Boğaziçi Tıp Dergisi
Boğaziçi Tıp Dergisi Cilt: 4 Sayı: 1 Yıl: 2017
Boğaziçi Tıp Dergisi Cilt: 4 Sayı: 1 Yıl: 2017

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Rohat Ak et al.<br />
BOĞAZİÇİ TIP DERGİSİ; 2017; 4 (1): 35-36<br />
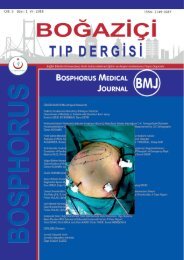
Figure 1: Brain CT scan of subarachnoid hemorrhage.<br />
DISCUSSION<br />
NPE is a clinical diagnosis based upon the<br />
occurrence of pulmonary edema in the appropriate<br />
setting and in the absence of a more<br />
likely alternative cause (3). In our patient sudden<br />
dyspnea and hypoxia developed after 6<br />
hours of SAH symptoms. The lack of diagnostic<br />
markers for special etiologies contributes<br />
to poor recognition and diagnosis wordwide.<br />
The reported prevalences for NPE after SAH<br />
are changing between 10%-40% (4). This range<br />
may be minimized by more recognition of<br />
ED doctors. The pathophysiologic mechanisms<br />
are thought to be pulmonary capillary pressure<br />
increase by transient pulmonary vasoconstriction<br />
after cerebrovascular accident, and/or in<br />
the pulmonary capillary bed, increased permeability<br />
reproduced by inflammatory mediators.<br />
In addition contributions of the hypothalamus,<br />
elevated intracranial pressure, and activation of<br />
the sympathoadrenal system may play role (5).<br />
In emergency departments, physicians should<br />
be alert of clinical presentation consisting of<br />
signs of oxygenation failure, such as dyspnea,<br />
tachypnea, tachycardia, cyanosis, pink frothy<br />
sputum, and crackles and rales on auscultation<br />
in patients with SAH (6). NPE must be kept<br />
in mind if bilateral, symmetric, smooth and<br />
diffuse, alveolar edema-like infiltrates were<br />
present in the chest radiography or thorax CT<br />
and PaO2/fraction of inspired oxygen is