 2011 www.time.com/time/magaz<strong>in</strong>e/article/0,9171,2080702,00.html#ixzz1XrbBPKuI.Ratha, Dilip. <strong>2010</strong>. Mobiliz<strong>in</strong>g <strong>the</strong> diaspora for reconstruction of <strong>Haiti</strong> via diaspora bonds. World Bank Blog.Available at: http://blogs.worldbank.org/peoplemove/mobiliz<strong>in</strong>g-<strong>the</strong>-diaspora-for-reconstruction-ofhaiti-via-diaspora-bonds.Ravenscroft K. <strong>2010</strong>. Images <strong>in</strong> psychiatry: <strong>Haiti</strong> <strong>earthquake</strong> psychiatric relief. Am J Psychiatry 167(9):1038.Ray, J. M., R.W. L<strong>in</strong>dsay, A.R. Kumar. <strong>2010</strong>. Treatment of <strong>earthquake</strong>-related craniofacial <strong>in</strong>juries aboard<strong>the</strong> USNS Comfort dur<strong>in</strong>g Operation Unified Response. Plast Reconstr Surg 126(6): 2102–8.Revista Española de Defensa. <strong>2010</strong>. Misión en Haití. (February) 23(26).Rice M.J., A. Gwertzman, T. F<strong>in</strong>ley, T.E. Morey. <strong>2010</strong>. Anes<strong>the</strong>tic practice <strong>in</strong> <strong>Haiti</strong> after <strong>the</strong> <strong>2010</strong> <strong>earthquake</strong>.Anes<strong>the</strong>sia and Analgesia 111(6):1445–9.Robertson‐Steel, I. 2006. Evolution of triage systems. Emergency Medic<strong>in</strong>e Journal 23(2): 154–5.Rooney A.L., P. R. van Ostenberg. 1999. Licensure, accreditation, and certification: approaches <strong>to</strong> health servicesquality. Be<strong>the</strong>sda, MD:USAID Quality Assurance Project.Schuftan C., A. Hoogendoorn, P. Capdegelle. 2007. Analyse de la situation humanitaire: evaluation ex-anteHaïti: Rapport f<strong>in</strong>al d’évaluation. [Report prepared for DG ECHO by Particip GmbH; Channel Research,June 2007].Schwartz, T.T., Y-F. Pierre, E. Calpas. 2011. Build<strong>in</strong>g assessments and rubble removal <strong>in</strong> quake-affected neighborhoods<strong>in</strong> <strong>Haiti</strong>: BARR Survey F<strong>in</strong>al Report. Wash<strong>in</strong>g<strong>to</strong>n, D.C.: LTL Strategies and USAID.151
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Sever, M. S., J. Kellum, E. Hoste, R. Vanholder. 2011. Application of <strong>the</strong> RIFLE criteria <strong>in</strong> patients withcrush-related acute kidney <strong>in</strong>jury after mass disasters. Nephrol Dial Transplant 26(2):515–24.Sever, M. S., N. Lameire, R. Vanholder. 2009. Renal disaster relief: from <strong>the</strong>ory <strong>to</strong> practice. Nephrol DialTransplant 24(6):1730–5.Sever, M.S., R. Vanholder, N. Lameire. 2006. Management of crush-related <strong>in</strong>juries after disasters. N EnglJ Med 354(10):1052–63.Sheng, Z.Y. 1987. Medical support <strong>in</strong> <strong>the</strong> Tangshan <strong>earthquake</strong>: a review of <strong>the</strong> management of mass casualtiesand certa<strong>in</strong> major <strong>in</strong>juries. J Trauma 27(10):1130–5.Siroco. Website. Accessed 10 September 2011. http://tcd.siroco.free.fr/actualites<strong>2010</strong>haiti.htm.Sphere Project. 2011. Humanitarian Charter and m<strong>in</strong>imum standards <strong>in</strong> humanitarian <strong>response</strong>. Available at:www.sphereproject.org/content/view/40/84/lang,English.Sribanditmongkol, P., P. Pongpanitanont, N. Porntrakulseree, et al. 2005. Forensic aspect of disaster casualtymanagement: tsunami victim identification <strong>in</strong> Thailand. Presentation at WHO conference. Available at:www.who.<strong>in</strong>t/hac/events/tsunamiconf/presentations/2_16_forensic_pongruk_doc.pdf.Stephenson , F. 2011. Simple wound care facilitates full heal<strong>in</strong>g <strong>in</strong> post-<strong>earthquake</strong> <strong>Haiti</strong>. Journal of WoundCare 20(1): 5–6.Swiss Agency for Development and Cooperation (SDC). 2011. Evaluation 2011/1: SDC humanitarian aid:emergency relief. Available at: www.deza.adm<strong>in</strong>.ch/ressources/resource_en_202917.pdf.Telford, J., J. Cosgrave, R. Hough<strong>to</strong>n. 2006. Jo<strong>in</strong>t evaluation of <strong>the</strong> <strong>in</strong>ternational <strong>response</strong> <strong>to</strong> <strong>the</strong> Indian OceanTsunami. Syn<strong>the</strong>sis report. London: Tsunami Evaluation Coalition.“Timel<strong>in</strong>e of relief efforts after <strong>the</strong> <strong>2010</strong> <strong>Haiti</strong> <strong>earthquake</strong>.” Accessed 20 May 2011. http://cheapnewyorkhotels.tv/timel<strong>in</strong>e-of-relief-efforts-after-<strong>the</strong>-<strong>2010</strong>-haiti-<strong>earthquake</strong>-sodium-tripolyphosphate-food-grade.Transparency International. 2011. Corruption Perceptions Index <strong>2010</strong>. Table 1. Accessed 1 August 2011.www.transparency.org/policy_research/surveys_<strong>in</strong>dices/cpi/<strong>2010</strong>/results.Tulane University, University of <strong>Haiti</strong>. 2011. <strong>Haiti</strong> humanitarian aid evaluation: structured analysis summaryreport. Tulane University, Disaster Resilience Leadership Academy.United Nations. 2005. Report and summary of ma<strong>in</strong> conclusions of <strong>the</strong> United Nations Regional Workshopon Lessons Learned and Best Practice <strong>in</strong> <strong>the</strong> Response <strong>to</strong> <strong>the</strong> Indian Ocean Tsunami, held <strong>in</strong>Medan, Indonesia 13–14 June 2005.United Nations. 2011. Stabilization Mission <strong>in</strong> <strong>Haiti</strong>. Accessed 1 August 2011. www.un.org/en/peacekeep<strong>in</strong>g/missions/m<strong>in</strong>ustah/background.shtml.United Nations Children’s Fund (UNICEF), World <strong>Health</strong> Organization, Pan American <strong>Health</strong> Organization.<strong>2010</strong>. <strong>Haiti</strong> <strong>earthquake</strong>: Technical Note on HIV and <strong>in</strong>fant feed<strong>in</strong>g. Accessed 20 July 2011. Availableat www.who.<strong>in</strong>t/hac/crises/hti/haiti_tecnical_note_hiv_<strong>in</strong>fant_feed<strong>in</strong>g.pdf.United Nations Development Programme. <strong>2010</strong>. Human Development Report <strong>2010</strong>. The real wealth of nations:pathways <strong>to</strong> human development. New York: UNDP.152
BIBLIOGRAPHYUnited Nations Office for <strong>the</strong> Coord<strong>in</strong>ation of Humanitarian Affairs (UN/OCHA), Disaster Assessmentand Coord<strong>in</strong>ation (UNDAC). <strong>2010</strong>. INSARAG <strong>Haiti</strong> <strong>earthquake</strong> <strong>response</strong> – an after-action review of<strong>response</strong>. Geneva: United Nations.United Nations Population Fund (UNFPA). <strong>2010</strong>. Midwifery and nurs<strong>in</strong>g schools destroyed by <strong>Haiti</strong><strong>earthquake</strong> (22 <strong>January</strong> <strong>2010</strong>). Available at: www.unfpa.org/public/news/pid/4756.United States Institute for Peace. <strong>2010</strong>. <strong>Haiti</strong>: a republic of NGO’s? Peace Brief 23. Available at: www.usip.org/files/resources/PB%2023%20<strong>Haiti</strong>%20a%20Republic%20of%20NGOs.pdf.United States. Census Bureau. <strong>2010</strong>. Population Survey of <strong>the</strong> U.S. Available at: www.census.gov/cps.United States. Department of <strong>Health</strong> and Human Services (HHS). <strong>2010</strong>a. National disaster medical systemhelp<strong>in</strong>g U.S. hospitals treat survivors of <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong>. Accessed 24 <strong>January</strong> <strong>2010</strong>. www.hhs.gov/haiti/ndms_ushospitals.html.———. <strong>2010</strong>b. Public health <strong>response</strong> situation update summary, February 19, <strong>2010</strong>. Accessed 10 September2011. www.phe.gov/emergency/news/sitreps/Pages/haiti<strong>earthquake</strong>.aspx.———. Centers for Disease Control and Prevention (CDC). <strong>2010</strong>a. CDC summary of <strong>in</strong>itial rapid assessment(IRA) conducted by UN OCHA <strong>in</strong> <strong>Haiti</strong> (19 February <strong>2010</strong>). Atlanta: CDC. Available from: http://one<strong>response</strong>.<strong>in</strong>fo/Disasters/<strong>Haiti</strong>/Coord<strong>in</strong>ation/publicdocuments/Summary_Report_v_3_5_19_Feb_<strong>2010</strong>.pdf.———. Centers for Disease Control and Prevention (CDC). <strong>2010</strong>b. Dengue fever/dengue haemorrhagicfever: <strong>Haiti</strong> pre-decision brief for public health action. (Update March <strong>2010</strong>). Available at:www.bt.cdc.gov/disasters/<strong>earthquake</strong>s/haiti/dengue_pre-decision_brief.asp.———. Centers for Disease Control and Prevention (CDC). 2011a. After-action report on <strong>the</strong> <strong>response</strong> <strong>to</strong><strong>the</strong> <strong>2010</strong> <strong>Haiti</strong> <strong>earthquake</strong>; February (31 pages). Atlanta: CDC.———. Centers for Disease Control and Prevention (CDC). 2011b. Post-<strong>earthquake</strong> <strong>in</strong>juries treated at afield hospital—<strong>Haiti</strong>, <strong>2010</strong>. MMWR 59(51);1673–7.United States. Department of State. 2011a. Fast facts on U.S. Government’s work <strong>in</strong> <strong>Haiti</strong>: fund<strong>in</strong>g.[Fact Sheet; Office of <strong>the</strong> <strong>Haiti</strong> Special Coord<strong>in</strong>a<strong>to</strong>r, 8 <strong>January</strong> 2011]. Accessed 18 February 2011.www.state.gov/p/wha/rls/fs/2011/154143.htm.———. 2011b. <strong>Haiti</strong>: one year later. Accessed 18 March 2011. www.state.gov/s/hsc/rls/154255.htm.———. 2011c. Post-<strong>earthquake</strong> USG <strong>Haiti</strong> strategy: <strong>to</strong>ward renewal and economic opportunity; Report, <strong>January</strong>3, 2011. Available at: www.state.gov/documents/organization/156448.pdf.United States. Department of <strong>the</strong> Navy. Website. Mexican ship capta<strong>in</strong>s visit Guns<strong>to</strong>n Hall dur<strong>in</strong>g <strong>Haiti</strong>mission. Accessed 20 July 2011. www.navy.mil/search/display.asp?s<strong>to</strong>ry_id=50975.United States. The White House, Office of <strong>the</strong> Press Secretary. <strong>2010</strong>. U.S. <strong>response</strong> <strong>to</strong> <strong>Haiti</strong> <strong>earthquake</strong>disaster; United States outl<strong>in</strong>es relief, rescue and reconstruction efforts <strong>in</strong> <strong>Haiti</strong> [Press release 10 March<strong>2010</strong>]. Available at: www.america.gov/st/texttrans-english/<strong>2010</strong>/March/<strong>2010</strong>0311094127xjsnommis0.607246.html.United States Geologic Survey. 2011. <strong>Haiti</strong> dom<strong>in</strong>ates <strong>earthquake</strong> fatalities <strong>in</strong> <strong>2010</strong>. Press release; 11 <strong>January</strong>2011. Available at: www.usgs.gov/newsroom/article.asp?ID=2679.153
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Van Alphen D. <strong>2010</strong>. Summary of <strong>the</strong> <strong>Health</strong> Cluster: Current state and set-up at one month of operations.Report <strong>to</strong> PAHO/WHO (February <strong>2010</strong>). Unpublished.Vanholder R., A. van der Tol, M. De Smet, et al. 2007. Earthquakes and crush syndrome casualties: lessonslearned from <strong>the</strong> Kashmir disaster. Kidney Int 71(1):17–23.Vanholder, R., N. Gibney, V.A. Luyckx, M.S. Sever. <strong>2010</strong>. Renal Disaster Relief Task Force <strong>in</strong> <strong>Haiti</strong> <strong>earthquake</strong>.Lancet 375(9721):1162–3.Vanholder R., D. Borniche , S. Claus, et al. 2011. When <strong>the</strong> earth trembles <strong>in</strong> <strong>the</strong> Americas: <strong>the</strong> experienceof <strong>Haiti</strong> and Chile. Nephron Cl<strong>in</strong> Pract 117(3):184–97.Vaughan, K.D. <strong>2010</strong>. Edi<strong>to</strong>rial. West Indian Med J 59(2):119–21.Wang, M.Y. <strong>2010</strong>. Devastation after <strong>the</strong> <strong>Haiti</strong> <strong>earthquake</strong>: a neurosurgeon’s journal. World Neurosurg73(5):438-41.Watson J.T., M. Gayer, M. A. Connolly. 2007. Epidemics after natural disasters. Emerg Infect Dis. 13(1):1–5.Weill Cornell Medical College. <strong>2010</strong>. GHESKIO: six months later. Accessed 11 March 2011. http://weill.cornell.edu/globalhealth/featured/gheskio_six_months_later.Weill Cornell Medical College. 2011. GHESKIO: one year later. Accessed 12 March 2011. http://weill.cornell.edu/globalhealth/onl<strong>in</strong>e-global-health-journal/global_health_news/update_from_gheskio_one_year_later.Wickrama K. A. 2008. Family context of mental health risk <strong>in</strong> tsunami affected mo<strong>the</strong>rs: f<strong>in</strong>d<strong>in</strong>gs from apilot study <strong>in</strong> Sri Lanka. Soc Sci Med 66(4):994–1007.W<strong>in</strong>ter, M., I. Osmers, S. Krieger. 2011. Unfallchirurgische Katastrophenhilfe nach dem Erdbeben <strong>in</strong> <strong>Haiti</strong><strong>2010</strong>–E<strong>in</strong> Erfahrungsbericht. [Emergency trauma surgery assistance follow<strong>in</strong>g <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong><strong>2010</strong> – a report on experiences.] Der Unfallchirug 114(1):79–84.World Bank. Hazard Management Unit. 2005. Natural disaster hotspots:a global risk analysis. Wash<strong>in</strong>g<strong>to</strong>n,D.C.: The World Bank. Available at: www.proventionconsortium.org/<strong>the</strong>mes/default/pdfs/Hotspots.pdf.World Bank. Databank Website. http://data.worldbank.org/<strong>in</strong>dica<strong>to</strong>r/NY.GNP.PCAP.CD/countries.World Bank. 2008. Data aga<strong>in</strong>st natural disasters. [Ch 2. Information gaps <strong>in</strong> relief, recovery and reconstruction<strong>in</strong> <strong>the</strong> aftermath of natural disasters.] Wash<strong>in</strong>g<strong>to</strong>n, D.C.: The World Bank.World Bank. The Worldwide Governance Indica<strong>to</strong>rs (WGI) project. http://<strong>in</strong>fo.worldbank.org/governance/wgi/<strong>in</strong>dex.asp.World Food Programme. <strong>2010</strong>. Haïti Nutrition et VIH/SIDA EMOP. [Activity update, 29 April <strong>2010</strong>].World Food Programme. 2011. Lessons from WFP personnel respond<strong>in</strong>g <strong>to</strong> <strong>the</strong> <strong>2010</strong> <strong>Haiti</strong> <strong>earthquake</strong> emergency.Geneva:WFP.World <strong>Health</strong> Organization and Inter-Agency Stand<strong>in</strong>g Committee (WHO/ IASC). 2007. Guidel<strong>in</strong>es onmental health and psychosocial support <strong>in</strong> emergency sett<strong>in</strong>gs. Available at: www.who.<strong>in</strong>t/mental_health/emergencies/guidel<strong>in</strong>es_iasc_mental_health_psychosocial_april_2008.pdf.154
