- Page 1 and 2:
UNIVERSITE SIDI MOHAMMED BEN ABDELL
- Page 3 and 4:
3.2.2.e-Techniques chirurgicales ..
- Page 5 and 6:
2.4-Ostéite ......................
- Page 7 and 8:
Les fractures-luxations de la chevi
- Page 9 and 10:
I-MATERIEL D’ETUDE : Notre étude
- Page 11 and 12:
• Ouverture cutanée oui non •
- Page 13 and 14:
5-Résultats : • Recul • Délai
- Page 15 and 16:
I- DONNEES EPIDEMIOLOGIQUES 1- REPA
- Page 17 and 18:
3- REPARTITION SELON LE COTE ATTEIN
- Page 19 and 20:
II- MECANISME La précision du méc
- Page 21 and 22:
Nous les avons classées selon la c
- Page 23 and 24:
IV- ETUDE ANATOMOPATHOLOGIQUE Il ex
- Page 25 and 26:
Nous nous sommes basés dans l'étu
- Page 27 and 28:
Réduction et ostéosynthèse (trai
- Page 29 and 30:
La répartition des ostéosynthèse
- Page 31 and 32:
VI- COMPLICATIONS POST-OPERATOIRES
- Page 33 and 34:
VII- RESULTATS FONCTIONNELS 1- CRIT
- Page 35 and 36:
2- RESULTATS GLOBAUX Sans tenir com
- Page 37:
I-Rappels anatomique et biomécaniq
- Page 41 and 42:
2. Rappel biomécanique : La chevil
- Page 43 and 44:
comme le confirment certaines lési
- Page 46 and 47:
II-EPIDEMIOLOGIE 1-FREQUENCE Les FL
- Page 48 and 49:
III-ETIOLOGIES : Les circonstances
- Page 50 and 51:
Dans près de la moitié des cas, l
- Page 52 and 53:
V-ETUDE RADIO-CLINIQUE: 1. ETUDE CL
- Page 54 and 55:
Radiographie d’une cheville norma
- Page 56 and 57:
2-2-2. Tomographies : Les tomograph
- Page 58 and 59:
A B C Classification de WEBER • C
- Page 60 and 61:
En fait, toutes ces classifications
- Page 62 and 63:
Classification de Ruedi et Heim (AO
- Page 64 and 65:
Hourlier , en 1981, et Vives , en 1
- Page 66 and 67:
La classification adoptée dans not
- Page 68 and 69:
Tableau IX : Les fractures de l’a
- Page 70 and 71:
signification évolutive ne tient p
- Page 72 and 73:
Cette classification est intéressa
- Page 74 and 75:
VII- DELAI OPERATOIRE : Le délai d
- Page 76 and 77: 1-REDUCTION DE LA LUXATION (38,53,8
- Page 78 and 79: Le parage chirurgical est un temps
- Page 80 and 81: Tableau XIII : Types de traitement
- Page 82 and 83: Photo 1 : Situation anatomique des
- Page 84 and 85: Photo 4 : situation de la voie d'ab
- Page 86 and 87: Le traitement chirurgical a fait ap
- Page 88 and 89: type III. Il a été associé à un
- Page 90 and 91: Photos 9 :Restitution de la longueu
- Page 92 and 93: L’immobilisation est assurée au
- Page 94 and 95: Le Tableau XIV récapitule quelques
- Page 96 and 97: • Aux interventions tardives. 2-
- Page 98 and 99: IX- COMPLICATIONS : La FLC présent
- Page 100 and 101: En fait, le risque infectieux est c
- Page 102 and 103: Tableau VIIIX: Facteurs qui augment
- Page 104 and 105: • Voies d’abord mal choisies. L
- Page 106 and 107: A : fracture totale communitive B :
- Page 108 and 109: Parmi les facteurs étiologiques me
- Page 110 and 111: littérature et semble même plus s
- Page 112 and 113: hyperpulsabilité artérielle. Ses
- Page 114 and 115: 3. Principes de l’examen kinésit
- Page 116 and 117: Conclusion 115
- Page 118 and 119: ICONOGRAPHIE 117
- Page 120 and 121: Photo 3 :Fracture bimalléolaire av
- Page 122 and 123: Photo 7 : FLC avec fracture de l'as
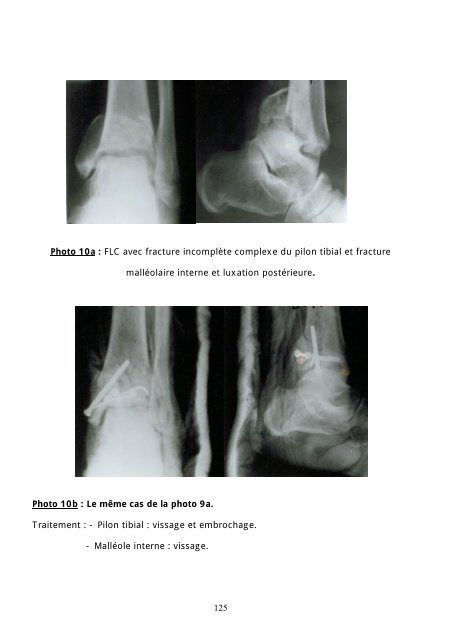
- Page 124 and 125: Photo 8b : Le même cas que celui d
- Page 128 and 129: Photo 12 :syndrome algodystrophique
- Page 130 and 131: RESUME 129
- Page 132 and 133: SUMMARY Sixty one cases of the ankl
- Page 134 and 135: BIBLIOGRAPHIE 133
- Page 136 and 137: 7. ANTHONY N,ACELLO G,WALLACE,NICHO
- Page 138 and 139: 19. BIGA N,DEFIVES T Fractures mall
- Page 140 and 141: 31. CESARI B,LORTAT-JACOB A,DINH A
- Page 142 and 143: 44. DEJEAN O Fracture bimalléolair
- Page 144 and 145: 57. GAGNEUX E,GERARD F Traitement d
- Page 146 and 147: J Chir (Paris) 1978 ;115,5 :289 70.
- Page 148 and 149: 83. LEVY B.A,VOGT K,HERRERA D,AND C
- Page 150 and 151: 95. MORVAN G Points de radio anatom
- Page 152 and 153: 107. RIEUNAU G Fractures bimalléol
- Page 154: 120. VARANGO G, KODO M, BAMBA I, LA