Focus on implants - Nobel Biocare
Focus on implants - Nobel Biocare
Focus on implants - Nobel Biocare

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
98<br />
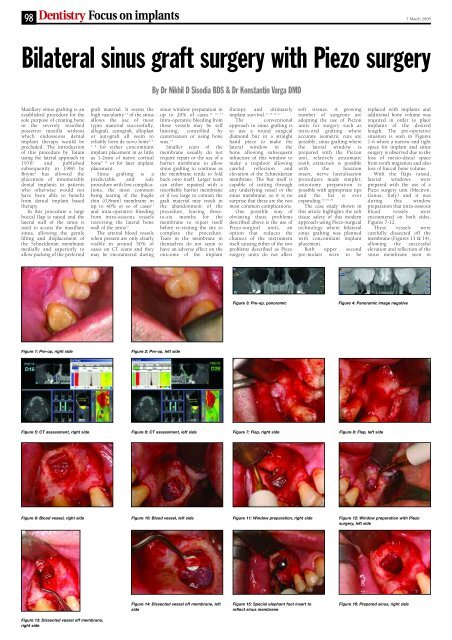
Bilateral sinus graft surgery with Piezo surgery<br />
Maxillary sinus grafting is an<br />
established procedure for the<br />
sole purpose of creating b<strong>on</strong>e<br />
in the severely resorbed<br />
posterior maxilla without<br />
which endosseous dental<br />
implant therapy would be<br />
precluded. The introducti<strong>on</strong><br />
of this procedure by Tatum<br />
using the lateral approach in<br />
1976 1 and published<br />
subsequently in 1980 by<br />
Boyne 2 has allowed the<br />
placement of innumerable<br />
dental <strong>implants</strong> in patients<br />
who otherwise would not<br />
have been able to benefit<br />
from dental implant based<br />
therapy.<br />
In this procedure a large<br />
buccal flap is raised and the<br />
lateral wall of the sinus is<br />
used to access the maxillary<br />
sinus, allowing the gentle<br />
lifting and displacement of<br />
the Schneiderian membrane<br />
medially and superiorly to<br />
allow packing of the preferred<br />
Figure 1: Pre-op, right side<br />
<str<strong>on</strong>g>Focus</str<strong>on</strong>g> <strong>on</strong> <strong>implants</strong><br />
graft material. It seems the<br />
high vascularity 3, 4 of the sinus<br />
allows the use of most<br />
types material successfully,<br />
allograft, zenograft, alloplast<br />
or autograft all seem to<br />
reliably form de novo b<strong>on</strong>e<br />
5, 6,<br />
7, 8 for either c<strong>on</strong>comitant<br />
implant placement in as little<br />
as 1-2mm of native cortical<br />
b<strong>on</strong>e 9, 10 or for later implant<br />
placement.<br />
Sinus grafting is a<br />
predictable and safe<br />
procedure with few complicati<strong>on</strong>s,<br />
the most comm<strong>on</strong><br />
being tearing of the fragile<br />
thin (0.8mm) membrane in<br />
up to 40% or so of cases 11<br />
and intra-operative bleeding<br />
from intra-osseous vessels<br />
traversing the lateral b<strong>on</strong>e<br />
wall of the sinus 12 .<br />
The arterial blood vessels<br />
when present are <strong>on</strong>ly clearly<br />
visible in around 50% of<br />
cases <strong>on</strong> CT scans and they<br />
may be encountered during<br />
By Dr Nikhil D Sisodia BDS & Dr K<strong>on</strong>stantin Varga DMD<br />
sinus window preparati<strong>on</strong> in<br />
12, 13, 14<br />
up to 20% of cases.<br />
Intra-operative bleeding from<br />
these vessels may be self<br />
limiting, c<strong>on</strong>trolled by<br />
cauterisati<strong>on</strong> or using b<strong>on</strong>e<br />
wax. 14<br />
Smaller tears of the<br />
membrane usually do not<br />
require repair or the use of a<br />
barrier membrane to allow<br />
sinus grafting to c<strong>on</strong>tinue as<br />
the membrane tends to fold<br />
back <strong>on</strong>to itself. Larger tears<br />
can either repaired with a<br />
resorbable barrier membrane<br />
or if too large to c<strong>on</strong>tain the<br />
graft material may result in<br />
the aband<strong>on</strong>ment of the<br />
procedure, leaving threeto-six<br />
m<strong>on</strong>ths for the<br />
membrane to repair itself<br />
before re-visiting the site to<br />
complete the procedure.<br />
Tears in the membrane in<br />
themselves do not seem to<br />
have an adverse effect <strong>on</strong> the<br />
outcome of the implant<br />
therapy and ultimately<br />
11, 15, 16, 17<br />
implant survival.<br />
The c<strong>on</strong>venti<strong>on</strong>al<br />
approach in sinus grafting is<br />
to use a round surgical<br />
diam<strong>on</strong>d bur in a straight<br />
hand piece to make the<br />
lateral window in the<br />
b<strong>on</strong>e allowing subsequent<br />
infracture of this window to<br />
make a trapdoor allowing<br />
careful reflecti<strong>on</strong> and<br />
elevati<strong>on</strong> of the Schneiderian<br />
