Collaborate Explore Discover
University of Chicago Cancer Research Center Scientific Report ...
University of Chicago Cancer Research Center Scientific Report ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Collaborate</strong> <strong>Explore</strong> <strong>Discover</strong>2008-2009Scientific Report
Director’s LetterDear Friends and Colleagues:It is my pleasure to present you with our 2008 – 2009 Scientific Report, which provides an account of theprogress we have made during the last two years. As the report documents, we are building on our strongtradition of innovative cancer research, expanding our programs, and strengthening our commitment topopulation research, epidemiology, and pediatric cancer studies. In 2008, the National Cancer Institutedesignated the University of Chicago Cancer Center (UCCRC) as a Comprehensive Cancer Center,acknowledging the “depth and breadth of research activities in each of three major areas: laboratory, clinical,and population-based research, with substantial transdisciplinary research that bridges these scientific areas.”Since 1996, we have grown from 136 to 212 members with peer-reviewed cancer research grants ofapproximately $98 million in total costs. Our members also have $25 million in non-peer reviewedgrants and contracts.As you will see in this report, our members have substantiated accomplishments in our renowned areas ofresearch, such as early-phase clinical trials, drug development, characterization of hematological malignantdiseases, new treatment paradigms in head and neck cancer, pharmacogenomics, medical imaging, andtumor immunology.We are building a world-class program in population research by recruiting key faculty in molecularepidemiology, environmental epidemiology, behavioral psychology, and chemoprevention trials research.For example, our new “Epidemiology and Recruitment Core” provides our members with uncommonexpertise and technology. We are enlisting superior faculty in other high priority areas, including systemsbiology, and are developing state-of-the-art capabilities in cancer stem cell research, metastasis research,pediatric sarcoma research, immunotherapy and translational immunology research, lymphoma research,and GI oncology.Our growing pediatric oncology program is robust with enhanced resources in its allogeneic transplantprogram, solid tumor biology and therapy program, and the expanded Pediatric Cancer Survivorship clinicaland research program. Cancer survivorship research and long-term clinical care of survivors is a chiefpriority. Consequently, we have developed the Breast Cancer Survivorship Clinic, opened in January 2008, asa joint initiative of the UCCRC Women’s Cancer Working Group, the UCCRC Breast Cancer SPORE, and theSection of Hematology/Oncology.We are proud of our past, enthusiastic about the present, and optimistic about the future. The dedication ourmembers and our supporters is the source of this confidence. The UCCRC thrives on ambitious, dauntinggoals. We can meet these challenges because of the commitment and generosity of our senior leaders,members, staff, Foundation, and many donors.With gratitude,Michelle M. Le Beau, PhDProfessor of MedicineDirector, University of Chicago Cancer Research Center
Immunology& CancerClinical & ExperimentalTherapeuticsMolecular Genetics& HematopoiesisCell Signaling &Gene RegulationOverview &AdministrationTable of ContentsOverview and Administration.. . . . . . . . . . . . . . . . . . . . . . . . . . . . 2AdvancedImagingProgramsCell Signaling and Gene Regulation Program .................6Molecular Genetics and Hematopoiesis Program .............28Immunology and Cancer Program . . . . . . . . . . . . . . . . . . . . . . . . .44Clinical and Experimental Therapeutics Program . . . . . . . . . . . .58Advanced Imaging Program ...............................80Cancer Risk and Prevention Program .......................98Clinical Trials Activity.................................120Shared Resources .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 124Cancer Risk& PreventionClincal TrialsActivitySharedResourcesOther Resources& CentersOther Resources and Centers............................132Highlights.............................................142HighlightsUCCRC SCIENTIFIC REPORT 20091
UCCRC senior staff (from left to right): Paul Butera, PhD, Hoyee Leong, PhD, Marcy List, PhD, Michelle Le Beau, PhD,Umberto Tachinardi, MD, Mary Ellen Connellan, MS, Maria Reyes, BS. Not pictured: Connie Skosey, RN
AdministrationUCCRC Executive CommitteeMichelle M. Le Beau, PhDDirectorProfessor of MedicineDirector, Cancer Cytogenetics LaboratoryMarcy A. L ist, PhDAssociate Director for AdministrationScientific Director, Cancer ClinicalTrials OfficeMarsha R. Rosner, PhDDeputy Director for Basic SciencesCharles B. Huggins ProfessorDirector, Ben May Department forCancer ResearchProfessor of Neurobiology, Pharmacologyand PhysiologyEverett E. Vokes, MDDeputy Director for Clinical SciencesJohn E. Ultmann ProfessorChairman of MedicineHabibul Ahsan, MDAssociate Director for Population ResearchProfessor of Health StudiesGeoffrey L. Greene, PhDAssociate Director for Basic Sciencesand EducationVirginia and D.K. Ludwig ProfessorAssociate Director, Ben May Departmentfor Cancer ResearchRick A. Kittles, PhDAssociate Director for Diversity andCommunity OutreachAssociate Professor of MedicineYves Lussier, MDDirector for Biomedical InformaticsAssociate Professor of MedicineMedicine Director, Center forBiomedical InformaticsMark J. Ratain, MDAssociate Director for Clinical SciencesLeon O. Jaobson Professor of MedicineChair, Committee on ClinicalPharmacology and PharmacogenomicsAdditional UCCRC SeniorLeaders and Members of theCancer Advisory CommitteeJulie A. Auger, BSAssociate Director for Core FacilitiesExecutive Director, Office of SharedResearch FacilitiesJohn Cunningham, MDProfessor and Section Chief of PediatricHematology/OncologyCarol S. Giometti, PhDBiosciences DirectorArgonne National LaboratoryOlufunmilayo Olopade, MBBSWalter L. Palmer Distinguished ServiceProfessor of MedicineAssociate Dean for Global MedicineMitchell C. Posner, MDThomas D. Jones Professor and Chiefof General SurgeryRichard L. Schilsky, MDProfessor of MedicineArieh Shalhav, MDFritz and Mary Lee Duda Chair,Professor and Chief of UrologyGary Steinberg, MDProfessor of SurgeryMichael Vannier, MDProfessor of RadiologyRalph Weichselbaum, MDDaniel K. Ludwig Professor andChairman of Radiation andCellular OncologyS. Diane Yamada, MDAssociate Professor of Obstetricsand GynecologyChief, Section of Synecological OncologyUCCRC Senior StaffPaul Butera, PhDDirector for CommunicationsMary Ellen Connellan, MSExecutive Director,Cancer Research FoundationHoyee Leong, PhDDirector for Scientific Communicationsand Strategic PartnershipsMaria Reyes, BSDirector for FinanceConnie Skosey, RNDirector for Clinical OperationsUmberto Tachinardi, MDDirector for Informatics
Overview &AdministrationUCCRC –External Advisory BoardJames K. Willson, MD (CHAIR)Director, Harold Simmons Cancer CenterUniversity of Texas SouthwesternMedical Center at DallasDonald Berry, PhDProfessor & Chair, Departmentof BiostatisticsM.D. Anderson Cancer CenterMichael A. Caligiuri, MDDirector, The Ohio State UniversityComprehensive Cancer CenterMary B. Daly, MD, PhDSenior VP for Population ScienceDirector, Cancer Prevention andControl ProgramFox Chase Cancer CenterStephen H. Friend, MD, PhDSenior Vice PresidentMerck & Co., Inc.Stanton L. Gerson, MDDirectorCase Comprehensive Cancer CenterSteven D. Gore, MDProfessor of OncologySidney Kimmel Comprehensive CancerCenter at Johns HopkinsPhilip D. Greenberg, MDProfessor of Medicine and ImmunologyUniversity of WashingtonH. Kim Lyerly, MDDirectorDuke Comprehensive Cancer CenterGloria Petersen, PhDProfessor of EpidemiologyMayo Clinic College of MedicineStephen E. Sallan, MDChief of Staff – Chief Medical Officer,Childrens Hospital Cancer CareDana-Farber Cancer InstituteMargaret R. Spitz, MDProfessor and ChairDepartment of EpidemiologyM D Anderson Cancer CenterDaniel Sullivan, MDProfessor, Department of RadiologyDuke University Medical SchoolMichael J. Weber, PhDDirector, Cancer Center at theUniversity of Virginia Health SystemJane Wegenke, BSAssociate Director – AdministrationUniversity of Wisconsin ComprehensiveCancer CenterMichael J. Welch, PhDProfessor of RadiologyDepartment of RadiologyWashington University Schoolof MedicineScott J. Leischow, PhDProfessor, Colleges of Medicine andPublic HealthArizona Cancer Center -The Universityof ArizonaC. Clifton Ling, PhD(Ad Hoc Imaging)Head, Radiation Biophysics LaboratoryMemorial Sloan-Kettering Cancer CenterUCCRC SCIENTIFIC REPORT 20095
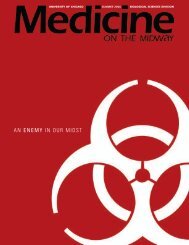
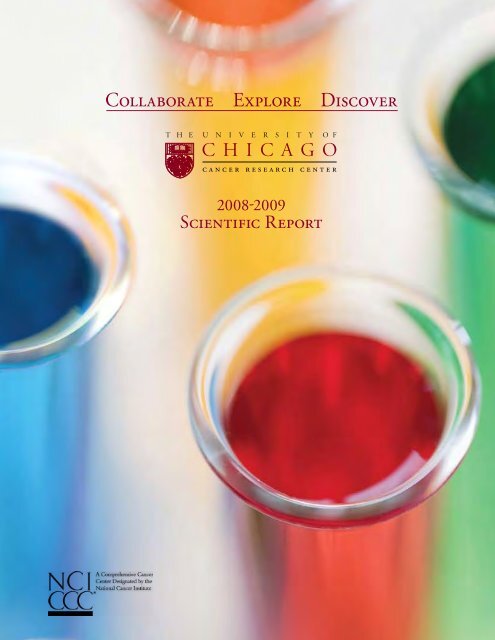
Program 1Cell Signaling and Gene Regulation4T07 metastatic mouse breast cancer cells stained with anti-APC antibody (red) and phalloidin (green). APCaccumulation is particularly associated with the ends of actin-rich cell protrusions. The protrusion-associatedAPC is necessary for the mesenchymal morphology of these cells because RNAi-mediated knockdown of APCresults in a more pronounced epithelial phenotype of the cells. (Image by C. Stengel and K. Goss)
The Program fosters collaborations between basic scientistsand clinical researchers to ultimately identify potentialtherapeutic targets and facilitate the testing of smallmolecule inhibitors of such targets.Cell Signaling &Gene RegulationOverview & GoalsThe Cell Signaling and Gene Regulation Programfocuses on determining the basic cell signalingand gene expression mechanisms that underliekey events in malignant transformation anddevelopment. The Program brings togethera diverse group of 43 basic and translationalinvestigators from 12 departments with a wealthof experience in chemistry, cell signaling,systems biology, developmental biology, and drugdiscovery. These investigators are dedicatedto discovering mechanisms of abnormal cellgrowth that could lead to innovative anti-cancertreatments.in cancerous versus normal cells, analysis oftranscription factor biology (including nuclearhormone receptors), and the structural biologyof key proteins involved in cancer etiology. TheProgram fosters collaborations between basicscientists and clinical researchers to ultimatelyidentify potential therapeutic targets and facilitatethe testing of small molecule inhibitors of suchtargets.The research aims of the Cell Signaling andGene Regulation Program are to (1) elucidatethe molecular mechanisms of tissue specific andcell type specific gene expression; (2) elucidatethe cellular mechanisms underlying cell growth/division and cell survival/death; (3) understandthe multi faceted mechanisms leading tocancer metastases; (4) use large scale, highthroughput and systems biology approaches,as well as genetic evolutionary approaches tounderstand cancer biology; and (5) discover noveldevelopmental pathways relevant to cancer cellsignaling. Particular strengths of the programinclude an emphasis on the detailed mechanisticanalysis of signal transduction and apoptoticpathways, understanding cell cycle regulationProgram Leaders:Marsha R. Rosner, PhDSuzanne D. Conzen, MDUCCRC SCIENTIFIC REPORT 20097
8MembersInvestigator*Kenneth Alexander MD, PhDEric Beyer MD, PhDDavid Boone PhDSteven Chmura MD, PhDSuzanne Conzen MDWei Du PhDNickolai Dulin PhDEdwin Ferguson PhDKathleen Goss PhDGeoffrey Greene PhDRex Haydon MD, PhDYu Ying He PhDTong-Chuan He MD, PhDAkira Imamoto PhDRichard Jones PhDShohei Koide PhDStephen Kron MD, PhDBruce Lahn PhDDeborah Lang PhDErnst Lengyel MD, PhDShutsung Liao PhDAnning Lin PhDHue Luu MDKay Macleod PhDCarl Maki PhDElizabeth McNally MD, PhDKathleen Millen PhDAndy Minn MD, PhDIvan Moskowitz MD, PhDMilan Mrksich PhDPiers Nash PhDMarcelo Nobrega MD, PhDMarcus Peter PhDClifton Ragsdale PhDIlaria Rebay PhDJalees Rehman MDCarrie Rinker-Schaeffer PhDBernard Roizman ScDMarsha Rosner PhDBenoit Roux PhDRavi Salgia MD, PhDJulian Solway MDTobin Sosnick PhDJohn Staley PhDWei-Jen Tang PhDAaron Turkewitz PhDJerrold Turner MD, PhDKevin White PhDChung-I Wu PhDYingming Zhao PhDUCCRC SCIENTIFIC REPORT 2009RankAssociate ProfessorProfessorAssistant ProfessorAssistant ProfessorAssociate ProfessorAssociate ProfessorAssociate ProfessorProfessorAssistant ProfessorProfessorAssistant ProfessorInstructorAssociate ProfessorAssociate ProfessorAssistant ProfessorAssociate ProfessorAssociate ProfessorProfessorAssistant ProfessorAssociate ProfessorProfessorProfessorAssistant ProfessorAssociate ProfessorAssistant ProfessorProfessorAssociate ProfessorAssistant ProfessorAssistant ProfessorProfessorAssistant ProfessorAssistant ProfessorProfessorAssociate ProfessorAssociate ProfessorAssistant ProfessorAssociate ProfessorProfessorProfessorProfessorProfessorProfessorAssociate ProfessorAssociate ProfessorProfessorAssociate ProfessorProfessorProfessorProfessorAssociate Professor* Reflects all Program membership during 2008-2009DepartmentPediatricsPediatricsMedicineRadiation and Cellular OncologyMedicineBen MayMedicineMolecular Genetics and Cell BiologySurgeryBen MaySurgeryMedicineSurgeryBen MayBen MayBiochemistry and Molecular BiologyMolecular Genetics and Cell BiologyHuman GeneticsMedicineOB/GYNBen MayBen MaySurgeryBen MayRadiation and Cellular OncologyMedicineHuman GeneticsRadiation and Cellular OncologyPediatricsChemistryBen MayHuman GeneticsBen MayNeurology, Pharmacy and PhysiologyBen MayMedicineSurgeryMolecular Genetics and Cell BiologyBen MayPediatricsMedicineMedicineBiochemistry and Molecular BiologyMolecular Genetics and Cell BiologyBen MayMolecular Genetics and Cell BiologyPathologyHuman GeneticsEcology and EvolutionBen May
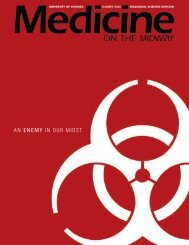
Featured Faculty Research Summaries †Investigators in the Cell Signaling and Gene Regulation Program use aglobal approach to improve the understanding of how genetic and cellsignaling alterations contribute to the pathogenesis of cancer. Researchthemes reflect the scientific goals of the Program and are highlighted below.Theme: Mechanisms of Gene RegulationMarcus Peter, PhDProfessor of The Ben May Department for Cancer ResearchCell Signaling &Gene RegulationFor 17 years, the core interest of the Peter laboratoryhas been the regulation of apoptosis signaling inhealth and disease with emphasis on the function ofthe death receptor Fas. The discovery of the deathinducing signaling complex (DISC) and the cloning ofa number of key signaling molecules in apoptosis, suchas caspase-8, c-FLIP, DEDD and DEDD2, was followedby the identification of the two signaling pathwaysof Fas that determine whether Fas induces apoptosisindependently of mitochondria or with the help ofmitochondrial amplification. About 6 years ago, theemphasis shifted towards nonapoptotic activitiesof Fas and its signaling components and their rolePersistent DNA damage foci in MCF-7 breast cancer cells 24 h after treatment within tumor progression. Fas mediated apoptosis wasionizing radiation and PARP inhibitor ABT-888, imaged by GFP-53BP1 chromatinbinding domain reporter. (Image by E. Efimova, R. Weichselbaum, and S. Kron)recognized to be just one of many activities of Fas.Stimulation of Fas on apoptosis resistant cancer cellswas shown to increase motility and invasiveness oftumor cells. These activities of Fas involve activation of the NF-kB and MAP kinase pathways. Interestingly, theseactivities were also dependent on the nature of the apoptosis signaling pathway utilized by Fas. Through thesestudies, the Peter lab became interested in the activity of micro(mi)RNAs, their role in tumor progression, and theinterplay between miRNAs and Fas functions.Current specific interests of the lab include1) the role of miR-98, also known as let-7, and miR-200 in tumorprogression; 2) the function of let-7 regulated oncofetal genes (LOGs); 3) the connection between miR-200,epithelial-mesenchymal transition (EMT) and cancer stem cells; and 4) the role of Fas and miRNAs in liver, ovarianand colon cancer.During the last year, the Peter lab has discovered two miRNAs as regulators of tumor progression. miRNAs aresmall noncoding RNAs that negatively regulate gene expression at a posttranscriptional level. The first miRNAfamily is let-7, which was found to be downregulated in tumor cells representing more advanced, less differentiatedcancers. HMGA2 was identified as a number one target for let-7. Together with Dr. Ernst Lengyel, the group wenton to demonstrate, for the first time, an inverse prognostic value of the ratio of let-7/HMGA2 expression in cancer.Ovarian cancer patients with a high ratio of let-7 to HMGA2 were found to have a much more favorable prognosisthan patients with a low ratio.The second miRNA family that was linked to cancer progression is miR-200. miR-200 was found to be a highlysignificant marker of epithelial cancer cells and almost completely absent in advanced mesenchymal cancer cells.Not only was miR-200 an excellent marker for epithelial cells, it turned out to be a powerful regulator of EMT.Altering miR-200 levels in cancer cells causes a change in the epithelial nature of the cells. Both miRNA familieshold great promise as general cancer therapeutics, since they both are dysregulated in various human cancers, andintroducing them into cancer cells may reverse tumor progression.† Note: Due to space constraints, only a small representative sample of Program members is presented here.UCCRC SCIENTIFIC REPORT 20099
Theme: Molecular Mechanisms of Apoptosis, Cell Growth, and Cell SurvivalKay Macleod, PhDAssociate Professor of The Ben May Department for Cancer ResearchAs solid tumors grow, they outstrip their ability to take upoxygen, glucose and other nutrients from the environment bydiffusion. The deficit in oxygen (hypoxia) elicits pleiotropiceffects in mammals, including increased glycolysis, angiogenesis,and erythropoiesis, all processes that maximize ATP generationand nutrient delivery, while also inhibiting processes such ascell cycle progression and protein translation that consumelarge amounts of ATP. The upregulation of glycolysis inparticular results in acidification of the microenvironment,Students and technicians working in one of the UCCRC’s dedicatedforcing adaptation to low pH such that, even when oxygen isresearch facilities, the Ellen and Melvin Gordon Center for Integrativerestored, tumor cells continue to depend on glycolysis and, inScience.some cases, are critically dependent on metabolic enzymes forsurvival. This has been referred to as the “glycolytic switch” andmay represent a novel “hallmark” of cancer that offers an opportunity to specifically target tumor cells, by blocking criticalmetabolic pathways. Another feature of tumor cells that are deprived of oxygen is the induction of autophagy, a survival processthat is activated in response to starvation. Autophagy promotes turnover of cellular constituents to re-generate metabolites andATP. Counter-intuitively, given its role in promoting cell survival, autophagy has been proposed to act as a tumor suppressormechanism via its role in limiting damaging reactive oxygen species by promoting turnover of mitochondria, preventing DNAdamage by maintaining nucleotide pools, and limiting necrosis and associated pro-tumorigenic inflammatory responses.Importantly, autophagy also induces cell cycle arrest, although the mechanism is not known.Work in the Macleod laboratory is focused on understanding the molecular basis by which hypoxia, oxidative stress andautophagy modulate tumor progression and metastasis. In recent years, the laboratory has focused on how cell survival ismodulated in response to hypoxia and nutrient deprivation, and showed for the first time that hypoxic cells induce autophagyto promote survival and that this process is dependent on aspects of the function of BNIP3 and BNIP3L, both HIF-inducibletarget genes. The molecular mechanism by which BNIP3 and BNIP3L promote autophagy is a key focus of on-going work in thelaboratory. Hypotheses being tested include a role in directly targeting mitochondria for degradation at the autophagosome toan indirect role in autophagy through effects on mitochondrial fission. Translational work has identified loss of BNIP3 activityas a potential biomarker for the progression of human breast cancer to invasiveness. Using mouse models of breast cancer toassess this and other aspects of autophagy in tumor suppression, the laboratory discovered that some tissues express BNIP3constitutively (such as the heart, skeletal muscle and liver). Phenotypic analysis of BNip3 null mice has highlighted a role forBNip3 in mitochondrial integrity in normal adult hepatocytes and also a novel function for BNip3 in fatty acid metabolismin response to starvation. Continued analysis of the phenotype in these mice is aimed at explaining these observations at themolecular level.The Macleod laboratory is also examining a role for autophagy in modulating outgrowth of disseminated tumor cells. Thepresence of tumor cells in the blood and bone marrow of women presenting with early stage breast cancer, as well as circulatingtumor cells in a significant number of women decades after their initial diagnosis and treatment, indicates that tumor cellscan disseminate early but remain dormant for long periods of time. The mechanisms governing tumor cell dormancy in breastcancer are not understood, but the Macleod group proposes that single cell dormancy brought about by cell cycle arrest may beexplained by the induction of autophagy as the tumor cell finds itself in an inhospitable environment to which it is not evolvedfor growth. The laboratory is exploring the mechanisms by which autophagy induces cell cycle arrest and further validating thiswork in mouse models. Finally, bringing together elements of tumor biology and metabolism, the laboratory is investigatingthe role of autophagy, mitochondrial integrity and metabolism in genetic prediposition to specific cancer types in humanpopulations.10UCCRC SCIENTIFIC REPORT 2009
Marsha Rosner, PhDProfessor of The Ben May Department for Cancer ResearchThe Rosner laboratory focuses on the mechanism by which signals are transmitted within the cell to specify particularoutputs leading to cell growth, differentiation or death. Dr. Rosner’s long-time focus has been on the regulation of the MAPkinase signaling cascade, an evolutionarily conserved kinase pathway that has been implicated in tumor cell progression,invasion and metastasis. Recent work from the laboratory has elucidated novel signaling cascades that regulate tumorcell cycle progression and metastasis via mechanisms involving microRNAs. One aspect of Dr. Rosner’s work involvescharacterizing the mechanism by which Raf Kinase Inhibitory Protein (RKIP), functions as a suppressor of breast cancermetastasis.Cell Signaling &Gene RegulationTumor metastasis suppressors are inhibitors of metastatic progression and colonization and, as such, represent importantmarkers for prognosis and potential effectors of therapeutic treatment. However, the mechanisms by which metastasissuppressors function are generally not understood. RKIP has been implicated as a suppressor of lung metastasis in a murinemodel using androgen-independent prostate tumor cells. A modulator of key regulatory pathways in mammalian cells, RKIPinhibits MAP kinase (MAPK) signaling by binding to Raf-1, preventing Raf-1 phosphorylation at activating sites. RKIP alsosuppresses NFkB activation, inhibits GRK2-mediated downregulation of G protein-coupled receptors, and potentiates theefficacy of chemotherapeutic agents. The Rosner laboratory has recently shown that RKIP ensures chromosomal integrityand genomic stability by preventing MAPK inhibition of Aurora B kinase and the spindle checkpoint. RKIP is missing ordepleted in a number of cancers including prostate, breast, melanoma, hepatocellular, and colorectal, suggesting that it mayfunction as a general metastasis suppressor for solid tumors. The Rosner laboratory has analyzed gene expression data fromprimary human breast tumors and determined that the RKIP signaling pathway is a prognostic marker for metastasis-freesurvival of breast cancer patients.Dr. Rosner’s recent studies have shown that RKIP suppresses invasion and metastasis by inhibiting the MAP kinase (MAPK)signaling pathway and inducing the microRNA let-7. MicroRNAs are noncoding RNAs of ~22 nucleotides that regulate keyprocesses in growth and development and have been implicated as tumor oncogenes or suppressors in cancer. Let-7/miR-98is an evolutionarily conserved microRNA family that has been implicated as a tumor suppressor of colon and lung cancer, andlet-7 loss is associated with breast tumors as well as other less differentiated human cancer cells. Let-7 has also been shownto suppress breast cancer stem cell properties (self-replication and pluripotent differentiation to multiple cell types) as well asproliferation and breast tumor growth. Thus the microRNA let-7 is an important link between regulation of metastasis andregulation of embryonic and cancer stem cells.Although let-7 has been implicated as a suppressor of breast cancer metastasis, few of its downstream signaling targets areknown. To determine which potential let-7 targets regulate metastatic progression upon loss of RKIP expression, The Rosnerlaboratory, in collaboration with Dr. Andy Minn, developed a new strategy based on gene set analysis of gene expressiondata from >1200 human breast tumors. The goal was to negatively correlate expression of putative let-7 targets with RKIPexpression. A similar approach was used to identify bone metastasis signature (BMS) genes that might be regulated by RKIP.The Rosner laboratory identified a novel RKIP/let-7-regulated signaling cascade, involving transcription factors that regulatekey BMS genes, and enabled the use of this cascade in predicting metastatic risk in patients. Dr. Rosner hopes to test thesepredictions in the clinic to determine their prognostic and therapeutic potential for both identifying patients most likely tosuffer metastatic disease as well as to identify the most effective treatments.UCCRC SCIENTIFIC REPORT 200911
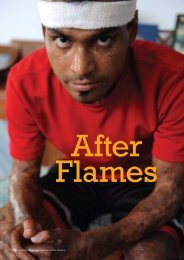
Theme: Cell Motility, Cell-Cell Adhesion, and MetastasisAndy Minn, MD, PhDAssistant Professor of Radiation and Cellular OncologyMetastasis is responsible for the vast majority ofbreast cancer-related deaths. At present, the bestway to cure breast cancer is to remove the diseaseprior to metastasis. Occasionally, surgery and localradiation are not sufficient to cure the disease becauseof the microscopic spread of cancer to other organs.In this situation, chemotherapy is administeredafter surgery, but with limited success because asignificant proportion of women with such diseasemanifests chemotherapy resistance and go on todevelop clinically significant metastatic disease(stage IV) months or years later. Thus, the window ofopportunity to cure breast cancer rapidly closes oncethe disease spreads. Attempts to re-open this windowhave been unsuccessful, leading to the prevailingwisdom that metastasis is incurable.A spontaneous intestinal tumor from Apc Min/+ mice stained with anti-beta-cateninantibody (green) and Hoechst dye (blue) to label the nuclei. In the normal intestinalmucosa (to the right of the image), beta-catenin is localized to the basolateralsurface of the epithelial cells where it mediates cell-cell interactions via the adherensjunction. In these tumors with loss of heterozygosity of the Apc tumor suppressor,beta-catenin accumulates in the cytoplasm and nuclei of the tumor cells (center ofimage) and regulates the transcription of tumor-associated target genes.(Image by K. Goss)For breast cancer, classical progression modelsshare the theme that genes controlling metastasisand resistance are stochastically acquired throughmutation. These models dictate that metastatic potential and resistance are cell-intrinsic and passed between cells, tumors,and disease sites, which has given rise to a common perception that cancer is uncontrollable once distant spread has occurred.In contrast to this reasoning, Dr. Minn’s laboratory hypothesizes the existence of metastases that are biologically limited incolonization, spread, and virulence and, therefore, represent what is called an oligometastatic state. His team envisions thatoligometastases are more likely to be sensitive to therapy due to a mechanistic coupling between genes that drive metastasis andthose that drive treatment resistance. The aims of Dr. Minn’s research are to characterize and mechanistically define genes andpathways that both mark and mediate metastasis and its resistance to treatment.Previous work in the laboratory identified a Lung Metastasis Gene Signature (LMS) that experimentally mediates and clinicallypredicts aggressive metastasis. Although the LMS accounts for a significant percentage of metastases among breast cancerpatients that develop distant relapse, the majority of patients with LMS-expressing primary cancers do not metastasize. Thissuggests an additional level of regulation and complexity that may occur subsequent to successful distant colonization.To understand mechanisms of treatment resistance better, Dr. Minn’s laboratory is collaborating with Dr. Ralph Weichselbaum(Clinical and Experimental Therapeutics Program) to study a gene expression signature for DNA damage resistance, denotedthe Interferon-Related DNA Damage Resistance Signature, or IRDS. Several key IRDS genes mediate experimental resistanceto chemotherapy and radiation, and their known involvement in interferon responses suggest unanticipated but interestingbiology. The team has recently shown that the IRDS is expressed in half of primary human cancers of various types and mayaccount for the majority of breast cancer patients with resistance to chemotherapy and radiation.By focusing on the LMS and IRDS as two biologically and clinically relevant models for metastasis and treatment resistance, amajor research goal of Dr. Minn’s laboratory is to explore the mechanistic underpinnings of why progression toward metastasisoften goes hand-in-hand with progression toward treatment resistance. Consistent with this notion, the majority of LMSexpressingprimary breast cancers also express the IRDS. Interestingly, the laboratory has discovered that tumor stroma maybe critically involved in these processes. Efforts that leverage a systems biology approach to understand important heterotypic12UCCRC SCIENTIFIC REPORT 2009
interactions, paracrine factors, and intracellular signaling events that govern the biology of the each signature are currentlyunderway. Ultimately, an important goal is to determine whether early detection of metastasis, similar to early detectionof primary cancer, can result in a biologically-definable period whereby immature tumor-microenvironmental interactionslimit metastatic colonization, spread, and resistance to therapy. If so, a subset of patients with metastasis may be amenable toaggressive and perhaps curative treatment.Carrie Rinker-Schaeffer, PhDAssociate Professor of SurgeryCell Signaling &Gene RegulationCancer metastasis is a complex, dynamic process that begins with dissemination of cells from the primary tumor andculminates in the formation of clinically detectable, overt metastases at one or more discontinuous secondary sites. Theprocess of invasion has been well studied, but the last steps in metastasis, metastatic colonization, remain largely unknown.Identifying pathways that control metastatic colonization may be critical for successful clinical management of cancerin both the metastatic and adjuvant settings. While genetic mutations or epigenetic changes may be required for cells toseparate and survive distant from the primary tumor, the environment within secondary tissues plays a substantial role indetermining whether disseminated cells survive and proliferate. Work in the Rinker-Schaeffer laboratory is focused on acritical unanswered question: Why do the majority of disseminated cells, which should be fully malignant, fail to proliferateimmediately at secondary sites, and how do these cells initiate growth and cause lethal disease? Over the past decade, thelaboratory has created unique model systems and developed biochemical tools to address this question mechanistically.This work is laying the foundation for the translational goal of identifying targets for inhibiting metastatic colonization andprolonging disease-free and overall survival.There is considerable interest in controlling the growth of cancer cells at metastatic sites. Therapeutic leads may be discernedby determining why disseminated cancer cells, which have molecular alterations that alter their growth properties, oftenlodge at target organs and persist as undetectable, or dormant disease. Many laboratories have worked on this question interms of angiogenesis, roles of oncogenes in conferring growth potential, or aspects of dormancy. The models used in thesestudies, however, did not enable the investigators to mechanistically interrogate effects on proliferation vs. apoptosis vs.quiescence in vivo. The Rinker-Schaeffer team chose to approach this problem from a different angle and use the unique toolsthey have developed over the past decade. The laboratory discovered that the stress-signaling kinase JNKK1/MKK4 cancontrol an early step in metastatic colonization and extended symptom-free survival in preclinical models of prostate andovarian cancers. Recent studies from the group support the hypothesis that activated JNKK1/MKK4 impairs proliferationof cells early in the course of metastatic colonization. It is remarkable that few, if any, studies have been conducted thatspecifically examine growth control of cells during metastatic colonization.The more intriguing question is how these cells ultimately bypass suppression and form overt metastases. Historically,fundamental tenets of metastasis biology dictate that acquisition of metastatic ability is the result of the “drive” of malignantcells towards growth. Thus it was predicted that bypass of suppression is simply the result of mutation-selection cycleswhich permanently inactivate JNKK1/MKK4 or members of its signaling cascade. Published data from the Rinker-Schaefferlaboratory challenge this paradigm and suggest that JNKK1-mediated suppression may be due to a reversible cell cycle arrestconcomitant with changes in JNKK1/MKK4 activation status. An exciting opportunity now exists to re-examine importantbut scattered literature on population-dependent behaviors of metastatic cells which have heretofore been refractory tomechanistic study. Understanding how a population of suppressed cells can adapt to its environment and initiate growthis critical to the development of adjuvant therapies that can be used in conjunction with local therapy to delay the onset ofmetastases. Ongoing studies are aimed at understanding how activated JNKK1/MKK4 regulates proliferation of disseminatedcells and the global mechanism(s) by which suppressed cells ultimately bypass suppression.UCCRC SCIENTIFIC REPORT 200913
Theme: Systems Biology and Genetic Evolution Relevant to CancerKevin White, PhDProfessor of Human GeneticsDr. White’s laboratory uses a combination of genomics, computational, and genetic approaches to investigate large-scalenetworks of factors that control gene expression during development and disease. A major challenge in the “genomic era” ofbiology is to assemble the thousands of genes and proteins encoded within each genome into comprehensive subsets that specifyparticular developmental events or physiological processes. The laboratory is approaching this challenge using Drosophilamelanogaster as a model and in the human genome directly.A recent Science publication confirms the laboratory’s successful strategy of using genomics and systems-level analysis of modelorganisms to identify factors that play crucial roles in human cancer. In this study, Dr. White’s team constructed a large-scalefunctional network model in D. melanogaster built around two key transcription factors involved in the process of embryonicsegmentation. Analysis of the model allowed the identification of a new role for the ubiquitin E3 ligase complex factor SPOP. InDrosophila, the gene encoding SPOP is a target of segmentation transcription factors. Drosophila SPOP mediates degradationof the Jun kinase phosphatase Puckered, thereby inducing tumor necrosis factor (TNF)/Eiger-dependent apoptosis. In humans,the laboratory found that SPOP plays a conserved role in TNF-mediated JNK signaling and is highly expressed in 99% of clearcell renal cell carcinomas (RCCs). SPOP expression distinguished histological subtypes of RCC and facilitated identificationof clear cell RCC as the primary tumor for metastatic lesions, indicating that SPOP is a highly sensitive and specific diagnosticbiomarker.The development of personalized genomic treatments for human cancers is the long-term goal of Dr. White’s laboratory. Aprogram was recently launched, called “The 100 Chicago Cancer Transcriptomes (100 CCT),” with the aim of sequencingentire expressed genome from human cancer samples. A unique aspect of the 100CCT project is that genomic researcherswork closely with physicians who routinely treat patients. The goal is to accelerate the translation of genomic discoveries intouseful diagnostic tools and therapeutic strategies. The laboratory employs the “next generation” sequencing Solexa platform toproduce “paired end” sequences in order to completely re-sequence transcript populations in a variety of human cancers, suchas t-AML, breast, prostate, ovarian, brain, head and neck, and lung carcinomas. For example, the laboratory is collaboratingwith Dr. Funmi Olopade (Cancer Risk and Prevention Program) to conduct a comprehensive transcriptome profiling of breastcancer subtypes in African-American and European American populations. The aims of this research are to 1) performmolecular characterization of the mutational and gene expression landscape in basal-like and luminal breast carcinomas; and2) conduct bioinformatic analysis to identify mutations and gene fusion candidates specific for these subtypes and uniqueto African Americans and Europeans. Using an advanced bioinformatic approach developed in his laboratory, Dr. White’steam recently discovered a new fusion gene in breast cancer cells that they are further screening to determine whether it is arecurring abnormality.Dr. White’s laboratory also studies the mechanism of Retinoic acid (RA) action in breast cancer prevention and treatment.To define the genetic network regulated by retinoic acid receptors (RARs), Dr. White’s team recently identified RAR genomictargets, using chromatin immunoprecipitation and expression analysis, and found that RAR binding throughout the genomeis highly co-incident with estrogen receptor α (ERα) binding, resulting in a widespread crosstalk of RA and estrogen signalingto antagonistically regulate breast cancer-associated genes. ERα and RAR binding sites appear to be co-evolved on a large scalethroughout the human genome, often resulting in competitive binding activity at nearby or overlapping cis-regulatory elements.The highly coordinated intersection between these critical nuclear hormone receptor signaling pathways provide a globalmechanism for balancing gene expression output via local regulatory interactions dispersed throughout the genome.14UCCRC SCIENTIFIC REPORT 2009
Suzanne Conzen, MDAssociate Professor of MedicineThe overall goal of the Conzen laboratory is to identify genetic and molecular mechanisms of mammalian stress signalingthat contribute to both normal human physiology and disease. It has been long hypothesized from epidemiological andclinical studies that a biological connection between human stress physiology and disease susceptibility exists, but themechanisms connecting these complex processes are poorly understood at the molecular genetics level. Glucocorticoids,a major hormone mediator of the stress response, provide an excellent model for studying a fundamental component ofstress circuitry. In 2000, the Conzen laboratory identified glucocorticoid receptor (GR)-initiated signaling as a novelsignaling mechanism that inhibits epithelial cell apoptosis in response to stress. Previously, glucocorticoid signaling hadbeen predominantly associated with inducing lymphocyte death (i.e., anti-inflammatory signaling) and with homeostaticenergy adjustment. Using systems analysis of GR-mediated gene expression and analysis of GR-regulated transcription factorbinding regions, the group’s observations have revealed novel pathways connecting the physiological stress response (GRactivation) with mechanisms of epithelial cell survival.Cell Signaling &Gene RegulationCurrently, the Conzen laboratory is using a variety of experimental approaches, including systems and traditional molecularbiology applied to both cell culture and mouse models, to uncover fundamental pathways of glucocorticoid-mediated cellsignaling that are relevant to human epithelial cell cancers. To understand the overall gene expression network downstreamof GR signaling in both pre-malignant breast epithelial and breast cancer cells, the Conzen group has performed time-courseglobal gene expression analyses following GR activation and identified at least two major pathways that regulate GR-mediatedgene expression and cell survival in these cells. Interestingly, these pathways link glucocorticoid signaling to modulation ofboth the PI3-K and MAPK signaling pathways.Secondly, with Drs. Diane Yamada and Gini Fleming (Clinical and Experimental Therpauetics Program), the laboratoryhas demonstrated that two key GR target genes [serum and glucocorticoid-inducible kinase1 (SGK1) and MAP kinasephosphatase-1 (MKP1)] are indeed upregulated in human ovarian epithelium following the administration of syntheticglucocorticoids to patients. Thirdly, the laboratory performed GR chromatin immunoprecipitation-Chip (ChIP-chip) inbreast epithelial cells exposed to physiological stress concentrations of glucocorticoid and, in collaboration with Dr. AnnaDi Rienzo (Cancer Risk and Prevention Program), identified glucocorticoid-dependent GR binding regions in the regulatoryregions of GR target genes with a strong signature of selective pressure and population-specific genetic variation. Suchvariation in GR target gene regulatory regions could lead to a better understanding of differences in individual responses toboth environmental stressors and pharmacological glucocorticoid administration.Finally, the laboratory, in collaboration with Dr. Martha McClintock (Cancer Risk and Prevention Program), is usingestablished mouse models of breast cancer in a transdisciplinary study to determine how chronic social stress (e.g., socialisolation) affects behavior, hormonal axes, and mammary cancer susceptibility. A component of this study is to analyze timecourse gene expression in the mammary glands using pathway analysis tools. Comparison of gene networks from mammaryglands of young female mice subjected to chronic social isolation from weaning (versus group living) has revealed significantdifferences in inflammatory and metabolic pathways. Unexpectedly, these mammary gland gene expression differences occurmost prominently in the mammary glands prior to the development of invasive mammary gland carcinomas. Together withstudies performed at the cellular and tissue levels, these pathways may identify novel targets for breast cancer prevention.UCCRC SCIENTIFIC REPORT 200915
Theme: Developmental BiologyIlaria Rebay, PhDAssociate Professor of The Ben May Department for Cancer ResearchThe long-term goal of the Rebay laboratory is tounderstand how cells generate, integrate, and respondto dynamic informational cues. To address this broadquestion, the laboratory uses Drosophila, and inparticular the fly eye, as a powerful model system inwhich to study cross-talk between signal transductionpathways and tissue specific transcriptional networks.Because the signaling mechanisms studied have beenhighly conserved in evolution, investigation of themolecular circuitries used in Drosophila can advancethe understanding of how cell fates are designated andmaintained in all animals, and why misregulation resultsin cancer and disease in humans. Current researchfocuses on elucidating the function and regulation oftwo independent but interconnected nuclear circuitriesoperating downstream of the receptor tyrosine kinase(RTK) pathway.Protein uptake in Tetrahymena thermophilia, a ciliated protozoan, via labelingwith a GFP-tagged protein. (Image by A. Turkewitz)First, the Rebay laboratory is studying the function andregulation of Yan, a conserved ETS family transcriptionalrepressor and RTK pathway antagonist. Reflecting critical roles in regulating cell proliferation, differentiation, and survivalduring normal development, misregulated ETS protein activity contributes via a variety of mechanisms to the initiation andprogression of many human cancers. For example, translocations involving the human counterpart of Drosophila Yan, referredto as Tel1, are among the most frequent chromosomal aberrations associated with leukemia. Both Tel1 and Yan self-associatevia an N-terminal protein-protein interaction domain called the Sterile Alpha Motif (SAM). In vitro, the isolated SAM canform homooligomers, leading to the hypothesis that polymerization might contribute to the mechanism of Tel1/Yan-mediatedtranscriptional repression. Intriguingly, in-frame fusions of the Tel1 SAM to an assortment of tyrosine kinases and transcriptionfactors are detected in the above mentioned leukemic translocations, suggesting that SAM-mediated self-association alsocontributes to oncogenesis. Thus, the specific aim of this project is to elucidate how SAM-mediated self-association regulatesnormal Tel1/Yan-mediated repression of transcriptional target genes during development. In the long-term, this knowledge mayfacilitate the design of specific molecular interventions to block the oncogenic properties of Tel1-SAM leukemic fusion proteins.The goal of the laboratory’s second project is to investigate the molecular mechanisms whereby a group of evolutionarilyconserved transcription factors, collectively termed the Retinal Determination (RD) gene network, interface with multiplesignaling pathways to direct eye specification and development. The research centers on a gene called Eyes absent (Eya),which the laboratory identified as a node of cross-talk between the RD network and the Epidermal Growth Factor RTKsignaling pathway. The Rebay group discovered that in addition to its role as a transcription factor, Eya functions as a proteintyrosine phosphatase. Both functions are required for Drosophila eye development, and perturbation of either activity leads todevelopmental abnormalities in mammals. RD genes, either individually or as a network, also regulate proliferation and cell fatespecification in a diverse array of developmental contexts in all metazoans, and consequently both increased expression andloss of gene function results in developmental perturbation and disease. For example, reduced Eya function results in ear, eye,kidney, heart and cranial-facial defects, whereas upregulation of Eya proteins appears to correlate with poor clinical outcome inpatients with epithelial ovarian cancer. Thus, a primary aim of this work is to elucidate the specific developmental contexts andsignaling pathways in which Eya participates, and how its dual functions are coordinated and coregulated.16UCCRC SCIENTIFIC REPORT 2009
Most recently, the laboratory discovered that subcellular partitioning of Eya protein between nucleus and cytoplasm iscritical for normal eye development and that phosphatase function is predominantly required in the cytosol. Cooperativeinteractions between Eya and the Abelson (Abl) tyrosine kinase were found to be critical for photoreceptor axon guidance inthe Drosophila visual system, and that mechanistically, Abl-mediated phosphorylation of Eya provides a critical cytoplasmicretention signal that presumably recruits Eya phosphatase activity to relevant signaling complexes. Abl is well-known as apotent oncogene, and its normal role in regulating actin cytoskeleton dynamics suggests that further investigation of Eya-Ablinteractions may provide new insight into the signaling networks regulating cell adhesion, motility, and invasiveness.Cell Signaling &Gene RegulationGeoffrey Greene, PhDProfessor of The Ben May Department for Cancer ResearchThe overall goal of research in Dr. Greene’s laboratory is to elucidate the molecular mechanisms by which female steroidhormones regulate development, differentiation, cellular proliferation and survival in hormone responsive tissues andcancers, especially breast cancer. Estrogens modulate the expression of diverse regulatory proteins and growth factors viaone or both of two estrogen receptor subtypes (ERα and ERβ). The Greene laboratory is actively studying multiple aspects ofER action, using a combination of in vitro, cell-based, and animal models.Current areas of focus include: 1) Defining the molecular/structural mechanisms by which selective estrogen receptormodulators (SERMs) elicit tissue-selective agonist or antagonist responses via one or both ER subtypes; 2) identifying novelER subtype-selective SERMs via a combination of structure-based drug design and de novo drug discovery; 3) characterizinga mouse knock-in model in which a mutated ERα does not recognize endogenous estrogens, but will respond to exogenoussynthetic ligands; 4) identifying the relative contributions and mechanisms of transcriptional versus rapid, nongenomic ERαactions in estrogen target tissues; 5) developing targeted nanoparticles for imaging and therapeutic applications, especiallyin breast/prostate cancers; 6) genome-wide mapping and characterization of ERα/β target genes (ER transcriptome); and 7)identification and characterization of protein components of the ER interactome. All of these projects have direct relevanceand application to breast and uterine cancer genesis, progression, treatment and prevention, as well as to the development ofcompounds that can be used for hormone replacement therapy in postmenopausal women.The laboratory recently generated an estrogen non-responsive estrogen receptor knock-in (ENERKI) mouse model to studythe role of ERα during endocrine and neuroendocrine development and mammary tumor genesis. The mutant ERα (G525L)that was introduced by gene replacement into these mice does not recognize endogenous estrogen but does recognizeexogenous synthetic estrogen agonists and antagonists, such as diethylstilbestrol (DES), propyl pyrazole triol (PPT) and4-hydroxytamoxifen (OHT). Mutant ERα can be turned on or off simply by giving mice DES or PPT, both potent estrogens.ERα signaling pathways that do not require ligand remain intact, allowing them to study these pathways as well. FemaleENERKI mice had hypoplastic uterine tissues and rudimentary mammary gland ductal trees. Females were infertile due toanovulation, and their ovaries contained hemorrhagic cystic follicles because of chronically elevated levels of LH.The ENERKI phenotype confirmed that ligand-induced activation of ERα is crucial in the female reproductive tract andmammary gland development. Growth factor treatments induced uterine epithelial proliferation in ovariectomized ENERKIfemales, directly demonstrating that ERα ligand-independent pathways were active. PPT treatments initiated at pubertystimulated ENERKI uterine development, whereas neonatal treatments were needed to restore mammary gland ductalelongation, indicating that neonatal ligand-induced ERα activation may prime mammary ducts to become more responsive toestrogens in adult tissues. This mouse is a useful model for in vivo evaluation of ligand-induced ERα pathways and temporalpatterns of response. Interestingly, DES did not stimulate an ENERKI uterotrophic response, possibly due to the upregulationof ERβ in ENERKI mice, which is exerting an antiproliferative function in the uterus. It remains to be determinedif the mammary gland is similarly affected by DES treatment. ENERKI mice will be crossed with several mouse modelsthat develop spontaneous mammary tumors to better understand the role of endogenous estrogen and ERα in mammarycancer genesis and progression. This model should also prove useful for studying the estrogen-mediated development andhomoeostasis of the reproductive tract, bone, cardiovasculature and central nervous system.UCCRC SCIENTIFIC REPORT 200917
Additional Program Highlights*Research•• The initial steps of ovarian cancer cell metastasis are mediated byMMP-2 cleavage of vitronectin and fibronectin. Ernst Lengyel, MD,PhD is searching for new methods to control the metastatic spreadof ovarian cancer. Since one of the first steps in the spread of thiscancer is the attachment of ovarian cancer cells to the peritoneal andomental surfaces, identifying factors that regulate cell attachment inthe abdominal cavity is critical to the development of therapeutic agentsthat prevent metastases. Dr. Lengyel and his colleagues discovered thatMMP-2 expression affects the metastatic spread of ovarian cancer cellsin a three dimensional tumor/stromal co-culture model. These findingscould help us to not only determine how to control cancer, but also howto inhibit its ability to spread to other organs (Kenny et al. J Clin Invest118:1367-1379, 2008).••Dr. Ravi SalgiaThe miR-200 Family Determines the Epithelial Phenotype ofCancer Cells by Targeting the E-Cadherin Repressors ZEB1 and ZEB2(intraprogrammatic). In a collaborative project, Marcus Peter, PhD and Dr. Lengyel examined whether cancer progressionshares similar processes with those that occur during embryonic development. The team evaluated the expression of 207microRNAs (miRNA) in the 60 cell lines of the drug screening panel maintained by the National Cancer Institute. Theydiscovered and confirmed, in primary ovarian cancer specimens, that the miR-200 miRNA family is a powerful markerfor grouping of primary cancers, consequently showing that a single key master regulating gene can control cell phenotype(Park et al. Genes Dev 22:894-907, 2008).••NFkappaB Selectivity of Estrogen Receptor Ligands is Revealed by Comparative Crystallographic Analyses. GeoffreyGreene, PhD and his colleagues showed that protein folding problems that are common to steroid hormone receptors arecircumvented by mutations that stabilize well-characterized conformations of the receptor. The approach used in this studypresents the structure of an unliganded steroid receptor, which reveals a ligand-accessible channel that allows the soaking ofpre-formed crystals. The ability to crystallize many receptor-ligand complexes with distinct pharmacophores helps to definestructural features of signaling specificity that would not be apparent in a single structure. This research exemplifies how thework of Program 1 members continues to push the boundaries of understanding activation of transcription factors that arehighly relevant to cancer (Nettles et al. Nat Chem Biol 4:241-247, 2008).18UCCRC SCIENTIFIC REPORT 2009* Due to space constraints, only a small representative sample of Program highlights is presented here.
