6 steps beyond the 5 Whys - AMMJ
6 steps beyond the 5 Whys - AMMJ
6 steps beyond the 5 Whys - AMMJ

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Diving deeper:<br />
6 <strong>steps</strong> <strong>beyond</strong><br />
<strong>the</strong> 5 <strong>Whys</strong>
Introduction<br />
When an incident or accident occurs at your workplace, what do<br />
you do to fix <strong>the</strong> problem?<br />
The “5 <strong>Whys</strong> process” is a common method to identify causes of<br />
<strong>the</strong> incident. But what do you do if this technique only presents<br />
fur<strong>the</strong>r symptoms ra<strong>the</strong>r than <strong>the</strong> real root causes?<br />
This eBook presents a useful method for taking <strong>the</strong> analysis<br />
fur<strong>the</strong>r than <strong>the</strong> 5 <strong>Whys</strong> process. The 6 <strong>steps</strong> <strong>beyond</strong> <strong>the</strong> 5 <strong>Whys</strong><br />
presents a logical framework for getting to <strong>the</strong> bottom of any<br />
incident or accident in your workplace.
The 5 <strong>Whys</strong> process<br />
At a mine site in far north Queensland, a freight train sits idle on <strong>the</strong><br />
track. For some reason, <strong>the</strong> train cannot be loaded with its coal, and is<br />
causing a costly stoppage at <strong>the</strong> mine facility. The mine operator needs<br />
to know what’s stopping <strong>the</strong> normal loading procedure.<br />
A starting point might be to run with <strong>the</strong> 5 <strong>Whys</strong> process, whereby you<br />
start asking questions – typically, at least 5 – about what happened.<br />
Why can’t <strong>the</strong> train be loaded?<br />
Because <strong>the</strong> loading conveyor belt has stopped.<br />
Why has <strong>the</strong> loading conveyor stopped?<br />
Because <strong>the</strong> drive motor on <strong>the</strong> conveyor pulley has tripped out.<br />
Why has <strong>the</strong> drive motor tripped out?<br />
Because <strong>the</strong>re was an overload on <strong>the</strong> drive motor.<br />
Why was <strong>the</strong>re an overload on <strong>the</strong> drive motor?<br />
Because <strong>the</strong> main bearing had seized.<br />
Why has <strong>the</strong> main bearing seized?<br />
Because <strong>the</strong>re was no lubrication in <strong>the</strong> bearing.<br />
By asking 5 simple questions, <strong>the</strong> mine operator arrives at a tangible<br />
solution: ensuring that bearings in <strong>the</strong> drive motor are adequately<br />
lubricated. As this simple example demonstrates, <strong>the</strong> 5 <strong>Whys</strong> process<br />
could potentially be sufficient as a simple form of root cause analysis,<br />
with no fur<strong>the</strong>r investigation needed.<br />
Yet, while investigators could use <strong>the</strong> 5 <strong>Whys</strong> process as a starting point,<br />
<strong>the</strong>y may however soon see <strong>the</strong> need to take <strong>the</strong> investigation fur<strong>the</strong>r.
A good first analysis…<br />
but is it enough?<br />
In some cases <strong>the</strong> 5 <strong>Whys</strong>’ linear nature can<br />
cause people to jump to conclusions and fail to<br />
arrive at <strong>the</strong> true cause or causes of an incident<br />
or accident. While <strong>the</strong> 5 <strong>Whys</strong> technique can be<br />
successfully used for very basic investigations, it<br />
does have a few limitations which any investigator<br />
should be aware of before using it.<br />
The limitations of <strong>the</strong> 5 <strong>Whys</strong> process include:<br />
• Tendency to stop at symptoms ra<strong>the</strong>r than<br />
finding lower level root causes<br />
• Inability to go <strong>beyond</strong> <strong>the</strong> investigator’s current<br />
knowledge – you can’t find causes for things<br />
you don’t already know<br />
• Lack of support to help <strong>the</strong> investigator to ask<br />
<strong>the</strong> right “why” questions<br />
• Results aren’t repeatable – different people<br />
often come up with different causes for <strong>the</strong><br />
same problem<br />
• Branching can occur – indicating that a more<br />
in-depth analysis is needed to get to <strong>the</strong> root<br />
cause<br />
Given that <strong>the</strong> 5 <strong>Whys</strong> process may not be enough,<br />
what follows? What should an investigator do<br />
when a more thorough, structured investigation is<br />
needed?