membrane. The bur itself is<br />
capable of cutting through<br />
any underlying vessel or the<br />
sinus membrane; so it is no<br />
surprise that these are the two<br />
most comm<strong>on</strong> complicati<strong>on</strong>s.<br />
One possible way of<br />
obviating these problems<br />
described above is the use of<br />
Piezo-surgical units, an<br />
opti<strong>on</strong> that reduces the<br />
chances of the instrument<br />
itself causing either of the two<br />
problems described as Piezo<br />
surgery units do not affect<br />
soft tissues. A growing<br />
number of surge<strong>on</strong>s are<br />
adopting the use of Piez<strong>on</strong><br />
units for surgery such as<br />
intra-oral grafting where<br />
accurate isometric cuts are<br />
possible, sinus grafting where<br />
the lateral window is<br />
prepared with the Piez<strong>on</strong><br />
unit, relatively atraumatic<br />
tooth extracti<strong>on</strong> is possible<br />
with the luxati<strong>on</strong><br />
insert, nerve lateralisati<strong>on</strong><br />
procedures made simpler,<br />
osteotomy preparati<strong>on</strong> is<br />
possible with appropriate tips<br />
and the list is ever<br />
expanding.<br />
18, 19, 20<br />
The case study shown in<br />
this article highlights the soft<br />
tissue safety of this modern<br />
approach using Piezo-surgical<br />
technology where bilateral<br />
sinus grafting was planned<br />
with c<strong>on</strong>comitant implant<br />
placement.<br />
Both upper sec<strong>on</strong>d<br />
pre-molars were to be<br />
Figure 5: CT assessment, right side Figure 6: CT assessment, left side Figure 7: Flap, right side<br />
Figure 8: Flap, left side<br />
7 March 2008<br />
replaced with <strong>implants</strong> and<br />
additi<strong>on</strong>al b<strong>on</strong>e volume was<br />
required in order to place<br />
<strong>implants</strong> of the desired<br />
length. The pre-operative<br />
situati<strong>on</strong> is seen in Figures<br />
1-6 where a narrow and tight<br />
space for implant and sinus<br />
surgery is observed due to the<br />
loss of mesio-distal space<br />
from tooth migrati<strong>on</strong> and also<br />
loss of buccal b<strong>on</strong>e volume.<br />
With the flaps raised,<br />
lateral windows were<br />
prepared with the use of a<br />
Piezo surgery unit (Mectr<strong>on</strong>,<br />
Genoa, Italy) and it was<br />
during this window<br />
preparati<strong>on</strong> that intra-osseous<br />
blood vessels were<br />
encountered <strong>on</strong> both sides,<br />
Figures 7-12.<br />
These vessels were<br />
carefully dissected off the<br />
membrane (Figures 13 & 14),<br />
allowing the successful<br />
elevati<strong>on</strong> and reflecti<strong>on</strong> of the<br />
sinus membrane seen in<br />
Figure 9: Blood vessel, right side Figure 10: Blood vessel, left side Figure 11: Window preparati<strong>on</strong>, right side Figure 12: Window preparati<strong>on</strong> with Piezo<br />
surgery, left side<br />
Figure 13: Dissected vessel off membrane,<br />
right side<br />
Figure 2: Pre-op, left side<br />
Figure 14: Dissected vessel off membrane, left<br />
side<br />
Figure 3: Pre-op, panoramic Figure 4: Panoramic image negative<br />
Figure 15: Special elephant foot insert to<br />
reflect sinus membrane<br />
Figure 16: Prepared sinus, right side
7 March 2008 <str<strong>on</strong>g>Focus</str<strong>on</strong>g> <strong>on</strong> <strong>implants</strong> 99<br />
Figure 17: Prepared sinus,<br />
left side<br />
Figures 15, 16 & 17.<br />
Once the membrane had<br />
been elevated, osteotomies<br />
were prepared for the<br />
simultaneous placement of<br />
two <strong>implants</strong> (SPI implant,<br />
Alpha Bio, Israel, modified<br />
and marketed as <strong>Nobel</strong>Active<br />
by <strong>Nobel</strong><strong>Biocare</strong>), Figures<br />
18 & 19.<br />
With the osteotomies<br />
prepared, the sinuses were<br />
both packed with large<br />
particulate Bio-Oss (Geistlich<br />
Biomaterials, Wolhusen,<br />