Selected New Funding•• The National Cancer Institute awarded Ravi Salgia, MD, PhD and his colleagues an R01 grant to determine the role ofpaxillin in non-small cell lung cancer (NSCLC), which will help uncover novel mechanisms for transformation, metastasisand, ultimately, therapy for lung cancer.•• Andy Minn, MD, PhD and his colleagues are the recipients of the Department of Defense Era of Hope Scholar Award tostudy how induction of the interferon-related gene signatures for DNA damage resistance by stroma increases treatmentresistance, and how the stroma regulates the lung metastasis signature genes and other metastasis genes.Cell Signaling &Gene Regulation••••Kevin White, PhD is the primary investigator in a program project (P50) funded by the National Institutes of Health tocreate a Center for Systems Biology in an initiative to promote interdisciplinary scientific investigation and educationin Chicago. The focus of this Center’s program is on developing a robust transcriptional network in physiological,developmental, and evolutionary time scales. The goal is being achieved through collaborations among experts ingenomics, developmental biology, evolutionary biology, stress and physiology, network modeling, high performance andgrid computing, chemistry, and physics.Shohei Koide, PhD has been awarded R21 funding from the National Institutes of Health/National Institute for DrugAbuse to develop an innovative and powerful technology platform for facile production of high-performance reagents.This new technology will help to fill a major void in current epigenetic research, making it feasible to establish a standardset of epigenetic capture reagents that can be widely be disseminated to the medical community.New Faculty Recruitments and UCCRC MembersRex Haydon, MD, PhD specializes in the surgical care of bone and soft tissue tumors and aims to understand the underlyingcauses of musculoskeletal neoplasms in order to develop novel and innovative treatments. Dr. Haydon focuses his researchon signaling pathways involved in sarcoma development and on the elucidation of blocks to differentiation that occur inosteosarcoma.Yu-Ying He, PhD’s research interests are in the molecular mechanisms of skin carcinogenesis induced by the environmentand the development of chemopreventive and therapeutic strategies to reduce the skin cancer burden. Dr. He’s currentresearch projects focus on understanding the fundamental mechanisms of cell proliferation, survival, transformation, andinflammation in the skin caused by ultraviolet radiation and other factors.Kathleen Goss, PhD is leading a research program that is aimed at understanding the APC/beta-catenin pathway indevelopment and tumorigenesis in order to facilitate the design of novel therapeutic approaches to target this pathway incancer.Ivan Moskowitz, MD, PhD studies the molecular basis of cardiac morphogenesis and Congenital Heart Disease. Dr.Moskowitz aims to identify and understand the genes involved in cardiac morphogenesis using forward and reverse geneticapproaches in mouse models. Recent work has focused on early aspects of cardiac valve development.Jalees Rehman, MD conducts cardiovascular research on the biology of regenerative stem and progenitor cells. His researchfocuses on cancer stem cell differentiation and cell signaling. Dr. Rehman is also interested in determining the differencesin cell death and metabolism between mature and regenerative cells, and aims to understand how regenerative celltransplantation can improve cardiovascular function in patients.Yingming Zhao, PhD’s research aims to develop mass spectrometry and bioinformatic tools to understand the function ofpost-translational modification (PTM) pathways which play critical roles in disease development. Dr. Zhao combines theuse of proteomic technologies with biochemical and molecular techniques to understand PTM networks further beyond thatprovided by conventional techniques.UCCRC SCIENTIFIC REPORT 200919
Selected Publications* : Intraprogrammatic Collaboration# : Interprogrammatic CollaborationAlexander, Kenneth MD, PhDIshibashi KL, Koopmans J, Curlin FA, Alexander KA, Ross LF. Paediatricians’attitudes and practices towards HPV vaccination. Acta Paediatr 97(11):1550-6,2008.Ishibashi KL, Koopmans J, Curlin FA, Alexander KA, Ross LF. Pediatricians aremore supportive of the human papillomavirus vaccine than the general public.South Med J 101(12):1216-21, 2008.Beyer, Eric MD, PhDKyle JW, Minogue PJ, Thomas BC, Domowicz DA, Berthoud VM, Hanck DA,Beyer EC. An intact connexin N-terminus is required for function but not gapjunction formation. J Cell Sci 121(Pt 16):2744-50, 2008.Lichtenstein A, Gaietta GM, Deerinck TJ, Crum J, Sosinsky GE, Beyer EC,Berthoud VM. The cytoplasmic accumulations of the cataract-associatedmutant, Connexin50P88S, are long-lived and form in the endoplasmicreticulum. Exp Eye Res 88(3):600-9, 2009.Luca F, Kashyap S, Southard C, Zou M, Witonsky D, Di Rienzo A, ConzenSD. Adaptive variation regulates the expression of the human SGK1 gene inresponse to stress. PLoS Genet 5(5):e1000489, 2009.Du, Wei PhDDeb DK, Tanaka-Matakatsu M, Jones L, Richardson HE, Du W. Winglesssignaling directly regulates cyclin E expression in proliferating embryonic PNSprecursor cells. Mech Dev 125(9-10):857-64, 2008.* # Luo X, Wang CZ, Chen J, Song WX, Luo J, Tang N, He BC, Kang Q, WangY, Du W, He TC, Yuan CS. Characterization of gene expression regulated byAmerican ginseng and ginsenoside Rg3 in human colorectal cancer cells. Int JOncol 32(5):975-83, 2008.Sukhanova MJ, Du W. Control of cell cycle entry and exiting from the secondmitotic wave in the Drosophila developing eye. BMC Dev Biol 8:7, 2008.* # Wang CZ, Aung HH, Zhang B, Sun S, Li XL, He H, Xie JT, He TC, Du W,Yuan CS. Chemopreventive effects of heat-processed Panax quinquefolius rooton human breast cancer cells. Anticancer Res 28(5A):2545-51, 2008.* # Wang CZ, Xie JT, Fishbein A, Aung HH, He H, Mehendale SR, He TC,Du W, Yuan CS. Antiproliferative effects of different plant parts of Panaxnotoginseng on SW480 human colorectal cancer cells. Phytother Res 23(1):6-13, 2009.Tanaka-Matakatsu M, Xu J, Cheng L, Du W. Regulation of apoptosis of rbfmutant cells during Drosophila development. Dev Biol 326(2):347-56, 2009.Chmura, Steven MD, PhD# Salama JK, Chmura SJ, Mehta N, Yenice KM, Stadler WM, Vokes EE, HarafDJ, Hellman S, Weichselbaum RR. An initial report of a radiation doseescalationtrial in patients with one to five sites of metastatic disease. ClinCancer Res 14(16):5255-9, 2008.# Al-Hallaq HA, Mell LK, Bradley JA, Chen LF, Ali AN, Weichselbaum RR,Newstead GM, Chmura SJ. Magnetic resonance imaging identifies multifocaland multicentric disease in breast cancer patients who are eligible for partialbreast irradiation. Cancer 113(9):2408-14, 2008.# Mell LK, Schomas DA, Salama JK, Devisetty K, Aydogan B, Miller RC, JaniAB, Kindler HL, Mundt AJ, Roeske JC, Chmura SJ. Association between bonemarrow dosimetric parameters and acute hematologic toxicity in anal cancerpatients treated with concurrent chemotherapy and intensity-modulatedradiotherapy. Int J Radiat Oncol Biol Phys 70(5):1431-7, 2008.# Cao J, Roeske JC, Chmura SJ, Salama JK, Shoushtari AN, Boyer AL, MartelMK. Calculation and prediction of the effect of respiratory motion on wholebreast radiation therapy dose distributions. Med Dosim 34(2):126-32, 2009.# Altman MB, Vesper BJ, Smith BD, Stinauer MA, Pelizzari CA, Aydogan B,Reft CS, Radosevich JA, Chmura SJ, Roeske JC. Characterization of a novelphantom for three-dimensional in vitro cell experiments. Phys Med Biol54(5):N75-82, 2009.Conzen, Suzanne MD# Jansen SA, Conzen SD, Fan X, Krausz T, Zamora M, Foxley S, River J,Newstead GM, Karczmar GS. Detection of in situ mammary cancer in atransgenic mouse model: in vitro and in vivo MRI studies demonstratehistopathologic correlation. Phys Med Biol 53(19):5481-93, 2008.Belova L, Brickley DR, Ky B, Sharma SK, Conzen SD. Hsp90 regulates thephosphorylation and activity of serum- and glucocorticoid-regulated kinase-1. JBiol Chem 283(27):18821-31, 2008.# Belova L, Delgado B, Kocherginsky M, Melhem A, Olopade OI, ConzenSD. Glucocorticoid receptor expression in breast cancer associates with olderpatient age. Breast Cancer Res Treat 116(3):441-7, 2009.Conzen SD. Minireview: nuclear receptors and breast cancer. Mol Endocrinol22(10):2215-28, 2008.Pew T, Zou M, Brickley DR, Conzen SD. Glucocorticoid (GC)-mediated downregulationof urokinase plasminogen activator expression via the serum andGC regulated kinase-1/forkhead box O3a pathway. Endocrinology 149(5):2637-45, 2008.# Melhem A, Yamada SD, Fleming GF, Delgado B, Brickley DR, Wu W,Kocherginsky M, Conzen SD. Administration of Glucocorticoids to OvarianCancer Patients Is Associated with Expression of the Anti-apoptotic GenesSGK1 and MKP1/DUSP1 in Ovarian Tissues. Clin Cancer Res 15(9):3196-204,2009.Dulin, Nickolai PhD# Yau DM, Sethakorn N, Taurin S, Kregel S, Sandbo N, Camoretti-MercadoB, Sperling AI, Dulin NO. Regulation of Smad-mediated gene transcription byRGS3. Mol Pharmacol 73(5):1356-61, 2008.Kwon IK, Schoenlein PV, Delk J, Liu K, Thangaraju M, Dulin NO, GanapathyV, Berger FG, Browning DD. Expression of cyclic guanosine monophosphatedependentprotein kinase in metastatic colon carcinoma cells blocks tumorangiogenesis. Cancer 112(7):1462-70, 2008.Sandbo N, Kregel S, Taurin S, Bhorade S, Dulin NO. Critical Role of SerumResponse Factor in Pulmonary Myofibroblast Differentiation Induced byTGF-β. Am J Respir Cell Mol Biol, 2009.Ferguson, Edwin PhDYu H, Seah A, Herman MA, Ferguson EL, Horvitz HR, Sternberg PW. Wnt andEGF pathways act together to induce C. elegans male hook development. DevBiol 327(2):419-32, 2009.Goss, Kathleen PhDProsperi JR, Becher KR, Willson TA, Collins MH, Witte DP, Goss KH. The APCtumor suppressor is required for epithelial integrity in the mouse mammarygland. J Cell Physiol 220(2):319-31, 2009.Greene, Geoffrey PhDLeong H, Mathur PS, Greene GL. Green tea catechins inhibit angiogenesisthrough suppression of STAT3 activation. Breast Cancer Res Treat, 2008.O’Neill EE, Blewett AR, Loria PM, Greene GL. Modulation of alphaCaMKIIsignaling by rapid ERalpha action. Brain Res 1222:1-17, 2008.Nettles KW, Bruning JB, Gil G, Nowak J, Sharma SK, Hahm JB, Kulp K,Hochberg RB, Zhou H, Katzenellenbogen JA, Katzenellenbogen BS, Kim Y,Joachmiak A, Greene GL. NFkappaB selectivity of estrogen receptor ligandsrevealed by comparative crystallographic analyses. Nat Chem Biol 4(4):241-7,2008.Sinkevicius KW, Burdette JE, Woloszyn K, Hewitt SC, Hamilton K, Sugg SL,Temple KA, Wondisford FE, Korach KS, Woodruff TK, Greene GL. An estrogenreceptor-alpha knock-in mutation provides evidence of ligand-independentsignaling and allows modulation of ligand-induced pathways in vivo.Endocrinology 149(6):2970-9, 2008.Nettles KW, Gil G, Nowak J, Metivier R, Sharma VB, Greene GL. CBP Is adosage-dependent regulator of nuclear factor-kappaB suppression by theestrogen receptor. Mol Endocrinol 22(2):263-72, 2008.Sinkevicius KW, Laine M, Lotan TL, Woloszyn K, Richburg JH, Greene GL.Estrogen-dependent and -independent estrogen receptor-alpha signalingseparately regulate male fertility. Endocrinology 150(6):2898-905, 2009.20UCCRC SCIENTIFIC REPORT 2009
Haiman CA, Garcia RR, Hsu C, Xia L, Ha H, Sheng X, Le Marchand L,Kolonel LN, Henderson BE, Stallcup MR, Greene GL, Press MF. Screening andassociation testing of common coding variation in steroid hormone receptorco-activator and co-repressor genes in relation to breast cancer risk: theMultiethnic Cohort. BMC Cancer 9:43, 2009.Haydon, Rex MD, PhD* Su Y, Luo X, He BC, Wang Y, Chen L, Zuo GW, Liu B, Bi Y, Huang J, ZhuGH, He Y, Kang Q, Luo J, Shen J, Chen J, Jin X, Haydon RC, He TC, LuuHH. Establishment and characterization of a new highly metastatic humanosteosarcoma cell line. Clin Exp Metastasis, 2009.He, Tong-Chuan MD, PhD* # Luo X, Wang CZ, Chen J, Song WX, Luo J, Tang N, He BC, Kang Q, WangY, Du W, He TC, Yuan CS. Characterization of gene expression regulated byAmerican ginseng and ginsenoside Rg3 in human colorectal cancer cells. Int JOncol 32(5):975-83, 2008.* # Sharff KA, Song WX, Luo X, Tang N, Luo J, Chen J, Bi Y, He BC, HuangJ, Li X, Jiang W, Zhu GH, Su Y, He Y, Shen J, Wang Y, Chen L, Zuo GW, LiuB, Pan X, Reid RR, Luu HH, Haydon RC, He TC. Hey1 basic helix-loop-helix(bHLH) protein plays an important role in mediating BMP9 induced osteogenicdifferentiation of mesenchymal progenitor cells. J Biol Chem 284(1):649-59,2009.* # Luo X, Chen J, Song WX, Tang N, Luo J, Deng ZL, Sharff KA, He G, Bi Y,He BC, Bennett E, Huang J, Kang Q, Jiang W, Su Y, Zhu GH, Yin H, He Y, WangY, Souris JS, Chen L, Zuo GW, Montag AG, Reid RR, Haydon RC, Luu HH, HeTC. Osteogenic BMPs promote tumor growth of human osteosarcomas thatharbor differentiation defects. Lab Invest 88(12):1264-77, 2008.* Luo X, Sharff KA, Chen J, He TC, Luu HH. S100A6 expression and functionin human osteosarcoma. Clin Orthop Relat Res 466(9):2060-70, 2008.He YY, Council SE, Feng L, Chignell CF. UVA-induced cell cycle progressionis mediated by a disintegrin and metalloprotease/epidermal growth factorreceptor/AKT/Cyclin D1 pathways in keratinocytes. Cancer Res 68(10):3752-8,2008.Ming M, He YY. PTEN: New Insights into Its Regulation and Function in SkinCancer. J Invest Dermatol, 2009.* Su Y, Luo X, He BC, Wang Y, Chen L, Zuo GW, Liu B, Bi Y, Huang J, ZhuGH, He Y, Kang Q, Luo J, Shen J, Chen J, Jin X, Haydon RC, He TC, LuuHH. Establishment and characterization of a new highly metastatic humanosteosarcoma cell line. Clin Exp Metastasis, 2009.* Kang Q, Song WX, Luo Q, Tang N, Luo J, Luo X, Chen J, Bi Y, He BC, ParkJK, Jiang W, Tang Y, Huang J, Su Y, Zhu GH, He Y, Yin H, Hu Z, Wang Y, ChenL, Zuo GW, Pan X, Shen J, Vokes T, Reid RR, Haydon RC, Luu HH, He TC. AComprehensive Analysis of the Dual Roles of BMPs in Regulating Adipogenicand Osteogenic Differentiation of Mesenchymal Progenitor Cells. Stem CellsDev 18(4):545-59, 2009.Imamoto, Akira PhD* Zeng L, Imamoto A, Rosner MR. Raf kinase inhibitory protein (RKIP): aphysiological regulator and future therapeutic target. Expert Opin Ther Targets12(10):1275-87, 2008.Seo JH, Suenaga A, Hatakeyama M, Taiji M, Imamoto A. Structural andfunctional basis of a role for CRKL in a fibroblast growth factor 8-induced feedforwardloop. Mol Cell Biol 29(11):3076-87, 2009.Jones, Richard PhDChuu CP, Chen RY, Barkinge JL, Ciaccio MF, Jones RB. Systems-level analysisof ErbB4 signaling in breast cancer: a laboratory to clinical perspective. MolCancer Res 6(6):885-91, 2008.Koide, Shohei PhDDutta S, Koide A, Koide S. High-throughput analysis of the protein sequencestabilitylandscape using a quantitative yeast surface two-hybrid system andfragment reconstitution. J Mol Biol 382(3):721-33, 2008.Gilbreth RN, Esaki K, Koide A, Sidhu SS, Koide S. A dominant conformationalrole for amino acid diversity in minimalist protein-protein interfaces. J MolBiol 381(2):407-18, 2008.Ye JD, Tereshko V, Frederiksen JK, Koide A, Fellouse FA, Sidhu SS,Koide S, Kossiakoff AA, Piccirilli JA. Synthetic antibodies for specificrecognition and crystallization of structured RNA. Proc Natl Acad Sci US A 105(1):82-7, 2008.Huang J, Koide A, Makabe K, Koide S. Design of protein function leapsby directed domain interface evolution. Proc Natl Acad Sci U S A105(18):6578-83, 2008.Tereshko V, Uysal S, Koide A, Margalef K, Koide S, Kossiakoff AA.Toward chaperone-assisted crystallography: protein engineeringenhancement of crystal packing and X-ray phasing capabilities of acamelid single-domain antibody (VHH) scaffold. Protein Sci 17(7):1175-87, 2008.* Granovsky AE, Clark MC, McElheny D, Heil G, Hong J, Liu X,Kim Y, Joachimiak G, Joachimiak A, Koide S, Rosner MR. Raf kinaseinhibitory protein function is regulated via a flexible pocket and novelphosphorylation-dependent mechanism. Mol Cell Biol 29(5):1306-20,2009.Uysal S, Vasquez V, Tereshko V, Esaki K, Fellouse FA, Sidhu SS, Koide S,Perozo E, Kossiakoff A. Crystal structure of full-length KcsA in its closedconformation. Proc Natl Acad Sci U S A 106(16):6644-9, 2009.Kron, Stephen MD, PhDUlanovskaya OA, Janjic J, Suzuki M, Sabharwal SS, Schumacker PT, KronSJ, Kozmin SA. Synthesis enables identification of the cellular target ofleucascandrolide A and neopeltolide. Nat Chem Biol 4(7):418-24, 2008.Kristjansdottir K, Wolfgeher D, Lucius N, Angulo DS, Kron SJ.Phosphoprotein profiling by PA-GeLC-MS/MS. J Proteome Res 7(7):2812-24, 2008.Wu D, Mand MR, Veach DR, Parker LL, Clarkson B, Kron SJ. A solidphaseBcr-Abl kinase assay in 96-well hydrogel plates. Anal Biochem375(1):18-26, 2008.# Bickenbach KA, Veerapong J, Shao MY, Mauceri HJ, Posner MC, KronSJ, Weichselbaum RR. Resveratrol is an effective inducer of CArG-drivenTNF-alpha gene therapy. Cancer Gene Ther 15(3):133-9, 2008.Parker L, Engel-Hall A, Drew K, Steinhardt G, Helseth DL Jr, JabonD, McMurry T, Angulo DS, Kron SJ. Investigating quantitation ofphosphorylation using MALDI-TOF mass spectrometry. J Mass Spectrom43(4):518-27, 2008.Volchenboum SL, Kristjansdottir K, Wolfgeher D, Kron SJ. Rapidvalidation of Mascot search results via stable isotope labeling, pairpicking, and deconvolution of fragmentation patterns. Mol CellProteomics 8(8):2011-22, 2009.Lahn, Bruce PhDPeng Y, Chen Z, Yu W, Zhou Q, Xu L, Mao FF, Huang G, Zhang X, Li S,Lahn BT, Xiang AP. Effects of thymic polypeptides on the thymopoiesisof mouse embryonic stem cells. Cell Biol Int 32(10):1265-1271, 2008.Wang P, Liu XM, Liu XM, Ma BF, Jia L, Wang D, Zhang XM, Yu XB, LahnBT, Xiang AP. Isolation, characterization and gene modification of fetalneural stem/progenitor cells from cynomolgus monkey. Neuroreport19(4):419-24, 2008.Yu W, Chen Z, Zhang J, Zhang L, Ke H, Huang L, Peng Y, Zhang X, Li S,Lahn BT, Xiang AP. Critical role of phosphoinositide 3-kinase cascadein adipogenesis of human mesenchymal stem cells. Mol Cell Biochem310(1-2):11-8, 2008.Xiang AP, Mao FF, Li WQ, Park D, Ma BF, Wang T, Vallender TW,Vallender EJ, Zhang L, Lee J, Waters JA, Zhang XM, Yu XB, Li SN, LahnBT. Extensive contribution of embryonic stem cells to the development ofan evolutionarily divergent host. Hum Mol Genet 17(1):27-37, 2008.Yang XH, Wu QL, Yu XB, Xu CX, Ma BF, Zhang XM, Li SN, Lahn BT,Xiang AP. Nestin expression in different tumours and its relevance tomalignant grade. J Clin Pathol 61(4):467-73, 2008.Lee JH, Gaetz J, Bugarija B, Fernandes CJ, Snyder GE, Bush EC, Lahn BT.Chromatin analysis of occluded genes. Hum Mol Genet 18(14):2567-74,2009.Lang, Deborah PhDPlummer RS, Shea CR, Nelson M, Powell SK, Freeman DM, Dan CP,Lang D. PAX3 expression in primary melanomas and nevi. Mod Pathol21(5):525-30, 2008.Cell Signaling &Gene RegulationUCCRC SCIENTIFIC REPORT 200921
Lang D, Mascarenhas JB, Powell SK, Halegoua J, Nelson M, Ruggeri BA. PAX6is expressed in pancreatic adenocarcinoma and is downregulated duringinduction of terminal differentiation. Mol Carcinog 47(2):148-56, 2008.* # Kanteti R, Nallasura V, Loganathan S, Tretiakova M, Kroll T,Krishnaswamy S, Faoro L, Cagle P, Husain AN, Vokes EE, Lang D, Salgia R.PAX5 is expressed in small-cell lung cancer and positively regulates c-Mettranscription. Lab Invest 89(3):301-14, 2009.Kubic JD, Young KP, Plummer RS, Ludvik AE, Lang D. Pigmentation PAX-ways:the role of Pax3 in melanogenesis, melanocyte stem cell maintenance, anddisease. Pigment Cell Melanoma Res 21(6):627-45, 2008.Lengyel, Ernst MD, PhD# Onujiogu N, Lengyel E, Yamada SD. Reversible posteriorleukoencephalopathy syndrome following intravenous paclitaxel andintraperitoneal cisplatin chemotherapy for fallopian tube cancer. GynecolOncol 111(3):537-9, 2008.* # Sawada K, Mitra AK, Radjabi AR, Bhaskar V, Kistner EO, Tretiakova M,Jagadeeswaran S, Montag A, Becker A, Kenny HA, Peter ME, Ramakrishnan V,Yamada SD, Lengyel E. Loss of E-cadherin promotes ovarian cancer metastasisvia alpha 5-integrin, which is a therapeutic target. Cancer Res 68(7):2329-39,2008.* Park SM, Gaur AB, Lengyel E, Peter ME. The miR-200 family determinesthe epithelial phenotype of cancer cells by targeting the E-cadherin repressorsZEB1 and ZEB2. Genes Dev 22(7):894-907, 2008.Terplan M, Temkin S, Tergas A, Lengyel E. Does equal treatment yield equaloutcomes? The impact of race on survival in epithelial ovarian cancer. GynecolOncol 111(2):173-8, 2008.Kenny HA, Kaur S, Coussens LM, Lengyel E. The initial steps of ovarian cancercell metastasis are mediated by MMP-2 cleavage of vitronectin and fibronectin.J Clin Invest 118(4):1367-79, 2008.# Radjabi AR, Sawada K, Jagadeeswaran S, Eichbichler A, Kenny HA, MontagA, Bruno K, Lengyel E. Thrombin induces tumor invasion through theinduction and association of matrix metalloproteinase-9 and beta1-integrin onthe cell surface. J Biol Chem 283(5):2822-34, 2008.Kenny HA, Lengyel E. MMP-2 functions as an early response protein in ovariancancer metastasis. Cell Cycle 8(5):683-8, 2009.Liao, Shutsung PhDChuu CP, Chen RY, Kokontis JM, Hiipakka RA, Liao S. Suppression ofandrogen receptor signaling and prostate specific antigen expression by(-)-epigallocatechin-3-gallate in different progression stages of LNCaP prostatecancer cells. Cancer Lett 275(1):86-92, 2009.Peng D, Hiipakka RA, Dai Q, Guo J, Reardon CA, Getz GS, Liao S.Antiatherosclerotic effects of a novel synthetic tissue-selective steroidalliver X receptor agonist in low-density lipoprotein receptor-deficient mice. JPharmacol Exp Ther 327(2):332-42, 2008.Peng D, Hiipakka RA, Reardon CA, Getz GS, Liao S. Differential antiatheroscleroticeffects in the innominate artery and aortic sinus by the liver Xreceptor agonist T0901317. Atherosclerosis 203(1):59-66, 2009.Lin, Anning PhD# Depaolo RW, Tang F, Kim I, Han M, Levin N, Ciletti N, Lin A, Anderson D,Schneewind O, Jabri B. Toll-like receptor 6 drives differentiation of tolerogenicdendritic cells and contributes to LcrV-mediated plague pathogenesis. CellHost Microbe 4(4):350-61, 2008.Deng H, Yu F, Chen J, Zhao Y, Xiang J, Lin A. Phosphorylation of Bad at Thr-201by JNK1 promotes glycolysis through activation of phosphofructokinase-1. JBiol Chem 283(30):20754-60, 2008.Luu, Hue MD* # Sharff KA, Song WX, Luo X, Tang N, Luo J, Chen J, Bi Y, He BC, HuangJ, Li X, Jiang W, Zhu GH, Su Y, He Y, Shen J, Wang Y, Chen L, Zuo GW, LiuB, Pan X, Reid RR, Luu HH, Haydon RC, He TC. Hey1 basic helix-loop-helix(bHLH) protein plays an important role in mediating BMP9 induced osteogenicdifferentiation of mesenchymal progenitor cells. J Biol Chem 284(1):649-59,2009.* # Luo X, Chen J, Song WX, Tang N, Luo J, Deng ZL, Sharff KA, He G, Bi Y,He BC, Bennett E, Huang J, Kang Q, Jiang W, Su Y, Zhu GH, Yin H, He Y, WangY, Souris JS, Chen L, Zuo GW, Montag AG, Reid RR, Haydon RC, Luu HH, HeTC. Osteogenic BMPs promote tumor growth of human osteosarcomas thatharbor differentiation defects. Lab Invest 88(12):1264-77, 2008.* Luo X, Sharff KA, Chen J, He TC, Luu HH. S100A6 expression and functionin human osteosarcoma. Clin Orthop Relat Res 466(9):2060-70, 2008.# Deng ZL, Sharff KA, Tang N, Song WX, Luo J, Luo X, Chen J, Bennett E, ReidR, Manning D, Xue A, Montag AG, Luu HH, Haydon RC, He TC. Regulation ofosteogenic differentiation during skeletal development. Front Biosci 13:2001-21,2008.* Su Y, Luo X, He BC, Wang Y, Chen L, Zuo GW, Liu B, Bi Y, Huang J, ZhuGH, He Y, Kang Q, Luo J, Shen J, Chen J, Jin X, Haydon RC, He TC, LuuHH. Establishment and characterization of a new highly metastatic humanosteosarcoma cell line. Clin Exp Metastasis, 2009.* Kang Q, Song WX, Luo Q, Tang N, Luo J, Luo X, Chen J, Bi Y, He BC, ParkJK, Jiang W, Tang Y, Huang J, Su Y, Zhu GH, He Y, Yin H, Hu Z, Wang Y, ChenL, Zuo GW, Pan X, Shen J, Vokes T, Reid RR, Haydon RC, Luu HH, He TC. AComprehensive Analysis of the Dual Roles of BMPs in Regulating Adipogenicand Osteogenic Differentiation of Mesenchymal Progenitor Cells. Stem CellsDev 18(4):545-59, 2009.Macleod, Kay PhD* # Lotan T, Hickson J, Souris J, Huo D, Taylor J, Li T, Otto K, Yamada SD,Macleod K, Rinker-Schaeffer CW. c-Jun NH2-terminal kinase activating kinase1/mitogen-activated protein kinase kinase 4-mediated inhibition of SKOV3ip.1ovarian cancer metastasis involves growth arrest and p21 up-regulation. CancerRes 68(7):2166-75, 2008.* # Taylor JL, Szmulewitz RZ, Lotan T, Hickson J, Griend DV, Yamada SD,Macleod K, Rinker-Schaeffer CW. New paradigms for the function of JNKK1/MKK4 in controlling growth of disseminated cancer cells. Cancer Lett272(1):12-22, 2008.Macleod KF. The role of the RB tumour suppressor pathway in oxidative stressresponses in the haematopoietic system. Nat Rev Cancer 8(10):769-81, 2008.Klionsky DJ, Abeliovich H, Agostinis P, Agrawal DK, Aliev G, Askew DS,Baba M, Baehrecke EH, Bahr BA, Ballabio A, Bamber BA, Bassham DC,Bergamini E, Bi X, Biard-Piechaczyk M, Blum JS, Bredesen DE, Brodsky JL,Brumell JH, Brunk UT, Bursch W, Camougrand N,. Guidelines for the useand interpretation of assays for monitoring autophagy in higher eukaryotes.Autophagy 4(2):151-75, 2008.Huiping Liu, James R. Knabb, Benjamin T. Spike, Macleod K, Elevated Parpsensitizes Rb deficient cells to DNA damage-induced necrosis. Mol. Cancer Res7(7):1099-109, 2009.Maki, Carl PhDMoran DM, Gawlak G, Jayaprakash MS, Mayar S, Maki CG. Geldanamycinpromotes premature mitotic entry and micronucleation in irradiated p53/p21deficient colon carcinoma cells. Oncogene, 2008.Shen H, Moran DM, Maki CG. Transient nutlin-3a treatment promotesendoreduplication and the generation of therapy-resistant tetraploid cells.Cancer Res 68(20):8260-8, 2008.Moran DM, Shen H, Maki CG. Puromycin-based vectors promote a ROSdependentrecruitment of PML to nuclear inclusions enriched with HSP70 andProteasomes. BMC Cell Biol 10:32, 2009.McNally, Elizabeth MD, PhDDoherty KR, Demonbreun AR, Wallace GQ, Cave A, Posey AD, Heretis K, PytelP, McNally EM. The endocytic recycling protein EHD2 interacts with myoferlinto regulate myoblast fusion. J Biol Chem 283(29):20252-60, 2008.Millen, Kathleen PhDMillen KJ, Gleeson JG. Cerebellar development and disease. Curr OpinNeurobiol 18(1):12-9, 2008.22UCCRC SCIENTIFIC REPORT 2009
Minn, Andy MD, PhD* # Weichselbaum RR, Ishwaran H, Yoon T, Nuyten DS, Baker SW, KhodarevN, Su AW, Shaikh AY, Roach P, Kreike B, Roizman B, Bergh J, Pawitan Y, vande Vijver MJ, Minn AJ. An interferon-related gene signature for DNA damageresistance is a predictive marker for chemotherapy and radiation for breastcancer. Proc Natl Acad Sci U S A 105(47):18490-5, 2008.Bos PD, Zhang XH, Nadal C, Shu W, Gomis RR, Nguyen DX, Minn AJ, vande Vijver MJ, Gerald WL, Foekens JA, Massague J. Genes that mediate breastcancer metastasis to the brain. Nature 459(7249):1005-9, 2009.Serganova I, Moroz E, Vider J, Gogiberidze G, Moroz M, Pillarsetty N,Doubrovin M, Minn A, Thaler HT, Massague J, Gelovani J, Blasberg R.Multimodality imaging of TGFβ signaling in breast cancer metastases. FASEB J23(8):2662-72, 2009.* Dangi-Garimella S, Yun J, Eves EM, Newman M, Erkeland SJ, Hammond SM,Minn AJ, Rosner MR. Raf kinase inhibitory protein suppresses a metastasissignalling cascade involving LIN28 and let-7. EMBO J 28(4):347-58, 2009.Mrksich, Milan PhDGurard-Levin ZA, Mrksich M. The activity of HDAC8 depends on local anddistal sequences of its peptide substrates. Biochemistry 47(23):6242-50, 2008.James J, Goluch ED, Hu H, Liu C, Mrksich M. Subcellular curvature at theperimeter of micropatterned cells influences lamellipodial distribution and cellpolarity. Cell Motil Cytoskeleton 65(11):841-52, 2008.Mrksich M. Using self-assembled monolayers to model the extracellularmatrix. Acta Biomater 5(3):832-41, 2009.Peter, Marcus PhD* # Sawada K, Mitra AK, Radjabi AR, Bhaskar V, Kistner EO, Tretiakova M,Jagadeeswaran S, Montag A, Becker A, Kenny HA, Peter ME, Ramakrishnan V,Yamada SD, Lengyel E. Loss of E-cadherin promotes ovarian cancer metastasisvia alpha 5-integrin, which is a therapeutic target. Cancer Res 68(7):2329-39,2008.* Park SM, Gaur AB, Lengyel E, Peter ME. The miR-200 family determinesthe epithelial phenotype of cancer cells by targeting the E-cadherin repressorsZEB1 and ZEB2. Genes Dev 22(7):894-907, 2008.# Park SM, Rajapaksha TW, Zhang M, Sattar HA, Fichera A, Ashton-RickardtPG, Peter ME. CD95 signaling deficient mice with a wild-type hematopoieticsystem are prone to hepatic neoplasia. Apoptosis 13(1):41-51, 2008.Feig C, Peter ME. Methods to analyze the palmitoylated CD95 high molecularweight death-inducing signaling complex. Methods Enzymol 442:83-100, 2008.Boyerinas B, Park SM, Shomron N, Hedegaard MM, Vinther J, Andersen JS,Feig C, Xu J, Burge CB, Peter ME. Identification of let-7-regulated oncofetalgenes. Cancer Res 68(8):2587-91, 2008.Schickel R, Boyerinas B, Park SM, Peter ME. MicroRNAs: key players in theimmune system, differentiation, tumorigenesis and cell death. Oncogene27(45):5959-74, 2008.Peter ME. Let-7 and miR-200 microRNAs: guardians against pluripotency andcancer progression. Cell Cycle 8(6):843-52, 2009.Ragsdale, Clifton PhDGan L, Olson JL, Ragsdale CW, Yu L. Poly(beta-aminosulfonamides) as genedelivery vectors: synthesis and in vitro screening. Chem Commun (Camb)(5):573-5, 2008.Rinker-Schaeffer, Carrie PhD* # Lotan T, Hickson J, Souris J, Huo D, Taylor J, Li T, Otto K, YamadaSD, Macleod K, Rinker-Schaeffer CW. c-Jun NH2-terminal kinaseactivating kinase 1/mitogen-activated protein kinase kinase 4-mediatedinhibition of SKOV3ip.1 ovarian cancer metastasis involves growth arrestand p21 up-regulation. Cancer Res 68(7):2166-75, 2008.* # Taylor JL, Szmulewitz RZ, Lotan T, Hickson J, Griend DV, YamadaSD, Macleod K, Rinker-Schaeffer CW. New paradigms for the functionof JNKK1/MKK4 in controlling growth of disseminated cancer cells.Cancer Lett 272(1):12-22, 2008.Hickson J, Diane Yamada S, Berger J, Alverdy J, O’Keefe J, Bassler B,Rinker-Schaeffer C. Societal interactions in ovarian cancer metastasis: aquorum-sensing hypothesis. Clin Exp Metastasis 26(1):67-76, 2009.Robinson VL, Shalhav O, Otto K, Kawai T, Gorospe M, Rinker-SchaefferCW. Mitogen-activated protein kinase kinase 4/c-Jun NH2-terminalkinase kinase 1 protein expression is subject to translational regulation inprostate cancer cell lines. Mol Cancer Res 6(3):501-8, 2008.* # Posadas EM, Al-Ahmadie H, Robinson VL, Jagadeeswaran R, OttoK, Kasza KE, Tretiakov M, Siddiqui J, Pienta KJ, Stadler WM, Rinker-Schaeffer C, Salgia R. FYN is overexpressed in human prostate cancer.BJU Int, 2008.# Taylor J, Hickson J, Lotan T, Yamada DS, Rinker-Schaeffer C. Usingmetastasis suppressor proteins to dissect interactions among cancer cellsand their microenvironment. Cancer Metastasis Rev 27(1):67-73.Roizman, Bernard ScD* # Weichselbaum RR, Ishwaran H, Yoon T, Nuyten DS, Baker SW,Khodarev N, Su AW, Shaikh AY, Roach P, Kreike B, Roizman B,Bergh J, Pawitan Y, van de Vijver MJ, Minn AJ. An interferon-relatedgene signature for DNA damage resistance is a predictive marker forchemotherapy and radiation for breast cancer. Proc Natl Acad Sci U S A105(47):18490-5, 2008.Gu H, Roizman B. The two functions of HSV-1 ICP0 - the inhibition ofsilencing by the CoREST/REST/HDAC complex and degradation of PML- are executed in tandem. J Virol 83(1):181-7, 2009.Durand LO, Roizman B. Role of cdk9 in the optimization of expressionof the genes regulated by ICP22 of herpes simplex virus 1. J Virol82(21):10591-9 Epub, 2008.Liang L, Roizman B. Expression of gamma interferon-dependent genes isblocked independently by virion host shutoff RNase and by US3 proteinkinase. J Virol 82(10):4688-96, 2008.Smith-Donald BA, Roizman B. The interaction of herpes simplex virus 1regulatory protein ICP22 with the cdc25C phosphatase is enabled in vitroby viral protein kinases US3 and UL13. J Virol 82(9):4533-43, 2008.Jovasevic V, Liang L, Roizman B. Proteolytic cleavage of VP1-2 is requiredfor release of herpes simplex virus 1 DNA into the nucleus. J Virol82(7):3311-9, 2008.Kalamvoki M, Qu J, Roizman B. Translocation and colocalization of ICP4and ICP0 in cells infected with herpes simplex virus 1 mutants lackingglycoprotein E, glycoprotein I, or the virion host shutoff product of theUL41 gene. J Virol 82(4):1701-13, 2008.Yang K, Poon AP, Roizman B, Baines JD. Temperature-sensitivemutations in the putative herpes simplex virus type 1 terminasesubunits pUL15 and pUL33 preclude viral DNA cleavage/packagingand interaction with pUL28 at the nonpermissive temperature. J Virol82(1):487-94, 2008.Cell Signaling &Gene RegulationRebay, Ilaria PhDXiong W, Dabbouseh NM, Rebay I. Interactions with the abelson tyrosinekinase reveal compartmentalization of eyes absent function between nucleusand cytoplasm. Dev Cell 16(2):271-9, 2009.Rehman, Jalees MDZhang Y, Herbert BS, Rajashekhar G, Ingram DA, Yoder MC, Clauss M,Rehman J. Premature senescence of highly proliferative endothelial progenitorcells is induced by tumor necrosis factor-alpha via the p38 mitogen-activatedprotein kinase pathway. FASEB J 23(5):1358-65, 2009.Zhang Y, Ingram DA, Murphy MP, Saadatzadeh MR, Mead LE, PraterDN, Rehman J. Release of proinflammatory mediators and expression ofproinflammatory adhesion molecules by endothelial progenitor cells. Am JPhysiol Heart Circ Physiol 296(5):H1675-82, 2009.Rosner, Marsha PhD* Zeng L, Imamoto A, Rosner MR. Raf kinase inhibitory protein (RKIP):a physiological regulator and future therapeutic target. Expert Opin TherTargets 12(10):1275-87, 2008.* Yfanti C, Mengele K, Gkazepis A, Weirich G, Giersig C, Kuo WL,Tang WJ, Rosner M, Schmitt M. Expression of metalloprotease insulindegradingenzyme insulysin in normal and malignant human tissues. IntJ Mol Med 22(4):421-31, 2008.* Weirich G, Mengele K, Yfanti C, Gkazepis A, Hellmann D,Welk A, Giersig C, Kuo WL, Rosner MR, Tang WJ, Schmitt M.Immunohistochemical evidence for ubiquitous distribution of themetalloendoprotease insulin-degrading enzyme (IDE, insulysin)in human non-malignant tissues and tumor cell lines. Biol Chem389(11):1441-5, 2008.UCCRC SCIENTIFIC REPORT 200923
Granovsky AE, Rosner MR. Raf kinase inhibitory protein: a signal transductionmodulator and metastasis suppressor. Cell Res 18(4):452-7, 2008.# Cohen EE, Zhu H, Lingen MW, Martin LE, Kuo WL, Choi EA, KocherginskyM, Parker JS, Chung CH, Rosner MR. A feed-forward loop involving proteinkinase Calpha and microRNAs regulates tumor cell cycle. Cancer Res 69(1):65-74, 2009.* Granovsky AE, Clark MC, McElheny D, Heil G, Hong J, Liu X, Kim Y,Joachimiak G, Joachimiak A, Koide S, Rosner MR. Raf kinase inhibitory proteinfunction is regulated via a flexible pocket and novel phosphorylation-dependentmechanism. Mol Cell Biol 29(5):1306-20, 2009.* Dangi-Garimella S, Yun J, Eves EM, Newman M, Erkeland SJ, Hammond SM,Minn AJ, Rosner MR. Raf kinase inhibitory protein suppresses a metastasissignalling cascade involving LIN28 and let-7. EMBO J 28(4):347-58, 2009.Roux, Benoit PhDBanavali NK, Roux B. Flexibility and charge asymmetry in the activation loopof Src tyrosine kinases. Proteins 74(2):378-89, 2009.Gan W, Roux B. Binding specificity of SH2 domains: Insight from free energysimulations. Proteins 74(4):996-1007, 2009.Pan AC, Roux B. Building Markov state models along pathways to determinefree energies and rates of transitions. J Chem Phys 129(6):064107, 2008.Pan AC, Sezer D, Roux B. Finding transition pathways using the string methodwith swarms of trajectories. J Phys Chem B 112(11):3432-40, 2008.Yang S, Roux B. Src kinase conformational activation: thermodynamics,pathways, and mechanisms. PLoS Comput Biol 4(3):e1000047, 2008.Deng Y, Roux B. Computation of binding free energy with molecular dynamicsand grand canonical Monte Carlo simulations. J Chem Phys 128(11):115103,2008.Yang S, Banavali NK, Roux B. Mapping the conformational transition in Srcactivation by cumulating the information from multiple molecular dynamicstrajectories. Proc Natl Acad Sci U S A 106(10):3776-81, 2009.Deng Y, Roux B. Computations of standard binding free energies withmolecular dynamics simulations. J Phys Chem B 113(8):2234-46, 2009.Park S, Bardhan JP, Roux B, Makowski L. Simulated x-ray scattering of proteinsolutions using explicit-solvent models. J Chem Phys 130(13):134114, 2009.Freddolino PL, Park S, Roux B, Schulten K. Force field bias in protein foldingsimulations. Biophys J 96(9):3772-80, 2009.Salgia, Ravi MD, PhD# Nimeiri HS, Oza AM, Morgan RJ, Friberg G, Kasza K, Faoro L, Salgia R,Stadler WM, Vokes EE, Fleming GF. Efficacy and safety of bevacizumab pluserlotinib for patients with recurrent ovarian, primary peritoneal, and fallopiantube cancer: a trial of the Chicago, PMH, and California Phase II Consortia.Gynecol Oncol 110(1):49-55, 2008.# Jagadeeswaran R, Surawska H, Krishnaswamy S, Janamanchi V, MackinnonAC, Seiwert TY, Loganathan S, Kanteti R, Reichman T, Nallasura V, SchwartzS, Faoro L, Wang YC, Girard L, Tretiakova MS, Ahmed S, Zumba O, SouliiL, Bindokas VP, Szeto LL, Gordon GJ, Bue. Paxillin is a target for somaticmutations in lung cancer: implications for cell growth and invasion. Cancer Res68(1):132-42, 2008.Siddiqui SS, Loganathan S, Krishnaswamy S, Faoro L, Jagadeeswaran R, SalgiaR. C. elegans as a model organism for in vivo screening in cancer: effects ofhuman c-Met in lung cancer affect C. elegans vulva phenotypes. Cancer BiolTher 7(6):856-63, 2008.Sittler T, Zhou J, Park J, Yuen NK, Sarantopoulos S, Mollick J, Salgia R, Giobbie-Hurder A, Dranoff G, Hodi FS. Concerted potent humoral immune responsesto autoantigens are associated with tumor destruction and favorable clinicaloutcomes without autoimmunity. Clin Cancer Res 14(12):3896-905, 2008.# Rudin CM, Salgia R, Wang X, Hodgson LD, Masters GA, Green M, Vokes EE.Randomized phase II Study of carboplatin and etoposide with or without thebcl-2 antisense oligonucleotide oblimersen for extensive-stage small-cell lungcancer: CALGB 30103. J Clin Oncol 26(6):870-6, 2008.# Seiwert TY, Jagadeeswaran R, Faoro L, Janamanchi V, Nallasura V, El DinaliM, Yala S, Kanteti R, Cohen EE, Lingen MW, Martin L, Krishnaswamy S,Klein-Szanto A, Christensen JG, Vokes EE, Salgia R. The MET receptor tyrosinekinase is a potential novel therapeutic target for head and neck squamous cellcarcinoma. Cancer Res 69(7):3021-31, 2009.Solway, Julian MDHe D, Natarajan V, Stern R, Gorshkova IA, Solway J, Spannhake EW, Zhao Y.Lysophosphatidic acid-induced transactivation of epidermal growth factorreceptor regulates cyclo-oxygenase-2 expression and prostaglandin E(2) releasevia C/EBPbeta in human bronchial epithelial cells. Biochem J 412(1):153-62,2008.Pinto LH, Eaton E, Chen B, Fleisher J, Shuster D, McCauley J, Kedainis D,Siepka SM, Shimomura K, Song EJ, Husain A, Lakser OJ, Mitchell RW, DowellML, Brown M, Camoretti-Mercado B, Naclerio R, Sperling AI, Levin SI, TurekFW, Solway J. Gene-environment interactions in a mutant mouse kindred withnative airway constrictor hyperresponsiveness. Mamm Genome 19(1):2-14,2008.Sosnick, Tobin PhDStrickland D, Moffat K, Sosnick TR. Light-activated DNA binding in a designedallosteric protein. Proc Natl Acad Sci U S A 105(31):10709-14, 2008.Tang, Wei-Jen PhD* Yfanti C, Mengele K, Gkazepis A, Weirich G, Giersig C, Kuo WL, TangWJ, Rosner M, Schmitt M. Expression of metalloprotease insulin-degradingenzyme insulysin in normal and malignant human tissues. Int J Mol Med22(4):421-31, 2008.* Weirich G, Mengele K, Yfanti C, Gkazepis A, Hellmann D, Welk A, Giersig C,Kuo WL, Rosner MR, Tang WJ, Schmitt M. Immunohistochemical evidence forubiquitous distribution of the metalloendoprotease insulin-degrading enzyme(IDE, insulysin) in human non-malignant tissues and tumor cell lines. BiolChem 389(11):1441-5, 2008.Malito E, Ralat LA, Manolopoulou M, Tsay JL, Wadlington NL, Tang WJ.Molecular Bases for the Recognition of Short Peptide Substrates and Cysteine-Directed Modifications of Human Insulin-Degrading Enzyme. Biochemistry47(48):12822-34, 2008.Guo Q, Jureller JE, Warren JT, Solomaha E, Florian J, Tang WJ. Protein-proteindocking and analysis reveal that two homologous bacterial adenylyl cyclasetoxins interact with calmodulin differently. J Biol Chem 283(35):23836-45,2008.Taha HM, Schmidt J, Gottle M, Suryanarayana S, Shen Y, Tang WJ, Gille A,Geduhn J, Konig B, Dove S, Seifert R. Molecular Analysis of the Interactionof Anthrax Adenylyl Cyclase Toxin, Edema Factor, with 2’(3’)-O-(N-(methyl)anthraniloyl)-Substituted Purine and Pyrimidine Nucleotides. Mol Pharmacol75(3):693-703, 2009.Spangler CM, Spangler C, Gottle M, Shen Y, Tang WJ, Seifert R, Schaferling M.A fluorimetric assay for real-time monitoring of adenylyl cyclase activity basedon terbium norfloxacin. Anal Biochem. 381(1):86-93, 2008.Kim C, Wilcox-Adelman S, Sano Y, Tang WJ, Collier RJ, Park JM.Antiinflammatory cAMP signaling and cell migration genes co-opted by theanthrax bacillus. Proc Natl Acad Sci U S A 105(16):6150-5, 2008.Kuo SR, Willingham MC, Bour SH, Andreas EA, Park SK, Jackson C, DuesberyNS, Leppla SH, Tang WJ, Frankel AE. Anthrax toxin-induced shock in rats isassociated with pulmonary edema and hemorrhage. Microb Pathog 44(6):467-72, 2008.Turner, Jerrold MD, PhD# Weber CR, Nalle SC, Tretiakova M, Rubin DT, Turner JR. Claudin-1 andclaudin-2 expression is elevated in inflammatory bowel disease and maycontribute to early neoplastic transformation. Lab Invest 88(10):1110-20, 2008.Shen L, Weber CR, Turner JR. The tight junction protein complex undergoesrapid and continuous molecular remodeling at steady state. J Cell Biol181(4):683-95, 2008.Annaba F, Sarwar Z, Kumar P, Saksena S, Turner JR, Dudeja PK, Gill RK,Alrefai WA. Modulation of ileal bile acid transporter (ASBT) activity bydepletion of plasma membrane cholesterol: association with lipid rafts. Am JPhysiol Gastrointest Liver Physiol 294(2):G489-97, 2008.Gill RK, Pant N, Saksena S, Singla A, Nazir TM, Vohwinkel L, Turner JR,Goldstein J, Alrefai WA, Dudeja PK. Function, expression, and characterizationof the serotonin transporter in the native human intestine. Am J PhysiolGastrointest Liver Physiol 294(1):G254-62, 2008.24UCCRC SCIENTIFIC REPORT 2009
Yu D, Turner JR. Stimulus-induced reorganization of tight junction structure:the role of membrane traffic. Biochim Biophys Acta 1778(3):709-16, 2008.Su L, Shen L, Clayburgh DR, Nalle SC, Sullivan EA, Meddings JB, AbrahamC, Turner JR. Targeted epithelial tight junction dysfunction causesimmune activation and contributes to development of experimental colitis.Gastroenterology 136(2):551-63, 2009.White, Kevin PhD# Hua S, Kallen CB, Dhar R, Baquero MT, Mason CE, Russell BA, Shah PK, LiuJ, Khramtsov A, Tretiakova MS, Krausz TN, Olopade OI, Rimm DL, White KP.Genomic analysis of estrogen cascade reveals histone variant H2A.Z associatedwith breast cancer progression. Mol Syst Biol. 4:188, 2008.Gauhar Z, Sun LV, Hua S, Mason CE, Fuchs F, Li TR, Boutros M, White KP.Genomic mapping of binding regions for the Ecdysone receptor proteincomplex. Genome Res 19(6):1006-13, 2009.Liu J, Ghanim M, Xue L, Brown CD, Iossifov I, Angeletti C, Hua S, Negre N,Ludwig M, Stricker T, Al-Ahmadie HA, Tretiakova M, Camp RL, Perera-Alberto M, Rimm DL, Xu T, Rzhetsky A, White KP. Analysis of Drosophilasegmentation network identifies a JNK pathway factor overexpressed in kidneycancer. Science 323(5918):1218-22, 2009.Cell Signaling &Gene RegulationUCCRC SCIENTIFIC REPORT 200925
Selected Major Grants and AwardsThe Cell Signaling and Gene Regulation Program has a funding base of $40,975,090 in annual total costs (current as of July 2009).This sum includes $7,151,438 in NCI funding and $25,178,189 in other NIH funding. Due to space constraints, only new awardspresented since January 1, 2008 with funding of $100,000 or more in annual total costs are listed here.Investigator Title Start DateWhite, KevinZhao, YinmingWhite, KevinChicago Systems Biology Center forthe Study of Transcriptional NetworksSystematic Screening for New HistoneMarksCenter for Bioinformatics andComputational BiologyEndDateAnnualTotal CostClassFunding Agency9/1/2008 8/31/2013 $3,021,428 N/A National Institutes of Health9/30/2008 8/3/2011 $790,454 R01 National Institutes of Health7/1/2008 6/30/2011 $765,000 N/ARosner, Marsha Signaling Pathways in Neuronal Cells 1/10/2009 12/31/2012 $421,202 R01McNally, ElizabethRoizman, BernardRoizman, BernardMcNally, ElizabethSarcoglycan in Myopathy and MuscleMembrane StabilityThe Functions of the US3 ProteinKinase of Herpes Simplex VirusDissection of the Functions of HerpesSimplex Virus ICPONuclear Membrane ProteinInteraction in Heart and MuscleDiseaseThe Searle Funds at theChicago Community TrustNational Inst. ofNeurological Disorders andStroke12/1/2008 11/30/2013 $390,000 R01 National Institutes of Health9/10/2008 8/31/2012 $385,000 R01 National Cancer Institute5/1/2008 4/30/2013 $382,057 R37 National Cancer Institute9/1/2008 5/31/2012 $378,614 R01Lin, Anning Wiring the UV Signaling Circuitry 2/8/2008 1/31/2013 $345,375 R01Rinker-Schaeffer,CarrieProstate Cancer MetastaticColonization: Role of MKK4National Heart, Lung, andBlood InstituteNational Institute ofEnvironmental HealthScience12/1/2008 11/30/2013 $328,815 R01 National Cancer InstituteSalgia, Ravi Role of Paxillin in Lung Cancer 6/2/2008 4/30/2013 $326,831 R01 National Cancer InstituteMillen, KathleenLiao, ShutsungMrksich, MilanLang, DeborahMacleod, KayKoide, ShoheiWu, Chung-IChmura, StevenPeter, MarcusMrksich, MilanZhao, YinmingMouse Models of Human CerebellarMalformationsMolecular Mechanisms of GrowthControl in Prostate CancerUltrahigh Performance Nanoantennasfor Surface Enhanced RamanSpectroscopyPax3, Melanocyte Stem Cells andMelanomaFunctions of BNIP3 in MammaryTumorigenesisNovel Affinity Reagents for EpigeneticsMarkersMicroRNA Evolution and SpeciesDivergence in DrosophiliaA Phase 1/2, Multi-Center, Safetyand Efficacy Study EvaluatingIntravenously Administered I-TM601in Patients with Progressive and/orRecurrent Malignant GliomaNovel Fas/CD95 SignalingMechanismsPeptide Arrays for UnderstandingHistone BiochemistryGlobal Characterization of LysineAcetylation in Cancer by a ProteomicsApproach8/15/2008 7/31/2009 $324,496 R56National Inst. ofNeurological Disorders andStroke2/1/2009 1/31/2013 $315,168 R01 National Cancer Institute5/1/2008 4/30/2009 $313,001 08 Department of Defense2/1/2009 12/31/2013 $312,000 R01 National Cancer Institute2/1/2009 12/31/2013 $303,853 R01 National Institutes of Health9/20/2008 7/31/2010 $301,864 N/A7/1/2008 6/30/2011 $301,309 R01National Institute on DrugAbuseNational Institute of GeneralMedical Sciences8/25/2008 8/24/2009 $290,258 N/A Transmolecular, Inc.9/17/2008 7/31/2012 $275,709 R01 National Cancer Institute4/1/2008 2/29/2012 $270,736 R01National Institute of GeneralMedical Sciences6/1/2008 4/30/2013 $261,083 R01 National Cancer Institute26UCCRC SCIENTIFIC REPORT 2009
Investigator Title Start DateSalgia, RaviSolway, JulianZhao, YinmingGreene, GeoffreyFerguson, EdwinSalgia, RaviNash, PiersKron, StephenKoide, ShoheiSalgia, RaviSalgia, RaviLengyel, ErnstRinker-Schaeffer,CarrieBoone, DavidSolway, JulianHaydon, RexRole of c-Met in SCLC and Potentialfor Novel TherapyEvaluation of Lovastatin in SeverePersistent Asthma (ElisPA)A Novel Proteomics Technology forProtein FarnesylationStructure-Function Analysis of ERAlpha/Beta Bound to Bazedoxifene/CEMixturesCharacterization of the Interactionsbetween a Stem Cell and its Niche InDrosophillaPhase I Safety, Pharmacokinetic andPharmacodynamic Study of PF-04217903 in Patients with AdvancedCancerProtein-protein Interactions in SignalTransductionMALDI Imaging of Cancer SignalingSignaturesHigh-Performance Affinity Reagentsfor Peptide EpitopesNovel Targeted Therapy in PancreaticCancerA Phase I Followed by a Randomized,Phase II Study of Carboplatin andEtoposide With or Without ObatoclaxAdministered Every 3 Weeks toPatients with Extensive State SmallCell Lung CancerDevelopment of Novel Therapeuticand Diagnostic Strategies for OvarianCancerIdentification of Effectors of MKK4-Mediated Suppression oin OvarianCancer Metastatic ColonizationFunctional Consequences ofAutophagy Mutations in Crohn’sDiseaseThe Influence of Budesonide andFormoterol on Force Fluctuation-Induced Relengthening of ContractedAirway Smooth MuscleSynergistic Use of Oteogenic BMP’s ina New Zealand White Rabbit Model ofSpine FusionEndDateAnnualTotal CostClassFunding Agency9/19/2008 2/28/2013 $251,380 R01 National Cancer Institute9/5/2008 8/31/2009 $231,000 R34National Institute of Allergyand Infectious Diseases1/16/2009 3/31/2010 $230,949 R33 National Cancer Institute4/25/2008 4/24/2009 $230,545 N/A1/1/2008 12/31/2011 $230,250 SSWyeth-AyerstPharmaceuticalsThe Ellison MedicalFoundation7/9/2008 7/8/2010 $208,209 N/A Pfizer, Inc.9/1/2008 8/31/2009 $180,562 N/A National Science Foundation7/16/2008 6/30/2010 $172,687 R21 National Cancer Institute4/4/2008 3/31/2010 $168,065 R21 National Cancer Institute3/1/2009 2/28/2011 $156,000 R21 National Cancer Institute5/28/2008 5/27/2010 $152,694 N/AGemin X BiotechnologiesInc.7/1/2008 6/30/2013 $150,000 N/A Burroughs Wellcome Fund6/1/2008 5/31/2009 $145,433 N/A Pardee Foundation, Elsa U.12/1/2008 11/30/2009 $139,274 N/A4/28/2008 4/27/2010 $126,906 N/A Astrazeneca1/1/2009 12/31/2009 $124,496 N/AKron, Stephen Chicago Laminome Project 11/1/2008 10/31/2010 $120,000 N/AMrksich, MilanSalgia, RaviRosner, MarshaCollaborative Proposal: EMT/MISC:Behavior Based Molecular RoboticsExpression and Function of the RONReceptor Tyrosine KinaseRegulation of Breast Cancer StemCells by Raf Kinase Inhibitory ProteinBroad Foundation, The Eliand Edythe L.Musculoskeletal TransplantFoundationThe Searle Funds at theChicago Community Trust9/1/2008 8/31/2011 $105,000 N/A National Science Foundation5/22/2008 5/21/2009 $100,000 N/A Biogen Idec Inc.1/1/2009 12/31/2009 $100,000 N/A Geyer Foundation, CharlotteCell Signaling &Gene RegulationUCCRC SCIENTIFIC REPORT 200927
Program 2Molecular Genetics and HematopoiesisRUNX1/ AML1 amplification in a pediatric pre B-ALL patient detected by fluorescence in situhybridization (FISH) analysis. Using a genomic probe (green) for the TEL gene at 12p13 and agenomic probe (red) for the RUNX1/AML1 gene at 21q22, FISH analysis shows two green signals(normal chromosomes 12), one red signal (normal chromosome 21), and multiple red signalson a derivative chromosome 21, indicative of an amplification of the RUNX1/AML1 gene, in ametaphase and two interphase cells. (Image by Y. Zhang)
In recent years, insights gained related to these goals havebegun to be translated into novel molecularly-targetedtherapeutic approaches for hematological malignancies.Overview & GoalsMolecular Genetics& HematopoiesisThe Molecular Genetics and HematopoiesisProgram is comprised of a tightly-integratedgroup of 28 members from four academicdepartments who are linked by common researchthemes. Members of this program have hadmajor roles in the cytogenetic and molecularanalysis of hematological malignant diseases,which have led to the identification of manygenes that are involved in normal hematopoiesis,as well as in the pathogenesis of leukemias andlymphomas.management of patients with these diseases; and(3) promote optimal use of resources within theUniversity of Chicago Cancer Research Centerand collaborating departments. In recent years,insights gained related to these goals have begunto be translated into novel molecularly-targetedtherapeutic approaches for hematologicalmalignancies.The overall goals of the Molecular Geneticsand Hematopoiesis Program are to: (1) fosterscientific interactions among investigatorsinvolved in clinical management and biologicalstudies of hematological malignancies; (2)promote translational research and facilitatethe transfer of laboratory research to theProgram Leaders:Wendy Stock, MDMichael Thirman, MDUCCRC SCIENTIFIC REPORT 200929
MembersInvestigator*John Anastasi MDAndrew Artz MDBeverly Baron MDJianjun Chen PhDKenneth Cohen MDJohn Cunningham MDLucy Godley MD, PhDFotini Gounari PhD, DSc.Sandeep Gurbuxani MBBS, PhDBarbara Kee PhDRichard Larson MDMichelle Le Beau PhDSusana Marino MD, PhDJames Nachman MDOlatoyosi Odenike MDKenan Onel MD, PhDElizabeth Rich MD, PhDJanet Rowley MD, DScHarinder Singh PhDDorothy Sipkins MD, PhDSonali Smith MDWendy Stock MDMichael Thirman MDKoen van Besien MDJames Vardiman MDAmittha Wickrema PhDYanming Zhang MDTodd Zimmerman MDRankAssociate ProfessorAssistant ProfessorAssociate ProfessorAssistant ProfessorAssistant ProfessorProfessorAssistant ProfessorAssistant ProfessorInstructorAssociate ProfessorProfessorProfessorAssociate ProfessorProfessorAssistant ProfessorAssistant ProfessorAssistant ProfessorProfessorProfessorAssistant ProfessorAssociate ProfessorProfessorAssociate ProfessorProfessorProfessorAssociate ProfessorAssistant ProfessorAssociate ProfessorDepartmentPathologyMedicinePathologyMedicineMedicinePediatricsMedicineMedicinePathologyPathologyMedicineMedicinePathologyPediatricsMedicinePediatricsMedicineMedicineMolecular Genetics and Cell BiologyMedicineMedicineMedicineMedicineMedicinePathologyMedicineMedicineMedicine30UCCRC SCIENTIFIC REPORT 2009* Reflects all Program membership during 2008-2009
