SBC Anthem BC PPO 80-G
SBC Anthem BC PPO 80-G
SBC Anthem BC PPO 80-G

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
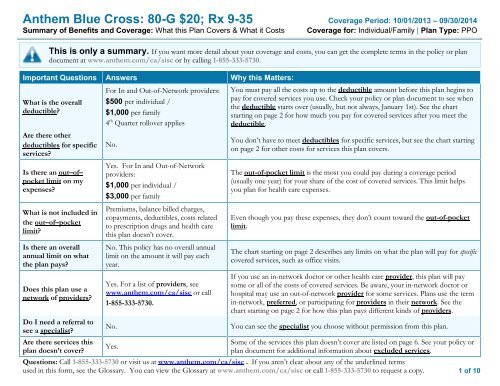
<strong>Anthem</strong> Blue Cross: <strong>80</strong>-G $20; Rx 9-35 Coverage Period: 10/01/2013 – 09/30/2014Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family | Plan Type: <strong>PPO</strong> Copayments are fixed dollar amounts (for example, $15) you pay for covered health care, usually when you receive the service. Coinsurance is your share of the costs of a covered service, calculated as a percent of the allowed amount for the service. For example, ifthe plan’s allowed amount for an overnight hospital stay is $1,000, your coinsurance payment of 20% would be $200. This may change ifyou haven’t met your deductible. The amount the plan pays for covered services is based on the allowed amount. If an out-of-network provider charges more than theallowed amount, you may have to pay the difference. For example, if an out-of-network hospital charges $1,500 for an overnight stay andthe allowed amount is $1,000, you may have to pay the $500 difference. (This is called balance billing.) This plan may encourage you to use in-network providers by charging you lower deductibles, copayments and coinsurance amounts.CommonMedical EventIf you visit a healthcare provider’s officeor clinicIf you have a testServices You May NeedPrimary care visit to treat an injury orillnessSpecialist visitYour Cost If YouUse anIn-networkProvider$20/visit$20/visitYour Cost If YouUse anOut-of-networkProviderBilled chargesexceeding out-ofnetworkfee scheduleBilled chargesexceeding out-ofnetworkfee scheduleChiropractorBilled chargesexceeding out-ofnetworkfee scheduleAcupuncturist0% coinsurance with$25/visit maxLimitations & ExceptionsDeductible applies to out-ofnetwork.Deductible applies to out-ofnetwork.Other practitioner office visitChiropractor20% coinsuranceafter deductibleAcupuncturist20% coinsuranceafter deductible with$50/visit maxChiropractorMedical necessity review is requiredafter the 5 th visit.AcupunctureCoverage is limited to 12 visits,combined in and out-of-network anddeductible applies.Preventive care/screening/immunization No Cost Share Not Covered –––––––––––none–––––––––––Diagnostic test (x-ray, blood work)Imaging (CT/PET scans, MRIs)20% coinsuranceafter deductible20% coinsuranceafter deductibleBilled chargesexceeding out-ofnetworkfee schedule0% coinsurance with$<strong>80</strong>0/test max–––––––––––none–––––––––––Coverage is limited to $<strong>80</strong>0 for outof-networkproviders.Questions: Call 1-855-333-5730 or visit us at www.anthem.com/ca/sisc . If you aren’t clear about any of the underlined termsused in this form, see the Glossary. You can view the Glossary at www.anthem.com/ca/sisc or call 1-855-333-5730 to request a copy.2 of 10
<strong>Anthem</strong> Blue Cross: <strong>80</strong>-G $20; Rx 9-35 Coverage Period: 10/01/2013 – 09/30/2014Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family | Plan Type: <strong>PPO</strong>CommonMedical EventIf you need drugs totreat your illness orconditionIf you haveoutpatient surgeryServices You May NeedTypically Generic drugsTypically Preferred/Formulary drugsTypically Non-preferred/non-formularydrugsTypically Specialty drugsFacility fee (e.g., ambulatory surgerycenter)Your Cost If YouUse anIn-networkProvider$9 Retail $18 Mail$35 Retail $90 Mail20% coinsuranceafter deductibleYour Cost If YouUse anOut-of-networkProviderMember may havegreater out of pocketexpense for using anon-preferredproviderMember may havegreater out of pocketexpense for using anon-preferredproviderMember may havegreater out of pocketexpense for using anon-preferredproviderMember may havegreater out of pocketexpense for using anon-preferredproviderOutpatient Facility50% coinsuranceAmbulatory SurgeryCenter0% coinsurance with$350/admission maxLimitations & ExceptionsMost generics available at Costco for$0 copayment.Brand diabetic supplies available atgeneric copayment. If the memberselects a brand drug when a genericequivalent is available the member isresponsible for the genericcopayment plus the cost differencebetween the generic and brandequivalent, even if the physicianindicates no substitutions.–––––––––––none––––––––––––––––––––––none–––––––––––Deductible applies to out-ofnetwork.Questions: Call 1-855-333-5730 or visit us at www.anthem.com/ca/sisc . If you aren’t clear about any of the underlined termsused in this form, see the Glossary. You can view the Glossary at www.anthem.com/ca/sisc or call 1-855-333-5730 to request a copy.3 of 10