6 <strong>steps</strong> <strong>beyond</strong><br />
<strong>the</strong> 5 <strong>Whys</strong><br />
If <strong>the</strong> 5 <strong>Whys</strong> process does not deliver <strong>the</strong> right answers, <strong>the</strong>n it would be<br />
pertinent to enact <strong>the</strong> following 6 <strong>steps</strong> for a more rigorous investigation of <strong>the</strong><br />
incident or accident. Try to do this as soon as possible, particularly step one.<br />
Collect more information<br />
Assemble <strong>the</strong> team<br />
Conduct <strong>the</strong> RCA<br />
Implement <strong>the</strong> solution<br />
(corrective actions)<br />
Measure <strong>the</strong> success of<br />
<strong>the</strong> corrective actions<br />
Advertise your successes
Collect more<br />
information
Collect more information<br />
Without <strong>the</strong> right information,<br />
assumptions and guesswork can lead<br />
you astray in your understanding of a<br />
problem… and will deliver no certainty<br />
in <strong>the</strong> outcomes of corrective actions.<br />
To really understand a problem, you need plenty of evidence.<br />
And you need it as soon as possible.<br />
As soon you identify that <strong>the</strong> 5 <strong>Whys</strong> process is not sufficient<br />
to resolve an incident, you should trigger an urgent search for<br />
more information. This becomes <strong>the</strong> first step <strong>beyond</strong> <strong>the</strong> 5<br />
<strong>Whys</strong>.<br />
Assign a person to <strong>the</strong> task of collecting as much information<br />
relating to <strong>the</strong> incident as possible. Put simply, <strong>the</strong> more<br />
information you have, <strong>the</strong> better off you’ll be.<br />
By acting quickly, <strong>the</strong> quality and quantity of <strong>the</strong> information<br />
you collect will be more consistent. A delay of hours – or,<br />
even worse, days – will negatively impact on <strong>the</strong> quality of <strong>the</strong><br />
information you ga<strong>the</strong>r, and hence <strong>the</strong> subsequent analysis<br />
could be hindered.
Collect more information<br />
Protect your information by<br />
cordoning off an area. Don’t allow<br />
people to touch or interfere with<br />
important evidence.<br />
Get statements from everyone who<br />
saw or had anything to do with<br />
<strong>the</strong> problem. A delay in ga<strong>the</strong>ring<br />
statements allows people to<br />
think about and rationalise what<br />
<strong>the</strong>y saw. The information in <strong>the</strong><br />
statements will subsequently<br />
change and people will be hard<br />
pressed to stick to <strong>the</strong> facts or be<br />
able to recognise <strong>the</strong> changes that<br />
have been made from what <strong>the</strong>y<br />
originally saw.<br />
Top tips<br />
• Act quickly to ga<strong>the</strong>r as much information as you can<br />
• The more evidence you can collect, <strong>the</strong> better<br />
• Assign one person to <strong>the</strong> job of collecting evidence<br />
• Don’t throw evidence away when cleaning up after an<br />
incident… make sure you save it!
Assemble<br />
<strong>the</strong> team
Assemble <strong>the</strong> team<br />
The team may need to be available for<br />
a significant period of time – so you’ll<br />
need <strong>the</strong> backing of management.<br />
Get <strong>the</strong> right people toge<strong>the</strong>r – people with <strong>the</strong> knowledge and<br />
experience to help you understand <strong>the</strong> problem.<br />
Assembling <strong>the</strong> team may take a few days or longer, but it is<br />
important. Without <strong>the</strong> right people, your investigation will lack<br />
<strong>the</strong> specific detail you need – resulting in a more generic report,<br />
which resembles a Failure Modes Effects Analysis (FMEA)<br />
that lists all possible causes with no real insight into <strong>the</strong> root<br />
causes.<br />
With <strong>the</strong> right people on board, your analysis will dive<br />
sufficiently deep to arrive at a workable solution.<br />
So who do you need to get? You want people who bring<br />
experience across different – yet relevant – job roles and people<br />
who have direct knowledge of <strong>the</strong> incident. Pick people with<br />
open minds who are willing to listen, to contribute and will<br />
help <strong>the</strong> investigation. These people should possess specific,<br />
relevant understanding of <strong>the</strong> issue - which will help you to<br />
arrive at a specific solution.