Featured Faculty Research Summaries †Investigators in the Molecular Genetics and Hematopoiesis Program aim tounderstand the molecular basis of normal and aberrant hematopoeisis to improvethe diagnosis and treatment of hematological diseases. Research themes includeelucidating the mechanisms of normal hematopoiesis and the pathogenesis ofleukemia, development and characterization of animal models of hematologicmalignancies, and conducting clinical trials of experimental therapeutics. Belowis a sampling of current research being conducted in the Program.Theme: Mechanisms of Normal HematopoiesisBarbara Kee, PhDAssociate Professor of PathologyResearch in the Kee laboratory is focused ondetermining the molecular mechanisms that guide cellfate choices in the hematopoietic system. The laboratoryhas been examining the role of the E2A transcriptionfactors and their antagonists, the Id (Inhibitor ofDifferentiation) proteins, in the development oflymphoid lineage cells. These proteins are knownto function in cell fate decisions in invertebrates. Inmammals, appropriate expression and function of theseE- and Id- proteins is required to prevent B-lymphocyte,T-lymphocyte, and natural killer (NK) cell immunedeficiencies and T-cell malignancy.Dr. Koen van BesienMolecular Genetics& HematopoiesisDr. Kee’s current specific aims are to 1) determine the role of E2A in promoting lymphoid differentiation fromhematopoietic stem cells; 2) determine the targets of E2A proteins that promote T lymphocyte lineage specification;3) determine the mechanism underlying T cell transformation in E2A-deficient mice; and 4) determine whether Idproteins play an essential role in NK cell lineage specification. These goals are being addressed using a combinationof in vitro and in vivo assays with cells derived from gene-targeted mice.The laboratory has recently demonstrated that E2A proteins are required for development of lymphoid-primedmultipotent progenitors (LMPPs), which are the progeny of HSCs that have lost the capacity to differentiate intomegakaryocytes and erythrocytes but retain the ability to become lymphocytes, macrophages, and granulocytes.This finding places the E2A proteins among the first transcription factors required for specification of the lymphoidfate. Within LMPPs, E2A is required for proper activation of lymphoid gene expression and further differentiationinto B-lymphocytes. T lymphocyte numbers are also reduced in E2A-deficient mice and may be explained by thefailure of LMPPs to appropriately express two genes, Notch1 and Ccr9. Ccr9 encodes a chemokine receptor thatpromotes migration of multipotent progenitors, such as LMPPs, into the thymus where T lymphocyte developmentoccurs. Notch1 encodes a transmembrane receptor that is essential for T lymphocyte lineage specification.Importantly, a few early T-lymphocyte progenitors are present in the thymus of E2A-deficient mice, and these cellsare able to signal through Notch1, resulting in increased Notch1 expression. However, the cells still fail to undergoproper T lymphocyte lineage specification.Dr. Kee’s recent results indicate that this failure of T lymphocyte lineage specification is due, at least in part, toan inability to control the expression of Gata3, a transcription factor that can block T cell development and divertcells into non-T lymphocyte fates when expressed at high levels. How E2A prevents over-expression of Gata3remains to be determined. Nonetheless, their results indicate that E2A promotes T lymphocyte lineage specificationthrough both activation and repression of multiple target genes. This work is expanding our understanding of themechanisms by which networks of transcription factors contribute to lymphoid specification and further reveal howan individual transcription factor can promote specification to multiple distinct lineages.† Note: Due to space constraints, only a small representative sample of Program members is presented here.UCCRC SCIENTIFIC REPORT 200931
Theme: Pathogenesis of LeukemiaDorothy Sipkins, MD, PhDAssistant Professor of MedicineThe Sipkins laboratory focuses on defining the molecular characteristicsof tissue microenvironments, or “niches”, that foster the survival andregeneration of both normal and cancerous hematopoietic stem cells. Thelaboratory also examines the impact of malignant growth on the functionof the normal hematopoietic stem cell niche. In combination with classicalmolecular and cell biology approaches, state-of-the-art in vivo multiphotonand confocal optical imaging techniques are utilized to explore thesequestions in real-time.Dr. Janet RowleyApplying these techniques to a mouse xenograft model of acutelymphoblastic leukemia (ALL), the laboratory has recently shown that ALLcell growth disrupts normal hematopoietic progenitor cell (HPC) bone marrow niches and creates abnormal microenvironmentsthat sequester transplanted human CD34+ (HPC enriched) cells. CD34+ cells in leukemic mice decline in number over timeand fail to mobilize into the peripheral circulation in response to cytokine stimulation. The Sipkins group demonstrated thatALL cells secrete large quantities of a cytokine, stem cell factor (SCF), normally present at low levels in the bone marrow. Byneutralizing SCF activity, the laboratory was able to inhibit CD34+ cell migration into malignant niches, normalize CD34+cell numbers, and restore CD34+ cell mobilization in leukemic mice. These data suggest that the tumor microenvironmentcauses HPC dysfunction by usurping normal HPC niches, and that therapeutic inhibition of HPC interaction with tumor nichesmay help maintain normal progenitor cell function in the setting of malignancy. This work, published recently in Science, hasexposed a novel therapeutic target that could potentially counteract the effects of cancer on normal bone marrow function.Other projects in the laboratory include examining the interactions of breast cancer metastases with the bone marrowmicroenvironment. The Sipkins group is also studying the role of microenvironmental derangements in facilitating theprogression of the Philadelphia chromosome-negative myeloproliferative disorders. The laboratory is also actively establishinga mesenchymal stem cell transplant model to understand the regulation of the mesenchymal stem cell pool in the bone marrowbetter, as well as its impact on the hematopoietic stem cell compartment.Jianjun Chen, PhDAssistant Professor of MedicineThe major research interest of the Chen laboratory is to conduct integrated analyses of cancer-“omics” on both protein-codingand non-coding genes (particularly, microRNAs) regarding both genetic and epigenetic changes in the development of leukemiaand lymphoma using a variety of techniques. The laboratory aims to obtain a more complete understanding of the complexgenetic and epigenetic alterations in cancer development, and to identify novel markers and targets for the diagnosis, prognosis,and treatment of cancers. MicroRNAs (miRNAs) are a class of small (~22 nucleotides) non-coding RNAs that regulate diversebiological processes and, thereby, play important regulatory roles in both health and disease. In addition, Dr. Chen is alsointerested in identifying leukemia-stem-cell-specific genetic and epigenetic changes on both protein-coding and non-codinggenes. These genes and the relevant pathways could serve as therapeutic targets in the future to overcome drug resistance.During the past two years, the Chen laboratory has made great progress in the study of leukemia and has reported severalimportant findings in the field. The Chen group, along with colleagues, performed a large-scale, genome-wide microRNA(miRNA) expression profiling assay to understand the distinct mechanisms in leukemogenesis between acute lymphoblasticleukemia (ALL) and acute myeloid leukemia (AML) and to identify novel markers for diagnosis and treatment. The teamidentified 27 miRNAs that are differentially expressed between ALL and AML. Among them, miRNA-128a and b aresignificantly overexpressed, while let-7b and miR-223 are significantly down-regulated in ALL compared to AML. They are the32UCCRC SCIENTIFIC REPORT 2009
most discriminatory miRNAs between ALL and AML. Furthermore, overexpression of miR-128 in ALL was at least partlyassociated with promoter hypomethylation. Using the expression signatures of a minimum of two of these miRNAs resultedin an accuracy rate of over 95% in the diagnosis of ALL and AML.In a second genome-wide miRNA expression analysis in 52 acute myeloid leukemia (AML) samples with commontranslocations, including t(8;21)/AML1(RUNX1)-ETO(RUNX1T1), inv(16)/CBFB-MYH11, t(15;17)/PML-RARA, and MLLrearrangements, distinct miRNA expression patterns were observed for t(15;17), MLL rearrangements, and core-bindingfactor (CBF) AMLs including both t(8;21) and inv(16) samples. Expression signatures of a minimum of two (i.e., miR-126/126),three (i.e., miR-224, miR-368, and miR-382), and seven (miR-17-5p and miR-20a, plus the aforementioned five) miRNAs couldaccurately discriminate CBF, t(15;17), and MLL-rearrangement AMLs, respectively, from each other. The Chen laboratoryand colleagues further showed that the elevated expression of miR-126/126 in CBF AMLs was associated with promoterdemethylation, but not with amplification or mutation of the genomic locus. Their gain- and loss-of-function experimentsshowed that miR-126/126 inhibited apoptosis and increased the viability of AML cells, and enhanced the colony formingability of mouse normal bone marrow progenitor cells alone and particularly, in co-operation with AML1-ETO, likely throughtargeting Polo-like kinase 2 (PLK2), a tumor suppressor. These results demonstrate that specific alterations in miRNAexpression distinguish AMLs with common translocations, and imply that the deregulation of specific miRNAs may play arole in the development of leukemia with these associated genetic rearrangements.Molecular Genetics& HematopoiesisTheme: Animal Models of Hematologic MalignanciesBeverly Baron, MDAssociate Professor of PathologyThe Baron group and others identified the BCL6 gene inassociation with recurring chromosomal translocationsthat accompany human lymphoid malignancies, especiallydiffuse large-cell B-cell lymphomas (DLBL). Thebreakpoints cluster around the first (noncoding) exon ofBCL6, and it is believed that BCL6 expression becomesderegulated because heterologous promoters/enhancersare substituted for the normal BCL6 regulatory sequencesas a result of these translocations. Perturbation of BCL6biology is likely to be very important in the pathogenesisof almost all human DLBL, since virtually all of them haveIntravenous injection of a novel B-lymphoma cell line into a syngeneicbeen found to contain BCL6 somatic mutations and/orC57BL6 mouse results in B220+ (green fluorescent cells) infiltrating nodularproliferations within liver tissue. Cells expressing lower levels of B220rearrangements, which are believed to result in abnormaldemonstrated plasmacytic differentiation. (Image by X. Luo and K. Cohen)regulation of BCL6 protein expression. BCL6 is expressedalso in a number of T-cell lymphomas. The BCL6 gene encodes a nuclear zinc finger protein containing 706 amino acids,which is similar to Kruppel-type zinc finger transcription factors, and is a transcriptional repressor. This protein is expressedat high levels in human lymphoid germinal center B cells, is needed for germinal center formation, and interacts with otherproteins that are components of histone deacetylase complexes.Dr. Baron’s laboratory described the first (and, to date, the only) mouse model of the human BCL6 transgene. The miceexpress the human BCL6 transgene constitutively specifically in lymphocytes, both B and T, and thus mimic a commontranslocation found in human lymphomas, the t(3;14)(q27;q32), in which the normal BCL6 regulatory sequences are lost, and,instead, immunoglobulin heavy chain (IGH) sequences are juxtaposed upstream of BCL6 coding sequences. A fraction ofthese mice develop spontaneous B- and T-cell lymphomas after a prolonged latency period, but the incidence is dramaticallyenhanced, and the time-frame shortened, following administration of N-ethyl-N-nitrosourea (ENU), which is an alkylatingagent that induces single-base mutations. This observation suggests that cooperating mutations play a critical role in BCL6-related lymphomagenesis.UCCRC SCIENTIFIC REPORT 200933
The ultimate goals of the laboratory are to identify new genes that interact with BCL6 and to gain a better understanding ofthe role of PDCD2 in lymphoma pathogenesis. Specific research aims are to 1) identify the genes that cooperate with BCL6 inthe biological events that lead to lymphoma development; and 2) study the programmed cell death-2 (PDCD2) gene, which thelaboratory previously identified as a target of BCL6.BCL6 may promote lymphoma development, at least in part, by interfering with normal cellular apoptosis events throughrepression of PDCD2. The laboratory recently showed that the BCL6 protein binds to the PDCD2 promoter both in vitro and invivo, that BCL6 can repress transcription from the PDCD2 promoter, and demonstrated the anticipated inverse relationship inthe expression patterns of BCL6 and PDCD2 in mouse lymphoid tissues as well as in human B- and T-cell lymphomas. Further,with the use of small interfering RNA duplexes, the Baron group was able to show that knockdown of the BCL6 protein in alymphoma cell line leads to increased PDCD2 protein expression. These studies will likely provide further insight into thisimportant human disease and support the development of new molecular tools for the treatment of lymphoma.Theme: Experimental TherapeuticsToyosi Odenike, MDAssistant Professor of MedicineThe long term goal of Dr. Odenike’s research is to translateour understanding of the molecular-genetic pathways involvedin malignant hematologic diseases into meaningful, moreefficacious and less toxic therapeutic interventions. Animmediate focus of this effort is the clinical and translationaldevelopment of novel agents that target epigenetic changes inmyeloid malignancies. Recruitment of histone deacetylases andDr. Kenan Onel with a pediatric patientDNA hypermethylation are two pathways of epigenetic silencingwhich have been linked and implicated in the transcriptionaldysregulation underlying a variety of myeloid neoplasia. Unlike gene deletions which are irreversible, epigenetic changes canpotentially be reversed by chromatin remodeling agents such as histone deacetylase and DNA methyltransferase inhibitors,restoring tumor cells to a more transcriptionally normal state. A number of ongoing and recently-completed projects are basedon the hypothesis that chromatin remodeling agents are active in a wide spectrum of myeloid neoplasms, and that the activity ofthese agents is mediated by epigenetic modulation of gene expression.Specific aims of Dr. Odenike’s research are to 1) determine the clinical and biologic relevance of histone deacetylase (HDAC)inhibition in AML; 2) determine the clinical and biologic relevance of DNA methyltransferase (DNMT) inhibition in chronicmyeloproliferative neoplasms; 3.) investigate the effects of these agents on modulation of gene expression; and 4) optimize theactivity of these agents in myeloid neoplasms by developing rationally-designed combinations.The Odenike team has investigated the HDAC inhibitor, depsipeptide, in a multi-center NCI sponsored trial conducted throughthe University of Chicago Phase II Consortium in relapsed and refractory AML. This trial has, for the first time, demonstratedthat depsipeptide has selective antileukemic activity in patients with Core Binding Factor (CBF) leukemias, a cytogenetic subsetof AML where recruitment of histone deacetylases is an established mechanism of leukemogenesis. In addition, specific targetgenes, such as CDKN2A, CDKN2B, and MDR1, were significantly upregulated in the subset of patients with CBF leukemias aspreviously hypothesized. This has served as an important “proof of principle” for the mechanism of action of HDAC inhibitorsin AML and provides a potential rationale for the clinical investigation of these compounds in combination with other agentsin AML. In addition, the Odenike team demonstrated in a multi-center NCI sponsored trial conducted through the Universityof Chicago Phase II Consortium that the DNMT inhibitor, decitabine, has clinical activity in myelofibrosis, a disease for whichthere is no standard therapy.34UCCRC SCIENTIFIC REPORT 2009
Currently, combined DNMT and HDAC inhibition is being investigated in myeloid neoplasms in the context of an ongoingPhase I trial, given the synergy that has been observed in vitro between these 2 pathways of epigenetic silencing. Future workwill focus on investigating combinations, involving agents that target aberrant transcription (such as chromatin remodelingagents) with those that inhibit dysregulated signaling pathways, in an effort to optimize the clinical and biologic effects ofthese agents in myeloid neoplasia.Sonali Smith, MDAssociate Professor of MedicineA major challenge in developing a research agenda for Hodgkin and non-Hodgkin lymphomas is the current recognitionof nearly 60 unique clinicopathologic subtypes. Many of the subtypes are in fact rare diseases with fewer than 5000 newcases per year throughout the country. The Lymphoma Program at The University of Chicago is a highly visible clinical andtranslational research program that has been in a period of substantial growth since 2001 and currently consists of fourfaculty members, including Drs. Koen van Besien, Sonali Smith, Kenneth Cohen, and Justin Kline. Dr. Smith, the associatedirector of the program, is institutional Principal Investigator on 10 clinical trials and hosts the annual International ChicagoLymphoma Symposium, the only lymphoma-dedicated symposium in the Midwest.Molecular Genetics& HematopoiesisThe Lymphoma Program at The University of Chicago has adopted a two-pronged approach in an effort to serve thevariety of patients seen in the clinic. The first is to provide opportunities for patients to participate in a range of clinicaltrials that are either subtype specific or that target a common oncogenic pathway believed to promote lymphomagenesis.Large scale front-line studies, intended for patients that are treatment-naïve, are primarily via collaborations forged withCALGB. Through the CALGB, Dr. Smith has published several reports, including a relatively widely quoted negative studyof thalidomide in patients with relapsed indolent lymphomas, which contrasts with the significant activity of secondgeneration immunomodulatory agents derived from thalidomide. The second programmatic approach is to focus onnew drug development for relapsed lymphomas through The University of Chicago Phase II Consortium. In this venue,investigator-initiated trials free of pharmaceutical bias are offered to patients with relapsed disease without other standardtreatment options. The University of Chicago, through this phase II mechanism, was the first to show activity of a classof agents called mTOR inhibitors against two of the most common types of lymphomas (diffuse large B-cell lymphomaand follicular lymphoma). mTOR, or mammalian target of rapamycin, is a ser/thr kinase that controls the start of mRNAtranslation. Several known oncogenic pathways converge upon mTOR, making it an attractive target to modulate upstreamsignals simultaneously. Furthermore, mTOR controls translation of several mRNA transcripts that are critical componentsof lymphomagenesis, including CCND1, VEGF, and MYC. Two subsequent proposals are being explored to examine mTORinhibition, in combination with other biologic agents, as well as with standard cytotoxic chemotherapy. In addition, theProgram seeks to identify predictive markers for response to mTOR inhibitors.The other major focus of the Lymphoma Program is to explore the role of both autologous and allogeneic hematopoietic stemcell transplantation for patients with relapsed lymphomas. High dose chemotherapy followed by autologous stem cell rescue(ASCT) can successfully salvage many patients with chemosensitive relapsed aggressive lymphomas, but relapse remains acommon and usually fatal event. The Program recently completed a trial evaluating the safety and efficacy of post-transplantimmunomodulation using GM-CSF and IL-2 to augment rituximab, with the goal of eradicating minimal/undetectableresidual disease following high dose chemotherapy to reduce relapse. Two ongoing studies are extending interest in posttransplantimmunomodulation, one trial using Ontak (toxin-linked monoclonal antibody against IL-2 receptor) followingtransplant for T-cell lymphomas and a second trial evaluating a novel monoclonal antibody targeting PD-1 as part of the B7-family of surface receptors for patients with diffuse large B-cell lymphomas.In summary, the Lymphoma program currently has 15 active therapeutic and database protocols addressing both commonand uncommon lymphoma patient populations. Dr. Smith’s future research objective is to expand on mTOR inhibition as aplatform for anti-lymphoma treatments.UCCRC SCIENTIFIC REPORT 200935
Additional Program Highlights*Research•• Regulation of B cell fate commitment and immunoglobulinheavy-chain gene rearrangements by Ikaros. Harinder Singh, PhDand colleagues have provided novel insights into B cell developmentby identifying the critical role of the transcription factor Ikaros.Drs. John Cunningham (Molecular Genetics andHematopoiesis Program) and Susan Cohn(Clinical and Experimental Therapuetics Program)These investigators demonstrated that the transcription factor EBF restored the regeneration of CD19+ pro-B cells fromIkaros-deficient hematopoietic progenitors. These pro-B cells, despite having normal expression of key transcription factors,EBF and Pax 5, were not committed to the B-cell fate and failed to recombine variable gene segments at the immunoblobulinheavy-chain locus. Expression of Ikaros promoted heavy-chain gene rearrangements by inducing expression of therecombination-activating genes as well as by controlling accessibility of the variable gene segments compaction of theimmunoglobulin heavy-chain locus. Thus, Ikaros is a key regulatory component of the network that regulates B cell fatecommitment and immunoglobulin heavy-chain gene recombination (Reynaud et al. Nat Immunol 9:927-936, 2008).••••••••MDM2 SMP309 and TP53 Arg72Pro Interact to Alter Therapy-Related Acute Myeloid Leukemia Susceptibility(Intra- and Interprogrammatic). Kenan Onel, MD and colleagues, including Program 2 members Drs. Richard Larsonand Michelle Le Beau and Dr. Nathan Ellis (Cancer Risk and Prevention Program), have determined that polymorphismsin two DNA repair genes, MDM2 and TP53, interact to increase susceptibility to the development of therapy-related AML.This effect was observed in patients treated with chemotherapy who had loss of chromosomes 5 and/or 7, and acquiredabnormalities associated with prior exposure to alkylator chemotherapy, but not in patients treated with radiotherapy. Thesedata suggest that MDM2 and TP53 variants interact to modulate responses to genotoxic therapy and are determinants of riskfor t-AML (Ellis et al. Blood 112:741-749, 2008).Pretreatment C-Reactive Protein is a Predictor for Outcomes After Reduced-Intensity Allogeneic HematopoieticCell Transplantation (Intraprogrammatic). Andrew Artz, MD and co-investigators, Amittha Wickrema, PhD, LucyGodley, MD, PhD, Toyosi Odenike, MD, Elizabeth Rich, MD, PhD, Wendy Stock, MD, Richard Larson, MD and Koen vanBesien, MD described the independent prognostic impact of two commonly used biomarkers – C-reactive protein (CRP) andinterleukin(IL)-6 – on outcome following allogeneic stem cell transplantation. Using samples from patients who underwenta uniform reduced-intensity conditioning (RIC) regimen, they found that elevated CRP levels prior to allogeneic stem celltransplant were highly predictive of greater non-relapse mortality. Their results are of interest since they suggest that asimple pre-transplant blood test may be useful for predicting transplant tolerance (Artz et al, Biol Blood Marrow Transplant14:1209-1216, 2008).Genome-wide association study to identify novel loci associated with therapy-related myeloid leukemia susceptibility(Interprogrammatic). Kenan Onel, MD and colleagues, including Program 2 members Drs. Michelle Le Beau and RichardLarson and Dr. Nancy Cox (Cancer Risk and Prevention Program), examined whether the effect sizes of variants associatedwith t-AML would be greater than in sporadic cancer and whether these variants could be detected even in a modest-sizedcohort. In an association study using Affymetrix Mapping 10K arrays, they found a significant excess of associations overchance. The investigators genotyped the 10 most significantly associated single nucleotide polymorphisms (SNPs) in anindependent t-AML cohort and obtained evidence of association with t-AML for 3 SNPs in the subset of patients with loss ofchromosomes 5 or 7 or both, acquired abnormalities associated with prior exposure to alkylator chemotherapy. Their resultsdemonstrate that the effect of genetic factors contributing to cancer risk is potentiated and more readily discernable int-AML compared with sporadic cancer (Knight et al, Blood 113(22):5575-5582, 2009).Determination of outcomes for adolescents and young adults with acute lymphoblastic leukemia treated on cooperativegroup protocols (Intraprogrammatic). James Nachman, MD and co-investigators including Drs. Wendy Stock, JamesVardiman, and Richard Larson, performed a retrospective comparison of presenting features, planned treatment, complete36UCCRC SCIENTIFIC REPORT 2009* Due to space constraints, only a small representative sample of Program highlights is presented here.
emission rate, and outcome of greater than 300 adolescents and young adults with newly diagnosed acute lymphoblasticleukemia (ALL) who were treated on consecutive trials in either the Children’s Cancer Group (CCG) or the Cancer andLeukemia Group B (CALGB). While complete remission rates were identical, patients in the CCG group had significantlyhigher 7-year event-free and overall survival rates compared to those in the CALGB group. Comparison of the regimensshowed that CCG patients received earlier and more intensive central nervous system prophylaxis and higher cumulativedoses of nonmyelosuppressive agents. As a result of these findings, a prospective study for adolescents and young adultswith ALL using the more successful approach of the CCG has been initiated (Stock et al, Blood 112(5):1646-54, 2008).Selected New Funding•• The National Cancer Institute awarded Lucy Godley, MD, PhD and her colleagues R01 funding to understand themechanisms by which epigenetic alterations originate within cancer cells. Investigators are studying how expression ofthe DNMT3B gene, which encodes one of three methyltransferases, affects mouse development, methylation patterns andphenotypes of cancer cells, and DNA methylation. Results will likely provide a basis for novel diagnostic and therapeuticstrategies applicable to virtually all forms of cancer.Molecular Genetics& Hematopoiesis••••Michelle Le Beau, PhD is the primary investigator in a program project (P01), funded by the National Cancer Institute, tostudy the molecular mechanisms and genetic susceptibilities leading to therapy-related acute myeloid leukemia (t-AML)and myelodysplastic syndrome (t-MDS) that develop after cytotoxic treatment with drugs targeting topoisomerase II.The project aims to identify genetic variants that may be genetic risk factors or biomarkers for t-AML, somatic alterationsassociated with t-AML, and myeloid leukemia tumor suppressor gene(s) (TSG). These studies may lead, ultimately, to thedevelopment of individualized cancer prevention and early detection strategies, such as altered primary therapy. Coinvestigatorsinclude Drs. Richard Larson, Kenan Onel, and Theodore Karrison (Clinical and Experimental TherapeuticsProgram).Jianjun Chen, PhD has been awarded an R01 grant from the National Cancer Institute to determine the role andfunctional mechanisms of an miRNA cluster in leukemogenesis. MicroRNAs (miRNAs, miRs) are an abundant classof small non-coding RNAs that regulate diverse biological processes. Recent studies suggest that a cluster of miRNAs,the miR-17-92 polycistron located at 13q31, functions as an oncogene in various cancers. The project aims to determinewhether the miR-17-92 cluster plays an essential role in leukemogenesis and in proliferation and differentiation ofhematopoietic progenitor cells. These studies are likely to identify the critical leukemia-related targets of the miRNAsand their roles and relevant pathways in leukemogenesis.New Faculty Recruitments and UCCRC MembersJianjun Chen, PhD’s research is focused on the integrated analyses of protein-coding and non-coding genes involved in thedevelopment of leukemia and lymphoma. Dr. Chen aims to gain an improved understanding of the genetic and epigeneticalterations that occur during cancer development and in leukemia stem cells in order to identify new markers and targetsfor cancer diagnosis and treatment. An additional goal of Dr. Chen’s research is to develop a reproducible method for thederivation of transplantable hematopoietic stem cells from embryonic stem cells or induced pluripotent stem cells.Kenneth Cohen, MD research aims to understand how non-malignant host cells within cancers contribute to tumor cellgrowth, metastasis, and protection from anti-cancer therapies. Dr. Cohen’s current research seeks to identify molecularmechanisms governing interactions between pro-angiogenic bone marrow-derived cells and tumor vascular development.Sandeep Gurbuxani, MBBS, PhD is interested in the mechanisms of resistance to chemotherapy-induced cell death incancer. The focus of his current research is the mechanism of glucocorticoid induced cell death (and resistance to this celldeath) in acute lymphoblastic leukemia.UCCRC SCIENTIFIC REPORT 200937
Selected Publications* : Intraprogrammatic Collaboration# : Interprogrammatic CollaborationAnastasi, John MD* Ozer O, Zhao YD, Ostler KR, Akin C, Anastasi J, Vardiman JW, Godley LA.The identification and characterisation of novel KIT transcripts in aggressivemast cell malignancies and normal CD34+ cells. Leuk Lymphoma 49(8):1567-77, 2008.* Baer MR, George SL, Caligiuri MA, Sanford BL, Bothun SM, Mrozek K,Kolitz JE, Powell BL, Moore JO, Stone RM, Anastasi J, Bloomfield CD, LarsonRA. Low-dose interleukin-2 immunotherapy does not improve outcomeof patients age 60 years and older with acute myeloid leukemia in firstcomplete remission: Cancer and Leukemia Group B Study 9720. J Clin Oncol26(30):4934-9, 2008.Anastasi J. Mantle, blastic, Burkitt. Leuk Lymphoma 49(4):655-6, 2008.Anastasi J. Identifying a new marker and potential therapeutic target in mantlecell lymphoma: cutting to the chase. Leuk Lymphoma 49(7):1236-7, 2008.* Qian Z, Mao L, Fernald AA, Yu H, Luo R, Jiang Y, Anastasi J, Valk PJ, DelwelR, Le Beau MM. Enhanced expression of FHL2 leads to abnormal myelopoiesisin vivo Leukemia, 2009.Artz, Andrew MD* Artz AS, Wickrema A, Dinner S, Godley LA, Kocherginsky M, Odenike O,Rich ES, Stock W, Ulaszek J, Larson RA, van Besien K. Pretreatment C-reactiveprotein is a predictor for outcomes after reduced-intensity allogeneichematopoietic cell transplantation. Biol Blood Marrow Transplant 14(11):1209-16, 2008.* Dew A, Collins D, Artz A, Rich E, Stock W, Swanson K, van Besien K. Paucityof HLA-identical unrelated donors for African-Americans with hematologicmalignancies: the need for new donor options. Biol Blood Marrow Transplant14(8):938-41, 2008.Lee SJ, Joffe S, Artz AS, Champlin RE, Davies SM, Jagasia M, Kernan NA,Loberiza FR Jr, Soiffer RJ, Eapen M. Individual physician practice variation inhematopoietic cell transplantation. J Clin Oncol 26(13):2162-70, 2008.Swierczek SI, Agarwal N, Nussenzveig RH, Rothstein G, Wilson A, ArtzA, Prchal JT. Hematopoiesis is not clonal in healthy elderly women. Blood112(8):3186-93, 2008.Lee SJ, Astigarraga CC, Eapen M, Artz AS, Davies SM, Champlin R, JagasiaM, Kernan NA, Loberiza FR Jr, Bevans M, Soiffer RJ, Joffe S. Variation insupportive care practices in hematopoietic cell transplantation. Biol BloodMarrow Transplant 14(11):1231-8, 2008.* # Poire X, Artz A, Larson RA, Kline J, Odenike O, Rich E, Godley L, Stock W,van Besien K. Allogeneic stem cell transplantation with alemtuzumab-basedconditioning for patients with advanced chronic myelogenous leukemia. LeukLymphoma 50(1):85-91, 2009.Besien KV, Kunavakkam R, Rondon G, De Lima M, Artz A, Oran B, Giralt S.Fludarabine-melphalan conditioning for AML and MDS: alemtuzumab reducesacute and chronic GVHD without affecting long-term outcomes. Biol BloodMarrow Transplant 15(5):610-7, 2009.Chen, Jianjun PhD* Li Z, Luo RT, Mi S, Sun M, Chen P, Bao J, Neilly MB, Jayathilaka N, JohnsonDS, Wang L, Lavau C, Zhang Y, Tseng C, Zhang X, Wang J, Yu J, Yang H,Wang SM, Rowley JD, Chen J, Thirman MJ. Consistent deregulation of geneexpression between human and murine MLL rearrangement leukemias. CancerRes 69(3):1109-16, 2009.Cohen, Kenneth MDSzotek PP, Chang HL, Brennand K, Fujino A, Pieretti-Vanmarcke R, Lo CelsoC, Dombkowski D, Preffer F, Cohen KS, Teixeira J, Donahoe PK. Normalovarian surface epithelial label-retaining cells exhibit stem/progenitor cellcharacteristics. Proc Natl Acad Sci U S A 105(34):12469-73, 2008.Cunningham, John MDHislop NR, Caddy J, Ting SB, Auden A, Vasudevan S, King SL, Lindeman GJ,Visvader JE, Cunningham JM, Jane SM. Grhl3 and Lmo4 play coordinate rolesin epidermal migration. Dev Biol 321(1):263-72, 2008.Wilanowski T, Caddy J, Ting SB, Hislop NR, Cerruti L, Auden A, ZhaoLL, Asquith S, Ellis S, Sinclair R, Cunningham JM, Jane SM. Perturbeddesmosomal cadherin expression in grainy head-like 1-null mice. EMBO J27(6):886-97, 2008.Freeman-Anderson NE, Zheng Y, McCalla-Martin AC, Treanor LM, ZhaoYD, Garfin PM, He TC, Mary MN, Thornton JD, Anderson C, Gibbons M,Saab R, Baumer SH, Cunningham JM, Skapek SX. Expression of the Arf tumorsuppressor gene is controlled by Tgf{beta}2 during development. Development136(12):2081-9, 2009.Godley, Lucy MD, PhD* # Stock W, Undevia SD, Bivins C, Ravandi F, Odenike O, Faderl S, Rich E,Borthakur G, Godley L, Verstovsek S, Artz A, Wierda W, Larson RA, Zhang Y,Cortes J, Ratain MJ, Giles FJ. A phase I and pharmacokinetic study of XK469R(NSC 698215), a quinoxaline phenoxypropionic acid derivative, in patients withrefractory acute leukemia. Invest New Drugs 26(4):331-8, 2008.* # Gordon MK, Sher D, Karrison T, Kebriaei P, Chuang K, Zhang Y,McDonnell D, Artz A, Godley L, Odenike O, Rich E, Michaelis L, ThirmanMJ, Wickrema A, van Besien K, Larson RA, Stock W. Successful autologousstem cell collection in patients with chronic myeloid leukemia in completecytogenetic response, with quantitative measurement of BCR-ABL expressionin blood, marrow, and apheresis products. Leuk Lymphoma 49(3):531-7, 2008.* Ozer O, Zhao YD, Ostler KR, Akin C, Anastasi J, Vardiman JW, Godley LA.The identification and characterisation of novel KIT transcripts in aggressivemast cell malignancies and normal CD34+ cells. Leuk Lymphoma 49(8):1567-77, 2008.* Klisovic RB, Stock W, Cataland S, Klisovic MI, Liu S, Blum W, Green M,Odenike O, Godley L, Burgt JV, Van Laar E, Cullen M, Macleod AR, BestermanJM, Reid GK, Byrd JC, Marcucci G. A phase I biological study of MG98, anoligodeoxynucleotide antisense to DNA methyltransferase 1, in patientswith high-risk myelodysplasia and acute myeloid leukemia. Clin Cancer Res14(8):2444-9, 2008.Carbonaro A, Mohanty SK, Huang H, Godley LA, Sohn LL. Cellcharacterization using a protein-functionalized pore. Lab Chip 8(9):1478-85,2008.* Artz AS, Wickrema A, Dinner S, Godley LA, Kocherginsky M, Odenike O,Rich ES, Stock W, Ulaszek J, Larson RA, van Besien K. Pretreatment C-reactiveprotein is a predictor for outcomes after reduced-intensity allogeneichematopoietic cell transplantation. Biol Blood Marrow Transplant 14(11):1209-16, 2008.* # Poire X, Artz A, Larson RA, Kline J, Odenike O, Rich E, Godley L, Stock W,van Besien K. Allogeneic stem cell transplantation with alemtuzumab-basedconditioning for patients with advanced chronic myelogenous leukemia. LeukLymphoma 50(1):85-91, 2009.Fackenthal JD, Godley LA. Aberrant RNA splicing and its functionalconsequences in cancer cells. Dis Model Mech 1(1):37-42, 2008.Gounari, Fotini PhD, DSc.Dose M, Gounari F. Fifty ways to Notch T-ALL. Blood 112(3):457-8, 2008.Li X, Gounari F, Protopopov A, Khazaie K, von Boehmer H. Oncogenesisof T-ALL and nonmalignant consequences of overexpressing intracellularNOTCH1. J Exp Med 205(12):2851-61, 2008.# Dose M, Sleckman BP, Han J, Bredemeyer AL, Bendelac A, Gounari F.Intrathymic proliferation wave essential for Vα 14+ natural killer T celldevelopment depends on c-Myc. Proc Natl Acad Sci U S A 106(21):8641-6, 2009.Hu MG, Deshpande A, Enos M, Mao D, Hinds EA, Hu GF, Chang R, Guo Z,Dose M, Mao C, Tsichlis PN, Gounari F, Hinds PW. A requirement for cyclindependentkinase 6 in thymocyte development and tumorigenesis. Cancer Res69(3):810-8, 2009.Gurbuxani, Sandeep MBBS, PhD* Kirsammer G, Jilani S, Liu H, Davis E, Gurbuxani S, Le Beau MM, CrispinoJD. Highly penetrant myeloproliferative disease in the Ts65Dn mouse model ofDown syndrome. Blood 111(2):767-75, 2008.* Dias S, Mansson R, Gurbuxani S, Sigvardsson M, Kee BL. E2A ProteinsPromote Development of Lymphoid-Primed Multipotent Progenitors.Immunity 29(2):217-27, 2008.* # Rosen DS, Smith S, Gurbuxani S, Yamini B. Extranodal hairy cell leukemiapresenting in the lumbar spine. J Neurosurg Spine 9(4):374-6, 2008.38UCCRC SCIENTIFIC REPORT 2009
Kee, Barbara PhDDias S, Xu W, McGregor S, Kee B. Transcriptional regulation of lymphocytedevelopment. Curr Opin Genet Dev. Curr Opin Genet Dev 18(5):441-8, 2008.* Dias S, Mansson R, Gurbuxani S, Sigvardsson M, Kee BL. E2A ProteinsPromote Development of Lymphoid-Primed Multipotent Progenitors.Immunity 29(2):217-27, 2008.Bhalla S, Spaulding C, Brumbaugh RL, Zagort DE, Massari ME, Murre C, KeeBL. differential roles for the E2A activation domains in B lymphocytes andmacrophages. J Immunol 180(3):1694-703, 2008.Gao J, Graves S, Koch U, Liu S, Jankovic V, Buonamici S, El Andaloussi A,Nimer SD, Kee BL, Taichman R, Radtke F, Aifantis I. Hedgehog signaling isdispensable for adult hematopoietic stem cell function. Cell Stem Cell 4(6):548-58, 2009.Kee BL, Dias S. A s-myly route toward lymphoid differentiation. Immunity30(4):474-6, 2009.Kee BL. E and ID proteins branch out. Nat Rev Immunol 9(3):175-84, 2009.Larson, Richard MD* # Ellis NA, Huo D, Yildiz O, Worrillow LJ, Banerjee M, Le Beau MM, LarsonRA, Allan JM, Onel K. MDM2 SNP309 and TP53 Arg72Pro interact to altertherapy-related acute myeloid leukemia susceptibility. Blood 112(3):741-9, 2008.Larson R. Allogeneic hematopoietic cell transplantation for adults with ALL.Bone Marrow Transplant 42 Suppl 1:S18-S24, 2008.Metzeler KH, Hummel M, Bloomfield CD, Spiekermann K, Braess J, SauerlandMC, Heinecke A, Radmacher M, Marcucci G, Whitman SP, Maharry K,Paschka P, Larson RA, Berdel WE, Buchner T, Wormann B, Mansmann U,Hiddemann W, Bohlander SK, Buske C. An 86 probe set gene expressionsignature predicts survival in cytogenetically normal acute myeloid leukemia.Blood 112(10):4193-201, 2008.* Baer MR, George SL, Caligiuri MA, Sanford BL, Bothun SM, Mrozek K,Kolitz JE, Powell BL, Moore JO, Stone RM, Anastasi J, Bloomfield CD, LarsonRA. Low-dose interleukin-2 immunotherapy does not improve outcomeof patients age 60 years and older with acute myeloid leukemia in firstcomplete remission: Cancer and Leukemia Group B Study 9720. J Clin Oncol26(30):4934-9, 2008.Paschka P, Marcucci G, Ruppert AS, Whitman SP, Mrozek K, Maharry K,Langer C, Baldus CD, Zhao W, Powell BL, Baer MR, Carroll AJ, CaligiuriMA, Kolitz JE, Larson RA, Bloomfield CD. Wilms’ tumor 1 gene mutationsindependently predict poor outcome in adults with cytogenetically normalacute myeloid leukemia: a cancer and leukemia group B study. J Clin Oncol26(28):4595-602, 2008.Hochhaus A, Baccarani M, Deininger M, Apperley JF, Lipton JH, Goldberg SL,Corm S, Shah NP, Cervantes F, Silver RT, Niederwieser D, Stone RM, DombretH, Larson RA, Roy L, Hughes T, Muller MC, Ezzeddine R, Countouriotis AM,Kantarjian HM. Dasatinib induces durable cytogenetic responses in patientswith chronic myelogenous leukemia in chronic phase with resistance orintolerance to imatinib. Leukemia 22(6):1200-6, 2008.Larson RA, Druker BJ, Guilhot F, O’Brien SG, Riviere GJ, Krahnke T,Gathmann I, Wang Y. Imatinib pharmacokinetics and its correlation withresponse and safety in chronic-phase chronic myeloid leukemia: a subanalysisof the IRIS study. Blood 111(8):4022-8, 2008.Le Beau, Michelle PhD* Li Z, Lu J, Sun M, Mi S, Zhang H, Luo RT, Chen P, Wang Y, Yan M, Qian Z,Neilly MB, Jin J, Zhang Y, Bohlander SK, Zhang DE, Larson RA, Le Beau MM,Thirman MJ, Golub TR, Rowley JD, Chen J. Distinct microRNA expressionprofiles in acute myeloid leukemia with common translocations. Proc NatlAcad Sci U S A 105(40):15535-40, 2008.* # Ellis NA, Huo D, Yildiz O, Worrillow LJ, Banerjee M, Le Beau MM, LarsonRA, Allan JM, Onel K. MDM2 SNP309 and TP53 Arg72Pro interact to altertherapy-related acute myeloid leukemia susceptibility. Blood 112(3):741-9, 2008.* Kirsammer G, Jilani S, Liu H, Davis E, Gurbuxani S, Le Beau MM, CrispinoJD. Highly penetrant myeloproliferative disease in the Ts65Dn mouse model ofDown syndrome. Blood 111(2):767-75, 2008.Mullighan CG, Miller CB, Radtke I, Phillips LA, Dalton J, Ma J, White D,Hughes TP, Le Beau MM, Pui CH, Relling MV, Shurtleff SA, Downing JR.BCR-ABL1 lymphoblastic leukaemia is characterized by the deletion of Ikaros.Nature 453(7191):110-4, 2008.Qian Z, Chen L, Fernald AA, Williams BO, Le Beau MM. A critical role for Apcin hematopoietic stem and progenitor cell survival. J Exp Med 205(9):2163-75,2008.* Knight JA, Skol AD, Shinde A, Hastings D, Walgren RA, Shao J,Tennant TR, Banerjee M, Allan JM, Le Beau MM, Larson RA, GraubertTA, Cox NJ, Onel K. A genome-wide association study to identify novelloci associated with therapy-related myeloid leukemia susceptibility.Blood 113(22):5575-82, 2009.* Qian Z, Mao L, Fernald AA, Yu H, Luo R, Jiang Y, Anastasi J, Valk PJ,Delwel R, Le Beau MM. Enhanced expression of FHL2 leads to abnormalmyelopoiesis in vivo. Leukemia, 2009.Nachman, James MD* Stock W, La M, Sanford B, Bloomfield CD, Vardiman JW, Gaynon P,Larson RA, Nachman J. What determines the outcomes for adolescentsand young adults with acute lymphoblastic leukemia treated oncooperative group protocols? A comparison of Children’s Cancer Groupand Cancer and Leukemia Group B studies. Blood 112(5):1646-54, 2008.# Seibel NL, Steinherz PG, Sather HN, Nachman JB, Delaat C, EttingerLJ, Freyer DR, Mattano LA Jr, Hastings CA, Rubin CM, Bertolone K,Franklin JL, Heerema NA, Mitchell TL, Pyesmany AF, La MK, EdensC, Gaynon PS. Early postinduction intensification therapy improvessurvival for children and adolescents with high-risk acute lymphoblasticleukemia: a report from the Children’s Oncology Group. Blood111(5):2548-55, 2008.French D, Hamilton LH, Mattano LA Jr, Sather HN, Devidas M,Nachman JB, Relling MV. A PAI-1 (SERPINE1) polymorphism predictsosteonecrosis in children with acute lymphoblastic leukemia: a reportfrom the Children’s Oncology Group. Blood 111(9):4496-9, 2008.Odenike, Olatoyosi MD* # Stock W,Undevia SD,Bivins C,Ravandi F,Odenike O,Faderl S,RichE,Borthakur G,Godley L,Verstovsek S,Artz A,Wierda W,LarsonRA,Zhang Y,Cortes J,Ratain MJ,Giles FJ. A phase I and pharmacokineticstudy of XK469R (NSC 698215), a quinoxaline phenoxypropionic acidderivative, in patients with refractory acute leukemia. Invest New Drugs26(4):331-8, 2008.* Klisovic RB, Stock W, Cataland S, Klisovic MI, Liu S, Blum W, GreenM, Odenike O, Godley L, Burgt JV, Van Laar E, Cullen M, Macleod AR,Besterman JM, Reid GK, Byrd JC, Marcucci G. A phase I biological studyof MG98, an oligodeoxynucleotide antisense to DNA methyltransferase1, in patients with high-risk myelodysplasia and acute myeloid leukemia.Clin Cancer Res 14(8):2444-9, 2008.* Artz AS, Wickrema A, Dinner S, Godley LA, Kocherginsky M, OdenikeO, Rich ES, Stock W, Ulaszek J, Larson RA, van Besien K. PretreatmentC-reactive protein is a predictor for outcomes after reduced-intensityallogeneic hematopoietic cell transplantation. Biol Blood MarrowTransplant 14(11):1209-16, 2008.* # Odenike OM, Larson RA, Gajria D, Dolan ME, Delaney SM, KarrisonTG, Ratain MJ, Stock W. Phase I study of the ribonucleotide reductaseinhibitor 3-aminopyridine-2-carboxaldehyde-thiosemicarbazone (3-AP)in combination with high dose cytarabine in patients with advancedmyeloid leukemia. Invest New Drugs 26(3):233-9, 2008.* Wetzler M, Donohue KA, Odenike OM, Feldman EJ, Hurd DD, StoneRM, Westerfelt P, Bloomfield CD, Larson RA. Feasibility of administeringoblimersen (G3139, Genasense) with imatinib mesylate in patients withimatinib resistant chronic myeloid leukemia--Cancer and leukemia groupB study 10107. Leuk Lymphoma 49(7):1274-8, 2008.* # Odenike OM, Alkan S, Sher D, Godwin JE, Huo D, Brandt SJ, GreenM, Xie J, Zhang Y, Vesole DH, Stiff P, Wright J, Larson RA, Stock W.Histone deacetylase inhibitor romidepsin has differential activity in corebinding factor acute myeloid leukemia. Clin Cancer Res 14(21):7095-101,2008.Onel, Kenan MD, PhD* # Ellis NA, Huo D, Yildiz O, Worrillow LJ, Banerjee M, Le Beau MM,Larson RA, Allan JM, Onel K. MDM2 SNP309 and TP53 Arg72Prointeract to alter therapy-related acute myeloid leukemia susceptibility.Blood 112(3):741-9, 2008.Kuptsova N, Chang-Claude J, Kropp S, Helmbold I, Schmezer P, vonFournier D, Haase W, Sautter-Bihl ML, Wenz F, Onel K, Ambrosone CB.Genetic predictors of long-term toxicities after radiation therapy forbreast cancer. Int J Cancer 122(6):1333-9, 2008.Molecular Genetics& HematopoiesisUCCRC SCIENTIFIC REPORT 200939
* Knight JA, Skol AD, Shinde A, Hastings D, Walgren RA, Shao J, Tennant TR,Banerjee M, Allan JM, Le Beau MM, Larson RA, Graubert TA, Cox NJ, Onel K.A genome-wide association study to identify novel loci associated with therapyrelatedmyeloid leukemia susceptibility. Blood 113(22):5575-82, 2009.Onel KB, Huo D, Hastings D, Fryer-Biggs J, Crow MK, Onel K. Lack ofassociation of the TP53 Arg72Pro SNP and the MDM2 SNP309 with systemiclupus erythematosus in Caucasian, African American, and Asian children andadults. Lupus 18(1):61-6, 2009.Rich, Elizabeth MD, PhD* # Stock W,Undevia SD,Bivins C,Ravandi F,Odenike O,Faderl S,RichE,Borthakur G,Godley L,Verstovsek S,Artz A,Wierda W,Larson RA,ZhangY,Cortes J,Ratain MJ,Giles FJ. A phase I and pharmacokinetic study of XK469R(NSC 698215), a quinoxaline phenoxypropionic acid derivative, in patients withrefractory acute leukemia. Invest New Drugs 26(4):331-8, 2008.* # Gordon MK, Sher D, Karrison T, Kebriaei P, Chuang K, Zhang Y,McDonnell D, Artz A, Godley L, Odenike O, Rich E, Michaelis L, ThirmanMJ, Wickrema A, van Besien K, Larson RA, Stock W. Successful autologousstem cell collection in patients with chronic myeloid leukemia in completecytogenetic response, with quantitative measurement of BCR-ABL expressionin blood, marrow, and apheresis products. Leuk Lymphoma 49(3):531-7, 2008.* Artz AS, Wickrema A, Dinner S, Godley LA, Kocherginsky M, Odenike O,Rich ES, Stock W, Ulaszek J, Larson RA, van Besien K. Pretreatment C-reactiveprotein is a predictor for outcomes after reduced-intensity allogeneichematopoietic cell transplantation. Biol Blood Marrow Transplant 14(11):1209-16, 2008.* Dew A, Collins D, Artz A, Rich E, Stock W, Swanson K, van Besien K. Paucityof HLA-identical unrelated donors for African-Americans with hematologicmalignancies: the need for new donor options. Biol Blood Marrow Transplant14(8):938-41, 2008.* Rosenbaum C, Peace D, Rich E, Van Besien K. Granulocyte colonystimulatingfactor-based stem cell mobilization in patients with sickle celldisease. Biol Blood Marrow Transplant 14(6):719-23, 2008.Arai S, Meagher R, Swearingen M, Myint H, Rich E, Martinson J, KlingemannH. Infusion of the allogeneic cell line NK-92 in patients with advanced renalcell cancer or melanoma: a phase I trial. Cytotherapy 10(6):625-32, 2008.* # Poire X, Artz A, Larson RA, Kline J, Odenike O, Rich E, Godley L, Stock W,van Besien K. Allogeneic stem cell transplantation with alemtuzumab-basedconditioning for patients with advanced chronic myelogenous leukemia. LeukLymphoma 50(1):85-91, 2009.Rowley, Janet MD, DSc* Li Z, Lu J, Sun M, Mi S, Zhang H, Luo RT, Chen P, Wang Y, Yan M, Qian Z,Neilly MB, Jin J, Zhang Y, Bohlander SK, Zhang DE, Larson RA, Le Beau MM,Thirman MJ, Golub TR, Rowley JD, Chen J. Distinct microRNA expressionprofiles in acute myeloid leukemia with common translocations. Proc NatlAcad Sci U S A 105(40):15535-40, 2008.Murmann AE, Mincheva A, Scheuermann MO, Gautier M, Yang F, Buitkamp J,Strissel PL, Strick R, Rowley JD, Lichter P. Comparative gene mapping in cattle,Indian muntjac, and Chinese muntjac by fluorescence in situ hybridization.Genetica 134(3):345-51, 2008.Rowley JD, Blumenthal T. Medicine. The cart before the horse. Science321(5894):1302-4, 2008.Kim YC, Wu Q, Chen J, Xuan Z, Jung YC, Zhang MQ, Rowley JD, Wang SM.The transcriptome of human CD34+ hematopoietic stem-progenitor cells. ProcNatl Acad Sci U S A 106(20):8278-83, 2009.Popovic R, Riesbeck LE, Velu CS, Chaubey A, Zhang J, Achille NJ, ErfurthFE, Eaton K, Lu J, Grimes HL, Chen J, Rowley JD, Zeleznik-Le NJ. Regulationof mir-196b by MLL and its overexpression by MLL fusions contributes toimmortalization. Blood 113(14):3314-22, 2009.* Li Z, Luo RT, Mi S, Sun M, Chen P, Bao J, Neilly MB, Jayathilaka N, JohnsonDS, Wang L, Lavau C, Zhang Y, Tseng C, Zhang X, Wang J, Yu J, Yang H,Wang SM, Rowley JD, Chen J, Thirman MJ. Consistent deregulation of geneexpression between human and murine MLL rearrangement leukemias. CancerRes 69(3):1109-16, 2009.Rowley JD. Chromosomal translocations: revisited yet again. Blood 112(6):2183-9, 2008.Singh, Harinder PhDLaslo P, Pongubala JM, Lancki DW, Singh H. Gene regulatory networksdirecting myeloid and lymphoid cell fates within the immune system. SeminImmunol 20(4):228-35, 2008.Singh H. PU.1, a shared transcriptional regulator of innate and adaptiveimmune cell fates. J Immunol 181(3):1595-6, 2008.Reddy KL, Singh H. Using molecular tethering to analyze the role of nuclearcompartmentalization in the regulation of mammalian gene activity. Methods45(3):242-51, 2008.Reynaud D, Demarco IA, Reddy KL, Schjerven H, Bertolino E, Chen Z,Smale ST, Winandy S, Singh H. Regulation of B cell fate commitment andimmunoglobulin heavy-chain gene rearrangements by Ikaros. Nat Immunol9(8):927-36, 2008.Johnson K, Hashimshony T, Sawai CM, Pongubala JM, Skok JA, Aifantis I,Singh H. Regulation of immunoglobulin light-chain recombination by thetranscription factor IRF-4 and the attenuation of interleukin-7 signaling.Immunity 28(3):335-45, 2008.Reddy KL, Zullo JM, Bertolino E, Singh H. Transcriptional repression mediatedby repositioning of genes to the nuclear lamina. Nature 452(7184):243-7, 2008.Pongubala JM, Northrup DL, Lancki DW, Medina KL, Treiber T, BertolinoE, Thomas M, Grosschedl R, Allman D, Singh H. Transcription factor EBFrestricts alternative lineage options and promotes B cell fate commitmentindependently of Pax5. Nat Immunol 9(2):203-15, 2008.Sipkins, Dorothy MD, PhDColmone A, Sipkins DA. Beyond angiogenesis: the role of endothelium in thebone marrow vascular niche. Transl Res 151(1):1-9, 2008.Colmone A, Amorim M, Pontier AL, Wang S, Jablonski E, Sipkins DA.Leukemic cells create bone marrow niches that disrupt the behavior of normalhematopoietic progenitor cells. Science 322(5909):1861-5, 2008.Sipkins DA. Chemotherapy and the bone marrow stroma. Leuk Lymphoma49(1):17-8, 2008.Smith, Sonali MD* # Rosen DS, Smith S, Gurbuxani S, Yamini B. Extranodal hairy cell leukemiapresenting in the lumbar spine. J Neurosurg Spine 9(4):374-6, 2008.Kenkre VP, Smith SM. Management of relapsed diffuse large B-cell lymphoma.Curr Oncol Rep 10(5):393-403, 2008.* Smith SM, van Besien K, Carreras J, Bashey A, Cairo MS, Freytes CO, GaleRP, Hale GA, Hayes-Lattin B, Holmberg LA, Keating A, Maziarz RT, McCarthyPL, Navarro WH, Pavlovsky S, Schouten HC, Seftel M, Wiernik PH, Vose JM,Lazarus HM, Hari P. Second autologous stem cell transplantation for relapsedlymphoma after a prior autologous transplant. Biol Blood Marrow Transplant14(8):904-12, 2008.Smith S. Anti-Bcl2 therapy in chronic myelogenous leukemia. Leuk Lymphoma49(7):1232-3, 2008.Smith SM, Grinblatt D, Johnson JL, Niedzwiecki D, Rizzieri D, Bartlett NL,Cheson BD. Thalidomide has limited single-agent activity in relapsed orrefractory indolent non-Hodgkin lymphomas: a phase II trial of the Cancer andLeukemia Group B. Br J Haematol 140(3):313-9, 2008.Stock, Wendy MD* # Stock W,Undevia SD,Bivins C,Ravandi F,Odenike O,Faderl S,RichE,Borthakur G,Godley L,Verstovsek S,Artz A,Wierda W,Larson RA,ZhangY,Cortes J,Ratain MJ,Giles FJ. A phase I and pharmacokinetic study of XK469R(NSC 698215), a quinoxaline phenoxypropionic acid derivative, in patients withrefractory acute leukemia. Invest New Drugs 26(4):331-8, 2008.* # Gordon MK, Sher D, Karrison T, Kebriaei P, Chuang K, Zhang Y,McDonnell D, Artz A, Godley L, Odenike O, Rich E, Michaelis L, ThirmanMJ, Wickrema A, van Besien K, Larson RA, Stock W. Successful autologousstem cell collection in patients with chronic myeloid leukemia in completecytogenetic response, with quantitative measurement of BCR-ABL expressionin blood, marrow, and apheresis products. Leuk Lymphoma 49(3):531-7, 2008.40UCCRC SCIENTIFIC REPORT 2009