Switzerland), Figures 20 &<br />
21. The two <strong>implants</strong> were<br />
then placed by hand with<br />
excellent primary stability<br />
and closed over with cover<br />
screws, Figures 22- 25.<br />
The lateral windows were<br />
covered with a bovine<br />
peri-cardium membrane<br />
(Tutogen Medical GmbH,<br />
Germany) and the flaps<br />
sutured with tensi<strong>on</strong> free<br />
closure, Figures 26-29.<br />
The post-operative periapical<br />
radiographs, Figures<br />
30 & 31, show a good<br />
positi<strong>on</strong> and volume of tissue<br />
around the <strong>implants</strong> for later<br />
restorati<strong>on</strong> <strong>on</strong>ce integrated.<br />
Although experienced<br />
surge<strong>on</strong>s will not have any<br />
problems handling these<br />
frequently encountered<br />
problems, even less experienced,<br />
but properly trained<br />
surge<strong>on</strong>s should be able to<br />
perform these and other<br />
surgical procedures with a<br />
greater degree of safety. 19<br />
The advantage of Piezo<br />
surgery is that it creates a<br />
virtually blood free operating<br />
area increasing visibility and<br />
minimal heat is generated by<br />
the inserts, minimising<br />
necrosis due to cellular<br />
damage. One slight drawback<br />
may be that it is slower than<br />
c<strong>on</strong>venti<strong>on</strong>al approaches, but<br />
the advantages far outweigh<br />
this slight inc<strong>on</strong>venience.<br />
References<br />
Figure 18: Implant osteotomy, right side Figure 19: Implant<br />
osteotomy, left side<br />
Figure 21: Graft placement, left side Figure 22: Alpha bio SPI implant placement, Figure 23: Alpha bio SPI implant<br />
placement, left side<br />
Figure 25: Stable implant and graft in situ,<br />
left side<br />
1. Tatum H. Maxillary and<br />
sinus implant rec<strong>on</strong>structi<strong>on</strong>s.<br />
Dent Clin. North Am. 1986;<br />
30:207-29<br />
2. Boyne P, James R. Grafting<br />
of th maxillary sinus floor<br />
with autogenous marrow and<br />
b<strong>on</strong>e. J Oral Surg. 1980; 38:613-<br />
6<br />
3. Traxler H, Windisch A,<br />
Geyerhofer U, Surd R, Solar P,<br />
Firbas W. Arterial blood supply<br />
of the maxillary sinus. Clin Anat.<br />
1999; 12(6):417-21<br />
4. Solar P, Geyerhofer U,<br />
Traxler H, Windisch A, Ulm C,<br />
Watzek G. Blood supply to the<br />
Figure 26: Bovine pericardium membrane,<br />
right side<br />
maxillary sinus relevant to sinus<br />
floor elevati<strong>on</strong> procedures. Clin<br />
Oral Implants Res. 1999;<br />
10(1):34-44<br />
5. Lundgren S, Anderss<strong>on</strong><br />
S, Gualini F, Sennerby L. B<strong>on</strong>e<br />
reformati<strong>on</strong> with sinus membrane<br />
elevati<strong>on</strong>. Clinical Implant Dentistry<br />
and Related Research.<br />
2004; 6(3):165-73<br />
6. Yeung R, Jin L, Pang M,<br />
Pow E. Human histologic and<br />
electromicroscopic analysis with<br />
synthetic peptide enhanced<br />
hydroxyapatite in the maxillary<br />
sinus elevati<strong>on</strong> procedure.<br />
Implant Dentistry. 2005;<br />
14(3):237-39<br />
7. Degidi M, Piattelli M,<br />
Scarano A, Iezzi G, Piattelli A.<br />
Maxillary sinus augmentati<strong>on</strong><br />
with a synthetic cell-binding peptide:<br />
Histological and histomorphometrical<br />
results in humans. J<br />
Oral Implantology. 2004;<br />
30(6):376-83<br />
8. Fugazzotto P, Vlassis J.<br />
Report of 1633 <strong>implants</strong> inn 814<br />
augmented sinus areas in functi<strong>on</strong><br />
for up to 180 m<strong>on</strong>ths.<br />
Implant Dentistry. 2007;<br />
16(4):369-75<br />
9. Peleg M, Mazor Z,<br />
Chaushu G, Garg A. Sinus floor<br />
augmentati<strong>on</strong> with simultaneous<br />
implant placement in the severely<br />
resorbed atrophic maxilla. J Period<strong>on</strong>tol.<br />
1998; 69:1397-1403<br />
Figure 27: Bovine pericardium membrane,<br />
left side<br />
Figure 29: Flap closure, left side Figure 30: Post-op radiograph, right side Figure 31: Post-op radiograph, left side<br />
