A note <strong>on</strong> <strong>Medicaid</strong> managed care terminologyIn the private health insurance world, “managed care” usually refers to an arrangement in which a healthmaintenance organizati<strong>on</strong> (HMO) – a closed panel of physicians, hospitals, and other providers – provides acomprehensive set of c<strong>on</strong>tractually-defined covered services for an enrolled populati<strong>on</strong>, for which it is paid a permember per m<strong>on</strong>th premium, known as a capitati<strong>on</strong> payment. The HMO is at financial risk for the full cost ofservices provided. In <strong>Medicaid</strong>, managed care encompasses more varied approaches to delivering and financingcare, including risk-based arrangements with HMOs, but also c<strong>on</strong>tracts with other health plans for a n<strong>on</strong>comprehensiveset of services, as well as n<strong>on</strong>-risk or partial risk arrangements through state-administered primarycare case management programs (described below). The KCMU/HMA survey collected informati<strong>on</strong> from statesregarding the three basic models of <strong>Medicaid</strong> managed care recognized under federal law and regulati<strong>on</strong>s:Risk-based managed care organizati<strong>on</strong>s (MCOs) or health plans. <strong>State</strong>s c<strong>on</strong>tract with MCOs to provide acomprehensive package of benefits to enrolled <strong>Medicaid</strong> beneficiaries, primarily <strong>on</strong> a capitati<strong>on</strong> basis (i.e., thestate pays a per-member-per-m<strong>on</strong>th (PMPM) premium to the plan).* <strong>Medicaid</strong> MCOs may be commercial HMOsthat also serve people with employer-sp<strong>on</strong>sored insurance, or they may be <strong>Medicaid</strong>-<strong>on</strong>ly plans with nocommercially insured members. <strong>State</strong>s develop their own <strong>Medicaid</strong> standards of participati<strong>on</strong> for MCOs, whichusually include adherence to specified protocols for enrollment and member support, requirements to ensureadequate to access to care, achievement of set benchmarks for quality and quality improvement, and datacollecti<strong>on</strong> and submissi<strong>on</strong> requirements. <strong>Medicaid</strong> MCOs may be licensed by the state, or they may operate undera c<strong>on</strong>tract with the <strong>Medicaid</strong> agency regardless of licensure.Primary <strong>Care</strong> Case Management (PCCM) programs. PCCM programs are also c<strong>on</strong>sidered a form of comprehensive<strong>Medicaid</strong> managed care. These state-administered programs build <strong>on</strong> the <strong>Medicaid</strong> fee-for-service system. <strong>State</strong>sc<strong>on</strong>tract with Primary <strong>Care</strong> Providers (PCPs) who agree to provide case management services to <strong>Medicaid</strong>enrollees assigned to them, including the locati<strong>on</strong>, coordinati<strong>on</strong>, and m<strong>on</strong>itoring of primary health services. <strong>State</strong>sgenerally set specific requirements for PCPs, such as the ability to provide a set of primary care services, minimumhours of operati<strong>on</strong> at each locati<strong>on</strong>, specific credentials or training, and resp<strong>on</strong>sibility for referrals to specialists. Inadditi<strong>on</strong> to fee-for-service reimbursement for services delivered, PCPs are usually paid a nominal m<strong>on</strong>thly casemanagement fee. PCPs are usually physicians, physician group practices or clinics (such as federally qualifiedhealth centers), but a state may also recognize nurse practiti<strong>on</strong>ers, nurse midwives, and physician assistants asPCPs. <strong>State</strong> <strong>Medicaid</strong> staff carry out (or sometimes c<strong>on</strong>tract out) the administrative functi<strong>on</strong>s related to PCCMprograms, from network development and credentialing to quality m<strong>on</strong>itoring and improvement, and