appropriate providers that is … sufficient to provide adequate access to all services covered under thec<strong>on</strong>tract.” 16 In establishing networks, MCOs are required to c<strong>on</strong>sider a number of factors, includinganticipated <strong>Medicaid</strong> enrollment, expected utilizati<strong>on</strong>, the geographic locati<strong>on</strong> of providers relative toenrollees, and physical accessibility for enrollees with disabilities. Female enrollees must have direct innetworkaccess to a women’s health specialist. The federal regulati<strong>on</strong>s also require plans to meet statestandards for timely access to care and services and make services available 24/7 when medicallynecessary.The survey asked states with MCOs to describe their network adequacy standards for primary care,obstetric care, specialty care, hospital care, and dental care.<strong>State</strong>s use a variety of network adequacy standards for primary care. <strong>State</strong>s set network adequacystandards for MCOs in different ways, such as requiring minimum provider-to-populati<strong>on</strong> ratios, anddistance and travel-time maximums. <strong>State</strong>s reported a range of minimum primary care provider (PCP)-to-enrollee standards. For example, Maryland and Massachusetts require at least <strong>on</strong>e PCP per 200<strong>Medicaid</strong> enrollees; in c<strong>on</strong>trast, in South Carolina, the required ratio is <strong>on</strong>e PCP per 2,500 enrollees. Twostates reported separate standards for pediatricians: Illinois requires <strong>on</strong>e PCP per 1,200 enrollees, but<strong>on</strong>e pediatrician per 2,000 child enrollees. Similarly, Virginia requires <strong>on</strong>e PCP per 1,500 enrollees, but<strong>on</strong>e PCP with pediatric training or experience for every 2,500 child enrollees.<strong>State</strong>s also reported a wide range of distance standards and frequently apply different standards forurban and rural areas. For example, Georgia requires two PCPs within eight miles of an MCO enrollee inurban areas and within 15 miles in rural areas, while New Mexico uses a 30-mile standard for urbanareas, 45 miles for rural areas, and 60 miles for fr<strong>on</strong>tier areas. A few states also reported differing waittimestandards for routine care and urgent care appointments. For example, in New Mexico, routine,asymptomatic primary preventive care appointments must be scheduled within 30 days; routine,symptomatic, n<strong>on</strong>-urgent primary care appointments within 14 days; and urgent care appointmentswithin 24 hours.Network adequacy standards for specialty care also vary. <strong>State</strong>s’ network adequacy standards forspecialists may also be set in terms of provider-to-populati<strong>on</strong> ratios or time or distance thresholds, andvary for urban and rural areas and by other factors. For example, Indiana requires two providers within60 miles of a member’s residence for some specialties and <strong>on</strong>e provider within 90 miles for others. InMassachusetts, the standard for the top five specialist types is 1 per 500 enrollees. For certain types ofspecialists, Pennsylvania requires a choice of two providers accepting new patients within 30 minutes inurban areas and 60 minutes in rural areas; for other types of specialists, <strong>on</strong>e provider within thosetime/distance parameters is required.Network adequacy standards for obstetric care vary widely as well. In many states, panel size anddistance requirements for obstetric care mirror the requirements