Iowa Medicaid Enterprise UB-04 Claim Form Health Insurance ...
Iowa Medicaid Enterprise UB-04 Claim Form Health Insurance ...
Iowa Medicaid Enterprise UB-04 Claim Form Health Insurance ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
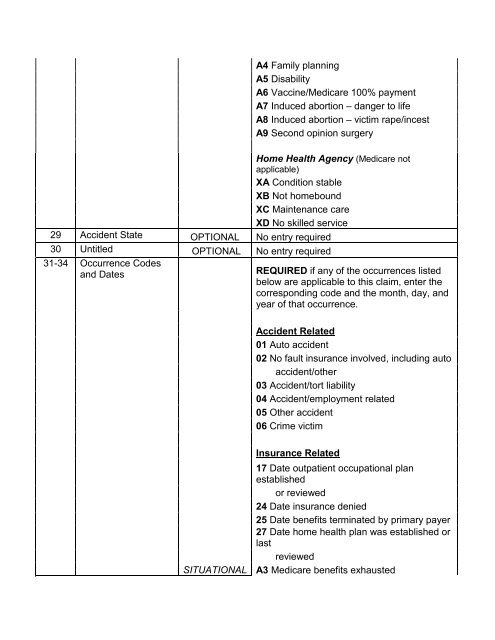
A4 Family planningA5 DisabilityA6 Vaccine/Medicare 100% paymentA7 Induced abortion – danger to lifeA8 Induced abortion – victim rape/incestA9 Second opinion surgeryHome <strong>Health</strong> Agency (Medicare notapplicable)XA Condition stableXB Not homeboundXC Maintenance careXD No skilled service29 Accident State OPTIONAL No entry required30 Untitled OPTIONAL No entry required31-34 Occurrence Codesand DatesREQUIRED if any of the occurrences listedbelow are applicable to this claim, enter thecorresponding code and the month, day, andyear of that occurrence.Accident Related01 Auto accident02 No fault insurance involved, including autoaccident/other03 Accident/tort liability<strong>04</strong> Accident/employment related05 Other accident06 Crime victimSITUATIONAL<strong>Insurance</strong> Related17 Date outpatient occupational planestablishedor reviewed24 Date insurance denied25 Date benefits terminated by primary payer27 Date home health plan was established orlastreviewedA3 Medicare benefits exhausted