Assemble <strong>the</strong> team<br />
Assign a skilled and experienced<br />
facilitator who is adept at<br />
controlling a group and keeping<br />
<strong>the</strong> investigation on track – without<br />
bias. Be wary of appointing a<br />
subject matter expert as <strong>the</strong>y may<br />
steer <strong>the</strong> group in a particular<br />
direction and who is going to argue<br />
with <strong>the</strong> subject matter expert?<br />
Top tips<br />
• Get management support to bring <strong>the</strong> people you need<br />
to <strong>the</strong> team, for as long as is needed<br />
• Appoint a skilled and experienced facilitator<br />
• The number of people should reflect <strong>the</strong> complexity of<br />
<strong>the</strong> incident<br />
• You may need an independent expert<br />
to join <strong>the</strong> team
Conduct <strong>the</strong> Root<br />
Cause Analysis
Conduct <strong>the</strong> Root Cause Analysis<br />
During <strong>the</strong> RCA, <strong>the</strong> facilitator should<br />
be inclusive, ask all <strong>the</strong> questions<br />
that need to be asked, and pursue<br />
all causal pathways to <strong>the</strong>ir logical<br />
conclusions<br />
Your goal is to conduct <strong>the</strong> RCA as soon as possible after <strong>the</strong> incident or<br />
accident occurs – so that <strong>the</strong> information is still fresh in people’s minds<br />
and remains untainted.<br />
Appoint a time and place for <strong>the</strong> investigation to occur, as soon as <strong>the</strong><br />
required group can be convened. Then, once <strong>the</strong> group meets, set basic<br />
ground rules around respecting o<strong>the</strong>rs’ opinions and encouraging an<br />
open dialogue.<br />
The first task in an RCA is to define <strong>the</strong> problem. Add context to <strong>the</strong><br />
problem by including information about when and where it happened,<br />
and clearly articulate <strong>the</strong> significance of <strong>the</strong> problem. This will<br />
determine <strong>the</strong> time and resources allocated to resolving it – and is an<br />
important beginning. At <strong>the</strong> end of <strong>the</strong> day it will also constitute your<br />
business case that you present to management for endorsement of your<br />
recommendations.<br />
Then, create your cause and effect chart. Collect information from all<br />
<strong>the</strong> people in <strong>the</strong> room and organise it logically according to <strong>the</strong> process<br />
that you are using.<br />
With <strong>the</strong> help of <strong>the</strong> entire group, you will gain a clear picture of <strong>the</strong><br />
problem at hand. At <strong>the</strong> same time, you will see what is unknown – and<br />
thus what requires fur<strong>the</strong>r investigation.
Conduct <strong>the</strong> Root Cause Analysis<br />
Use <strong>the</strong> completed cause and effect<br />
chart to assist you in searching for<br />
solutions. If you can eliminate a cause -<br />
you break <strong>the</strong> link between causes and<br />
<strong>the</strong> effect won’t happen. By eliminating<br />
just one cause you can demonstrate to<br />
everyone <strong>the</strong> effect that it will have by<br />
referring to your cause and effect chart.<br />
If you do end up with a large number<br />
of possible solutions, consider how to<br />
achieve <strong>the</strong> desired outcome with <strong>the</strong><br />
least amount of time, effort, or money.<br />
Prioritise your options and implement<br />
<strong>the</strong> best of <strong>the</strong>m. Establish a set of<br />
criteria by which you can objectively<br />
judge which are <strong>the</strong> better solutions.<br />
Top tips<br />
• Follow <strong>the</strong> RCA process<br />
• You don’t have to be <strong>the</strong> subject matter expert, so don’t<br />
profess to be one<br />
• Teamwork is key – value all participants’ contributions<br />
• Keep asking “why” or “caused by” questions for as long as<br />
you need to<br />
• Don’t stop too soon with your questioning
Implement <strong>the</strong> solutions<br />
(corrective actions)
Implement <strong>the</strong> solutions (corrective actions)<br />
Be clear about who is responsible for<br />
each corrective action. You don’t want<br />
to create <strong>the</strong> opportunity for people<br />
to be able to pass <strong>the</strong> buck with “I<br />
thought Bob was going to do it.”<br />
Your RCA should produce a number of corrective actions.<br />
These should be implemented as soon as practically<br />
possible.<br />
Have a mechanism in place by which <strong>the</strong> implementation<br />
of corrective actions can be tracked. This system should<br />
appoint a single person to each corrective action, and<br />
include a clear timeframe for completion. This allows for<br />
progress to be evaluated.
