Iowa Medicaid Enterprise UB-04 Claim Form Health Insurance ...
Iowa Medicaid Enterprise UB-04 Claim Form Health Insurance ...
Iowa Medicaid Enterprise UB-04 Claim Form Health Insurance ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
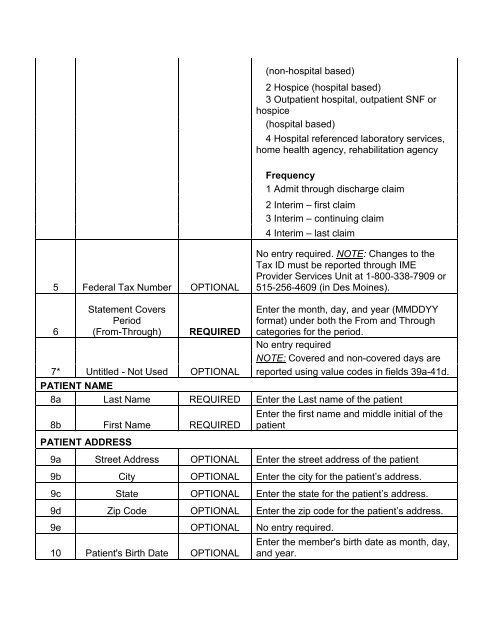
(non-hospital based)2 Hospice (hospital based)3 Outpatient hospital, outpatient SNF orhospice(hospital based)4 Hospital referenced laboratory services,home health agency, rehabilitation agencyFrequency1 Admit through discharge claim2 Interim – first claim3 Interim – continuing claim4 Interim – last claim5 Federal Tax Number OPTIONALNo entry required. NOTE: Changes to theTax ID must be reported through IMEProvider Services Unit at 1-800-338-7909 or515-256-4609 (in Des Moines).6Statement CoversPeriod(From-Through)REQUIRED7* Untitled - Not Used OPTIONALEnter the month, day, and year (MMDDYYformat) under both the From and Throughcategories for the period.No entry requiredNOTE: Covered and non-covered days arereported using value codes in fields 39a-41d.PATIENT NAME8a Last Name REQUIRED Enter the Last name of the patient8b First Name REQUIREDPATIENT ADDRESSEnter the first name and middle initial of thepatient9a Street Address OPTIONAL Enter the street address of the patient9b City OPTIONAL Enter the city for the patient’s address.9c State OPTIONAL Enter the state for the patient’s address.9d Zip Code OPTIONAL Enter the zip code for the patient’s address.9e OPTIONAL No entry required.10 Patient's Birth Date OPTIONALEnter the member's birth date as month, day,and year.