Aged Care & Rehabilitation Clinical Services Plan 2007 – 2012
Aged Care & Rehabilitation Clinical Services Plan 2007 – 2012
Aged Care & Rehabilitation Clinical Services Plan 2007 – 2012

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
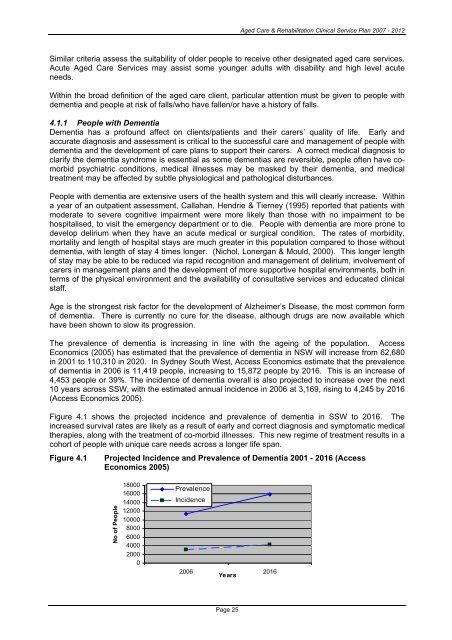
<strong>Aged</strong> <strong>Care</strong> & <strong>Rehabilitation</strong> <strong>Clinical</strong> Service <strong>Plan</strong> <strong>2007</strong> - <strong>2012</strong>Similar criteria assess the suitability of older people to receive other designated aged care services.Acute <strong>Aged</strong> <strong>Care</strong> <strong>Services</strong> may assist some younger adults with disability and high level acuteneeds.Within the broad definition of the aged care client, particular attention must be given to people withdementia and people at risk of falls/who have fallen/or have a history of falls.4.1.1 People with DementiaDementia has a profound affect on clients/patients and their carers’ quality of life. Early andaccurate diagnosis and assessment is critical to the successful care and management of people withdementia and the development of care plans to support their carers. A correct medical diagnosis toclarify the dementia syndrome is essential as some dementias are reversible, people often have comorbidpsychiatric conditions, medical illnesses may be masked by their dementia, and medicaltreatment may be affected by subtle physiological and pathological disturbances.People with dementia are extensive users of the health system and this will clearly increase. Withina year of an outpatient assessment, Callahan, Hendrie & Tierney (1995) reported that patients withmoderate to severe cognitive impairment were more likely than those with no impairment to behospitalised, to visit the emergency department or to die. People with dementia are more prone todevelop delirium when they have an acute medical or surgical condition. The rates of morbidity,mortality and length of hospital stays are much greater in this population compared to those withoutdementia, with length of stay 4 times longer. (Nichol, Lonergan & Mould, 2000). This longer lengthof stay may be able to be reduced via rapid recognition and management of delirium, involvement ofcarers in management plans and the development of more supportive hospital environments, both interms of the physical environment and the availability of consultative services and educated clinicalstaff.Age is the strongest risk factor for the development of Alzheimer’s Disease, the most common formof dementia. There is currently no cure for the disease, although drugs are now available whichhave been shown to slow its progression.The prevalence of dementia is increasing in line with the ageing of the population. AccessEconomics (2005) has estimated that the prevalence of dementia in NSW will increase from 62,680in 2001 to 110,310 in 2020. In Sydney South West, Access Economics estimate that the prevalenceof dementia in 2006 is 11,419 people, increasing to 15,872 people by 2016. This is an increase of4,453 people or 39%. The incidence of dementia overall is also projected to increase over the next10 years across SSW, with the estimated annual incidence in 2006 at 3,169, rising to 4,245 by 2016(Access Economics 2005).Figure 4.1 shows the projected incidence and prevalence of dementia in SSW to 2016. Theincreased survival rates are likely as a result of early and correct diagnosis and symptomatic medicaltherapies, along with the treatment of co-morbid illnesses. This new regime of treatment results in acohort of people with unique care needs across a longer life span.Figure 4.1Projected Incidence and Prevalence of Dementia 2001 - 2016 (AccessEconomics 2005)No of People180001600014000120001000080006000400020000PrevalenceIncidence2006 2016YearsPage 25