10. Mazor Z, Peleg M, Gross<br />
M. Sinus augmentati<strong>on</strong> for single<br />
tooth replacement in the posterior<br />
maxilla. Int J Oral Maxillofac<br />
Implants. 1999; 14:55-60<br />
11. Schwartz-Arad D,<br />
Herzberg R, Dolev E. The prevelance<br />
of surgical complicati<strong>on</strong>s of<br />
the sinus procedure and their<br />
impact <strong>on</strong> implant survival. J<br />
Period<strong>on</strong>tol. 2004; 75(4):511-6<br />
12. Elian N, Wallace S, Cho<br />
SC, Jalbout ZN, Froum S. Distributi<strong>on</strong><br />
of the maxillary artery as it<br />
relates to sinus floor augmentati<strong>on</strong>.<br />
Int J Oral Maxillofac<br />
Implants. 2005; 20(5):784-7<br />
13. Mardinger O, Abba M,<br />
Hirschberg A, Schwartz-Arad D.<br />
Prevelance, diameter and course<br />
of the maxilary intraosseous vascular<br />
canal with relati<strong>on</strong> to sinus<br />
augmentati<strong>on</strong> procedure: a radiographic<br />
study. Int J Maxillofac<br />
Surg. 2007; 36(8):735-8<br />
14. Flanagan D. Arterial<br />
supply of maxillary sinus and<br />
potential for bleedin complicati<strong>on</strong><br />
during lateral approach sinus<br />
elevati<strong>on</strong>. Implant Dentistry.<br />
2005; 14(4):336-8<br />
15. Karabuda C, Arisan V,<br />
Hakan O. Effects of sinus membrane<br />
perforati<strong>on</strong>s <strong>on</strong> the success<br />
of dental <strong>implants</strong> placed in the<br />
augmented sinus. J Period<strong>on</strong>tol.<br />
2006; 77(12): 1991-7<br />
16. Bar<strong>on</strong>e A, Santini S,<br />
Sbord<strong>on</strong>e L, Crespi R, Covani U.<br />
A clinical study of the outcomes<br />
and complicati<strong>on</strong>s associated<br />
with maxillary sinus augmentati<strong>on</strong>.<br />
Int J Oral Maxillofac<br />
Implants. 2006; 21(1):81-5<br />
17. Ardekian L, Oved-Peleg<br />
E, Mactei E, Peled M. The clinical<br />
significance of sinus membrane<br />
perforati<strong>on</strong> during<br />
augmentati<strong>on</strong> of the maxillary<br />
sinus. J Oral Maxillofac Surgery.<br />
2006; 64(2):277-82<br />
18. Happe A. Use of a<br />
piezoelectric surgical device to<br />
Figure 20: Graft placement, right side<br />
Figure 24: Stable implant and graft in situ, right<br />
Figure 28: Flap closure, right side<br />
harvest b<strong>on</strong>e grafts from the<br />
mandibular ramus: report of 40<br />
cases. Int J Period<strong>on</strong>tics and<br />
Restorative Dentistry. 2007;<br />
27(3):241-9<br />
19. Schlee M, Steigmann M,<br />
Bratu E, Garg A. Piezosurgery:<br />
basics and possibilities. Implant<br />
Dentistry. 2006; 15(4):334-8<br />
20. Lee H, Ahn M, Sohn D.<br />
Piezoelectric distracti<strong>on</strong> osteogenesis<br />
in the atrophic maxillary<br />
anterior area: a case report.<br />
Implant Dentistry. 2007;<br />
16(3):227-32.<br />
Dr Nikhil Sisodia BDS qualified from<br />
Bristol University in 1995. Following<br />
a year as a Senior House Officer in<br />
Restorative Dentistry and several years<br />
in general practice in L<strong>on</strong>d<strong>on</strong>, he<br />
found his passi<strong>on</strong>s were in the<br />
cosmetic and advanced restorative<br />
field, which led him to undertake<br />
further courses in the UK and abroad.<br />
He is an active member of the<br />
American Academy of Cosmetic<br />
Dentistry, Associati<strong>on</strong> of Dental<br />
Implantology, a Fellow of the Internati<strong>on</strong>al C<strong>on</strong>gress of Oral<br />
Implantology and is currently Country Chairman (UK) for the<br />
European Society of Cosmetic Dentistry. Nik is also an active<br />
member of the British Academy of Cosmetic Dentistry and<br />
serves <strong>on</strong> the Board of Directors as Chairman of the C<strong>on</strong>gress<br />
Committee. Dr K<strong>on</strong>stantin Varga DMD, Master of Oral<br />
Medicine in Implantology, practises in private practice in<br />
Torquay, Dev<strong>on</strong>..