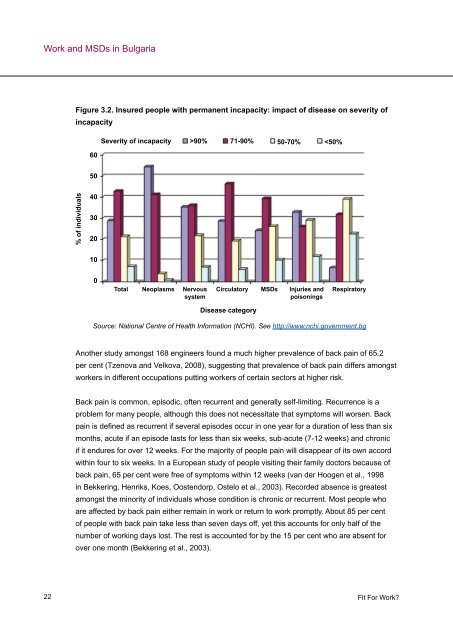
<strong>Work</strong> and MSDs in Bulgaria 22 Figure 3.2. Insured people with permanent incapacity: impact of disease on severity of incapacity % of individuals 60 50 40 30 20 10 0 Severity of incapacity >90% 71-90% 50-70%
<strong>Work</strong> and MSDs in Bulgaria It is important to recognise that there is a difference between having symptoms, care seeking, lost productivity and disability, and the factors that contribute to them (Burton, 2005). This means that whilst individuals may experience musculoskeletal pain (in their back, <strong>for</strong> example), it is not possible to predict their strategies <strong>for</strong> dealing with illness or injury (seeking medical attention <strong>for</strong> example), how it will affect their work per<strong>for</strong>mance, whether they will take time off work and whether, ultimately, they will become one of the very small minority who become permanently disabled by their condition. The important question is there<strong>for</strong>e why, when so many people experience back pain, does it have such an adverse effect on some and not others? There is a growing consensus that psychological factors are the differentiating factor as they are strongly associated with the progression of back pain from an acute to a chronic condition that affects two to seven per cent of people (Burton, 2005), to becoming a disability (Burton, 2005; Bekkering et al., 2003). 3.2.2 <strong>Work</strong>-related upper limb disorders According to the fourth EWCS (Parent-Thirion et al., 2007), 30.3 per cent of <strong>Bulgarian</strong> workers <strong>report</strong> that they have experienced muscular pain in their neck, shoulders and upper limbs. Kostova and Koleva (2001) estimated the prevalence rates of cervicobrachial syndrome (characterised by stiffness and neck pain, also radiating to the arms) amongst workers in a fertilizer plant to be 16.2 per cent <strong>for</strong> those over 40, and 10 per cent <strong>for</strong> those less than 40 years of age. As in the case of low back pain, prevalence was higher <strong>for</strong> women than <strong>for</strong> men (22.9 per cent compared with 8.3 per cent). WRULDs are MSDs affecting the upper part of the body caused or aggravated by work and the working environment. However, there is considerable debate about the definition and diagnostic criteria <strong>for</strong> WRULDs, which are also commonly referred to as ‘sprains or strains’, ‘repetitive strain injuries or disorders’, or ‘cumulative trauma disorders’. Both specific and nonspecific disorders and symptoms can be covered by this category. Van Eerd, Beaton, Cole, Lucas, Hogg-Johnson et al. (2003) identified 27 different classification systems <strong>for</strong> work-related MSDs, of which no two were found to be alike. The fact that a single disorder is often described in different ways only amplifies the problem. Critically, van Eerd et al. (2003) found that the different classification systems did not agree on which disorders should be included. This definitional problem makes it difficult to calculate the number of people with WRULDs and to develop a common understanding of the associated risk factors. Whilst no agreed classification exists there is a common consensus that symptoms of WRULDs can present in the tendons, muscles, joints, blood vessels and/or the nerves and may include pain, discom<strong>for</strong>t, numbness, and tingling sensations in the affected area. WRULDs can be specific and non-specific conditions (Aptel, Aublet-Cuvelier and Cnockaert 2002) and attempts <strong>Fit</strong> For <strong>Work</strong>? 23
- Page 1 and 2: Fit For Work? Rosemary Thomas Kseni
- Page 3 and 4: Contents 1. Executive summary 5 2.
- Page 5 and 6: 1. Executive summary The ‘Fit for
- Page 7 and 8: What can be done? Executive summary
- Page 9 and 10: Executive summary We have found imp
- Page 11 and 12: Increasing work intensity is a very
- Page 13 and 14: 2.2 MSDs: The European context Intr
- Page 15 and 16: 2.4 A note on definition Introducti
- Page 17 and 18: 2.5 Structure of the report Introdu
- Page 19 and 20: Figure 3.1. Number of MSDs inpatien
- Page 21: • Stamina and resilience; • Cog
- Page 25 and 26: of RA and specific leukocyte antige
- Page 27 and 28: injuries or back pain 15 ; Sieper,
- Page 29 and 30: 2001). The study also found that fo
- Page 31 and 32: • Local or whole-body exposure to
- Page 33 and 34: workers of developing rheumatoid ar
- Page 35 and 36: 3.4 The wider economic and social i
- Page 37 and 38: Work and MSDs in Bulgaria Direct co
- Page 39 and 40: presented in the Table 3.3 below. T
- Page 41 and 42: 3.5 Summary Work and MSDs in Bulgar
- Page 43 and 44: Job retention and return to work pr
- Page 45 and 46: 4.2 The social security regime for
- Page 47 and 48: Further indirect costs of disabilit
- Page 49 and 50: 4.3 Conditionspecific interventions
- Page 51 and 52: RA in Bulgaria who receive biologic
- Page 53 and 54: Interventions Since it was first pr
- Page 55 and 56: apart from norms of shift work. 43
- Page 57 and 58: Box 2. Case Study - EPIQ Electronic
- Page 59 and 60: the beliefs that both parties have
- Page 61 and 62: 4.6 Summary 4.5.4 Improved employer
- Page 63 and 64: 5.1 Recommendations for employers 5
- Page 65 and 66: 5.3 Recommendations for GPs and spe
- Page 67 and 68: Conclusions and recommendations •
- Page 69 and 70: Breen, A., Langworthy, J. and Bagus
- Page 71 and 72: der Tempel, H. and van der Linden,
- Page 73 and 74:
Guzman, J., Esmail, R., Karjalainen
- Page 75 and 76:
References Nachemson, A., Waddell,
- Page 77 and 78:
Waddell, G. and Burton, A. K., (200
- Page 79 and 80:
Appendix 2: Sample ‘Fit’ Note S
- Page 81 and 82:
Sources: Eurostat Statistical Datab
- Page 83 and 84:
Sources: Parent-Thirion, Fernández
- Page 85 and 86:
Hourly labour costs 2007 Average ho
- Page 87 and 88:
% sickness absence due to health re
- Page 89 and 90:
Appendix 3: Benchmarking grid Refer
- Page 91 and 92:
The aim of the project is to stimul
- Page 93 and 94:
Appendix 4: Fit for Work Europe Wha
- Page 96:
We provide: Research Advisory Consu