BIBLIOGRAPHYWorld <strong>Health</strong> Organization (WHO). 1999. Inter Agency Guidel<strong>in</strong>es on Drug Donations (due for revision <strong>in</strong><strong>2010</strong>). Available at: http://whqlibdoc.who.<strong>in</strong>t/hq/1999/WHO_EDM_PAR_99.4.pdf.———. <strong>2010</strong>a. Culture and mental health <strong>in</strong> <strong>Haiti</strong>: a literature review (Publication No. WHO/ MSD/MER/10. <strong>2010</strong>). Geneva: WHO. www.who.<strong>in</strong>t/mental_health/emergencies/culture_mental_health_haiti_eng.pdf.———. <strong>2010</strong>b. Evaluation des risques pour la santé publique et <strong>in</strong>terventions. Séisme: <strong>Haiti</strong>. (WHO/HSE/GAR/DCE/<strong>2010</strong>.1). Geneva: WHO.———. <strong>2010</strong>c. Guidance for health sec<strong>to</strong>r assessment <strong>to</strong> support <strong>the</strong> post-disaster recovery process. Version2.2 (17 December <strong>2010</strong>). Available at: www.who.<strong>in</strong>t/hac/techguidance/<strong>to</strong>ols/manuals/pdna_health_sec<strong>to</strong>r_17dec10.pdf.———.<strong>2010</strong>d. Public health risk assessment and <strong>in</strong>terventions: <strong>earthquake</strong>, <strong>Haiti</strong>. Port-au-Pr<strong>in</strong>ce: WHOOffice.———. <strong>2010</strong>e. So<strong>in</strong>s Obstétricaux Gratuits—Pour une grossesse à mo<strong>in</strong>dre risque chez les femmes et les nourrissons.WHO/MPS/10.07. Geneva: WHO.———. <strong>2010</strong>f. Water and sanitation <strong>in</strong> health emergencies: <strong>the</strong> role of WHO <strong>in</strong> <strong>the</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong><strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong>, 12 <strong>January</strong> <strong>2010</strong>. Wkly Epidemiol Rec. 85(36):349–54. Available at www.who.<strong>in</strong>t/wer/<strong>2010</strong>/wer8536.pdf.Yeskey, K. <strong>2010</strong>. The Key Role of NDMS <strong>in</strong> Disaster Response. Testimony before <strong>the</strong> Committee onHomeland Security and Governmental Affairs, U.S. Department of <strong>Health</strong> and Human Services, <strong>2010</strong>.Accessed 5 March 2011. www.hhs.gov/asl/testify/<strong>2010</strong>/07/t<strong>2010</strong>0722a.html.Zanotti L. <strong>2010</strong>. Cacophonies of aid, failed state build<strong>in</strong>g and NGOs <strong>in</strong> <strong>Haiti</strong>: sett<strong>in</strong>g <strong>the</strong> stage for disaster,envision<strong>in</strong>g <strong>the</strong> future. Third World Q 31(5):755–71.155
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>List of acronymsAECIDCARICOMCCCMCDCCDEMACERFDANAERCEUFAOFFHFMTGroupe URDHHSHQIASCICRCIDPIECIFRCIHRCIHRINSARAGIRAAgencia Española de Cooperación Internacional para el Desarrollo(Spanish Agency for International Development Cooperation)Caribbean CommunityCamp Coord<strong>in</strong>ation and Camp ManagementCenters for Disease Control and Prevention (United States)Caribbean Disaster Emergency Management AgencyUnited Nations Central Emergency Response FundDamage Assessment and Needs AnalysisEmergency Relief Coord<strong>in</strong>a<strong>to</strong>r (United Nations)European UnionFood and Agricultural Organization of <strong>the</strong> United NationsForeign Field HospitalForeign Medical TeamGroupe Urgence-Réhabilitation-Développement<strong>Health</strong> and Human Services (United States, Department of)HeadquartersInter-Agency Stand<strong>in</strong>g CommitteeInternational Committee of <strong>the</strong> Red CrossInternally displaced personINSARAG External ClassificationInternational Federation of Red Cross and Red Crescent SocietiesInterim <strong>Haiti</strong> Recovery CommissionInternational <strong>Health</strong> RegulationsInternational Search and Rescue Advisory GroupInitial Rapid Assessment156
LIST OF ACRONYMSLRRDLSSMINUSTAHMOHMSFMSPPNGOOASOCHAPAHOPDNAPROMESSRINAHSOPsSUMAUNUNAIDSUNDACUNDSSUNICEFUSAIDUSGSWASHWBWFPWHOL<strong>in</strong>k<strong>in</strong>g Relief, Rehabilitation, and DevelopmentLogistics Support SystemMission des Nations Unies pour la Stabilisation en Haïti(United Nations Stabilization Mission <strong>in</strong> <strong>Haiti</strong>)M<strong>in</strong>istry of <strong>Health</strong> (also MoH)Médec<strong>in</strong>s Sans Frontières (Doc<strong>to</strong>rs without Borders)M<strong>in</strong>istère de Santé Publique et Population(<strong>Haiti</strong>an M<strong>in</strong>istry of <strong>Health</strong>)Nongovernmental organizationOrganization of American StatesOffice for <strong>the</strong> Coord<strong>in</strong>ation of Humanitarian Affairs (UN)Pan American <strong>Health</strong> OrganizationPost-Disaster Needs AssessmentProgramme de Médicaments Essentiels(Essential Medic<strong>in</strong>es Program <strong>in</strong> <strong>Haiti</strong>)Rapid Initial Needs Assessment for <strong>Haiti</strong>Standard Operat<strong>in</strong>g ProceduresSupply Management SystemUnited NationsUnited Nations Program on HIV/AIDSUnited Nations Disaster Assessment and Coord<strong>in</strong>ationUnited Nations Department of Safety and SecurityUnited Nations Children’s FundUnited States Agency for International DevelopmentUnited States Geological SurveyWater, Sanitation, and HygieneWorld BankWorld Food Programme (UN)World <strong>Health</strong> Organization157
Prior <strong>to</strong> <strong>the</strong> <strong>earthquake</strong>, nearly two-thirds ofLorem ipsum doler sit ameall <strong>Haiti</strong>ans made <strong>the</strong>ir liv<strong>in</strong>g <strong>in</strong> <strong>the</strong> agriculturalsec<strong>to</strong>r, ma<strong>in</strong>ly from small-scale subsistencefarm<strong>in</strong>g, Rum et quate mak<strong>in</strong>g volorio <strong>the</strong>m volorestibus more vulnerable quidessimusaut untem et eaque rectibea prae Git et<strong>to</strong>damage landanti from ulliquat frequent et offictem. natural Et disasters, etus, untiuratiusant vellect orest, omniet volupta tquae.which Nam, es has nim been sequi exacerbated cuptaturi berati by <strong>the</strong> velibus country’s asexerspera is necusci debisqu oditem eos<strong>to</strong>widespread deforestation.officiust vel ipsundaerum eatquunt ute iumeatat.Pho<strong>to</strong>: PAHO/WHO, Armando Waak
Annex1Conditions<strong>in</strong> <strong>Haiti</strong> prior<strong>to</strong> <strong>the</strong> <strong>earthquake</strong>The Republic of <strong>Haiti</strong> occupies <strong>the</strong> western third of <strong>the</strong> Island of Hispaniola, which itshares with <strong>the</strong> Dom<strong>in</strong>ican Republic. The country is divided <strong>in</strong><strong>to</strong> 10 departments andhas an estimated population of 10 million.Nearly half of <strong>Haiti</strong>’s population (47%) lives <strong>in</strong> urban areas, <strong>the</strong> largest be<strong>in</strong>g <strong>the</strong> Portau-Pr<strong>in</strong>cemetropolitan area (which has a population estimated at 2.3 million). Themetropolitan area has expanded considerably <strong>in</strong> population but not so much <strong>in</strong> size <strong>in</strong><strong>the</strong> last 20 years, lead<strong>in</strong>g <strong>to</strong> overcrowded, improvised settlements on <strong>the</strong> steep slopessurround<strong>in</strong>g <strong>the</strong> old city.In terms of population density, <strong>Haiti</strong> ranks second after Barbados (and a few islandterri<strong>to</strong>ries <strong>in</strong> <strong>the</strong> Caribbean) <strong>in</strong> <strong>the</strong> Region of <strong>the</strong> Americas. The density is particularlyhigh <strong>in</strong> Port-au-Pr<strong>in</strong>ce.159
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Social, political, and economic determ<strong>in</strong>ants 146<strong>Haiti</strong> was <strong>the</strong> first country <strong>to</strong> ga<strong>in</strong> sovereignty <strong>in</strong> Lat<strong>in</strong> America and <strong>the</strong> Caribbeanand <strong>in</strong> 2004 it celebrated 200 years of <strong>in</strong>dependence. With nearly two centuriesof dicta<strong>to</strong>rship and <strong>in</strong>termittent attempts at democracy beg<strong>in</strong>n<strong>in</strong>g <strong>in</strong> <strong>the</strong> late1980s, <strong>the</strong> country has suffered recurrent periods of political <strong>in</strong>stability. Follow<strong>in</strong>g<strong>the</strong> 1991 military coup, an OAS/UN embargo was enforced <strong>in</strong> 1993. The oustedPresident Aristide returned <strong>to</strong> <strong>the</strong> country <strong>in</strong> 1994. One of <strong>the</strong> first decisions of thisnew Government was <strong>to</strong> dismantle <strong>the</strong> army, leav<strong>in</strong>g <strong>the</strong> police forces as <strong>the</strong> onlynational security <strong>in</strong>stitution.Follow<strong>in</strong>g a political crisis, <strong>in</strong> March 2004 a new transitional government was <strong>in</strong>stalledwith <strong>the</strong> support of <strong>the</strong> United Nations Stabilization Mission (MINUSTAH),pav<strong>in</strong>g <strong>the</strong> way for presidential and parliamentary elections <strong>in</strong> February 2006. Presidentialelections were scheduled <strong>to</strong> take place <strong>in</strong> <strong>2010</strong> and <strong>the</strong> country was enter<strong>in</strong>g<strong>in</strong><strong>to</strong> <strong>the</strong> elec<strong>to</strong>ral period at <strong>the</strong> end of 2009. The government was <strong>in</strong> a weak positionwhen <strong>the</strong> <strong>earthquake</strong> struck <strong>in</strong> <strong>January</strong> <strong>2010</strong>. 147The vast majority of <strong>Haiti</strong>ans cont<strong>in</strong>ue <strong>to</strong> live under precarious conditions, <strong>in</strong> povertyand marg<strong>in</strong>alization. This poverty especially affects women heads of households, as<strong>the</strong>y are often <strong>the</strong> primary breadw<strong>in</strong>ners.The UNDP Human Development Report issued <strong>in</strong> <strong>2010</strong> (with data from 2007), illustrates <strong>the</strong> pre<strong>earthquake</strong>situation <strong>in</strong> <strong>Haiti</strong>:• Ranks 145 out of 169 countries for <strong>the</strong> human development <strong>in</strong>dex. This <strong>in</strong>dex improvedslightly s<strong>in</strong>ce 2005, but rema<strong>in</strong>s <strong>the</strong> lowest among Caribbean and Central Americancountries;• In Lat<strong>in</strong> America and <strong>the</strong> Caribbean multidimensional poverty affects from 2% of <strong>the</strong> population(Uruguay) <strong>to</strong> 57% (<strong>Haiti</strong>); 148• Among <strong>the</strong> few countries do<strong>in</strong>g very poorly both on gender equality and human developmentare <strong>the</strong> Central African Republic, <strong>Haiti</strong>, and Mozambique.Income distribution is <strong>in</strong>equitable: 4% of <strong>the</strong> population has 66% of <strong>the</strong> nation’swealth, while 10% has practically noth<strong>in</strong>g. Foreign commercial <strong>in</strong>vestment is m<strong>in</strong>imaland manufactur<strong>in</strong>g or service employment is practically nonexistent for <strong>the</strong>majority of <strong>the</strong> population. Imports (<strong>in</strong>clud<strong>in</strong>g food and fuel) exceed exports by afac<strong>to</strong>r of four.Deficient farm<strong>in</strong>g practices on steep terra<strong>in</strong> have accelerated soil erosion, as <strong>the</strong> run-offfrom tropical ra<strong>in</strong>s flushes arable land <strong>to</strong>ward <strong>the</strong> sea, fur<strong>the</strong>r obstruct<strong>in</strong>g urban dra<strong>in</strong>-146 Compiled from various sources, <strong>in</strong>clud<strong>in</strong>g: Institut <strong>Haiti</strong>en de Statistique et Informatique (IHSI <strong>2010</strong>); World Bank,<strong>Haiti</strong> at a glance (2006); PAHO/WHO, <strong>Health</strong> <strong>in</strong> <strong>the</strong> Americas (2007); WHO, <strong>Haiti</strong> health profile (<strong>2010</strong>); United Nations,World population prospects: <strong>the</strong> 2008 revision (2009).147 The presidential elections f<strong>in</strong>ally <strong>to</strong>ok place at <strong>the</strong> end of <strong>2010</strong>, but <strong>the</strong>re was an <strong>in</strong>ternational challenge of <strong>the</strong> results. Asecond round of elections were completed <strong>in</strong> 2011.148 The UNDP Multidimensional Poverty Index (MPI) complements <strong>in</strong>come poverty measures by reflect<strong>in</strong>g <strong>the</strong> deprivationsthat a poor person faces all at once with respect <strong>to</strong> education, health, and liv<strong>in</strong>g standard. It assesses poverty at <strong>the</strong><strong>in</strong>dividual level, with poor persons be<strong>in</strong>g those who are deprived <strong>in</strong> multiple areas, and <strong>the</strong> extent of <strong>the</strong>ir poverty be<strong>in</strong>gmeasured by <strong>the</strong> range of <strong>the</strong>ir deprivations.160
HAITI PRIOR TO THE EARTHQUAKE - Annex 1age systems already clogged by huge quantities of urban debris. Heavy deforestation isnoticeable from <strong>the</strong> air, almost del<strong>in</strong>eat<strong>in</strong>g <strong>the</strong> border between <strong>Haiti</strong> and <strong>the</strong> Dom<strong>in</strong>icanRepublic. Sanitation management is <strong>in</strong>effective or nonexistent, so excreta and householdwaste heavily pollute surface water.An estimated 25% <strong>to</strong> 50% of national <strong>in</strong>come comes from remittances from <strong>the</strong> approximatelyone million <strong>Haiti</strong>ans liv<strong>in</strong>g and work<strong>in</strong>g abroad, mostly <strong>in</strong> <strong>the</strong> UnitedStates, Canada, and France. Accord<strong>in</strong>g <strong>to</strong> <strong>the</strong> <strong>2010</strong> Population Survey of <strong>the</strong> U.S., <strong>in</strong>2009 nearly one-third of <strong>Haiti</strong>an immigrants <strong>in</strong> <strong>the</strong> U.S. belonged <strong>to</strong> households thatearned more than US$ 60,000. In comparison, less than 15% of <strong>the</strong> immigrants fromMexico, Dom<strong>in</strong>ican Republic, and El Salvador <strong>in</strong> <strong>the</strong> U.S. had that level of household<strong>in</strong>come. A quarter of <strong>Haiti</strong>an immigrants, especially women, are reportedly <strong>in</strong><strong>the</strong> relatively higher pay<strong>in</strong>g health care and education sec<strong>to</strong>rs; only a small numberof <strong>the</strong>m are <strong>in</strong> <strong>the</strong> construction sec<strong>to</strong>r (Ratha <strong>2010</strong>). Emigration of highly qualifiedhealth personnel is a serious issue.Salaries of civil servants <strong>in</strong> <strong>Haiti</strong>, health professionals <strong>in</strong>cluded, rema<strong>in</strong> unpaid formonths at a time. This leaves professionals little option but moonlight<strong>in</strong>g or charg<strong>in</strong>gfees for services <strong>to</strong> make a liv<strong>in</strong>g.Governance, or ra<strong>the</strong>r <strong>the</strong> lack of it, is often cited as one of <strong>the</strong> most serious shortcom<strong>in</strong>gs<strong>in</strong> <strong>Haiti</strong>. In 2008, Transparency International’s “Corruption Perception Index”ranked <strong>Haiti</strong> 177 out of 180 countries (<strong>the</strong> last five were Afghanistan, <strong>Haiti</strong>, Iraq,Myanmar, and Somalia). In <strong>2010</strong>, that score (on a scale of 10) improved from 1.1–1.7(2008) <strong>to</strong> 2.2, mov<strong>in</strong>g <strong>Haiti</strong>’s rank<strong>in</strong>g <strong>to</strong> 146 out of 178.It is undeniable that poor national governance is a major obstacle <strong>in</strong> <strong>Haiti</strong>, but <strong>the</strong><strong>in</strong>ternational community should assume its share of responsibility for bypass<strong>in</strong>g<strong>the</strong> government—<strong>the</strong>reby weaken<strong>in</strong>g it—for most decisions and projects. An <strong>in</strong>ternational“blank check” (f<strong>in</strong>ancially and politically) written <strong>to</strong> NGOs that oftenhave <strong>the</strong>ir own agenda and shortcom<strong>in</strong>gs is legitimiz<strong>in</strong>g a culture of unaccountability<strong>in</strong> <strong>the</strong> public service sec<strong>to</strong>r (Zanotti <strong>2010</strong>). Officials who are not mean<strong>in</strong>gfullyconsulted and have no authority over <strong>the</strong> resources assigned <strong>to</strong> foreignimplement<strong>in</strong>g agencies (NGOs) cannot feel responsible.It is estimated that between 3,000 and 10,000 NGOs are operat<strong>in</strong>g <strong>in</strong> <strong>Haiti</strong>, one of<strong>the</strong> highest densities of NGOs per capita <strong>in</strong> <strong>the</strong> world. Accord<strong>in</strong>g <strong>to</strong> <strong>the</strong> U.S. Institutefor Peace (<strong>2010</strong>), USAID budgeted some US$ 300 million for <strong>Haiti</strong> <strong>in</strong> fiscal year2007–2008, all of which was implemented through NGOs. These projects often hadmore money than <strong>the</strong> entire <strong>Haiti</strong>an M<strong>in</strong>istry of Plann<strong>in</strong>g. For this reason, <strong>Haiti</strong> hasbeen called “<strong>the</strong> Republic of NGOs.”