* Klisovic RB, Stock W, Cataland S, Klisovic MI, Liu S, Blum W, Green M,Odenike O, Godley L, Burgt JV, Van Laar E, Cullen M, Macleod AR, BestermanJM, Reid GK, Byrd JC, Marcucci G. A phase I biological study of MG98, anoligodeoxynucleotide antisense to DNA methyltransferase 1, in patientswith high-risk myelodysplasia and acute myeloid leukemia. Clin Cancer Res14(8):2444-9, 2008.* # Odenike OM, Larson RA, Gajria D, Dolan ME, Delaney SM, Karrison TG,Ratain MJ, Stock W. Phase I study of the ribonucleotide reductase inhibitor3-aminopyridine-2-carboxaldehyde-thiosemicarbazone (3-AP) in combinationwith high dose cytarabine in patients with advanced myeloid leukemia. InvestNew Drugs 26(3):233-9, 2008.Rizzieri DA, Feldman E, Dipersio JF, Gabrail N, Stock W, Strair R, Rivera VM,Albitar M, Bedrosian CL, Giles FJ. A phase 2 clinical trial of deforolimus(AP23573, MK-8669), a novel mammalian target of rapamycin inhibitor, inpatients with relapsed or refractory hematologic malignancies. Clin Cancer Res14(9):2756-62, 2008.* Stock W, La M, Sanford B, Bloomfield CD, Vardiman JW, Gaynon P,Larson RA, Nachman J. What determines the outcomes for adolescents andyoung adults with acute lymphoblastic leukemia treated on cooperativegroup protocols? A comparison of Children’s Cancer Group and Cancer andLeukemia Group B studies. Blood 112(5):1646-54, 2008.* # Odenike OM, Alkan S, Sher D, Godwin JE, Huo D, Brandt SJ, Green M,Xie J, Zhang Y, Vesole DH, Stiff P, Wright J, Larson RA, Stock W. Histonedeacetylase inhibitor romidepsin has differential activity in core binding factoracute myeloid leukemia. Clin Cancer Res 14(21):7095-101, 2008.Thirman, Michael MD* Li Z, Lu J, Sun M, Mi S, Zhang H, Luo RT, Chen P, Wang Y, Yan M, Qian Z,Neilly MB, Jin J, Zhang Y, Bohlander SK, Zhang DE, Larson RA, Le Beau MM,Thirman MJ, Golub TR, Rowley JD, Chen J. Distinct microRNA expressionprofiles in acute myeloid leukemia with common translocations. Proc NatlAcad Sci U S A 105(40):15535-40, 2008.* # Gordon MK, Sher D, Karrison T, Kebriaei P, Chuang K, Zhang Y,McDonnell D, Artz A, Godley L, Odenike O, Rich E, Michaelis L, ThirmanMJ, Wickrema A, van Besien K, Larson RA, Stock W. Successful autologousstem cell collection in patients with chronic myeloid leukemia in completecytogenetic response, with quantitative measurement of BCR-ABL expressionin blood, marrow, and apheresis products. Leuk Lymphoma 49(3):531-7, 2008.Chen J, Santillan DA, Koonce M, Wei W, Luo R, Thirman MJ, Zeleznik-LeNJ, Diaz MO. Loss of MLL PHD finger 3 is necessary for MLL-ENL-inducedhematopoietic stem cell immortalization. Cancer Res 68(15):6199-207, 2008.* Li Z, Luo RT, Mi S, Sun M, Chen P, Bao J, Neilly MB, Jayathilaka N, JohnsonDS, Wang L, Lavau C, Zhang Y, Tseng C, Zhang X, Wang J, Yu J, Yang H,Wang SM, Rowley JD, Chen J, Thirman MJ. Consistent deregulation of geneexpression between human and murine MLL rearrangement leukemias. CancerRes 69(3):1109-16, 2009.van Besien, Koen MD* Artz AS, Wickrema A, Dinner S, Godley LA, Kocherginsky M, Odenike O,Rich ES, Stock W, Ulaszek J, Larson RA, van Besien K. Pretreatment C-reactiveprotein is a predictor for outcomes after reduced-intensity allogeneichematopoietic cell transplantation. Biol Blood Marrow Transplant 14(11):1209-16, 2008.# Kline J, Subbiah S, Lazarus HM, van Besien K. Autologous graft-versus-hostdisease: harnessing anti-tumor immunity through impaired self-tolerance.Bone Marrow Transplant 41(6):505-13, 2008.Flowers ME, Apperley JF, van Besien K, Elmaagacli A, Grigg A, Reddy V,Bacigalupo A, Kolb HJ, Bouzas L, Michallet M, Prince HM, Knobler R, ParentiD, Gallo J, Greinix HT. A multicenter prospective phase 2 randomized studyof extracorporeal photopheresis for treatment of chronic graft-versus-hostdisease. Blood 112(7):2667-74, 2008.van Besien KW. Superiority of reduced-intensity conditioning for Hodgkin’slymphoma. J Clin Oncol 26(24):4045-6, 2008.van Besien K, Carreras J, Bierman PJ, Logan BR, Molina A, King R, NelsonG, Fay JW, Champlin RE, Lazarus HM, Vose JM, Hari PN. Unrelated donorhematopoietic cell transplantation for non-hodgkin lymphoma: long-termoutcomes. Biol Blood Marrow Transplant 15(5):554-63, 2009.Martin PJ, Storer BE, Rowley SD, Flowers ME, Lee SJ, Carpenter PA, WingardJR, Shaughnessy PJ, DeVetten MP, Jagasia M, Fay JW, van Besien K, GuptaV, Kitko C, Johnston LJ, Maziarz RT, Arora M, Jacobson PA, Weisdorf D.Evaluation of mycophenolate mofetil for initial treatment of chronic graftversus-hostdisease. Blood 113(21):5074-82, 2009.Devetten MP, Hari PN, Carreras J, Logan BR, van Besien K, Bredeson CN,Freytes CO, Gale RP, Gibson J, Giralt SA, Goldstein SC, Gupta V, MarksDI, Maziarz RT, Vose JM, Lazarus HM, Anderlini P. Unrelated donorreduced-intensity allogeneic hematopoietic stem cell transplantationfor relapsed and refractory Hodgkin lymphoma. Biol Blood MarrowTransplant 15(1):109-17, 2009.Vardiman, James MD* Ozer O, Zhao YD, Ostler KR, Akin C, Anastasi J, Vardiman JW, GodleyLA. The identification and characterisation of novel KIT transcriptsin aggressive mast cell malignancies and normal CD34+ cells. LeukLymphoma 49(8):1567-77, 2008.* Stock W, La M, Sanford B, Bloomfield CD, Vardiman JW, Gaynon P,Larson RA, Nachman J. What determines the outcomes for adolescentsand young adults with acute lymphoblastic leukemia treated oncooperative group protocols? A comparison of Children’s Cancer Groupand Cancer and Leukemia Group B studies. Blood 112(5):1646-54, 2008.Pullarkat ST, Vardiman JW, Slovak ML, Rao DS, Rao NP, Bedell V, SaidJW. Megakaryocytic blast crisis as a presenting manifestation of chronicmyeloid leukemia. Leuk Res 32(11):1770-5, 2008.* Grinblatt DL, Yu D, Hars V, Vardiman JW, Powell BL, Nattam S,Silverman LR, de Castro C 3rd, Stone RM, Bloomfield CD, Larson RA.Treatment of myelodysplastic syndrome with 2 schedules and doses oforal topotecan: a Randomized Phase 2 Trial by the Cancer and LeukemiaGroup B (CALGB 19803). Cancer 115(1):84-93, 2009.Tefferi A, Vardiman JW. Classification and diagnosis ofmyeloproliferative neoplasms: the, 2008 World Health Organizationcriteria and point-of-care diagnostic algorithms. Leukemia 22(1):14-22,2008.Wickrema, Amittha PhDZhou L, Nguyen AN, Sohal D, Ying Ma J, Pahanish P, Gundabolu K,Hayman J, Chubak A, Mo Y, Bhagat TD, Das B, Kapoun AM, NavasTA, Parmar S, Kambhampati S, Pellagatti A, Braunchweig I, Zhang Y,Wickrema A, Medicherla S, Boultwood J, Platanias LC, Higgins LS.Inhibition of the TGF-beta receptor I kinase promotes hematopoiesis inMDS. Blood 112(8):3434-43, 2008.* Zhou Y, Uddin S, Zimmerman T, Kang JA, Ulaszek J, Wickrema A.Growth control of multiple myeloma cells through inhibition of glycogensynthase kinase-3. Leuk Lymphoma 49(10):1945-53, 2008.* Kang JA, Zhou Y, Weis TL, Liu H, Ulaszek J, Satgurunathan N, ZhouL, van Besien K, Crispino J, Verma A, Low PS, Wickrema A. Osteopontinregulates actin cytoskeleton and contributes to cell proliferation inprimary erythroblasts. J Biol Chem 283(11):6997-7006, 2008.Patterson ST, Li J, Kang JA, Wickrema A, Williams DB, ReithmeierRA. Loss of specific chaperones involved in membrane glycoproteinbiosynthesis during the maturation of human erythroid progenitor cells.J Biol Chem 284(21):14547-57, 2009.Redig AJ, Sassano A, Majchrzak-Kita B, Katsoulidis E, Liu H, Altman JK,Fish EN, Wickrema A, Platanias LC. Activation of Protein Kinase Cη byType I Interferons. J Biol Chem 284(16):10301-14, 2009.Yamamoto ML, Clark TA, Gee SL, Kang JA, Schweitzer AC, WickremaA, Conboy JG. Alternative pre-mRNA splicing switches modulate geneexpression in late erythropoiesis. Blood 113(14):3363-70, 2009.Zhang, Yanming MD* # Stock W, Undevia SD, Bivins C, Ravandi F, Odenike O, Faderl S, RichE, Borthakur G, Godley L, Verstovsek S, Artz A, Wierda W, Larson RA,Zhang Y, Cortes J, Ratain MJ, Giles FJ. A phase I and pharmacokineticstudy of XK469R (NSC 698215), a quinoxaline phenoxypropionic acidderivative, in patients with refractory acute leukemia. Invest New Drugs26(4):331-8, 2008.* Li Z, Lu J, Sun M, Mi S, Zhang H, Luo RT, Chen P, Wang Y, Yan M,Qian Z, Neilly MB, Jin J, Zhang Y, Bohlander SK, Zhang DE, LarsonRA, Le Beau MM, Thirman MJ, Golub TR, Rowley JD, Chen J. DistinctmicroRNA expression profiles in acute myeloid leukemia with commontranslocations. Proc Natl Acad Sci U S A 105(40):15535-40, 2008.Molecular Genetics& HematopoiesisUCCRC SCIENTIFIC REPORT 200941
* # Gordon MK, Sher D, Karrison T, Kebriaei P, Chuang K, Zhang Y,McDonnell D, Artz A, Godley L, Odenike O, Rich E, Michaelis L, ThirmanMJ, Wickrema A, van Besien K, Larson RA, Stock W. Successful autologousstem cell collection in patients with chronic myeloid leukemia in completecytogenetic response, with quantitative measurement of BCR-ABL expressionin blood, marrow, and apheresis products. Leuk Lymphoma 49(3):531-7, 2008.* # Odenike OM, Alkan S, Sher D, Godwin JE, Huo D, Brandt SJ, Green M,Xie J, Zhang Y, Vesole DH, Stiff P, Wright J, Larson RA, Stock W. Histonedeacetylase inhibitor romidepsin has differential activity in core bindingfactor acute myeloid leukemia. Clin Cancer Res 14(21):7095-101, 2008.* Li Z, Luo RT, Mi S, Sun M, Chen P, Bao J, Neilly MB, Jayathilaka N, JohnsonDS, Wang L, Lavau C, Zhang Y, Tseng C, Zhang X, Wang J, Yu J, Yang H,Wang SM, Rowley JD, Chen J, Thirman MJ. Consistent deregulation of geneexpression between human and murine MLL rearrangement leukemias.Cancer Res 69(3):1109-16, 2009.Zimmerman, Todd MD* Zhou Y, Uddin S, Zimmerman T, Kang JA, Ulaszek J, Wickrema A. Growthcontrol of multiple myeloma cells through inhibition of glycogen synthasekinase-3. Leuk Lymphoma 49(10):1945-53, 2008.Chanan-Khan AA, Niesvizky R, Hohl RJ, Zimmerman TM, Christiansen NP,Schiller GJ, Callander N, Lister J, Oken M, Jagannath S. Phase III randomisedstudy of dexamethasone with or without oblimersen sodium for patients withadvanced multiple myeloma. Leuk Lymphoma 50(4):559-65,, 2009.42UCCRC SCIENTIFIC REPORT 2009
Selected Major Grants and AwardsThe Molecular Genetics and Hematopoiesis Program has a funding base of $9,097,675 in annual total costs (current as of July2009). This sum includes $3,088,137 in NCI funding and $670,795 in other NIH funding. Due to space constraints, only newawards presented since January 1, 2008 with funding of $100,000 or more in annual total costs are listed here.Investigator Title Start DateLe Beau, MichelleThirman, MichaelKee, BarbaraChen, JianjunChen, JianjunSmith, SonaliLe Beau, MichelleRowley, JanetGounari, FotiniLarson, RichardEtiology of Alkylator-Induced MyeloidLeukemiaPeptide and Small MoleculeTherapeutics for HematologicMalignanciesRegulation of LymphocyteDevelopment by HLH ProteinsThe Role and Functional Mechanismof a miRNA Cluster, mir-17-92 inLeukemogenesis3UTR Variation of MicroRNA TargetsDuring Stem Cell Differentiation andHematopoiesisA Phase 1/2a Open-Label Studyof Praletrexate and Gemcitabinewith Vitamin B12 and Folic AcidSupplementation in Patientswith Relapsed or RefractoryLymphoproliferative MalignanciesMechanisms of TreatmentResponsiveness and Resistance inMyeloid MalignanciesComparisons of Microarray andMicroRNA for Diagnosis andPrognosisWnt/b-Catenin Signaling in T-CellTransformationA Multi-Center, Open Label, SingleArm Study of Weekly Alvocidib inPatients with Previously TreatedB-Cell Chronic LymphocyticLeukemia (CLL) or ProlymphocyticLeukemia (PLL) Arising from CLLEndDateAnnualTotal CostClassFunding Agency9/1/2008 8/31/2013 $1,667,989 PO1 National Cancer Institute10/1/2006 9/30/2011 $1,050,000 N/AThe Leukemia & LymphomaSociety7/3/2008 5/31/2013 $292,163 R01 National Cancer Institute6/1/2008 4/30/2013 $286,661 R01 National Cancer Institute7/1/2008 6/30/2011 $275,000 N/AMathers CharitableFoundation7/17/2008 7/16/2010 $241,344 N/A Allos Therrapeutics, Inc.10/1/2008 9/30/2013 $229,500 SCOR10/1/2008 9/30/2011 $200,000 N/AThe Leukemia & LymphomaSocietyThe Leukemia & LymphomaSociety5/1/2008 4/30/2010 $191,875 R21 National Institutes of Health4/14/2008 4/13/2010 $178,500 N/A Sanofi-Aventis U.S. Inc.Le Beau, Michelle Institutional Research Grant 1/1/2009 12/31/2011 $120,000 58 American Cancer SocietyGodley, LucyA Phase I, Multi-Dose Study ofSGN-33 (antiCD33 mAB, HuM195,lintuzumab) in Patients with6/25/2008 6/24/2010 $120,000 N/A Seattle Genetics, Inc.Acute Myeloid Leukemia andMyelodysplastic SyndromeStock, WendyA Phase 2/3 Study to Evaluate theSafety & Efficacy of Lumiliximabin Combination with Fludarabine,Cyclosphosphamide, and RituximabVs. Fludarabine, Cyclophosphamide,and Rituximab Alone in Subjectsw/Relapsed Chronic LymphocyticLukemia8/8/2008 8/7/2010 $116,000 N/A Biogen Idec Inc.Kee, BarbaraSmith, SonaliTranscriptional Deregulation andLymphocyte TransformationPhase I Dose-Escalation Study ofBruton's Tyrosine Kinase (Btk)Inhibitor PCI-32765 in Recurrent BCell Lymphoma7/1/2008 6/30/2013 $110,000 N/AThe Leukemia & LymphomaSociety10/30/2008 12/31/2009 $104,137 N/A Pharmacyclics, Inc.Molecular Genetics& HematopoiesisUCCRC SCIENTIFIC REPORT 200943
Program 3Immunology and CancerScanning electron microscope image from normal circulating human blood showing red blood cells andwhite blood cells, including lymphocytes, a monocyte, a neutrophil, and many small disc-shaped platelets.(Image by B. Wetzel and H. Schaefer, National Cancer Institute)
The Program has evolved into an important example ofbi-directional translational research, with ideas movingfreely between bench and bedside.Overview & GoalsThe overall goals of the Immunology and CancerProgram are to understand the interface betweenthe host immune system and malignant tumorsand, ultimately, to manipulate the interaction topromote immune-mediated tumor destruction inpatients with cancer. The Program has evolvedinto an important example of bi-directionaltranslational research, with ideas moving freelybetween bench and bedside, and consists of 21members (one of whom is a Howard Hughesinvestigator) derived from 6 departments.therefore, span the following domains: (1)fundamental investigations in immunology thathave relevance to the cancer context; (2) mousemodels of anti-tumor immunity; and (3) clinicalstudies of human anti-tumor immunity and novelimmunotherapies. Observations made in studiesof basic immunologic concepts direct the design ofpreclinical and clinical investigations, and resultsof clinical studies generate new hypotheses thatare being addressed back in murine systems.Immunology& CancerThe Immunology and Cancer Program aimsto understand all definable aspects of immuneresponse against tumors, which will be vitalfor developing and optimizing immune-basedcancer therapeutics. The scientific goals,Program Leader:Thomas Gajewski, MD, PhDUCCRC SCIENTIFIC REPORT 200945
MembersInvestigator*Erin Adams PhDMaria-Luisa Alegre MD, PhDAlbert Bendelac MD, PhDAnita Chong PhDMarcus Clark MDYang-Xin Fu MD, PhDThomas Gajewski MD, PhDTatyana Golovkina PhDJose Guevara-Patino MD, PhDBana Jabri MD, PhDJustin Kline MDVinay Kumar MD, PhDMaciej Lesniak MDMark McKee MDVu Nguyen MDGlenn Randall PhDRaymond Roos MDHans Schreiber MD, PhDAnne Sperling PhDUrsula Storb MDPing Yu MDJian Zhang MDRankAssistant ProfessorAssociate ProfessorProfessorProfessorProfessorProfessorAssociate ProfessorAssociate ProfessorAssistant ProfessorAssociate ProfessorAssistant ProfessorProfessorAssociate ProfessorAssociate ProfessorAssistant ProfessorAssistant ProfessorProfessorProfessorAssociate ProfessorProfessorInstructorAssistant ProfessorDepartmentBiochemistry and Molecular BiologyMedicinePathologySurgeryMedicinePathologyPathologyMicrobiologySurgeryMedicineMedicinePathologySurgerySurgeryMedicineMicrobiologyNeurologyPathologyMedicineMolecular Genetics and Cell BiologyPathologyMedicine46UCCRC SCIENTIFIC REPORT 2009* Reflects all Program membership during 2008-2009
Featured Faculty Research Summaries †Research themes in the Immunology and Cancer Program represent a spectrum oftopics in fundamental immunology, preclinical models of tumor immunology, andimmunotherapy clinical trials. Although a major focus of the general cancer immunologycommunity has been on adaptive T cell responses against tumor antigens and how toincrease their frequency and efficacy, this program has expanded efforts to investigateinnate immunity as it relates to host awareness of tumor presence. The interfacebetween the innate and adaptive segments of the immune system likely is a majordetermining factor dictating whether immune-mediated tumor control is successful. Inaddition, our program has focused significantly on understanding features of the tumormicroenvironment as they relate to the success versus failure of immune-mediated tumordestruction. Highlights for some major research themes are outlined below.Fundamental ImmunologyAlbert Bendelac, MD, PhDProfessor of PathologyImmunology& CancerDr. Bendelac studies a subset of T cells called NKTcells. NKT cells are viewed to be a component of theinnate immune system in that they express a memorylikesurface phenotype in the periphery and canrapidly produce effector cytokines without need of adifferentiation step following activation. Dr. Bendelac’slaboratory has made multiple seminal observationson the biology of NKT cells. His group has used novelapproaches to identify the ligands of the invariant NKTcell T cell receptor. Specifically, this TCR recognizesglycolipid antigens presented by CD1d molecules. Suchligands can be derived from pathogen-infected tissues,or by upregulated expression of normal products inself-tissues. It is thought that the latter represents themechanism by which NKT cells can become activated by tumor cells.Use of the UCCRC’s Leica SP5 AOBS spectral 2-photon confocalmicroscope, designed for live cell imaging.Recently, the Bendelac team has deciphered key mechanisms that govern the development of the NKT cell subset.Using gene expression profiling and confirmatory approaches, the transcription factor PLZF has been found tobe necessary for NKT cell development. PLZF-deficient mice failed to expand and differentiate NKT cells in thethymus. Interestingly, it also has been observed that PLZF regulates the development of a subset of γδ T cells thathave an innate-type phenotype. Together, these data have identified a specific transcriptional program that directsthe development of subsets of T cells having an innate signature. These results increase our understanding of NKTcell biology that should guide further interrogation into their role in anti-tumor immune responses.Erin Adams, PhDAssistant Professor of Biochemistry and Molecular BiologyThe research in Dr. Adams’ laboratory focuses on studying the molecular principles of immune recognition,particularly in a subset of T cells called γδ T cells. Although they can express a diverse repertoire of T cell receptors(TCRs), γδ cells are viewed as part of the innate immune system. These cells predominate in the epithelial tissuesand, in some cases, have the ability to directly recognize and lyse tumor cells. The laboratory seeks to understandimmune cell receptor-mediated signaling responsible for the discrimination of self versus non-self, and the factorsthat contribute to either enhanced auto-reactivity (auto-immune diseases) or those used by pathogens or tumors toevade immune detection. In contrast to the more abundant αβ T cells which express an αβ TCR, γδ T cells probetheir environment through a structurally similar, yet distinct, γδ TCR. Although many of the antigens for antibodies† Note: Due to space constraints, only a small representative sample of Program members is presented here.UCCRC SCIENTIFIC REPORT 200947
and αβ TCRs are well known, the ligands recognized by γδ TCRs as antigenic determinants remain much of a mystery. Inaddition, whether the diversity generated by the rearrangement process is even necessary for antigen recognition by thesereceptors remains unclear. For known ligands, the molecular details of antigenic recognition are still unknown. The Adamslaboratory seeks to define the role(s) of these cells in the immune response, specifically against cancer, by 1) defining the ligandsthey recognize in these tissues; and 2) understanding the molecular details of γδ TCR ligand recognition and how this is alteredin self/non-self discrimination.A major set of projects pursued in the lab focuses on γδ TCR recognition of nonclassical MHC molecules. The γδ T cellpopulation that recognizes T22 shares a simple motif in one of the antigen recognition loops of its TCRs: Trp (W) followed by aconserved EGYEL block of amino acids. Across the TCRs examined, there is variation in the number and nature of amino acidresidues between the W and EGYEL. Dr. Adams has previously shown how one of the T22 reactive TCRs uses this motif to bindto T22. By solving the three dimensional structure of the G8 γδ TCR with T22, the majority of the binding interface between theTCR and T22 was shown to involve the CDR3d loop that contains the W…EGYEL motif. Furthermore, the study demonstratedthat transferring the CDR3d loop, from these T22 reactive γδ TCRs to a naïve αβ TCR (used as a scaffold), endowed the scaffoldwith T22 binding ability, with affinities greater than that of the wildtype TCRs.The Adams laboratory is also studying three γδ TCRs that bind to the human nonclassical major histocompatibility complex(MHC) molecule, CD1c. Unlike T22, which does not bind and present a variable ligand, CD1c binds a variety of lipid molecules.These lipids are anchored in the CD1c molecule by their lipid tails, which are accommodated in hydrophobic “tunnels” buriedin the CD1c core. The head groups of the lipids, which come from a variety of sources, are exposed to the outer solvent and,presumably, the TCRs that bind to this surface. The laboratory is currently pursuing the three dimensional structure of CD1cand defining the lipid antigens that are recognized as antigenic determinants by γδ TCRs.Together, these fundamental studies on NKT cells and γδ T cells are increasing our understanding of the development,function, and receptor-mediated activation of these less- abundant, though critically important, lymphocyte subsets from theinnate immune system. These biologic principles will guide studies of innate recognition of tumors in other model systems, andultimately should point to new opportunities for therapeutic intervention.In Vivo Tumor ImmunologyHans Schreiber, MD, PhDProfessor of PathologyDr. Schreiber’s laboratory focuses research efforts onunderstanding the roles of tumor stromal cell elements, bothin supporting tumor growth and in mediating resistance toimmune-mediated tumor rejection. Using mouse models, Dr.Schreiber’s group was among the first to demonstrate that asubset of myeloid-lineage cells was important to aid in the growthof implanted tumors, and that depletion of these Gr1 + cells couldresult in tumor regression. Another critical discovery from theSchreiber laboratory is the observation that for T cells to beable to reject a tumor in vivo, tumor antigens need to be “crosspresented”by host antigen presenting cells. While this mightbe important for the initial priming and activation of anti-tumor T cells, it also could participate at the effector phase of theanti-tumor immune response. In fact, the Schreiber group has shown that adoptively transferred tumor antigen-specific T cells,when they work effectively, must kill both the tumor cells and the stromal cell elements within the tumor microenvironment.This has been a paradigm-shifting observation that is changing the way people think about T cell-mediated tumor destruction.Using this adoptive T cell transfer system as a model, the Schreiber laboratory has more recently deciphered the mechanismsby which effective tumor elimination occurs. Indeed, they have observed that immune-mediated elimination of tumor stromal48UCCRC SCIENTIFIC REPORT 2009
cells depends on IFN-γ and TNF, and that the stromal cells themselves must express receptors for these cytokines. Therefore,this “bystander killing” of the tumor through destruction of stromal cells in the tumor microenvironment is cytokinemediated.Together, these results argue for the importance of stromal cells in supporting tumor growth and indicate the utility intargeting stromal cells as a component of immunotherapeutic interventions. They also suggest that the interaction betweenT cells and stromal cells in human anti-tumor immune responses should be similarly investigated in cancer patients.Yang-Xin Fu, MD, PhDProfessor of PathologyCross-talk between immune cells and stromal cells can establish a microenvironment that is necessary for lymphoid tissuedevelopment, central and peripheral tolerance, and efficient migration of immune responses. However, little is knownabout the molecular mechanisms that underlie the interactions between lymphocytes and stromal cells. Dr. Fu proposesthat lymphotoxin (LT) from T cells and LTβR on stromal cells establishes a lymphoid microenvironment for cross-talk andefficient and self-contained immune responses. More specifically, a set of distinct adhesion molecules and tissue chemokinesfrom stromal cells are regulated by lymphocytes for a flexible, delicate, and rapid immune response inside and outsidelymphoid tissues. Studies in the Fu laboratory have revealed that lymphotoxin, tumor necrosis factor (TNF), and LIGHT(another ligand for LT receptor) are key cytokines for establishing organized lymphoid structures inside and outside lymphoidorgans/tissues critical for the organization of immune responses. Through gene targeting and antibody stimulation/blockadeof LT/LIGHT core family members on different lymphocytes, the Fu group has revealed the contribution of the LT/LIGHTpathway in the formation of primary and secondary lymphoid tissues and the development of various immune responses atthe cellular and molecular level. These molecular pathways can be applied to the tumor context to generate potent antitumorimmune responses that are capable of promoting complete tumor rejection in vivo.Immunology& CancerOne issue in anti-tumor immunity is that lack of effective infiltration of immune cells and proper expression of costimulatorymolecules prevents effective immune response against established tumors. Understanding of the biology ofLIGHT has enabled the Fu group to study the creation of a lymphoid-like microenvironment as a new strategy to promotetumor control. When expressed in the tumor microenvironment, LIGHT signals via the LTβR on stromal cells which attractsT cells and other immune cells into tumor sites. In addition, LIGHT co-activates T cells via a second receptor, HVEM.Together, these signals cause the development of lymphoid-like structures within those tumors, which allows activationof tumor-specific T cells and promotes tumor destruction. The Fu laboratory is currently focusing on different deliverysystems to target LIGHT to tumor sites. These include adenoviral vectors for intratumoral injection, and coupling LIGHTto monoclonal antibodies. Combination strategies integrating LIGHT expression with conventional cancer therapeutics alsoare being explored. Optimal strategies that are most effective in mice will be moved forward into clinical application.Clinical/Translational Cancer ImmunologyThomas Gajewski, MD, PhDAssociate Professor of Pathology and MedicineDr. Gajewski’s research team studies fundamental aspects of T cell regulation as theyare relevant for the cancer context, applies this information towards preclinical modelsof anti-tumor immunity, and then uses this information to guide the development ofnew immunotherapeutic approaches in cancer patients. The team has developed avaccine approach utilizing tumor antigen peptides combined with the cytokine IL-12.This approach has progressed from mouse preclinical experiments through phase I andphase II clinical trials in patients with advanced melanoma. Clinically, vaccination hasresulted in a response rate of approximately 10% and stable disease rate of 20%. Becausenot all patients respond to this therapy, intensive investigations have been pursued toidentify biologic characteristics of patients and tumors that may be associated withclinical benefit. Pre-treatment tumor biopsy gene expression profiling has identified aDr. Thomas GajewskiUCCRC SCIENTIFIC REPORT 200949
transcriptional profile in the tumor site that is associated with response versus resistance to active immunization. This analysishas revealed new key steps in the anti-tumor immune response that may dictate whether anti-tumor T cells can succeed incausing tumor rejection. These new concepts are being studied in preclinical models, and those studied have revealed newapproaches that are being moved forward back into clinical application.The above gene expression profiling experiments have indicated three levels of barrier that could govern efficacy of anti-tumorimmune responses. First, some tumors show evidence of innate immune activation centered on type I IFNs, which is associatedwith the presence of activated T cells. Mouse experiments have confirmed that host type I IFNs are necessary for spontaneouspriming of anti-tumor T cells. Therefore, intratumoral application of type I IFNs may represent an attractive strategy to moveforward clinically. Second, only a subset of tumors express chemokines that are capable of recruiting activated T cells intothe tumor microenvironment. Tumors that lack chemokines are poor at attracting appropriately activated T cells into tumorsites and, thus, can be resistant to immune-mediated attack. Therefore, strategies to induce chemokine production withintumor sites also are attractive to consider for clinical translation. Third, tumors that do show evidence of inflammation andsuccessfully attract activated T cells paradoxically express several immune-suppressive pathways that block the activity of Tcells at the tumor site. These include the inhibitory ligand PD-L1 that engages the negative regulatory receptor PD-1 on T cells;the tryptophan-catabolizing enzyme indoleamine-2,3-dioxygenase (IDO) that has been shown to induce peripheral tolerance;and FoxP3 + regulatory T cells (Tregs). In addition, lack of B7 costimulatory molecules supports a state of T cell anergy.Together, these four suppressive mechanisms create a tumor microenvironment that blocks the ability of tumor antigen-specificT cells to induce tumor rejection. Preclinical models have indicated that interference with one or more of these mechanismscan powerfully improve immune-mediated tumor control in vivo. Strategies to translate these approaches into the clinic areunderway.Justin Kline, MDAssistant Professor of MedicineThe Kline laboratory studies putative immune evasion mechanisms in pre-clinical cancer models, with the overall goal ofdeveloping strategies aimed at their reversal in order to improve anti-tumor immune responses in ways that can be translatedinto clinical application. The work has largely centered around two mechanisms, the first being suppression of conventionalT cells by regulatory T cells (Tregs), a suppressive population of CD4 + T cells. Tregs can potently inhibit anti-tumor immuneresponses both in mouse models and in cancer patients. A second mechanism is T cell anergy. The Kline laboratory hasdeveloped strategies to reverse anergy, which can have a profound impact on tumor rejection. One such approach that isamenable to clinical translation is through homeostatic proliferation in a lymphopenic host. Pre-clinical research from thelaboratory suggests that when Tregs are depleted from a purified population of polyclonal T cells, prior to adoptive transferinto a host rendered lymphopenic following the administration of low doses of total body irradiation, potent immunemediatedtumor rejection ensues. Mechanistic studies have suggested that the combination of Treg depletion and homeostaticproliferation leads to augmented priming and sustained effector function of tumor-antigen specific T cells. This approachhas demonstrated success in both pre-clinical solid tumor and hematological malignancy models, suggesting its potentialtranslation to a broad variety of cancer patients.These data have motivated the development of clinical approaches to deplete Tregs and/or reverse T cell anergy. The Klineteam is currently developing a phase I/II study in to translate these pre-clinical findings toward cancer patients. In the phase Iportion of the study, cohorts of patients with advanced melanoma will undergo a steady-state leukapheresis, from which T cellswill be purified and Treg will be depleted. Subsequently, patients will be assigned to receive escalating fractions of low-dosetotal body irradiation (50-200 cGy) to determine a non-myeloablative dose, which successfully depletes conventional T cells andTreg and permits the homeostatic proliferation of adoptively-transferred Treg-depleted T cells. Once the optimal dose of totalbody irradiation has been determined, the phase II portion of the trial will begin, in which patients will additionally receivea cancer vaccine. Immune responses will be monitored by IFN-γ ELISpot and MHC tetramer analysis to determine whethervaccination is capable of augmenting anti-tumor immune responses seen following adoptive T cell transfer alone. Futurestudies will continue to investigate negative regulatory mechanisms in the laboratory setting, where promising findings can betranslated into early-phase clinical studies for patients with cancer.50UCCRC SCIENTIFIC REPORT 2009
Additional Program Highlights*Research•• Endocytic sequestration of the B cell antigen receptor and toll-like receptor9 in anergic cells (Intraprogrammatic). Marcus Clark, MD, Marisa Alegre,MD, PhD, and colleagues have studied the cell biology of B cell anergy. Theyhave found that anergic B cells, which are refractory to toll-like receptor (TLR)activation by nucleoprotein autoantigens, show sequestration of the B cell antigenreceptor (BCR) and TLR9 just outside late endosomes. These results provide anexplanation for why anergic B cells are refractory to both BCR and TLR-mediatedactivation, an observation which has relevance both for autoimmunity and foranti-tumor antibody responses against self proteins (O’Neill et al. Proc Natl AcadSci U S A 106:6262-7, 2009).•• Cytosolic PLA2 is required for CTL-mediated immunopathology of celiacdisease via NKG2D and IL-15. Bana Jabri, MD, PhD and colleagues havecontinued investigations into the mechanisms by which CD8 + T cells mediateDrs. Maciej Lesniak (left) and Kelly Nicholas (right)pathology in celiac disease. The have found that IL-15 and the NKG2D receptoract together to promote local tissue destruction. Analysis of signal transductionevents has indicated that cytosolic phospholipase A 2(PLA 2) is activated to generate arachidonic acid release, which isnecessary for the activity of these cells. This represents a distinct mechanism of activation of cytotoxic T lymphocytes(CTLs) via a non-T cell receptor-dependent pathway. Such strategies also could be exploited to promote immunemediatedtumor destruction (Tang et al. J Exp Med. 206:707-19, 2009).Immunology& Cancer••TLR signals promote IL-6/IL-17-dependent transplant rejection (Intraprogrammatic). Marisa Alegre, MD, PhD andAnita Chong, PhD, along with their colleagues, have continued to explore the mechanism by which TLR agonists canbreak peripheral immunologic tolerance and promote rejection of transplanted allografts in vivo. They have observedthat the TLR9 agonist, CpG, can prevent transplant tolerance through a mechanism which involves induction of TH17-phenotype cells. These results have implications for how to approach breaking of peripheral tolerance against growingtumors in vivo (Chen et al. J Immunol. 182:6217-25, 2009).+••Therapeutic effects of ablative radiation on local tumors requires CD8 T cells: changing strategies for cancertreatment (Interprogrammatic). The laboratories of Yang-Xin Fu, MD, PhD and Ralph Weichselbaum, MD (Clinicaland Experimental Therapeutics Program) have explored the mechanisms by which high-dose radiation can effectivelydestroy tumors in mouse models in vivo. Contrary to expectations, they found that the efficacy of radiation dependedsignificantly upon participation by the host immune system. Thus, similar to certain chemotherapeutic drugs, CD8 +T cells are required for in vivo therapeutic efficacy. These observations have implications for how radiation should beoptimally integrated with other immunomodulatory interventions in the clinic (Lee et al. Blood 114:589-95, 2009).••A safety and efficacy study of local delivery of interleukin-12 transgene by PPC polymer in a model of experimentalglioma. Matt Lesniak, MD and colleagues have investigated local immunotherapeutic strategies that could support thecontrol of intracranial glioma tumors in mice. They found that delivery of the cytokine IL-12, as a plasmid in a novelpolymeric vehicle, could significantly improve tumor control and survival in mice, an effect which was synergistic withbiodegradable carmustine (BCNU) chemotherapy. A similar approach has potential for clinical translation in gliomapatients. (Sonabend et al. Anticancer Drugs 19:133-42, 2008).* Due to space constraints, only a small representative sample of Program highlights is presented here.UCCRC SCIENTIFIC REPORT 200951
••The impact of regulatory T cells on T cell immunity following hematopoeitic cell transplantation. Vu Nguyen, MDhas explored the impact of regulatory T cells (Tregs) in the context of graft-versus-host disease (GVHD) in allogeneic bonemarrow transplantation. Results indicate that Tregs suppress GVHD and enhance lymphoid reconstitution in a mousemodel. Along with previous results showing that a graft-versus-tumor effect was preserved, these observations form afoundation for developing Treg-adoptive therapy protocols for patients undergoing allogeneic stem cell transplantation(Nguyen et al. Blood 111:945-53, 2008).••The HLA-A2-Restricted PSMA Peptide LLHETDSAV is Poorly Immunogenic in Patients with Metastatic ProstateCancer (Interprogrammatic). Thomas Gajewski, MD, PhD, Walter Stadler, MD, (Clinical and Experimental TherapeuticsProgram) and colleagues have pursued a clinical vaccination strategy for prostate cancer involving prostate-specificmembrane antigen (PSMA) as a potential antigen for T-cell recognition. In their study, which utilized PSMA peptideLLHETDSAV-pulsed peripheral blood mononuclear cells (PBMC) + IL-12, they found that the vaccine was well-toleratedbut did not generate a clinical response. This was due to poor immunogenicity of this particular antigen. The resultssuggest that alternative prostate cancer antigens should be pursued and establish a paradigm for carrying out additionalimmunotherapy trials in patients with genitourinary malignancies (Knight et al. Prostate 69:142-148, 2008).••Chemokine expression in melanoma metastases associated with CD8+ T cell recruitment (Intraprogrammatic). ThomasGajewski, MD, PhD, Mark McKee, MD, and colleagues have studied the gene expression profile of melanoma metastasesfrom individual patients. They have observed that a subset of tumors expresses chemokines that can recruit activated Tcells into tumor sites. Mouse xenograft models have confirmed that high chemokine-expressing melanoma cell lines showmarkedly augmented attraction of activated CD8 + T cells into the tumor microenvironment. These studies imply thatimproving T cell homing may represent a novel strategy to improve immune-mediated tumor control in vivo (Harlin et al.Cancer Res 69:3077-85, 2009).Selected New Funding•• Tatyana Golovkina, PhD is the recipient of a National Cancer Institute R01 award to identify mechanisms of retrovirusresistance in I/LnJ mice. Under control of a single recessive gene, virus infectivity controller 1 (vic1), these mice confersustained resistance to both Mammary Tumor Virus (MMTV) and Murine Leukemia Virus (MuLV) infection. Dr.Golovkina aims to further characterize the expression and function of vic1.••••Lead investigator Hans Schreiber, MD, PhD, along with colleagues Thomas Gajewski, MD, PhD and Yang-Xin Fu, MD, PhDhas successfully competed for renewal of their program project, funded by the National Cancer Institute (P01), aimed toimprove the destructive power of CD8 + T cells and find strategies for enlisting additional mechanisms and treatments in asynergistic manner. The results of these studies should highlight new strategies for therapeutic manipulation that could beconsidered for clinical application in the future.Justin Kline, MD was awarded a grant from the National Cancer Institute (K23) to investigate the effectiveness of total bodyirradiation in inducing lymphopenia in cancer patients, and determine whether homeostatic proliferation of autologouspolyclonal T cells depleted of regulatory T cells occurs following transfer to such irradiated hosts. This research, ifsuccessful, could serve as a platform for future clinical trials and may have a significant impact on the delivery of novelcancer immunotherapeutic strategies to patients.•• Anne Sperling, PhD was awarded an S10 shared instrumentation grant from the National Center for Research Resources fora new, high sensitivity, 14-paramter BD LSRII flow cytometer in the University of Chicago Flow Cytometry Core Facility.This instrumentation provides state-of-the-art technology for identifying and enumerating individual living cells in a preciseand rapid fashion, and serves as an indispensible tool for numerous areas of biomedical research, including host defense,autoimmune diseases, and mechanisms of cancer and immunology.52UCCRC SCIENTIFIC REPORT 2009
••••Ursula Storb, MD was the recipient of an R21 grant from the National Institute of Allergy and Infectious Diseases tostudy the mechanism by which the cytidine deaminase, AID, interacts with sequences in which it deaminates cytidineto uridine. This process initiates somatic hypermutation of immunoglobulin genes, which can result in highly specificantibodies against pathogens or cause lymphoid malignancies and autoimmunity.Vu Nguyen, MD received a Mentored Clinical Scientist Research Career Development award (K08) from the NationalInstitutes of Health to investigate the properties of ex vivo expanded CD4 + CD25 + regulatory T cells (Treg) in animalmodels of hematopoietic cell transplantation (HCT). This project will help determine whether ex vivo expanded Tregadds benefit to HCT, which is potentially curative for a variety of hematologic cancers, but is limited in application bygraft versus host disease and the lack of donors.••Maciej Lesniak, MD is the recipient of a National Institutes of Health R01 award to study regulatory T cells in malignantglioma. Dr. Lesniak, along with co-investigators Thomas Gajewski, MD, PhD and Yang-Xin Fu, MD, PhD, aim to elucidatethe mechanisms leading to CD4 + CD25 + regulatory T cell (Treg) infiltration and suppression in glioblastoma multiforme(GBM), the most common primary malignant tumor of the adult central nervous system.Immunology& CancerNew Faculty Recruitments and UCCRC MembersVu Nguyen, MD’s research examines the development and function of regulatory T cells in models of hematologicmalignancies and stem cell transplantation. The goal of his research is to develop targeted molecular and cellular treatmentstrategies that separate graft-versus-host disease from the beneficial graft-versus-tumor reaction.UCCRC SCIENTIFIC REPORT 200953
Selected Publications* : Intraprogrammatic Collaboration# : Interprogrammatic CollaborationAdams, Erin PhDAdams EJ, Strop P, Shin S, Chien YH, Garcia KC. An autonomous CDR3deltais sufficient for recognition of the nonclassical MHC class I molecules T10 andT22 by gammadelta T cells. Nat Immunol 9(7):777-84, 2008.Alegre, Maria-Luisa MD, PhD* Alegre ML, Leemans J, Le Moine A, Florquin S, De Wilde V, Chong A,Goldman M. The multiple facets of toll-like receptors in transplantationbiology. Transplantation 86(1):1-9, 2008.* Alegre ML, Goldstein DR, Chong AS. Toll-like receptor signaling intransplantation. Curr Opin Organ Transplant 13(4):358-65, 2008.* Chen L, Ahmed E, Wang T, Wang Y, Ochando J, Chong AS, Alegre ML.TLR signals promote IL-6/IL-17-dependent transplant rejection. J Immunol182(10):6217-25, 2009.* O’Neill SK, Veselits ML, Zhang M, Labno C, Cao Y, Finnegan A, UccelliniM, Alegre ML, Cambier JC, Clark MR. Endocytic sequestration of the B cellantigen receptor and toll-like receptor 9 in anergic cells. Proc Natl Acad Sci U SA 106(15):6262-7, 2009.* Alegre ML, Chen L, Wang T, Ahmed E, Wang CR, Chong A. Antagonisticeffect of toll-like receptor signaling and bacterial infections on transplantationtolerance. Transplantation 87(9 Suppl):S77-9, 2009.* Molinero LL, Yang J, Gajewski T, Abraham C, Farrar MA, Alegre ML.CARMA1 controls an early checkpoint in the thymic development of FoxP3+regulatory T cells. J Immunol 182(11):6736-43, 2009.Zimmer MI, Nguyen HP, Wang B, Xu H, Colmone A, Felio K, Choi HJ, Zhou P,Alegre ML, Wang CR. Polymorphisms in CD1d affect antigen presentation andthe activation of CD1d-restricted T cells. Proc Natl Acad Sci U S A 106(6):1909-14, 2009.Bendelac, Albert MD, PhDSavage AK, Constantinides MG, Han J, Picard D, Martin E, Li B, Lantz O,Bendelac A. The transcription factor PLZF directs the effector program of theNKT cell lineage. Immunity 29(3):391-403, 2008.Zajonc DM, Savage PB, Bendelac A, Wilson IA, Teyton L. Crystal structuresof mouse CD1d-iGb3 complex and its cognate Valpha14 T cell receptorsuggest a model for dual recognition of foreign and self glycolipids. J Mol Biol377(4):1104-16, 2008.Allende ML, Zhou D, Kalkofen DN, Benhamed S, Tuymetova G, Borowski C,Bendelac A, Proia RL. S1P1 receptor expression regulates emergence of NKTcells in peripheral tissues. FASEB J 22(1):307-15, 2008.# Dose M, Sleckman BP, Han J, Bredemeyer AL, Bendelac A, Gounari F.Intrathymic proliferation wave essential for Vα 14+ natural killer T celldevelopment depends on c-Myc. Proc Natl Acad Sci U S A 106(21):8641-6, 2009.Yin N, Long X, Goff RD, Zhou D, Cantu C 3rd, Mattner J, Mezard PS, TeytonL, Bendelac A, Savage PB. Alpha anomers of iGb3 and Gb3 stimulate cytokineproduction by natural killer T cells. ACS Chem Biol 4(3):199-208, 2009.Chong, Anita PhD* Alegre ML, Leemans J, Le Moine A, Florquin S, De Wilde V, Chong A,Goldman M. The multiple facets of toll-like receptors in transplantationbiology. Transplantation 86(1):1-9, 2008.* Alegre ML, Goldstein DR, Chong AS. Toll-like receptor signaling intransplantation. Curr Opin Organ Transplant 13(4):358-65, 2008.Li Y, Ma L, Yin D, Shen J, Chong AS. Long-term control of alloreactive B cellresponses by the suppression of T cell help. J Immunol 180(9):6077-84, 2008.* Wang T, Chen L, Ahmed E, Ma L, Yin D, Zhou P, Shen J, Xu H, Wang CR,Alegre ML, Chong AS. Prevention of allograft tolerance by bacterial infectionwith Listeria monocytogenes. J Immunol 180(9):5991-9, 2008.Ma L, Xiang Z, Sherrill TP, Wang L, Blackwell TS, Williams P, Chong A, ChariR, Yin DP. Bioluminescence imaging visualizes activation of nuclear factorkappaBin mouse cardiac transplantation. Transplantation 85(6):903-10, 2008.* Chen L, Ahmed E, Wang T, Wang Y, Ochando J, Chong AS, Alegre ML.TLR signals promote IL-6/IL-17-dependent transplant rejection. J Immunol182(10):6217-25, 2009.Clark, Marcus MD* O’Neill SK, Veselits ML, Zhang M, Labno C, Cao Y, Finnegan A, UccelliniM, Alegre ML, Cambier JC, Clark MR. Endocytic sequestration of the B cellantigen receptor and toll-like receptor 9 in anergic cells. Proc Natl Acad Sci U SA 106(15):6262-7, 2009.Mandal M, Crusio KM, Meng F, Liu S, Kinsella M, Clark MR, Takeuchi O,Aifantis I. Regulation of lymphocyte progenitor survival by the proapoptoticactivities of Bim and Bid. Proc Natl Acad Sci U S A 105(52):20840-5, 2008.Fu, Yang-Xin MD, PhD* Yu P, Fu YX. Targeting tumors with LIGHT to generate metastasis-clearingimmunity. Cytokine Growth Factor Rev 19(3-4):285-94, 2008.* Zhang B, Zhang Y, Bowerman NA, Schietinger A, Fu YX, Kranz DM, RowleyDA, Schreiber H. Equilibrium between host and cancer caused by effector Tcells killing tumor stroma. Cancer Res 68(5):1563-71, 2008.Zhu M, Fu YX. Coordinating development of medullary thymic epithelial cells.Immunity 29(3):386-8, 2008.Papa S, Zazzeroni F, Fu YX, Bubici C, Alvarez K, Dean K, Christiansen PA,Anders RA, Franzoso G. Gadd45beta promotes hepatocyte survival during liverregeneration in mice by modulating JNK signaling. J Clin Invest 118(5):1911-23,2008.Zhao J, Yang X, Auh SL, Kim KD, Tang H, Fu YX. Do adaptive immune cellssuppress or activate innate immunity?. Trends Immunol 30(1):8-12, 2009.Zhao J, Kim KD, Yang X, Auh S, Fu YX, Tang H. Hyper innate responses inneonates lead to increased morbidity and mortality after infection. Proc NatlAcad Sci U S A 105(21):7528-33, 2008.# Lee Y, Auh SL, Wang Y, Burnette B, Wang Y, Meng Y, Beckett M, SharmaR, Chin R, Tu T, Weichselbaum RR, Fu YX. Therapeutic effects of ablativeradiation on local tumor require CD8+ T cells: changing strategies for cancertreatment. Blood 114(3):589-95, 2009.Gajewski, Thomas MD, PhD# Knight D, Peterson AC, Rini BI, Harlin H, Gajewski TF, Stadler WM. TheHLA-A2-restricted PSMA peptide LLHETDSAV is poorly immunogenic inpatients with metastatic prostate cancer. Prostate 69(2):142-8, 2009.* Kline J, Brown IE, Zha YY, Blank C, Strickler J, Wouters H, Zhang L, GajewskiTF. Homeostatic proliferation plus regulatory T-cell depletion promotes potentrejection of B16 melanoma. Clin Cancer Res 14(10):3156-67, 2008.Zheng Y, Zha Y, Gajewski TF. Molecular regulation of T-cell anergy. EMBO Rep9(1):50-5, 2008.* Harlin H, Meng Y, Peterson AC, Zha Y, Tretiakova M, Slingluff C, McKee M,Gajewski TF. Chemokine expression in melanoma metastases associated withCD8+ T-cell recruitment. Cancer Res 69(7):3077-85, 2009.Praveen K, Zheng Y, Rivas F, Gajewski TF. Protein kinase Ctheta focusing at thecSMAC is a consequence rather than cause of TCR signaling and is dependenton the MEK/ERK pathway. J Immunol 182(10):6022-30, 2009.Camacho LH, Antonia S, Sosman J, Kirkwood JM, Gajewski TF, Redman B,Pavlov D, Bulanhagui C, Bozon VA, Gomez-Navarro J, Ribas A. Phase I/IItrial of tremelimumab in patients with metastatic melanoma. J Clin Oncol27(7):1075-81, 2009.Gordon IO, Wade T, Chin K, Dickstein J, Gajewski TF. Immune-mediatedred cell aplasia after anti-CTLA-4 immunotherapy for metastatic melanoma.Cancer Immunol Immunother 58(8):1351-3, 2009.Golovkina, Tatyana PhDCase LK, Petell L, Yurkovetskiy L, Purdy A, Savage KJ, Golovkina TV.Replication of beta- and gamma retroviruses is restricted in I/LnJ mice via thesame genetic mechanism. J Virol 82(3):1438-47, 2008.54UCCRC SCIENTIFIC REPORT 2009
