Diagnosis and Management of Pituitary Tumors
Diagnosis and Management of Pituitary Tumors
Diagnosis and Management of Pituitary Tumors

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
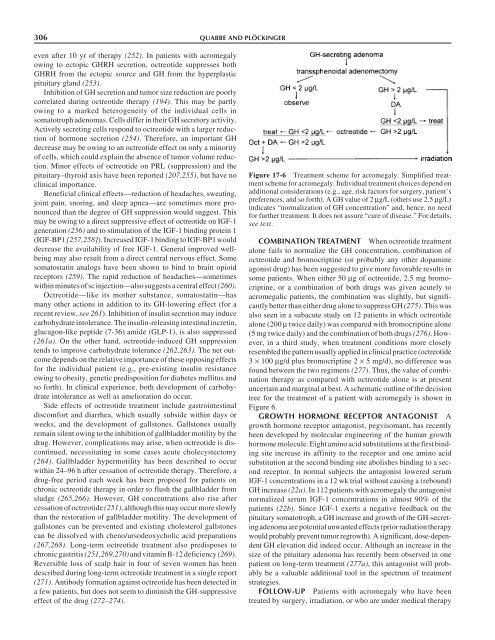
306 QUABBE AND PLÖCKINGEReven after 10 yr <strong>of</strong> therapy (252). In patients with acromegalyowing to ectopic GHRH secretion, octreotide suppresses bothGHRH from the ectopic source <strong>and</strong> GH from the hyperplasticpituitary gl<strong>and</strong> (253).Inhibition <strong>of</strong> GH secretion <strong>and</strong> tumor size reduction are poorlycorrelated during octreotide therapy (194). This may be partlyowing to a marked heterogeneity <strong>of</strong> the individual cells insomatotroph adenomas. Cells differ in their GH secretory activity.Actively secreting cells respond to octreotide with a larger reduction<strong>of</strong> hormone secretion (254). Therefore, an important GHdecrease may be owing to an octreotide effect on only a minority<strong>of</strong> cells, which could explain the absence <strong>of</strong> tumor volume reduction.Minor effects <strong>of</strong> octreotide on PRL (suppression) <strong>and</strong> thepituitary–thyroid axis have been reported (207,255), but have noclinical importance.Beneficial clinical effects—reduction <strong>of</strong> headaches, sweating,joint pain, snoring, <strong>and</strong> sleep apnea—are sometimes more pronouncedthan the degree <strong>of</strong> GH suppression would suggest. Thismay be owing to a direct suppressive effect <strong>of</strong> octreotide on IGF-1generation (256) <strong>and</strong> to stimulation <strong>of</strong> the IGF-1 binding protein 1(IGF-BP1 [257,258]). Increased IGF-1 binding to IGF-BP1 woulddecrease the availability <strong>of</strong> free IGF-1. General improved wellbeingmay also result from a direct central nervous effect. Somesomatostatin analogs have been shown to bind to brain opioidreceptors (259). The rapid reduction <strong>of</strong> headaches—sometimeswithin minutes <strong>of</strong> sc injection—also suggests a central effect (260).Octreotide—like its mother substance, somatostatin—hasmany other actions in addition to its GH-lowering effect (for arecent review, see 261). Inhibition <strong>of</strong> insulin secretion may inducecarbohydrate intolerance. The insulin-releasing intestinal incretin,glucagon-like peptide (7-36) amide (GLP-1), is also suppressed(261a). On the other h<strong>and</strong>, octreotide-induced GH suppressiontends to improve carbohydrate tolerance (262,263). The net outcomedepends on the relative importance <strong>of</strong> these opposing effectsfor the individual patient (e.g., pre-existing insulin resistanceowing to obesity, genetic predisposition for diabetes mellitus <strong>and</strong>so forth). In clinical experience, both development <strong>of</strong> carbohydrateintolerance as well as amelioration do occur.Side effects <strong>of</strong> octreotide treatment include gastrointestinaldiscomfort <strong>and</strong> diarrhea, which usually subside within days orweeks, <strong>and</strong> the development <strong>of</strong> gallstones. Gallstones usuallyremain silent owing to the inhibition <strong>of</strong> gallbladder motility by thedrug. However, complications may arise, when octreotide is discontinued,necessitating in some cases acute cholecystectomy(264). Gallbladder hypermotility has been described to occurwithin 24–96 h after cessation <strong>of</strong> octreotide therapy. Therefore, adrug-free period each week has been proposed for patients onchronic octreotide therapy in order to flush the gallbladder fromsludge (265,266). However, GH concentrations also rise aftercessation <strong>of</strong> octreotide (251), although this may occur more slowlythan the restoration <strong>of</strong> gallbladder motility. The development <strong>of</strong>gallstones can be prevented <strong>and</strong> existing cholesterol gallstonescan be dissolved with cheno/ursodeoxycholic acid preparations(267,268). Long-term octreotide treatment also predisposes tochronic gastritis (251,269,270)<strong>and</strong> vitamin B-12 deficiency (269).Reversible loss <strong>of</strong> scalp hair in four <strong>of</strong> seven women has beendescribed during long-term octreotide treatment in a single report(271). Antibody formation against octreotide has been detected ina few patients, but does not seem to diminish the GH-suppressiveeffect <strong>of</strong> the drug (272–274).Figure 17-6 Treatment scheme for acromegaly. Simplified treatmentscheme for acromegaly. Individual treatment choices depend onadditional considerations (e.g., age, risk factors for surgery, patient’spreferences, <strong>and</strong> so forth). A GH value <strong>of</strong> 2 µg/L (others use 2.5 µg/L)indicates “normalization <strong>of</strong> GH concentration” <strong>and</strong>, hence, no needfor further treatment. It does not assure “cure <strong>of</strong> disease.” For details,see text.COMBINATION TREATMENT When octreotide treatmentalone fails to normalize the GH concentration, combination <strong>of</strong>octreotide <strong>and</strong> bromocriptine (or probably any other dopamineagonist drug) has been suggested to give more favorable results insome patients. When either 50 µg <strong>of</strong> octreotide, 2.5 mg bromocriptine,or a combination <strong>of</strong> both drugs was given acutely toacromegalic patients, the combination was slightly, but significantlybetter than either drug alone to suppress GH (275). This wasalso seen in a subacute study on 12 patients in which octreotidealone (200 µ twice daily) was compared with bromocriptine alone(5 mg twice daily) <strong>and</strong> the combination <strong>of</strong> both drugs (276). However,in a third study, when treatment conditions more closelyresembled the pattern usually applied in clinical practice (octreotide3 × 100 µg/d plus bromocriptine 2 × 5 mg/d), no difference wasfound between the two regimens (277). Thus, the value <strong>of</strong> combinationtherapy as compared with octreotide alone is at presentuncertain <strong>and</strong> marginal at best. A schematic outline <strong>of</strong> the decisiontree for the treatment <strong>of</strong> a patient with acromegaly is shown inFigure 6.GROWTH HORMONE RECEPTOR ANTAGONIST Agrowth hormone receptor antagonist, pegvisomant, has recentlybeen developed by molecular engineering <strong>of</strong> the human growthhormone molecule. Eight amino acid substitutions at the first bindingsite increase its affinity to the receptor <strong>and</strong> one amino acidsubstitution at the second binding site abolishes binding to a secondreceptor. In normal subjects the antagonist lowered serumIGF-1 concentrations in a 12 wk trial without causing a (rebound)GH increase (22a). In 112 patients with acromegaly the antagonistnormalized serum IGF-1 concentrations in almost 90% <strong>of</strong> thepatients (22b). Since IGF-1 exerts a negative feedback on thepituitary somatotroph, a GH increase <strong>and</strong> growth <strong>of</strong> the GH-secretingadenoma are potential unwanted effects (prior radiation therapywould probably prevent tumor regrowth). A significant, dose-dependentGH elevation did indeed occur. Although an increase in thesize <strong>of</strong> the pituitary adenoma has recently been observed in onepatient on long-term treatment (277a), this antagonist will probablybe a valuable additional tool in the spectrum <strong>of</strong> treatmentstrategies.FOLLOW-UP Patients with acromegaly who have beentreated by surgery, irradiation, or who are under medical therapy