

training module for medical officers primary health centre - NVBDCP
training module for medical officers primary health centre - NVBDCP
training module for medical officers primary health centre - NVBDCP
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
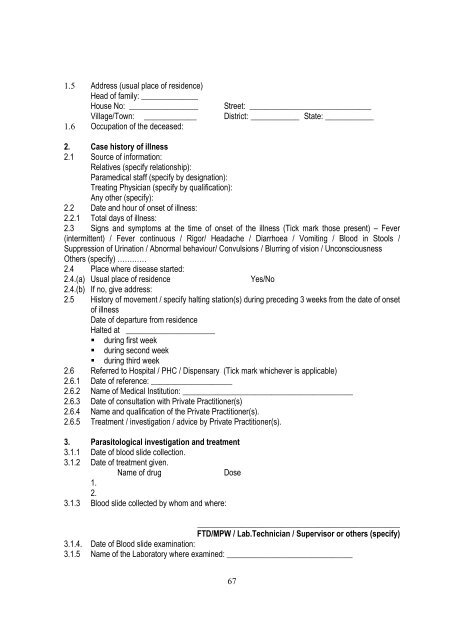
1.5 Address (usual place of residence)Head of family: ______________House No: _________________ Street: ______________________________Village/Town: _____________ District: ____________ State: ____________1.6 Occupation of the deceased:2. Case history of illness2.1 Source of in<strong>for</strong>mation:Relatives (specify relationship):Para<strong>medical</strong> staff (specify by designation):Treating Physician (specify by qualification):Any other (specify):2.2 Date and hour of onset of illness:2.2.1 Total days of illness:2.3 Signs and symptoms at the time of onset of the illness (Tick mark those present) – Fever(intermittent) / Fever continuous / Rigor/ Headache / Diarrhoea / Vomiting / Blood in Stools /Suppression of Urination / Abnormal behaviour/ Convulsions / Blurring of vision / UnconsciousnessOthers (specify) …………2.4 Place where disease started:2.4.(a) Usual place of residenceYes/No2.4.(b) If no, give address:2.5 History of movement / specify halting station(s) during preceding 3 weeks from the date of onsetof illnessDate of departure from residenceHalted at ______________________ during first week during second week during third week2.6 Referred to Hospital / PHC / Dispensary (Tick mark whichever is applicable)2.6.1 Date of reference: ____________________2.6.2 Name of Medical Institution: __________________________________________2.6.3 Date of consultation with Private Practitioner(s)2.6.4 Name and qualification of the Private Practitioner(s).2.6.5 Treatment / investigation / advice by Private Practitioner(s).3. Parasitological investigation and treatment3.1.1 Date of blood slide collection.3.1.2 Date of treatment given.Name of drugDose1.2.3.1.3 Blood slide collected by whom and where:__________________________________________________FTD/MPW / Lab.Technician / Supervisor or others (specify)3.1.4. Date of Blood slide examination:3.1.5 Name of the Laboratory where examined: _______________________________67













