Download e-copy - Smile Dental Journal
Download e-copy - Smile Dental Journal
Download e-copy - Smile Dental Journal

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
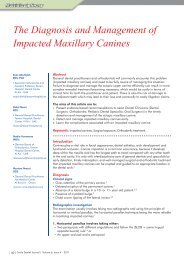
Neutral Zone in Complete Dentures:<br />
Systematic Analysis of Evidence and Technique<br />
• Ahmad A. Jum’ah, BDS(Hons), MSc/PhD (Clin) Student-Second year<br />
Restorative Dentistry Department, Leeds <strong>Dental</strong> Institute, University of Leeds, UK<br />
dnaahj@leeds.ac.uk<br />
• Peter J. Nixon, Senior Consultant in Restorative Dentistry, Leeds <strong>Dental</strong> Hospital,<br />
Leeds Teaching Hospitals Trust (LTHT), England, UK<br />
Abstract<br />
Neutral zone technique is a physiologic and functional approach that is widely and concisely described as a treatment<br />
modality for unstable lower complete denture cases. It serves as a guide of where to set teeth and how to contour the<br />
polished surface of the denture to ensure optimal stability, retention, facial support and aesthetics. In patients with<br />
compromised support and poor denture adaptability, this technique is considered as a valuable tool in the prosthodontist’s<br />
armoury especially where dental implants are contraindicated or unfeasible. The aim of this article is to describe the concept<br />
and technique of neutral zone, discuss rationale, indications and to evaluate this technique from evidence-based perspective.<br />
Abbreviations: NZ: Neutral zone, CD: complete denture, VDO: Vertical dimension at occlusion.<br />
Introduction<br />
Stability of lower CDs is well recognized as a potentially<br />
difficult treatment aim to achieve. Looseness and discomfort<br />
are the most frequent complaints reported by patients and<br />
they are quite often difficult to manage by dentists.<br />
Neuromuscular control is said to be the key determinant<br />
of stability of lower CD as the area available for support is<br />
far less than maxillary support area. Size and position of<br />
prosthetic teeth and the contours of polished surface have<br />
a crucial role in lower CD stability as they are subjected to<br />
destabilizing forces from the tongue, lips and cheeks if they<br />
are placed in hindrance with function of these structures. 1<br />
Throughout time, many concepts and theories emerged<br />
to describe where prosthetic teeth of CD should<br />
be positioned. Some of them adopted mechanical<br />
principles, 2,3 others used biometric guides 4 and a minority<br />
advocated mathematical formulas based on natural teeth<br />
position and dimensions. 5 These dogmatic or arbitrary<br />
approaches have been challenged and found insufficient,<br />
in fact not only by rigorous research, but also by failure<br />
to restore function, aesthetic and comfort in patients with<br />
severely atrophic mandibular ridges (Class V Atwood’s 6 ),<br />
patients with enlarged tongue and cases of marginal or<br />
segmental mandibulectomy. To overcome such problem,<br />
the neutral zone technique was advocated.<br />
The neutral zone, zone of minimal conflict, 7 zone of<br />
equilibrium, 8 potential denture space 9 and the dead<br />
space 10 are all terms used to describe the potential area<br />
where forces generated in an outward direction from the<br />
tongue are being neutralized or balanced by the inward<br />
forces generated by lips and cheeks during functional<br />
activities. Setting teeth and contouring polished surface<br />
of lower CD within this zone, makes the prosthesis less<br />
subjected to dislodging forces and adds more to stability. 11<br />
Analysis of functional forces<br />
Understanding the unique and synergistic interplay<br />
and complex movements of muscles of cheeks, lips<br />
and tongue is the first step in construction of lower<br />
CD that is stabilized rather than being dislodged by<br />
movements of these structures. 11,12 Description of forces<br />
applied to the lower CD purely on the basis of direction<br />
is an oversimplification, yet, it is quite useful for better<br />
understanding of the concept. 12<br />
The outward forces are principally generated by the<br />
tongue and lingual frenum into which, genioglossus<br />
muscle is inserted. Teeth should be set and flanges should<br />
be contoured in harmony with tongue size, position and<br />
shape during rest and function. In rest position, the tongue<br />
rests on lingual cusps of posterior teeth and lingual<br />
flanges posteriorly and anteriorly. The tongue space<br />
determined by position of teeth is far more important<br />
during function. Setting teeth too lingualy will encroach<br />
on this space and the tongue tends to dislodge denture<br />
in function. The height of posterior teeth is of a great<br />
importance in stability of lower CD as well. Having the<br />
tongue resting on lingual cusps will reduce the horizontal<br />
(outward) force and apply force with vertical (downward)<br />
component which enhances stability and retention. 11<br />
Inward forces are generated by cheeks resulting from<br />
contraction of the buccinator muscle that pushes food<br />
bullous on top of occlusal surfaces of posterior teeth.<br />
Flanges contoured and teeth set too buccal are at<br />
increased risk of being dislodged by the action of this<br />
muscle. Anteriorly, lip muscles (mentalis and orbicularis<br />
oris) are the source of inward forces generated during<br />
speaking and swallowing. Contraction of these muscles<br />
to attain seal during these activities can destabilize lower<br />
CD with teeth and flanges placed too far labially. The<br />
modiolus is a knot-like structure found in corners of the<br />
| 8 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011