Echocardiographic Evaluation of Pericardial Disease - Casecag.com
Echocardiographic Evaluation of Pericardial Disease - Casecag.com
Echocardiographic Evaluation of Pericardial Disease - Casecag.com

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
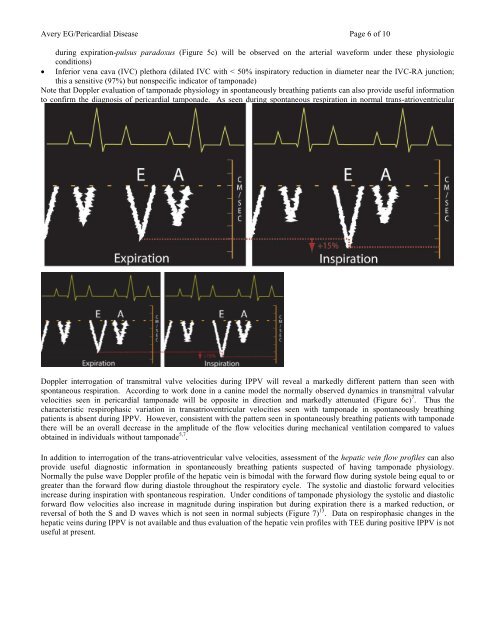
Avery EG/<strong>Pericardial</strong> <strong>Disease</strong> Page 6 <strong>of</strong> 10during expiration-pulsus paradoxus (Figure 5c) will be observed on the arterial waveform under these physiologicconditions)• Inferior vena cava (IVC) plethora (dilated IVC with < 50% inspiratory reduction in diameter near the IVC-RA junction;this a sensitive (97%) but nonspecific indicator <strong>of</strong> tamponade)Note that Doppler evaluation <strong>of</strong> tamponade physiology in spontaneously breathing patients can also provide useful informationto confirm the diagnosis <strong>of</strong> pericardial tamponade. As seen during spontaneous respiration in normal trans-atrioventricularvalve Doppler pr<strong>of</strong>iles there is a decrease in transmitral velocity flow pr<strong>of</strong>iles during inspiration (Figure 2ba). In severetamponade this decrease can be as much as 37% (Figure 6a). The transtricuspid valve velocities increase by as much as 77%with tamponade physiology during spontaneous respiration 13 (Figure 6b). The magnitude <strong>of</strong> the transatrioventricular velocitieswill be reduced in absolute value although the respirophasic variation will be accentuated in pericardial tamponade duringspontaneous respiration. The mechanism accounting for the exaggerated respirophasic variation in tamponade is an insulation<strong>of</strong> the heart from the intrathoracic pressure changes associated with the respiratory cycle.Figure 6a 1 – Spont. Respiration: Tamponade – Transmitral Figure 6b 1 – Spont. Respiration: Tamponade - TranstricuspidFigure 6c 1 – IPPV: Tamponade - TransmitralDoppler interrogation <strong>of</strong> transmitral valve velocities during IPPV will reveal a markedly different pattern than seen withspontaneous respiration. According to work done in a canine model the normally observed dynamics in transmitral valvularvelocities seen in pericardial tamponade will be opposite in direction and markedly attenuated (Figure 6c) 7 . Thus thecharacteristic respirophasic variation in transatrioventricular velocities seen with tamponade in spontaneously breathingpatients is absent during IPPV. However, consistent with the pattern seen in spontaneously breathing patients with tamponadethere will be an overall decrease in the amplitude <strong>of</strong> the flow velocities during mechanical ventilation <strong>com</strong>pared to valuesobtained in individuals without tamponade 5,7 .In addition to interrogation <strong>of</strong> the trans-atrioventricular valve velocities, assessment <strong>of</strong> the hepatic vein flow pr<strong>of</strong>iles can alsoprovide useful diagnostic information in spontaneously breathing patients suspected <strong>of</strong> having tamponade physiology.Normally the pulse wave Doppler pr<strong>of</strong>ile <strong>of</strong> the hepatic vein is bimodal with the forward flow during systole being equal to orgreater than the forward flow during diastole throughout the respiratory cycle. The systolic and diastolic forward velocitiesincrease during inspiration with spontaneous respiration. Under conditions <strong>of</strong> tamponade physiology the systolic and diastolicforward flow velocities also increase in magnitude during inspiration but during expiration there is a marked reduction, orreversal <strong>of</strong> both the S and D waves which is not seen in normal subjects (Figure 7) 13 . Data on respirophasic changes in thehepatic veins during IPPV is not available and thus evaluation <strong>of</strong> the hepatic vein pr<strong>of</strong>iles with TEE during positive IPPV is notuseful at present.