Implement <strong>the</strong> solutions (corrective actions)<br />
Make sure you follow up<br />
on each corrective action –<br />
check back with <strong>the</strong> individual<br />
responsible, to make sure that<br />
progress is being made.<br />
Top tips<br />
• Give ownership of a solution to an individual, not a group<br />
or department<br />
• Assign a due-date for each corrective action<br />
• Support people in <strong>the</strong>ir efforts to implement corrective<br />
actions
Measure <strong>the</strong> success of<br />
<strong>the</strong> corrective actions
Measure <strong>the</strong> success of <strong>the</strong> corrective actions<br />
By quantifying <strong>the</strong> success of your<br />
efforts, you are unequivocally<br />
demonstrating <strong>the</strong> value of RCA.<br />
How much downtime have you avoided? How much money have<br />
you saved? Measure <strong>the</strong> impact of your RCA and its subsequent<br />
corrective actions.<br />
By talking in figures – about increases in production tonnes,<br />
or a decrease in downtime, or dollars saved – you will be able<br />
to demonstrate <strong>the</strong> success of your actions. After all, <strong>the</strong>se<br />
measures are often <strong>the</strong> very reason you did <strong>the</strong> RCA in <strong>the</strong><br />
first place; plus, <strong>the</strong>y are tangible and readily understood by<br />
management.
Measure <strong>the</strong> success of <strong>the</strong> corrective actions<br />
Many industries fall over when it<br />
comes to <strong>the</strong> measurement of any<br />
change that <strong>the</strong> corrective actions<br />
have engendered. Yet this step is<br />
very important. By substantiating<br />
<strong>the</strong> success of corrective actions,<br />
greater credibility is given to<br />
<strong>the</strong> investigation process and<br />
any future investigations will<br />
receive even more support from<br />
management teams.<br />
Top tips<br />
• Identify which key performance indicators are being used<br />
to measure success<br />
• Use ‘before and after’ figures to prove it
Advertise your<br />
successes
Advertise your successes<br />
By demonstrating how much value<br />
you’ve brought to your company, it<br />
will be easier to bring <strong>the</strong> right people<br />
to <strong>the</strong> investigative team next time<br />
around.<br />
Publish your RCA report, and promote <strong>the</strong> great results<br />
that you measured in <strong>the</strong> previous step.<br />
As you will have discovered, <strong>the</strong> 6 <strong>steps</strong> <strong>beyond</strong> <strong>the</strong> 5<br />
<strong>Whys</strong> require a significant investment of both time and<br />
resources.<br />
To help ensure that <strong>the</strong>se resources are made available<br />
for <strong>the</strong> next RCA, <strong>the</strong>n <strong>the</strong> positive outcomes of <strong>the</strong><br />
investigation conducted should be advertised to <strong>the</strong><br />
broader work community.