Guevara-Patino, Jose MD, PhDDenman CJ, McCracken J, Hariharan V, Klarquist J, Oyarbide-Valencia K,Guevara-Patino JA, Le Poole IC. HSP70i accelerates depigmentation in a mousemodel of autoimmune vitiligo. J Invest Dermatol 128(8):2041-8, 2008.Engelhorn ME, Guevara-Patino JA, Merghoub T, Liu C, Ferrone CR, RizzutoGA, Cymerman DH, Posnett DN, Houghton AN, Wolchok JD. Mechanisms ofimmunization against cancer using chimeric antigens. Mol Ther 16(4):773-81,2008.Lundberg K, Roos AK, Pavlenko M, Leder C, Wehrum D, Guevara-PatinoJ, Andersen RS, Pisa P, A modified epitope identified for generation andmonitoring of PSA-specific T cells in patients on early phases of PSA-basedimmunotherapeutic protocols. Vaccine 27(10):1557-65, 2009.Liu Y, Peng Y, Mi M, Guevara-Patino J, Munn DH, Fu N, He Y, Lentivectorimmunization stimulates potent CD8 T cell responses against melanomaself-antigen tyrosinase-related protein 1 and generates antitumor immunity inmice. J Immunol 182(10):5960-9, 2009.Nandi S, Ulasov IV, Tyler MA, Sugihara AQ, Molinero L, Han Y, Zhu ZB,Lesniak MS. Low-dose radiation enhances survivin-mediated virotherapyagainst malignant glioma stem cells. Cancer Res 68(14):5778-84, 2008.Sonabend AM, Rolle CE, Lesniak MS. The role of regulatory T cells inmalignant glioma. Anticancer Res 28(2B):1143-50, 2008.Andaloussi AE, Han Y, Lesniak MS. Progression of intracranial gliomadisrupts thymic homeostasis and induces T-cell apoptosis in vivo. CancerImmunol Immunother 57(12):1807-16, 2008.Sonabend AM, Ulasov IV, Tyler MA, Rivera AA, Mathis JM, Lesniak MS.Mesenchymal stem cells effectively deliver an oncolytic adenovirus tointracranial glioma. Stem Cells 26(3):831-41, 2008.Sonabend AM, Velicu S, Ulasov IV, Han Y, Tyler B, Brem H, MatarMM, Fewell JG, Anwer K, Lesniak MS. A safety and efficacy study oflocal delivery of interleukin-12 transgene by PPC polymer in a model ofexperimental glioma. Anticancer Drugs 19(2):133-42, 2008.Jabri, Bana MD, PhD# Depaolo RW, Tang F, Kim I, Han M, Levin N, Ciletti N, Lin A, Anderson D,Schneewind O, Jabri B. Toll-like receptor 6 drives differentiation of tolerogenicdendritic cells and contributes to LcrV-mediated plague pathogenesis. CellHost Microbe 4(4):350-61, 2008.Ebert EC, Jabri B. Massive interleukin-12-induced interferon-gammaproduction by interleukin-15-stimulated lamina propria lymphocytes followedby down-regulation of the interleukin-12 receptor. Immunology 124(4):453-60,2008.Tang F, Chen Z, Ciszewski C, Setty M, Solus J, Tretiakova M, Ebert E, HanJ, Lin A, Guandalini S, Groh V, Spies T, Green P, Jabri B. Cytosolic PLA2 isrequired for CTL-mediated immunopathology of celiac disease via NKG2D andIL-15. J Exp Med 206(3):707-19, 2009.Kline, Justin MD# Kline J, Subbiah S, Lazarus HM, van Besien K. Autologous graft-versus-hostdisease: harnessing anti-tumor immunity through impaired self-tolerance.Bone Marrow Transplant 41(6):505-13, 2008.* Kline J, Brown IE, Zha YY, Blank C, Strickler J, Wouters H, Zhang L, GajewskiTF. Homeostatic proliferation plus regulatory T-cell depletion promotes potentrejection of B16 melanoma. Clin Cancer Res 14(10):3156-67, 2008.Kline J. Will changing the face of WT1 make it more attractive to T cells?. LeukLymphoma 50(2):156-7, 2009.* Zhang L, Gajewski TF, Kline J. PD-1/PD-L1 interactions inhibit antitumorimmune responses in a murine acute myeloid leukemia model. Blood114(8):1545-52, 2009.# Poire X, Artz A, Larson RA, Kline J, Odenike O, Rich E, Godley L, Stock W,van Besien K. Allogeneic stem cell transplantation with alemtuzumab-basedconditioning for patients with advanced chronic myelogenous leukemia. LeukLymphoma 50(1):85-91, 2009.* Driessens G, Kline J, Gajewski TF. Costimulatory and coinhibitory receptorsin anti-tumor immunity. Immunol Rev 229(1):126-44, 2009.McKee, Mark MD* Harlin H, Meng Y, Peterson AC, Zha Y, Tretiakova M, Slingluff C,McKee M, Gajewski TF. Chemokine expression in melanoma metastasesassociated with CD8+ T-cell recruitment. Cancer Res 69(7):3077-85,2009.Nguyen, Vu MDNguyen VH, Shashidhar S, Chang DS, Ho L, Kambham N, BachmannM, Brown JM, Negrin RS. The impact of regulatory T cells on T cellimmunity following hematopoeitic cell transplantation. Blood 111(2):945-53, 2008.Randall, Glenn PhDBerger KL, Cooper JD, Heaton NS, Yoon R, Oakland TE, Jordan TX,Mateu G, Grakoui A, Randall G. Roles for endocytic trafficking andphosphatidylinositol 4-kinase III alpha in hepatitis C virus replication.Proc Natl Acad Sci U S A 106(18):7577-82, 2009.Schreiber, Hans MD, PhD# Zhang B, Karrison T, Rowley DA, Schreiber H. IFN-gamma- and TNFdependentbystander eradication of antigen-loss variants in establishedmouse cancers. J Clin Invest 118(4):1398-404, 2008.* Zhang B, Zhang Y, Bowerman NA, Schietinger A, Fu YX, Kranz DM,Rowley DA, Schreiber H. Equilibrium between host and cancer caused byeffector T cells killing tumor stroma. Cancer Res 68(5):1563-71, 2008.Schreiber H. Tumor-specific immune responses. Semin Immunol20(5):265-6, 2008.Schietinger A, Philip M, Schreiber H. Specificity in cancerimmunotherapy. Semin Immunol 20(5):276-85, 2008.Chopra N, Gan W, Schreiber H, Kurutz JW, Meredith SC. Versatile cyclictemplates for assembly of axially oriented ligands. Bioconjug Chem20(2):231-40, 2009.Immunology& CancerKumar, Vinay MD, PhDChlewicki LK, Velikovsky CA, Balakrishnan V, Mariuzza RA, Kumar V.Molecular basis of the dual functions of 2B4 (CD244). J Immunol 180(12):8159-67, 2008.Lesniak, Maciej MDPaul CP, Everts M, Glasgow JN, Dent P, Fisher PB, Ulasov IV, Lesniak MS, Stoff-Khalili MA, Roth JC, Preuss MA, Dirven CM, Lamfers ML, Siegal GP, Zhu ZB,Curiel DT. Characterization of infectivity of knob-modified adenoviral vectorsin glioma. Cancer Biol Ther 7(5):786-93, 2008.Ulasov IV, Tyler MA, Rivera AA, Nettlebeck DM, Douglas JT, Lesniak MS.Evaluation of E1A double mutant oncolytic adenovectors in anti-glioma genetherapy. J Med Virol 80(9):1595-603, 2008.Sperling, Anne PhD# Yau DM, Sethakorn N, Taurin S, Kregel S, Sandbo N, Camoretti-Mercado B, Sperling AI, Dulin NO. Regulation of Smad-mediated genetranscription by RGS3. Mol Pharmacol 73(5):1356-61, 2008.Cannon JL, Collins A, Mody PD, Balachandran D, Henriksen KJ,Smith CE, Tong J, Clay BS, Miller SD, Sperling AI. CD43 regulates Th2differentiation and inflammation. J Immunol 180(11):7385-93, 2008.Tesciuba AG, Shilling RA, Agarwal MD, Bandukwala HS, Clay BS,Moore TV, Weinstock JV, Welcher AA, Sperling AI. ICOS costimulationexpands Th2 immunity by augmenting migration of lymphocytes todraining lymph nodes. J Immunol 181(2):1019-24, 2008.UCCRC SCIENTIFIC REPORT 200955
Storb, Ursula MD# Longerich S, Orelli BJ, Martin RW, Bishop DK, Storb U. Brca1 inimmunoglobulin gene conversion and somatic hypermutation. DNA Repair(Amst) 7(2):253-66, 2008.Shen HM, Bozek G, Pinkert CA, McBride K, Wang L, Kenter A, Storb U.Expression of AID transgene is regulated in activated B cells but not in restingB cells and kidney. Mol Immunol 45(7):1883-92, 2008.Shen HM, Poirier MG, Allen MJ, North J, Lal R, Widom J, Storb U. Theactivation-induced cytidine deaminase (AID) efficiently targets DNA innucleosomes but only during transcription. J Exp Med 206(5):1057-71, 2009.Yu, Ping MD* Yu P, Fu YX. Targeting tumors with LIGHT to generate metastasis-clearingimmunity. Cytokine Growth Factor Rev 19(3-4):285-94, 2008.Zhang, Jian MD* Qiao G, Li Z, Molinero L, Alegre ML, Ying H, Sun Z, Penninger JM, ZhangJ. T-cell receptor-induced NF-kappaB activation is negatively regulated by E3ubiquitin ligase Cbl-b. Mol Cell Biol 28(7):2470-80, 2008.Bao L, Haas M, Pippin J, Wang Y, Miwa T, Chang A, Minto AW, Petkova M,Qiao G, Song WC, Alpers CE, Zhang J, Shankland SJ, Quigg RJ. Focal andsegmental glomerulosclerosis induced in mice lacking decay-acceleratingfactor in T cells. J Clin Invest 119(5):1264-74, 2009.56UCCRC SCIENTIFIC REPORT 2009
Selected Major Grants and AwardsThe Immunology and Cancer Program has a funding base of $12,536,841 in annual total costs (current as of June 15, 2009).This sum includes $3,536,249 in NCI funding and $6,551,885 in other NIH funding. Due to space constraints, only new awardspresented since January 1, 2008 with funding of $100,000 or more in annual total costs are listed here.Investigator Title Start DateSchreiber, HansCD8+ T Cells and ImmunologicalTumor RegressionEndDateAnnualTotal CostClassFunding Agency7/26/2008 5/31/2013 $1,543,335 P01 National Cancer InstituteBendelac, Albert Glycolipid Presentation by CD1d 4/1/2008 3/31/2013 $1,304,014 P01Clark, MarcusGolovkina,TatyanaLesniak, MaciejGuevara-Patino,JoseGajewski, ThomasTertiary Lymphoid Neogenesis inHuman Lupus NephritisCloning of the Vic1 gene, a NovelRetrovirus Restriction FactorConditionally Replicative AdenoviralVectors for Malignant GliomaFunctional Profiling of Tumor-InducedImmune SuppressionDeletion of Inhibitory Genes in Post-Thymic T Cells to Study ImmuneTolerance8/15/2008 7/31/2013 $338,800 R01National Institute of Allergyand Infectious DiseasesNational Instituteof Arthritis andMusculoskeletal and SkinDiseases7/17/2008 5/31/2013 $316,675 R01 National Cancer Institute1/9/2008 12/31/2012 $312,556 R01 National Cancer Institute1/1/2008 12/31/2011 $240,000 08 American Cancer Society7/1/2008 6/30/2010 $231,000 R21Sperling, Anne BD LSR II Flow Cytometer 1/15/2009 1/14/2010 $223,835 S10Lesniak, MaciejStorb, UrsulaGuevara-Patino,JoseKline, JustinDevelopment of an Adenoviral VectorWith Chimeric Fiber for MalignantGliomaAID in Somatic Mutation ofImmunoglobulin GenesDisparate Suppression of NaiveEffector and Memory T cells inTumor-Bearing HostsA Study to Assess the Safety andBiological Activity of RecombinantHuman Interleukin-18 Administeredby Intravenous Infusion in aCombination with Rituximab in AdultPatients with B Cell Non-HodgkinsLymphomaNational Institute of Allergyand Infectious DiseasesNational Center forResearch Resources4/1/2008 3/31/2010 $215,325 R21 National Cancer Institute2/15/2009 1/31/2011 $195,000 R21National Institute of Allergyand Infectious Diseases1/1/2008 12/31/2009 $172,688 R21 National Cancer Institute6/5/2008 6/4/2010 $165,097 N/A Glaxo Smith KleinFu, Yang-Xin Antibody LIGHT Fusion 9/10/2008 9/10/2009 $151,872 N/A Biogen Idec Inc.Guevara-Patino,JoseKline, JustinChong, AnitaGuevara-Patino,JoseDNA Vaccine for Seasonal andPandemic InfluenzaHomeostatic Proliferation andRegulatory T Cell Depletion as CancerImmunotherapyThe Effect of Pioglitazone onPancreatic Beta Cell RegenerationTargeting HSP70 in AutoimmuneVitiligo8/1/2008 7/31/2010 $149,700 U01 National Institutes of Health7/1/2008 6/30/2013 $129,843 K23 National Cancer Institute3/9/2009 3/8/2011 $126,343 N/ATakeda Chemical Industries,LTD.9/1/2008 8/31/2013 $105,217 R01 National Institutes of HealthImmunology& CancerUCCRC SCIENTIFIC REPORT 200957
Dr. Susan Cohn with a patientProgram 4Clinical and Experimental Therapeutics
The overall goal of the program is to foster interactionbetween basic and clinical investigators that will resultin innovative and effective therapies for cancer patients.Overview & GoalsThe Clinical and Experimental TherapeuticsProgram is a cohesive, integrated group thatbrings together a diverse team of 53 membersrepresenting 9 different departments. Theoverall goal of the program is to fosterinteraction between basic and clinicalinvestigators that will result in innovative andeffective therapies for cancer patients. Thetranslational nature of much of the research donein this program, along with the leadership roleassumed by many program members in studiesconducted by national clinical trials cooperativegroups, illustrates the impact of this programin developing new therapies for oncology. Theprogram has a long-standing focus on drugdevelopment at all phases of clinical testing anda strong pharmacogenetic component. The typesof trials range from preclinical development toinvestigator-initiated Phase I clinical trials, toPhase II trials in the regional Phase II network, toPhase III studies with CALGB.The scientific goals of the program are to (1)foster interaction between basic and clinicalinvestigators that will result in innovativeand effective therapies; (2) to integrate newdrugs into the development of multimodalitytherapies for patients with advanced solidtumors; and (3) pursue a broad program ofpreclinical, translational, and clinical research inpharmacogenetics and pharmacology.Program Leaders:M. Eileen Dolan, PhDClinical & ExperimentalTherapeuticsEverett Vokes, MDUCCRC SCIENTIFIC REPORT 200959
60MembersInvestigator*Douglas Bishop PhDElizabeth Blair MDEzra Cohen MDSusan Cohn MDPhilip Connell MDChristopher Daugherty MDGlyn Dawson PhDM. Eileen Dolan PhDScott Eggener MDMark Ferguson MDAlessandro Fichera MDGini Fleming MDHarvey Golomb MDDaniel Haraf MDJohn Hart MDChuan He PhDJavad Hekmatpanah MDPhilip Hoffman MDRoger Hurst MDFederico Innocenti MD, PhDEdwin Kaplan MDTheodore Karrison PhDHedy Kindler MDMark Lingen DDS, PhDMarcy List PhDYves Lussier MDMichael Maitland MD, PhDBruce Minsky MDRita Nanda MDTerrance Peabody MDLouis Portugal MDEdwin Posadas MDMitchell Posner MDMark Ratain MDKevin Roggin MDCharles Rubin MDJoseph Salama MDRichard Schilsky MDTanguy Seiwert MDArieh Shalhav MDMark Siegler MDMichael Simon MDDavid Song MDWalter Stadler MDGary Steinberg MDKerstin Stenson MDRonald Thisted PhDEverett Vokes MDRalph Weichselbaum MDH. Rosie Xing PhDSeiko Diane Yamada MDBakhtiar Yamini MDChun-Su Yuan MD, PhDUCCRC SCIENTIFIC REPORT 2009RankProfessorAssociate ProfessorAssociate ProfessorProfessorAssistant ProfessorProfessorProfessorProfessorAssistant ProfessorProfessorAssociate ProfessorProfessorProfessorProfessorProfessorAssociate ProfessorProfessorProfessorAssociate ProfessorAssistant ProfessorProfessorAssociate ProfessorAssociate ProfessorAssociate ProfessorAssociate Director AdministrationAssociate ProfessorAssistant ProfessorProfessorAssistant ProfessorProfessorAssociate ProfessorAssistant ProfessorProfessorProfessorAssistant ProfessorAssociate ProfessorAssistant ProfessorProfessorInstructorProfessorProfessorProfessorAssociate ProfessorProfessorProfessorAssociate ProfessorProfessorProfessorProfessorAssistant ProfessorAssociate ProfessorAssistant ProfessorAssociate ProfessorDepartment* Reflects all Program membership during 2008-2009Radiation and Cellular OncologySurgeryMedicinePediatricsRadiation and Cellular OncologyMedicinePediatricsMedicineSurgerySurgerySurgeryMedicineMedicineRadiation and Cellular OncologyPathologyChemistrySurgeryMedicineSurgeryMedicineSurgeryHealth StudiesMedicinePathologyUCCRCMedicineMedicineRadiation and Cellular OncologyMedicineSurgerySurgeryMedicineSurgeryMedicineSurgeryPediatricsRadiation and Cellular OncologyMedicineMedicineSurgeryMedicineSurgerySurgeryMedicineSurgerySurgeryHealth StudiesMedicineRadiation and Cellular OncologyPathologyOB/GYNSurgeryAnesthesia/Critical Care
Featured Faculty Research Summaries †Investigators in the Clinical and Experimental Therapeutics Program aim toimprove cancer therapies by focusing on several research themes includingthe development of novel cancer therapeutics, pharmacogenomics of cancertherapeutics, and the interaction of chemotherapy and radiation. Presentedbelow are highlights of current studies in the Program.Development of Novel Cancer Therapeutic Agents and Combined Modality Therapy ConceptsEzra Cohen, MDAssociate Professor of MedicineSquamous Cell Carcinoma of the Head and Neck (HNSCC) is the 6 th leading causeof cancer mortality worldwide. Current therapeutic advances have clearly reacheda plateau and new avenues of research need to be explored. With few exceptions,the benefit of available systemic therapies in recurrent or metastatic malignancies,including SCCHN, is limited and usually of short duration. As such, Dr. Cohen’sprevious signaling work in SCCHN cell lines focuses on two main areas in search ofnovel therapies to improve outcomes – the AGC kinase family and intrinsic resistanceto epidermal growth factor receptor (EGFR) inhibition.Dr. Cohen’s studies demonstrated that protein kinase C (PKC) isoforms are criticalDr. Mitchell Posnermediators of SCCHN growth both in vitro and in vivo. In fact, enzastaurin, an acyclicbisindolylmaleimide that displays potent selective inhibition of classic and novel PKCisoforms was active and reduced proliferation in SCCHN cell lines. To elucidate putative targets of enzastaurin inSCCHN the Cohen laboratory performed gene expression arrays and discovered that expression of cell cycle genes,including cyclins D and E, were significantly altered by exposure to enzastaurin. Interestingly, cyclin D1 protein levelsappeared to predict in vitro sensitivity to the agent. Moreover, inhibition of cyclin D1 expression reversed resistance inan insensitive cell line, whereas cyclin D1 transfection in a sensitive cell line rendered the cells resistant to enzastaurin.Initially, the underlying mechanisms for these observations were hypothesized to relate to signaling mediated by PKCisoforms. However, dynamic modeling of putative targets of enzastaurin and cyclin D1 inhibition demonstrated thatthe effect is most likely secondary to inhibition of AKT. In fact, depletion of AKT by siRNA reduces cell viability ofSCCHN cell lines, inhibits cyclin D1 expression, and reverses resistance to enzastaurin. In addition to AKT affectingSCCHN viability and proliferation, the Cohen group implicated the pathway as a critical mediator of resistanceto EGFR inhibitors. The small molecule tyrosine kinase inhibitor (TKI), gefitinib, was tested in a panel of SCCHNcell lines to determine the IC 50in an in vitro cell viability assay. In all cell lines, the agent inhibited phosphorylationof EGFR, as expected. However, only in the cell lines resistant to gefitinib (defined as IC 50> 10mM) was AKTphosphorylation preserved upon exposure to the agent. Therefore, constitutive activation of AKT independent of EGFRcontributes to resistance to an EGFR TKI. In SCCHN, dysregulation of the PI3K/AKT pathway occurs frequentlyand has been linked to radiation resistance and poor outcome. Additional work supports a role of AKT in regulatinganother proto-oncogene that is often amplified, CCND1, and as a major mechanism of resistance to EGFR inhibitors.Clinical & ExperimentalTherapeuticsBeyond inhibiting specific targets relevant to SCCHN, the Cohen laboratory in collaboration with Argonne NationalLaboratory has generated epidermal growth factor (EGF)-antibody-coated PLGA-PEG nanoparticles encapsulatingcisplatin. Since EGFR is universally expressed in SCCHN, the group hypothesized that the antibody coatingwould direct the nanoparticles to SCCHN tumor cells. Furthermore, the nanoparticle shell contains iron, whicheffectively allows magnetic guidance. These nanoparticles were green fluorescent protein (GFP)-tagged and injectedintraperitoneally (IP) into mice harboring SQ20B head and neck cancer hind-limb xenografts. Preliminary datademonstrate that after 30 minutes of applied magnetic field of approximately 1 Tesla, the tracks of the fluorescentparticles can be observed and the nanoparticles concentrate in tumor cells. When mice bearing SQ20B xenograftswere treated IP with EGF-coated, cisplatin-containing nanoparticles, significant tumor regression was observed† Note: Due to space constraints, only a small representative sample of Program members is presented here.UCCRC SCIENTIFIC REPORT 200961
compared to mice treated with IP cisplatin alone or vehicle control. Interestingly, cisplatin-nanoparticles demonstrated greaterefficacy despite containing a 10-fold lower concentration of the drug than was administered to mice receiving cisplatin alone.In summary, the Cohen laboratory is interested in extending findings into therapy for patients with SCCHN. Specifically,the group is investigating the role of PI3K/AKT pathway inhibition using agents in development. Moreover, the laboratory iscontinuing to study other mechanisms of resistance to therapy in SCCHN by developing second generation EGFR inhibitors andimproving agent delivery using nanoparticles.Joseph Salama, MDAssistant Professor of Radiation and Cellular OncologyDr. Salama studies the outcomes of patients with upper aeordigestive cancers (head and neck and lung) treated with combinedchemotherapy and radiotherapy, and also has an active interest in improving the outcomes of patients with limited metastaticcancer traditionally treated only with chemotherapy or, in select cases, surgery. Patients with limited metastatic disease,or oligometastases, represent a subset of patients who may be curable with aggressive treatment directed at known sites ofmetastasis. Dr. Salama’s research focuses on improving outcomes for oligometastatic patients by clarifying characteristicsof these patients, refining novel radiation treatment techniques for oligometastatic cancers alone or in combination withchemotherapy, as well as identification of genetic pathways unique to oligometastatic patients.Dr. Salama has been studying the application of a novel radiotherapy technique, hypofractionated image-guided radiotherapy,a combination of technical advances in radiotherapy planning and delivery, specifically to all known metastatic depositsin patients with metastases that are limited in number and location. Through an ongoing dose-escalation study, safe andeffective doses of hypofractionated image-guided radiotherapy for different body sites have been identified with 70% of treatedmetastases being controlled. Further analyses have identified that escalating radiation doses are associated with improvedcontrol rates. Additionally, of the 56 patients treated to date 32% have achieved disease control (either no evidence of diseaseor no disease progression). The Salama team has analyzed tumor control with various imaging modalities, and found thatreduction in positron emission tomography intensity is the most sensitive method to gauge response to this treatment. Theseinitial findings have been recently published in Clinical Cancer Research. Currently, Dr. Salama is collaborating with MemorialSloan Kettering Cancer Center to compare a single large dose of radiotherapy versus five intermediate doses.As the majority of patients studied had control of treated metastases, but progression within new metastatic sites, combinationof hypofractionated image-guided radiotherapy with systemic therapy seems warranted. Therefore, in collaboration with Dr.Everett E. Vokes, the Salama team has activated a randomized phase II trial in patients with limited volume metastatic nonsmallcell lung cancer in attempt to determine if the combination of docetaxel and cisplatin and hypofractionated image-guidedradiotherapy improves survival of patients compared to those treated with docetaxel and cisplatin alone.Additionally, in collaboration with Dr. Ralph R. Weichselbaum, Dr. Salama is seeking to understand the genetic characteristicsof patients who have limited metastatic cancer. The genetic determinants of why some patients have cancer metastasizing tolimited sites, while others have a distribution of metastasis throughout their body, is not at all understood. An analysis of tumorspecimens derived from patients with limited metastatic disease from primary tumors as well as metastases will be performedto seek out key pathways involved in the development and response to treatment of oligometastatic patients.Douglas Bishop, PhDProfessor of Radiation and Cellular OncologyThe Bishop laboratory has worked to identify molecular targets that can be exploited in the treatment of cancers. This haspredominantly centered on DNA repair pathways that are involved in tumor cell resistance to common cancer treatments.Specifically, the Bishop group has focused on proteins involved in the homologous recombinational (HR) DNA repair pathway,which is involved in radiation-induced DNA damage and is critically important for repair of cross-links induced by platinumbasedchemotherapies and mitomycin C. The laboratory is primarily investigating the HR protein, RAD51, which is the centralrecombinase in this DNA repair pathway. Several studies have suggested that RAD51 protein is highly expressed in a varietyof human cancer cells, and that this over-expression confers resistance to radiation therapy and chemotherapy. Projects62UCCRC SCIENTIFIC REPORT 2009
in the laboratory are aimed at 1) blocking the function of RAD51with inhibitory small molecules, in an attempt to sensitize cells tochemotherapy and radiotherapy; and 2) stimulating RAD51, with thegoal of protecting normal tissues from cytotoxic therapies.The laboratory recently published its first study of RAD51-modifyingcompounds. This work involved a compound called RS-1, which wasidentified from a high-throughput chemical screen for compoundsthat enhance the ability of RAD51 to bind DNA. RS-1 was shown toenhance assembly of functional RAD51 protein filaments on DNA andDr. Rita Nandato stimulate HR activity in-vitro. When introduced into cells in culture,a significant dose dependent protection of normal human dermalfibroblasts was observed against the toxic effects of cisplatin. The protective effect was observed in the same concentrationrange (low micromolar) as was required for stimulation in biochemical assays. Work is ongoing to improve upon RS-1 activityvia medicinal chemistry collaborations and to identify newer, more active compounds.Planned and ongoing work will evaluate whether RAD51-stimulatory compounds can reduce mutagenesis and protect normaltissues from DNA-damaging therapies in animal models. The Bishop laboratory is also testing the ability of these compoundsto treat Fanconi Anemia (FA), a cancer susceptibility syndrome in which cells have impaired HR activity. Preliminary studiessuggest that some compounds can successfully rescue the HR deficiency of cells derived from FA patients. The laboratoryalso plans to explore the role of RAD51 expression, a new avenue of research derived from previous studies on homologousrecombination in budding yeast. This work demonstrated that under some circumstances, RAD51 (and its relative DMC1)forms non-recombinogenic complexes on DNA. Results from the laboratory suggest that these “dead-end” complexes canreduce the rate of cell proliferation. Studies are currently being initiated to determine if the high level of RAD51 expressionin tumor cells results in the formation of dead-end complexes. If so, the compounds that the laboratory has identified, whichstabilize the interaction of RAD51 with DNA, may enhance the ability of dead-end complexes to block replication of tumorcells.Clinical & ExperimentalTherapeuticsIn addition, the Bishop group is working on a new functional test of alleles of the breast cancer susceptibility gene, BRCA1.This test involves the DT40 cell line, which is a chicken Β lymphocyte cell line that exhibits high rates of homologousrecombination. Slight defects in BRCA1-dependent recombination and repair are detectable in these cells. The laboratory is inthe process of carrying out proof-of-principle experiments to determine how closely human BRCA1 function mirrors that ofchicken Brca1. If the function is conserved in chicken cells, the laboratory will be able to assess whether a particular variantof human BRCA1 is functionally defective. This work may potentially have important prognostic value as novel BRCA1variants are discovered.H. Rosie Xing, PhDAssistant Professor of PathologyThe core research conducted in the Xing laboratory is a mechanistic-driven, basic science program focused on translationalcancer biology. The main goals are to define the role of deregulated signaling transduction events in human oncogenesis andmetastatic dissemination, and to translate such mechanistic understanding for the development of novel cancer therapeuticagents and the design of multi-modality/multi-agent treatment strategies. Through intra- and inter-programmaticcollaborations, the laboratory has integrated approaches and tools of bioinformatics and systems biology (Yves Lussier,Clinical and Experimental Therapeutics Program), in vivo molecular imaging science (Chin-Tu Chen and Patrick LaRiviere, Advanced Imaging Program), cancer therapeutics (Everett Vokes, RalphWeischelbaum, Ezra Cohen, and TanguySeiwert, Clinical and Experimental Therapeutics Program), structural biology, and molecular pathology (Mark Lingen,Clinical and Experimental Therapeutics Program ) to accelerate discovery science and facilitate clinical translation. Thecombined expertise of the laboratory’s extended scientific collaborations facilitates investigations that are relevant to cancermanagement and have promising potential for translation.UCCRC SCIENTIFIC REPORT 200963
Using a structure-based rationale, the Xing laboratory targeted a non-ATP binding functional domain of KSR (a validatedeffector of oncogenic Ras) and conducted a virtual screening of an NCI compound library. A small molecule inhibitor of KSR,which exhibits broad spectrum and potent anti-neoplastic activity in vitro, was identified and characterized. The laboratory iscurrently working with the NCI RAND program to develop this agent for potential clinical applications.In two recent studies conducted in squamous carcinoma of the head and neck (HNSCC), the Xing laboratory demonstrated howintegration of systems biology approaches accelerates the translation of discovery science. In the first study, the group reportedthe first computationally predicted and biologically validated microRNA-regulated protein-protein interaction network, anduncovered previously unknown connections between microRNA regulation, network topology, and expression dynamics.Further, the laboratory showed that miR-204, a computationally predicted and prioritized microRNA, is a potent suppressor ofHNSCC metastasis. A strong clinical association was shown between overexpression of functional miR-204 gene targets and anearlier relapse in a sub-type of HNSCC tumors expressing an EGFR-pathway signature.In the second study, the Xing group demonstrated that utilization of the systems strategy unbiasely and effectively identifiesderegulated signaling pathways and molecular networks associated with treatment resistance. Consequently, these aberrantsignaling mechanisms could be exploited for the development of “pathway rewiring”-based combinations as an alternative to theindividual gene target-based paradigm. Using this approach, the laboratory illustrated that HNSCC cancer cells can effectivelyexploit the molecular interactions between EGFR and mTOR to confer reciprocal resistance. Thus, the combination of anti-EGFR and anti-mTOR agents will likely achieve optimal prevention of resistance. Furthermore, the Xing laboratory studies therole of a permissive tumor stromal microenvironment in tumor initiation, maintenance and response to cancer. Using xenograftmodels of human cancer, the group demonstrated that in vivo administration of the combination regimen, including an EGFRand a mTOR inhibitor, through differential and effective co-targeting of cancer cells and tumor stroma, leads to HNSCC tumorregression. A Phase II trial is being planning at the University of Chicago to test the therapeutic efficacy of this combination forthe treatment of head and neck cancer.In a separate study, the laboratory used a molecular in vivo optical imaging approach to characterize tumor vascular responseto anti-cancer therapies. The feasibility of serial imaging of tumor vascular response was demonstrated in real-time using livemice, providing the first in vivo experimental evidence that the effectiveness of anti-angiogenic agents can be achieved eitherthrough vessel destruction or, alternatively, through normalization. This approach will be used in combination with clinicallyrelevantimaging modalities (PET/CT/SPECT) to derive translational imaging markers in future studies.Pharmacogenomics of Anticancer AgentsMike Maitland, MD, PhDAssistant Professor of MedicineDr. Maitland leads the Biomarker Development Laboratory, aresearch program that bridges the Core Laboratories and theclinical elements of the Cancer Center’s Clinical and ExperimentalTherapeutics Program. Biomarkers are characteristics that areobjectively measured and frequently evaluated as indicators ofdisease processes or responses to drug treatment. Biomarkerscan be helpful tools for speeding the development of or betterDr. Philip Connellpersonalizing the use of new cancer therapies. Dr. Maitland’slaboratory addresses the many obstacles between discovering biomarkers and making them useful for advancing cancer care.Currently, his program focuses on developing biomarkers to improve the use of angiogenesis inhibitors.64In the past year, Dr. Maitland’s team has made two important discoveries on how cancer patients differ in response toangiogenesis inhibitors. Understanding these differences will likely facilitate safer and more effective dosing of these drugs. Forexample, many patients develop high blood pressure when administered FDA-approved agents in this class of drugs, includingAvastin, Nexavar (generic = sorafenib), or Sutent (generic = sunitinib). The time required for this effect was unclear,UCCRC SCIENTIFIC REPORT 2009
and whether the effect occurred only in patients with pre-existing hypertension was unknown. Supported, in part, by aUniversity of Chicago Cancer Research Center protocol-specific grant, the research team measured changes in blood pressurewith state-of-the-art equipment and detected changes on the very first day of treatment, much earlier than had been thought.After 7 days, the average blood pressure increased from 121/71 mmHg to 132/79 mmHg, and most patients experiencedapproximately 10 mmHg systolic and 8 mmHg diastolic increases in blood pressure. However, 14/54 patients had no increase,whereas 8/54 had large increases in blood pressure. One explanation for the wide variation in response is that patients withno increase in blood pressure are under-dosed, those with the high increases in blood pressure are overdosed, and that bloodpressure can be used to guide safe dosing of these drugs. The research team is now conducting a follow-up trial to test thisconcept.The Biomarker Development Laboratory has also been studying a blood protein marker, sVEGFR2. Levels of sVEGFR2decrease following the administration of sorafenib, sunitinib, or similar drug therapies, but also vary between individuals.Understanding the mechanism of sVEGFR2 variation may provide clues for why these drugs are more effective in selectpatients. Dr. Maitland’s group learned that levels of sVEGFR2 vary in healthy individuals, are not dependent on the presenceof tumors, and do not change much with exercise. The research team collaborated with geneticists at the University ofMaryland who have studied a community with shared, well recorded ancestry and a lifestyle similar to that of their ancestors,the Old Order Amish of Lancaster, Pennsylvania. The team measured sVEGFR2 in over 700 Amish volunteers and performedgenetic mapping. Results indicate that one region of a single chromosome has a large effect on the variation of sVEGFR2levels across individuals. In future studies, the team will identify specific genes in the identified region in order to developa test that might predict therapeutic response to sorafenib, sunitinib, and other drugs in this important new class of anticanceragents.Clinical & ExperimentalTherapeuticsM. Eileen Dolan, PhDProfessor of MedicinePharmacogenetics aims at both maximizing efficacy and minimizing adverse effects of chemotherapy by identifying thegenetic component of variation in drug response. The overall goal of Dr. Dolan’s research program is to identify predictivepharmacogenetic markers in individuals at greatest risk for adverse events or non-response in efforts to improve currentoncology practice. The main approaches that are employed in the laboratory include the candidate gene approach and thewhole genome approach. The candidate gene approach considers only well understood genes and/or pathways involved inthe metabolism or mechanism of action of a given drug and is most effective if the gene product has a large effect on drugpharmacokinetics or pharmacodynamics. However, this is often not the case. Therefore, Dr. Dolan’s laboratory has takenadvantage of the whole genome approach in an attempt to disclose previously unknown relationships between genotypeor expression and a given phenotype such as drug toxicity. This approach can be used to link multiple single nucleotidepolymorphisms (SNPs) and haplotypes to drug response with no a priori assumptions. The Dolan group is developingstrategies to corroborate initial associations through replication in independent cohorts and/or through assessment of afunctional role of the associated SNPs or haplotypes.Specific aims of the Dolan laboratory are to 1) determine the underlying genetic and molecular mechanisms responsiblefor sensitivity to toxicities or non-response associated with chemotherapeutic agents; 2) build useful cellular models fordiscovery and validation of chemotherapeutic-specific genetic variants for clinical evaluation; 3) evaluate pharmacogeneticfindings related to chemotherapeutic agents in clinical trials; and 4) share information related to utility of cell lines fordiscovery and validation of genetic variants important in pharmacologic endpoints.Performing genome wide association studies with cancer patients is particularly difficult because of the large number ofpatients required and because most patients receive multiple drugs. Most importantly, chemotherapy cannot be givento unaffected family members for genetic studies; therefore, the Dolan laboratory studies cell lines from unaffectedindividuals that are part of the International HapMap project, which are rich in genotypic information. Cellular phenotypes,such as chemotherapeutic-induced toxicity or apoptosis, are evaluated for association with genotypes. Current avenuesof investigation include the incorporation of knowledge about microRNAs, the integration of epigenomic data, andUCCRC SCIENTIFIC REPORT 200965
incorporation of other genetic elements such as copy number variants (CNVs). The goal of the Dolan laboratory is to integrateall relevant data such as SNPs, CNVs, microRNAs, and DNA methylation changes, to assemble a comprehensive model forpredicting drug response and toxicity, which could serve as the basis for designing drug therapy based on a patient’s specificgenetic profile. However, interpreting this data to prospectively guide dosage and drug regimens will require large prospectiveclinical trials to validate the findings.In a recent study, the Dolan laboratory, using lymphoblastoid cell lines derived from individuals of European (CEU) or African(YRI) ancestry, identified genetic factors important in susceptibility to toxicity associated with cytarabine arabinoside (ara-C),an antimetabolite used to treat hematologic malignancies. The candidate gene approach identified SNP70 within deoxycytidinekinase (DCK), an enzyme involved in formation of AraCTP, the active drug form. LCLs that are heterozygous for SNP 70demonstrated an increased sensitivity to ara-C, higher mRNA expression of DCK, and significantly higher intracellular levels ofara-CTP compared to homozygous LCLs, suggesting that this SNP affects DCK function. Using the genome wide approach, thelaboratory interrogated more than 2 million SNPs for association with susceptibility to ara-C and focused on SNPs that affectedgene expression. A unique pharmacogenetic signature, consisting of 4 SNPs explaining 51% of the variability in sensitivity toara-C among the CEU and 5 SNPs explaining 58% of the variation among the YRI populations, was identified. Gene expressioncytotoxicityrelationships were validated for a subset of genes in a separate group of lymphoblastoid cell lines. These uniquegenetic signatures comprise novel genes that can now be studied further in functional studies and clinical trials.Interaction of Chemotherapy and RadiationRalph Weichselbaum, MDProfessor of Radiation and Cellular OncologyThe Weichselbaum laboratory is engaged in the investigationand clinical translation of two major gene therapies. Bothstrategies involve radiotherapy, combining activation ofcytotoxic/immune activating genes by radiation within areplication-defective adenoviruses and the activation ofreplication of genetically-engineered/attenuated herpes viruses.Research in the laboratory focuses on the identification ofbasic mechanisms and clinical translation of TNFerade withradiation, herpes simplex virus-1 (HSV-1) oncolytic therapy,gene signatures and radio-chemo resistance, immune responseto radiation therapy, and control of distant metastasis by radiation therapy.Dr. Kerstin StensonThe Weichselbaum laboratory has identified radiation response elements (RREs) in the EGR1 promoter that increase geneexpression in response to ionizing radiation. When cloned upstream of therapeutic genes, RREs permit spatial and temporalcontrol of transgene transcription. This approach was developed using tumor necrosis factor alpha (TNFα) as the therapeutictransgene. Although known to be a potent radiation sensitizer, systemic delivery of TNFα resulted in severe toxicity in phaseI studies. An adenovector (Ad) approach was used to design a replication-deficient Ad to transduce cells with the TNFαgene under the control of the RRE of EGR1 (Ad.EGR.TNFα). In preclinical animal models, Ad.EGR.TNFα combined withfractionated radiation produced enhanced expression of TNFα within tumor xenografts and tumor growth regression comparedwith Ad.EGR.TNFα or radiation alone. The laboratory has demonstrated that tumor-associated endothelium is the principaltarget for Ad.Egr.TNFα radiosensitization. TNFerade represents a potential therapeutic strategy that exploits nonoverlappingtoxicity to enhance the radiation response in human tumors compared with conventional radiation or chemoradiotherapy. Incollaboration with Dr. Everett Vokes and others, the effects of TNFerade will be tested in recurrent head and neck cancer andprostate cancer in phase I trials. A phase 3 trial in pancreatic cancer is currently underway.In collaboration with Bernard Roizman (Cell Signaling and Gene Regulation Program), the laboratory has studied activationof genetically engineered herpes viruses by ionizing radiation and reported that radiation enhances late viral gene expression66UCCRC SCIENTIFIC REPORT 2009
y activating late promoters as early as two hours after radiation. The radiation activation of late viral genes is mediated bythe P38 kinase pathway, which is not required for late viral gene expression. These results suggest that ionizing radiationupregulates late promoters active in the course of viral DNA synthesis and provide the basis for activating viral replication andtumor oncolysis, thereby overcoming attenuation of the virus.As a consequence of investigating the molecular basis of radioresistance, the Weichselbaum laboratory identified a geneticsignature in the interferon pathway, referred to as the interferon related gene signature for DNA damage (IRDS). Thelaboratory showed that experimentally-derived interferon-related, DNA-damage resistant signatures are associated withresistance and/or chemotherapy across different cancer cell lines. The IRDS genes, STAT-1, ISG 15, and IFIT1 all mediateexperimental resistance. In collaboration with Andy Minn (Cell Signaling and Gene Regulation Program), analysis of clinicaldatabases demonstrated that IRDS-positive and -negative states exist among common human cancers. In breast cancer, theefficacy of adjuvant chemotherapy and radiotherapy is predicted by the IRDS that is associated with a poor prognosis.In collaboration with Yang-Xin Fu (Immunology and Cancer Program), the laboratory is also studying anti-tumor immuneeffects mediated by radiotherapy. The Weichselbaum group has observed that reduction of tumor burden following modifiedhypofractionated radiotherapy depends in part on immune responses, and that hypofractionated radiotherapy increasesdendritic cell maturation for T cell priming, leading to reduction/eradication of primary tumor or metastasis in a CD8+ T celldependentfashion. The laboratory further demonstrated that radiation-initiated immune responses and tumor reduction areabrogated by conventional fractionated radiotherapy or adjuvant chemotherapy, but greatly amplified by local immunotherapy,leading to the eradication of metastasis. These results challenge the rationale for current commonly-used intensive radio/chemotherapy strategies and provides the basis for combination treatments with radiotherapy and immunotherapy.Clinical & ExperimentalTherapeuticsBakhtiar Yamini, MDAssistant Professor of SurgeryMalignant gliomas are the most common form of primary brain tumor. Patients with these lesions have an overall mediansurvival of approximately 1 year. Although ionizing radiation (IR) is the primary post surgical treatment modality, theaddition of chemotherapy has been shown to modestly improve patient prognosis. The monofunctional methylating agent,temozolomide (TMZ), has become the prototypical anti-glioma agent because of its relatively predictable toxicity and itsefficacy in combination with IR. Translational studies in Dr. Yamini’s laboratory focus on combining TMZ with IR and othertherapeutic modalities to improve anti-glioma treatment efficacy. In this regard, Dr. Yamini’s work is closely affiliated withDr. Ralph Weichselbaum. Studies in animal models of malignant glioma also involve the use of targeted nanoparticle vectors,which the laboratory is attempting to distribute through the brain by convection enhanced delivery (CED).Dr. Yamini’s laboratory is also examining the mechanism of action of methylating agents like TMZ. These studies haverevealed that methylators inhibit the activation of the transcription factor, nuclear factor-κB (NF-κB). Specifically, Dr.Yamini’s team has determined that inhibition of NF-κB is a response to mismatch repair (MMR)-directed processing of O 6 -methylguanine (O 6 -MeG), the primary cytotoxic lesion induced by TMZ. This pathway is important in the apoptotic responseto O 6 -MeG, and loss of the ability to inhibit NF-κB attenuates TMZ-induced killing. By mediating the O 6 -MeG-induced DNAdamage response, NF-κB acts in a damage-induced tumor suppressive manner, facilitating the apoptotic removal of irreparablydamaged cells. Dr. Yamini hopes that elucidating the role of NF-κB in the response to DNA methylation will not only enablethe design of new combination anti-glioma treatment strategies, but will also enable better understanding of the carcinogenicside-effects of methylating chemotherapeutic agents.Specific aims of the laboratory are to 1) examine the role of NF-κB in the response to DNA methylation damage; 2) investigateand develop combination anti-glioma treatment regimens that incorporate TMZ and IR and NF-κB modulation; and 3) developa nanoparticle vector for direct intraparenchymal delivery of therapeutic agent to the brain.After initially reporting that O 6 -MeG lesions block NF-κB DNA-binding, the laboratory has recently been investigating thesignaling for this pathway. Studies reveal that NF-κB functions as an effector mediating the MMR-directed apoptotic response.UCCRC SCIENTIFIC REPORT 200967
Additional Program Highlights*Research•• Crystal Structures of DNA/RNA Repair Enzymes AlkB and ABH2 Bound todsDNA. Escherichia coli AlkB and its human homologues ABH2 and ABH3 repairDNA/RNA base lesions by using a direct oxidative dealkylation mechanism. ChuanHe, PhD, and his colleagues determined the first crystal structures of AlkB-dsDNA andDrs. Richard Schilsky, Ezra Cohen, and Mark RatainABH2-dsDNA complexes, stabilized by a chemical cross-linking strategy. The study alsoreveals that AlkB uses an unprecedented base-flipping mechanism to access the damaged base: it squeezes together the twobases flanking the flipped-out one to maintain the base stack, explaining the preference of AlkB for repairing ssDNA lesionsover dsDNA ones. In addition, the first crystal structure of ABH2 provides a structural basis for designing inhibitors of thishuman DNA repair protein (Yang, et al., Nature 452:961-965, 2008).••Significance of MYCN amplification in international neuroblastoma staging system stage 1 and 2 neuroblastoma: areport from the International Neuroblastoma Risk Group database. Treatment of patients with localized neuroblastomawith unfavorable biologic features is controversial. To evaluate the outcome of children with low-stage MYCN-amplifiedneuroblastoma and develop a rational treatment strategy, Susan Cohn, MD, and her colleagues analyzed data from theInternational Neuroblastoma Risk Group (INRG) database containing 2,660 patients with low-stage (InternationalNeuroblastoma Staging System stages 1 and 2) neuroblastoma, known MYCN status, and available follow-up data. Resultsindicated that patients with MYCN-amplified, low-stage tumors had less favorable event-free survival (EFS) and overallsurvival (OS) than did patients with nonamplified tumors (53% +/- 8% and 72% +/- 7% v 90% +/- 1% and 98% +/- 1%,respectively). The data also suggest that tumor cell ploidy could potentially be used to identify candidates for reductions intherapy (Bagatell, et al., J Clin Oncol 27(3):365-70, 2008).••A chemical compound that stimulates the human homologous recombination protein RAD51. RAD51 and othermembers of the RecA family of strand exchange proteins assemble on ssDNA to form presynaptic filaments, whichcarry out the central steps of homologous recombination. A microplate-based assay was developed for high-throughputmeasurement of hRAD51 filament formation on ssDNA. With this method, Philip Connell, MD, and colleagues includingRalph Weichselbaum, MD, and Douglas Bishop, PhD, screened a 10,000 compound library, leading to the identification of asmall molecule (RS-1) that enhances hRAD51 binding in a wide range of biochemical conditions. Results indicate that RS-1enhances the homologous recombination activity of hRAD51 by promoting the formation of active presynaptic filaments.Cell survival assays in normal neonatal human dermal fibroblasts demonstrated that RS-1 promotes a dose-dependentresistance to the cross-linking chemotherapeutic drug cisplatin. Given that RAD51-dependent recombination is a majordeterminant of cisplatin resistance, RS-1 seems to stimulate homologous recombination repair proficiency, and has manypotential applications in both research and medical settings. (Jayathilaka, et al., Proc Natl Acad Sci USA 105(41):15848-532008, 2008).••Comprehensive pharmacogenetic analysis of irinotecan neutropenia and pharmacokinetics. Federico Innocenti, MD,PhD, along with collaborators including M. Eileen Dolan, PhD and Mark Ratain, MD, identified genetic variation, in additionto the UGT1A1*28 polymorphism, that can explain the variability in irinotecan (CPT-11) pharmacokinetics and neutropeniain cancer patients. Using clinical and genetic data from 85 advanced cancer patients treated with single-agent CPT-11 every3 weeks at doses of 300 mg/m 2 and 350 mg/m 2 , forty-two common variants were genotyped in 12 candidate genes of the CPT-11 pathway. Based on this exploratory analysis, common polymorphisms in genes encoding for ABC and SLC transportersmay have a significant impact on the pharmacokinetics and pharmacodynamics of CPT-11 (Innocenti, et al., J Clin Oncol27(16):2604-14, 2009).••The MET receptor tyrosine kinase is a potential novel therapeutic target for head and neck squamous cell carcinoma.Recurrent/metastatic head and neck cancer remains a devastating disease with insufficient treatment options. TanguySeiwert, MD, and collaborators including Everett Vokes, MD, and Ravi Salgia, MD, PhD (Cell Signaling and Gene RegulationProgram), investigated the MET receptor tyrosine kinase as a novel target for the treatment of head and neck squamous68UCCRC SCIENTIFIC REPORT 2009* Due to space constraints, only a small representative sample of Program highlights is presented here.
