Iowa Medicaid Enterprise UB-04 Claim Form Health Insurance ...
Iowa Medicaid Enterprise UB-04 Claim Form Health Insurance ...
Iowa Medicaid Enterprise UB-04 Claim Form Health Insurance ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
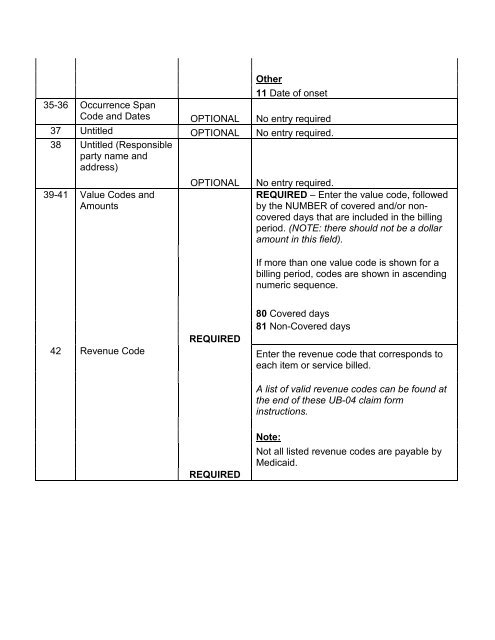
Other11 Date of onset35-36 Occurrence SpanCode and Dates OPTIONAL No entry required37 Untitled OPTIONAL No entry required.38 Untitled (Responsibleparty name andaddress)39-41 Value Codes andAmountsOPTIONALNo entry required.REQUIRED – Enter the value code, followedby the NUMBER of covered and/or noncovereddays that are included in the billingperiod. (NOTE: there should not be a dollaramount in this field).If more than one value code is shown for abilling period, codes are shown in ascendingnumeric sequence.42 Revenue CodeREQUIRED80 Covered days81 Non-Covered daysEnter the revenue code that corresponds toeach item or service billed.A list of valid revenue codes can be found atthe end of these <strong>UB</strong>-<strong>04</strong> claim forminstructions.REQUIREDNote:Not all listed revenue codes are payable by<strong>Medicaid</strong>.