<strong>Health</strong> status 149Table A.1 offers a comparative summary of selected <strong>in</strong>dica<strong>to</strong>rs for <strong>Haiti</strong>, Dom<strong>in</strong>ican Republic,and <strong>the</strong> entire Lat<strong>in</strong> American and Caribbean region (exclud<strong>in</strong>g North America).149 Sources for this section <strong>in</strong>clude: PAHO/WHO, <strong>Health</strong> <strong>in</strong> <strong>the</strong> Americas 2007 (at www.paho.org/HIA/home<strong>in</strong>g.html);PAHO/WHO, 2009 Basic Indica<strong>to</strong>rs; and <strong>Haiti</strong>, PDNA analytical matrix June <strong>2010</strong>.161
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Table A.1 Selected <strong>in</strong>dica<strong>to</strong>rs for <strong>Haiti</strong>, Dom<strong>in</strong>ican Republic,and <strong>the</strong> Lat<strong>in</strong> American and Caribbean regionSelected <strong>in</strong>dica<strong>to</strong>rs <strong>Haiti</strong> Dom<strong>in</strong>icanRepublicLat<strong>in</strong> America& CaribbeanPopulation density/km 2 367 211 Estimated 29Urban population (projected % for <strong>2010</strong>) 48.2 69.7 78.8Life expectancy (years) 61.5 72.7 73.5Mortality under 5 years/1,000 Pop (2007) 76 24 38Under-registration of mortality94.7 47 16.1(%, 2003–2005)Malaria API /1,000 Pop (2008) 9.8 3.3 11.1Hospital beds /10,000 (2005–2008) 13 10 18Measles/MMR Immunization(% coverage, 2008)58 95 94Sources: WHO, World <strong>Health</strong> Statistics, 2009 www.who.<strong>in</strong>t/whosis/whostat/EN_WHS09_Table6.pdf; World Bank,<strong>Haiti</strong> at a glance; Dom<strong>in</strong>ican Republic at a glance.Core health <strong>in</strong>dica<strong>to</strong>rs are, <strong>in</strong>deed, alarm<strong>in</strong>g. Mortality rates are by far <strong>the</strong> highest <strong>in</strong> <strong>the</strong>Region of <strong>the</strong> Americas, with <strong>the</strong> crude mortality rate of 12 deaths per 1,000 population;under-5 mortality rate of 76 deaths per 1,000 live births; <strong>in</strong>fant mortality rate of 57 deathsper 1,000 live births—that is, 1 <strong>in</strong> every 12 children dies before her/his first birthday;and <strong>the</strong> maternal mortality rate of 670 deaths per 100,000 live births. 150 Life expectancyat birth, estimated at 61.5 years (59.7 <strong>in</strong> males and 63.2 <strong>in</strong> females) is <strong>the</strong> lowest <strong>in</strong> <strong>the</strong>Americas. Birth rate rema<strong>in</strong>s high, at 25 per 1,000 <strong>in</strong> urban areas and 30 per 1,000 <strong>in</strong> ruralareas; <strong>the</strong> average number of children per woman is 3 <strong>in</strong> urban areas and 4 <strong>in</strong> rural areas.Quantified data on communicable diseases are limited <strong>in</strong> normal times. Disaggregateddata on morbidity or mortality by cause, gender or age are mostly unavailableexcept for malaria, which has an annual parasite <strong>in</strong>cidence (API) three times that of<strong>the</strong> Dom<strong>in</strong>ican Republic.Acute diarrheal disease is highly prevalent: 2 out of 5 children aged 6 <strong>to</strong> 11 (40%), and1 out of 4 children under 5 years old (25%) experienced one or more episodes of diarrhea<strong>in</strong> any two-week period. All o<strong>the</strong>r age groups are also disproportionately affected.However, <strong>the</strong> last outbreak of cholera had been reported <strong>in</strong> <strong>Haiti</strong> over 100 years prior<strong>to</strong> <strong>the</strong> <strong>earthquake</strong> and <strong>the</strong> disease was <strong>to</strong>tally absent until <strong>the</strong> outbreak <strong>in</strong> late <strong>2010</strong>. 151In spite of <strong>the</strong> poor sanitation and lack of access <strong>to</strong> safe water, <strong>Haiti</strong> was spared dur<strong>in</strong>g<strong>the</strong> 1991–1993 cholera outbreak that started <strong>in</strong> Peru and killed over 4,000 people <strong>in</strong><strong>the</strong> Western hemisphere.<strong>Haiti</strong> has <strong>the</strong> highest <strong>in</strong>cidence of tuberculosis <strong>in</strong> <strong>the</strong> Americas (about 30,000 newcases per year); it is reportedly <strong>the</strong> seventh lead<strong>in</strong>g cause of death <strong>in</strong> <strong>the</strong> country. TB/HIV co-<strong>in</strong>fection rate is close <strong>to</strong> 30%.162150 Mortality statistics <strong>in</strong> normal times are very <strong>in</strong>complete: under-registration is estimated <strong>to</strong> be 94.7%. Death certificatesare filled out for only 1 <strong>in</strong> 20 deaths (5% coverage), and yet 1 <strong>in</strong> every 3 death certificates records an ill-def<strong>in</strong>ed cause ofdeath.151 A national epidemic of cholera started <strong>in</strong> Oc<strong>to</strong>ber <strong>2010</strong> <strong>in</strong> <strong>the</strong> Artibonite department, an area that was not affected by <strong>the</strong><strong>earthquake</strong>.
HAITI PRIOR TO THE EARTHQUAKE - Annex 1HIV/AIDS and sexually transmitted <strong>in</strong>fections (STIs) are common <strong>in</strong> <strong>Haiti</strong>. Accord<strong>in</strong>g <strong>to</strong><strong>the</strong> 2005-2006 Mortality, Morbidity, and Service Utilization Survey for <strong>Haiti</strong> (EMMUS-IV), estimates put HIV prevalence at 2.2% (2.3% among women aged 15–49 and 2%among men aged 15–59). <strong>Haiti</strong>’s HIV/AIDS program is cited as one of <strong>the</strong> most successful<strong>in</strong> <strong>the</strong> world, on <strong>the</strong> way <strong>to</strong> provid<strong>in</strong>g universal treatment for HIV/AIDS nationwide(Koenig et al. <strong>2010</strong>). 152Vacc<strong>in</strong>e-preventable diseases such as diph<strong>the</strong>ria and neo-natal tetanus are all <strong>to</strong>ocommon. Grave concern arises from <strong>the</strong> extremely low immunization coverage ratesfor measles (54%); diph<strong>the</strong>ria, pertussis and tetanus (68%); and polio (66%) <strong>in</strong>children under 1 year old. In 2009 an epidemic of diph<strong>the</strong>ria with 29 confirmedcases affected Port-au-Pr<strong>in</strong>ce and rural departments. By <strong>the</strong> end of <strong>the</strong> year WHOepidemiologists feared an explosive outbreak <strong>in</strong> <strong>the</strong> shanty<strong>to</strong>wns of <strong>the</strong> Port-au-Pr<strong>in</strong>ce metropolitan area (<strong>in</strong>clud<strong>in</strong>g Carrefour). In <strong>the</strong> past, <strong>Haiti</strong> has led severalmeasles vacc<strong>in</strong>ation campaigns, <strong>the</strong> last one <strong>in</strong> 2007 aga<strong>in</strong>st measles/rubella forchildren and adolescents between 1 and 19 years old. The last case of <strong>in</strong>digenousmeasles reported <strong>in</strong> <strong>Haiti</strong> was <strong>in</strong> 2001.Tropical diseases such as leprosy and lymphatic filariasis rema<strong>in</strong>ed prevalent <strong>in</strong> spiteof progress <strong>in</strong> <strong>the</strong>ir control.Dengue was first confirmed <strong>in</strong> <strong>Haiti</strong> <strong>in</strong> 1964, but national surveillance of dengue hasnot taken place. Accord<strong>in</strong>g <strong>to</strong> <strong>the</strong> CDC, a study of 215 children <strong>in</strong> Port-au-Pr<strong>in</strong>ce <strong>in</strong>1996 showed that 85% had been previously <strong>in</strong>fected with one or two dengue virusserotypes. Studies dur<strong>in</strong>g prior foreign military operations found “m<strong>in</strong>imal numbersof symp<strong>to</strong>matic community cases or hospitalizations, while high attack rate and severecases were reported among foreign military and foreign civilian personnel <strong>in</strong> <strong>Haiti</strong>”(CDC <strong>2010</strong>b).The delivery of health services<strong>Health</strong> services delivery is mostly private with a small public component. An estimated75% of health care is provided by NGOs, faith-based groups, and o<strong>the</strong>r foreignmedical providers.The public health services network <strong>in</strong> <strong>Haiti</strong> is organized <strong>in</strong> three levels:1. The primary level comprises ± 600 cl<strong>in</strong>ics with and without beds, and 45 communityhospitals;2. The secondary level <strong>in</strong>cludes n<strong>in</strong>e department hospitals; 1533. The tertiary level represents <strong>the</strong> six university hospitals (five are <strong>in</strong> Port-au-Pr<strong>in</strong>ce;<strong>the</strong> pr<strong>in</strong>cipal one is <strong>the</strong> University Hospital—HUEH).152 This success is tied <strong>to</strong> a strong foundation for HIV care that was <strong>in</strong> place before external fund<strong>in</strong>g became available. This<strong>in</strong>cludes national guidel<strong>in</strong>es prepared by <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong>; political commitment at <strong>the</strong> highest levels of government;NGOs that had been provid<strong>in</strong>g high quality care <strong>in</strong> <strong>Haiti</strong> for decades; and <strong>the</strong> assistance of <strong>the</strong> Global Fund <strong>to</strong>Fight AIDS, TB, and Malaria, <strong>the</strong> U.S. President’s Emergency Plan for AIDS Relief (PEPFAR), and o<strong>the</strong>r private donors(Koenig et al. <strong>2010</strong>).153 There are 10 departments <strong>in</strong> <strong>Haiti</strong>, but <strong>the</strong> West department, where <strong>the</strong> capital is located, has only university hospitals.163
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>S<strong>in</strong>ce 2009, five <strong>in</strong>tegrated diagnostic centers have been established <strong>to</strong> serve as a bridgebetween first and second care levels, but <strong>the</strong>y have not yet been <strong>in</strong>tegrated with <strong>the</strong> res<strong>to</strong>f <strong>the</strong> system. A decentralized organization was also formulated through Communal<strong>Health</strong> Units (one CHU for 80,000–140,000 people) but this had not been effectivelyimplemented at <strong>the</strong> time of <strong>the</strong> <strong>earthquake</strong>. Decentralization is still <strong>in</strong> its <strong>in</strong>fancy andbe<strong>in</strong>g implemented very slowly. As a result, most of <strong>the</strong> functions are still very centralizedwith <strong>the</strong> roles and responsibilities between levels poorly def<strong>in</strong>ed. There is noframework for <strong>the</strong> participation of communities <strong>in</strong> management of <strong>the</strong> CHU. Thereis also major confusion about roles and responsibilities among levels of care (i.e., <strong>the</strong>CHU provide primary level care as well as serv<strong>in</strong>g as departmental hospitals).Accord<strong>in</strong>g <strong>to</strong> 2007 reports, nearly half of <strong>the</strong> population lacked access <strong>to</strong> basic health care.F<strong>in</strong>ancial barriers were seen as <strong>the</strong> ma<strong>in</strong> problem. There was a fee for services and localhealth facilities were heavily dependent on this <strong>in</strong>come <strong>to</strong> pay for part of <strong>the</strong>ir staff andservices. When accessible, services were poor due <strong>to</strong> lack of quality control, <strong>in</strong>frastructuraldeficiencies, poor communication equipment, electrical blackouts, water problems, andgeneral deterioration of <strong>the</strong> facilities.A jo<strong>in</strong>t <strong>in</strong>itiative of <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong>, PAHO/WHO, and CIDA was launched<strong>in</strong> 2007 <strong>to</strong> provide access <strong>to</strong> free obstetric care (So<strong>in</strong>s Obstétricaux Gratuits, or SOG).Follow<strong>in</strong>g <strong>the</strong> <strong>earthquake</strong>, a similar free program was <strong>in</strong>stituted for children under age5 (So<strong>in</strong>s Infantiles Gratuits, or SIG).Specialized services such as rehabilitation for persons with disabilities or mental healthcare are far beh<strong>in</strong>d <strong>the</strong> level and quality <strong>in</strong> neighbor<strong>in</strong>g countries.The National Blood Safety Program (NBSP) was created by <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong><strong>to</strong> establish standards for safe blood transfusions, <strong>in</strong>crease voluntary blood donations,and facilitate access <strong>to</strong> safe blood for patients. Between 2004 and 2009, blood collectionrose by 250%, <strong>the</strong> number of blood units <strong>in</strong>creased from 9,000 <strong>to</strong> 22,000, andvoluntary blood donations rose from 47% <strong>to</strong> 70%. The NBSP hoped <strong>to</strong> reach <strong>the</strong> goalof 100% voluntary donations by <strong>2010</strong>.Inequities are widespread <strong>in</strong> health service delivery: 68% of women <strong>in</strong> <strong>the</strong> wealthiestqu<strong>in</strong>tile deliver <strong>in</strong> a health facility while only 6% of <strong>the</strong> poorest qu<strong>in</strong>tile does. A highmajority (90%) of <strong>the</strong> urban population is with<strong>in</strong> 30 m<strong>in</strong>utes of a health facility, butthis is <strong>the</strong> case for only about 50% of people <strong>in</strong> rural areas.In a review carried out <strong>in</strong> 2007 on governance of <strong>the</strong> health sec<strong>to</strong>r, leadership andregulation functions were seen as “weak or very weak,” at central, departmental, andperiphery levels. Most of <strong>the</strong> services are operated or delivered by a mix of public andprivate not-for-profit entities without an effective pre-exist<strong>in</strong>g policy dialogue/coord<strong>in</strong>ationmechanism with relevant development partners.On <strong>the</strong> positive side, numerous health NGOs and faith-based organizations that haveplayed a major role <strong>in</strong> humanitarian <strong>response</strong> <strong>in</strong> o<strong>the</strong>r major disasters were alreadypresent with ongo<strong>in</strong>g programs <strong>in</strong> <strong>Haiti</strong> at <strong>the</strong> time of <strong>the</strong> <strong>earthquake</strong>. Their familiaritywith <strong>the</strong> situation and <strong>the</strong> existence of a support and logistics mechanism will becritical as <strong>Haiti</strong> rebuilds after <strong>the</strong> impact.The private for-profit sec<strong>to</strong>r is small (< 5% of services), is not regulated, and providesservices <strong>to</strong> higher <strong>in</strong>come patients often pend<strong>in</strong>g <strong>the</strong>ir referral <strong>to</strong> foreign facilities.164