cell carcinoma (HNSCC). An analysis of HNSCC tissue samples and cell lines indicatedthat MET is functionally important with prominent overexpression, increased genecopy number, and mutations. MET inhibition abrogated MET functions, includingproliferation, migration/motility, and angiogenesis, indicating that MET is a promising,novel target for HNSCC and that combination approaches with cisplatin or EGFRinhibitors should be explored. (Seiwert, et al., Cancer Res 69(7):3021-31, 2009).Dr. Walter Stadler••Patient anxiety about prostate cancer independently predicts early initiation of androgen deprivation therapy forbiochemical cancer recurrence in older men: a prospective cohort study. Androgen deprivation therapy (ADT) is firstlinetherapy for patients with prostate cancer (PCA) who experience biochemical recurrence (BCR). However, the optimaltiming of ADT initiation is uncertain, and earlier ADT initiation can cause toxicities that lower quality of life (QOL).Walter Stadler, MD, and his colleagues tested the hypothesis that elevated cancer anxiety leads to earlier ADT initiationfor BCR in older men. Results from a prospective cohort study reveal that cancer anxiety independently and robustlypredicts earlier ADT initiation in older men with BCR. For older patients with PCA, earlier ADT initiation may notchange life expectancy and can negatively impact QOL. PCA-specific anxiety is a potential target for a decision-makingintervention in this setting (Dale, et al., J Clin Oncol 27(10):1557-63, 2009).Selected New Funding•• Chun-Su Yuan, MD, PhD, is the primary investigator in a program project (P01), funded by the National Center forComplementary and Alternative Medicine of the National Institutes of Health, to study two selected botanicals,unsteamed and steamed American ginseng and notoginseng, as agents against colorectal cancer. The overall goal ofthe project is to characterize the anti-tumor activities and mechanisms of action of these two herbs and their activeconstituents through collaborative efforts with Tong-Chuan He, MD, PhD and Wei Du, PhD (members of the CellSignaling and Gene Regulation Program).Clinical & ExperimentalTherapeutics••••••Bakhtiar Yamini, MD, with funding from the National Institutes of Health, is investigating nanoparticles and andnanocapsules for glioma targeting. In collaboration with researchers at Argonne National Lab and LNKChemsolutions,Dr. Yamini will optimize the fabrication of PLGA/Fe3O4 nanoparticles that encapsulate therapeutic agent and can bedistributed by convection enhanced delivery (CED) through the brain. The hypothesis is that the nanoparticles can betracked using in vivo MR imaging during treatment.M. Eileen Dolan, PhD is the recipient of an R21 grant from the National Cancer Institute to determine the underlyingcause for the inter-ethnic differences in sensitivity to chemotherapy. The overall goal is to develop an unbiased genomewidemodel to identify germline genetic variants, mRNA or miRNA expression including those in an underservedpopulation, that predict risk for adverse reactions and non-response to chemotherapy.Everett Vokes, MD, received funding from the American Society of Clinical Oncology to study concomitantchemoradiotherapy and translational gene therapy for intermediate stage malignancy of the lung, head, and neck. Thestudy aims to investigate the use of TNFerade as a radiation sensitizer. TNFerade consists of the TNF gene linked to aradiation inducible promoter and an adenovirus for delivery to tumor cells. Dr. Vokes is also studying gene therapy withan oncolytic herpes simplex virus analog and investigating the role of the cMet pathway in possible prevention strategiesand therapeutic interventions.New Faculty Recruitments and UCCRC MembersScott Eggener, MD specializes in the care of patients with urologic cancers, utilizing surgical, medical, and for selectpatients, non-interventional approaches. His research focuses on improving surgical techniques, optimizing outcomes, andoffering clinical trials for patients with kidney, bladder, testicular, and prostate cancer.Arieh Shalhav, MD is a pioneer in minimally-invasive laparoscopic urologic surgery. He has the most extensive experience inthe country in laparoscopic surgery of the kidney. Dr. Shalhav’s research has enhanced medical professionals’ understandingof the effects of renal ischemia and ways to avoid its related damage during surgery.UCCRC SCIENTIFIC REPORT 200969
Selected Publications* : Intraprogrammatic Collaboration# : Interprogrammatic CollaborationBishop, Douglas PhD* Jayathilaka K, Sheridan SD, Bold TD, Bochenska K, Logan HL, WeichselbaumRR, Bishop DK, Connell PP. A chemical compound that stimulates thehuman homologous recombination protein RAD51. Proc Natl Acad Sci U S A105(41):15848-53, 2008.Sheridan SD, Yu X, Roth R, Heuser JE, Sehorn MG, Sung P, Egelman EH, BishopDK. A comparative analysis of Dmc1 and Rad51 nucleoprotein filaments.Nucleic Acids Res 36(12):4057-66, 2008.# Longerich S, Orelli BJ, Martin RW, Bishop DK, Storb U. Brca1 inimmunoglobulin gene conversion and somatic hypermutation. DNA Repair(Amst) 7(2):253-66, 2008.Ferrari SR, Grubb J, Bishop DK. The Mei5-Sae3 protein complex mediatesDmc1 activity in Saccharomyces cerevisiae. J Biol Chem 284(18):11766-70, 2009.Blair, Elizabeth MD* Salama JK, Stenson KM, List MA, Mell LK, Maccracken E, Cohen EE, Blair E,Vokes EE, Haraf DJ. Characteristics associated with swallowing changes afterconcurrent chemotherapy and radiotherapy in patients with head and neckcancer. Arch Otolaryngol Head Neck Surg 134(10):1060-5, 2008.* # Cohen EE, Baru J, Huo D, Haraf DJ, Crowley M, Witt ME, Blair EA,Weichselbaum RR, Rosen F, Vokes EE, Stenson K. Efficacy and safety of treatingT4 oral cavity tumors with primary chemoradiotherapy. Head Neck 31(8):1013-21, 2009.* Cohen EE, Davis DW, Karrison TG, Seiwert TY, Wong SJ, Nattam S, KozloffMF, Clark JI, Yan DH, Liu W, Pierce C, Dancey JE, Stenson K, Blair E, Dekker A,Vokes EE. Erlotinib and bevacizumab in patients with recurrent or metastaticsquamous-cell carcinoma of the head and neck: a phase I/II study. LancetOncol 10(3):247-57, 2009.Cohen, Ezra MD* Seiwert TY, Haraf DJ, Cohen EE, Stenson K, Witt ME, Dekker A,Kocherginsky M, Weichselbaum RR, Chen HX, Vokes EE. Phase I study ofbevacizumab added to fluorouracil- and hydroxyurea-based concomitantchemoradiotherapy for poor-prognosis head and neck cancer. J Clin Oncol. Apr1, 26(10):1732-41, 2008.* Seiwert TY, Cohen EE. Targeting angiogenesis in head and neck cancer.Semin Oncol 35(3):274-85, 2008.* # Cohen EE, Zhu H, Lingen MW, Martin LE, Kuo WL, Choi EA,Kocherginsky M, Parker JS, Chung CH, Rosner MR. A feed-forward loopinvolving protein kinase Calpha and microRNAs regulates tumor cell cycle.Cancer Res 69(1):65-74, 2009.* # Seiwert TY, Jagadeeswaran R, Faoro L, Janamanchi V, Nallasura V, ElDinali M, Yala S, Kanteti R, Cohen EE, Lingen MW, Martin L, Krishnaswamy S,Klein-Szanto A, Christensen JG, Vokes EE, Salgia R. The MET receptor tyrosinekinase is a potential novel therapeutic target for head and neck squamous cellcarcinoma. Cancer Res 69(7):3021-31, 2009.* Cohen EE, Davis DW, Karrison TG, Seiwert TY, Wong SJ, Nattam S, KozloffMF, Clark JI, Yan DH, Liu W, Pierce C, Dancey JE, Stenson K, Blair E, Dekker A,Vokes EE. Erlotinib and bevacizumab in patients with recurrent or metastaticsquamous-cell carcinoma of the head and neck: a phase I/II study. LancetOncol 10(3):247-57, 2009.Cohn, Susan MDSchneiderman J, London WB, Brodeur GM, Castleberry RP, Look AT, CohnSL. Clinical significance of MYCN amplification and ploidy in favorable-stageneuroblastoma: a report from the Children’s Oncology Group. J Clin Oncol26(6):913-8, 2008.Fox E, Maris JM, Widemann BC, Goodspeed W, Goodwin A, KromplewskiM, Fouts ME, Medina D, Cohn SL, Krivoshik A, Hagey AE, Adamson PC,Balis FM. A phase I study of ABT-751, an orally bioavailable tubulin inhibitor,administered daily for 21 days every 28 days in pediatric patients with solidtumors. Clin Cancer Res 14(4):1111-5, 2008.Hartford C, Volchenboum SL, Cohn SL. 3 + 3 not equal to (Rolling) 6. J ClinOncol 26(2):170-1, 2008.Cohn SL, Pearson AD, London WB, Monclair T, Ambros PF, Brodeur GM,Faldum A, Hero B, Iehara T, Machin D, Mosseri V, Simon T, Garaventa A,Castel V, Matthay KK. The International Neuroblastoma Risk Group (INRG)classification system: an INRG Task Force report. J Clin Oncol 27(2):289-97,2009.Monclair T, Brodeur GM, Ambros PF, Brisse HJ, Cecchetto G, Holmes K,Kaneko M, London WB, Matthay KK, Nuchtern JG, von Schweinitz D, SimonT, Cohn SL, Pearson AD. The International Neuroblastoma Risk Group (INRG)staging system: an INRG Task Force report. J Clin Oncol 27(2):298-303, 2009.Bagatell R, Beck-Popovic M, London WB, Zhang Y, Pearson AD, MatthayKK, Monclair T, Ambros PF, Cohn SL. Significance of MYCN amplificationin international neuroblastoma staging system stage 1 and 2 neuroblastoma:a report from the International Neuroblastoma Risk Group database. J ClinOncol 27(3):365-70, 2009.Connell, Philip MD* Jayathilaka K, Sheridan SD, Bold TD, Bochenska K, Logan HL, WeichselbaumRR, Bishop DK, Connell PP. A chemical compound that stimulates thehuman homologous recombination protein RAD51. Proc Natl Acad Sci U S A105(41):15848-53, 2008.Connell PP, Hellman S. Advances in radiotherapy and implications for the nextcentury: a historical perspective. Cancer Res 69(2):383-92, 2009.Dawson, Glyn PhDKilkus JP, Goswami R, Dawson SA, Testai FD, Berdyshev EV, Han X, DawsonG. Differential regulation of sphingomyelin synthesis and catabolism inoligodendrocytes and neurons. J Neurochem 106(4):1745-57, 2008.Qin J, Goswami R, Dawson S, Dawson G. Expression of the receptor foradvanced glycation end products in oligodendrocytes in response to oxidativestress. J Neurosci Res 86(11):2414-22, 2008.Dolan, M. Eileen PhD# Huang RS, Chen P, Wisel S, Duan S, Zhang W, Cook EH, Das S, Cox NJ,Dolan ME. Population Specific GSTM1 Copy Number Variation. Hum MolGenet 18(2):366-72, 2009.# Huang RS, Duan S, Kistner EO, Bleibel WK, Delaney SM, Fackenthal DL,Das S, Dolan ME. Genetic variants contributing to daunorubicin-inducedcytotoxicity. Cancer Res 68(9):3161-8, 2008.# Duan S, Huang RS, Zhang W, Bleibel WK, Roe CA, Clark TA, ChenTX, Schweitzer AC, Blume JE, Cox NJ, Dolan ME. Genetic architecture oftranscript-level variation in humans. Am J Hum Genet 82(5):1101-13, 2008.# Zhang W, Duan S, Kistner EO, Bleibel WK, Huang RS, Clark TA, Chen TX,Schweitzer AC, Blume JE, Cox NJ, Dolan ME. Evaluation of genetic variationcontributing to differences in gene expression between populations. Am J HumGenet 82(3):631-40, 2008.Shukla SJ, Duan S, Badner JA, Wu X, Dolan ME. Susceptibility loci involvedin cisplatin-induced cytotoxicity and apoptosis. Pharmacogenet Genomics18(3):253-62, 2008.Duan S, Huang RS, Zhang W, Mi S, Bleibel WK, Kistner EO, Cox NJ, DolanME. Expression and alternative splicing of folate pathway genes in HapMaplymphoblastoid cell lines. Pharmacogenomics 10(4):549-63, 2009.Hartford CM, Duan S, Delaney SM, Mi S, Kistner EO, Lamba JK, Huang RS,Dolan ME. Population-specific genetic variants important in susceptibility tocytarabine arabinoside cytotoxicity. Blood 113(10):2145-53, 2009.Eggener, Scott MDEggener SE, Yossepowitch O, Roehl KA, Loeb S, Yu X, Catalona WJ.Relationship of prostate-specific antigen velocity to histologic findings in aprostate cancer screening program. Urology 71(6):1016-9, 2008.Eggener SE, Yossepowitch O, Kundu S, Motzer RJ, Russo P. Risk score andmetastasectomy independently impact prognosis of patients with recurrentrenal cell carcinoma. J Urol 180(3):873-8, discussion 878, 2008.Yossepowitch O, Thompson RH, Leibovich BC, Eggener SE, Pettus JA,Kwon ED, Herr HW, Blute ML, Russo P. Positive surgical margins at partialnephrectomy: predictors and oncological outcomes. J Urol 179(6):2158-63,2008.Berglund RK, Masterson TA, Vora KC, Eggener SE, Eastham JA, GuillonneauBD. Pathological upgrading and up staging with immediate repeat biopsy inpatients eligible for active surveillance. J Urol 180(5):1964-7, discussion 1967-8,2008.70UCCRC SCIENTIFIC REPORT 2009
Eggener SE, Mueller A, Berglund RK, Ayyathurai R, Soloway C, Soloway MS,Abouassaly R, Klein EA, Jones SJ, Zappavigna C, Goldenberg L, ScardinoPT, Eastham JA, Guillonneau B. A multi-institutional evaluation of activesurveillance for low risk prostate cancer. J Urol 181(4):1635-41, discussion 1641,2009.Eggener SE. The clinical diversity of postchemotherapy germ cell teratoma.Cancer 115(6):1138-41, 2009.Eggener SE, Vickers AJ, Serio AM, Donovan MJ, Khan FM, Bayer-Zubek V,Verbel D, Cordon-Cardo C, Reuter VE, Bianco FJ Jr, Scardino PT. Comparisonof models to predict clinical failure after radical prostatectomy. Cancer115(2):303-10, 2009.Ferguson, Mark MD* Choong NW, Vokes EE, Haraf DJ, Tothy PK, Ferguson MK, Kasza K, RudinCM, Hoffman PC, Krauss SA, Szeto L, Mauer AM. Phase I study of inductionchemotherapy and concomitant chemoradiotherapy with irinotecan,carboplatin, and paclitaxel for stage III non-small cell lung cancer. J ThoracOncol 3(1):59-67, 2008.* # Konda VJ, Ross AS, Ferguson MK, Hart JA, Lin S, Naylor K, Noffsinger A,Posner MC, Dye C, Cislo B, Stearns L, Waxman I. Is the risk of concomitantinvasive esophageal cancer in high-grade dysplasia in Barrett’s esophagusoverestimated?. Clin Gastroenterol Hepatol 6(2):159-64, 2008.Ferguson MK, Lehman AG, Bolliger CT, Brunelli A. The role of diffusingcapacity and exercise tests. Thorac Surg Clin 18(1):9-17, v, 2008.Ferguson MK, Vigneswaran WT. Diffusing capacity predicts morbidity afterlung resection in patients without obstructive lung disease. Ann Thorac Surg85(4):1158-64, discussion 1164-5, 2008.Ferguson MK, Vigneswaran WT. Changes in patient presentation andoutcomes for major lung resection over three decades. Eur J Cardiothorac Surg33(3):497-501, 2008.* # Jagadeeswaran R, Surawska H, Krishnaswamy S, Janamanchi V, MackinnonAC, Seiwert TY, Loganathan S, Kanteti R, Reichman T, Nallasura V, SchwartzS, Faoro L, Wang YC, Girard L, Tretiakova MS, Ahmed S, Zumba O, SouliiL, Bindokas VP, Szeto LL, Gordon GJ, Bue. Paxillin is a target for somaticmutations in lung cancer: implications for cell growth and invasion. Cancer Res68(1):132-42, 2008.Ferguson MK, Parma CM, Celauro AD, Vigneswaran WT. Quality of life andmood in older patients after major lung resection. Ann Thorac Surg 87(4):1007-12, discussion 1012-3, 2009.Fichera, Alessandro MD* # Dougherty U, Sehdev A, Cerda S, Mustafi R, Little N, Yuan W,Jagadeeswaran S, Chumsangsri A, Delgado J, Tretiakova M, Joseph L, Hart J,Cohen EE, Aluri L, Fichera A, Bissonnette M. Epidermal growth factor receptorcontrols flat dysplastic aberrant crypt foci development and colon cancerprogression in the rat azoxymethane model. Clin Cancer Res 14(8):2253-62,2008.# Delgado JS, Mustafi R, Yee J, Cerda S, Chumsangsri A, Dougherty U,Lichtenstein L, Fichera A, Bissonnette M. Sorafenib Triggers Antiproliferativeand Pro-Apoptotic Signals in Human Esophageal Adenocarcinoma Cells. DigDis Sci 53(12):3055-64, 2008.# Khare S, Mustafi R, Cerda S, Yuan W, Jagadeeswaran S, Dougherty U,Tretiakova M, Samarel A, Cohen G, Wang J, Moore C, Wali R, Holgren C,Joseph L, Fichera A, Li YC, Bissonnette M. Ursodeoxycholic acid suppressesCox-2 expression in colon cancer: roles of Ras, p38, and CCAAT/enhancerbindingprotein. Nutr Cancer 60(3):389-400, 2008.# Park SM, Rajapaksha TW, Zhang M, Sattar HA, Fichera A, Ashton-RickardtPG, Peter ME. CD95 signaling deficient mice with a wild-type hematopoieticsystem are prone to hepatic neoplasia. Apoptosis 13(1):41-51, 2008.* Fichera A, Silvestri MT, Hurst RD, Rubin MA, Michelassi F. LaparoscopicRestorative Proctocolectomy with Ileal Pouch Anal Anastomosis: AComparative Observational Study on Long-term Functional Results. JGastrointest Surg 13(3):526-32, 2009.* Silvestri MT, Hurst RD, Rubin MA, Michelassi F, Fichera A. Chronicinflammatory changes in the anal transition zone after stapled ileal pouch-analanastomosis: is mucosectomy a superior alternative?. Surgery 144(4):533-7,discussion 537-9, 2008.Holder-Murray J, Fichera A. Anal transition zone in the surgical managementof ulcerative colitis. World J Gastroenterol 15(7):769-73, 2009.Fleming, Gini MD* Rudin CM, Liu W, Desai A, Karrison T, Jiang X, Janisch L, Das S,Ramirez J, Poonkuzhali B, Schuetz E, Fackenthal DL, Chen P, ArmstrongDK, Brahmer JR, Fleming GF, Vokes EE, Carducci MA, Ratain MJ.Pharmacogenomic and pharmacokinetic determinants of erlotinibtoxicity. J Clin Oncol 26(7):1119-27, 2008.# Polite BN, Cirrincione C, Fleming GF, Berry DA, Seidman A, Muss H,Norton L, Shapiro C, Bakri K, Marcom K, Lake D, Schwartz JH, HudisC, Winer EP. Racial differences in clinical outcomes from metastaticbreast cancer: a pooled analysis of CALGB 9342 and 9840--Cancer andLeukemia Group B. J Clin Oncol 26(16):2659-65, 2008.* # Nimeiri HS, Oza AM, Morgan RJ, Friberg G, Kasza K, Faoro L,Salgia R, Stadler WM, Vokes EE, Fleming GF. Efficacy and safety ofbevacizumab plus erlotinib for patients with recurrent ovarian, primaryperitoneal, and fallopian tube cancer: a trial of the Chicago, PMH, andCalifornia Phase II Consortia. Gynecol Oncol 110(1):49-55, 2008.Garcia AA, Hirte H, Fleming G, Yang D, Tsao-Wei DD, Roman L,Groshen S, Swenson S, Markland F, Gandara D, Scudder S, Morgan R,Chen H, Lenz HJ, Oza AM. Phase II clinical trial of bevacizumab andlow-dose metronomic oral cyclophosphamide in recurrent ovariancancer: a trial of the California, Chicago, and Princess Margaret Hospitalphase II consortia. J Clin Oncol 26(1):76-82, 2008.# Grushko TA, Filiaci VL, Mundt AJ, Ridderstrale K, Olopade OI,Fleming GF. An exploratory analysis of HER-2 amplification andoverexpression in advanced endometrial carcinoma: a GynecologicOncology Group study. Gynecol Oncol 108(1):3-9, 2008.* # Melhem A, Yamada SD, Fleming GF, Delgado B, Brickley DR, WuW, Kocherginsky M, Conzen SD. Administration of Glucocorticoids toOvarian Cancer Patients Is Associated with Expression of the AntiapoptoticGenes SGK1 and MKP1/DUSP1 in Ovarian Tissues. ClinCancer Res 15(9):3196-204, 2009.Schultheis AM, Lurje G, Rhodes KE, Zhang W, Yang D, Garcia AA,Morgan R, Gandara D, Scudder S, Oza A, Hirte H, Fleming G, RomanL, Lenz HJ. Polymorphisms and clinical outcome in recurrent ovariancancer treated with cyclophosphamide and bevacizumab. Clin CancerRes 14(22):7554-63, 2008.Haraf, Daniel MD* Cohn AB, Lang PO, Agarwal JP, Peng SL, Alizadeh K, Stenson KM,Haraf DJ, Cohen EE, Vokes EE, Gottlieb LJ. Free-flap reconstruction inthe doubly irradiated patient population. Plast Reconstr Surg 122(1):125-32, 2008.* Knab BR, Salama JK, Solanki A, Stenson KM, Cohen EE, Witt ME,Haraf DJ, Vokes EE. Functional organ preservation with definitivechemoradiotherapy for T4 laryngeal squamous cell carcinoma. AnnOncol 19(9):1650-4, 2008.* Seiwert TY, Haraf DJ, Cohen EE, Stenson K, Witt ME, Dekker A,Kocherginsky M, Weichselbaum RR, Chen HX, Vokes EE. Phase I study ofbevacizumab added to fluorouracil- and hydroxyurea-based concomitantchemoradiotherapy for poor-prognosis head and neck cancer. J ClinOncol 26(10):1732-41, 2008.* # Choong NW, Mauer AM, Haraf DJ, Lester E, Hoffman PC, KozloffM, Lin S, Dancey JE, Szeto L, Grushko T, Olopade OI, Salgia R, VokesEE. Phase I trial of erlotinib-based multimodality therapy for inoperablestage III non-small cell lung cancer. J Thorac Oncol 3(9):1003-11, 2008.* Choong NW, Vokes EE, Haraf DJ, Tothy PK, Ferguson MK, Kasza K,Rudin CM, Hoffman PC, Krauss SA, Szeto L, Mauer AM. Phase I studyof induction chemotherapy and concomitant chemoradiotherapy withirinotecan, carboplatin, and paclitaxel for stage III non-small cell lungcancer. J Thorac Oncol 3(1):59-67, 2008.* # Salama JK, Chmura SJ, Mehta N, Yenice KM, Stadler WM, Vokes EE,Haraf DJ, Hellman S, Weichselbaum RR. An initial report of a radiationdose-escalation trial in patients with one to five sites of metastaticdisease. Clin Cancer Res 14(16):5255-9, 2008.* # Cohen EE, Baru J, Huo D, Haraf DJ, Crowley M, Witt ME, Blair EA,Weichselbaum RR, Rosen F, Vokes EE, Stenson K. Efficacy and safety oftreating T4 oral cavity tumors with primary chemoradiotherapy. HeadNeck 31(8):1013-21, 2009.Clinical & ExperimentalTherapeuticsUCCRC SCIENTIFIC REPORT 200971
Hart, John MD* # Dougherty U, Sehdev A, Cerda S, Mustafi R, Little N, Yuan W,Jagadeeswaran S, Chumsangsri A, Delgado J, Tretiakova M, Joseph L, Hart J,Cohen EE, Aluri L, Fichera A, Bissonnette M. Epidermal growth factor receptorcontrols flat dysplastic aberrant crypt foci development and colon cancerprogression in the rat azoxymethane model. Clin Cancer Res 14(8):2253-62,2008.# Nathanson JW, Yadron NE, Farnan J, Kinnear S, Hart J, Rubin DT. p53mutations are associated with dysplasia and progression of dysplasia in patientswith Crohn’s disease. Dig Dis Sci 53(2):474-80, 2008.* # Konda VJ, Ross AS, Ferguson MK, Hart JA, Lin S, Naylor K, Noffsinger A,Posner MC, Dye C, Cislo B, Stearns L, Waxman I. Is the risk of concomitantinvasive esophageal cancer in high-grade dysplasia in Barrett’s esophagusoverestimated?. Clin Gastroenterol Hepatol 6(2):159-64, 2008.# Tao Y, Hart J, Lichtenstein L, Joseph L, Ciancio M, Hu S, Chang EB,Bissonnette M. Inducible Heat Shock Protein70 Prevents Multifocal FlatDysplastic Lesions and Invasive Tumors in an Inflammatory Model of ColonCancer. Carcinogenesis 30(1):175-82, 2009.Li YR, Akbari E, Tretiakova MS, Hart J, Akbari M, Urbanski SJ, GaoZH. Primary hepatic malignant fibrous histiocytoma: clinicopathologiccharacteristics and prognostic value of ezrin expression. Am J Surg Pathol32(8):1144-58, 2008.Tretiakova MS, Hart J, Shabani-Rad MT, Zhang J, Gao ZH. Distinctionof hepatocellular adenoma from hepatocellular carcinoma with andwithout cirrhosis using E-cadherin and matrix metalloproteinaseimmunohistochemistry. Mod Pathol 22(8):1113-20, 2009.He, Chuan PhDQiu Z, Lu L, Jian X, He C. A diazirine-based nucleoside analogue for efficientDNA interstrand photocross-linking. J Am Chem Soc 130(44):14398-9, 2008.Jia G, Yang CG, Yang S, Jian X, Yi C, Zhou Z, He C. Oxidative demethylationof 3-methylthymine and 3-methyluracil in single-stranded DNA and RNA bymouse and human FTO. FEBS Lett 582(23-24):3313-9, 2008.Yang CG, Yi C, Duguid EM, Sullivan CT, Jian X, Rice PA, He C. Crystalstructures of DNA/RNA repair enzymes AlkB and ABH2 bound to dsDNA.Nature 452(7190):961-5, 2008.Shigdel UK, Zhang J, He C. Diazirine-based DNA photo-cross-linking probesfor the study of protein-DNA interactions. Angew Chem Int Ed Engl 47(1):90-3,2008.Lin Y, Zhao T, Jian X, Farooqui Z, Qu X, He C, Dinner AR, Scherer NF.Using the bias from flow to elucidate single DNA repair protein sliding andinteractions with DNA. Biophys J 96(5):1911-7, 2009.Yi C, Yang CG, He C. A Non-Heme Iron-Mediated Chemical Demethylation inDNA and RNA. Acc Chem Res, 2009.Shigdel UK, He C. A new 1’-methylenedisulfide deoxyribose that forms anefficient cross-link to DNA cytosine-5 methyltransferase (DNMT). J Am ChemSoc 130(52):17634-5, 2008.Hoffman, Philip MD* Miller AA, Wang XF, Gu L, Hoffman P, Khatri J, Dunphy F, Edelman MJ,Bolger M, Vokes EE, Green MR. Phase II randomized study of dose-densedocetaxel and cisplatin every 2 weeks with pegfilgrastim and darbepoetin alfawith and without the chemoprotector BNP7787 in patients with advanced nonsmallcell lung cancer (CALGB 30303). J Thorac Oncol 3(10):1159-65, 2008.* # Choong NW, Mauer AM, Haraf DJ, Lester E, Hoffman PC, Kozloff M, LinS, Dancey JE, Szeto L, Grushko T, Olopade OI, Salgia R, Vokes EE. Phase I trialof erlotinib-based multimodality therapy for inoperable stage III non-small celllung cancer. J Thorac Oncol 3(9):1003-11, 2008.* Choong NW, Vokes EE, Haraf DJ, Tothy PK, Ferguson MK, Kasza K, RudinCM, Hoffman PC, Krauss SA, Szeto L, Mauer AM. Phase I study of inductionchemotherapy and concomitant chemoradiotherapy with irinotecan,carboplatin, and paclitaxel for stage III non-small cell lung cancer. J ThoracOncol 3(1):59-67, 2008.Hurst, Roger MD* Fichera A, Silvestri MT, Hurst RD, Rubin MA, Michelassi F. LaparoscopicRestorative Proctocolectomy with Ileal Pouch Anal Anastomosis: AComparative Observational Study on Long-term Functional Results. JGastrointest Surg 13(3):526-32, 2009.* Silvestri MT, Hurst RD, Rubin MA, Michelassi F, Fichera A. Chronicinflammatory changes in the anal transition zone after stapled ileal pouch-analanastomosis: is mucosectomy a superior alternative?. Surgery 144(4):533-7,discussion 537-9, 2008.Innocenti, Federico MD, PhD* Undevia SD, Innocenti F, Ramirez J, House L, Desai AA, Skoog LA, Singh DA,Karrison T, Kindler HL, Ratain MJ. A phase I and pharmacokinetic study ofthe quinoxaline antitumour Agent R(+)XK469 in patients with advanced solidtumours. Eur J Cancer 44(12):1684-92, 2008.* # Innocenti F, Liu W, Fackenthal D, Ramirez J, Chen P, Ye X, WuX, Zhang W, Mirkov S, Das S, Cook E Jr, Ratain MJ. Single nucleotidepolymorphism discovery and functional assessment of variation in the UDPglucuronosyltransferase2B7 gene. Pharmacogenet Genomics 18(8):683-97,2008.* Innocenti F, Mirkov S, Nagasubramanian R, Ramirez J, Liu W, Bleibel WK,Shukla SJ, Hennessy K, Rosner GL, Cook E Jr, Eileen Dolan M, Ratain MJ. TheWerner’s syndrome 4330T>C (Cys1367Arg) gene variant does not affect thein vitro cytotoxicity of topoisomerase inhibitors and platinum compounds.Cancer Chemother Pharmacol 63(5):881-7, 2009.* Perera MA, Innocenti F, Ratain MJ. Pharmacogenetic testing for uridinediphosphate glucuronosyltransferase 1A1 polymorphisms: are we there yet?.Pharmacotherapy 28(6):755-68, 2008.* Rosner GL, Panetta JC, Innocenti F, Ratain MJ. Pharmacogenetic pathwayanalysis of irinotecan. Clin Pharmacol Ther 84(3):393-402, 2008.* # Innocenti F, Kroetz DL, Schuetz E, Dolan ME, Ramirez J, Relling M, ChenP, Das S, Rosner GL, Ratain MJ. Comprehensive Pharmacogenetic Analysis ofIrinotecan Neutropenia and Pharmacokinetics. J Clin Oncol 27(16):2604-14,2009.* Yong WP, Kim TW, Undevia SD, Innocenti F, Ratain MJ. R(+)XK469 inhibitshydroxylation of S-warfarin by CYP2C9. Eur J Cancer, 2009.Kaplan, Edwin MDLui WO, Zeng L, Rehrmann V, Deshpande S, Tretiakova M, Kaplan EL,Leibiger I, Leibiger B, Enberg U, Hoog A, Larsson C, Kroll TG. CREB3L2-PPARgamma fusion mutation identifies a thyroid signaling pathway regulatedby intramembrane proteolysis. Cancer Res 68(17):7156-64, 2008.Karrison, Theodore PhD* Rudin CM, Liu W, Desai A, Karrison T, Jiang X, Janisch L, Das S, Ramirez J,Poonkuzhali B, Schuetz E, Fackenthal DL, Chen P, Armstrong DK, BrahmerJR, Fleming GF, Vokes EE, Carducci MA, Ratain MJ. Pharmacogenomic andpharmacokinetic determinants of erlotinib toxicity. J Clin Oncol 26(7):1119-27,2008.# Zhang B, Karrison T, Rowley DA, Schreiber H. IFN-gamma- and TNFdependentbystander eradication of antigen-loss variants in established mousecancers. J Clin Invest 118(4):1398-404, 2008.* Undevia SD, Innocenti F, Ramirez J, House L, Desai AA, Skoog LA, Singh DA,Karrison T, Kindler HL, Ratain MJ. A phase I and pharmacokinetic study ofthe quinoxaline antitumour Agent R(+)XK469 in patients with advanced solidtumours. Eur J Cancer 44(12):1684-92, 2008.* # Hahn OM, Yang C, Medved M, Karczmar G, Kistner E, Karrison T,Manchen E, Mitchell M, Ratain MJ, Stadler WM. Dynamic contrast-enhancedmagnetic resonance imaging pharmacodynamic biomarker study of sorafenibin metastatic renal carcinoma. J Clin Oncol 26(28):4572-8, 2008.* # Odenike OM, Larson RA, Gajria D, Dolan ME, Delaney SM, Karrison TG,Ratain MJ, Stock W. Phase I study of the ribonucleotide reductase inhibitor3-aminopyridine-2-carboxaldehyde-thiosemicarbazone (3-AP) in combinationwith high dose cytarabine in patients with advanced myeloid leukemia. InvestNew Drugs 26(3):233-9, 2008.* Hartford CM, Desai AA, Janisch L, Karrison T, Rivera VM, Berk L, LoewyJW, Kindler H, Stadler WM, Knowles HL, Bedrosian C, Ratain MJ. A phaseI trial to determine the safety, tolerability, and maximum tolerated doseof deforolimus in patients with advanced malignancies. Clin Cancer Res15(4):1428-34, 2009.* Cohen EE, Davis DW, Karrison TG, Seiwert TY, Wong SJ, Nattam S, KozloffMF, Clark JI, Yan DH, Liu W, Pierce C, Dancey JE, Stenson K, Blair E, Dekker A,Vokes EE. Erlotinib and bevacizumab in patients with recurrent or metastaticsquamous-cell carcinoma of the head and neck: a phase I/II study. LancetOncol 10(3):247-57, 2009.72UCCRC SCIENTIFIC REPORT 2009
Kindler, Hedy MD* Undevia SD, Innocenti F, Ramirez J, House L, Desai AA, Skoog LA, Singh DA,Karrison T, Kindler HL, Ratain MJ. A phase I and pharmacokinetic study ofthe quinoxaline antitumour Agent R(+)XK469 in patients with advanced solidtumours. Eur J Cancer 44(12):1684-92, 2008.* # Mell LK, Schomas DA, Salama JK, Devisetty K, Aydogan B, Miller RC, JaniAB, Kindler HL, Mundt AJ, Roeske JC, Chmura SJ. Association between bonemarrow dosimetric parameters and acute hematologic toxicity in anal cancerpatients treated with concurrent chemotherapy and intensity-modulatedradiotherapy. Int J Radiat Oncol Biol Phys 70(5):1431-7, 2008.# Jackman DM, Kindler HL, Yeap BY, Fidias P, Salgia R, Lucca J, Morse LK,Ostler PA, Johnson BE, Janne PA. Erlotinib plus bevacizumab in previouslytreated patients with malignant pleural mesothelioma. Cancer 113(4):808-14,2008.* Kratzke RA, Wang X, Wong L, Kratzke MG, Green MR, Vokes EE, VogelzangNJ, Kindler HL, Kern JA. Response to the methylation inhibitor dihydro-5-azacytidine in mesothelioma is not associated with methylation of p16INK4a:results of cancer and leukemia group B 159904. J Thorac Oncol 3(4):417-21,2008.* Hartford CM, Desai AA, Janisch L, Karrison T, Rivera VM, Berk L, LoewyJW, Kindler H, Stadler WM, Knowles HL, Bedrosian C, Ratain MJ. A phaseI trial to determine the safety, tolerability, and maximum tolerated doseof deforolimus in patients with advanced malignancies. Clin Cancer Res15(4):1428-34, 2009.Tsao AS, Wistuba I, Roth JA, Kindler HL. Malignant pleural mesothelioma. JClin Oncol 27(12):2081-90, 2009.Simon GR, Verschraegen CF, Janne PA, Langer CJ, Dowlati A, Gadgeel SM,Kelly K, Kalemkerian GP, Traynor AM, Peng G, Gill J, Obasaju CK, KindlerHL. Pemetrexed plus gemcitabine as first-line chemotherapy for patientswith peritoneal mesothelioma: final report of a phase II trial. J Clin Oncol26(21):3567-72, 2008.Lingen, Mark DDS, PhD* Lingen MW, Kalmar JR, Karrison T, Speight PM. Critical evaluation ofdiagnostic aids for the detection of oral cancer. Oral Oncol 44(1):10-22, 2008.* # Jagadeeswaran R, Surawska H, Krishnaswamy S, Janamanchi V, MackinnonAC, Seiwert TY, Loganathan S, Kanteti R, Reichman T, Nallasura V, SchwartzS, Faoro L, Wang YC, Girard L, Tretiakova MS, Ahmed S, Zumba O, SouliiL, Bindokas VP, Szeto LL, Gordon GJ, Bue. Paxillin is a target for somaticmutations in lung cancer: implications for cell growth and invasion. Cancer Res68(1):132-42, 2008.Radhakrishnan R, Solomon M, Satyamoorthy K, Martin LE, Lingen MW.Tissue microarray - a high-throughput molecular analysis in head and neckcancer. J Oral Pathol Med 37(3):166-76, 2008.Hasina R, Whipple ME, Martin LE, Kuo WP, Ohno-Machado L, LingenMW. Angiogenic heterogeneity in head and neck squamous cell carcinoma:biological and therapeutic implications. Lab Invest 88(4):342-53, 2008.* # Cohen EE, Zhu H, Lingen MW, Martin LE, Kuo WL, Choi EA,Kocherginsky M, Parker JS, Chung CH, Rosner MR. A feed-forward loopinvolving protein kinase Calpha and microRNAs regulates tumor cell cycle.Cancer Res 69(1):65-74, 2009.* # Seiwert TY, Jagadeeswaran R, Faoro L, Janamanchi V, Nallasura V, ElDinali M, Yala S, Kanteti R, Cohen EE, Lingen MW, Martin L, Krishnaswamy S,Klein-Szanto A, Christensen JG, Vokes EE, Salgia R. The MET receptor tyrosinekinase is a potential novel therapeutic target for head and neck squamous cellcarcinoma. Cancer Res 69(7):3021-31, 2009.Hasina R, Martin LE, Kasza K, Jones CL, Jalil A, Lingen MW. ABT-510 is aneffective chemopreventive agent in the mouse 4-nitroquinoline 1-oxide modelof oral carcinogenesis. Cancer Prev Res (Phila Pa) 2(4):385-93, 2009.List, Marcy PhD* Salama JK, Stenson KM, List MA, Mell LK, Maccracken E, Cohen EE, Blair E,Vokes EE, Haraf DJ. Characteristics associated with swallowing changes afterconcurrent chemotherapy and radiotherapy in patients with head and neckcancer. Arch Otolaryngol Head Neck Surg 134(10):1060-5, 2008.* Paskett ED, Herndon JE 2nd, Day JM, Stark NN, Winer EP, Grubbs SS, PavyMD, Shapiro CL, List MA, Hensley ML, Naughton MA, Kornblith AB, HabinKR, Fleming GF, Bittoni MA. Applying a conceptual model for examininghealth-related quality of life in long-term breast cancer survivors: CALGBstudy 79804. Psychooncology 17(11):1108-20, 2008.Lussier, Yves MDJabado OJ, Liu Y, Conlan S, Quan PL, Hegyi H, Lussier Y, Briese T,Palacios G, Lipkin WI. Comprehensive viral oligonucleotide probe designusing conserved protein regions. Nucleic Acids Res 36(1):e3, 2008.# Sam LT, Mendonca EA, Li J, Blake J, Friedman C, Lussier YA.PhenoGO: an integrated resource for the multiscale mining of clinicaland biological data. BMC Bioinformatics 10 Suppl 2:S8, 2009.Liu Y, Sam L, Li J, Lussier YA. Robust methods for accurate diagnosisusing pan-microbiological oligonucleotide microarrays. BMCBioinformatics 10 Suppl 2:S11, 2009.Pantazatos SP, Li J, Pavlidis P, Lussier YA. of Neuroimaging andMicroarray Datasets through Mapping and Model-Theoretic SemanticDecomposition of Unstructured Phenotypes. Cancer Informatics :875–94, 2009.Yang X, Huang Y, Chen J, Xie J, Sun X, Lussier YA. Mechanism-AnchoredProfiling derived from Epigenetic Networks Predicts Outcome in AcuteLymphoblastic Leukemia. In press, BMC Bioinformatic.Maitland, Michael MD, PhDArcher SL, Gomberg-Maitland M, Maitland ML, Rich S, Garcia JG,Weir EK. Mitochondrial metabolism, redox signaling, and fusion:a mitochondria-ROS-HIF-1alpha-Kv1.5 O2-sensing pathway at theintersection of pulmonary hypertension and cancer. Am J Physiol HeartCirc Physiol 294(2):H570-8, 2008.* Moreno-Vinasco L, Gomberg-Maitland M, Maitland ML, Desai AA,Singleton PA, Sammani S, Sam L, Liu Y, Husain AN, Lang RM, RatainMJ, Lussier YA, Garcia JG. Genomic assessment of a multikinaseinhibitor, sorafenib, in a rodent model of pulmonary hypertension.Physiol Genomics 33(2):278-91, 2008.Maitland ML. Cardiovascular toxicity of new agents. Clin Adv HematolOncol 6(9):657-9, 2008.Snider KL, Maitland ML. Cardiovascular toxicities: clues to optimaladministration of vascular endothelial growth factor signaling pathwayinhibitors. Target Oncol 4(2):67-76, 2009.Minsky, Bruce MDAjani JA, Winter K, Komaki R, Kelsen DP, Minsky BD, Liao Z, BradleyJ, Fromm M, Hornback D, Willett CG. Phase II randomized trial oftwo nonoperative regimens of induction chemotherapy followed bychemoradiation in patients with localized carcinoma of the esophagus:RTOG 0113. J Clin Oncol 26(28):4551-6, 2008.# Liauw SL, Minsky BD. The use of capecitabine in the combinedmodalitytherapy for rectal cancer. Clin Colorectal Cancer 7(2):99-104,2008.Leibold T, Shia J, Ruo L, Minsky BD, Akhurst T, Gollub MJ, Ginsberg MS,Larson S, Riedel E, Wong WD, Guillem JG. Prognostic implications of thedistribution of lymph node metastases in rectal cancer after neoadjuvantchemoradiotherapy. J Clin Oncol 26(13):2106-11, 2008.Guillem JG, Diaz-Gonzalez JA, Minsky BD, Valentini V, Jeong SY,Rodriguez-Bigas MA, Coco C, Leon R, Hernandez-Lizoain JL, AristuJJ, Riedel ER, Nitti D, Wong WD, Pucciarelli S. cT3N0 rectal cancer:potential overtreatment with preoperative chemoradiotherapy iswarranted. J Clin Oncol 26(3):368-73, 2008.Nahas CS, Akhurst T, Yeung H, Leibold T, Riedel E, Markowitz AJ,Minsky BD, Paty PB, Weiser MR, Temple LK, Wong WD, LarsonSM, Guillem JG. Positron emission tomography detection of distantmetastatic or synchronous disease in patients with locally advancedrectal cancer receiving preoperative chemoradiation. Ann Surg Oncol15(3):704-11, 2008.Schwartz GK, Winter K, Minsky BD, Crane C, Thomson PJ, Anne P,Gross H, Willett C, Kelsen D. Randomized phase II trial evaluatingtwo paclitaxel and cisplatin-containing chemoradiation regimens asadjuvant therapy in resected gastric cancer (RTOG-0114). J Clin Oncol27(12):1956-62, 2009.Guillem JG, Minsky BD. Extended perineal resection of distal rectalcancers: surgical advance, increased utilization of neoadjuvant therapies,proper patient selection or all of the above?. J Clin Oncol 26(21):3481-2,2008.Clinical & ExperimentalTherapeuticsUCCRC SCIENTIFIC REPORT 200973
Nanda, Rita MD# Wei M, Xu J, Dignam J, Nanda R, Sveen L, Fackenthal J, Grushko TA,Olopade OI. Estrogen receptor alpha, BRCA1, and FANCF promotermethylation occur in distinct subsets of sporadic breast cancers. Breast CancerRes Treat 111(1):113-20, 2008.# Olopade OI, Grushko TA, Nanda R, Huo D. Advances in breast cancer:pathways to personalized medicine. Clin Cancer Res 14(24):7988-99, 2008.Peabody, Terrance MDCorby RR, Stacy GS, Peabody TD, Dixon LB. Radiofrequency ablation ofsolitary eosinophilic granuloma of bone. AJR Am J Roentgenol 190(6):1492-4,2008.# Ryan CW, Montag AG, Hosenpud JR, Samuels B, Hayden JB, Hung AY,Mansoor A, Peabody TD, Mundt AJ, Undevia S. Histologic response of doseintensechemotherapy with preoperative hypofractionated radiotherapy forpatients with high-risk soft tissue sarcomas. Cancer 112(11):2432-9.Posadas, Edwin MD* # Posadas EM, Al-Ahmadie H, Robinson VL, Jagadeeswaran R, Otto K, KaszaKE, Tretiakov M, Siddiqui J, Pienta KJ, Stadler WM, Rinker-Schaeffer C, SalgiaR. FYN is overexpressed in human prostate cancer. BJU Int., 2008.Dahut WL, Scripture C, Posadas E, Jain L, Gulley JL, Arlen PM, Wright JJ, Yu Y,Cao L, Steinberg SM, Aragon-Ching JB, Venitz J, Jones E, Chen CC, Figg WD.A phase II clinical trial of sorafenib in androgen-independent prostate cancer.Clin Cancer Res 14(1):209-14, 2008.Azad NS, Posadas EM, Kwitkowski VE, Steinberg SM, Jain L, Annunziata CM,Minasian L, Sarosy G, Kotz HL, Premkumar A, Cao L, McNally D, Chow C,Chen HX, Wright JJ, Figg WD, Kohn EC. Combination targeted therapy withsorafenib and bevacizumab results in enhanced toxicity and antitumor activity.J Clin Oncol 26(22):3709-14, 2008.* Bylow KA, Atkins MB, Posadas EM, Stadler WM, McDermott DF. PhaseII trial of carboplatin and paclitaxel in papillary renal cell carcinoma. ClinGenitourin Cancer 7(1):39-42, 2009.* Szmulewitz R, Mohile S, Posadas E, Kunnavakkam R, Karrison T, ManchenE, Stadler WM. A Randomized Phase 1 Study of Testosterone Replacement forPatients with Low-Risk Castration-Resistant Prostate Cancer. Eur Urol, 2009.* Lara PN Jr, Longmate J, Evans CP, Quinn DI, Twardowski P, Chatta G,Posadas E, Stadler W, Gandara DR. A phase II trial of the Src-kinase inhibitorAZD0530 in patients with advanced castration-resistant prostate cancer: aCalifornia Cancer Consortium study. Anticancer Drugs 20(3):179-84, 2009.Posner, Mitchell MD* Posner MC, Niedzwiecki D, Venook AP, Hollis DR, Kindler HL, MartinEW, Schilsky RL, Goldberg RM. A phase II prospective multi-institutionaltrial of adjuvant active specific immunotherapy following curative resectionof colorectal cancer hepatic metastases: cancer and leukemia group B study89903. Ann Surg Oncol 15(1):158-64, 2008.* # Konda VJ, Ross AS, Ferguson MK, Hart JA, Lin S, Naylor K, Noffsinger A,Posner MC, Dye C, Cislo B, Stearns L, Waxman I. Is the risk of concomitantinvasive esophageal cancer in high-grade dysplasia in Barrett’s esophagusoverestimated?. Clin Gastroenterol Hepatol 6(2):159-64, 2008.* # Bickenbach KA, Veerapong J, Shao MY, Mauceri HJ, Posner MC, Kron SJ,Weichselbaum RR. Resveratrol is an effective inducer of CArG-driven TNFalphagene therapy. Cancer Gene Ther 15(3):133-9, 2008.* Mauceri HJ, Beckett MA, Liang H, Sutton HG, Pitroda S, Galka E, EfimovaE, Darga T, Khodarev NN, King CR, Posner MC, Hellman S, Kufe DW,Weichselbaum RR. Translational strategies exploiting TNF-alpha that sensitizetumors to radiation therapy. Cancer Gene Ther 16(4):373-81, 2009.* Roach PB, Roggin KK, Selkov E Jr, Posner MC, Silverstein JC. Use of a novel,web-based educational platform facilitates intraoperative training in a surgicaloncology fellowship program. Ann Surg Oncol 16(5):1100-7, 2009.Khodarev NN, Roach P, Pitroda SP, Golden DW, Bhayani M, Shao MY, DargaTE, Beveridge MG, Sood RF, Sutton HG, Beckett MA, Mauceri HJ, PosnerMC, Weichselbaum RR. STAT1 Pathway Mediates Amplification of MetastaticPotential and Resistance to Therapy. PLoS ONE 4(6):e5821, 2009.Berman RS, Kurtzman SH, Posner MC, Gershenwald JE. Society of surgicaloncology fellowship training: Where we have been, where we are now, andwhere we are going. J Surg Oncol 100(3):179-81, 2009.Ratain, Mark MD* Daugherty CK, Ratain MJ, Emanuel EJ, Farrell AT, Schilsky RL. Ethical,scientific, and regulatory perspectives regarding the use of placebos in cancerclinical trials. J Clin Oncol 26(8):1371-8, 2008.* Rudin CM, Liu W, Desai A, Karrison T, Jiang X, Janisch L, Das S, Ramirez J,Poonkuzhali B, Schuetz E, Fackenthal DL, Chen P, Armstrong DK, BrahmerJR, Fleming GF, Vokes EE, Carducci MA, Ratain MJ. Pharmacogenomic andpharmacokinetic determinants of erlotinib toxicity. J Clin Oncol 26(7):1119-27,2008.* # Hahn OM, Yang C, Medved M, Karczmar G, Kistner E, Karrison T,Manchen E, Mitchell M, Ratain MJ, Stadler WM. Dynamic contrast-enhancedmagnetic resonance imaging pharmacodynamic biomarker study of sorafenibin metastatic renal carcinoma. J Clin Oncol 26(28):4572-8, 2008.* # Innocenti F, Liu W, Fackenthal D, Ramirez J, Chen P, Ye X, WuX, Zhang W, Mirkov S, Das S, Cook E Jr, Ratain MJ. Single nucleotidepolymorphism discovery and functional assessment of variation in the UDPglucuronosyltransferase2B7 gene. Pharmacogenet Genomics 18(8):683-97,2008.* Zhang W, Ratain MJ, Dolan ME. The HapMap Resource is Providing NewInsights into Ourselves and its Application to Pharmacogenomics. BioinformBiol Insights 2:15-23, 2008.* # Odenike OM, Larson RA, Gajria D, Dolan ME, Delaney SM, Karrison TG,Ratain MJ, Stock W. Phase I study of the ribonucleotide reductase inhibitor3-aminopyridine-2-carboxaldehyde-thiosemicarbazone (3-AP) in combinationwith high dose cytarabine in patients with advanced myeloid leukemia. InvestNew Drugs 26(3):233-9, 2008.* Rosner GL, Panetta JC, Innocenti F, Ratain MJ. Pharmacogenetic pathwayanalysis of irinotecan. Clin Pharmacol Ther 84(3):393-402, 2008.* Hartford CM, Desai AA, Janisch L, Karrison T, Rivera VM, Berk L, LoewyJW, Kindler H, Stadler WM, Knowles HL, Bedrosian C, Ratain MJ. A phaseI trial to determine the safety, tolerability, and maximum tolerated doseof deforolimus in patients with advanced malignancies. Clin Cancer Res15(4):1428-34, 2009.* # Innocenti F, Kroetz DL, Schuetz E, Dolan ME, Ramirez J, Relling M, ChenP, Das S, Rosner GL, Ratain MJ. Comprehensive Pharmacogenetic Analysis ofIrinotecan Neutropenia and Pharmacokinetics. J Clin Oncol 27(16):2604-14,2009.Roggin, Kevin MDBickenbach K, Galka E, Roggin KK. Molecular mechanisms ofcholangiocarcinogenesis: are biliary intraepithelial neoplasia and intraductalpapillary neoplasms of the bile duct precursors to cholangiocarcinoma?. SurgOncol Clin N Am 18(2):215-24, 2009.* Roach PB, Roggin KK, Selkov E Jr, Posner MC, Silverstein JC. Use of a novel,web-based educational platform facilitates intraoperative training in a surgicaloncology fellowship program. Ann Surg Oncol 16(5):1100-7, 2009.Rubin, Charles MD# Seibel NL, Steinherz PG, Sather HN, Nachman JB, Delaat C, Ettinger LJ,Freyer DR, Mattano LA Jr, Hastings CA, Rubin CM, Bertolone K, FranklinJL, Heerema NA, Mitchell TL, Pyesmany AF, La MK, Edens C, Gaynon PS.Early postinduction intensification therapy improves survival for children andadolescents with high-risk acute lymphoblastic leukemia: a report from theChildren’s Oncology Group. Blood 111(5):2548-55, 2008.Salama, Joseph MD* Salama JK, Stenson KM, List MA, Mell LK, Maccracken E, Cohen EE, Blair E,Vokes EE, Haraf DJ. Characteristics associated with swallowing changes afterconcurrent chemotherapy and radiotherapy in patients with head and neckcancer. Arch Otolaryngol Head Neck Surg 134(10):1060-5, 2008.* Salama JK, Stenson KM, Kistner EO, Mittal BB, Argiris A, Witt ME, RosenF, Brockstein BE, Cohen EE, Haraf DJ, Vokes EE. Induction chemotherapy andconcurrent chemoradiotherapy for locoregionally advanced head and neckcancer: a multi-institutional phase II trial investigating three radiotherapy doselevels. Ann Oncol 19(10):1787-94, 2008.* Knab BR, Salama JK, Solanki A, Stenson KM, Cohen EE, Witt ME, Haraf DJ,Vokes EE. Functional organ preservation with definitive chemoradiotherapy forT4 laryngeal squamous cell carcinoma. Ann Oncol 19(9):1650-4, 2008.* # Salama JK, Chmura SJ, Mehta N, Yenice KM, Stadler WM, Vokes EE,Haraf DJ, Hellman S, Weichselbaum RR. An initial report of a radiation doseescalationtrial in patients with one to five sites of metastatic disease. ClinCancer Res 14(16):5255-9, 2008.74UCCRC SCIENTIFIC REPORT 2009
