Iowa Medicaid Enterprise UB-04 Claim Form Health Insurance ...
Iowa Medicaid Enterprise UB-04 Claim Form Health Insurance ...
Iowa Medicaid Enterprise UB-04 Claim Form Health Insurance ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
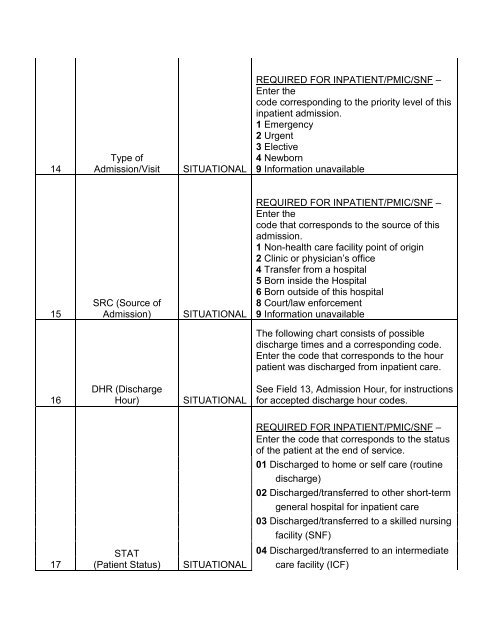
14Type ofAdmission/VisitSITUATIONALREQUIRED FOR INPATIENT/PMIC/SNF –Enter thecode corresponding to the priority level of thisinpatient admission.1 Emergency2 Urgent3 Elective4 Newborn9 Information unavailable15SRC (Source ofAdmission)SITUATIONALREQUIRED FOR INPATIENT/PMIC/SNF –Enter thecode that corresponds to the source of thisadmission.1 Non-health care facility point of origin2 Clinic or physician’s office4 Transfer from a hospital5 Born inside the Hospital6 Born outside of this hospital8 Court/law enforcement9 Information unavailableThe following chart consists of possibledischarge times and a corresponding code.Enter the code that corresponds to the hourpatient was discharged from inpatient care.16DHR (DischargeHour)SITUATIONALSee Field 13, Admission Hour, for instructionsfor accepted discharge hour codes.REQUIRED FOR INPATIENT/PMIC/SNF –Enter the code that corresponds to the statusof the patient at the end of service.01 Discharged to home or self care (routinedischarge)02 Discharged/transferred to other short-termgeneral hospital for inpatient care03 Discharged/transferred to a skilled nursingfacility (SNF)17STAT(Patient Status)SITUATIONAL<strong>04</strong> Discharged/transferred to an intermediatecare facility (ICF)