Advertise your successes<br />
Promoting your results will<br />
engender management<br />
support for <strong>the</strong> RCA process<br />
and <strong>the</strong> process itself will gain<br />
favour and support from your<br />
colleagues.<br />
Sharing <strong>the</strong> report will also<br />
help <strong>the</strong> entire business unit<br />
to learn from <strong>the</strong> incidents or<br />
accidents that have occurred.<br />
By sharing all of your findings,<br />
you will be building on <strong>the</strong><br />
collective wisdom of your<br />
company.<br />
Top tips<br />
• Put <strong>the</strong> results on a poster in a prominent position<br />
• Share <strong>the</strong> full report with all relevant stakeholders<br />
• Share with <strong>the</strong> broader work community<br />
• Quantify your successes in a way that is easy<br />
for o<strong>the</strong>rs to understand
Case Study<br />
Now that you have a good understanding<br />
of each of <strong>the</strong> 6 Steps Beyond <strong>the</strong> 5 Why’s,<br />
let’s refer back to <strong>the</strong> initial case study<br />
used to illustrate <strong>the</strong> 5 Why method and<br />
how diving deeper <strong>beyond</strong> this method,<br />
using <strong>the</strong> “6 <strong>steps</strong>”, can allow you to get to<br />
<strong>the</strong> root causes of a problem.<br />
If we were to initiate <strong>the</strong> “6 Steps”, a<br />
search for all relevant information would<br />
be undertaken. Statements, photographs<br />
and a search for all maintenance history<br />
on <strong>the</strong> drive motor are all collected.<br />
(Step 1)<br />
The RCA is <strong>the</strong>n undertaken (Step 3).<br />
Clarification of <strong>the</strong> purpose of <strong>the</strong><br />
investigation, in this case preventing <strong>the</strong><br />
recurrence of <strong>the</strong> “Delay in loading <strong>the</strong><br />
train”, is <strong>the</strong> first step. Then context to<br />
<strong>the</strong> problem is included by identifying<br />
“When” it occurred, “Where” it happened<br />
and how “Significant” <strong>the</strong> problem is (for<br />
example; damage to reputation, cost of<br />
any demurrage for delayed shipments<br />
etc). Quantifying <strong>the</strong> costs will create an<br />
understanding of just how significant this<br />
problem is.<br />
With management’s support, key<br />
personnel have been identified to<br />
participate in <strong>the</strong> investigation and invited<br />
to attend. An experienced facilitator has<br />
been appointed based on <strong>the</strong>ir ability to<br />
handle all <strong>the</strong> individuals in <strong>the</strong> group and<br />
to control <strong>the</strong> (potentially large) group<br />
size.<br />
The room that has been booked is suited<br />
for <strong>the</strong> size of <strong>the</strong> group and <strong>the</strong> facilities<br />
allow for <strong>the</strong> recording and organisation of<br />
large amounts of information. The more<br />
room <strong>the</strong>re is <strong>the</strong> better as it allows <strong>the</strong><br />
facilitator to spread <strong>the</strong> information out in<br />
logical paths to make it easy for o<strong>the</strong>rs to<br />
follow. The facilitator can <strong>the</strong>n separate<br />
cause paths and cater for <strong>the</strong> expansion of<br />
<strong>the</strong>m. (Step 2)
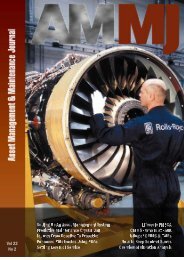
Next, <strong>the</strong> cause and effect chart is created. The problem is already known, so <strong>the</strong> team now<br />
undertakes an exhaustive search for all causes. Being minimalistic may speed things up but<br />
will also limit <strong>the</strong> number of opportunities that present <strong>the</strong>mselves to control <strong>the</strong> problem.<br />
If minimalistic, you will probably end up with strong lineal connection of information. If<br />
expansive, we will see a chart that will grow from your initial effect and expand into a number<br />
of causal pathways. Please refer to <strong>the</strong> example below.<br />
Action<br />
Conveyor has stopped<br />
Caused by<br />
Primary Effect<br />
Delay in train loading<br />
Caused by<br />
Condition<br />
Conveyor loads <strong>the</strong> train<br />
Condition<br />
Only 1 Loading Conveyor<br />
Caused by<br />
Caused by<br />
STOP<br />
STOP<br />
Condition<br />
6 hours to replace<br />
drive motor<br />
Caused by<br />
?<br />
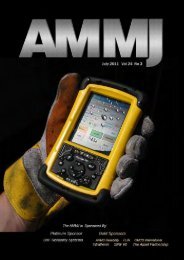
When expanded on fur<strong>the</strong>r, this is what a chart starts to look like.<br />
Condition<br />
motor operating<br />
Caused by<br />
Action<br />
Conveyor has stopped<br />
Caused by<br />