* # Mell LK, Schomas DA, Salama JK, Devisetty K, Aydogan B, Miller RC, JaniAB, Kindler HL, Mundt AJ, Roeske JC, Chmura SJ. Association between bonemarrow dosimetric parameters and acute hematologic toxicity in anal cancerpatients treated with concurrent chemotherapy and intensity-modulatedradiotherapy. Int J Radiat Oncol Biol Phys 70(5):1431-7, 2008.* Macdermed DM, Weichselbaum RR, Salama JK. A rationale for the targetedtreatment of oligometastases with radiotherapy. J Surg Oncol 98(3):202-6, 2008.# Cao J, Roeske JC, Chmura SJ, Salama JK, Shoushtari AN, Boyer AL, MartelMK. Calculation and prediction of the effect of respiratory motion on wholebreast radiation therapy dose distributions. Med Dosim 34(2):126-32, 2009.Schilsky, Richard MDSchilsky RL. How not to treat cancer. Lancet Oncol 9(6):504-5, 2008.Zon R, Meropol NJ, Catalano RB, Schilsky RL. American Society of ClinicalOncology Statement on minimum standards and exemplary attributes ofclinical trial sites. J Clin Oncol 26(15):2562-7, 2008.* Strauss GM, Herndon JE 2nd, Maddaus MA, Johnstone DW, Johnson EA,Harpole DH, Gillenwater HH, Watson DM, Sugarbaker DJ, Schilsky RL,Vokes EE, Green MR. Adjuvant Paclitaxel Plus Carboplatin Compared WithObservation in Stage IB Non-Small-Cell Lung Cancer: CALGB 9633 With theCancer and Leukemia Group B, Radiation Therapy Oncology Group, and NorthCentral Cancer Treatment Group Study Groups. J Clin Oncol 26(31):5043-51,2008.Lamont EB, Herndon JE 2nd, Weeks JC, Henderson IC, Lilenbaum R, SchilskyRL, Christakis NA. Measuring clinically significant chemotherapy-relatedtoxicities using Medicare claims from Cancer and Leukemia Group B (CALGB)trial participants. Med Care 46(3):303-8, 2008.* Daugherty CK, Ratain MJ, Emanuel EJ, Farrell AT, Schilsky RL. Ethical,scientific, and regulatory perspectives regarding the use of placebos in cancerclinical trials. J Clin Oncol 26(8):1371-8, 2008.* Posner MC, Niedzwiecki D, Venook AP, Hollis DR, Kindler HL, MartinEW, Schilsky RL, Goldberg RM. A phase II prospective multi-institutionaltrial of adjuvant active specific immunotherapy following curative resectionof colorectal cancer hepatic metastases: cancer and leukemia group B study89903. Ann Surg Oncol 15(1):158-64, 2008.Schilsky RL, Gordon G, Gilmer TM, Courtneidge SA, Matrisian LM, GradO, Nelson WG. The Translational Research Working Group developmentalpathway for anticancer agents (drugs or biologics). Clin Cancer Res 14(18):5685-91, 2008.Seiwert, Tanguy MD* Seiwert TY, Haraf DJ, Cohen EE, Stenson K, Witt ME, Dekker A,Kocherginsky M, Weichselbaum RR, Chen HX, Vokes EE. Phase I study ofbevacizumab added to fluorouracil- and hydroxyurea-based concomitantchemoradiotherapy for poor-prognosis head and neck cancer. J Clin Oncol26(10):1732-41, 2008.* # Jagadeeswaran R, Surawska H, Krishnaswamy S, Janamanchi V, MackinnonAC, Seiwert TY, Loganathan S, Kanteti R, Reichman T, Nallasura V, SchwartzS, Faoro L, Wang YC, Girard L, Tretiakova MS, Ahmed S, Zumba O, SouliiL, Bindokas VP, Szeto LL, Gordon GJ, Bue. Paxillin is a target for somaticmutations in lung cancer: implications for cell growth and invasion. Cancer Res68(1):132-42, 2008.* Seiwert TY, Cohen EE. Targeting angiogenesis in head and neck cancer.Semin Oncol 35(3):274-85, 2008.* # Ma PC, Tretiakova MS, MacKinnon AC, Ramnath N, Johnson C, DietrichS, Seiwert T, Christensen JG, Jagadeeswaran R, Krausz T, Vokes EE, Husain AN,Salgia R. Expression and mutational analysis of MET in human solid cancers.Genes Chromosomes Cancer 47(12):1025-37, 2008.* # Faoro L, Loganathan S, Westerhoff M, Modi R, Husain AN, Tretiakova M,Seiwert T, Kindler HL, Vokes EE, Salgia R. Protein kinase C beta in malignantpleural mesothelioma. Anticancer Drugs 19(9):841-8, 2008.* # Seiwert TY, Jagadeeswaran R, Faoro L, Janamanchi V, Nallasura V, ElDinali M, Yala S, Kanteti R, Cohen EE, Lingen MW, Martin L, Krishnaswamy S,Klein-Szanto A, Christensen JG, Vokes EE, Salgia R. The MET receptor tyrosinekinase is a potential novel therapeutic target for head and neck squamous cellcarcinoma. Cancer Res 69(7):3021-31, 2009.* Cohen EE, Davis DW, Karrison TG, Seiwert TY, Wong SJ, Nattam S, KozloffMF, Clark JI, Yan DH, Liu W, Pierce C, Dancey JE, Stenson K, Blair E, Dekker A,Vokes EE. Erlotinib and bevacizumab in patients with recurrent or metastaticsquamous-cell carcinoma of the head and neck: a phase I/II study. LancetOncol 10(3):247-57, 2009.Shalhav, Arieh MD* Thong AE, Shikanov S, Katz MH, Gofrit ON, Eggener S, Zagaja GP,Shalhav AL, Zorn KC. A Single Microfocus (5% or Less) of Gleason6 Prostate Cancer at Biopsy-Can We Predict Adverse PathologicalOutcomes?. J Urol 180(6):2436-40, 2008.* Gofrit ON, Zorn KC, Silvestre J, Shalhav AL, Zagaja GP, Msezane LP,Steinberg GD. The predictive value of multi-targeted fluorescent in-situhybridization in patients with history of bladder cancer. Urol Oncol26(3):246-9, 2008.* Gofrit ON, Stadler WM, Zorn KC, Lin S, Silvestre J, Shalhav AL,Zagaja GP, Steinberg GD. Adjuvant chemotherapy in lymph node positivebladder cancer. Urol Oncol 27(2):160-4, 2009.* Gofrit ON, Zorn KC, Steinberg GD, Zagaja GP, Shalhav AL. The WillRogers phenomenon in urological oncology. J Urol 179(1):28-33, 2008.Shalhav AL, Shikanov SA. Does radiofrequency ablation preserve longtermrenal function in patients with small renal masses?. Nat Clin PractUrol 5(8):420-1, 2008.* Zorn KC, Bernstein AJ, Gofrit ON, Shikanov SA, Mikhail AA, SongDH, Zagaja GP, Shalhav AL. Long-term functional and oncologicaloutcomes of patients undergoing sural nerve interposition graftingduring robot-assisted laparoscopic radical prostatectomy. J Endourol22(5):1005-12, 2008.* Wiltz AL, Shikanov S, Eggener SE, Katz MH, Thong AE, SteinbergGD, Shalhav AL, Zagaja GP, Zorn KC. Robotic Radical Prostatectomy inOverweight and Obese Patients: Oncological and Validated-FunctionalOutcomes. Urology 73(2):316-22, 2009.Siegler, Mark MDTorke AM, Simmerling M, Siegler M, Kaya D, Alexander GC. Rethinkingthe ethical framework for surrogate decision making: a qualitative studyof physicians. J Clin Ethics 19(2):110-9, 2008.Cooley DA, Fung JJ, Young JB, Starzl TE, Siegler M, Chen PW. Transplantinnovation and ethical challenges: what have we learned? A collectionof perspectives and panel discussion. Cleve Clin J Med 75 Suppl 6:S24-9,discussion S30-2, 2008.Dugdale LS, Siegler M, Rubin DT. Medical professionalism and thedoctor-patient relationship. Perspect Biol Med 51(4):547-53, 2008.Song, David MD* Zorn KC, Bernstein AJ, Gofrit ON, Shikanov SA, Mikhail AA, SongDH, Zagaja GP, Shalhav AL. Long-term functional and oncologicaloutcomes of patients undergoing sural nerve interposition graftingduring robot-assisted laparoscopic radical prostatectomy. J Endourol22(5):1005-12, 2008.Wu LC, Iteld L, Song DH. Supercharging the transverse rectus abdominismusculocutaneous flap: breast reconstruction for the overweight andobese population. Ann Plast Surg 60(6):609-13, 2008.Reynolds WS, Gottlieb LJ, Lucioni A, Rapp DE, Song DH, BalesGT. Vesicovaginal fistula repair with rectus abdominus myofascialinterposition flap. Urology 71(6):1119-23, 2008.Stadler, Walter MD* # Hahn OM, Yang C, Medved M, Karczmar G, Kistner E, KarrisonT, Manchen E, Mitchell M, Ratain MJ, Stadler WM. Dynamic contrastenhancedmagnetic resonance imaging pharmacodynamic biomarkerstudy of sorafenib in metastatic renal carcinoma. J Clin Oncol26(28):4572-8, 2008.* # Nimeiri HS, Oza AM, Morgan RJ, Friberg G, Kasza K, Faoro L,Salgia R, Stadler WM, Vokes EE, Fleming GF. Efficacy and safety ofbevacizumab plus erlotinib for patients with recurrent ovarian, primaryperitoneal, and fallopian tube cancer: a trial of the Chicago, PMH, andCalifornia Phase II Consortia. Gynecol Oncol 110(1):49-55, 2008.* # Salama JK, Chmura SJ, Mehta N, Yenice KM, Stadler WM, Vokes EE,Haraf DJ, Hellman S, Weichselbaum RR. An initial report of a radiationdose-escalation trial in patients with one to five sites of metastaticdisease. Clin Cancer Res 14(16):5255-9, 2008.* # Posadas EM, Al-Ahmadie H, Robinson VL, Jagadeeswaran R, OttoK, Kasza KE, Tretiakov M, Siddiqui J, Pienta KJ, Stadler WM, Rinker-Schaeffer C, Salgia R. FYN is overexpressed in human prostate cancer.BJU Int 103(2):171-7, 2009.Clinical & ExperimentalTherapeuticsUCCRC SCIENTIFIC REPORT 200975
# Yang C, Karczmar GS, Medved M, Oto A, Zamora M, Stadler WM.Reproducibility assessment of a multiple reference tissue method forquantitative dynamic contrast enhanced-MRI analysis. Magn Reson Med61(4):851-9, 2009.# Dale W, Hemmerich J, Bylow K, Mohile S, Mullaney M, Stadler WM. Patientanxiety about prostate cancer independently predicts early initiation ofandrogen deprivation therapy for biochemical cancer recurrence in older men:a prospective cohort study. J Clin Oncol 27(10):1557-63, 2009.* Bylow KA, Atkins MB, Posadas EM, Stadler WM, McDermott DF. PhaseII trial of carboplatin and paclitaxel in papillary renal cell carcinoma. ClinGenitourin Cancer 7(1):39-42, 2009.Steinberg, Gary MDMsezane L, Reynolds WS, Mhapsekar R, Gerber G, Steinberg G. Open surgicalrepair of ureteral strictures and fistulas following radical cystectomy andurinary diversion. J Urol 179(4):1428-31, 2008.* Gofrit ON, Zorn KC, Silvestre J, Shalhav AL, Zagaja GP, Msezane LP,Steinberg GD. The predictive value of multi-targeted fluorescent in-situhybridization in patients with history of bladder cancer. Urol Oncol 26(3):246-9, 2008.* Gofrit ON, Stadler WM, Zorn KC, Lin S, Silvestre J, Shalhav AL, Zagaja GP,Steinberg GD. Adjuvant chemotherapy in lymph node positive bladder cancer.Urol Oncol 27(2):160-4, 2009.* Gofrit ON, Zorn KC, Steinberg GD, Zagaja GP, Shalhav AL. The Will Rogersphenomenon in urological oncology. J Urol 179(1):28-33. Epub, 2007 Nov 13,2008.Katz MH, Steinberg GD. Sex and race in bladder cancer: what we have learnedand future directions. Cancer 115(1):10-2, 2009.deVere White RW, Katz MH, Steinberg GD. The case for neoadjuvantchemotherapy and cystectomy for muscle invasive bladder cancer. J Urol181(5):1994-7, 2009.* Gofrit ON, Orvieto MA, Zorn KC, Steinberg GD, Zagaja GP, Shalhav AL.Serum creatinine can be used as a surrogate for glomerular filtration rate insingle renal unit models. Can J Urol 16(1):4452-7, discussion 4457, 2009.Stenson, Kerstin MD* Salama JK, Stenson KM, List MA, Mell LK, Maccracken E, Cohen EE, Blair E,Vokes EE, Haraf DJ. Characteristics associated with swallowing changes afterconcurrent chemotherapy and radiotherapy in patients with head and neckcancer. Arch Otolaryngol Head Neck Surg 134(10):1060-5, 2008.* Cohn AB, Lang PO, Agarwal JP, Peng SL, Alizadeh K, Stenson KM, HarafDJ, Cohen EE, Vokes EE, Gottlieb LJ. Free-flap reconstruction in the doublyirradiated patient population. Plast Reconstr Surg 122(1):125-32, 2008.* Salama JK, Stenson KM, Kistner EO, Mittal BB, Argiris A, Witt ME, RosenF, Brockstein BE, Cohen EE, Haraf DJ, Vokes EE. Induction chemotherapy andconcurrent chemoradiotherapy for locoregionally advanced head and neckcancer: a multi-institutional phase II trial investigating three radiotherapy doselevels. Ann Oncol 19(10):1787-94, 2008.* Knab BR, Salama JK, Solanki A, Stenson KM, Cohen EE, Witt ME, Haraf DJ,Vokes EE. Functional organ preservation with definitive chemoradiotherapy forT4 laryngeal squamous cell carcinoma. Ann Oncol 19(9):1650-4, 2008.* Seiwert TY, Haraf DJ, Cohen EE, Stenson K, Witt ME, Dekker A,Kocherginsky M, Weichselbaum RR, Chen HX, Vokes EE. Phase I study ofbevacizumab added to fluorouracil- and hydroxyurea-based concomitantchemoradiotherapy for poor-prognosis head and neck cancer. J Clin Oncol26(10):1732-41, 2008.* # Cohen EE, Baru J, Huo D, Haraf DJ, Crowley M, Witt ME, Blair EA,Weichselbaum RR, Rosen F, Vokes EE, Stenson K. Efficacy and safety of treatingT4 oral cavity tumors with primary chemoradiotherapy. Head Neck 31(8):1013-21, 2009.* Cohen EE, Davis DW, Karrison TG, Seiwert TY, Wong SJ, Nattam S, KozloffMF, Clark JI, Yan DH, Liu W, Pierce C, Dancey JE, Stenson K, Blair E, Dekker A,Vokes EE. Erlotinib and bevacizumab in patients with recurrent or metastaticsquamous-cell carcinoma of the head and neck: a phase I/II study. LancetOncol 10(3):247-57, 2009.Vokes, Everett MD* Rudin CM, Liu W, Desai A, Karrison T, Jiang X, Janisch L, Das S, Ramirez J,Poonkuzhali B, Schuetz E, Fackenthal DL, Chen P, Armstrong DK, BrahmerJR, Fleming GF, Vokes EE, Carducci MA, Ratain MJ. Pharmacogenomic andpharmacokinetic determinants of erlotinib toxicity. J Clin Oncol 26(7):1119-27,2008.* Seiwert TY, Haraf DJ, Cohen EE, Stenson K, Witt ME, Dekker A,Kocherginsky M, Weichselbaum RR, Chen HX, Vokes EE. Phase I study ofbevacizumab added to fluorouracil- and hydroxyurea-based concomitantchemoradiotherapy for poor-prognosis head and neck cancer. J Clin Oncol26(10):1732-41, 2008.* Choong NW, Vokes EE, Haraf DJ, Tothy PK, Ferguson MK, Kasza K, RudinCM, Hoffman PC, Krauss SA, Szeto L, Mauer AM. Phase I study of inductionchemotherapy and concomitant chemoradiotherapy with irinotecan,carboplatin, and paclitaxel for stage III non-small cell lung cancer. J ThoracOncol 3(1):59-67, 2008.* # Salama JK, Chmura SJ, Mehta N, Yenice KM, Stadler WM, Vokes EE,Haraf DJ, Hellman S, Weichselbaum RR. An initial report of a radiation doseescalationtrial in patients with one to five sites of metastatic disease. ClinCancer Res 14(16):5255-9, 2008.* # Jagadeeswaran R, Surawska H, Krishnaswamy S, Janamanchi V, MackinnonAC, Seiwert TY, Loganathan S, Kanteti R, Reichman T, Nallasura V, SchwartzS, Faoro L, Wang YC, Girard L, Tretiakova MS, Ahmed S, Zumba O, SouliiL, Bindokas VP, Szeto LL, Gordon GJ, Bue. Paxillin is a target for somaticmutations in lung cancer: implications for cell growth and invasion. Cancer Res68(1):132-42, 2008.* # Ma PC, Tretiakova MS, MacKinnon AC, Ramnath N, Johnson C, DietrichS, Seiwert T, Christensen JG, Jagadeeswaran R, Krausz T, Vokes EE, Husain AN,Salgia R. Expression and mutational analysis of MET in human solid cancers.Genes Chromosomes Cancer 47(12):1025-37, 2008.* # Seiwert TY, Jagadeeswaran R, Faoro L, Janamanchi V, Nallasura V, ElDinali M, Yala S, Kanteti R, Cohen EE, Lingen MW, Martin L, Krishnaswamy S,Klein-Szanto A, Christensen JG, Vokes EE, Salgia R. The MET receptor tyrosinekinase is a potential novel therapeutic target for head and neck squamous cellcarcinoma. Cancer Res 69(7):3021-31, 2009.* Cohen EE, Davis DW, Karrison TG, Seiwert TY, Wong SJ, Nattam S, KozloffMF, Clark JI, Yan DH, Liu W, Pierce C, Dancey JE, Stenson K, Blair E, Dekker A,Vokes EE. Erlotinib and bevacizumab in patients with recurrent or metastaticsquamous-cell carcinoma of the head and neck: a phase I/II study. LancetOncol 10(3):247-57, 2009.Weichselbaum, Ralph MD* Jayathilaka K, Sheridan SD, Bold TD, Bochenska K, Logan HL, WeichselbaumRR, Bishop DK, Connell PP. A chemical compound that stimulates thehuman homologous recombination protein RAD51. Proc Natl Acad Sci U S A105(41):15848-53, 2008.* # Salama JK, Chmura SJ, Mehta N, Yenice KM, Stadler WM, Vokes EE,Haraf DJ, Hellman S, Weichselbaum RR. An initial report of a radiation doseescalationtrial in patients with one to five sites of metastatic disease. ClinCancer Res 14(16):5255-9, 2008.* # Bickenbach KA, Veerapong J, Shao MY, Mauceri HJ, Posner MC, Kron SJ,Weichselbaum RR. Resveratrol is an effective inducer of CArG-driven TNFalphagene therapy. Cancer Gene Ther 15(3):133-9, 2008.# Weichselbaum RR, Ishwaran H, Yoon T, Nuyten DS, Baker SW, KhodarevN, Su AW, Shaikh AY, Roach P, Kreike B, Roizman B, Bergh J, Pawitan Y, vande Vijver MJ, Minn AJ. An interferon-related gene signature for DNA damageresistance is a predictive marker for chemotherapy and radiation for breastcancer. Proc Natl Acad Sci U S A 105(47):18490-5, 2008.* # Cohen EE, Baru J, Huo D, Haraf DJ, Crowley M, Witt ME, Blair EA,Weichselbaum RR, Rosen F, Vokes EE, Stenson K. Efficacy and safety of treatingT4 oral cavity tumors with primary chemoradiotherapy. Head Neck 31(8):1013-21, 2009.# Liauw SL, Fricano J, Correa D, Weichselbaum RR, Jani AB. Dose-escalatedradiation therapy for intermediate-risk prostate cancer: patient selectionfor androgen deprivation therapy using percentage of positive cores. Cancer115(8):1784-90, 2009.# Lee Y, Auh SL, Wang Y, Burnette B, Wang Y, Meng Y, Beckett M, SharmaR, Chin R, Tu T, Weichselbaum RR, Fu YX. Therapeutic effects of ablativeradiation on local tumor require CD8+ T cells: changing strategies for cancertreatment. Blood 114(3):589-95, 2009.76UCCRC SCIENTIFIC REPORT 2009
Yamada, Seiko Diane MD# Onujiogu N, Lengyel E, Yamada SD. Reversible posteriorleukoencephalopathy syndrome following intravenous paclitaxel andintraperitoneal cisplatin chemotherapy for fallopian tube cancer. GynecolOncol 111(3):537-9, 2008.# Sawada K, Mitra AK, Radjabi AR, Bhaskar V, Kistner EO, Tretiakova M,Jagadeeswaran S, Montag A, Becker A, Kenny HA, Peter ME, Ramakrishnan V,Yamada SD, Lengyel E. Loss of E-cadherin promotes ovarian cancer metastasisvia alpha 5-integrin, which is a therapeutic target. Cancer Res 68(7):2329-39,2008.# Lotan T, Hickson J, Souris J, Huo D, Taylor J, Li T, Otto K, Yamada SD,Macleod K, Rinker-Schaeffer CW. c-Jun NH2-terminal kinase activating kinase1/mitogen-activated protein kinase kinase 4-mediated inhibition of SKOV3ip.1ovarian cancer metastasis involves growth arrest and p21 up-regulation. CancerRes 68(7):2166-75, 2008.# Taylor JL, Szmulewitz RZ, Lotan T, Hickson J, Griend DV, Yamada SD,Macleod K, Rinker-Schaeffer CW. New paradigms for the function of JNKK1/MKK4 in controlling growth of disseminated cancer cells. Cancer Lett272(1):12-22, 2008.# Taylor J, Hickson J, Lotan T, Yamada DS, Rinker-Schaeffer C. Usingmetastasis suppressor proteins to dissect interactions among cancer cells andtheir microenvironment. Cancer Metastasis Rev 27(1):67-73.* # Melhem A, Yamada SD, Fleming GF, Delgado B, Brickley DR, Wu W,Kocherginsky M, Conzen SD. Administration of Glucocorticoids to OvarianCancer Patients Is Associated with Expression of the Anti-apoptotic GenesSGK1 and MKP1/DUSP1 in Ovarian Tissues. Clin Cancer Res 15(9):3196-204,2009.Yamini, Bakhtiar MD# Rosen DS, Smith S, Gurbuxani S, Yamini B. Extranodal hairy cell leukemiapresenting in the lumbar spine. J Neurosurg Spine 9(4):374-6, 2008.Yuan, Chun-Su MD, PhD# Luo X, Wang CZ, Chen J, Song WX, Luo J, Tang N, He BC, Kang Q,Wang Y, Du W, He TC, Yuan CS. Characterization of gene expressionregulated by American ginseng and ginsenoside Rg3 in human colorectalcancer cells. Int J Oncol 32(5):975-83, 2008.# Wang CZ, Aung HH, Zhang B, Sun S, Li XL, He H, Xie JT, He TC,Du W, Yuan CS. Chemopreventive effects of heat-processed Panaxquinquefolius root on human breast cancer cells. Anticancer Res28(5A):2545-51, 2008.# Wang CZ, Xie JT, Fishbein A, Aung HH, He H, Mehendale SR, He TC,Du W, Yuan CS. Antiproliferative effects of different plant parts of Panaxnotoginseng on SW480 human colorectal cancer cells. Phytother Res23(1):6-13, 2009.Li XL, Wang CZ, Mehendale SR, Sun S, Wang Q, Yuan CS. Panaxadiol,a purified ginseng component, enhances the anti-cancer effects of5-fluorouracil in human colorectal cancer cells. Cancer ChemotherPharmacol, 2009.Wang CZ, Ni M, Sun S, Li XL, He H, Mehendale SR, Yuan CS. Detectionof adulteration of notoginseng root extract with other panax species byquantitative HPLC coupled with PCA. J Agric Food Chem 57(6):2363-7,2009.Wang CZ, Li XL, Wang QF, Mehendale SR, Fishbein AB, Han AH, Sun S,Yuan CS. The mitochondrial pathway is involved in American ginsenginducedapoptosis of SW-480 colon cancer cells. Oncol Rep 21(3):577-84,2009.Clinical & ExperimentalTherapeuticsUCCRC SCIENTIFIC REPORT 200977
Selected Major Grants and AwardsThe Clinical and Experimetnal Therapeutics Program has a funding base of $22,558,038 in annual total costs (current as of July2009). This sum includes $6,717,757 in NCI funding and $6,586,262 in other NIH funding. Due to space constraints, only newawards presented since January 1, 2008 with funding of $100,000 or more in annual total costs are listed here.Investigator Title Start DateYuan, Chun-SuWeichselbaum,RalphRatain, MarkMaitland, MichaelVokes, EverettDolan, EileenRatain, MarkKindler, HedyCenter for Herbal Research onColorectal CancerLudwig for Cancer ResearchProgramA Randomized DiscontinuationStudy of Brivanib Alanate (BMS-582664) vs. Placebo In Subjectswith Advanced Tumors Focusingon Baseline Expression of FGF-2ProteinPhase Ib Study to Evaluate theSafety of Combining IGF-1RAntagonist R1507 with MultipleStandard Chemotherapy DrugTreatments in Patients withAdvanced MalignanciesRandomized Phase II Trialof Taxotere, Cisplatin, andHypofractionated Radiotherapyvs Cisplatin and Taxotere forLimited Volume Stage IV NonsmallCell Lung Cancer (SynergisticMetastases Annihilation withRadiotherapy and Taxotere(SMART)Incorporation of microRNAexpression in pharmacogeneticprediction modelsPhase I Multicenter, Open-Label,Dose Escalating, Clinical andPharmacokinetic Study of PM01183in Patients with Advanced SolidTumors20070411: "A Phase lb/2 Open Label,Dose Escalation Study of AMG 655in Combination with AMG 479 inSubjects with Advanced, Refractory,Solid TumorsEndDateAnnualTotal CostClass9/30/2008 7/31/2013 $1,200,000 P011/1/2008 12/31/2010 $533,333 N/A4/8/2008 1/31/2011 $499,440 N/AFunding AgencyNational Center forComplementary andAlternative MedicineLudwig Fund for CancerResearch, Virginia andD.K.Bristol-Myers SquibbCompany3/9/2009 11/30/2010 $309,430 N/A Hoffmann-Laroche3/27/2009 3/26/2010 $289,825 N/A Sanofi-Aventis U.S. Inc.3/1/2009 2/28/2011 $205,920 R21 National Cancer Institute2/5/2009 2/4/2011 $195,000 N/A Pharmamar, S.A.2/11/2009 2/10/2011 $154,237 N/A Amgen78UCCRC SCIENTIFIC REPORT 2009
Investigator Title Start DateSeiwert, TanguyYamini, BakhtiarKindler, HedyKindler, HedyVokes, EverettVokes, EverettHe, Chuan1200.23: Phase IIb/III Randomized,Double Blind Trial of BIBW 2992Plus BSC vs Placebo Plus BSCin Non-Small Cell Lung CancerPatients Failing Erlotinib orGefitinibNanoparticles and Nanocapsules forGlioma TargetingMORAb-009-003: An Open-LabelClinical Trial of MORAb-009 inCombination with Pemetrexedand Cisplatin in Subjects withMesotheliomaPhase I/II Study of a TripletCombination of CBP501,Pemetrexed and Cisplatin inPatients with Advanced SolidTumors and in Chemotherapy-naivePatients with Malignant PleuralMesotheliomaStudy to Determine the Effectof Dose Schedules of R1507 orPlacebo, Both in Combination WithErlotinib (Tarceva), on Progression-Free Survival in Patients withAdvanced Non-Small Cell LungCancer with Disease Progressionafter ChemotherapyConcomitant Chemradiotherapyand Translational Gene TherapyTrials for Intermediate StageMalignancy of the Lung Head andNeckHow Staphyloccus Aureus sensesHost Immune DefensesEndDateAnnualTotal CostClassFunding Agency7/14/2008 7/13/2010 $124,395 N/A Boehringer Ingelheim Ltd9/12/2008 8/31/2009 $113,333 R43 National Cancer Institute2/10/2009 2/9/2011 $108,619 N/A Morphotek, Inc.8/1/2008 12/31/2010 $105,643 N/A Canbas Co. LTD.12/31/2008 6/30/2010 $102,270 N/A Hoffmann-Laroche7/1/2008 6/30/2013 $100,000 N/A7/1/2008 6/30/2013 $100,000 N/AAmerican Society ofClinical OncologyBurroughs WellcomeFundClinical & ExperimentalTherapeuticsUCCRC SCIENTIFIC REPORT 200979
Program 5Advanced Imaging
The University of Chicago Cancer Research Centeris at the forefront of the imaging revolution.Overview & GoalsImaging is an increasingly critical part of cancerdiagnosis and treatment. Advances in imagingallow early detection of cancer when it is most easilycured. In addition, imaging can be used to assessresponse to therapy and serves as an integral partof clinical trials for new drugs, as well as facilitatesthe development of customized, optimal therapiesfor individual patients. Image-guidance is essentialfor accurate delivery of radiotherapy and othertreatments, e.g., focused ultrasound. The rapiddevelopment of technology for imaging and imageguidedtherapy is transforming cancer care. As aresult, this is a time of unprecedented opportunityand challenge for translational imaging research. TheNCI, the ACS, and other national organizations havemade support for research in imaging a priority.(single photon emission computed tomography),and PET (positron emission tomography)imaging; (3) developing new methods of imageacquisition such as MRIS (magnetic resonanceimaging and spectroscopy) and EPR (electronparamagnetic resonance imaging); (4) identifyingimaging methods for oncology practice andfor the evaluation of response to target-basedcancer drugs; (5) providing imaging support forclinical trials; and (6) investigating methods forthe evaluation of imaging systems, especially asthey apply to computer-aided diagnosis and newimaging instrumentation. The Program strives toachieve these goals by integrating and focusingthe work of investigators with established researchprograms and by promoting collaborations.AdvancedImagingThe University of Chicago Cancer Research Centeris at the forefront of the imaging revolution.Extraordinary advances in imaging pioneered at theUCCRC are helping specialists diagnose cancer inits early, less harmful stages, and attack canceroustumors with greater precision and with less harm tohealthy tissue. Imaging research at the University ofChicago ranges from studies of many animal modelsof cancer, to in vitro studies of tissues and cells, toclinical research studies of patients and volunteers.The Advanced Imaging Program is structured sothat pre-clinical studies closely parallel clinicalresearch to create synergies that produce newideas and strongly support translational research.Consequently, the Advanced Imaging Program playsa key role in research at the UCCRC. The Programconsists of 27 members from two departments.The scientific goals of the Program include (1)investigating new methods for computerized imageanalysis to help in the early diagnosis of cancer(breast, lung, colon, and prostate carcinomas); (2)investigating new methods of image reconstructionfor use in CT (computed tomography), SPECTProgram Leaders:Gregory Karczmar, PhDHeber MacMahon, MDUCCRC SCIENTIFIC REPORT 200981
MembersInvestigator*Hiroyuki Abe MDHania Al-Hallaq PhDDaniel Appelbaum MDStephen Archer MDSamuel Armato PhDRichard Baron MDChin-Tu Chen PhDAbraham Dachman MDKunio Doi PhDMaryellen Giger PhDHoward Halpern MD, PhDYulei Jiang PhDChien-Min Kao PhDGregory Karczmar PhDPatrick La Riviere PhDStanley Liauw MDHeber MacMahon MDCharles Metz PhDGillian Newstead MB ChBRobert Nishikawa PhDAytekin Oto MDXiaochun Pan PhDCharles Pelizzari PhDBrian Roman PhDCharlene Sennett MDKenji Suzuki PhDMichael Vannier MDRankAssistant ProfessorAssistant ProfessorAssistant ProfessorProfessorAssociate ProfessorProfessorAssociate ProfessorProfessorProfessorProfessorProfessorAssociate ProfessorAssistant ProfessorProfessorAssistant ProfessorAssistant ProfessorProfessorProfessorProfessorAssociate ProfessorAssociate ProfessorProfessorAssociate ProfessorAssistant ProfessorAssistant ProfessorAssistant ProfessorProfessorDepartmentRadiologyRadiation and Cellular OncologyRadiologyMedicineRadiologyRadiologyRadiologyRadiologyRadiologyRadiologyRadiation and Cellular OncologyRadiologyRadiologyRadiologyRadiologyRadiation and Cellular OncologyRadiologyRadiologyRadiologyRadiologyRadiologyRadiologyRadiation and Cellular OncologyRadiologyRadiologyRadiologyRadiology82UCCRC SCIENTIFIC REPORT 2009* Reflects all Program membership during 2008-2009
Featured Faculty Research Summaries †The Advanced Imaging Program plays a key role in facilitating collaborationsamong investigators at the University of Chicago. Investigators have madesignificant advances in computer-aided diagnosis, new methods for imagereconstruction and acquisition, new imaging techniques for cancer therapyevaluation, and image-guided therapy for in vitro cancer-related applications.Highlights of research progress in areas including computed tomography,x-ray, magnetic resonance are outlined below.Theme: Computer-Aided DiagnosisSamuel Armato III, PhDAssociate Professor of RadiologyDr. Armato’s research focus is in the field of computeraideddiagnosis (CAD), which combines the disciplinesof physics, mathematics, computer science, and statisticsto analyze medical images for the early detection,diagnosis, and quantification of disease. Specifically, hehas been developing and investigating CAD methodsin chest radiology for the automated detection oflung nodules in thoracic computed tomographyDr. Kenji Suzuki(CT) scans, the automated volumetric assessment ofpleural mesothelioma in CT scans, the assessment ofmesothelioma response to therapy, and the analysis of temporal subtraction image quality in chest radiography. Heis also interested in the issue of inter-observer variability in diagnostic image interpretation, especially in the contextof establishing “truth” for CAD studies.AdvancedImagingDue in part to the strengths of its thoracic CAD research, The University of Chicago (with Dr. Armato as PrincipalInvestigator) was selected by the National Cancer Institute to form the Lung Image Database Consortium (LIDC)with four other academic institutions. This consortium is creating an image database as an international researchresource for the development, training, and evaluation of CAD methods for lung nodules in CT. The LIDC hasbeen engaged in a process to identify and resolve an array of challenging technical and clinical issues to provide asolid foundation for a robust database of 1000 thoracic CT scans, each annotated by a group of four expert chestradiologists through a two-phase reading process. Dr. Armato has been the lead investigator of several LIDCresearch projects. In one study involving the first 30 LIDC cases, a total of 59 lesions were assigned to the “nodule> 3 mm” category by at least one radiologist. Of these lesions, 27 (45.8%) received such an assignment from all fourradiologists, and 17 (28.8%) were identified as such by only a single radiologist. This study demonstrated the extent ofinter-observer variability in the task of lung nodule identification, even among experienced subspecialty radiologists.In another study, LIDC data was used to evaluate the lung nodule detection performance of experienced radiologistsin the context of other experienced radiologists. The number of “true” nodules as defined by various combinations ofradiologists ranged from 15-89. The mean nodule-detection sensitivities across radiologists and different definitionsof “truth” ranged from 51.0-83.2%, whereas mean false-positive rates ranged from 0.33-1.39 per case.Dr. Armato has developed computerized methods for the quantification of mesothelioma tumor extent in CT scans;such measurements, performed in a consistent manner, are essential to the conduct of clinical trials that seek toinvestigate treatment regimens for malignant pleural mesothelioma. Although manual measurement of tumorthickness on CT scans is the current standard for assessing response to therapy, this approach is tedious and oftenincomplete. The variability of manual mesothelioma tumor thickness measurements was found to be near 30% whenexperienced observers were asked to obtain measurements from the same series of CT scans. When presented withthe output of a semi-automated measurement system, observers accepted the computer output without modification† Note: Due to space constraints, only a small representative sample of Program members is presented here.UCCRC SCIENTIFIC REPORT 200983
in as many as 86% of the measurement sites; of all measurements across all observers, 89% were changed by 2 mm or less.Computer-assisted methods are expected to become important components of mesothelioma treatment protocols by makingthe quantification of tumor response to therapy more efficient, reproducible, and consistent. Dr. Armato’s research is nowchallenging the applicability of the current response criteria used clinically to evaluate a mesothelioma patient’s response totherapy.Kunio Doi, PhDProfessor of RadiologyRecently, computer-aided diagnosis (CAD) has become a component of the routine clinical work for the detection of breastcancer on mammograms. More than 8,000 CAD systems have been installed around the world, and about one half ofthe facilities for breast clinics in the U.S. have implemented CAD for diagnosis of breast cancer on mammograms. Theseobservations indicate that CAD is beginning to be applied widely in the detection and/or differential diagnosis of many differenttypes of abnormalities, such as breast cancer, lung cancer, colon cancer, brain tumors and cardiovascular diseases in medicalimages to assist physicians’ image interpretation.A large-scale systematic program for research and development of CAD schemes was initiated in the early 1980s at the KurtRossmann Laboratories for Radiologic Image Research in the Department of Radiology at the University of Chicago. Initially,three research projects were selected for 1) detection and/or quantitative analysis of stenoses in vascular imaging; 2) detection oflung nodules in chest radiographs; and 3) detection of clustered microcalcifications in mammograms. Although the sensitivitiesof these schemes for detection of lesions were relatively high (about 85%) even at that time, the number of false positives (fourper image) was very large. To examine the potential uses of CAD in clinical situations, an observer performance study wascarried out with and without computer output. Surprisingly, radiologists’ performance in detecting microcalcifications wasimproved significantly when the computer output was available, even with a large number of false positives.After these initial findings, many investigators around the world have followed the research and development of many differentCAD schemes for the detection and classification of various diseases. In the future, CAD schemes are likely to be assembledas packages and implemented as a part of PACS. For example, the package for chest CAD may include computerized detectionof lung nodules, interstitial opacities, cardiomegaly, vertebral fractures, and interval changes in chest images, as well ascomputerized classification of benign and malignant nodules and the differential diagnosis of interstitial lung diseases. All ofthe chest images taken for any purpose will be subjected to a computerized search for many different types of abnormalitiesincluded in the CAD package and, thus, potential sites of lesions together with the probability of a certain disease may bedisplayed on the workstation.At present, the majority of images in PACS are not being used for clinical purposes, except for images that are comparedbetween time points for a single patient. Therefore, the vast majority of images in PACS are currently “sleeping”. Providing a setof benign and malignant images, or a set of images with known pathology similar to an unknown new case in question wouldbe useful for providing radiologists with confidence in their differential diagnosis. The development of a reliable method forquantifying the similarity of a pair of images (or lesions) would allow radiologists to search for and retrieve similar cases fromPACS for visual comparison. Dr. Doi’s recent studies indicate that the similarity between a pair of lung nodules in CT andbetween lesions in mammograms can be quantified by a new psychophysical measure using an artificial neural network that istrained with corresponding image features and by use of subjective ratings from a group of radiologists.Yulei Jiang, PhDAssociate Professor of RadiologyA major goal of research in the Jiang laboratory is to develop CAD methods. With CAD, a radiologist interprets clinicalimages and makes clinical diagnoses and decisions in consultation with the results of computer analysis of the same images.Computer-aided detection techniques are used clinically to identify potential lesions in an image. Dr. Jiang’s team hasdeveloped a computer technique that can classify breast calcifications in mammograms as malignant or benign more accuratelythan radiologists can. The technique has been shown in a laboratory study to help radiologists recommend more biopsies for84UCCRC SCIENTIFIC REPORT 2009
patients who actually have breast cancer and recommend fewer biopsies for patients who actually have benign lesions. Thespecific aims of research in the laboratory are to 1) develop CAD methods for the detection and diagnosis of breast cancer inmammograms and prostate cancer in histology images; 2) evaluate the clinical effectiveness of CAD methods; and 3) gain afundamental understanding of diagnostic observer performance.In recent work, Dr. Jiang and collaborators developed a computer technique that recognizes prostate adenocarcinomain digitized immunohistochemistry images of prostate tissue sections stained with a triple-antibody cocktail of alphamethylacyl-CoAracemase (AMACR), p63, and high-molecular-weight cytokeratin (HMWCK). The computer technique wasfirst developed on 20 training images and 15 test images, then evaluated in a blinded study on 299 images. The sensitivity andspecificity of the computer image analysis ranged from 85–88% and 89–97%, respectively, depending on whether high-gradeprostatic intraepithelial neoplasia and cases with atypical diagnosis were included in the calculation. The study shows thattheir novel automated computer technique can accurately identify prostatic adenocarcinoma in the triple-antibody cocktailstainedprostate sections. Further research is ongoing to improve the computer technique and make it easy to use clinically.Development of a similar computer technique that analyzes H&E images is also ongoing.In another recent work, Dr. Jiang collaborated with Dr. Diana L. Miglioretti of Group Health Cooperative, Seattle,Washington, and Drs. Charles Metz and Robert Schmidt and published an article entitled, “Breast cancer detection rate:Designing imaging trials to demonstrate improvements” in Radiology. They analyzed data of over 2 ¼ million screeningmammograms interpreted by 510 radiologists in seven US regional registries, and found large variability in the apparentcancer detection rate calculated for each individual radiologist. The average cancer detection rate was 3.91 cancers perthousand screening examinations, and the standard deviation of the cancer detection rate was 1.93 cancers per thousandexaminations. One implication of such large variability is that they estimate ascertaining the cancer detection rate in aclinical trial is difficult and requires extremely large numbers of both screening participants and interpreting radiologists.This difficulty is exacerbated if the goal is to show that a new imaging modality is better than the standard practice. Theycalculated the effect of this large variability on the statistical powers of clinical trials and found most published clinical trialsof digital mammography and computer-aided detection, including some very large studies, seriously lacked in power. Thestudy shows that ascertaining the clinical effect of computer-aided detection requires extremely large clinical studies, and thedanger is great of reaching incorrect conclusions with studies of insufficient power.AdvancedImagingTheme: New Methods of Image Reconstruction and AcquisitionXiaochun Pan, PhDProfessor of RadiologyThe research interest of Dr. Pan’s laboratory centers on thedevelopment of tomographic imaging methodology, theory, andbiomedical and other applications. Tomographic imaging is anon-invasive approach to acquiring morphologic, physiologic, orfunctional information within the subject under study. Computedtomography (CT) and magnetic resonance imaging (MRI) aretwo examples of tomographic imaging techniques that haveimpacted tremendously on health care and biomedical research.As tomographic imaging research is multidisciplinary, the Panlaboratory is also collaborating with investigators of differentdisciplines, including clinicians and biological scientists, oncampus and from other institutions around the world. Althoughthe laboratory seeks to address fundamental and theoreticalproblems that arise in advanced tomographic imaging,research efforts are application-driven, aiming at tacklingproblems of practical significance. Therefore, the laboratoryhas also maintained active interactions and collaborations withIn vivo MR images of mousecolons at 9.4 Tesla: detection ofcolonic polyps and colorectaltumors in mice. The figureillustrates serial spin echo MRimages of the same mousetreated with a mutagen,azoxymethane: normal colon,colonic polyps, and colorectaltumor, as labeled. Smallpre-cancerous polyps can bedetected and monitored forthe progression of the disease.(Images courtesy of D. Mustafireflecting work in collaborationwith M. Bissonnette, E. Chang, X.Fan, J. Hart, and G. Karczmar)UCCRC SCIENTIFIC REPORT 200985
investigators and engineers from companies that are developing advanced tomographic imaging techniques for clinical and preclinicalapplications, for security scan, and for industrial non-destructive inspection.The Pan group has been conducting research in several areas of tomographic imaging sciences, including instrumentationdevelopment for obtaining anatomic as well as functional images of small animals in molecular imaging research, and theoryand algorithm development for cone-beam CT for clinical and other applications. Research is also being conducted withcollaborators on the development of fast imaging methods in MRI and of new technologies tailored to imaging specific organsand diseases.A great deal of research effort has recently been devoted to the development and evaluation of new theory and algorithms foraccurate image reconstruction in advanced, helical cone-beam CT. Advanced cone-beam CT offers high volume-scanningspeed and temporal resolution, which allows for the development and improvement of important clinical imaging applications,such as cardiac imaging, virtual colonoscopy, and CT-based lung cancer screening. Investigators in the field have been activelydeveloping mathematically exact theory and practically useful algorithms for derivation of high-quality volumetric imagesfrom data acquired with cone-beam CT. Dr. Pan’s research in this area has led to the establishment of a set of new concepts,theory, and algorithms that offer not only a fundamental understanding of the mathematical aspects of the cone-beam CTproblem, but also the basis for the development of additional innovative algorithms for obtaining accurate images. The work alsoreveals a host of possibilities in designing new imaging approaches targeted only to selected region of interests, which had beenconsidered theoretically impossible previously. Some of these new imaging approaches can have significant implications forreducing the motion effect and radiation dose in in vivo CT imaging.The Pan laboratory has also been interested in limited-data scanning in CT, where X-ray dose is reduced to the bare minimumto accomplish a given imaging task. An example of this is digital breast tomosynthesis (DBT). This semi-tomographic modalityexposes patients to an X-ray dose not much larger than standard digital mammography, approximately 100 times less than atypical CT scan. DBT promises to improve cancer detectability by utilizing the limited tomographic information to removeoverlapping structures from normal breast tissues. The new set of algorithms being developed may lower the required X-rayintensity even further, which is important if DBT is to be used as a mammographic screening tool. Other similar projectsinvolve the development of image-reconstruction algorithms for few-view data taken with onboard imagers to supportradiation-therapy accounting and to measure respiratory motion.Brian Roman, PhDAssistant Professor of RadiologyDr. Roman established the Physiological and Molecular Imaging Laboratory in 2005 in the Department of Radiology in orderto combine modern physiological and molecular biological techniques with non-invasive imaging modalities. Biologicaland physiological techniques are combined with magnetic resonance imaging (MRI) to acquire images in which contrastenhancement can be mapped to function. MR images are acquired using the UCCRC Lynn S. Florsheim Magnetic ResonanceImaging and Spectroscopy Laboratory (http://mris.bsd.uchicago.edu)9.4T scanner. A diverse group of biologists, molecularbiologists, bioengineers, veterinary technicians, and MR physicists are responsible for implementing the wide range oftechniques used in the laboratory. Research is focused on MR techniques and how they can be used towards an understandingof pancreatic and muscle tissue. Three specific aims of the research include 1) the use of MR to detect gene expression in theheart; 2) the development of MR techniques for imaging pancreatic beta cell and islet function; and 3) the development of MRtechniques for early detection of pancreatic cancer.To detect gene expression in the heart, the laboratory is developing techniques to link gene expression to MR image contrastfor early detection of cardiac hypertrophy, a process that usually cannot be reversed upon clinical detection. The laboratoryis engineering a transgenic mouse that expresses a MR reporter protein driven by an inducible cardiac hypertrophic promoterincluding atrial naturetic peptide (ANP) and brain naturetic peptide (BNP). This strategy benefits from using a ubiquitousand endogenous protein as the reporter, thereby removing problems with immunoreactivity. Additionally, since the reporter86UCCRC SCIENTIFIC REPORT 2009
