Iowa Medicaid Enterprise UB-04 Claim Form Health Insurance ...
Iowa Medicaid Enterprise UB-04 Claim Form Health Insurance ...
Iowa Medicaid Enterprise UB-04 Claim Form Health Insurance ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
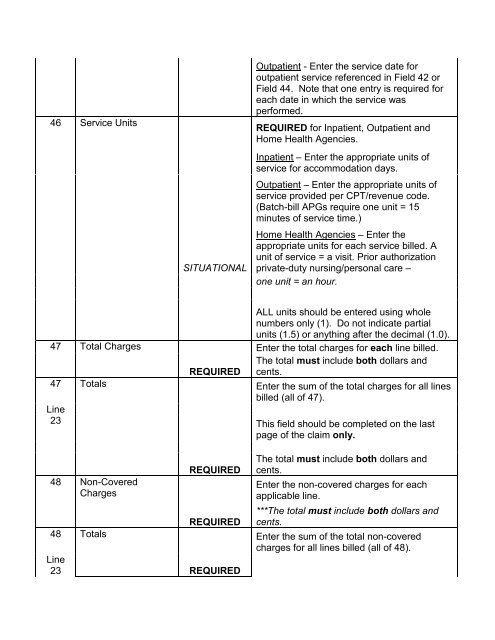
46 Service UnitsSITUATIONALOutpatient - Enter the service date foroutpatient service referenced in Field 42 orField 44. Note that one entry is required foreach date in which the service wasperformed.REQUIRED for Inpatient, Outpatient andHome <strong>Health</strong> Agencies.Inpatient – Enter the appropriate units ofservice for accommodation days.Outpatient – Enter the appropriate units ofservice provided per CPT/revenue code.(Batch-bill APGs require one unit = 15minutes of service time.)Home <strong>Health</strong> Agencies – Enter theappropriate units for each service billed. Aunit of service = a visit. Prior authorizationprivate-duty nursing/personal care –one unit = an hour.ALL units should be entered using wholenumbers only (1). Do not indicate partialunits (1.5) or anything after the decimal (1.0).47 Total ChargesEnter the total charges for each line billed.The total must include both dollars andREQUIRED cents.47 TotalsEnter the sum of the total charges for all linesbilled (all of 47).Line23 This field should be completed on the lastpage of the claim only.48 Non-CoveredCharges48 TotalsLine23REQUIREDREQUIREDREQUIREDThe total must include both dollars andcents.Enter the non-covered charges for eachapplicable line.***The total must include both dollars andcents.Enter the sum of the total non-coveredcharges for all lines billed (all of 48).