Condition<br />
Drive Motor Drives<br />
conveyor<br />
Action<br />
Drive motor tripped out<br />
Caused by<br />
Caused by<br />
STOP<br />
Action<br />
Motor was overloaded<br />
Caused by<br />
Action<br />
Bearing seized<br />
Condition<br />
Seized bearing overloads<br />
motor<br />
Caused by<br />
Caused by<br />
Condition<br />
Motor has overload<br />
protection<br />
Caused by<br />
STOP<br />
Primary Effect<br />
Delay in train loading<br />
Caused by<br />
Condition<br />
Conveyor loads <strong>the</strong> train<br />
Condition<br />
Only 1 Loading Conveyor<br />
Caused by<br />
Caused by<br />
STOP<br />
STOP<br />
Condition<br />
6 hours to replace<br />
drive motor<br />
Caused by<br />
?<br />
This is before <strong>the</strong> team has even got to why <strong>the</strong> bearing has seized. Problems are rarely as<br />
simple as <strong>the</strong>y seem. We tend to want to do things simply however this comes at <strong>the</strong> cost of<br />
good understanding. Whilst you may understand, it is possible that o<strong>the</strong>rs will struggle to<br />
follow your logic. If all <strong>the</strong> information is not put into play <strong>the</strong>n you rely on assumptions and a<br />
common interpretation, which is precisely why many misunderstandings occur.
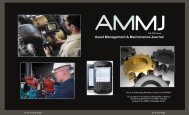
Let’s explore fur<strong>the</strong>r on why <strong>the</strong> bearing seized by adding to <strong>the</strong> existing chart.<br />
Primary Effect<br />
Bearing seized<br />
Caused by<br />
Action<br />
Metal welded toge<strong>the</strong>r<br />
Condition<br />
welding seizes<br />
<strong>the</strong> bearing<br />
Caused<br />
by<br />
STOP<br />
Caused by<br />
Action<br />
Temperature exceeded<br />
melting point<br />
Condition<br />
Metal melting point “X”<br />
Caused<br />
by<br />
STOP<br />
Caused by<br />
STOP<br />
Caused by<br />
Action<br />
Bearing was operating<br />
Condition<br />
High friction in bearing<br />
Condition<br />
Didn’t trip out<br />
Caused by<br />
?<br />
Caused by<br />
Action<br />
Metal expansion<br />
in bearing<br />
Condition<br />
Minimal clearnace<br />
in bearing<br />
Caused by<br />
STOP<br />
Caused by<br />
Action<br />
High heat generated<br />
Condition<br />
Metal expands with heat<br />
Caused by<br />
STOP<br />
Caused by<br />
STOP<br />
Caused by<br />
Action<br />
Bearing operating<br />
Condition<br />
Low lubrication<br />
Caused by<br />
?<br />
Caused by<br />
Action<br />
Tube Blocked<br />
Condition<br />
Autolube System<br />
Caused by<br />
STOP<br />
So what do we notice? The same problem has been explored, however <strong>the</strong> complexity and<br />
detail of <strong>the</strong> problem has certainly increased. If you want to establish a comprehensive<br />
understanding of <strong>the</strong> problem throughout <strong>the</strong> company, <strong>the</strong> 6 Steps Beyond 5 Why’s will allow<br />
you to do this. A strong understanding of <strong>the</strong> problem will lead to implementing effective and<br />
timely solutions. (Step 4)<br />
Measuring <strong>the</strong> success of <strong>the</strong> corrective action will need to be undertaken after a period of<br />
time to ascertain <strong>the</strong> success of <strong>the</strong> solutions. (Step 5)<br />
Advertising success and sharing reports will create a positive dynamic within <strong>the</strong> company for<br />
<strong>the</strong> support of <strong>the</strong> Root Cause Analysis program, whilst also educating all employees within<br />
<strong>the</strong> company at <strong>the</strong> same time. (Step 6)
Conclusion<br />
In this eBook, we looked at <strong>the</strong> 5 <strong>Whys</strong> process – and identified<br />
that, in some cases, it does not get to <strong>the</strong> root causes of an<br />
incident or accident.<br />
Realising that you have to dive deeper, it is important to give<br />
this investigation some structure. This will help to guarantee<br />
<strong>the</strong> consistency – and performance – of outcomes.<br />
As <strong>the</strong> ‘6 <strong>steps</strong> <strong>beyond</strong> <strong>the</strong> 5 <strong>Whys</strong> demonstrates, planning and<br />
preparation are <strong>the</strong> keys to implementing a successful RCA and<br />
<strong>the</strong>n initiating corrective actions.<br />
To avoid <strong>the</strong> ‘blame game’ and really get to <strong>the</strong> bottom of<br />
incidents within your organisation, we encourage you to<br />
consider all <strong>the</strong> <strong>steps</strong> that have been outlined here when you<br />
next conduct an RCA that goes fur<strong>the</strong>r than <strong>the</strong> 5 <strong>Whys</strong> process.