<strong>Anthem</strong> Blue Cross: <strong>80</strong>-G $20; Rx 9-35 Coverage Period: 10/01/2013 – 09/30/2014Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family | Plan Type: <strong>PPO</strong>CommonMedical EventIf you needimmediate medicalattentionIf you have ahospital stayServices You May NeedPhysician/surgeon feesEmergency room servicesEmergency medical transportationUrgent careFacility fee (e.g., hospital room)Physician/surgeon feeYour Cost If YouUse anIn-networkProvider20% coinsuranceafter deductible$100/visit beforedeductible and20% coinsuranceafter deductible20% coinsuranceafter deductible$20/visit20% coinsuranceafter deductible20% coinsuranceafter deductibleYour Cost If YouUse anOut-of-networkProviderBilled chargesexceeding out-ofnetworkfee schedule$100/visit beforedeductible and20% coinsuranceafter deductibleDeductible applies,billed chargesexceeding maximumallowedBilled chargesexceeding out-ofnetworkfee schedule0% coinsurance with$600/day maxBilled chargesexceeding out-ofnetworkfee scheduleLimitations & ExceptionsYou are responsible for billedcharges exceeding scheduled amountfor out-of-network providers.Copayment waived if admitted. Youare responsible for billed chargesexceeding maximum allowed amountfor out-of-network providers.–––––––––––none–––––––––––Costs may vary by site of service.You should refer to your formalcontract of coverage for details.Deductible applies to out-ofnetwork.Preauthorization isrequired.–––––––––––none–––––––––––Questions: Call 1-855-333-5730 or visit us at www.anthem.com/ca/sisc . If you aren’t clear about any of the underlined termsused in this form, see the Glossary. You can view the Glossary at www.anthem.com/ca/sisc or call 1-855-333-5730 to request a copy.4 of 10
<strong>Anthem</strong> Blue Cross: <strong>80</strong>-G $20; Rx 9-35 Coverage Period: 10/01/2013 – 09/30/2014Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family | Plan Type: <strong>PPO</strong>CommonMedical EventServices You May NeedYour Cost If YouUse anIn-networkProviderYour Cost If YouUse anOut-of-networkProviderLimitations & ExceptionsIf you have mentalhealth, behavioralhealth, or substanceabuse needsIf you are pregnantMental/Behavioral health outpatientservicesMental/Behavioral health inpatientservicesSubstance use disorder outpatient servicesSubstance use disorder inpatient servicesPrenatal and postnatal careDelivery and all inpatient servicesOffice Visit$20/visitFacility Visit20% coinsuranceafter deductible20% coinsuranceafter deductibleOffice Visit$20/visitFacility Visit20% coinsuranceafter deductible20% coinsuranceafter deductible20% coinsuranceafter deductible20% coinsuranceafter deductibleOffice VisitBilled chargesexceeding out-ofnetworkfee scheduleFacility Visit50% coinsuranceafter deductible0% coinsurance with$600/day maxOffice Visit0% coinsuranceafter deductibleFacility Visit50% coinsuranceafter deductible0% coinsurance with$600/day maxBilled chargesexceeding out-ofnetworkfee schedule0% coinsurance with$600/day maxFacility VisitPreauthorization is required. Youare responsible for billed chargesexceeding maximum allowed amountfor out-of-network providers.Deductible applies to out-ofnetwork.Preauthorization isrequired.Office VisitDeductible waived for in-networkproviders. You are responsible forbilled charges exceeding scheduledamount for out-of-networkproviders.Facility VisitYou are responsible for billedcharges exceeding scheduled amountfor out-of-network providers.Deductible applies to out-ofnetwork.Preauthorization isrequired.–––––––––––none–––––––––––Deductible applies to out-ofnetwork.Questions: Call 1-855-333-5730 or visit us at www.anthem.com/ca/sisc . If you aren’t clear about any of the underlined termsused in this form, see the Glossary. You can view the Glossary at www.anthem.com/ca/sisc or call 1-855-333-5730 to request a copy.5 of 10
<strong>Anthem</strong> Blue Cross: <strong>80</strong>-G $20; Rx 9-35 Coverage Period: 10/01/2013 – 09/30/2014Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family | Plan Type: <strong>PPO</strong>CommonMedical EventIf you need helprecovering or haveother special healthneedsIf your child needsdental or eye careServices You May NeedHome health careRehabilitation servicesHabilitation servicesSkilled nursing careDurable medical equipmentHospice serviceYour Cost If YouUse anIn-networkProvider20% coinsuranceafter deductible20% coinsuranceafter deductible20% coinsuranceafter deductible20% coinsuranceafter deductible20% coinsuranceafter deductibleNo Cost ShareYour Cost If YouUse anOut-of-networkProviderBilled chargesexceeding maximumallowedBilled chargesexceeding out-ofnetworkfee scheduleBilled chargesexceeding out-ofnetworkfee schedule0% coinsurance with$600/day maxBilled chargesexceeding out-ofnetworkfee schedule20% coinsuranceafter deductibleLimitations & ExceptionsCoverage is limited to 100occurrences every 12 months.Preauthorization is required.All physical medicine services aresubject to medical necessity review.Coverage is limited to 100 visits peryear. Deductible applies to out-ofnetwork.