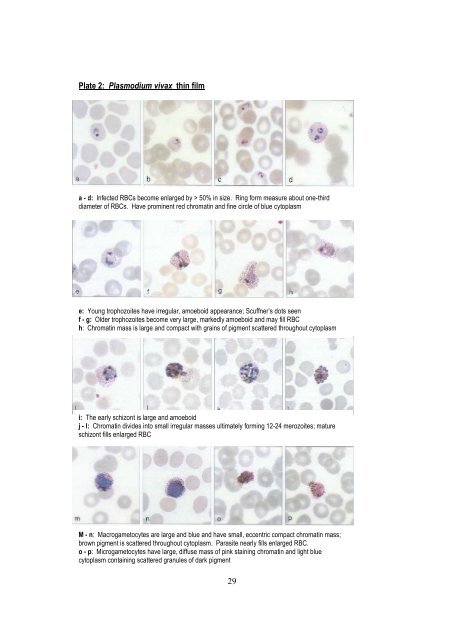
Plate 2: Plasmodium vivax thin filma - d: Infected RBCs become enlarged by > 50% in size. Ring <strong>for</strong>m measure about one-thirddiameter of RBCs. Have prominent red chromatin and fine circle of blue cytoplasme: Young trophozoites have irregular, amoeboid appearance; Scuffner’s dots seenf - g: Older trophozoites become very large, markedly amoeboid and may fill RBCh: Chromatin mass is large and compact with grains of pigment scattered throughout cytoplasmi: The early schizont is large and amoeboidj - l: Chromatin divides into small irregular masses ultimately <strong>for</strong>ming 12-24 merozoites; matureschizont fills enlarged RBCM - n: Macrogametocytes are large and blue and have small, eccentric compact chromatin mass;brown pigment is scattered throughout cytoplasm. Parasite nearly fills enlarged RBC.o - p: Microgametocytes have large, diffuse mass of pink staining chromatin and light bluecytoplasm containing scattered granules of dark pigment29
3.3: MALARIA CASE MANAGEMENTAntimalarial drugsChloroquineChloroquine is a 4-aminoquinoline used extensively <strong>for</strong> treatment and prevention of malaria.Widespread resistance has now rendered it ineffective against P. falciparum in most parts of the world,although it still maintains considerable efficacy <strong>for</strong> treatment of other species of malaria. Chloroquineinterferes with parasite haem detoxification. Resistance is related to genetic changes in transporters(PfCRT, PfMDR), which reduce the concentrations of chloroquine at its site of action, the parasite foodvacuole. The principal limiting adverse effects in practice are the unpleasant taste, which may upsetchildren, and pruritus, which may be severe in dark-skinned patients. Other less common side effectsinclude headache, various skin eruptions and gastrointestinal disturbances, such as nausea, vomitingand diarrhea.AmodiaquineAmodiaquine is a 4-aminoquinoline with a mode of action similar to that of chloroquine. Its adverseeffects are also similar to those of chloroquine. Amodiaquine is associated with less pruritus and ismore palatable than chloroquine. It is associated with a much higher risk of agranulocytosis and, to alesser degree, of hepatitis when used <strong>for</strong> prophylaxis.SulfadoxineSulfadoxine is a slowly eliminated sulfonamide which is a competitive inhibitor of dihydropteroatesynthase, the bacterial enzyme responsible <strong>for</strong> incorporation of p-amino benzoic acid in the synthesis offolic acid. Sulfadoxine is used in a fixed-dose combination of 20 parts of sulfadoxine with 1 part ofpyrimethamine. Hypersensitivity reactions can be severe because of its slow elimination and may affectdifferent organ systems. Nausea, vomiting, anorexia and diarrhea may occur. Cutaneousmanifestations can be severe and include pruritus, photosensitivity reactions, exfoliative dermatitis,erythema nodosum, toxic epidermal necrolysis and Stevens-Johnson syndrome. Treatment withsulfadoxine should be stopped in any patient developing a rash because of the risk of severe allergicreactions.PyrimethaminePyrimethamine is a diaminopyrimidine used in combination with a sulfonamide and it exerts itsantimalarial activity by inhibiting plasmodial dihydrofolate reductase thus blocking the synthesis ofnucleic acids in the malarial parasite. Pyrimethamine is generally very well tolerated. Administration <strong>for</strong>prolonged periods may cause depression of haematopoiesis due to interference with folic acidmetabolism. Skin rashes and hypersensitivity reactions also occur.MefloquineMefloquine is a 4-methanolquinoline and is related to quinine. It is effective against all <strong>for</strong>ms of malaria.Minor adverse effects are common following mefloquine treatment, most frequently nausea, vomiting,abdominal pain, anorexia, diarrhea, headache, dizziness, loss of balance, dysphoria, somnolence andsleep disorders, notably insomnia and abnormal dreams. Neuropsychiatric disturbances (seizures,encephalopathy, psychosis) are less common but are more severe.30