Iowa Medicaid Enterprise UB-04 Claim Form Health Insurance ...
Iowa Medicaid Enterprise UB-04 Claim Form Health Insurance ...
Iowa Medicaid Enterprise UB-04 Claim Form Health Insurance ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
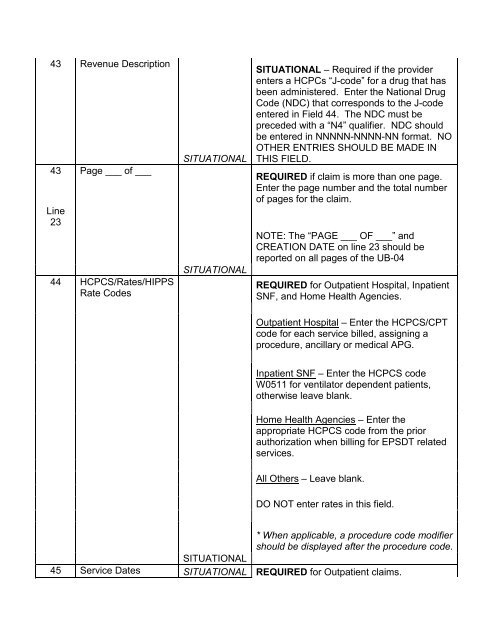
43 Revenue Description43 Page ___ of ___Line2344 HCPCS/Rates/HIPPSRate CodesSITUATIONALSITUATIONALSITUATIONAL – Required if the providerenters a HCPCs “J-code” for a drug that hasbeen administered. Enter the National DrugCode (NDC) that corresponds to the J-codeentered in Field 44. The NDC must bepreceded with a “N4” qualifier. NDC shouldbe entered in NNNNN-NNNN-NN format. NOOTHER ENTRIES SHOULD BE MADE INTHIS FIELD.REQUIRED if claim is more than one page.Enter the page number and the total numberof pages for the claim.NOTE: The “PAGE ___ OF ___” andCREATION DATE on line 23 should bereported on all pages of the <strong>UB</strong>-<strong>04</strong>REQUIRED for Outpatient Hospital, InpatientSNF, and Home <strong>Health</strong> Agencies.Outpatient Hospital – Enter the HCPCS/CPTcode for each service billed, assigning aprocedure, ancillary or medical APG.Inpatient SNF – Enter the HCPCS codeW0511 for ventilator dependent patients,otherwise leave blank.Home <strong>Health</strong> Agencies – Enter theappropriate HCPCS code from the priorauthorization when billing for EPSDT relatedservices.All Others – Leave blank.DO NOT enter rates in this field.* When applicable, a procedure code modifiershould be displayed after the procedure code.SITUATIONAL45 Service Dates SITUATIONAL REQUIRED for Outpatient claims.