the stateusually (though not always) assumes full financial risk.N<strong>on</strong>-comprehensive prepaid health plans (PHPs). <strong>State</strong>s c<strong>on</strong>tract with PHPs <strong>on</strong> a risk basis to provide eithercomprehensive or n<strong>on</strong>-comprehensive benefits to enrolled <strong>Medicaid</strong> beneficiaries. Federal regulati<strong>on</strong>s that govern<strong>Medicaid</strong> managed care refer to MCOs as a comprehensive type of PHP, and identify two types of n<strong>on</strong>comprehensivePHPs. A prepaid inpatient health plan (PIHP) provides, arranges for, or otherwise has resp<strong>on</strong>sibilityfor a defined set of services that includes some type of inpatient hospital or instituti<strong>on</strong>al services, such as inpatientbehavioral health care. A prepaid ambulatory health plan (PAHP) provides, arranges for, or otherwise hasresp<strong>on</strong>sibility for some type of outpatient care <strong>on</strong>ly. Comm<strong>on</strong> types of n<strong>on</strong>-comprehensive PHPs provide <strong>on</strong>lybehavioral health services or <strong>on</strong>ly dental services, which, in many instances, are “carved out” of the benefitpackage provided by MCOs. Like MCOs, n<strong>on</strong>-comprehensive PHPs may be state-licensed or may operate under ac<strong>on</strong>tract with the <strong>Medicaid</strong> agency regardless of licensure.__________________________*“Comprehensive” is defined in federal regulati<strong>on</strong>s (at 42 CFR §438.2) as inpatient hospital services and any of thefollowing services, or any three or more of the following services: (1) outpatient hospital services; (2) rural healthclinic services; (3) FQHC services; (4) other laboratory and x-ray services; (5) nursing facility services; (6) early andperiodic screening, diagnostic, and treatment (EPSDT) services; (7) family planning services; (8) physician services,and (9) home health services.12 00
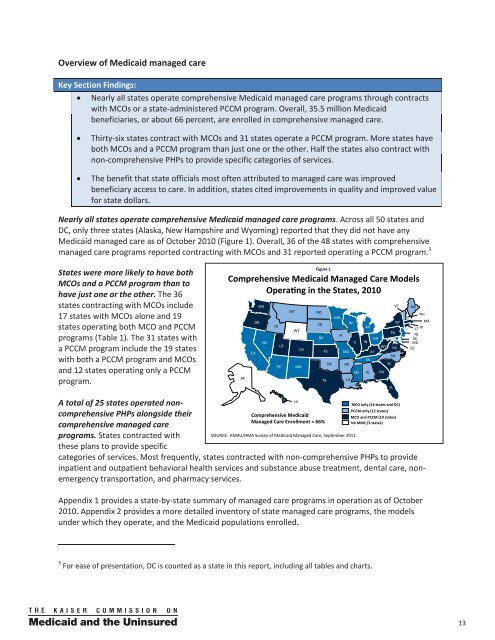
Overview of of <strong>Medicaid</strong> managed careKey Key Secti<strong>on</strong> Secti<strong>on</strong> Findings: Findings:Nearly Nearly all all states states operate operate comprehensive comprehensive <strong>Medicaid</strong> <strong>Medicaid</strong> managed managed care care programs programs through through c<strong>on</strong>tracts c<strong>on</strong>tractswith with MCOs MCOs or or a state-administered state-administered PCCM PCCM program. program. Overall, Overall, 35.5 35.5 milli<strong>on</strong> milli<strong>on</strong> <strong>Medicaid</strong> <strong>Medicaid</strong>beneficiaries, beneficiaries, or or about about 66 66 percent, percent, are are enrolled enrolled in in comprehensive comprehensive managed managed care. care.Thirty-six Thirty-six states states c<strong>on</strong>tract c<strong>on</strong>tract with with MCOs MCOs and and 31 31 states states operate operate a PCCM PCCM program. program. More More states states have haveboth both MCOs MCOs and and a PCCM PCCM program program than than just just <strong>on</strong>e <strong>on</strong>e or or the the other. other. Half Half the the states states also also c<strong>on</strong>tract c<strong>on</strong>tract with withn<strong>on</strong>-comprehensive n<strong>on</strong>-comprehensive PHPs PHPs to to provide provide specific specific categories categories of of services. services.The The benefit benefit that that state state officials officials most most often often attributed attributed to to managed managed care care was was improved improvedbeneficiary beneficiary access access to to care. care. In In additi<strong>on</strong>, additi<strong>on</strong>, states states cited cited improvements improvements in in quality quality and and improved improved value valuefor for state state dollars. dollars.Nearly Nearly all all states states operate operate comprehensive comprehensive <strong>Medicaid</strong> <strong>Medicaid</strong> managed managed care care programs. programs. Across Across all all 50 50 states states and andDC, DC, <strong>on</strong>ly <strong>on</strong>ly three three states states (Alaska, (Alaska, New New Hampshire Hampshire and and Wyoming) Wyoming) reported reported that that they they did did not not have have any any<strong>Medicaid</strong> <strong>Medicaid</strong> managed managed care care as as of of October October 2010 2010 (Figure (Figure 1). 