Clinical evaluation of monitor unit software and the application of ...
Clinical evaluation of monitor unit software and the application of ...
Clinical evaluation of monitor unit software and the application of ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
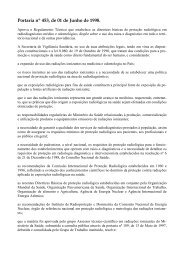
DEVIATION [%]<br />
6%<br />
4%<br />
2%<br />
0%<br />
-2%<br />
-4%<br />
-6%<br />
-8%<br />
-10%<br />
Pelvic fields<br />
(157)<br />
fields were checked for step-<strong>and</strong>-shoot IMRT delivery <strong>and</strong><br />
dynamic MLC IMRT delivery. Mean deviations (incl. st<strong>and</strong>ard<br />
deviations) between MUV <strong>and</strong> <strong>the</strong> local TPS were<br />
1.0 ± 7.3% for dynamic IMRT delivery <strong>and</strong> 1.3 ± 3.2% for<br />
step-<strong>and</strong>-shoot IMRT delivery, respectively. Step-<strong>and</strong>-shoot<br />
IMRT results in <strong>the</strong> thorax were again biased by tissue inhomogeneity;<br />
no dynamic IMRT was performed in <strong>the</strong> thoracic<br />
region. For dynamic IMRT cases in <strong>the</strong> pelvis good agreement<br />
was obtained between MUV <strong>and</strong> <strong>the</strong> local TPS (mean:<br />
1.6 ± 1.5%).<br />
In order to verify IMRT fields against ionisation chamber<br />
measurements <strong>and</strong> to compare <strong>the</strong> achievable accuracy<br />
for IM fields with <strong>the</strong> one for open beams, a few treatment<br />
plans were recalculated in a homogeneous phantom with<br />
both MUV <strong>and</strong> <strong>the</strong> TPS. In o<strong>the</strong>r words, recalculated IMRT<br />
verification plans were considered in this part. Table 4 summarizes<br />
<strong>the</strong> results for open static beams <strong>and</strong> IMRT cases,<br />
both on an individual field basis <strong>and</strong> for composite treatment<br />
plans. These results confirm <strong>the</strong> high accuracy <strong>of</strong> <strong>the</strong><br />
independent dose/MU calculation s<strong>of</strong>tware MUV in homogeneous<br />
conditions, i.e. when comparing ionisation chamber<br />
measurements with dose calculations in identical conditions<br />
D. Georg et al. / Radio<strong>the</strong>rapy <strong>and</strong> Oncology 85 (2007) 306–315 311<br />
Thoracic fields<br />
(65)<br />
Head & neck<br />
fields (83)<br />
Fig. 2. Illustration <strong>of</strong> <strong>the</strong> improvements for radiological depth corrections at <strong>the</strong> field level. Median <strong>and</strong> quartiles for pelvic fields (total 157),<br />
thoracic fields (total 65) <strong>and</strong> head-<strong>and</strong>-neck fields (total 83) when using geometric or radiological depth for independent dose calculations<br />
(filled circles...with radiological path length correction, filled diamonds...all data).<br />
Table 3<br />
Summary <strong>of</strong> deviations between MUV <strong>and</strong> <strong>the</strong> local treatment planning system, as a function <strong>of</strong> conformal treatment technique <strong>and</strong><br />
treatment site (RL... radiological depth)<br />
Pelvic fields Thorax fields Head-<strong>and</strong>-neck fields<br />
All data RL data All data RL data All data RL data<br />
Open beams 0.5 ± 1.3% (273) 0.6 ± 1.3% (107) 2.6 ± 7.6% (95) 1.6 ± 2.2% (51) 0.5 ± 2.1% (75) 1.0 ± 1.1% (45)<br />
Physical wedges 0.9 ± 2.3% (46) 1.3 ± 2.6% (31) 1.1 ± 1.0% (17) 1.2 ± 0.9% (8) 0.6 ± 1.5% (48) 1.1 ± 1.5% (24)<br />
Dynamic wedges 0.2 ± 2.6% (38) 1.3 ± 1.5% (19) 3.2 ± 7.8% (36) 0.6 ± 2.5% (6) 0.0 ± 2.0% (22) 0.3 ± 1.4% (14)<br />
The numbers in brackets indicate <strong>the</strong> total number <strong>of</strong> fields per category<br />
in a water phantom or a solid verification phantom without<br />
homogeneities. There are, however, additional uncertainties<br />
in both TPS calculations <strong>and</strong> calculations performed<br />
with MUV, due to <strong>the</strong> extent <strong>and</strong> accuracy in modelling<br />
rounded leaf ends, tongue-<strong>and</strong>-groove effects, leaf transmission<br />
or <strong>the</strong> distribution <strong>of</strong> <strong>the</strong> direct source (X-ray target).<br />
When compared to open beams, larger mean<br />
deviations <strong>and</strong> st<strong>and</strong>ard deviations for individual IMRT fields<br />
(see Table 4a) are also influenced by <strong>the</strong> larger overall<br />
experimental uncertainty for ionisation chamber measurements<br />
in IMRT treatments [24]. Large relative deviations<br />
are also influenced by <strong>the</strong> beam contribution to <strong>the</strong> overall<br />
treatment plan <strong>and</strong> for composite treatment plans excellent<br />
agreement was found between ionisation chamber measurements<br />
<strong>and</strong> calculations performed with MUV, see Table 4b.<br />
<strong>Clinical</strong> action levels<br />
Fig. 3a <strong>and</strong> b show treatment site dependent frequency<br />
distributions <strong>of</strong> deviations between MUV <strong>and</strong> TPS calculations.<br />
The dashed lines indicate a deviation level <strong>of</strong> ±3% or<br />
±5%. For all treatment sites <strong>the</strong>re were systematic deviations<br />
which are biased by dose calculation uncertainties