

Dementia
gi2hff
gi2hff
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
GBD region<br />
(green = imputed)<br />
Basic<br />
ADL<br />
Combined<br />
ADL<br />
Australasia 2.0 3.3 2.6<br />
Asia Pacific, High Income 2.0 3.6 2.6<br />
Oceania 3.6 4.6 1.2<br />
Asia, Central 1.2 2.7 3.3<br />
Asia, East 3.6 4.7 1.2<br />
Asia, South 1.3 2.7 2.6<br />
Asia,<br />
South-East<br />
1.3 2.7 2.6<br />
Europe, Western 1.1 3.5 3.3<br />
Europe, Central 2.1 4.4 3.4<br />
Europe, Eastern 2.1 4.4 3.4<br />
North America, High Income 2.1 4.0 2.8<br />
Caribbean 3.0 3.0 2.1<br />
Latin America, Andean 2.9 2.9 2.6<br />
Latin America, Central 1.9 1.9 3.1<br />
Latin America, Southern 2.9 4.4 2.6<br />
Latin America, Tropical 2.9 2.9 2.6<br />
North Africa / Middle East 1.0 1.4 2.8<br />
Sub-Saharan Africa, Central 2.0 3.6 2.6<br />
Sub-Saharan Africa, East 2.0 3.6 2.6<br />
Sub-Saharan Africa,<br />
Southern<br />
2.0 3.6 2.6<br />
Sub-Saharan Africa, West 2.0 3.6 2.6<br />
All 2.0 3.6 2.6<br />
Supervision<br />
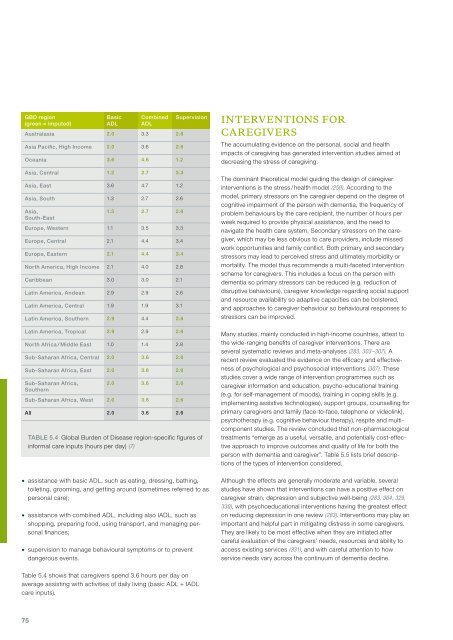
Table 5.4 Global Burden of Disease region-specific figures of<br />
informal care inputs (hours per day) (7)<br />
Interventions for<br />
caregivers<br />
The accumulating evidence on the personal, social and health<br />
impacts of caregiving has generated intervention studies aimed at<br />
decreasing the stress of caregiving.<br />
The dominant theoretical model guiding the design of caregiver<br />
interventions is the stress / health model (259). According to the<br />
model, primary stressors on the caregiver depend on the degree of<br />
cognitive impairment of the person with dementia, the frequency of<br />
problem behaviours by the care recipient, the number of hours per<br />
week required to provide physical assistance, and the need to<br />
navigate the health care system. Secondary stressors on the caregiver,<br />
which may be less obvious to care providers, include missed<br />
work opportunities and family conflict. Both primary and secondary<br />
stressors may lead to perceived stress and ultimately morbidity or<br />
mortality. The model thus recommends a multi-faceted intervention<br />
scheme for caregivers. This includes a focus on the person with<br />
dementia so primary stressors can be reduced (e.g. reduction of<br />
disruptive behaviours), caregiver knowledge regarding social support<br />
and resource availability so adaptive capacities can be bolstered,<br />
and approaches to caregiver behaviour so behavioural responses to<br />
stressors can be improved.<br />
Many studies, mainly conducted in high-income countries, attest to<br />
the wide-ranging benefits of caregiver interventions. There are<br />
several systematic reviews and meta-analyses (283, 303–307). A<br />
recent review evaluated the evidence on the efficacy and effectiveness<br />
of psychological and psychosocial interventions (307). These<br />
studies cover a wide range of intervention programmes such as<br />
caregiver information and education, psycho-educational training<br />
(e.g. for self-management of moods), training in coping skills (e.g.<br />
implementing assistive technologies), support groups, counselling for<br />
primary caregivers and family (face-to-face, telephone or videolink),<br />
psychotherapy (e.g. cognitive behaviour therapy), respite and multicomponent<br />
studies. The review concluded that non-pharmacological<br />
treatments “emerge as a useful, versatile, and potentially cost-effective<br />
approach to improve outcomes and quality of life for both the<br />
person with dementia and caregiver”. Table 5.5 lists brief descriptions<br />
of the types of intervention considered.<br />
• assistance with basic ADL, such as eating, dressing, bathing,<br />
toileting, grooming, and getting around (sometimes referred to as<br />
personal care);<br />
• assistance with combined ADL, including also IADL, such as<br />
shopping, preparing food, using transport, and managing personal<br />
finances;<br />
• supervision to manage behavioural symptoms or to prevent<br />
dangerous events.<br />
Although the effects are generally moderate and variable, several<br />
studies have shown that interventions can have a positive effect on<br />
caregiver strain, depression and subjective well-being (283, 304, 329,<br />
330), with psychoeducational interventions having the greatest effect<br />
on reducing depression in one review (283). Interventions may play an<br />
important and helpful part in mitigating distress in some caregivers.<br />
They are likely to be most effective when they are initiated after<br />
careful evaluation of the caregivers’ needs, resources and ability to<br />
access existing services (331), and with careful attention to how<br />
service needs vary across the continuum of dementia decline.<br />
Table 5.4 shows that caregivers spend 3.6 hours per day on<br />
average assisting with activities of daily living (basic ADL + IADL<br />
care inputs).<br />
75