HAITI PRIOR TO THE EARTHQUAKE - Annex 1In addition <strong>to</strong> a thriv<strong>in</strong>g, private pharmaceutical <strong>in</strong>dustry, PROMESS (Programme deMédicaments Essentiels) is <strong>the</strong> central procurement facility and warehouse of essentialdrugs for <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong> and most of its non-profit partners. Established<strong>in</strong> 1992 dur<strong>in</strong>g <strong>the</strong> embargo after a coup d’état, this program, managed by <strong>the</strong> PanAmerican <strong>Health</strong> Organization, serves as <strong>the</strong> national pharmacy, offer<strong>in</strong>g essentialsupplies and drugs at or below cost thanks <strong>to</strong> <strong>the</strong> support of donor agencies. A wells<strong>to</strong>ckedand managed central warehouse has proven <strong>to</strong> be an <strong>in</strong>valuable asset <strong>in</strong> pastdisasters strik<strong>in</strong>g <strong>Haiti</strong>. However, because PROMESS is dependent on outside fund<strong>in</strong>gand completion of agreements between <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong> and all its partners,it has not evolved <strong>in</strong><strong>to</strong> a national system offer<strong>in</strong>g <strong>the</strong> complete range of items requiredfor health care.Governance problems <strong>in</strong> <strong>Haiti</strong> are well-known but <strong>the</strong>y cannot be attributed solely <strong>to</strong>government shortcom<strong>in</strong>gs: As noted at <strong>the</strong> multi-sec<strong>to</strong>ral level, <strong>the</strong> fragmentation ofservices is also due <strong>to</strong> donor policies result<strong>in</strong>g <strong>in</strong> several vertical programs be<strong>in</strong>g wellfunded while o<strong>the</strong>rs are poorly supported if at all. Self-funded health NGOs are reluctant<strong>to</strong> respect M<strong>in</strong>istry norms and procedures because <strong>the</strong>y are pursu<strong>in</strong>g <strong>the</strong>ir ownobjectives <strong>in</strong> l<strong>in</strong>e with <strong>the</strong>ir own policies, standards, and pro<strong>to</strong>cols. “Lead<strong>in</strong>g” such asec<strong>to</strong>r under such conditions is, <strong>in</strong>deed, almost an impossible task.In terms of <strong>in</strong>formation management, <strong>the</strong>re is <strong>in</strong>adequate <strong>in</strong>formation <strong>to</strong> supportdecision-mak<strong>in</strong>g at strategic and operational levels. The existence of many parallel orvertical health <strong>in</strong>formation systems based on projects f<strong>in</strong>anced by specific donors hasnot contributed <strong>to</strong> streaml<strong>in</strong><strong>in</strong>g <strong>the</strong> <strong>in</strong>formation.Water and sanitationWhile only 58% of <strong>the</strong> general population has some access <strong>to</strong> improved dr<strong>in</strong>k<strong>in</strong>gwatersources, <strong>in</strong> urban sett<strong>in</strong>gs access is estimated at 70% (Schuftan et al. 2007). Inurban areas, safe dr<strong>in</strong>k<strong>in</strong>g water is provided, for a fee, by a commercial (or <strong>in</strong> some<strong>in</strong>stances subsidized) distribution network of treated water (reverse osmosis mostly).Even <strong>the</strong> poor urban population <strong>in</strong> <strong>the</strong> capital will <strong>in</strong>vest <strong>the</strong>ir limited resources forhigh quality, <strong>in</strong>dustrially processed water sold retail, by <strong>the</strong> gallon. Small <strong>in</strong>dividualplastic bags sold as high quality water are believed not <strong>to</strong> come from safe <strong>in</strong>dustrialsources. Piped public distribution system is rudimentary and limited even <strong>in</strong> Portau-Pr<strong>in</strong>ce.Accord<strong>in</strong>g <strong>to</strong> <strong>the</strong> <strong>Haiti</strong>an Institute for Statistics (IHSI), only 8% of houseshave piped water and <strong>the</strong>y are ma<strong>in</strong>ly located <strong>in</strong> limited areas of Port-au-Pr<strong>in</strong>ce. Pipedwater <strong>in</strong> <strong>Haiti</strong> is not fit <strong>to</strong> dr<strong>in</strong>k.Only 19% of <strong>Haiti</strong>ans have access <strong>to</strong> improved sanitation and disposal of excreta(29% <strong>in</strong> urban areas and 12% <strong>in</strong> rural). Those who have access <strong>to</strong> a septic tank orlatr<strong>in</strong>e use <strong>the</strong> services of a group of specialized workers called bayakou, who manuallyempty excreta. Dedicated sites for discharge are mostly absent, a situation that <strong>in</strong>duceshigh environmental and health risks. As a sewage system is nonexistent <strong>in</strong> most poorsuburban areas, accumulated solid and liquid waste are flushed away periodically by<strong>the</strong> ra<strong>in</strong>s through an unma<strong>in</strong>ta<strong>in</strong>ed s<strong>to</strong>rm dra<strong>in</strong>age system.165
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>NutritionThe pre-<strong>earthquake</strong> global acute malnutrition (GAM) rate was estimated at 4.5% for<strong>the</strong> affected areas, with severe acute malnutrition at 0.8%. 154 At <strong>the</strong>se levels, an estimated17,500 children under 5 years old are suffer<strong>in</strong>g from acute malnutrition and3,100 of <strong>the</strong>se are severely malnourished and <strong>in</strong> need of life-sav<strong>in</strong>g assistance. Whilehigh, <strong>the</strong>se levels are markedly under those considered a humanitarian emergency(10%). Stunt<strong>in</strong>g rates are significant (30% <strong>in</strong> 2005). 155Nutrition <strong>in</strong>terventions have been scarce, and <strong>the</strong> lack of coord<strong>in</strong>ation at central anddepartmental levels have had important negative effects on <strong>the</strong> efficiency of <strong>the</strong>se <strong>in</strong>terventions.In an article published by <strong>the</strong> World Bank, <strong>the</strong> author made <strong>the</strong> follow<strong>in</strong>gobservations about deficits <strong>in</strong> nutrition programs prior <strong>to</strong> <strong>the</strong> <strong>earthquake</strong>:• “There was no structure <strong>in</strong> place <strong>to</strong> address nutrition security comprehensively.The approach was patchwork, with small, mostly donor- and NGO-run programsoperat<strong>in</strong>g <strong>in</strong> dist<strong>in</strong>ct areas.• “The health system had serious coverage gaps and was not oriented, nor endowedwith <strong>the</strong> human and material resources, <strong>to</strong> address nutrition issues.• “Programmatic coord<strong>in</strong>ation was an enormous challenge. There was little communicationacross implementers or with government.• “Program focus was not sufficiently aligned with <strong>Haiti</strong>’s priority nutrition securityproblems or with <strong>in</strong>ternational best practices. The majority of nutrition programs<strong>in</strong> <strong>Haiti</strong> focused on <strong>the</strong> treatment of acute malnutrition because <strong>the</strong> problem ismore visible” (Bassett <strong>2010</strong>).It should be po<strong>in</strong>ted out that <strong>in</strong> 2009 national guidel<strong>in</strong>es <strong>to</strong> address malnutrition weredeveloped, <strong>in</strong>clud<strong>in</strong>g a National Pro<strong>to</strong>col for <strong>the</strong> Management of Acute Malnutrition.This was undertaken through <strong>the</strong> concerted efforts of <strong>the</strong> Nutrition Department of<strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong>, several NGOs, and donors (<strong>in</strong> particular <strong>the</strong> EC’s Direc<strong>to</strong>rate-General for Humanitarian Aid). Follow<strong>in</strong>g hurricanes that hit <strong>Haiti</strong> <strong>in</strong> 2008, a NutritionCluster was set up by UNICEF, which was replaced <strong>in</strong> 2009 by <strong>the</strong> NationalNutrition Committee led by <strong>the</strong> M<strong>in</strong>istry of <strong>Health</strong>.Malnutrition <strong>in</strong> <strong>Haiti</strong> is <strong>the</strong> end-result of extreme poverty associated with low educationlevel. It is primarily an economic and equity issue ra<strong>the</strong>r a health one. In addition<strong>to</strong> economic and equity issues underly<strong>in</strong>g causes of malnutrition such as food <strong>in</strong>security,<strong>in</strong>fant feed<strong>in</strong>g practices, maternal and child health, health care access, and waterand sanitation conditions and practices are strong contribut<strong>in</strong>g fac<strong>to</strong>rs.154 Nutritional survey carried out by <strong>the</strong> <strong>Haiti</strong>an M<strong>in</strong>istry of <strong>Health</strong> and Action aga<strong>in</strong>st Hunger (December 2008–March 2009).155 World Bank, <strong>Haiti</strong> at glance, <strong>2010</strong>.166
HAITI PRIOR TO THE EARTHQUAKE - Annex 1Mental healthThe Centre de Psychiatrie Mars et Kl<strong>in</strong>e and <strong>the</strong> Hospital Psychiatrique Défilé deBeudet are <strong>the</strong> only two government-run, psychiatric facilities <strong>in</strong> metropolitan Portau-Pr<strong>in</strong>ce.No public <strong>in</strong>stitution offers mental health services outside <strong>the</strong> capital, butseveral small, private centers have emerged. The Mars et Kl<strong>in</strong>e center is <strong>the</strong> sole nationalfacility for treatment of acute (short-term) cases while <strong>the</strong> Hospital Défilé deBeudet is dedicated <strong>to</strong> severe chronic cases.Mental health approaches <strong>in</strong> <strong>Haiti</strong> were centered on medical and hospital <strong>in</strong>terventionsfar from <strong>the</strong> community-based approach recommended by WHO. There iswidespread belief that mental illness is caused by supernatural forces, which fur<strong>the</strong>rcomplicates a modern approach.Figure A.1 shows that <strong>the</strong> ratio of psychiatrists per 100,000 <strong>in</strong>habitants <strong>in</strong> <strong>Haiti</strong> is <strong>the</strong>lowest <strong>in</strong> <strong>the</strong> Caribbean and Central American regions.Figure A.1 Psychiatrists per 100,000 population<strong>in</strong> selected countries of Central America and <strong>the</strong> Caribbean3.533.463.062.522.071.51.3910.50.90.810.570.230PanamaCosta RicaDom<strong>in</strong>icanRepublicEl SalvadorNicaraguaHondurasGuatemalaHaiPsychiatrists per 100,000 populationSource: Based on data collected by V. Aparicio, WHO Advisor, Mission report on mental health and psychosocial supportfollow<strong>in</strong>g <strong>the</strong> <strong>Haiti</strong> <strong>earthquake</strong> (3–26 February 2011).Gender-based violenceGender-based violence was a well-known issue prior <strong>to</strong> <strong>the</strong> <strong>earthquake</strong>. A study carriedout by <strong>the</strong> Inter-American Development Bank <strong>in</strong> <strong>Haiti</strong> <strong>in</strong> 2006 reported tha<strong>to</strong>ne-third of women and girls reported <strong>in</strong>cidents of physical or sexual violence. TheInter-American Commission on Human Rights (OAS) reports that more than 50percent of those who had experienced violence were under <strong>the</strong> age of 18. A 2006 surveystudy attests <strong>to</strong> <strong>the</strong> rampant use of rape as both a <strong>to</strong>ol and outcome of violence,167
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>document<strong>in</strong>g that 35,000 women were victimized <strong>in</strong> <strong>the</strong> area surveyed (Kolbe andHutson 2006). The real scale of <strong>the</strong> problem is not fully known because of a lack ofcentral figures on rapes.Gender-based violence is often considered <strong>to</strong> be most common <strong>in</strong> poor slum areaswhere overcrowd<strong>in</strong>g, poverty, and lack of education are fac<strong>to</strong>rs. In <strong>Haiti</strong>, it is also aserious problem <strong>in</strong> more wealthy segments of <strong>the</strong> society:“Poor, mostly rural families send <strong>the</strong>ir children <strong>to</strong> cities <strong>to</strong> live withwealthier families whom <strong>the</strong>y th<strong>in</strong>k will provide <strong>the</strong> children with food,shelter and an education, <strong>in</strong> exchange for some work. Sadly, <strong>the</strong> parents’dream is often a nightmare for <strong>the</strong>se children known as restaveks. ...Sixty-fivepercent of <strong>the</strong> victims are girls between <strong>the</strong> ages of six and fourteen.They work excessive hours, receive little or no school<strong>in</strong>g, are unpaid andare often physically and sexually abused” (Cde Baca <strong>2010</strong>).The importance of address<strong>in</strong>g gender-based violence <strong>in</strong> time of disaster was acknowledgeddur<strong>in</strong>g <strong>the</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> cyclones of 2008. The Inter-Agency Stand<strong>in</strong>g Committeeissued a three-page summary of <strong>the</strong> <strong>in</strong>formation available on gender-basedviolence prior <strong>to</strong> <strong>the</strong> <strong>earthquake</strong>. 156168156 Produced on 29 <strong>January</strong> <strong>2010</strong> by <strong>the</strong> IASC Sub-work<strong>in</strong>g Group on Gender <strong>in</strong> Humanitarian Action. http://gender.one<strong>response</strong>.<strong>in</strong>fo.