PUBLIC TRAINING COURSES<br />
We hold public training courses in cities throughout <strong>the</strong> world. Learn<br />
more about our 2 Day Facilitators Course<br />
onsite training<br />
All our training courses are available for delivery onsite at your<br />
facility or a training venue of your choice. If you choose to book onsite<br />
training, we highly recommend doing <strong>the</strong> 3 day Facilitator course which<br />
offers students <strong>the</strong> opportunity to work on a real life problem from <strong>the</strong>ir<br />
workplace under <strong>the</strong> guidance of one of our experienced trainers.<br />
OnSite Training Benefits<br />
• Cost effective for a larger group size<br />
• Avoid travel expenses for attendees<br />
• Reduced time away from work for students<br />
• Schedule convenience - working around your availability and<br />
schedule<br />
• Personalisation and customisation for certain courses to make it<br />
relevant for students<br />
• Get all team members speaking a common RCA language<br />
FACILITATION SERVICES<br />
Sometimes <strong>the</strong>re will be an issue of sensitivity that requires greater<br />
objectivity and facilitation skills in finding out <strong>the</strong> root cause and<br />
developing solutions. Click to learn how we can help.<br />
Learn more about <strong>the</strong> Apollo Root Cause Analysis TM<br />
method at www.apollorootcause.com
About ARMS Reliability<br />
ARMS Reliability is a service, software, and training organisation<br />
providing a “one stop shop” for Root Cause Analysis, as well as<br />
Reliability Engineering, RAMS, and Maintenance Optimisation for both<br />
new and existing projects.<br />
Since 1997, ARMS Reliability has been an authorised training provider of<br />
<strong>the</strong> Apollo Root Cause Analysis TM methodology. In 2012, our agreement<br />
went global and ARMS Reliability now provides RCA training, software,<br />
and services throughout <strong>the</strong> world.<br />
5 <strong>Whys</strong> + Apollo Root Cause<br />
Analysis TM Method<br />
Many of our clients use <strong>the</strong> 5 <strong>Whys</strong> process as <strong>the</strong>ir base level<br />
methodology for very simple incidents and use <strong>the</strong> Apollo Root Cause<br />
Analysis TM method for more complex problems. The Apollo Root Cause<br />
Analysis TM method truly is scalable – it can be used for any size and<br />
complexity of problem and can be integrated into a root cause analysis<br />
program that is tailored to your organisation’s needs.<br />
For more information on how ARMS Reliability can help, please contact<br />
us at <strong>the</strong> office location nearest you (details below).<br />
You can also make an enquiry on www.apollorootcause.com<br />
www.apollorootcause.com<br />
info@apollorootcause.com<br />
NORTH / CENTRAL / SOUTH AMERICA<br />
P: +1 512 795 5291<br />
AUSTRALIA / ASIA / NEW ZEALAND<br />
P: +61 3 5255 5357<br />
EUROPE<br />
P: +44 122 445 9362<br />
SOUTH AFRICA<br />
P: +27 10 500 8232<br />
North America | Latin America | Europe | Asia | Africa | Australia