Full Clinical Guidelines - Community First Health Plans.
Full Clinical Guidelines - Community First Health Plans.
Full Clinical Guidelines - Community First Health Plans.

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
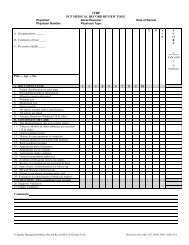
CHILDREN’S SERVICES HANDBOOK<br />
P<br />
h<br />
y<br />
s<br />
i<br />
c<br />
a<br />
l<br />
O<br />
t<br />
h<br />
e<br />
r<br />
P<br />
r<br />
o<br />
b<br />
l<br />
e<br />
m<br />
s<br />
Do you have any concerns about these things? ❑ Yes ❑ No<br />
If you think your child may have a health problem, has he/she seen a doctor<br />
or nurse about the problem? ❑ Yes ❑ No<br />
❑ Has daytime wetting<br />
❑ Soils pants<br />
❑ Will not eat<br />
❑ Has headaches<br />
❑ Has lost or gained a lot of weight<br />
❑ Has sleeping problems, nightmares, sleep-walking, early waking<br />
❑ Vomits (throws up) often<br />
❑ Has stomach aches often<br />
❑ Lacks energy<br />
Is this child accident-prone? ❑ Yes ❑ No<br />
Is anything causing your family stress right now? ❑ Yes ❑ No<br />
Has this child or his/her parents been subject to neglect, physical, sexual, or emotional abuse? If yes, what from?<br />
_____________________ When? ________ ❑ Yes ❑ No<br />
Treatment initiated? ❑ Yes ❑ No<br />
Is this child at risk for out-of-home placement because of behavior problems? ❑ Yes ❑ No<br />
Comments: (Please write anything else you want us to know about in this space.)<br />
Date: ____________<br />
Signature: ______________________________________________________<br />
Relation to patient: _______________________________________________<br />
CH-323<br />
CPT ONLY - COPYRIGHT 2010 AMERICAN MEDICAL ASSOCIATION. ALL RIGHTS RESERVED.<br />
H EALTH PLANS<br />
www.cfhp.com<br />
129