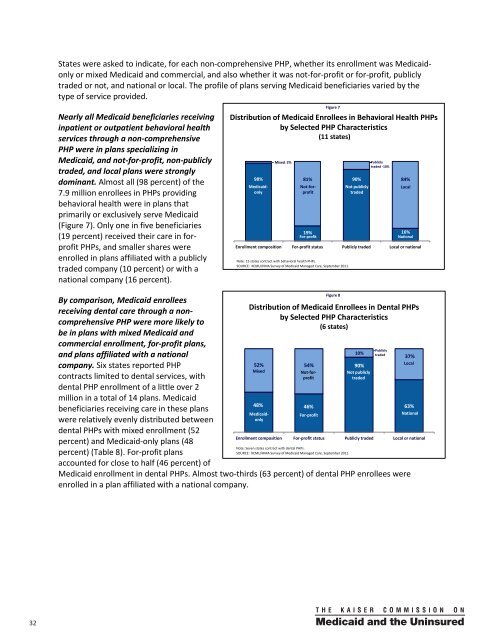
<strong>State</strong>s were asked to indicate, for each n<strong>on</strong>-comprehensive PHP, whether its enrollment was <strong>Medicaid</strong><strong>on</strong>lyor mixed <strong>Medicaid</strong> and commercial, and also whether it was not-for-profit or for-profit, publiclytraded or not, and nati<strong>on</strong>al or local. The profile of plans serving <strong>Medicaid</strong> beneficiaries varied by thetype of service provided.Nearly all <strong>Medicaid</strong> beneficiaries receivinginpatient or outpatient behavioral healthservices through a n<strong>on</strong>-comprehensivePHP were in plans specializing in<strong>Medicaid</strong>, and not-for-profit, n<strong>on</strong>-publiclytraded, and local plans were str<strong>on</strong>glydominant. Almost all (98 percent) of the7.9 milli<strong>on</strong> enrollees in PHPs providingbehavioral health were in plans thatprimarily or exclusively serve <strong>Medicaid</strong>(Figure 7). Only <strong>on</strong>e in five beneficiaries(19 percent) received their care in forprofitPHPs, and smaller shares wereenrolled in plans affiliated with a publiclytraded company (10 percent) or with anati<strong>on</strong>al company (16 percent).By comparis<strong>on</strong>, <strong>Medicaid</strong> enrolleesreceiving dental care through a n<strong>on</strong>comprehensivePHP were more likely tobe in plans with mixed <strong>Medicaid</strong> andcommercial enrollment, for-profit plans,and plans affiliated with a nati<strong>on</strong>alcompany. Six states reported PHPc<strong>on</strong>tracts limited to dental services, withdental PHP enrollment of a little over 2milli<strong>on</strong> in a total of 14 plans. <strong>Medicaid</strong>beneficiaries receiving care in these planswere relatively evenly distributed betweendental PHPs with mixed enrollment (52percent) and <strong>Medicaid</strong>-<strong>on</strong>ly plans (48percent) (Table 8). For-profit plansaccounted for close to half (46 percent) ofFigure 7Distributi<strong>on</strong> of <strong>Medicaid</strong> Enrollees in Behavioral Health PHPsby Selected PHP Characteristics(11 states)<strong>Medicaid</strong> enrollment in dental PHPs. Almost two-thirds (63 percent) of dental PHP enrollees wereenrolled in a plan affiliated with a nati<strong>on</strong>al company.98%Mixed– 2%81% 90%84%19%For-profit16%Nati<strong>on</strong>alEnrollment compositi<strong>on</strong> For-profit status Publicly traded Local or nati<strong>on</strong>alNote: 15 states c<strong>on</strong>tract with behavioral health PHPs.SOURCE: KCMU/HMA <str<strong>on</strong>g>Survey</str<strong>on</strong>g> of <strong>Medicaid</strong> <strong>Managed</strong> <strong>Care</strong>, September 2011.Figure 8Not publiclytradedPubliclytraded -10%LocalDistributi<strong>on</strong> of <strong>Medicaid</strong> Enrollees in Dental PHPsby Selected PHP Characteristics(6 states)<strong>Medicaid</strong><strong>on</strong>ly52% 54%MixedNot-forprofit48% 46%<strong>Medicaid</strong><strong>on</strong>lyNot-forprofitFor-profit10%90%Not publiclytraded37%Local63%Nati<strong>on</strong>alEnrollment compositi<strong>on</strong> For-profit status Publicly traded Local or nati<strong>on</strong>alNote: Seven states c<strong>on</strong>tract with dental PHPs.SOURCE: KCMU/HMA <str<strong>on</strong>g>Survey</str<strong>on</strong>g> of <strong>Medicaid</strong> <strong>Managed</strong> <strong>Care</strong>, September 2011.Publiclytraded32 00
