RESidENcy PROGRAM Scholarly and Community Medicine Projects
RESidENcy PROGRAM Scholarly and Community Medicine Projects
RESidENcy PROGRAM Scholarly and Community Medicine Projects

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
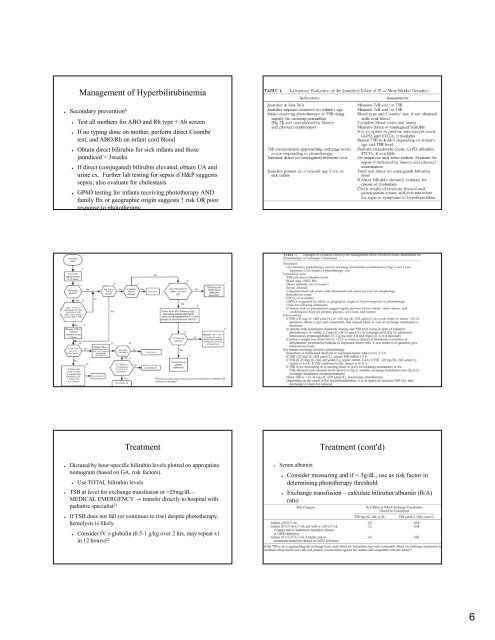
Management of Hyperbilirubinemia<br />
● Secondary prevention 6<br />
● Test all mothers for ABO <strong>and</strong> Rh type + Ab screen<br />
● If no typing done on mother, perform direct Coombs'<br />
test, <strong>and</strong> ABO/Rh on infant cord blood<br />
● Obtain direct bilirubin for sick infants <strong>and</strong> those<br />
jaundiced > 3weeks<br />
● If direct (conjugated) bilirubin elevated, obtain UA <strong>and</strong><br />
urine cx. Further lab testing for sepsis if H&P suggests<br />
sepsis; also evaluate for cholestasis<br />
● GP6D testing for infants receiving phototherapy AND<br />
family Hx or geographic origin suggests ↑ risk OR poor<br />
response to phototherapy<br />
Treatment<br />
● Dictated by hour-specific bilirubin levels plotted on appropriate<br />
nomogram (based on GA, risk factors).<br />
● Use TOTAL bilirubin levels<br />
● TSB at level for exchange transfusion or >25mg/dL –<br />
MEDICAL EMERGENCY → transfer f di directly l to hhospital i lwith i h<br />
pediatric specialist21 ● If TSB does not fall (or continues to rise) despite phototherapy,<br />
hemolysis is likely<br />
● Consider IV γ-globulin (0.5-1 g/kg over 2 hrs, may repeat x1<br />
in 12 hours) 22<br />
● Serum albumin<br />
Treatment (cont'd)<br />
● Consider measuring <strong>and</strong> if < 3g/dL, use as risk factor in<br />
determining phototherapy threshold<br />
● Exchange transfusion – calculate bilirubin/albumin (B/A)<br />
ratio<br />
6