

European Resuscitation Council Guidelines for Resuscitation ... - CPR
European Resuscitation Council Guidelines for Resuscitation ... - CPR
European Resuscitation Council Guidelines for Resuscitation ... - CPR

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
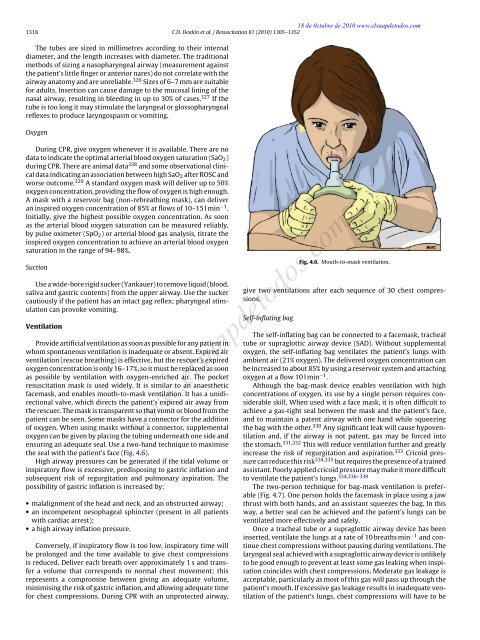
18 de 0ctubre de 2010 www.elsuapdetodos.com1318 C.D. Deakin et al. / <strong>Resuscitation</strong> 81 (2010) 1305–1352The tubes are sized in millimetres according to their internaldiameter, and the length increases with diameter. The traditionalmethods of sizing a nasopharyngeal airway (measurement againstthe patient’s little finger or anterior nares) do not correlate with theairway anatomy and are unreliable. 326 Sizes of 6–7 mm are suitable<strong>for</strong> adults. Insertion can cause damage to the mucosal lining of thenasal airway, resulting in bleeding in up to 30% of cases. 327 If thetube is too long it may stimulate the laryngeal or glossopharyngealreflexes to produce laryngospasm or vomiting.OxygenDuring <strong>CPR</strong>, give oxygen whenever it is available. There are nodata to indicate the optimal arterial blood oxygen saturation (SaO 2 )during <strong>CPR</strong>. There are animal data 328 and some observational clinicaldata indicating an association between high SaO 2 after ROSC andworse outcome. 329 A standard oxygen mask will deliver up to 50%oxygen concentration, providing the flow of oxygen is high enough.A mask with a reservoir bag (non-rebreathing mask), can deliveran inspired oxygen concentration of 85% at flows of 10–15 l min −1 .Initially, give the highest possible oxygen concentration. As soonas the arterial blood oxygen saturation can be measured reliably,by pulse oximeter (SpO 2 ) or arterial blood gas analysis, titrate theinspired oxygen concentration to achieve an arterial blood oxygensaturation in the range of 94–98%.SuctionUse a wide-bore rigid sucker (Yankauer) to remove liquid (blood,saliva and gastric contents) from the upper airway. Use the suckercautiously if the patient has an intact gag reflex; pharyngeal stimulationcan provoke vomiting.VentilationProvide artificial ventilation as soon as possible <strong>for</strong> any patient inwhom spontaneous ventilation is inadequate or absent. Expired airventilation (rescue breathing) is effective, but the rescuer’s expiredoxygen concentration is only 16–17%, so it must be replaced as soonas possible by ventilation with oxygen-enriched air. The pocketresuscitation mask is used widely. It is similar to an anaestheticfacemask, and enables mouth-to-mask ventilation. It has a unidirectionalvalve, which directs the patient’s expired air away fromthe rescuer. The mask is transparent so that vomit or blood from thepatient can be seen. Some masks have a connector <strong>for</strong> the additionof oxygen. When using masks without a connector, supplementaloxygen can be given by placing the tubing underneath one side andensuring an adequate seal. Use a two-hand technique to maximisethe seal with the patient’s face (Fig. 4.6).High airway pressures can be generated if the tidal volume orinspiratory flow is excessive, predisposing to gastric inflation andsubsequent risk of regurgitation and pulmonary aspiration. Thepossibility of gastric inflation is increased by:• malalignment of the head and neck, and an obstructed airway;• an incompetent oesophageal sphincter (present in all patientswith cardiac arrest);• a high airway inflation pressure.Conversely, if inspiratory flow is too low, inspiratory time willbe prolonged and the time available to give chest compressionsis reduced. Deliver each breath over approximately 1 s and transfera volume that corresponds to normal chest movement; thisrepresents a compromise between giving an adequate volume,minimising the risk of gastric inflation, and allowing adequate time<strong>for</strong> chest compressions. During <strong>CPR</strong> with an unprotected airway,Fig. 4.6. Mouth-to-mask ventilation.give two ventilations after each sequence of 30 chest compressions.Self-inflating bagThe self-inflating bag can be connected to a facemask, trachealtube or supraglottic airway device (SAD). Without supplementaloxygen, the self-inflating bag ventilates the patient’s lungs withambient air (21% oxygen). The delivered oxygen concentration canbe increased to about 85% by using a reservoir system and attachingoxygen at a flow 10 l min −1 .Although the bag-mask device enables ventilation with highconcentrations of oxygen, its use by a single person requires considerableskill. When used with a face mask, it is often difficult toachieve a gas-tight seal between the mask and the patient’s face,and to maintain a patent airway with one hand while squeezingthe bag with the other. 330 Any significant leak will cause hypoventilationand, if the airway is not patent, gas may be <strong>for</strong>ced intothe stomach. 331,332 This will reduce ventilation further and greatlyincrease the risk of regurgitation and aspiration. 333 Cricoid pressurecan reduce this risk 334,335 but requires the presence of a trainedassistant. Poorly applied cricoid pressure may make it more difficultto ventilate the patient’s lungs. 334,336–339The two-person technique <strong>for</strong> bag-mask ventilation is preferable(Fig. 4.7). One person holds the facemask in place using a jawthrust with both hands, and an assistant squeezes the bag. In thisway, a better seal can be achieved and the patient’s lungs can beventilated more effectively and safely.Once a tracheal tube or a supraglottic airway device has beeninserted, ventilate the lungs at a rate of 10 breaths min −1 and continuechest compressions without pausing during ventilations. Thelaryngeal seal achieved with a supraglottic airway device is unlikelyto be good enough to prevent at least some gas leaking when inspirationcoincides with chest compressions. Moderate gas leakage isacceptable, particularly as most of this gas will pass up through thepatient’s mouth. If excessive gas leakage results in inadequate ventilationof the patient’s lungs, chest compressions will have to bewww.elsuapdetodos.com













