

use of tumor markers in testicular, prostate, colorectal, breast, and ...
use of tumor markers in testicular, prostate, colorectal, breast, and ...
use of tumor markers in testicular, prostate, colorectal, breast, and ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Tumor Markers <strong>in</strong> Testicular Cancers 9<br />
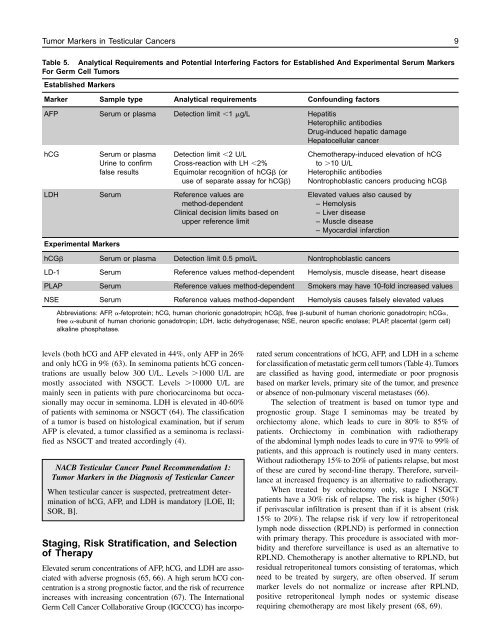
Table 5. Analytical Requirements <strong>and</strong> Potential Interfer<strong>in</strong>g Factors for Established And Experimental Serum Markers<br />
For Germ Cell Tumors<br />
Established Markers<br />
Marker Sample type Analytical requirements Confound<strong>in</strong>g factors<br />
AFP Serum or plasma Detection limit 1 g/L Hepatitis<br />
Heterophilic antibodies<br />
Drug-<strong>in</strong>duced hepatic damage<br />
Hepatocellular cancer<br />
hCG Serum or plasma Detection limit 2 U/L Chemotherapy-<strong>in</strong>duced elevation <strong>of</strong> hCG<br />
Ur<strong>in</strong>e to confirm Cross-reaction with LH 2% to 10 U/L<br />
false results Equimolar recognition <strong>of</strong> hCG (or Heterophilic antibodies<br />
<strong>use</strong> <strong>of</strong> separate assay for hCG) Nontrophoblastic cancers produc<strong>in</strong>g hCG<br />
LDH Serum Reference values are Elevated values also ca<strong>use</strong>d by<br />
method-dependent – Hemolysis<br />
Cl<strong>in</strong>ical decision limits based on – Liver disease<br />
upper reference limit – Muscle disease<br />
– Myocardial <strong>in</strong>farction<br />
Experimental Markers<br />
hCG Serum or plasma Detection limit 0.5 pmol/L Nontrophoblastic cancers<br />
LD-1 Serum Reference values method-dependent Hemolysis, muscle disease, heart disease<br />
PLAP Serum Reference values method-dependent Smokers may have 10-fold <strong>in</strong>creased values<br />
NSE Serum Reference values method-dependent Hemolysis ca<strong>use</strong>s falsely elevated values<br />
Abbreviations: AFP, -fetoprote<strong>in</strong>; hCG, human chorionic gonadotrop<strong>in</strong>; hCG, free -subunit <strong>of</strong> human chorionic gonadotrop<strong>in</strong>; hCG,<br />
free -subunit <strong>of</strong> human chorionic gonadotrop<strong>in</strong>; LDH, lactic dehydrogenase; NSE, neuron specific enolase; PLAP, placental (germ cell)<br />
alkal<strong>in</strong>e phosphatase.<br />
levels (both hCG <strong>and</strong> AFP elevated <strong>in</strong> 44%, only AFP <strong>in</strong> 26%<br />
<strong>and</strong> only hCG <strong>in</strong> 9% (63). In sem<strong>in</strong>oma patients hCG concentrations<br />
are usually below 300 U/L. Levels 1000 U/L are<br />
mostly associated with NSGCT. Levels 10000 U/L are<br />
ma<strong>in</strong>ly seen <strong>in</strong> patients with pure choriocarc<strong>in</strong>oma but occasionally<br />
may occur <strong>in</strong> sem<strong>in</strong>oma. LDH is elevated <strong>in</strong> 40-60%<br />
<strong>of</strong> patients with sem<strong>in</strong>oma or NSGCT (64). The classification<br />
<strong>of</strong> a <strong>tumor</strong> is based on histological exam<strong>in</strong>ation, but if serum<br />
AFP is elevated, a <strong>tumor</strong> classified as a sem<strong>in</strong>oma is reclassified<br />
as NSGCT <strong>and</strong> treated accord<strong>in</strong>gly (4).<br />
NACB Testicular Cancer Panel Recommendation 1:<br />