for primary care – with all theirvariati<strong>on</strong>. Some network adequacy standards are not expressed in quantitative terms (e.g., “networkmust be adequate to serve members; otherwise MCO must approve out-of-network care” or “openaccess to OB services” or “sufficient to serve assigned populati<strong>on</strong>”), likely making them more difficult tom<strong>on</strong>itor and enforce. Hawaii requires <strong>on</strong>e obstetric provider <strong>on</strong> each island a plan serves. <strong>State</strong>s alsoreported specific timeliness requirements for prenatal care. For example, Nevada requires plans toprovide an appointment for prenatal care within seven days of the first request in the first trimester and16 42 CFR §438.206.26 00
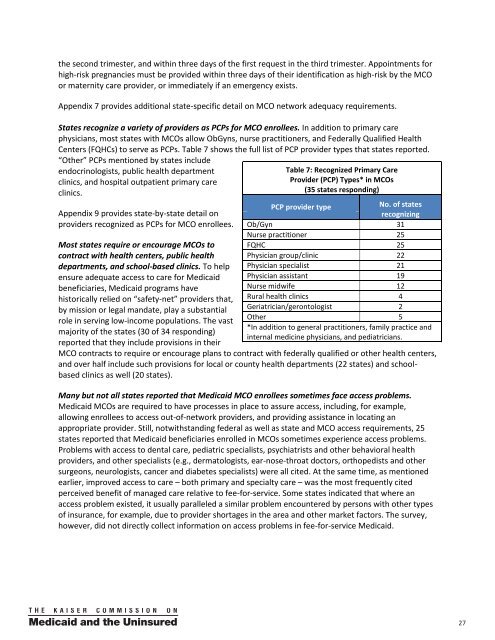
the sec<strong>on</strong>d trimester, and within three days of the first request in the third trimester. Appointments forhigh-risk pregnancies must be provided within three days of their identificati<strong>on</strong> as high-risk by the MCOor maternity care provider, or immediately if an emergency exists.Appendix 7 provides additi<strong>on</strong>al state-specific detail <strong>on</strong> MCO network adequacy requirements.<strong>State</strong>s recognize a variety of providers as PCPs for MCO enrollees. In additi<strong>on</strong> to primary carephysicians, most states with MCOs allow ObGyns, nurse practiti<strong>on</strong>ers, and Federally Qualified HealthCenters (FQHCs) to serve as PCPs. Table 7 shows the full list of PCP provider types that states reported.“Other” PCPs menti<strong>on</strong>ed by states includeendocrinologists, public health departmentclinics, and hospital outpatient primary careclinics.Appendix 9 provides state-by-state detail <strong>on</strong>providers recognized as PCPs for MCO enrollees.Most states require or encourage MCOs toc<strong>on</strong>tract with health centers, public healthdepartments, and school-based clinics. To helpensure adequate access to care for <strong>Medicaid</strong>beneficiaries, <strong>Medicaid</strong> programs havehistorically relied <strong>on</strong> “safety-net” providers that,by missi<strong>on</strong> or legal mandate, play a substantialrole in serving low-income populati<strong>on</strong>s. The vastmajority of the states (30 of 34 resp<strong>on</strong>ding)reported that they include provisi<strong>on</strong>s in theirTable 7: Recognized Primary <strong>Care</strong>Provider (PCP) Types* in MCOs(35 states resp<strong>on</strong>ding)PCP provider typeNo. of statesrecognizingOb/Gyn 31Nurse practiti<strong>on</strong>er 25FQHC 25Physician group/clinic 22Physician specialist 21Physician assistant 19Nurse midwife 12Rural health clinics 4Geriatrician/ger<strong>on</strong>tologist 2Other 5*In additi<strong>on</strong> to general practiti<strong>on</strong>ers, family practice andinternal medicine physicians, and pediatricians.MCO c<strong>on</strong>tracts to require or encourage plans to c<strong>on</strong>tract with federally qualified or other health centers,and over half include such provisi<strong>on</strong>s for local or county health departments (22 states) and schoolbasedclinics as well (20 states).Many but not all states reported that <strong>Medicaid</strong> MCO enrollees sometimes face access problems.