Annex2Chronologyof eventsfollow<strong>in</strong>g <strong>the</strong><strong>Haiti</strong> <strong>earthquake</strong>The chronology of <strong>the</strong> 90 days follow<strong>in</strong>g <strong>the</strong> 12 <strong>January</strong> <strong>2010</strong> <strong>earthquake</strong> providesvaluable <strong>in</strong>formation about <strong>the</strong> events and <strong>the</strong>ir sequence.This cha<strong>in</strong> of events re<strong>in</strong>forces <strong>the</strong> concept that while hazards such as <strong>earthquake</strong>s cantrigger a crisis, <strong>the</strong> disasters <strong>the</strong>mselves are not natural but ra<strong>the</strong>r <strong>the</strong> result of a seriesof human actions.This annex collects <strong>the</strong> ma<strong>in</strong> facts recorded <strong>in</strong> one of <strong>the</strong> few reports available from <strong>the</strong>day of <strong>the</strong> quake, known as <strong>the</strong> <strong>Haiti</strong> Earthquake Situation Report (Sitrep), preparedby <strong>the</strong> United Nations Office for <strong>the</strong> Coord<strong>in</strong>ation of Humanitarian Affairs (OCHA),with support from national and <strong>in</strong>ternational agencies and NGOs. The review covers<strong>the</strong> first 33 Sitreps, from 12 <strong>January</strong> <strong>to</strong> 12 April <strong>2010</strong>.The chronology is organized around four issues:1. Security and access2. Official figures issued by <strong>the</strong> Government of <strong>Haiti</strong>3. Emergency management4. <strong>Health</strong> situation169
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Date Security and access Official figures Emergency management actions <strong>Health</strong> status12 Jan<strong>2010</strong>Day 113 JanDay 214 JanDay 315 JanDay 4Earthquake M. 7.0 occurredat 4:53pm localtime.[1] Tsunami struck <strong>the</strong>coast 5 m<strong>in</strong>utes after <strong>the</strong><strong>earthquake</strong>. Calculatedspeed of <strong>the</strong> tidal wave336Km/h.[2] At 6:45pm <strong>the</strong>tsunami watch is cancelled.[3] Caribbean CatastropheRisk Insurance Facility(CCRIF) <strong>to</strong> make <strong>the</strong> f<strong>in</strong>alcalculation and payout <strong>to</strong><strong>Haiti</strong> after 14 days. [4]The airport <strong>in</strong> PaP isreportedly operational,under control of <strong>the</strong> U.S.troops, and only open forhumanitarian air flights.Roads <strong>to</strong> <strong>the</strong> capital arepartly blocked. The UNHeadquarters at <strong>the</strong> Chris<strong>to</strong>pherHotel collapsed <strong>in</strong><strong>the</strong> <strong>earthquake</strong>. [6]“The airport is operationalfor humanitarian andmilitary flights. Air TrafficControl is respond<strong>in</strong>g <strong>to</strong><strong>in</strong>com<strong>in</strong>g aircraft, but withlimited capabilities. Thereis very limited aircraft-handl<strong>in</strong>gcapacity.” “The port isnot operational.” [7]“Operations are heavilyconstra<strong>in</strong>ed due <strong>to</strong> <strong>the</strong> lackof fuel, transport, communicationsand handl<strong>in</strong>gcapacity at <strong>the</strong> airport.Some flights are be<strong>in</strong>gre-routed through San<strong>to</strong>Dom<strong>in</strong>go airport, which isalso becom<strong>in</strong>g congested.”“The port rema<strong>in</strong>s nonoperational.”[8]There are no officialreports.There are no officialreports.“The Governmentis sett<strong>in</strong>g up an operationssite close<strong>to</strong> <strong>the</strong> airport.” [7.]There were no officialreports.OCHA releases <strong>the</strong> Earthquake SituationReport #1: The capital of <strong>Haiti</strong>, Port-au-Pr<strong>in</strong>ce(PaP), has been severely affected <strong>in</strong>clud<strong>in</strong>gcritical city <strong>in</strong>frastructure components suchas electricity, water and phone services.Electricity is not available and communicationsare difficult. At this stage <strong>the</strong>re is verylimited access because of debris and o<strong>the</strong>robstacles on <strong>the</strong> roads. The airport of PaP isreported <strong>to</strong> be closed. The Presidential Palaceand Government build<strong>in</strong>gs are reported <strong>to</strong>have been seriously damaged. Accord<strong>in</strong>g<strong>to</strong> prelim<strong>in</strong>ary reports, several UN as well aso<strong>the</strong>r national build<strong>in</strong>gs have collapsed orhave been damaged. Populations may also beaffected <strong>in</strong> Carrefour and Jacmel. There are noimpact figures nor estimates. [5]Situation Report #2: “The number of people<strong>in</strong> need of humanitarian assistance will not bedeterm<strong>in</strong>ed until <strong>the</strong> extent of <strong>the</strong> damageis known. The death <strong>to</strong>ll is unknown but isexpected <strong>to</strong> be high.” “S&R teams are arriv<strong>in</strong>gfrom Guadeloupe, <strong>the</strong> Dom<strong>in</strong>ican Republicand <strong>the</strong> United States. They are be<strong>in</strong>g deployed<strong>to</strong> major public build<strong>in</strong>gs, hotels andhospitals.” [6]Situation Report #3: “A helicopter assessmentby <strong>the</strong> UN Mission . . . found some areas with50 percent destruction or serious damage,with many build<strong>in</strong>gs completely collapsed.PaP and o<strong>the</strong>r urban centres, such as Jacmeland Carrefour, are affected.” “The death <strong>to</strong>llrema<strong>in</strong>s unknown.” “There is no water supply.”“Communications are down and <strong>the</strong>re is noelectricity.” [7]Situation Report #4: “Identification of bodiesrema<strong>in</strong>s a problem, <strong>in</strong> conjunction withassign<strong>in</strong>g responsibility for <strong>the</strong> recovery ofbodies. The Government is identify<strong>in</strong>g variousgrave sites. No reliable figures are available on<strong>the</strong> extent of fatalities.” “Phone communicationrema<strong>in</strong>s difficult <strong>in</strong> most of <strong>the</strong> capital.However, text messages are gett<strong>in</strong>g through.Internet connections are possible <strong>in</strong> some areas,but constant access rema<strong>in</strong>s difficult.” [8]Initial reports <strong>in</strong>dicate alarge number of casualtiesand widespread damagewith an urgent need forSearch and Rescue (S&R). [5]“The hospital <strong>in</strong> Petionville,a hillside PaP district,is destroyed and mos<strong>to</strong>f <strong>the</strong> medical centreshave collapsed.” “MSF hasreported treat<strong>in</strong>g about600 people <strong>in</strong> <strong>the</strong> affectedarea and is look<strong>in</strong>g atsend<strong>in</strong>g additional medicalsupplies.” [6]The <strong>Health</strong> Cluster is ledby <strong>the</strong> World <strong>Health</strong> Organization(WHO). Most of<strong>the</strong> health resources andsupplies need <strong>to</strong> go <strong>to</strong> <strong>the</strong>Dom<strong>in</strong>ican Republic and<strong>the</strong>n by land <strong>to</strong> <strong>Haiti</strong>. [7]“The Pan American <strong>Health</strong>Organization (PAHO/WHO) is establish<strong>in</strong>g afield office <strong>in</strong> Jimaní (Dom<strong>in</strong>icanRepublic) <strong>to</strong> serveas a permanent bridgebetween this border cityand <strong>to</strong> PaP (approximatelya 90-m<strong>in</strong>ute journey).The office will be a stag<strong>in</strong>g/transferpo<strong>in</strong>t foremergency humanitariansupplies and personnelneeded <strong>in</strong> <strong>the</strong> <strong>Haiti</strong><strong>response</strong> operation.” [8]170
CHRONOLOGY OF EVENTS FOLLOWING THE HAITI EARTHQUAKE - Annex 2Date Security and access Official figures Emergency management actions <strong>Health</strong> status16 JanDay 517 JanDay 618 JanDay 719 JanDay 8“The limited capacity of<strong>the</strong> airport comb<strong>in</strong>ed withheavy and unplanned airtraffic rema<strong>in</strong>s a challenge,result<strong>in</strong>g <strong>in</strong> many flightsbe<strong>in</strong>g de<strong>to</strong>ured and delayed.. . . However lack oftransport and fuel rema<strong>in</strong> aproblem mak<strong>in</strong>g it difficult<strong>to</strong> move goods <strong>to</strong> o<strong>the</strong>rlocations. With no s<strong>to</strong>ragefacility, <strong>the</strong> airport is nowpacked with goods andteams. Safety and securityrema<strong>in</strong>s an important concern.”“PaP seaport is stillnon-operational.”[9]“The PaP airport is heavilycongested. . . . Fuel rema<strong>in</strong>san issue for humanitarianoperations. . . The portrema<strong>in</strong>s unusable.” [10]“MINUSTAH reports that<strong>the</strong> overall security situation<strong>in</strong> PaP rema<strong>in</strong>s stable,with limited, localizedviolence and loot<strong>in</strong>g occurr<strong>in</strong>g.”“Twenty-six countries,<strong>in</strong>clud<strong>in</strong>g Argent<strong>in</strong>a,Canada, France, Russia and<strong>the</strong> USA, have providedsignificant military assets<strong>to</strong>wards <strong>the</strong> emergency<strong>response</strong>. These assets<strong>in</strong>cluded field hospitals,troops, military aircraft,hospital ships, cargo shipsand helicopters. MINUS-TAH currently has 3,400troops and police on <strong>the</strong>ground.”[11]“Despite logistical andsecurity constra<strong>in</strong>ts, <strong>the</strong> affectedpopulation is receiv<strong>in</strong>gan <strong>in</strong>creas<strong>in</strong>g numberof relief supplies, <strong>in</strong>clud<strong>in</strong>gmedical assistance, food,water and shelter.” [12]“The M<strong>in</strong>istry ofInterior estimatesthat one millionpeople have beenseverely affectedby <strong>the</strong> <strong>earthquake</strong>and that 250,000are <strong>in</strong> urgent needof assistance.Authorities believethat 50,000 peoplehave died, but sofar 13,000 bodieshave been accountedfor.” [9]“The Governmenthas fur<strong>the</strong>radvised severelyaffected populations<strong>to</strong> leave <strong>the</strong>city if <strong>the</strong>y havefamily or friends<strong>in</strong> non-affectedareas. To this end, itprovided cash andfuel <strong>to</strong> a transportcompany <strong>to</strong> providefree transport.. . . thousands ofdisplaced are leav<strong>in</strong>gPaP for ruralareas.” [11]“The Governmenthas devised eightzones for <strong>the</strong> distributionof humanitarianassistance. Ama<strong>in</strong> concern for<strong>the</strong> Governmentcont<strong>in</strong>ues <strong>to</strong> be<strong>the</strong> revitalizationof economic activities.”[12]Situation Report #5: “There have been 58 liverescues so far by <strong>the</strong>se teams (Search & RescueInternational Teams). . . . Approximately60% of <strong>the</strong> worst affected areas of PaP andsurround<strong>in</strong>g communities have been covered.”[9] The major constra<strong>in</strong>ts for <strong>the</strong> USARoperation are security, transport, communicationsand fuel.Situation Report #6: “S&R teams extracted 13live rescues on 16 <strong>January</strong> br<strong>in</strong>g<strong>in</strong>g <strong>the</strong> <strong>to</strong>talnumber of lives saved by <strong>the</strong>se teams <strong>to</strong> 71.” [10]Situation Report #7: “Urban Search-and-Rescue teams have saved 90 lives. Two morelive rescues were reported on 18 <strong>January</strong>.”“An <strong>in</strong>itial assessment by <strong>the</strong> United NationsEnvironment Programme, from 13 <strong>to</strong> 17 <strong>January</strong>,<strong>in</strong>dicated no major acute environmentalemergencies, but enormous issues for <strong>the</strong>anticipated recovery phase. The most urgentissues <strong>in</strong>clude waste management, medicalwaste, disposal of corpses and disposal ofdemolition material.” [11]Situation Report #8 “The revised <strong>to</strong>tal of livessaved by <strong>in</strong>ternational search-and-rescueteams is over 121 people. . . At <strong>the</strong> peak of <strong>the</strong>search-and-rescue effort, <strong>the</strong>re were 52 teamson <strong>the</strong> ground with 1,820 rescue workers and175 dogs.” “Water distribution has been constra<strong>in</strong>edby limited fuel supplies. Distributionwas planned for 176 distribution po<strong>in</strong>ts on 19<strong>January</strong>.” [12]“WHO/PAHO estimatesthat <strong>the</strong> number of deadranges between 40,000and 50,000 people. A massburial of 3,000 bodieswas reported yesterday.. . .(In PaP) at least eighthospitals and/or healthcentres have collapsed orsusta<strong>in</strong>ed serious damage.…At least five hospitalsare function<strong>in</strong>g. “[9] Adialysis center with 8 unitswas operational.“The <strong>Health</strong> Cluster (21organizations lead byWHO) reports that sevenfield hospitals have arrivedand three are fullyoperational. . . Handl<strong>in</strong>g ofdead bodies rema<strong>in</strong>s anissue.” [10]“All hospitals with<strong>in</strong> <strong>the</strong>PaP area are overwhelmedwith <strong>in</strong>com<strong>in</strong>g patients.Many fracture cases needurgent surgical <strong>in</strong>terventiondue <strong>to</strong> extendedperiods without care.”“Major gaps <strong>in</strong>clude surgicalcapacity, follow-up ofsurgical patients, maternitycare, and coverageof areas of populationdisplacements. . . . PAHO/WHO is coord<strong>in</strong>at<strong>in</strong>g <strong>the</strong>health sec<strong>to</strong>r <strong>response</strong>from operation bases <strong>in</strong>PaP and San<strong>to</strong> Dom<strong>in</strong>go.An operations centreis also be<strong>in</strong>g set up <strong>in</strong>Jimaní, <strong>in</strong> <strong>the</strong> Dom<strong>in</strong>icanRepublic.” [11]<strong>Haiti</strong> has “49 hospitalsnationwide . . . <strong>in</strong>clud<strong>in</strong>g11 hospitals <strong>in</strong> PaP. Eighthospitals and health-carefacilities <strong>in</strong> and aroundPaP are damaged.” “TheM<strong>in</strong>ister of Interior hasstarted spray<strong>in</strong>g causticsoda over bodies andbuild<strong>in</strong>gs where bodieshave still not been recovered.”“The provision ofwater <strong>to</strong> hospitals, ga<strong>the</strong>r<strong>in</strong>gsites and commonareas are <strong>the</strong> priorities fordistribution.” [12]171