–––––––––––none––––––––––––––––––––––none–––––––––––Eye exam Not Covered Not Covered –––––––––––none–––––––––––Glasses Not Covered Not Covered –––––––––––none–––––––––––Dental check-up Not Covered Not Covered –––––––––––none–––––––––––Questions: Call 1-855-333-5730 or visit us at www.anthem.com/ca/sisc . If you aren’t clear about any of the underlined termsused in this form, see the Glossary. You can view the Glossary at www.anthem.com/ca/sisc or call 1-855-333-5730 to request a copy.6 of 10
<strong>Anthem</strong> Blue Cross: <strong>80</strong>-G $20; Rx 9-35 Coverage Period: 10/01/2013 – 09/30/2014Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family | Plan Type: <strong>PPO</strong>Excluded Services & Other Covered Services:Services Your Plan Does NOT Cover (This isn’t a complete list. Check your policy or plan document for other excluded services.)• Cosmetic surgery• Dental care (Adult)• Infertility treatment• Long-term care• Private-duty nursing• Routine foot care• Weight loss programsOther Covered Services (This isn’t a complete list. Check your policy or plan document for other covered services and your costs for theseservices.)• Acupuncture (limits apply)• Bariatric surgery (must be preauthorized andperformed at a qualified Center of MedicalExcellence Facility)• Chiropractic care (subject to review for medicalnecessity)• Hearing aids (limited to $700 per 24months)• Most coverage provided outside the UnitedStates. Seewww.<strong>BC</strong>BS.com/bluecardworldwide• Non-emergency care when traveling outsidethe U.S.• Routine eye care (Adult) (as part of routinephysical exam)Your Rights to Continue Coverage:If you lose coverage under the plan, then, depending upon the circumstances, Federal and State laws may provide protections that allow you to keep healthcoverage. Any such rights may be limited in duration and will require you to pay a premium, which may be significantly higher than the premium you paywhile covered under the plan. Other limitations on your rights to continue coverage may also apply.For more information on your rights to continue coverage, contact the plan at Tulare Foundation 1-<strong>80</strong>0-322-5709; Kern Foundation 1-<strong>80</strong>0-322-5709;Woodland Hills 1-<strong>80</strong>0-825-5541; Coastal TPA 1-<strong>80</strong>0-564-7475. You may also contact your state insurance department, the U.S. Department of Labor,Employee Benefits Security Administration at 1-866-444-3272 or www.dol.gov/ebsa, or the U.S. Department of Health and Human Services at 1-877-267-2323 x61565 or www.cciio.cms.gov.Questions: Call 1-855-333-5730 or visit us at www.anthem.com/ca/sisc . If you aren’t clear about any of the underlined termsused in this form, see the Glossary. You can view the Glossary at www.anthem.com/ca/sisc or call 1-855-333-5730 to request a copy.7 of 10
<strong>Anthem</strong> Blue Cross: <strong>80</strong>-G $20; Rx 9-35 Coverage Period: 10/01/2013 – 09/30/2014Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family | Plan Type: <strong>PPO</strong>Your Grievance and Appeals Rights:If you have a complaint or are dissatisfied with a denial of coverage for claims under your plan, you may be able to appeal or file a grievance. Forquestions about your rights, this notice, or assistance, you can contact:California Department of Managed Health Care Help Center (DMHC business only) State of California (CDI business only)9<strong>80</strong> 9 th Street, Suite 500 DEPARTMENT OF INSURANCESacramento, CA 95814 CLAIMS SERVICE BUREAU1-888-466-2219 300 South Spring Street, South Towerwww.healthhelp.ca.govhelpline@dmhc.ca.gov Los Angeles, CA 90013www.insurance.ca.govFor additional assistance regarding appeals you may contact the Department of Labor’s Employee Benefits Security Administration at 1-866-444-EBSA(3272) or www.dol.gov/ebsa/healthreform.Language Access Services:––––––––––––––––––––––To see examples of how this plan might cover costs for a sample medical situation, see the next page.––––––––––––––––––––––Questions: Call 1-855-333-5730 or visit us at www.anthem.com/ca/sisc . If you aren’t clear about any of the underlined termsused in this form, see the Glossary. You can view the Glossary at www.anthem.com/ca/sisc or call 1-855-333-5730 to request a copy.8 of 10