<strong>Medicaid</strong> MCOs are required to have processes in place to assure access, including, for example,allowing enrollees to access out-of-network providers, and providing assistance in locating anappropriate provider. Still, notwithstanding federal as well as state and MCO access requirements, 25states reported that <strong>Medicaid</strong> beneficiaries enrolled in MCOs sometimes experience access problems.Problems with access to dental care, pediatric specialists, psychiatrists and other behavioral healthproviders, and other specialists (e.g., dermatologists, ear-nose-throat doctors, orthopedists and othersurge<strong>on</strong>s, neurologists, cancer and diabetes specialists) were all cited. At the same time, as menti<strong>on</strong>edearlier, improved access to care – both primary and specialty care – was the most frequently citedperceived benefit of managed care relative to fee-for-service. Some states indicated that where anaccess problem existed, it usually paralleled a similar problem encountered by pers<strong>on</strong>s with other typesof insurance, for example, due to provider shortages in the area and other market factors. The survey,however, did not directly collect informati<strong>on</strong> <strong>on</strong> access problems in fee-for-service <strong>Medicaid</strong>.27
- Page 1 and 2: kaisercommission onmedicaidand theu
- Page 3 and 4: kaisercommission onmedicaidand theu
- Page 5 and 6: Table of ContentsExecutive Summary
- Page 7 and 8: EXECUTIVE SUMMARYMedicaid, the publ
- Page 9 and 10: party enrollment brokers to provide
- Page 11 and 12: HEDIS©, CAHPS©, and state-specifi
- Page 13: ConclusionFor over 30 years, state
- Page 16 and 17: from the recession and the slow rec
- Page 18 and 19: A note on Medicaid managed care ter
- Page 20 and 21: Managed caremodelTable 1: Medicaid
- Page 23 and 24: States are increasingly mandating m
- Page 25 and 26: States with Medicaid MCOsKey Sectio
- Page 27 and 28: States have “auto-assignment” a
- Page 29 and 30: excess of a specified threshold for
- Page 31: Dental care and outpatient and inpa
- Page 35 and 36: eported that they limit PCP panel s
- Page 37 and 38: States with non-comprehensive PHPsK
- Page 39 and 40: Measuring, monitoring, and improvin
- Page 41 and 42: seven states required 10 measures o
- Page 43 and 44: CAHPS© surveys. North Carolina is
- Page 45 and 46: Special initiatives to improve qual
- Page 47 and 48: public health efforts to reduce dis
- Page 49 and 50: Medicaid managed long-term care and
- Page 51 and 52: (e.g., need to credential Adult <st
- Page 53 and 54: In many states, broader efforts foc
- Page 55 and 56: Looking ahead: Medicaid managed car
- Page 57 and 58: ConclusionFor over 30 years, state
- Page 59 and 60: APPENDIX 2: Summary of Medicaid Man
- Page 61 and 62: Program Name(e.g., Popular Name, 19
- Page 63 and 64: APPENDIX 3: MCO Contracts, Plan Cha
- Page 65 and 66: State(No. ofcontracts)NameEnrollmen
- Page 67 and 68: State(No. ofcontracts)NameEnrollmen
- Page 69 and 70: APPENDIX 5: MCO Capitation Rate-Set
- Page 71 and 72: APPENDIX 7: MCO Network Adequacy Re
- Page 73 and 74: State Primary Care Obstetric Care S
- Page 75 and 76: APPENDIX 9: Providers Recognized as
- Page 77 and 78: APPENDIX 11: PCCM Administrative Se
- Page 79 and 80: APPENDIX 13: Initiatives to Improve
- Page 81 and 82: I. MANAGED CARE OVERVIEW1. Total Ma
- Page 83 and 84:
4. Enrollment Requirements.a. We ar
- Page 85 and 86:
ii. Please indicate whether the fac
- Page 87 and 88:
c. Required Providers: We are inter
- Page 89 and 90:
IV. NON-COMPREHENSIVE PREPAID HEALT
- Page 91 and 92:
. Does your state use CAHPS© surve
- Page 93 and 94:
VI. SPECIAL INITIATIVESAll states s
- Page 95 and 96:
Appendix I: Managed Care Contracts1
- Page 97:
Appendix II: Clinical Quality Perfo
- Page 100:
1330 G S T R E E T NW, W A S H I N