La documentazione sanitaria e sociale in RSA - Provincia di Mantova
La documentazione sanitaria e sociale in RSA - Provincia di Mantova
La documentazione sanitaria e sociale in RSA - Provincia di Mantova

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
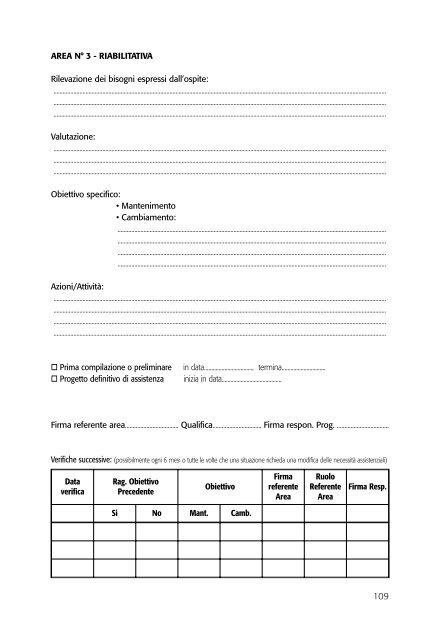
AREA N° 3 - RIABILITATIVA<br />
Rilevazione dei bisogni espressi dall’ospite:<br />
..........................................................................................................................................................................................................................<br />
..........................................................................................................................................................................................................................<br />
..........................................................................................................................................................................................................................<br />
Valutazione:<br />
..........................................................................................................................................................................................................................<br />
..........................................................................................................................................................................................................................<br />
..........................................................................................................................................................................................................................<br />
Obiettivo specifico:<br />
• Mantenimento<br />
• Cambiamento:<br />
................................................................................................................................................................................<br />
................................................................................................................................................................................<br />
................................................................................................................................................................................<br />
................................................................................................................................................................................<br />
Azioni/Attività:<br />
..........................................................................................................................................................................................................................<br />
..........................................................................................................................................................................................................................<br />
..........................................................................................................................................................................................................................<br />
..........................................................................................................................................................................................................................<br />
Prima compilazione o prelim<strong>in</strong>are<br />
Progetto def<strong>in</strong>itivo <strong>di</strong> assistenza<br />
<strong>in</strong> data.................................. term<strong>in</strong>a..............................<br />
<strong>in</strong>izia <strong>in</strong> data.........................................<br />
Firma referente area................................... Qualifica................................ Firma respon. Prog. ..................................<br />
Verifiche successive: (possibilmente ogni 6 mesi o tutte le volte che una situazione richieda una mo<strong>di</strong>fica delle necessità assistenziali)<br />
Data<br />
verifica<br />
Rag. Obiettivo<br />
Precedente<br />
Obiettivo<br />
Firma<br />
referente<br />
Area<br />
Ruolo<br />
Referente<br />
Area<br />
Firma Resp.<br />
Si No Mant. Camb.<br />
109