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Date Security and access Official figures Emergency management actions <strong>Health</strong> status20 JanDay 921 JanDay 1022 JanDay 1123 JanDay 12The PaP airport reportsabout 150 planes are land<strong>in</strong>gdaily. F<strong>in</strong>d<strong>in</strong>g free slotsfor large aircraft is still achallenge. [13]“The road from <strong>the</strong> Dom<strong>in</strong>icanRepublic rema<strong>in</strong>s<strong>the</strong> best option for <strong>the</strong>majority of <strong>in</strong>com<strong>in</strong>gcargo.” “The PaP port isfunctional.” “The securitysituation <strong>in</strong> PaP rema<strong>in</strong>sstable although <strong>the</strong>re areisolated cases of loot<strong>in</strong>gand violence. MINUSTAHcurrently requires militaryescorts for <strong>the</strong> delivery ofaid by UN agencies.” [14]“The security situationrema<strong>in</strong>s stable but <strong>the</strong> potentialfor unrest rema<strong>in</strong>s.There is concern that<strong>in</strong> some Port-au-Pr<strong>in</strong>ceneighborhoods (Belair,Martissant and Cité Soleil),formerly <strong>in</strong>carceratedcrim<strong>in</strong>als have returnedand are attempt<strong>in</strong>g <strong>to</strong>reconstitute gangs.”[15]“DPC hasestimated that<strong>the</strong> <strong>earthquake</strong>resulted <strong>in</strong> 75,000persons killed,200,000 <strong>in</strong>juredand one milliondisplaced. “[13]“As of 22 <strong>January</strong>,<strong>the</strong> Governmenthas accounted for111,481 confirmeddeaths <strong>in</strong> four departments(SouthEast, West, Nippesand West).” [15]Situation Report #9: “IOM estimates that <strong>the</strong>reare more than 300 makeshift settlementsscattered throughout <strong>the</strong> city, with an estimated370,000 people liv<strong>in</strong>g under improvisedshelter with no access <strong>to</strong> water supplies,accord<strong>in</strong>g <strong>to</strong> recent assessments.” [13]Situation Report #10: “The [UN] cluster estimatesthat <strong>the</strong> number of displaced peopleis between 500,000 and 700,000 (currentplann<strong>in</strong>g figure). . . .Of <strong>the</strong> 508 makeshiftsites identified by <strong>the</strong> Government, some 350have been assessed (68%) by cluster partners.These 350 sites currently accommodatearound 472,000 people and only six sites haveaccess <strong>to</strong> water sources. A new 400-personsite was established on 21 <strong>January</strong> <strong>in</strong> Delmas.”[14]Situation Report #11: "The Government hasdeclared <strong>the</strong> S&R phase over. There were 132live rescues by <strong>in</strong>ternational S&R teams." "Sofar, more than 130,000 people have beenassisted. . . with transportation <strong>to</strong> leave <strong>the</strong>city, accord<strong>in</strong>g <strong>to</strong> DPC." Artibonite departmenthas received 50,573 people; North Westdepartment 30,000; Centre department;20,530; North department 12,500; GrandeAnse 9,000; and South department 9,000. The<strong>to</strong>tal number of people leav<strong>in</strong>g PaP by privatemeans rema<strong>in</strong>s undeterm<strong>in</strong>ed.”[15]“Assessments of hospitalfacilities will cont<strong>in</strong>ue <strong>to</strong>look at hospital <strong>in</strong>frastructure,referral systems and<strong>the</strong> organization of transportationof patients.” “Asof 19 <strong>January</strong>, <strong>the</strong> WASHCluster has established 82distribution sites for water,and has 180 water truckswith a <strong>to</strong>tal capacity <strong>to</strong>provide water <strong>to</strong> 180,000people.” [13]“PROMESS, <strong>the</strong> ma<strong>in</strong>medical s<strong>to</strong>rage anddistribution facility managedby PAHO/WHO,is provid<strong>in</strong>g medic<strong>in</strong>esand medical supplies forfree <strong>to</strong> 50 organizationswork<strong>in</strong>g <strong>in</strong> hospitals andcl<strong>in</strong>ics. The supplies havebeen offered s<strong>in</strong>ce 13<strong>January</strong> and each day<strong>the</strong> number of requests<strong>in</strong>creases.” The removalof medical waste fromhospitals and whereverhealth care is provided is achallenge. [14]Currently <strong>the</strong>re are 40function<strong>in</strong>g health facilities<strong>in</strong> PaP, 8 of which arefield hospitals. Urgentsurgical <strong>in</strong>terventions aredecreas<strong>in</strong>g and <strong>the</strong> followupof <strong>the</strong> post-surgicalpatients is a problem thatneeds <strong>to</strong> be solved. Informationmanagement is achallenge for all clusters/sec<strong>to</strong>rs. [1] "At present,<strong>Haiti</strong>’s immunizationprogram is not function<strong>in</strong>gand tetanus is <strong>the</strong>disease of most immediateconcern, accord<strong>in</strong>g <strong>to</strong>WHO." [15]Improved waste management(solid and healthcare) is tak<strong>in</strong>g place <strong>in</strong>hospitals, <strong>in</strong>clud<strong>in</strong>g <strong>the</strong>appropriate disposal ofamputated body parts. [2]172
CHRONOLOGY OF EVENTS FOLLOWING THE HAITI EARTHQUAKE - Annex 2Date Security and access Official figures Emergency management actions <strong>Health</strong> status24 JanDay 1325 JanDay 1427 Jan-Day 1628 JanDay 1729 JanDay 18The security situation <strong>in</strong>PaP rema<strong>in</strong>s stable but<strong>the</strong>re have been isolated<strong>in</strong>stances of loot<strong>in</strong>g and arecent <strong>in</strong>cident where MI-NUSTAH troops fired warn<strong>in</strong>gshots and used teargas. “More and more policeofficers are report<strong>in</strong>g forduty, <strong>in</strong>creas<strong>in</strong>g capacity<strong>to</strong> an estimated 60-70percent of pre-<strong>earthquake</strong>levels <strong>in</strong> PaP.” [17]Commercial activities haveresumed <strong>in</strong> many parts of<strong>the</strong> country. The securitysituation <strong>in</strong> PaP and o<strong>the</strong>raffected areas rema<strong>in</strong>sstable. Military escorts arerequired for UN relief distributions.[18]"The port has beendeclared unsafe for <strong>in</strong>com<strong>in</strong>gships. PaP airport isoperat<strong>in</strong>g at peak capacitywith an average of 120<strong>in</strong>com<strong>in</strong>g flights per day.""While <strong>the</strong> overall securitysituation <strong>in</strong> PaP rema<strong>in</strong>sstable, crowd control at aiddistribution po<strong>in</strong>ts.” [19]"The Governmentestimates <strong>the</strong>death <strong>to</strong>ll from<strong>the</strong> 12 <strong>January</strong><strong>earthquake</strong> at112,250 deathsand 194,000 <strong>in</strong>jured.The numberof people <strong>in</strong> needof shelter rangesfrom 800,000 <strong>to</strong>one million."[16]The M<strong>in</strong>isterialConference on<strong>Haiti</strong> <strong>to</strong>ok place<strong>in</strong> Montreal on 25<strong>January</strong>.“The Governmentis report<strong>in</strong>g that112,392 havedied and 196,501people havebeen <strong>in</strong>jured by<strong>the</strong> <strong>earthquake</strong>.The number ofdisplaced peopleranges from800,000 <strong>to</strong> onemillion.”[18]Situation Report #12: "The Governmentestimates that 235,000 people have left PaPus<strong>in</strong>g <strong>the</strong> free transportation be<strong>in</strong>g providedby <strong>the</strong> Government." "Water cont<strong>in</strong>ues <strong>to</strong> bedistributed daily at 115 sites <strong>in</strong> PaP reach<strong>in</strong>gan estimated 235,000 people." [16]Situation Report #13: “The distribution of assistancecont<strong>in</strong>ues <strong>in</strong> PaP and o<strong>the</strong>r affectedareas such as Jacmel, Carrefour, Léogâne andPetit Goâve. Tents, food, health (post-operativecare and epidemiological surveillance),sanitation and hygiene are <strong>the</strong> priorities forassistance.”[17]Situation Report #14: “An <strong>in</strong>crease <strong>in</strong> commodityprices has been reported fur<strong>the</strong>r<strong>in</strong>creas<strong>in</strong>g <strong>the</strong> number of people who aredependent on humanitarian assistance. . . .Cash-for-work and cash-for-food programmesare start<strong>in</strong>g <strong>to</strong> be used <strong>to</strong> engage <strong>Haiti</strong>ans <strong>in</strong><strong>the</strong> recovery effort and <strong>to</strong> help stimulate <strong>the</strong>local economy. . . . All schools rema<strong>in</strong> closedbut schools <strong>in</strong> non-affected departments willreopen on 1 February.” [18]<strong>Health</strong> report <strong>in</strong>dicates people with <strong>in</strong>jurieshave received medical attention, even thoughsome require surgical care.Situation Report #15: "As of 28 <strong>January</strong>, <strong>the</strong>Government reported that more than 341,000persons have departed PaP for locationsoutside <strong>the</strong> capital. . . . Over a third of <strong>the</strong> <strong>to</strong>tal– some 133,000 <strong>in</strong>dividuals – have arrived <strong>in</strong>Artibonite department." [19]"43 hospitals are function<strong>in</strong>g<strong>in</strong> <strong>the</strong> PaP area, 12field hospitals (half ofwhich are military hospitals)and two hospitalships (US and Mexico).There is a need for more<strong>in</strong>formation from areasoutside of PaP. . . Importantchallenges rema<strong>in</strong>especially <strong>in</strong> <strong>the</strong> areas ofpost-operative care and<strong>the</strong> adaptation of thousandsof people who havelost limbs. . . No reportedoutbreaks of communicablediseases." [16]“The M<strong>in</strong>istry of <strong>Health</strong> of<strong>the</strong> Dom<strong>in</strong>ican Republicestimates that as of 22<strong>January</strong>, 495 <strong>Haiti</strong>anpatients are <strong>in</strong> n<strong>in</strong>e hospitals<strong>in</strong> <strong>the</strong> Dom<strong>in</strong>icanRepublic. The majority(247 people) are <strong>in</strong> <strong>the</strong>Buen Samaritano Hospital<strong>in</strong> Jimaní. The <strong>in</strong>flux of patientsrequir<strong>in</strong>g emergencycare <strong>in</strong> <strong>the</strong>se hospitalsis decl<strong>in</strong><strong>in</strong>g.” [17]Cases of tetanus and suspectedcases of measleshave been reported <strong>in</strong>Léogâne . A vacc<strong>in</strong>ationcampaign aga<strong>in</strong>st diph<strong>the</strong>riaand tetanus, DTTand measles will beg<strong>in</strong>on February 2. Water isreach<strong>in</strong>g 308,000 peoplethrough 133 distributionpo<strong>in</strong>ts <strong>in</strong> PaP. The coverage<strong>in</strong> Léogâne and Jacmelhas been expandedalso. Additional boreholesand new contrac<strong>to</strong>rsare be<strong>in</strong>g identified <strong>to</strong><strong>in</strong>crease production anddistribution capacity. [18]Turn<strong>in</strong>g po<strong>in</strong>t between<strong>the</strong> life-sav<strong>in</strong>g and <strong>the</strong>post-operative carephases."Several organizationshave reported cases oftetanus and chicken pox.An isolated case of typhoidhas been reported.…In terms of medicalsupplies, crutches and x-ray equipment are <strong>in</strong> shortsupply and specialists <strong>in</strong>orthopedic and <strong>in</strong>ternalmedic<strong>in</strong>e are <strong>in</strong> highdemand, accord<strong>in</strong>g <strong>to</strong> <strong>the</strong>Cluster." [19]173
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Date Security and access Official figures Emergency management actions <strong>Health</strong> status1 FebDay 213 FebDay 235 FebDay 25“The PaP airport is handl<strong>in</strong>gapproximately 120-150 planes per day. . . . Theoverall security situationacross <strong>the</strong> country rema<strong>in</strong>sstable but potentiallyvolatile.”[20]"Grow<strong>in</strong>g gang rivalriesrema<strong>in</strong> a concern <strong>in</strong> PaP.UNPOL and HNP cont<strong>in</strong>ue<strong>to</strong> ma<strong>in</strong>ta<strong>in</strong> <strong>in</strong>creasedpatrols <strong>in</strong> Cité Soleil andMarché de Fer. The Governmentdecided <strong>to</strong> extend<strong>the</strong> state of emergencywhich was due <strong>to</strong> expireon 1 February for a fur<strong>the</strong>rtwo weeks." [22]"Some 80 <strong>to</strong> 90 flights perday are land<strong>in</strong>g at PaPairport, down from <strong>the</strong>peak of 120-150 flightsper day." "Cont<strong>in</strong>gencyplann<strong>in</strong>g is underway <strong>to</strong>prepare for <strong>the</strong> upcom<strong>in</strong>gra<strong>in</strong>y season, tak<strong>in</strong>g <strong>in</strong><strong>to</strong>consideration displacedpopulations and logisticshortcom<strong>in</strong>gs." [23]Prime M<strong>in</strong>istersays, "as angry protestsover <strong>the</strong> slowarrival of aid flaredon <strong>the</strong> rubblestrewnstreets,"<strong>to</strong> <strong>the</strong> AgenceFrance-Presse(AFP): "There aremore than 200,000people who havebeen clearly identifiedas people whoare dead," samereport <strong>in</strong>dicates“aid agencies havesounded <strong>the</strong> alarmthat donations for<strong>Haiti</strong> relief havebeen desperatelylow compared<strong>to</strong> after <strong>the</strong> 2004Asian tsunami,which had a death<strong>to</strong>ll of about220,000.” [21]"The DPC isverify<strong>in</strong>g <strong>the</strong> latestfigures for deadand <strong>in</strong>jured (Declaredby <strong>the</strong> PrimeM<strong>in</strong>ister on Feb 3)but has not issuedan official updates<strong>in</strong>ce 28 <strong>January</strong>when it reportedthat 112,405 haddied and 196,595were <strong>in</strong>jured." [23]Situation Report #16: “The Government hasrevised <strong>the</strong> number of people leav<strong>in</strong>g PaP foroutly<strong>in</strong>g departments <strong>to</strong> 482,349 people, asof 31 <strong>January</strong>. “[20]“Situation Report # 17: Sanitation is becom<strong>in</strong>ga major concern at many of <strong>the</strong> temporarysites. . . . The WFP food surge cont<strong>in</strong>ues. Some1 million people have been reached s<strong>in</strong>ce <strong>the</strong>onset of <strong>the</strong> emergency; 338,000 people havereceived two-week rations of rice over <strong>the</strong>past 3 days.” [22]Situation Report #18: "Seven organized settlementshave been established for 42,000 displacedpeople; some 460,000 people rema<strong>in</strong><strong>in</strong> 315 spontaneous settlements throughoutPaP, accord<strong>in</strong>g <strong>to</strong> IOM." [23]“The need for <strong>the</strong> establishmen<strong>to</strong>f post-operativecare facilities and mobilecl<strong>in</strong>ics persists. Due <strong>to</strong> <strong>the</strong>large numbers of patientswho are now homeless,hospitals are challengedwith where <strong>to</strong> dischargepatients. In collaborationwith <strong>the</strong> regional wastehaul<strong>in</strong>gauthority, PAHO/WHO has set up a collectionsystem <strong>to</strong> removemedical waste <strong>in</strong> all hospitalsand dispose <strong>the</strong>m <strong>in</strong>safe and organized landfillsites.” [20]“<strong>Health</strong> Cluster partnershave recorded over 1,000amputations <strong>in</strong> PaP. Thereare also reports that some50 people have beenparalyzed from sp<strong>in</strong>al cord<strong>in</strong>juries.” “Medical wastemanagement servicesare reportedly only be<strong>in</strong>gused by two hospitals<strong>in</strong> PaP. Some hospitalsappear <strong>to</strong> be send<strong>in</strong>gwaste on <strong>the</strong>ir own <strong>to</strong><strong>the</strong> landfill site.” “Manymedical supplies are still<strong>in</strong> large conta<strong>in</strong>ers <strong>in</strong> PaPand need <strong>to</strong> be sorted andprioritized. This processis caus<strong>in</strong>g some delays <strong>in</strong>gett<strong>in</strong>g supplies distributed.”[22]"Sanitation and vec<strong>to</strong>rcontrol is becom<strong>in</strong>g amajor concern. . . ." ". . .no notification of eventswith epidemic potential,accord<strong>in</strong>g <strong>to</strong> PAHO/WHO.Disease surveillancecont<strong>in</strong>ues. There are 52government-def<strong>in</strong>edsent<strong>in</strong>el sites, 12 ofwhich are located <strong>in</strong> <strong>the</strong>metropolitan PaP area.Investigations are alsobe<strong>in</strong>g conducted by threemobile teams from <strong>the</strong>M<strong>in</strong>istry of <strong>Health</strong>, <strong>the</strong> USCenters for Disease Controland PAHO/WHO." [23]174