Measuring, m<strong>on</strong>itoring, and improving quality in <strong>Medicaid</strong> managed careKey Secti<strong>on</strong> Findings:All states with MCOs and most states with PCCM programs require HEDIS© or other measuresof performance and CAHPS© or other surveys of patient experience. Required measures focusheavily <strong>on</strong> <strong>Medicaid</strong> priority areas such as prenatal and post-partum care, child health,preventive care, management of asthma, diabetes, and other chr<strong>on</strong>ic c<strong>on</strong>diti<strong>on</strong>s, and access.Of the 48 states with MCOs and/or PCCM programs, over a quarter also measure and m<strong>on</strong>itorquality in their fee-for-service delivery systems.Of the 36 states with MCOs, 16 require health plans to be accredited by a recognized nati<strong>on</strong>alaccrediting organizati<strong>on</strong>, such as NCQA, to participate in <strong>Medicaid</strong>.Over three-fourths of states with MCOs publicly report <strong>on</strong> the quality of their MCOs, and half ofPCCM states publish quality reports <strong>on</strong> their PCCM programs. A smaller number of states alsopublicly report <strong>on</strong> PHP performance. Sixteen states with MCOs reported that they prepare aquality report card, using HEDIS©, CAHPS©, and state-specific measures, that <strong>Medicaid</strong>beneficiaries can use to compare and choose health plans.Quality improvement projects in the states with MCOs reveal the breadth of state priorities,including, am<strong>on</strong>g others, improved birth outcomes, increased access to pediatric subspecialists,identificati<strong>on</strong> of high-risk individuals for case management, and coordinati<strong>on</strong> betweenbehavioral health and medical providers.<strong>Managed</strong> care provides a platform for states to ensure the quality of care for <strong>Medicaid</strong> beneficiaries.Federal regulati<strong>on</strong>s define requirements that both states and health plans must meet to measure,m<strong>on</strong>itor, ensure, and improve the quality of care provided to <strong>Medicaid</strong> beneficiaries enrolled in riskbasedmanaged care, including both MCOs and n<strong>on</strong>-comprehensive PHPs. Each state c<strong>on</strong>tracting withplans must have a written quality strategy that includes specified elements, including nati<strong>on</strong>alperformance measures, and must, through its c<strong>on</strong>tracts, ensure plan compliance with standards set bythe state. C<strong>on</strong>tracts with plans must require <strong>on</strong>going quality assessment and performance improvementprojects (PIP), and submissi<strong>on</strong> of performance data to the state; states must also arrange for annualexternal reviews of the quality, appropriateness, and timeliness of services furnished to <strong>Medicaid</strong>enrollees. Similar requirements do not exist for fee-for-service.With electr<strong>on</strong>ic data increasingly available <strong>on</strong> many aspects of utilizati<strong>on</strong>, clinical outcomes, and patientexperience, states have growing opportunities to examine health plan and health system performanceacross a broad spectrum of quality-related measures. <strong>Managed</strong> care offers a structure in whichperformance can be measured and enforced. Through managed care