1). Overall, Overall, 36 36 of of the the 48 48 states states with with comprehensivecomprehensivemanaged managed care care programs programs reported reported c<strong>on</strong>tracting c<strong>on</strong>tracting with with MCOs MCOs and and 31 31 reported reported operating operating a PCCM PCCM program. program. 3<strong>State</strong>s <strong>State</strong>s were were more more likely likely to to have have both bothMCOs MCOs and and a PCCM PCCM program program than than to tohave have just just <strong>on</strong>e <strong>on</strong>e or or the the other. other. The The 36 36states states c<strong>on</strong>tracting c<strong>on</strong>tracting with with MCOs MCOs include include17 17 states states with with MCOs MCOs al<strong>on</strong>e al<strong>on</strong>e and and 19 19states states operating operating both both MCO MCO and and PCCM PCCMprograms programs (Table (Table 1). 1). The The 31 31 states states with witha PCCM PCCM program program include include the the 19 19 states stateswith with both both a PCCM PCCM program program and and MCOs MCOsand and 12 12 states states operating operating <strong>on</strong>ly <strong>on</strong>ly a PCCM PCCMprogram. program.Figure 1Figure 1Comprehensive <strong>Medicaid</strong> <strong>Managed</strong> <strong>Care</strong> Models Comprehensive ComprehensiveComprehensive <strong>Medicaid</strong> <strong>Medicaid</strong><strong>Medicaid</strong> Opera4ng<strong>Managed</strong> <strong>Managed</strong><strong>Managed</strong> in the 6tates7<strong>Care</strong> <strong>Care</strong> in <strong>Care</strong> Models in 2919the the <strong>State</strong>s, <strong>State</strong>s, 2010 2010Opera4ng in the 6tates7 2919 WA VT ME WA MT ND VT ME NH MT ND MN NH OR SD MN WI NY MA OR ID WI MI NY MA RI ID WY SD CT MI PA WY IA CT RI NJ NE OH PA IA NJ DE NV NE IL IN OH DE MD NV UT IL IN WV CO VA MD DC UT CA KS MO KY WV CO VA DC NC CA KS MO KY TN NC OK AR SC AZ TN NM OK AR SC AZ NM MS AL GA AK MS AL GA TX LA AK TX LA FL FL A total total of of 25 25 states states operated operated n<strong>on</strong>comprehensivcomprehensivePHPs PHPs al<strong>on</strong>gside al<strong>on</strong>gside their theirComprehensive <strong>Medicaid</strong> PCCM MCO MCO MCO <strong>on</strong>ly and and PCCMHI n<strong>on</strong>-MCO MCO <strong>on</strong>ly <strong>on</strong>ly (17<strong>on</strong>ly <strong>on</strong>ly states) (17(17 (16 states)HI states) states and DC) MCO <strong>on</strong>ly (17 states)MCO PCCM PCCM PCCM <strong>on</strong>ly (16 <strong>on</strong>ly (12 states)<strong>on</strong>ly (12 <strong>on</strong>ly (12 states)states) (12 states) and DC) and PCCM and (12PCCM (24 states) (19PCCM (24 (19 states) states) comprehensive <strong>Managed</strong> <strong>Care</strong> Enrollment = 66% comprehensive managed managed careComprehensive <strong>Medicaid</strong> MCO No No and MMC MMCcareNo No MMC MMC PCCM (3 states) (3 states)(3 states) (3 (19 states) states) <strong>Managed</strong> <strong>Care</strong> Enrollment = 66% No MMC (3 states) programs. programs. <strong>State</strong>s <strong>State</strong>s c<strong>on</strong>tracted c<strong>on</strong>tracted withSOURCE: KCMU/HMA <str<strong>on</strong>g>Survey</str<strong>on</strong>g> of <strong>Medicaid</strong> <strong>Managed</strong> <strong>Care</strong>, September 2011.withSOURCE: SOURCE: KCMU/HMA <str<strong>on</strong>g>Survey</str<strong>on</strong>g> of <strong>Medicaid</strong> <strong>Managed</strong> <strong>Care</strong>, <strong>Care</strong>, September September 2011. 