CHRONOLOGY OF EVENTS FOLLOWING THE HAITI EARTHQUAKE - Annex 2Date Security and access Official figures Emergency management actions <strong>Health</strong> status8 FebDay 2811 FebDay 3116 FebDay 3619 FebDay 3922 FebDay 42“The security situationrema<strong>in</strong>s unchanged but<strong>the</strong>re is grow<strong>in</strong>g concernover potential restivenessand crime prompted byshortages of shelter, jobsand sanitation.” [24]“Commercial cargo flightshave started arriv<strong>in</strong>g atPaP airport.” “The securitysituation throughout <strong>the</strong>country rema<strong>in</strong>s stabledespite <strong>in</strong>creased reportsof isolated <strong>in</strong>cidents.”[25]“The Office of <strong>the</strong> HighCommissioner for HumanRights and <strong>the</strong> UnitedNations High Commissionerfor Refugees arejo<strong>in</strong>tly urg<strong>in</strong>g countries<strong>to</strong> suspend all <strong>in</strong>voluntaryreturns <strong>to</strong> <strong>Haiti</strong> due <strong>to</strong> <strong>the</strong>cont<strong>in</strong>u<strong>in</strong>g humanitariancrisis. They have called onall countries <strong>to</strong> cont<strong>in</strong>uegrant<strong>in</strong>g <strong>in</strong>terim protectionmeasures on humanitariangrounds until suchtime as people can returnsafely and susta<strong>in</strong>ably.” [26]“The security situationrema<strong>in</strong>s stable, and whilesome demonstrationshave taken place <strong>in</strong> PaPover <strong>the</strong> last days, nomajor <strong>in</strong>cidents have beenreported.” [27]"Security <strong>in</strong> displacementsites, especially <strong>in</strong> largesettlements, cont<strong>in</strong>ues <strong>to</strong>be a concern and requiresa more permanent policepresence." [28]“As of 15 February,<strong>the</strong> nationalCivil ProtectionAgency estimatesthat 217,366people died from<strong>the</strong> 12 <strong>January</strong><strong>earthquake</strong>, an<strong>in</strong>crease of 5,000people s<strong>in</strong>ce <strong>the</strong>last estimateswere released on 6February.” [26]"DPC estimatesthat 222,517 peopledied follow<strong>in</strong>g<strong>the</strong> 12 <strong>January</strong><strong>earthquake</strong>, an<strong>in</strong>crease of 5,000people s<strong>in</strong>ce <strong>the</strong>last estimates werereleased on 15February." [28]Situation Report #19: “Cont<strong>in</strong>gency plann<strong>in</strong>gis underway <strong>to</strong> prepare for <strong>the</strong> upcom<strong>in</strong>gra<strong>in</strong>y season, tak<strong>in</strong>g <strong>in</strong><strong>to</strong> considerationdisplaced populations and logistic shortcom<strong>in</strong>gs.”[24]Situation Report #20: “The Governmentreported that 211 live rescues were achievedby <strong>in</strong>ternational and national S&R teams asof 9 February. A <strong>to</strong>tal of 139 live rescues werecarried out by <strong>in</strong>ternational teams and 72 bynational teams.”[25]Situation Report #21: “Provision of shelter andcamp coord<strong>in</strong>ation cont<strong>in</strong>ue <strong>to</strong> be challeng<strong>in</strong>g,<strong>in</strong>clud<strong>in</strong>g <strong>the</strong> need for debris removaland <strong>the</strong> identification of land for settlements.There is an urgent need <strong>to</strong> create adequatesanitation conditions for displaced populations,especially <strong>in</strong> congested settlementsites.” [26]Situation Report #22: “The Post-DisasterNeeds Assessment (PDNA), <strong>to</strong> be carried outby <strong>the</strong> Government of <strong>Haiti</strong> and supportedby development partners . . . was officiallylaunched <strong>in</strong> PaP on 18 February. Focus<strong>in</strong>g onkey areas of <strong>the</strong> early recovery phase (sanitation,food security, water, debris managementand removal and transitional shelter). . . .” [27]Situation Report #23: ''The number of peoplewho have left PaP for outly<strong>in</strong>g departmentshas <strong>in</strong>creased <strong>to</strong> 597,801 people from <strong>the</strong> previousfigure of 511,405. An estimated 160,000persons have come from PaP <strong>to</strong> <strong>the</strong> borderarea with <strong>the</strong> Dom<strong>in</strong>ican Republic." [28]Safe dr<strong>in</strong>k<strong>in</strong>g water (5litres per person perday) is provided <strong>to</strong> over780,000 people throughwater tanker<strong>in</strong>g and watertreatment plants at 300sites across Port au Pr<strong>in</strong>ce,Léogâne , and Jacmel. [24]There is a decl<strong>in</strong>e <strong>in</strong>trauma <strong>in</strong>juries requir<strong>in</strong>gtreatment but <strong>the</strong> needfor overall medical careis ris<strong>in</strong>g. The M<strong>in</strong>istry of<strong>Health</strong>’s surveillance systemreports acute respira<strong>to</strong>ry<strong>in</strong>fections as <strong>the</strong> ma<strong>in</strong>cause of morbidity. [25]“There are currently 396health NGOs registered <strong>in</strong><strong>Haiti</strong>, however, many of<strong>the</strong>m are due <strong>to</strong> depart<strong>the</strong> country <strong>in</strong> <strong>the</strong> com<strong>in</strong>gweeks, without sufficientnew capacity planned <strong>to</strong>arrive.” “There is a risk ofa large-scale outbreakof diarrhea, given <strong>the</strong>present overcrowd<strong>in</strong>g,poor sanitation and lackof effective waste disposalsystems <strong>in</strong> spontaneoussettlement sites.” [27]"There has been an<strong>in</strong>crease <strong>in</strong> allegations ofgender-based violence <strong>in</strong>general terms. Cases arebe<strong>in</strong>g referred <strong>to</strong> healthservices." [28]175
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Date Security and access Official figures Emergency management actions <strong>Health</strong> status25 FebDay 451 MarDay 494 MarDay 529 MarDay 5711 MarDay 5915 MarDay 63"The transition from USMilitary assets <strong>to</strong> commercialhandl<strong>in</strong>g at <strong>the</strong> portand airport is complete.The humanitarian cargovillage at <strong>the</strong> airport isclosed and all offload<strong>in</strong>gis performed by privatelycontracted entities." [30]"Preparation work is start<strong>in</strong>gon two sites, VillagesDes Oranges and Tabarre 2,identified by <strong>the</strong> Governmentfor <strong>the</strong> relocation ofdisplaced persons fromo<strong>the</strong>r high-risk settlementsites." [33]There is an <strong>in</strong>crease <strong>in</strong>reports of Gender-BasedViolence (GBV) cases;MINUSTAH, UNPOL and<strong>the</strong> <strong>Haiti</strong>an National Policehave jo<strong>in</strong>ed forces <strong>to</strong> patrol,moni<strong>to</strong>r and evaluatesecurity issues related <strong>to</strong>GBV and Child Protection<strong>in</strong> IDP camps <strong>in</strong> PaP andLéogâne. [34]The death <strong>to</strong>ll hasrisen <strong>to</strong> 222,570people, an <strong>in</strong>creaseof 53. 1.3 millionpeople live <strong>in</strong>spontaneoussettlement sites.604,215 peoplehave left PaP. [30]"Two months after<strong>the</strong> <strong>earthquake</strong>,official figures fromDPC states that anestimated 222,517people died andano<strong>the</strong>r 310,928were <strong>in</strong>jured." [34]Situation Report #24: "Toge<strong>the</strong>r with <strong>the</strong>decongestion of spontaneous settlementsites, creat<strong>in</strong>g adequate sanitaryconditions will be crucial <strong>in</strong> order <strong>to</strong>mitigate <strong>the</strong> risk of a large-scale outbreakof waterborne diseases <strong>in</strong> <strong>the</strong> com<strong>in</strong>gweeks." [29]Situation Report #25: "Heavy ra<strong>in</strong>fall<strong>in</strong> Nippes and Sud departments led <strong>to</strong>flood<strong>in</strong>g on 27 February, kill<strong>in</strong>g at least13 people and caus<strong>in</strong>g <strong>the</strong> temporaryevacuation of 3,428 o<strong>the</strong>rs." [30]Situation Report #26: The Governmentand humanitarian ac<strong>to</strong>rs are coord<strong>in</strong>at<strong>in</strong>g<strong>to</strong> determ<strong>in</strong>e humanitarian needs <strong>in</strong>Nippes and Sud departments follow<strong>in</strong>gfloods on 27 February. [31]Situation Report #27: "With <strong>the</strong> early onse<strong>to</strong>f ra<strong>in</strong>s, shelter and sanitation rema<strong>in</strong><strong>the</strong> most urgent priorities; <strong>the</strong> distributionw<strong>in</strong>dow for agricultural <strong>in</strong>puts hasbeen reduced significantly by ra<strong>in</strong> andresult<strong>in</strong>g landslides <strong>in</strong> <strong>the</strong> <strong>earthquake</strong>affectedareas." [32]Situation Report #28: "Two months <strong>in</strong><strong>to</strong><strong>the</strong> humanitarian <strong>response</strong>, more than4.3 million people have received food assistance,1.2 million people are receiv<strong>in</strong>gdaily water distributions, and more than300,000 children and adults have beenvacc<strong>in</strong>ated." [33]Situation Report #29: "As of 15 March,433 sites (<strong>in</strong>clud<strong>in</strong>g spontaneous andtransitional) with a <strong>to</strong>tal population of682,693 <strong>in</strong>dividuals or 132,383 familieshave been identified <strong>in</strong> <strong>the</strong> PaP area andsome communes <strong>in</strong> Jacmel." [34]"Through <strong>the</strong> ongo<strong>in</strong>g vacc<strong>in</strong>ationcampaign <strong>in</strong> temporarysettlements, over 8,000 childrenunder seven years of agehave been vacc<strong>in</strong>ated aga<strong>in</strong>stdiph<strong>the</strong>ria, tetanus and pertussisand over 5,000 aga<strong>in</strong>stmeasles and rubella." [29]"Government figures show asteady rise <strong>in</strong> reported casesof suspected malaria. This is <strong>to</strong>be expected dur<strong>in</strong>g <strong>the</strong> currentseason and consider<strong>in</strong>g<strong>the</strong> conditions of people liv<strong>in</strong>g<strong>in</strong> close quarters <strong>in</strong> <strong>the</strong> spontaneoussettlements." [32]"An estimated 494,600 childrenunder five and 197,840pregnant and lactat<strong>in</strong>gwomen have been affected bythis disaster. All are consideredat risk of malnutrition andneed <strong>to</strong> be targeted <strong>in</strong> blanketsupplementary feed<strong>in</strong>g.""Many trucks deliver<strong>in</strong>g waterare not chlor<strong>in</strong>ated. Reportsfrom primary health providersshow <strong>in</strong>sufficient quantities ofwater for hygiene purposes.Many smaller settlements areunderserved by humanitarianassistance." [33]PAHO/WHO has facilitatedcoord<strong>in</strong>ation of 314 healthpartners <strong>to</strong> aid governmentefforts. Eight cluster subgroupshave been established:health care and mobile cl<strong>in</strong>ics,hospital and trauma care,health <strong>in</strong>formation management,reproductive health,mental health and psychologicalsupport, disabilities, medicalsupplies, early warn<strong>in</strong>g ofcommunicable diseases andreproductive health." [34]176
CHRONOLOGY OF EVENTS FOLLOWING THE HAITI EARTHQUAKE - Annex 2Date Security and access Official figures Emergency management actions <strong>Health</strong> status19 MarDay 6724 MarDay 7231 MarDay 7911 AprDay 90There is an <strong>in</strong>creas<strong>in</strong>gnumber of reports detail<strong>in</strong>gtensions betweendisplaced persons locatedon private land and landowners.Some cases haveresulted <strong>in</strong> forceful evictionsfrom <strong>the</strong> land. [36]“Thereare 460 siteswith a <strong>to</strong>tal populationof 1,170,000<strong>in</strong>dividuals <strong>in</strong>PaP."[35]"The Post-DisasterNeeds Assessmentf<strong>in</strong>d<strong>in</strong>gs reveal that<strong>the</strong> <strong>to</strong>tal value ofdamage and lossescaused by <strong>the</strong> <strong>earthquake</strong>is estimatedat US$7.8 billion(US$4.3 billionrepresents physicaldamage and US$3.5billion are economiclosses). The damageand losses are <strong>the</strong>equivalent of morethan 120% of <strong>the</strong>2009 gross domesticproduct (GDP)." [36]"The InternationalDonors’ ConferenceTowards a New Futurefor <strong>Haiti</strong>, at <strong>the</strong>UN headquarters <strong>in</strong>New York, yieldedmore than US$9billion for <strong>Haiti</strong>’sreconstruction….Ofthis amount, aboutUS$5.3 billion waspledged for <strong>the</strong> next18 months <strong>to</strong> beg<strong>in</strong><strong>Haiti</strong>’s path <strong>to</strong> longtermrecovery."[38]Situation Report #30: “The cont<strong>in</strong>u<strong>in</strong>g <strong>in</strong>crease<strong>in</strong> both <strong>the</strong> number of camps and <strong>the</strong>size of exist<strong>in</strong>g camps is prov<strong>in</strong>g quite challeng<strong>in</strong>gfor implement<strong>in</strong>g agencies. Anecdotalevidence suggests that a percentageof <strong>the</strong>se <strong>in</strong>creases are persons not directlyaffected by <strong>the</strong> <strong>earthquake</strong>." "DPC reports40,000 displaced persons from <strong>earthquake</strong>affectedareas resid<strong>in</strong>g with host families <strong>in</strong><strong>the</strong> North department. . . host<strong>in</strong>g arrangementshave placed considerable economicstra<strong>in</strong> on households. . . "[35]Situation Report #31: "Follow<strong>in</strong>g heavyra<strong>in</strong>s <strong>in</strong> <strong>Haiti</strong> last week, <strong>the</strong> DPC states thatno damage <strong>to</strong> <strong>in</strong>frastructure or loss of lifehas been reported." "While TransitionalShelter programs have started <strong>in</strong> parts of<strong>the</strong> affected area; obta<strong>in</strong><strong>in</strong>g agreemen<strong>to</strong>n land rema<strong>in</strong>s a key obstacle <strong>to</strong> speedy<strong>response</strong>."[36]Situation Report #32: "A large portion ofemergency shelters constructed will requirestreng<strong>the</strong>n<strong>in</strong>g for <strong>the</strong> ra<strong>in</strong>y season. . . . Lackof certa<strong>in</strong>ty regard<strong>in</strong>g land tenure, potentiallength of stay and ultimate ownershipcont<strong>in</strong>ues <strong>to</strong> be of concern throughout<strong>the</strong> affected areas: both for relocation ofpriority sites and for plann<strong>in</strong>g of transitionalshelters."[37]Situation Report #33: "Figures from <strong>the</strong>latest Displacement Track<strong>in</strong>g Matrix (DTM)identified 1,373 settlement sites <strong>in</strong> PaP,Jacmel, Léogâne , Petit and Grande Goâve,which was considerably higher than <strong>in</strong>itialestimates. Of <strong>the</strong>se identified sites, only 289had Camp Management agencies present,thus register<strong>in</strong>g an overall coverage rate of21%. Some 411,090 households (2,090,877<strong>in</strong>dividuals) are estimated <strong>to</strong> be displaced."[38]"302,000 children havebeen displaced <strong>to</strong> o<strong>the</strong>rdepartments, with an additional720,000 childrenaffected by <strong>the</strong> <strong>earthquake</strong>but rema<strong>in</strong><strong>in</strong>g <strong>in</strong><strong>the</strong>ir home communities.Of this figure, 309,500children are currentlyliv<strong>in</strong>g <strong>in</strong> spontaneoustemporary settlementsites, which lack basicsocial services.” [35]"Many patients transported<strong>to</strong> <strong>the</strong> Dom<strong>in</strong>icanRepublic for healthcareafter <strong>the</strong> <strong>earthquake</strong> nowneed transportation back<strong>to</strong> <strong>Haiti</strong>. The ICRC and IOMwill likely assist <strong>in</strong> coord<strong>in</strong>at<strong>in</strong>grepatriation. . . .Mental health problemshave <strong>in</strong>creased s<strong>in</strong>ce <strong>the</strong><strong>earthquake</strong>. With only 24psychiatrists <strong>in</strong> <strong>the</strong> country,<strong>the</strong> lack of mentalhealthcare is more acutethan ever. . . . Sanitationand hygiene rema<strong>in</strong> <strong>to</strong>ppriority, particularly <strong>in</strong> <strong>the</strong>spontaneous settlementsites, where sanitationrema<strong>in</strong>s <strong>in</strong>adequate."[36]"From 28 February <strong>to</strong> 20March, 17 malaria cases,12 dengue fever cases and4 tuberculosis cases havebeen recorded with<strong>in</strong><strong>the</strong> zone of <strong>in</strong>terventionwhich has 25 first aid unitsand 3 hospitals. Over lastweek, 3 new cases of malariahave been detected<strong>in</strong> Fond Parisien and <strong>the</strong>cases of dengue cont<strong>in</strong>ue<strong>to</strong> rise."[37]177