Tumor Markers <strong>in</strong> the Diagnosis <strong>of</strong> Testicular Cancer<br />
When <strong>testicular</strong> cancer is suspected, pretreatment determ<strong>in</strong>ation<br />
<strong>of</strong> hCG, AFP, <strong>and</strong> LDH is m<strong>and</strong>atory [LOE, II;<br />
SOR, B].<br />
Stag<strong>in</strong>g, Risk Stratification, <strong>and</strong> Selection<br />
<strong>of</strong> Therapy<br />
Elevated serum concentrations <strong>of</strong> AFP, hCG, <strong>and</strong> LDH are associated<br />
with adverse prognosis (65, 66). A high serum hCG concentration<br />
is a strong prognostic factor, <strong>and</strong> the risk <strong>of</strong> recurrence<br />
<strong>in</strong>creases with <strong>in</strong>creas<strong>in</strong>g concentration (67). The International<br />
Germ Cell Cancer Collaborative Group (IGCCCG) has <strong>in</strong>corpo-<br />
rated serum concentrations <strong>of</strong> hCG, AFP, <strong>and</strong> LDH <strong>in</strong> a scheme<br />
for classification <strong>of</strong> metastatic germ cell <strong>tumor</strong>s (Table 4). Tumors<br />
are classified as hav<strong>in</strong>g good, <strong>in</strong>termediate or poor prognosis<br />
based on marker levels, primary site <strong>of</strong> the <strong>tumor</strong>, <strong>and</strong> presence<br />
or absence <strong>of</strong> non-pulmonary visceral metastases (66).<br />
The selection <strong>of</strong> treatment is based on <strong>tumor</strong> type <strong>and</strong><br />
prognostic group. Stage I sem<strong>in</strong>omas may be treated by<br />
orchiectomy alone, which leads to cure <strong>in</strong> 80% to 85% <strong>of</strong><br />
patients. Orchiectomy <strong>in</strong> comb<strong>in</strong>ation with radiotherapy<br />
<strong>of</strong> the abdom<strong>in</strong>al lymph nodes leads to cure <strong>in</strong> 97% to 99% <strong>of</strong><br />
patients, <strong>and</strong> this approach is rout<strong>in</strong>ely <strong>use</strong>d <strong>in</strong> many centers.<br />
Without radiotherapy 15% to 20% <strong>of</strong> patients relapse, but most<br />
<strong>of</strong> these are cured by second-l<strong>in</strong>e therapy. Therefore, surveillance<br />
at <strong>in</strong>creased frequency is an alternative to radiotherapy.<br />
When treated by orchiectomy only, stage I NSGCT<br />
patients have a 30% risk <strong>of</strong> relapse. The risk is higher (50%)<br />
if perivascular <strong>in</strong>filtration is present than if it is absent (risk<br />
15% to 20%). The relapse risk if very low if retroperitoneal<br />
lymph node dissection (RPLND) is performed <strong>in</strong> connection<br />
with primary therapy. This procedure is associated with morbidity<br />
<strong>and</strong> therefore surveillance is <strong>use</strong>d as an alternative to<br />
RPLND. Chemotherapy is another alternative to RPLND, but<br />
residual retroperitoneal <strong>tumor</strong>s consist<strong>in</strong>g <strong>of</strong> teratomas, which<br />
need to be treated by surgery, are <strong>of</strong>ten observed. If serum<br />
marker levels do not normalize or <strong>in</strong>crease after RPLND,<br />
positive retroperitoneal lymph nodes or systemic disease<br />
requir<strong>in</strong>g chemotherapy are most likely present (68, 69).