<strong>Anthem</strong> Blue Cross: <strong>80</strong>-G $20; Rx 9-35 Coverage Period: 10/01/2013 – 09/30/2014Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family | Plan Type: <strong>PPO</strong>About these CoverageExamples:These examples show how this plan might covermedical care in given situations. Use theseexamples to see, in general, how much financialprotection a sample patient might get if they arecovered under different plans.This isnot a costestimator.Don’t use these examples toestimate your actual costsunder this plan. The actualcare you receive will bedifferent from theseexamples, and the cost ofthat care will also bedifferent.See the next page forimportant information aboutthese examples.Having a baby(normal delivery)• Amount owed to providers: $7,540• Plan pays $5540• Patient pays $2000Sample care costs:Hospital charges (mother) $2,700Routine obstetric care $2,100Hospital charges (baby) $900Anesthesia $900Laboratory tests $500Prescriptions $200Radiology $200Vaccines, other preventive $40Total $7,540Patient pays:Deductibles $500Copays $300Coinsurance $1000Limits or exclusions $200Total $2000Managing type 2 diabetes(routine maintenance ofa well-controlled condition)• Amount owed to providers: $5,400• Plan pays $4000• Patient pays $1400Sample care costs:Prescriptions $2,900Medical Equipment and Supplies $1,300Office Visits and Procedures $700Education $300Laboratory tests $100Vaccines, other preventive $100Total $5,400Patient pays:Deductibles $200Copays $1100Coinsurance $0Limits or exclusions $100Total $1400Note: These numbers assume the patient isparticipating in our diabetes wellnessprogram. If you have diabetes and do notparticipate in the wellness program, yourcosts may be higher. For more informationabout the diabetes wellness program, pleasecontact <strong>Anthem</strong> at 1-855-333-5730.Questions: Call 1-855-333-5730 or visit us at www.anthem.com/ca/sisc . If you aren’t clear about any of the underlined termsused in this form, see the Glossary. You can view the Glossary at www.anthem.com/ca/sisc or call 1-855-333-5730 to request a copy.9 of 10
<strong>Anthem</strong> Blue Cross: <strong>80</strong>-G $20; Rx 9-35 Coverage Period: 10/01/2013 – 09/30/2014Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family | Plan Type: <strong>PPO</strong>Questions and answers about the Coverage Examples:What are some of theassumptions behind theCoverage Examples?Costs don’t include premiums.Sample care costs are based on nationalaverages supplied by the U.S.Department of Health and HumanServices, and aren’t specific to aparticular geographic area or health plan.The patient’s condition was not anexcluded or preexisting condition.All services and treatments started andended in the same coverage period.There are no other medical expenses forany member covered under this plan.Out-of-pocket expenses are based onlyon treating the condition in the example.The patient received all care from innetworkproviders. If the patient hadreceived care from out-of-networkproviders, costs would have been higher.What does a Coverage Exampleshow?For each treatment situation, the CoverageExample helps you see how deductibles,copayments, and coinsurance can add up. Italso helps you see what expenses might be leftup to you to pay because the service ortreatment isn’t covered or payment is limited.Does the Coverage Examplepredict my own care needs? No. Treatments shown are just examples.The care you would receive for thiscondition could be different based on yourdoctor’s advice, your age, how serious yourcondition is, and many other factors.Does the Coverage Examplepredict my future expenses?No. Coverage Examples are not costestimators. You can’t use the examples toestimate costs for an actual condition. Theyare for comparative purposes only. Yourown costs will be different depending onthe care you receive, the prices yourproviders charge, and the reimbursementyour health plan allows.Can I use Coverage Examplesto compare plans?Yes. When you look at the Summary ofBenefits and Coverage for other plans,you’ll find the same Coverage Examples.When you compare plans, check the“Patient Pays” box in each example. Thesmaller that number, the more coveragethe plan provides.Are there other costs I shouldconsider when comparingplans?Yes. An important cost is the premiumyou pay. Generally, the lower yourpremium, the more you’ll pay in out-ofpocketcosts, such as copayments,deductibles, and coinsurance. Youshould also consider contributions toaccounts such as health savings accounts(HSAs), flexible spending arrangements(FSAs) or health reimbursement accounts(HRAs) that help you pay out-of-pocketexpenses.Questions: Call 1-855-333-5730 or visit us at www.anthem.com/ca/sisc . If you aren’t clear about any of the underlined termsused in this form, see the Glossary. You can view the Glossary at www.anthem.com/ca/sisc or call 1-855-333-5730 to request a copy.10 of 10