


You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
CONTINUING EDUCATION AND TRAINING<br />
Gain 2 CET credits - enter online at www.otcet.co.uk or by post<br />
corneal swelling to a level comparable to<br />
normal overnight swelling, thus<br />
reintroducing <strong>the</strong> option of fitting ScCLs<br />
without <strong>the</strong> complicating impact of<br />
incorporating a fenestration 3,4,5 .<br />
Advantages and<br />
disadvantages of ScCLs<br />
Advantages<br />
The large size creates a scleral bearing surface<br />
and retains a pre-corneal fluid reservoir<br />
providing optical neutralisation of an astigmatic<br />
or irregular corneal surface and<br />
corneal hydration. Very high powers, up to<br />
+/- 40.00D, are possible because <strong>the</strong>re are<br />
minimal lid traction and centre of gravity<br />
effects. They cannot be dislodged by <strong>the</strong> lids<br />
and are often relatively comfortable even<br />
for <strong>the</strong> unadapted eye because <strong>the</strong> lid<br />
margin is in contact with <strong>the</strong> surface of <strong>the</strong><br />
lens ra<strong>the</strong>r than <strong>the</strong> edge. If RGP non-ventilated<br />
ScCLs are used, corneal contact can be<br />
minimal.<br />
ScCLs, including RGP lenses, can be kept<br />
dry when not being worn. There is no risk of<br />
contaminated storage solutions since none<br />
is used, so <strong>the</strong> risk of infections is reduced.<br />
They are robust, <strong>the</strong> surface can be polished<br />
or resurfaced periodically, and <strong>the</strong>y are not<br />
easily lost. Less dextrous patients may<br />
find <strong>the</strong>m easier to handle because <strong>the</strong>y do<br />
not need to be precariously balanced<br />
on a fingertip.<br />
Disadvantages<br />
While not producing any lid sensation, <strong>the</strong>re<br />
is a feeling and an appearance of bulk, and<br />
some people are intimidated by <strong>the</strong>ir large<br />
size. They cover a large area of <strong>the</strong> anterior<br />
globe, considerably reducing <strong>the</strong> oxygen<br />
available to <strong>the</strong> cornea, although <strong>the</strong> introduction<br />
of RGP materials has led to a major<br />
improvement. Because <strong>the</strong>y are fitted with<br />
corneal clearance, <strong>the</strong> VA and <strong>the</strong> ability of<br />
<strong>the</strong> lens to reduce distortions in ectatic<br />
corneal conditions may be reduced compared<br />
to rigid corneal lenses. However, if an<br />
RGP ScCL can be worn when a corneal lens<br />
cannot, <strong>the</strong> comparison is not valid.<br />
Indications<br />
ScCLs are indicated simply when <strong>the</strong> unique<br />
advantages of ScCLs can be applied. They<br />
can be considered to manage any eye condition<br />
if <strong>the</strong>re is a strong enough reason for<br />
contact lens correction, and in <strong>the</strong> management<br />
of some ocular surface disease. There<br />
have been a number of publications in<br />
recent years describing ScCL applications.<br />
6,7,8,9,10,11,12,13,14,15,16,17,18<br />
Irregular or abnormal<br />
corneal topography<br />
Corneal ectasia<br />
Keratoconus or o<strong>the</strong>r primary corneal<br />
ectasias (PCE) form <strong>the</strong> majority of current<br />
indications for ScCLs. RGP corneal lenses<br />
Figure 2 Irregular corneal topography<br />
as a consequence of a transplant that has<br />
unexpectedly sprung forward. There is a<br />
clear depression in <strong>the</strong> superior<br />
mid-periphery which would be a major<br />
problem for corneal lens fitting. A nonventilated<br />
RGP ScCL is unaffected by a<br />
localised irregularity like this provided it is<br />
sealed on <strong>the</strong> sclera<br />
may be simply impossible to fit in very<br />
advanced cases, for example, as shown in<br />
Figure 1, but <strong>the</strong>re is also an application for<br />
ScCLs when corneal lenses persistently<br />
dislodge, or are not well tolerated due to<br />
excessive mobility or <strong>the</strong> formation of<br />
epi<strong>the</strong>lial erosions.<br />
Corneal transplant<br />
The second largest group for which ScCLs<br />
are indicated are post-corneal transplants if<br />
<strong>the</strong>re is a residual refractive error, or if <strong>the</strong><br />
surface remains irregular, illustrated in<br />
Figure 2. Even if <strong>the</strong> astigmatism is very<br />
high, which still happens sometimes even<br />
with <strong>the</strong> most expert surgery, non-ventilated<br />
RGP ScCL fitting post-transplant is usually<br />
a comparatively straightforward exercise.<br />
The lenses are fitted with full corneal<br />
clearance irrespective of corneal topography,<br />
<strong>the</strong>refore <strong>the</strong> appearance is much <strong>the</strong><br />
same whe<strong>the</strong>r <strong>the</strong> cylinder is 2.00D or in<br />
excess of 20.00D.<br />
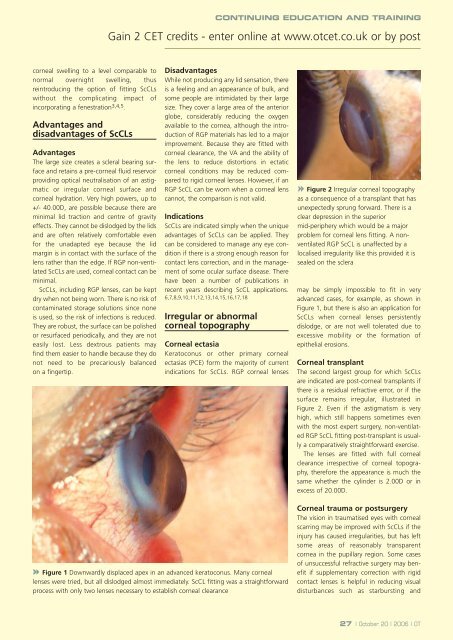
Figure 1 Downwardly displaced apex in an advanced keratoconus. Many corneal<br />
lenses were tried, but all dislodged almost immediately. ScCL fitting was a straightforward<br />
process with only two lenses necessary to establish corneal clearance<br />
Corneal trauma or postsurgery<br />
The vision in traumatised eyes with corneal<br />
scarring may be improved with ScCLs if <strong>the</strong><br />
injury has caused irregularities, but has left<br />
some areas of reasonably transparent<br />
cornea in <strong>the</strong> pupillary region. Some cases<br />
of unsuccessful refractive surgery may benefit<br />
if supplementary correction with rigid<br />
contact lenses is helpful in reducing visual<br />
disturbances such as starbursting and<br />
27 | October 20 | 2006 | OT













