Iowa Medicaid Enterprise UB-04 Claim Form Health Insurance ...
Iowa Medicaid Enterprise UB-04 Claim Form Health Insurance ...
Iowa Medicaid Enterprise UB-04 Claim Form Health Insurance ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
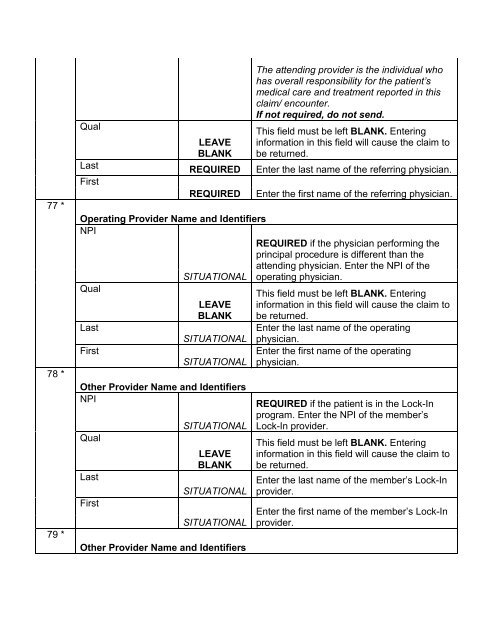
77 *78 *79 *QualLastFirstLEAVEBLANKREQUIREDREQUIREDThe attending provider is the individual whohas overall responsibility for the patient’smedical care and treatment reported in thisclaim/ encounter.If not required, do not send.This field must be left BLANK. Enteringinformation in this field will cause the claim tobe returned.Enter the last name of the referring physician.Enter the first name of the referring physician.Operating Provider Name and IdentifiersNPIREQUIRED if the physician performing theprincipal procedure is different than theattending physician. Enter the NPI of theSITUATIONAL operating physician.QualThis field must be left BLANK. EnteringLEAVE information in this field will cause the claim toBLANK be returned.LastEnter the last name of the operatingSITUATIONAL physician.FirstEnter the first name of the operatingSITUATIONAL physician.Other Provider Name and IdentifiersNPIQualLastFirstSITUATIONALLEAVEBLANKSITUATIONALSITUATIONALOther Provider Name and IdentifiersREQUIRED if the patient is in the Lock-Inprogram. Enter the NPI of the member’sLock-In provider.This field must be left BLANK. Enteringinformation in this field will cause the claim tobe returned.Enter the last name of the member’s Lock-Inprovider.Enter the first name of the member’s Lock-Inprovider.