OUTLOOK
January 2013 - IPCSA
January 2013 - IPCSA

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
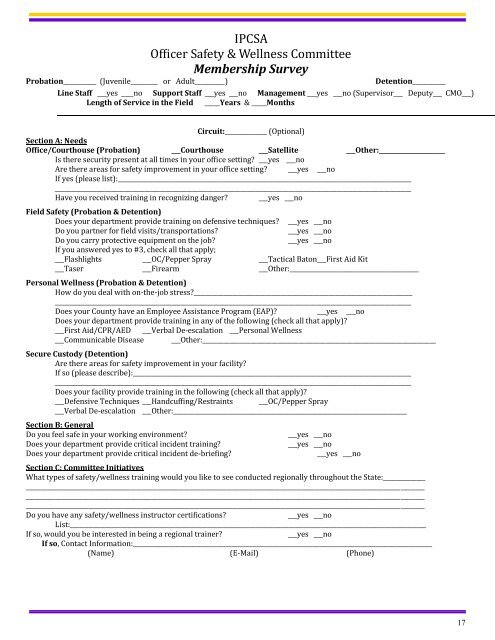
IPCSAOfficer Safety & Wellness CommitteeMembership SurveyProbation___________ (Juvenile_________ or Adult__________)Detention___________Line Staff ___yes ____no Support Staff ___yes ___no Management ___yes ___no (Supervisor___ Deputy___ CMO___)Length of Service in the Field _____Years & _____MonthsCircuit:______________ (Optional)Section A: NeedsOffice/Courthouse (Probation) ___Courthouse ___Satellite ___Other:______________________Is there security present at all times in your office setting? ___yes ___noAre there areas for safety improvement in your office setting? ___yes ___noIf yes (please list):_________________________________________________________________________________________________________________________________________________________________________________________________________________________Have you received training in recognizing danger? ___yes ___noField Safety (Probation & Detention)Does your department provide training on defensive techniques? ___yes ___noDo you partner for field visits/transportations?___yes ___noDo you carry protective equipment on the job?___yes ___noIf you answered yes to #3, check all that apply;___Flashlights ___OC/Pepper Spray ___Tactical Baton___First Aid Kit___Taser ___Firearm ___Other:___________________________________________Personal Wellness (Probation & Detention)How do you deal with on-the-job stress?________________________________________________________________________________________________________________________________________________________________________________________________Does your County have an Employee Assistance Program (EAP)? ___yes ___noDoes your department provide training in any of the following (check all that apply)?___First Aid/CPR/AED ___Verbal De-escalation ___Personal Wellness___Communicable Disease ___Other:______________________________________________________________________________Secure Custody (Detention)Are there areas for safety improvement in your facility?If so (please describe):____________________________________________________________________________________________________________________________________________________________________________________________________________________Does your facility provide training in the following (check all that apply)?___Defensive Techniques ___Handcuffing/Restraints ___OC/Pepper Spray___Verbal De-escalation ___Other:______________________________________________________________________________Section B: GeneralDo you feel safe in your working environment?Does your department provide critical incident training?Does your department provide critical incident de-briefing?___yes ___no___yes ___no___yes ___noSection C: Committee InitiativesWhat types of safety/wellness training would you like to see conducted regionally throughout the State:_____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________Do you have any safety/wellness instructor certifications?___yes ___noList:_______________________________________________________________________________________________________________________If so, would you be interested in being a regional trainer?___yes ___noIf so, Contact Information:____________________________________________________________________________________________________(Name) (E-Mail) (Phone)17