c<strong>on</strong>tracts, states can specifybenchmarks for acceptable performance and hold health plans accountable for their achievement, andstructure payment to reward (or penalize) good (or poor) performance. The survey asked states anumber of questi<strong>on</strong>s c<strong>on</strong>cerning the nature and breadth of current and planned activity aimed atmeasuring and improving quality in <strong>Medicaid</strong>.Appendix 12 provides a summary of states’ use of selected quality tools.Of the 36 states with MCOs, 16 require that risk-based plans be accredited to participate in <strong>Medicaid</strong>.One means by which states can assure quality in risk-based plans is to require that, as a c<strong>on</strong>diti<strong>on</strong> ofparticipating in <strong>Medicaid</strong>, they obtain accreditati<strong>on</strong> from a nati<strong>on</strong>al accrediting body, such as the33
- Page 1 and 2: kaisercommission onmedicaidand theu
- Page 3 and 4: kaisercommission onmedicaidand theu
- Page 5 and 6: Table of ContentsExecutive Summary
- Page 7 and 8: EXECUTIVE SUMMARYMedicaid, the publ
- Page 9 and 10: party enrollment brokers to provide
- Page 11 and 12: HEDIS©, CAHPS©, and state-specifi
- Page 13: ConclusionFor over 30 years, state
- Page 16 and 17: from the recession and the slow rec
- Page 18 and 19: A note on Medicaid managed care ter
- Page 20 and 21: Managed caremodelTable 1: Medicaid
- Page 23 and 24: States are increasingly mandating m
- Page 25 and 26: States with Medicaid MCOsKey Sectio
- Page 27 and 28: States have “auto-assignment” a
- Page 29 and 30: excess of a specified threshold for
- Page 31 and 32: Dental care and outpatient and inpa
- Page 33 and 34: the second trimester, and within th
- Page 35 and 36: eported that they limit PCP panel s
- Page 37: States with non-comprehensive PHPsK
- Page 41 and 42: seven states required 10 measures o
- Page 43 and 44: CAHPS© surveys. North Carolina is
- Page 45 and 46: Special initiatives to improve qual
- Page 47 and 48: public health efforts to reduce dis
- Page 49 and 50: Medicaid managed long-term care and
- Page 51 and 52: (e.g., need to credential Adult <st
- Page 53 and 54: In many states, broader efforts foc
- Page 55 and 56: Looking ahead: Medicaid managed car
- Page 57 and 58: ConclusionFor over 30 years, state
- Page 59 and 60: APPENDIX 2: Summary of Medicaid Man
- Page 61 and 62: Program Name(e.g., Popular Name, 19
- Page 63 and 64: APPENDIX 3: MCO Contracts, Plan Cha
- Page 65 and 66: State(No. ofcontracts)NameEnrollmen
- Page 67 and 68: State(No. ofcontracts)NameEnrollmen
- Page 69 and 70: APPENDIX 5: MCO Capitation Rate-Set
- Page 71 and 72: APPENDIX 7: MCO Network Adequacy Re
- Page 73 and 74: State Primary Care Obstetric Care S
- Page 75 and 76: APPENDIX 9: Providers Recognized as
- Page 77 and 78: APPENDIX 11: PCCM Administrative Se
- Page 79 and 80: APPENDIX 13: Initiatives to Improve
- Page 81 and 82: I. MANAGED CARE OVERVIEW1. Total Ma
- Page 83 and 84: 4. Enrollment Requirements.a. We ar
- Page 85 and 86: ii. Please indicate whether the fac
- Page 87 and 88: c. Required Providers: We are inter
- Page 89 and 90:
IV. NON-COMPREHENSIVE PREPAID HEALT
- Page 91 and 92:
. Does your state use CAHPS© surve
- Page 93 and 94:
VI. SPECIAL INITIATIVESAll states s
- Page 95 and 96:
Appendix I: Managed Care Contracts1
- Page 97:
Appendix II: Clinical Quality Perfo
- Page 100:
1330 G S T R E E T NW, W A S H I N