Iowa Medicaid Enterprise UB-04 Claim Form Health Insurance ...
Iowa Medicaid Enterprise UB-04 Claim Form Health Insurance ...
Iowa Medicaid Enterprise UB-04 Claim Form Health Insurance ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
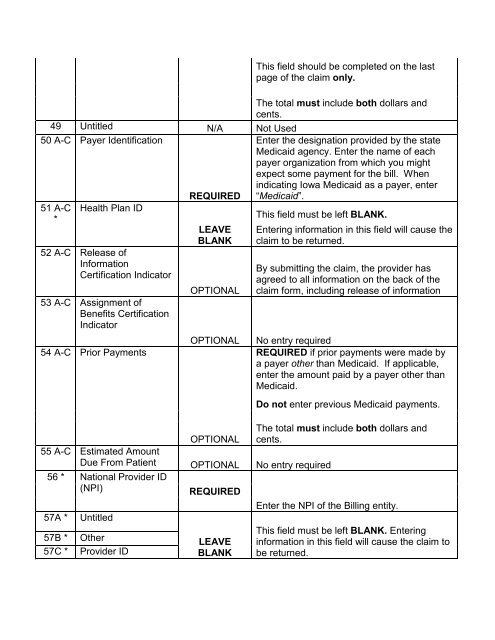
This field should be completed on the lastpage of the claim only.The total must include both dollars andcents.49 Untitled N/A Not Used50 A-C Payer Identification51 A-C*<strong>Health</strong> Plan ID52 A-C Release ofInformationCertification Indicator53 A-C Assignment ofBenefits CertificationIndicator54 A-C Prior PaymentsREQUIREDLEAVEBLANKOPTIONALOPTIONALEnter the designation provided by the state<strong>Medicaid</strong> agency. Enter the name of eachpayer organization from which you mightexpect some payment for the bill. Whenindicating <strong>Iowa</strong> <strong>Medicaid</strong> as a payer, enter“<strong>Medicaid</strong>”.This field must be left BLANK.Entering information in this field will cause theclaim to be returned.By submitting the claim, the provider hasagreed to all information on the back of theclaim form, including release of informationNo entry requiredREQUIRED if prior payments were made bya payer other than <strong>Medicaid</strong>. If applicable,enter the amount paid by a payer other than<strong>Medicaid</strong>.Do not enter previous <strong>Medicaid</strong> payments.The total must include both dollars andOPTIONAL cents.55 A-C Estimated AmountDue From Patient OPTIONAL No entry required56 * National Provider ID(NPI)REQUIRED57A *57B *57C *UntitledOtherProvider IDLEAVEBLANKEnter the NPI of the Billing entity.This field must be left BLANK. Enteringinformation in this field will cause the claim tobe returned.