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>Key f<strong>in</strong>d<strong>in</strong>gs1. Violence. The impact of <strong>the</strong> <strong>earthquake</strong> on people was characterized by direct trauma caused by <strong>the</strong> collapseof structures. In subsequent days, <strong>in</strong>juries occurred <strong>in</strong> traffic accidents, demonstrations, robbery and assaultdur<strong>in</strong>g transport and delivery of aid, and <strong>in</strong> particular, <strong>the</strong>re was an alarm<strong>in</strong>g <strong>in</strong>crease <strong>in</strong> rape and genderbasedviolence <strong>in</strong> camps and temporary settlements. Dur<strong>in</strong>g <strong>the</strong> 90 days of this study <strong>the</strong>re was a noted fearof civil unrest, with demonstrations and mass protests, primarily controlled by <strong>the</strong> MINUSTAH.2. Isolation and displacement. The impact of <strong>the</strong> <strong>earthquake</strong> on <strong>the</strong> physical structure of <strong>the</strong> Port-au-Pr<strong>in</strong>ceairport and port, and <strong>the</strong> obstruction of roads by debris generated extreme hardships <strong>in</strong> terms of access andmobilization with<strong>in</strong> <strong>the</strong> most affected areas, aggravated by <strong>the</strong> unusual <strong>in</strong>crease <strong>in</strong> traffic, by air, land, and sea.Simultaneously, a significant number of <strong>the</strong> population (estimated at more than 600,000 people) left <strong>the</strong> affectedareas <strong>to</strong> o<strong>the</strong>r regions with<strong>in</strong> <strong>the</strong> country.3. Mortality figures. Dur<strong>in</strong>g <strong>the</strong> first 10 days of <strong>the</strong> aftermath an <strong>in</strong>creas<strong>in</strong>g number of deaths were estimated,stabiliz<strong>in</strong>g at 112,000. On 2 February, with <strong>the</strong> decl<strong>in</strong>e of <strong>in</strong>ternational aid, <strong>the</strong> media compared <strong>Haiti</strong>’s<strong>earthquake</strong> <strong>to</strong> <strong>the</strong> 2004 Indian Ocean tsunami, which immediately generated a public statement by <strong>the</strong>Prime M<strong>in</strong>ister, almost doubl<strong>in</strong>g <strong>the</strong> official figures. The Direc<strong>to</strong>rate of Civil Protection (DPC) held <strong>to</strong> <strong>the</strong>orig<strong>in</strong>al figures <strong>in</strong>dicat<strong>in</strong>g that <strong>the</strong>y would review <strong>the</strong>m, and two weeks later <strong>in</strong>dicated that 222,570 deathswere recorded. Thus <strong>the</strong> <strong>Haiti</strong> figure outnumbers <strong>the</strong> death <strong>to</strong>ll from <strong>the</strong> Indian Ocean tsunami (220,000deaths). This situation is similar <strong>to</strong> what happened after Hurricane Mitch <strong>in</strong> 1998, when <strong>the</strong> <strong>in</strong>ternationalcommunity focused on <strong>the</strong> tragedy caused by <strong>the</strong> Casitas Volcano flash floods <strong>in</strong> Nicaragua with 1,212deaths, divert<strong>in</strong>g attention from <strong>the</strong> situation <strong>in</strong> Honduras. The reaction of <strong>the</strong> Honduras government wasevident: <strong>the</strong> death <strong>to</strong>ll rose suddenly from 334 <strong>to</strong> 6,600, a number that was repeated until it was f<strong>in</strong>ally accepted<strong>in</strong> <strong>the</strong> <strong>in</strong>ternational data systems [39].4. Change <strong>in</strong> health care needs. In <strong>the</strong> first two weeks, trauma care demanded nearly all <strong>the</strong> attention of <strong>the</strong>few rema<strong>in</strong><strong>in</strong>g health services and all <strong>the</strong> health teams deployed <strong>to</strong> <strong>Haiti</strong>. The provision of water services,energy, and waste collection <strong>in</strong> health centers was a challenge for PAHO and health authorities. Follow<strong>in</strong>g<strong>the</strong> <strong>in</strong>itial period, <strong>the</strong>re was a marked decrease <strong>in</strong> demand for <strong>earthquake</strong>-related trauma care, but an important<strong>in</strong>crease <strong>in</strong> demand for general medical care. Two months after <strong>the</strong> <strong>earthquake</strong>, <strong>the</strong> health <strong>in</strong>formationsystem detected an <strong>in</strong>crease <strong>in</strong> mental health problems, malaria, and dengue fever.5. Environmental health deterioration. The poor sanitation conditions prior <strong>to</strong> <strong>the</strong> event, <strong>to</strong>ge<strong>the</strong>r with <strong>the</strong>high concentration of people <strong>in</strong> camps, <strong>the</strong> difficulties <strong>in</strong> <strong>the</strong> provision of potable water, <strong>in</strong>adequate systemsof excreta disposal and waste collection, disruption <strong>in</strong> <strong>the</strong> regular health services, <strong>the</strong> onset of <strong>the</strong> ra<strong>in</strong>y season,and <strong>the</strong> remarkably difficult logistical conditions <strong>in</strong> <strong>Haiti</strong> demanded a massive mobilization <strong>to</strong> preven<strong>to</strong>utbreaks of communicable diseases by <strong>the</strong> health authorities and <strong>the</strong> <strong>in</strong>ternational community. But <strong>the</strong>rewas a risk fac<strong>to</strong>r that did not get any attention: <strong>the</strong> arrival <strong>to</strong> <strong>the</strong> island of thousands of <strong>in</strong>dividuals fromdifferent parts of <strong>the</strong> world who could <strong>in</strong>troduce a communicable disease <strong>to</strong> <strong>the</strong> island. N<strong>in</strong>e months after<strong>the</strong> quake <strong>the</strong> first cases of cholera were detected. The disease was caused by Vibrio cholerae serogroup O1,serotype Ogawa, a stra<strong>in</strong> found <strong>in</strong> South Asia [40].178
CHRONOLOGY OF EVENTS FOLLOWING THE HAITI EARTHQUAKE - Annex 2References (Annex 2)1. USGS-Magnitude 7.0 - <strong>Haiti</strong> Region.http://<strong>earthquake</strong>.usgs.gov/<strong>earthquake</strong>s/eq<strong>in</strong><strong>the</strong>news/<strong>2010</strong>/us<strong>2010</strong>rja6/#details.2. NOAA Center fort Tsunami Research - Tsunami Event - <strong>January</strong> 12, <strong>2010</strong>, <strong>Haiti</strong>.http://nctr.pmel.noaa.gov/haiti<strong>2010</strong>0112.3. Tsunami message number 3.http://reliefweb.<strong>in</strong>t/node/339965.4. CCRIF Moni<strong>to</strong>rs Earthquake <strong>in</strong> <strong>Haiti</strong>. http://reliefweb.<strong>in</strong>t/node/340132.5. OCHA. <strong>Haiti</strong> Earthquake Situation Report #1, 12 <strong>January</strong> <strong>2010</strong>.http://reliefweb.<strong>in</strong>t/sites/reliefweb.<strong>in</strong>t/files/resources/7FFA2880038FE2AA492576AA00182827-Full_Report.pdf.6. ———. <strong>Haiti</strong> Earthquake Situation Report #2, 13 <strong>January</strong> <strong>2010</strong>.www.redr.org.uk/washmaterials/content/D%20-%20WASH%20Related%20Diseases/D4%20-%20Group%20Work/D_HO_OCHA%20SitRep%202%2013th%20Jan%<strong>2010</strong>.pdf.7. ———. <strong>Haiti</strong> Earthquake Situation Report #3, 14 <strong>January</strong> <strong>2010</strong>.https://www.cimicweb.org/Documents/<strong>Haiti</strong>%20Documents/OCHA%20Incident%20Report%203.pdf.8. ———. <strong>Haiti</strong> Earthquake Situation Report #4, 15 <strong>January</strong> <strong>2010</strong>.http://blog.givewell.org/attachments/haitisituationreport<strong>2010</strong>0115.pdf.9. ———. <strong>Haiti</strong> Earthquake Situation Report #5, 16 <strong>January</strong> <strong>2010</strong>.http://reliefweb.<strong>in</strong>t/sites/reliefweb.<strong>in</strong>t/files/resources/57C9BBCDC417E4B2492576AE000199FD-Full_Report.pdf.10. ———. <strong>Haiti</strong> Earthquake Situation Report #6, 17 <strong>January</strong> <strong>2010</strong>.www.c<strong>in</strong>u.org.mx/haiti/docs/ID_6824_MS_Redhum_HT._Informe._OCHA_Informe_de_Situacion_No.6_por_Terremo<strong>to</strong>(<strong>in</strong>gles).pdf.11. ———. <strong>Haiti</strong> Earthquake Situation Report #7, 18 <strong>January</strong> <strong>2010</strong>.http://reliefweb.<strong>in</strong>t/sites/reliefweb.<strong>in</strong>t/files/resources/7922C7505D4AD77F492576B0000A8044-Full_Report.pdf.12. ———. <strong>Haiti</strong> Earthquake Situation Report #8, 19 <strong>January</strong> <strong>2010</strong>.http://reliefweb.<strong>in</strong>t/sites/reliefweb.<strong>in</strong>t/files/resources/0160C1FDCFADA27D492576B1000FE565-Full_Report.pdf.13. ———. <strong>Haiti</strong> Earthquake Situation Report #9, 20 <strong>January</strong> <strong>2010</strong>.https://www.cimicweb.org/Documents/<strong>Haiti</strong>%20Documents/OCHA%20Incident%20Report%209.pdf.14. ———. <strong>Haiti</strong> Earthquake Situation Report #10, 21 <strong>January</strong> <strong>2010</strong>.http://www.c<strong>in</strong>u.org.mx/haiti/docs/OCHASituationReportNo10_<strong>Haiti</strong>Earthquake21Jan<strong>2010</strong>.pdf.15. ———. <strong>Haiti</strong> Earthquake Situation Report #11, 22 <strong>January</strong> <strong>2010</strong>.http://one<strong>response</strong>.<strong>in</strong>fo/Disasters/<strong>Haiti</strong>/publicdocuments/OCHA%20Situation%20Report%20No.11%20<strong>Haiti</strong>%20Earthquake%20-%2022%20Jan%20<strong>2010</strong>.pdf.16. ———. <strong>Haiti</strong> Earthquake Situation Report #12, 23 <strong>January</strong> <strong>2010</strong>.http://reliefweb.<strong>in</strong>t/sites/reliefweb.<strong>in</strong>t/files/resources/A5B95A3F73E981C3492576B6000F5F46-Full_Report.pdf.17. ———. <strong>Haiti</strong> Earthquake Situation Report #13, 25 <strong>January</strong> <strong>2010</strong>.http://blog.givewell.org/attachments/ocha-haiti-jan25.pdf.18. ———. <strong>Haiti</strong> Earthquake Situation Report #14, 27 <strong>January</strong> <strong>2010</strong>.http://reliefweb.<strong>in</strong>t/sites/reliefweb.<strong>in</strong>t/files/resources/BBB1958E3D1F9875492576B9001A2DE5-Full_Report.pdf.19. ———. <strong>Haiti</strong> Earthquake Situation Report #15, 29 <strong>January</strong> <strong>2010</strong>.http://reliefweb.<strong>in</strong>t/sites/reliefweb.<strong>in</strong>t/files/resources/3568C93412C1A812492576BB001AA708-Full_Report.pdf.179
<strong>Health</strong> <strong>response</strong> <strong>to</strong> <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> <strong>Haiti</strong> <strong>January</strong> <strong>2010</strong>20. ———. <strong>Haiti</strong> Earthquake Situation Report #16, 1 February <strong>2010</strong>.http://reliefweb.<strong>in</strong>t/sites/reliefweb.<strong>in</strong>t/files/resources/D25C5A8D4392B88A492576BE001A3FD6-Full_Report.pdf.21. Agence France-Presse (AFP): <strong>Haiti</strong> death <strong>to</strong>ll <strong>to</strong>ps 200 000 as aid anger mounts, 03 Feb <strong>2010</strong>.http://reliefweb.<strong>in</strong>t/node/344108[4.22. OCHA. <strong>Haiti</strong> Earthquake Situation Report #17, 3 February <strong>2010</strong>.http://reliefweb.<strong>in</strong>t/sites/reliefweb.<strong>in</strong>t/files/resources/0D9BB02C81D4C0BB492576C0001D2ACC-Full_Report.pdf.23. ———. <strong>Haiti</strong> Earthquake Situation Report #18, 5 February <strong>2010</strong>.http://reliefweb.<strong>in</strong>t/sites/reliefweb.<strong>in</strong>t/files/resources/D071E8A40383A4BD492576C2001D2EB8-Full_Report.pdf.24. ———. <strong>Haiti</strong> Earthquake Situation Report #19, 8 February <strong>2010</strong>.http://reliefweb.<strong>in</strong>t/sites/reliefweb.<strong>in</strong>t/files/resources/5D041C189B9C3E2D492576C5001EDC8D-Full_Report.pdf.25. ———. <strong>Haiti</strong> Earthquake Situation Report #20, 11 February <strong>2010</strong>.http://reliefweb.<strong>in</strong>t/sites/reliefweb.<strong>in</strong>t/files/resources/1FBA6ADC332AD880492576C80021E214-Full_Report.pdf.26. ———. <strong>Haiti</strong> Earthquake Situation Report #21, 16 February <strong>2010</strong>.http://reliefweb.<strong>in</strong>t/sites/reliefweb.<strong>in</strong>t/files/resources/0B09A5ED6E25C636492576CD002336C3-Full_Report.pdf.27. ———. <strong>Haiti</strong> Earthquake Situation Report #22, 19 February <strong>2010</strong>.http://reliefweb.<strong>in</strong>t/sites/reliefweb.<strong>in</strong>t/files/resources/53B700B5F8780C94852576CF0059199B-Full_Report.pdf.28. ———. <strong>Haiti</strong> Earthquake Situation Report #23, 22 February <strong>2010</strong>.http://reliefweb.<strong>in</strong>t/sites/reliefweb.<strong>in</strong>t/files/resources/CEB1B7C987DB2763492576D3001ECF55-Full_Report.pdf.29. ———. <strong>Haiti</strong> Earthquake Situation Report #24, 25 February <strong>2010</strong>. http://reliefweb.<strong>in</strong>t/node/347003.30. ———. <strong>Haiti</strong> Earthquake Situation Report #25, 1 March <strong>2010</strong>.http://reliefweb.<strong>in</strong>t/sites/reliefweb.<strong>in</strong>t/files/resources/4307AA39A67F4238852576DA006C3539-Full_Report.pdf.31. ———. <strong>Haiti</strong> Earthquake Situation Report #26, 4 March <strong>2010</strong>.http://reliefweb.<strong>in</strong>t/sites/reliefweb.<strong>in</strong>t/files/resources/EFF273EDC9FC7822C12576DD0032DD94-Full_Report.pdf.32. ———. <strong>Haiti</strong> Earthquake Situation Report #27, 9 March <strong>2010</strong>.http://reliefweb.<strong>in</strong>t/sites/reliefweb.<strong>in</strong>t/files/resources/33CAB4687357E388852576E1006B5D55-Full_Report.pdf.33. ———. <strong>Haiti</strong> Earthquake Situation Report #28, 11 March <strong>2010</strong>.http://reliefweb.<strong>in</strong>t/sites/reliefweb.<strong>in</strong>t/files/resources/296BA274DDBA1B11852576E4005A04A6-Full_Report.pdf.34. ———. <strong>Haiti</strong> Earthquake Situation Report #29, 15 March <strong>2010</strong>.http://reliefweb.<strong>in</strong>t/sites/reliefweb.<strong>in</strong>t/files/resources/5AD02F92CC09F56C852576E800691102-Full_Report.pdf.35. ———. <strong>Haiti</strong> Earthquake Situation Report #30, 19 March <strong>2010</strong>.http://reliefweb.<strong>in</strong>t/sites/reliefweb.<strong>in</strong>t/files/resources/E815D7C4A129D0F3852576EB00673547-Full_Report.pdf.36. ———. <strong>Haiti</strong> Earthquake Situation Report #31, 24 March <strong>2010</strong>.http://reliefweb.<strong>in</strong>t/sites/reliefweb.<strong>in</strong>t/files/resources/8B3740D9D65B5AA6852576F1006DF6DA-Full_Report.pdf.37. ———. <strong>Haiti</strong> Earthquake Situation Report #32, 31 March <strong>2010</strong>.http://reliefweb.<strong>in</strong>t/sites/reliefweb.<strong>in</strong>t/files/resources/EE8BDFA342BA2D9F852576FA0076F3D9-Full_Report.pdf.38. ———. <strong>Haiti</strong> Earthquake Situation Report #33, 12 April <strong>2010</strong>.http://reliefweb.<strong>in</strong>t/sites/reliefweb.<strong>in</strong>t/files/resources/04A48A6EAC9DB2E24925770300820BE0-Full_Report.pdf.39. Olson, R.S., R. Alvarez, B. Baird, A. Estrada, V. Gawronski, J.P. Sarmien<strong>to</strong>. The s<strong>to</strong>rms of 1998: Hurricanes Georges and Mitch.Impacts, <strong>in</strong>stitutional <strong>response</strong>, and disaster politics <strong>in</strong> three countries. Boulder, Colorado: Natural Hazards Research and ApplicationsInformation Center, Special Publication 38, 2001 Pg. 34.18040. http://www.<strong>in</strong>fectioncontrol<strong>to</strong>day.com/news/<strong>2010</strong>/11/cdc-announces-labora<strong>to</strong>ry-test-results-of-cholera-outbreak-stra<strong>in</strong>-<strong>in</strong>-haiti.aspx.
The 12 <strong>January</strong> <strong>2010</strong> <strong>earthquake</strong> was <strong>the</strong> most devastat<strong>in</strong>g of many major sudden-impact naturaldisasters affect<strong>in</strong>g <strong>Haiti</strong> <strong>in</strong> <strong>the</strong> last 10 years. The health impact of <strong>the</strong> <strong>earthquake</strong> <strong>in</strong> absolute terms(number of dead and <strong>in</strong>jured) was among <strong>the</strong> highest <strong>in</strong> recent times. When <strong>the</strong> needs are compared<strong>to</strong> <strong>the</strong> country’s <strong>response</strong> capacity, this disaster was truly unprecedented.The level of <strong>response</strong>, especially <strong>in</strong> <strong>the</strong> health sec<strong>to</strong>r, was generous, even overwhelm<strong>in</strong>g. Organizationof <strong>the</strong> massive, global <strong>response</strong> was challeng<strong>in</strong>g, and many of <strong>the</strong> problems seen <strong>in</strong> pastdisasters were replayed <strong>in</strong> <strong>Haiti</strong>. Information was scarce, decisions were often not evidence-based,and <strong>the</strong>re were serious gaps <strong>in</strong> overall or sec<strong>to</strong>ral coord<strong>in</strong>ation.This book presents lessons <strong>to</strong> be learned from <strong>Haiti</strong> with <strong>the</strong> aim of improv<strong>in</strong>g <strong>the</strong> health sec<strong>to</strong>r’s<strong>response</strong> <strong>in</strong> major, sudden-onset disasters <strong>in</strong> <strong>the</strong> future. It also identifies opportunities provided by<strong>the</strong> disaster for mak<strong>in</strong>g significant changes <strong>in</strong> health services <strong>in</strong> <strong>Haiti</strong>. One of <strong>the</strong> key lessons of <strong>the</strong><strong>Haiti</strong> tragedy is that coord<strong>in</strong>ation can only be effective where national authorities are equipped <strong>to</strong>assume leadership and establish relief and recovery priorities.The authors have drawn on <strong>the</strong>ir own extensive experience <strong>in</strong> <strong>in</strong>ternational disaster management,and syn<strong>the</strong>sized material from reports, evaluations, peer-reviewed scientific publications, and over150 <strong>in</strong>terviews. A review group was convened by PAHO/WHO <strong>to</strong> corroborate <strong>the</strong> f<strong>in</strong>d<strong>in</strong>gs andconclusions of this publication.The book gives particular emphasis <strong>to</strong> those lessons that are of general <strong>in</strong>terest, i.e., not specific <strong>to</strong><strong>the</strong> case of <strong>Haiti</strong>. The <strong>in</strong>ternational community has much <strong>to</strong> learn from <strong>the</strong> <strong>response</strong> <strong>in</strong> <strong>Haiti</strong> whereit has shown an ability <strong>to</strong> repeat its errors and shortcom<strong>in</strong>gs from past disasters.This document can be viewed on <strong>the</strong> Internet at:www.paho.org/disastersArea on Emergency Preparedness and Disaster Reliefwww.paho.org/disastersdisaster-publications@paho.org