2011. SOURCE: KCMU/HMA <str<strong>on</strong>g>Survey</str<strong>on</strong>g> of <strong>Medicaid</strong> <strong>Managed</strong> <strong>Care</strong>, September 2011. these these plans plans to to provide provide specific specificcategories categories of of services. services. Most Most frequently, frequently, states states c<strong>on</strong>tracted c<strong>on</strong>tracted with with n<strong>on</strong>-comprehensive n<strong>on</strong>-comprehensive PHPs PHPs to to provide provideinpatient inpatient and and outpatient outpatient behavioral behavioral health health services services and and substance substance abuse abuse treatment, treatment, dental dental care, care, n<strong>on</strong>emergencemergencytransportati<strong>on</strong>, transportati<strong>on</strong>, and and pharmacy pharmacy services.n<strong>on</strong>-services.Appendix Appendix 1 provides provides a state-by-state state-by-state summary summary of of managed managed care care programs programs in in operati<strong>on</strong> operati<strong>on</strong> as as of of October October2010. 2010. Appendix Appendix 2 provides provides a more more detailed detailed inventory inventory of of state state managed managed care care programs, programs, the the models modelsunder under which which they they operate, operate, and and the the <strong>Medicaid</strong> <strong>Medicaid</strong> populati<strong>on</strong>s populati<strong>on</strong>s enrolled. enrolled.3 ForForeaseeaseofofpresentati<strong>on</strong>,presentati<strong>on</strong>,DCDCisiscountedcountedasasa statestateininthisthisreport,report,includingincludingallalltablestablesandandcharts.charts.13
- Page 1 and 2: kaisercommission onmedicaidand theu
- Page 3 and 4: kaisercommission onmedicaidand theu
- Page 5 and 6: Table of ContentsExecutive Summary
- Page 7 and 8: EXECUTIVE SUMMARYMedicaid, the publ
- Page 9 and 10: party enrollment brokers to provide
- Page 11 and 12: HEDIS©, CAHPS©, and state-specifi
- Page 13: ConclusionFor over 30 years, state
- Page 16 and 17: from the recession and the slow rec
- Page 20 and 21: Managed caremodelTable 1: Medicaid
- Page 23 and 24: States are increasingly mandating m
- Page 25 and 26: States with Medicaid MCOsKey Sectio
- Page 27 and 28: States have “auto-assignment” a
- Page 29 and 30: excess of a specified threshold for
- Page 31 and 32: Dental care and outpatient and inpa
- Page 33 and 34: the second trimester, and within th
- Page 35 and 36: eported that they limit PCP panel s
- Page 37 and 38: States with non-comprehensive PHPsK
- Page 39 and 40: Measuring, monitoring, and improvin
- Page 41 and 42: seven states required 10 measures o
- Page 43 and 44: CAHPS© surveys. North Carolina is
- Page 45 and 46: Special initiatives to improve qual
- Page 47 and 48: public health efforts to reduce dis
- Page 49 and 50: Medicaid managed long-term care and
- Page 51 and 52: (e.g., need to credential Adult <st
- Page 53 and 54: In many states, broader efforts foc
- Page 55 and 56: Looking ahead: Medicaid managed car
- Page 57 and 58: ConclusionFor over 30 years, state
- Page 59 and 60: APPENDIX 2: Summary of Medicaid Man
- Page 61 and 62: Program Name(e.g., Popular Name, 19
- Page 63 and 64: APPENDIX 3: MCO Contracts, Plan Cha
- Page 65 and 66: State(No. ofcontracts)NameEnrollmen
- Page 67 and 68: State(No. ofcontracts)NameEnrollmen
- Page 69 and 70:
APPENDIX 5: MCO Capitation Rate-Set
- Page 71 and 72:
APPENDIX 7: MCO Network Adequacy Re
- Page 73 and 74:
State Primary Care Obstetric Care S
- Page 75 and 76:
APPENDIX 9: Providers Recognized as
- Page 77 and 78:
APPENDIX 11: PCCM Administrative Se
- Page 79 and 80:
APPENDIX 13: Initiatives to Improve
- Page 81 and 82:
I. MANAGED CARE OVERVIEW1. Total Ma
- Page 83 and 84:
4. Enrollment Requirements.a. We ar
- Page 85 and 86:
ii. Please indicate whether the fac
- Page 87 and 88:
c. Required Providers: We are inter
- Page 89 and 90:
IV. NON-COMPREHENSIVE PREPAID HEALT
- Page 91 and 92:
. Does your state use CAHPS© surve
- Page 93 and 94:
VI. SPECIAL INITIATIVESAll states s
- Page 95 and 96:
Appendix I: Managed Care Contracts1
- Page 97:
Appendix II: Clinical Quality Perfo
- Page 100:
1330 G S T R E E T NW, W A S H I N