is induced by the pathology, a maximum dynamic range can be obtained as the heart progresses from a baseline to apathological state. The laboratory is adapting this strategy towards the detection of cell proliferation in cancer models.The growing incidence of diabetes was the driving force for developing techniques to monitor pancreatic beta cell function.Beta cell production and release of insulin is preceded by membrane depolarization, which is triggered by changes inextracellular glucose and the influx of calcium. Early stages of this project involved proof of concept studies link theseactivation steps with MRI contrast. Manganese (Mn) was implemented as a calcium analog and a MRI contrast agent, as thelaboratory was successful in demonstrating that activated beta cells take up Mn in cell lines, as well as in both animal andhuman isolated islets, upon glucose stimulation. The apparent change in contrast is directly related to the release of insulinand therefore beta cell function. The laboratory is the pioneer of this technique and has successfully translated it to in vivomodels, resulting in functional MR images of the intact pancreas.The laboratory is currently adapting the Mn-MRI technique and developing complementary methods to detect pancreaticadenocarcinomas. An upregulation of calcium binding proteins and associated T-tubules occurs during the development ofthese tumors. As Mn is often considered a calcium analog, an underlying assumption is that these cancer cells will take upMn to a greater extent compared to non-cancer cells. The laboratory has obtained MR images of cultured pancreatic cancercells following exposure and growth with Mn, which indicate that Mn is taken up during growth and can be distinguishedfrom non-cancer cells. These findings have been examined in situ using xenograft models and are anticipated to facilitate anon-invasive method for monitoring tumor growth and therapeutic effectiveness.Theme: New Imaging Techniques for Oncology Practice and Therapy EvaluationHeber MacMahon, MDProfessor of RadiologyResearch in the Thoracic Imaging Section of the Departmentof Radiology has been focused on clinical applications ofimage processing and computer-aided diagnosis for improvedaccuracy in the detection and characterization of lung cancer.Initial detection of lung cancer is still most commonly made bychest radiography, and much of our research has been directedtowards developing methods to facilitate earlier and moreconsistent diagnosis, as well as monitoring of existing disease.The techniques have included energy subtraction, temporalsubtraction, rib suppression, and computer-aided detection. Inrecent years, the Thoracic Imaging Section has started to workwith commercial companies, which are developing advancedclinical products that incorporate these technologies.Magnetic resonance imaging of mouse mammary tumors in theUCCRC’s Lynn S. Florsheim MRIS Lab.AdvancedImagingThe current thrust of imaging research is the area of improving performance of radiologists in detection and characterizationof new disease in chest radiographs and CT scans. This has involved the application and evaluation of image processingtechniques to reduce rib opacity in order to improve nodule detection, evaluation of energy subtraction, and developmentof temporal subtraction to improve detection of interval change. While energy subtraction is a commercially availabletechnique with proven efficacy, other methods such as rib suppression and temporal subtraction are software-onlyapproaches that have the advantage of not requiring specialized acquisition equipment nor any increase in radiation dose.In a recent pilot study, Dr. MacMahon’s team compared the performance of radiologists viewing standard chest radiographsin detecting small lung cancers, compared to a novel rib suppression technique and dual energy subtraction. A significantimprovement in detection accuracy was demonstrated using rib suppression alone, while a further highly significant benefitwas shown with energy subtraction. This finding is important, because even a small improvement in detection accuracy canUCCRC SCIENTIFIC REPORT 200987
have important clinical implications in a modality as ubiquitous as chestradiography. Temporal subtraction is a complementary approach that canamplify interval change on sequential radiographs. After many years ofdevelopment at the University of Chicago, it has been licensed and furtherrefined to the point where it is ready to be tested in clinical practice. Theteam is currently working to determine how best to integrate temporalsubtraction with our clinical viewing system to initiate what would be thefirst such clinical trial in the United States.Detection of thoracic lesions is not limited to the initial disease presentation;it can play a role in monitoring and therapy evaluation as well, and tools thatimproved detection and characterization of thoracic disease have potentialfor more sensitive detection of disease recurrence. Although several newerIllustrations of flat lesions which exhibit uncommon flattools, such as PET and perfusion imaging are under investigation for thismorphology. (a) A flat lesion on a fold (10 mm; adenoma)in the cecum was detected correctly by our computeraideddetection scheme (indicated by an arrow). (b)purpose, the large majority of therapy monitoring is still based on simplemeasurement of selected reference lesions by radiologists. This is a necessaryA small flat lesion (6 mm; adenoma) in the cecum wasdetected correctly by our computer-aided detectionbut tedious task, which is time-consuming for radiologists, and suffersscheme. (Image by K. Suzuki)from considerable variation and inaccuracy. To address this issue, the teamis working to develop a software tool that will provide semi-automatedthree-dimensional volume measurements of tumor nodules, lymph nodes and liver metastases, while tracking lesions overtime on multiple sequential scans. The goal of this project is to provide a fully-integrated system that can provide oncologistswith accurate and reproducible tumor volume measurements, while facilitating the radiologists’ task. Although the systemcan actually detect new lung lesions with good accuracy, such detection tasks are being pushed onto the “back-burner” as adirect result of the difficulty of obtaining FDA clearance for clinical use. Nonetheless, accurate measurement and tracking ofradiologist-detected reference lesions has potential to have a major impact on oncologic practice, by reducing subjectivity andhuman error.Aytekin Oto, MDAssociate Professor of RadiologyDr. Oto is working in collaboration with the Lynn S. Florsheim MRIS Lab, directed by Drs. Karczmar and Roman, and Dr.Walter Stadler`s (Clinical and Experimental Therapeutics Program) laboratory to explore more accurate diagnosis of prostatecancer by MR imaging. Additionally, he is developing and validating MR image analysis methods to improve the amount andreproducibility of diagnostic information obtained from MRI through three ongoing research projects.The goal of the first project is to determine the role of dynamic contrast enhanced MR imaging (DCE-MRI) in the non-invasiveevaluation of histologic grading (Gleason score) and angiogenesis of prostate cancer. Specific objectives in this project are to 1)determine the relation between DCE-MRI derived kinetic parameters and the Gleason score of the prostate cancer lesions; 2)evaluate which parameters of DCE-MRI will correlate with mean vascular density and VEGF expression in the prostate cancer;and 3) determine whether the pharmacokinetic parameters estimated from DCE-MRI can improve detection of prostate cancerand extracapsular extension (ECE).The second project focuses on MR microscopy of prostatectomy specimens for automated whole organ histopathology.Histopathologic validation of imaging findings is required to improve the quality and consistency of new technology andto understand prostate cancer disease processes and treatment. Currently, the gold standard method for histopathologicalvalidation is expert visual inspection of whole mount prostatectomy specimens, a process that is costly, laborious, and notwidely available. In this project, a 9.4T MR imaging system will be used for imaging of fresh prostatectomy specimens, prior toroutine histopathological evaluation. On completion, this project will demonstrate the feasibility of using high field dedicatedMR imaging to increase efficiency and accuracy of pathologists and/or as an alternative to routine fixation and histopathologicalanalysis.88UCCRC SCIENTIFIC REPORT 2009
This research has significant potential to improve the quality and consistency of imaging and produce improvementsin technology for prostate cancer diagnosis and treatment. Specific aims are to 1) determine the feasibility of 9.4T MRImicroscopy of fresh and fixed ex vivo prostate specimens; 2) verify imaging findings of 9.4T scans with whole mount andstandard prostate histopathology; and 3) design and test a system for registration of multimodality in vivo and ex vivoprostate image analysis that uses MRI as the basis for superimposition of datasets.Finally, the third project focuses on optimization of an endrorectal prostate MR protocol. One specific aim is to developan optimal protocol for prostate scans that includes use of the Philips endorectal probe, fast spin echo imaging, diffusionweighted imaging, dynamic contrast enhanced MRI, and metabolic spectroscopy when appropriate. Results obtained withthese methods will be compared qualitatively and quantitatively with results obtained on GE scanners. The comparison willbe based on average image metrics over the group of patients imaged on each scanner. Comparisons will be made by patientswho are matched in terms of age and Gleason score. The second aim is to incorporate new experimental imaging approachesinto the standard Philips protocol, including new approaches to the analysis of DCE-MRI and the addition of HiSS to theprostate imaging protocol.Michael Vannier, MDProfessor of RadiologyImaging plays a central role in research and clinical medicine for many diseases, especially cancer. Imaging has grown inimportance because of the advances in technology that allow more precise location of lesions, the ability to guide therapy andspare normal tissues, and, more recently, a means to measure response to therapy and predict outcome. Clinical trials arebeneficial to cancer patients by providing access to new therapies. Imaging is essential for many of these trials to measure thelocation and extent of cancer, and, in some cases, to determine if an individual responds to the new therapy. This is a complextask, since many trials involve a combination of conventional and new therapies, so sensitive methods are used that candiscriminate the contribution of each. Experimental imaging methods are used in the laboratory for preclinical studies, andthe most advanced of these methods have been adapted or “translated” from the laboratory to the clinic. Some of the mostdemanding applications of imaging, which require the most advanced methods, are integrated into new clinical trials.AdvancedImagingIn brain tumor therapy, for example, imaging is essential to detect lesions, locate them precisely, and to measure their extent.In addition, imaging can measure the microvasculature, metabolism, and status of the blood-brain barrier, as well as theirchanges over time due to the effects of tumors or therapies. The amount of information provided by advanced imaging haseclipsed all other methods for certain lesions, so many clinical trials are built around the available imaging methods andtechnology. During the past 2 years, the University of Chicago has joined many highly innovative and important vanguardtrials of drug-radiotherapy-surgery combination trials underway at the nation’s leading centers. To qualify as a site, enrollvolunteer subjects, complete the complex protocols, and evaluate each new therapy, advanced technology was installedand tested for image acquisition, intravenous contrast administration, data archiving, post-processing analysis, and qualitycontrol. The benefits of the new therapies are difficult to evaluate while these trials are underway, but it appears likely thatsome of them will soon replace conventional therapies since the outcomes are superior, and toxicity is less.Nowadays, it is not unusual for a clinical trial to use dynamic contrast enhancement (where a multitude of images areacquired over time after IV contrast injection), proton spectroscopy, diffusion weighted imaging (that is sensitive toapoptosis, for example), perfusion measurement, and 3D morphometrics to evaluate tumors before and after therapy. In someinstances, several of these techniques are combined to evaluate multimodal therapy, such as chemoradiotherapy.Through the Advanced Imaging Program, the University of Chicago has been among the nation’s most productive centersbased on the number of subjects enrolled who have completed these trials. The efforts of many clinical disciplines areinvolved, for example, in brain tumor therapy. Drs. M. Kelly Nicholas, Director of the Neuro-Oncology Program, StevenChmura in radiotherapy, and Michael Vannier in radiology have worked together closely with Dr. Maryann Schroeder, inradiation oncology who oversees the protocol and procedures, and Paul Worthington, technical supervisor in MRI. Sponsorsof this research include the National Cancer Institute, oncology cooperative groups (ACRIN and RTOG), and industry.UCCRC SCIENTIFIC REPORT 200989
Theme: Image-Guided TherapyCharles Pelizzari, PhDAssociate Professor of Radiation and Cellular OncologyRadiation therapy has relied on image guidance in the form of CT andMRI based planning for patient irradiations, and planar radiography forverification of correct patient position since the early 1980’s. Today andinto the future, image guidance takes many forms, including the use of3D imaging modalities such as ultrasound and cone-beam CT for patientsetup, real-time monitoring of patient motion during treatment, andthe use of functional and molecular imaging in planning and also in theassessment of therapy response. The aim of image-guided therapy researchis to develop innovative applications of multiple imaging modalities, withthe goal of optimizing the treatment of each individual patient with thehighest geometric accuracy, taking full account of the relevant aspects ofthe patient’s tumor biology revealed by imaging, as they may affect thecourse of treatment.Dr. Charlene SennettFor pretreatment patient localization, Drs. Pelizzari and Xiaochaun Pan are developing new approaches to cone-beam CT, suchas targeted imaging where only the immediate surroundings of the treatment region are illuminated by the imaging X-ray beam.This both reduces unnecessary dose to non-tumor tissues and improves image quality by reducing the contribution of scatteredradiation. They are also working in collaboration with Dr. Gregory Karczmar to investigate the potential for creating smalllesions with high-intensity focused ultrasound that can serve as fiducial marks to guide various forms of therapy.Research into the use of functional imaging for planning and assessment of therapy is exemplified by the collaborations amongDrs. Charles Pelizzari, Howard Halpern, Gregory Karczmar, and Ralph Weichselbaum (Clinical and Experimental Therpauetics),concerning multimodality imaging to characterize functional changes in response to a combined radiation and antiangiogenicgene therapy. The ultimate goal of the project is to develop an image-guided adaptive therapeutic approach, where a localimaging “signature” of tumor response can be used to identify regions which are and are not responding well, and to use thisinformation to adapt the spatial distribution of gene vector injection and/or intensity-modulated radiation dose distribution toboost the less well responding regions. Preclinical studies have utilized a combination of perfusion sensitive dynamic contrastenhanced (DCE) MRI with the 4.7T and 9.4T magnets in the MRIS facility, and electron paramagnetic resonance (EPR) oxygenmapping using the spectroscopic imaging techniques pioneered in Dr. Halpern’s EPR research resource. EPR imaging is capableof mapping oxygenation in vivo with resolution of 1mm in space, and 3 mm Hg in oxygen tension.A significant and reproducible effect has been revealed through registration of spin echo MRI, DCE MRI contrast uptake,and EPR oxygen tension images of the same tumor, before and 3 days after radiation-inducible antiangiogenic gene therapy.Following treatment, the tumor appears better perfused (increased MRI contrast uptake) and better oxygenated (higher valuesin EPR pO2 map). This is consistent with the concept of vascular normalization by antiangiogenic agents leading to reperfusionand reoxygenation.Additional Program Highlights*90UCCRC SCIENTIFIC REPORT 2009
Additional Program Highlights*Research••Power spectral analysis of mammographic parenchymal patterns for breast cancer risk assessment. MaryellenGiger, PhD and colleagues (Olopade, Cancer Risk and Prevention Program) performed a study evaluating the usefulness ofpower law spectral analysis on mammographic mutant cell patterns in breast cancer risk assessment. The study collectedand digitized the mammograms from 172 subjects (women with BRCA1/BRCA2 gene mutation and low-risk women).Understanding these different patterns could help to explain which women may need to be more aggressively screened forbreast cancer to prevent the growth and development of mutant cells. The results of this study suggested that there wasa significant difference between the 30 BRCA1/BRCA2 gene mutation carriers and the 142 low-risk women. This studyis an example of how the successful development of innovative and personalized treatments can benefit from the closeintegration of clinical and technical skills (Li et al. J Digit Imaging 21:145-152, 2008).••Magnetic resonance imaging identifies multifocal and multicentric disease in breast cancer patients who areeligible for partial breast irradiation. In a retrospective study led by Hania Al-Hallaq, PhD, Gillian Newstead, MBChB, and Ralph Weichselbaum, MD, (Clinical and Experimental Therapeutics Program), the authors hypothesized thatmagnetic resonance imaging (MRI) would alter partial breast irradiation (PBI) eligibility by identifying cancers outsidethe PBI volume - as compared with mammography alone. Since 2002, 450 patients with invasive breast cancer wereconsidered for this study, 110 of which were identified as eligible for PBI. Patients were randomized to receive eitherwhole-breast radiotherapy or PBI, and MRI reports were reviewed to determine whether the MRI was effective in helpingto identify secondary lesions. The results suggest that the MRI was able to identify secondary lesions in 10-percent,multifocal disease in 3.6 percent, multicentric disease in 4.5 percent, and contralateral disease in 1.8 percent of patients.These results suggest that MRI usage should be considered to assess PBI eligibility to minimize potential failures andidentify secondary cancers with more accuracy (Al-Hallaq et al. Cancer 113:2408-2414, 2008).AdvancedImaging••Detection of in situ mammary cancer in a transgenic mouse model: in vitro and in vito MRI studies demonstratehistopathologic correlation. Sunnaz Jansen, PhD, Greg Karczmar, PhD, Gillian Newstead, MB ChB, and their colleagues(Suzanne Conzen, Cell Signaling and Gene Regulation Program) studied a transgenicmouse model that develops mammary cancer very similar to that of human breast cancer.Eleven mice were subjected to in vivo and in vitro imaging using the 9.4 Tesla magnet, andthe ratio of image-detected versus histologically-detected cancers was examined. Theresults showed that 12/12 intramammary lymph nodes, 1/1 relatively large (approximately5mm) tumor, 17/18 small (approximately 1mm) tumors, and 13/16 ducts distended withDCIS greater than 300 microns, were detected by MR images with no false-positives. Theresults indicate that the new magnetic imaging procedure can detect very early breastcancer in mice, a precursor to invasive cancer. These studies of model systems are leadingto more effective MRI methods that can be used clinically to effectively diagnose and treatcancer patients (Jansen et al. Phys Med Biol 53:5481-5493, 2008).••Electron paramagnetic resonance oxygen image hypoxic fraction plus radiation dosestrongly correlates with tumor cure in FSa fibrosarcomas. Howard Halpern, MD,PhD, and his colleagues have pioneered the use of electron paramagnetic imaging to maphypoxia in tumors based on the linewidth of the EPR (electron paramagnetic resonanceimaging) signal from specially-designed probes. Experiments were performed on 34 FSafibrosarcomas implanted in the legs of mice. EPR images were acquired from the tumorswhile mice were breathing air and under conditions where blood flow to the tumor wasinterrupted so that the tumors were hypoxic. Under the same conditions, the tumors wereIn vivo magnetic resonance (MR) imageand corresponding H&E stained sectiondemonstrating a murine invasive tumor.(Image by S. Jansen, S. Conzen, X. Fan, T.Krausz, M. Zamora, S. Foxley, J. River, G.Newstead, and G. Karczmar)* Due to space constraints, only a small representative sample of Program highlights is presented here.UCCRC SCIENTIFIC REPORT 200991
irradiated to a variety of doses near the dose at which fifty-percent of FSa tumors are cured. Tumor tissue was distinguishedfrom normal tissue using co-registration of the EPR oxygen images with spin-echo magnetic resonance images, and oxygenlevels in tumor and surrounding tissue were calculated from EPR data. Bivariate analysis of the tumors demonstrated thatcure rate correlated with radiation dose (p = 0.004) and with EPR measurements of oxygen tension lower than 10 mm ofmercury (p = 0.023). These results demonstrate that the degree of hypoxia measured by MRI, combined with the radiationdose, accurately predicts the response of tumors and suggest the potential of non-invasive electron paramagnetic resonanceto guide clinical treatment planning and improve outcomes for patients (Elas et al. Int J Radiat Oncol Biol Phys 71:542-549,2008).••Sensitivity to tumor microvasculature without contrast agents in high spectral and spatial resolution MR images.Greg Karczmar, PhD, and his colleagues investigated whether high spectral and spatial resolution (HiSS) MRI detects tumorvasculature without contrast agents, based on the sensitivity of the water resonance line shape to tumor blood vessels.HiSS data from AT6.1 tumors inoculated in the hind legs of rats (N = 8) were collected pre- and post-blood pool contrastagent (iron-oxide particles) injection. The waterline in small voxels was significantly more asymmetric at the tumor rimcompared to the tumor center and normal muscle (P < 0.003). Composite images were synthesized, with the intensity ineach voxel determined by the Fourier component (FC) of the water resonance having the greatest relative image contrast atthat position. Regions with high contrast in FC images (FCIs) were compared to FCIs with CE-MRI as the “gold standard” ofvascular density. The FCIs had 75% +/- 13% sensitivity, 74% +/- 10% specificity, and 91% +/- 4% positive predictive value (PPV)for vasculature detection at the tumor rim. These results suggest that tumor microvasculature can be detected using HiSSimaging without the use of contrast agents (Foxley et al., Magn Reson Med 61(2):291-298, 2009).Selected New Funding•• Xiaochuan Pan, PhD, and his colleagues are the recipients of an Illinois Department of Public Health grant to examine anenhanced form of magnetic resonance imaging (MRI). Dynamic contrast enhanced MRI (DCEMRI) is a powerful MRImethod, but its sensitivity and specificity are limited. Dr. Pan and his team are, therefore, pursuing another innovativeapproach to obtaining accurate breast images from a variety of k-space samples. The data would be used to increasethe sensitivity and specificity of DCEMRI, which would ultimately lead to enhanced early detection of cancer when it isrelatively easy to cure.••Patrick La Riviere, PhD, and his colleagues are developing a new method to overcome the limitations of non-contrastcomputed tomography (NC-CT) scans. Funded by an R01 grant from the National Cancer Institute, Dr. La Riviere plansto accomplish this by increasing the intrinsic contrast-to-noise ratio by reducing noise while preserving resolution usingprojection-domain smoothing and restoration with explicit models of measurement statistics. Successful completionof this work may help to provide superior CT imaging performance for patients with chronic kidney disease, contrastallergy, obesity, and for screening applications where radiation dose is limited. It would also lead to improved diagnosticperformance in emergency examinations.•• The National Center for Research Resources has supported the acquisition of a high-performance hybrid microCT/microSPECT imaging system and the setup of an animal imaging facility for both structural and functional imaging. Withthis instrument, Chin-Tu Chen, PhD and colleagues have established routine SPECT and CT imaging capabilities at theUniversity of Chicago for quantitative measurements of important anatomic and physiological parameters in animal studies,thus greatly enhancing the research of a number of NIH funded investigators, and offering pilot study opportunities to manyothers. Employing SPECT/CT imaging is anticipated to improve the diagnosis of diseases, effectively monitor treatment,and enhance the development of new drugs and therapies.92UCCRC SCIENTIFIC REPORT 2009
••••••Maryellen Giger, PhD, received funding from the Department of Energy to develop multi-modality, image-based markersfor assessing breast density and parenchymal structure that may be used alone or together with clinical measures, as wellas biomarkers, for use in determining the risk of breast cancer. Such image-based markers are expected to be useful forimproved assessment of patients at high risk for breast cancer and for monitoring the response of preventive treatments.The research involves the multimodality optimization of methods for breast image acquisition, analysis, and display.Image analysis is being optimized for full-field digital mammography, breast ultrasound, and breast MRI.Howard Halpern, MD, PhD, and colleagues were awarded a grant from the National Institute of Biological Imaging andBioengineering to develop very low frequency electron paramagnetic resonance imaging (EPRI) for in vivo physiology.High resolution images of molecular oxygenation can provide crucial guides to the delivery and monitoring of cancertherapy. EPR imaging of oxygen provides a unique combination of spatial and oxygen resolution and uniform sensitivitywith depth in tissue. The project reflects a multidisciplinary effort to improve the resolution of EPRI oxygen images forsmall animals with the long term goal of human image acquisition.Chien-Min Kao, PhD, was the recipient of an R21 grant from the National Cancer Institute to investigate and developnovel TOF PET reconstruction methods and imaging strategies. These new methods and strategies will more fully realizethe potentials of TOF PET imaging and hence enhance the already important role of PET imaging in cancer research andin the clinic. Results from this study are anticipated to advance TOF-PET imaging by creating new choices and flexibilitiesin data utilization, imaging strategies and system design.New Faculty Recruitments and UCCRC MembersStanley Liauw, MD specializes in the treatment of genitourinary and gastrointestinal cancers. Dr. Liauw’s research interestsinclude prostate cancer outcomes after dose-escalated external beam radiation therapy or brachytherapy, toxicity modelingfollowing radiation therapy, adjuvant radiation therapy after prostatectomy, quality of life issues, and mechanisms ofradiation resistance.AdvancedImagingUCCRC SCIENTIFIC REPORT 200993
Selected Publications* : Intraprogrammatic Collaboration# : Interprogrammatic CollaborationAbe, Hiroyuki MD* Jansen SA, Fan X, Karczmar GS, Abe H, Schmidt RA, Newstead GM.Differentiation between benign and malignant breast lesions detected by. MagnReson Med 59(4):747-54, 2008.* Jansen SA, Fan X, Karczmar GS, Abe H, Schmidt RA, Giger M, NewsteadGM. DCEMRI of breast lesions: is kinetic analysis equally effective for bothmass and nonmass-like enhancement?. Med Phys 35(7):3102-9, 2008.* Abe H, Schmidt RA, Kulkarni K, Sennett CA, Mueller JS, Newstead GM.Axillary Lymph Nodes Suspicious for Breast Cancer Metastasis: Sampling withUS-guided 14-Gauge Core-Needle Biopsy--Clinical Experience in 100 Patients.Radiology 250(1):41-9, 2009.* Shiraishi J, Abe H, Ichikawa K, Schmidt RA, Doi K. Observer Study forEvaluating Potential Utility of a Super-High-Resolution LCD in the Detectionof Clustered Microcalcifications on Digital Mammograms. J Digit Imaging,2009.Al-Hallaq, Hania PhD* # Al-Hallaq HA, Mell LK, Bradley JA, Chen LF, Ali AN, Weichselbaum RR,Newstead GM, Chmura SJ. Magnetic resonance imaging identifies multifocaland multicentric disease in breast cancer patients who are eligible for partialbreast irradiation. Cancer 113(9):2408-14, 2008.Lee, C.-H., Cheng, S.-H., Wang, Y.-J., Chen, Y.-C., Chen, N.-T., Souris, J.,Chen, C.-T., Mou, C.-Y., Yang, C.-S., and Lo, L.-W. Near-Infrared MesoporousSilica Nanoparticles for Optical Imaging: Characterization and In VivoBiodistribution. Advanced Functional Materials 19:215-222, 2009.Dachman, Abraham MD* Suzuki K, Yoshida H, Nappi J, Armato SG 3rd, Dachman AH. Mixture ofexpert 3D massive-training ANNs for reduction of multiple types of falsepositives in CAD for detection of polyps in CT colonography. Med Phys35(2):694-703, 2008.Sheran J, Dachman AH. Quality of CT colonography-related web sites forconsumers. J Am Coll Radiol 5(4):593-7, 2008.Flicker MS, Tsoukas AT, Hazra A, Dachman AH. Economic impact ofextracolonic findings at computed tomographic colonography. J Comput AssistTomogr 32(4):497-503, 2008.Johnson CD, Chen MH, Toledano AY, Heiken JP, Dachman A, Kuo MD, MeniasCO, Siewert B, Cheema JI, Obregon RG, Fidler JL, Zimmerman P, Horton KM,Coakley K, Iyer RB, Hara AK, Halvorsen RA Jr, Casola G, Yee J, Herman BA,Burgart LJ, Limburg PJ. Accuracy of CT colonography for detection of largeadenomas and cancers. N Engl J Med 359(12):1207-17, 2008.Dachman AH, Kelly KB, Zintsmaster MP, Rana R, Khankari S, Novak JD, AliAN, Qalbani A, Fletcher JG. Formative evaluation of standardized training forCT colonographic image interpretation by novice readers. Radiology 249(1):167-77, 2008.Liedenbaum MH, de Vries AH, Halligan S, Bossuyt PM, Dachman AH, DekkerE, Florie J, Gryspeerdt SS, Jensch S, Johnson CD, Laghi A, Taylor SA, Stoker J.CT colonography polyp matching: differences between experienced readers.Eur Radiol 19(7):1723-30, 2009.Appelbaum, Daniel MDRubin DT, Surma BL, Gavzy SJ, Schnell KM, Bunnag AP, Huo D, AppelbaumDE. Positron emission tomography (PET) used to image subclinicalinflammation associated with ulcerative colitis (UC) in remission. InflammBowel Dis 15(5):750-5, 2009.Archer, Stephen MDMarsboom G, Archer SL. Pathways of proliferation: new targets to inhibit thegrowth of vascular smooth muscle cells. Circ Res 103(10):1047-9, 2008.Armato, Samuel PhD# Armato SG 3rd, Entwisle J, Truong MT, Nowak AK, Ceresoli GL, ZhaoB, Misri R, Kindler HL. Current state and future directions of pleuralmesothelioma imaging. Lung Cancer 59(3):411-20, 2008.Armato S 3rd, Meyer C, McNitt-Gray M, McLennan G, Reeves A, Croft B,Clarke L. The Reference Image Database to Evaluate Response to Therapy inLung Cancer (RIDER) Project: A Resource for the Development of Change-Analysis Software. Clin Pharmacol Ther 84(4):448-56, 2008.* Suzuki K, Yoshida H, Nappi J, Armato SG 3rd, Dachman AH. Mixture ofexpert 3D massive-training ANNs for reduction of multiple types of falsepositives in CAD for detection of polyps in CT colonography. Med Phys35(2):694-703, 2008.Sensakovic WF, Starkey A, Roberts RY, Armato SG 3rd. Discrete-space versuscontinuous-space lesion boundary and area definitions. Med Phys 35(9):4070-8,2008.# Faoro L, Hutto JY, Salgia R, El-Zayaty SA, Ferguson MK, Cheney RT, ReidME, Armato SG 3rd, Krausz T, Husain AN. Lymphatic vessel density is notassociated with lymph node metastasis in non-small cell lung carcinoma. ArchPathol Lab Med 132(12):1882-8, 2008.* Armato SG 3rd, Roberts RY, Kocherginsky M, Aberle DR, Kazerooni EA,Macmahon H, van Beek EJ, Yankelevitz D, McLennan G, McNitt-Gray MF,Meyer CR, Reeves AP, Caligiuri P, Quint LE, Sundaram B, Croft BY, ClarkeLP. Assessment of radiologist performance in the detection of lung nodules:dependence on the definition of “truth”. Acad Radiol 16(1):28-38, 2009.Chen, Chin-Tu PhDLin KM, Hsu CH, Chang WS, Chen CT, Lee TW, Chen CT. Human breasttumor cells express multimodal imaging reporter genes. Mol Imaging Biol10(5):253-63, 2008.Doi, Kunio PhD* Li F, Engelmann R, Metz CE, Doi K, MacMahon H. Lung cancers missedon chest radiographs: results obtained with a commercial computer-aideddetection program. Radiology 246(1):273-80, 2008.* Li F, Engelmann R, Doi K, MacMahon H. Improved detection of small lungcancers with dual-energy subtraction chest radiography. AJR Am J Roentgenol190(4):886-91, 2008.Kasai S, Li F, Shiraishi J, Doi K. Usefulness of computer-aided diagnosisschemes for vertebral fractures and lung nodules on chest radiographs. AJR AmJ Roentgenol 191(1):260-5, 2008.Shiraishi J, Sugimoto K, Moriyasu F, Kamiyama N, Doi K. Computer-aideddiagnosis for the classification of focal liver lesions by use of contrast-enhancedultrasonography. Med Phys 35(5):1734-46, 2008.* Shiraishi J, Abe H, Ichikawa K, Schmidt RA, Doi K. Observer Study forEvaluating Potential Utility of a Super-High-Resolution LCD in the Detectionof Clustered Microcalcifications on Digital Mammograms. J Digit Imaging,2009.* Li F, Engelmann R, Doi K, Macmahon H. True Detection Versus “Accidental”Detection of Small Lung Cancer by a Computer-Aided Detection (CAD)Program on Chest Radiographs. J Digit Imaging, 2009.Muramatsu C, Li Q, Schmidt R, Shiraishi J, Doi K. Investigation ofpsychophysical similarity measures for selection of similar images in thediagnosis of clustered microcalcifications on mammograms. Med Phys35(12):5695-702, 2008.Giger, Maryellen PhD# Li H, Giger ML, Olopade OI, Chinander MR. Power spectral analysis ofmammographic parenchymal patterns for breast cancer risk assessment. J DigitImaging 21(2):145-52, 2008.Wilkie JR, Giger ML, Chinander MR, Engh CA, Hopper RH Jr, Martell JM.Temporal radiographic texture analysis in the detection of periprostheticosteolysis. Med Phys 35(1):377-87, 2008.* Drukker K, Gruszauskas NP, Sennett CA, Giger ML. Breast US computeraideddiagnosis workstation: performance with a large clinical diagnosticpopulation. Radiology 248(2):392-7, 2008.* Gruszauskas NP, Drukker K, Giger ML, Sennett CA, Pesce LL. Performanceof breast ultrasound computer-aided diagnosis: dependence on image selection.Acad Radiol 15(10):1234-45, 2008.* Li H, Giger ML, Yuan Y, Chen W, Horsch K, Lan L, Jamieson AR, Sennett CA,Jansen SA. Evaluation of computer-aided diagnosis on a large clinical full-fielddigital mammographic dataset. Acad Radiol 15(11):1437-45, 2008.94UCCRC SCIENTIFIC REPORT 2009
* Horsch K, Giger ML, Metz CE. Prevalence scaling: applications to anintelligent workstation for the diagnosis of breast cancer. Acad Radiol15(11):1446-57, 2008.* Yuan Y, Giger ML, Li H, Sennett C. Correlative feature analysis on FFDM.Med Phys 35(12):5490-500, 2008.Giger ML, Chan HP, Boone J. Anniversary paper: History and status of CADand quantitative image analysis: the role of Medical Physics and AAPM. MedPhys 35(12):5799-820, 2008.Drukker K, Sennett CA, Giger ML. Automated method for improving systemperformance of computer-aided diagnosis in breast ultrasound. IEEE TransMed Imaging 28(1):122-8, 2009.Halpern, Howard MD, PhD* Elas M, Bell R, Hleihel D, Barth ED, McFaul C, Haney CR, Bielanska J,Pustelny K, Ahn KH, Pelizzari CA, Kocherginsky M, Halpern HJ. Electronparamagnetic resonance oxygen image hypoxic fraction plus radiation dosestrongly correlates with tumor cure in FSa fibrosarcomas. Int J Radiat OncolBiol Phys 71(2):542-9, 2008.* # Haney CR, Parasca AD, Fan X, Bell RM, Zamora MA, Karczmar GS,Mauceri HJ, Halpern HJ, Weichselbaum RR, Pelizzari CA. Characterizationof response to radiation mediated gene therapy by means of multimodalityimaging. Magn Reson Med 62(2):348-56, 2009.Jiang, Yulei PhDKrupinski EA, Jiang Y. Anniversary paper: evaluation of medical imagingsystems. Med Phys 35(2):645-59, 2008.Peng Y, Jiang Y, Chuang ST, Yang XJ. Computer-aided Detection of ProstateCancer on Tissue Sections. Appl Immunohistochem Mol Morphol, 2009.Kao, Chien-Min PhDKao CM. Windowed image reconstruction for time-of-flight positron emissiontomography. Phys Med Biol 53(13):3431-45, 2008.Karczmar, Gregory PhD* Jansen SA, Fan X, Karczmar GS, Abe H, Schmidt RA, Newstead GM.Differentiation between benign and malignant breast lesions detected by. MagnReson Med 59(4):747-54, 2008.# Hahn OM, Yang C, Medved M, Karczmar G, Kistner E, Karrison T, ManchenE, Mitchell M, Ratain MJ, Stadler WM. Dynamic contrast-enhanced magneticresonance imaging pharmacodynamic biomarker study of sorafenib inmetastatic renal carcinoma. J Clin Oncol 26(28):4572-8, 2008.* # Jansen SA, Conzen SD, Fan X, Krausz T, Zamora M, Foxley S, RiverJ, Newstead GM, Karczmar GS. Detection of in situ mammary cancer ina transgenic mouse model: in vitro and in vivo MRI studies demonstratehistopathologic correlation. Phys Med Biol 53(19):5481-93, 2008.* # Yang C, Karczmar GS, Medved M, Oto A, Zamora M, Stadler WM.Reproducibility assessment of a multiple reference tissue method forquantitative dynamic contrast enhanced-MRI analysis. Magn Reson Med61(4):851-9, 2009.* # Haney CR, Parasca AD, Fan X, Bell RM, Zamora MA, Karczmar GS,Mauceri HJ, Halpern HJ, Weichselbaum RR, Pelizzari CA. Characterizationof response to radiation mediated gene therapy by means of multimodalityimaging. Magn Reson Med 62(2):348-56, 2009.Foxley S, Fan X, Mustafi D, Haney C, Zamora M, Markiewicz E, Medved M,Wood AM, Karczmar GS. Sensitivity to tumor microvasculature withoutcontrast agents in high spectral and spatial resolution MR images. Magn ResonMed 61(2):291-8, 2009.La Riviere, Patrick PhDLa Riviere PJ, Vargas P. Correction for resolution nonuniformities causedby anode angulation in computed tomography. IEEE Trans Med Imaging27(9):1333-41, 2008.# Liauw SL, Weichselbaum RR, Zagaja GP, Jani AB. Salvage radiotherapyafter postprostatectomy biochemical failure: does pretreatmentradioimmunoscintigraphy help select patients with locally confineddisease?. Int J Radiat Oncol Biol Phys 71(5):1316-21, 2008.# Liauw SL, Fricano J, Correa D, Weichselbaum RR, Jani AB. Doseescalatedradiation therapy for intermediate-risk prostate cancer: patientselection for androgen deprivation therapy using percentage of positivecores. Cancer 115(8):1784-90, 2009.# Gutt R, Liauw SL, Weichselbaum RR. Adjuvant radiotherapy forresected pancreatic cancer: a lack of benefit or a lack of adequate trials?.Nat Clin Pract Gastroenterol Hepatol 6(1):38-46, 2009.Jani AB, Johnstone PA, Liauw SL, Master VA, Brawley OW. Age and gradetrends in prostate cancer (1974-2003): a Surveillance, Epidemiology, andEnd Results Registry analysis. Am J Clin Oncol 31(4):375-8, 2008.Trabulsi EJ, Valicenti RK, Hanlon AL, Pisansky TM, Sandler HM,Kuban DA, Catton CN, Michalski JM, Zelefsky MJ, Kupelian PA, LinDW, Anscher MS, Slawin KM, Roehrborn CG, Forman JD, Liauw SL,Kestin LL, DeWeese TL, Scardino PT, Stephenson AJ, Pollack A. Amulti-institutional matched-control analysis of adjuvant and salvagepostoperative radiation therapy for pT3-4N0 prostate cancer. Urology72(6):1298-302, discussion 1302-4, 2008.Yeung AR, Liauw SL, Amdur RJ, Mancuso AA, Hinerman RW, MorrisCG, Villaret DB, Werning JW, Mendenhall WM. Lymph node-positivehead and neck cancer treated with definitive radiotherapy: can treatmentresponse determine the extent of neck dissection?. Cancer 112(5):1076-82,2008.MacMahon, Heber MD* Li F, Engelmann R, Metz CE, Doi K, MacMahon H. Lung cancersmissed on chest radiographs: results obtained with a commercialcomputer-aided detection program. Radiology 246(1):273-80, 2008.* MacMahon H, Li F, Engelmann R, Roberts R, Armato S. Dual energysubtraction and temporal subtraction chest radiography. J ThoracImaging 23(2):77-85, 2008.* Li F, Engelmann R, Doi K, MacMahon H. Improved detection of smalllung cancers with dual-energy subtraction chest radiography. AJR Am JRoentgenol 190(4):886-91, 2008.* Kumazawa S, Muramatsu C, Li Q, Li F, Shiraishi J, Caligiuri P,Schmidt RA, MacMahon H, Doi K. An investigation of radiologists’perception of lesion similarity: observations with paired breast masseson mammograms and paired lung nodules on CT images. Acad Radiol15(7):887-94, 2008.* Armato SG 3rd, Roberts RY, Kocherginsky M, Aberle DR, KazerooniEA, Macmahon H, van Beek EJ, Yankelevitz D, McLennan G, McNitt-Gray MF, Meyer CR, Reeves AP, Caligiuri P, Quint LE, Sundaram B, CroftBY, Clarke LP. Assessment of radiologist performance in the detectionof lung nodules: dependence on the definition of “truth”. Acad Radiol16(1):28-38, 2009.* Li F, Engelmann R, Doi K, Macmahon H. True Detection Versus“Accidental” Detection of Small Lung Cancer by a Computer-AidedDetection (CAD) Program on Chest Radiographs. J Digit Imaging, 2009.Metz, Charles PhDHillis SL, Berbaum KS, Metz CE. Recent developments in the Dorfman-Berbaum-Metz procedure for multireader ROC study analysis. AcadRadiol 15(5):647-61, 2008.* Horsch K, Giger ML, Metz CE. Potential effect of different radiologistreporting methods on studies showing benefit of CAD. Acad Radiol15(2):139-52, 2008.* Li F, Engelmann R, Metz CE, Doi K, MacMahon H. Lung cancersmissed on chest radiographs: results obtained with a commercialcomputer-aided detection program. Radiology 246(1):273-80, 2008.* Horsch K, Giger ML, Metz CE. Prevalence scaling: applications to anintelligent workstation for the diagnosis of breast cancer. Acad Radiol15(11):1446-57, 2008.AdvancedImagingLiauw, Stanley MD# Liauw SL, Minsky BD. The use of capecitabine in the combined-modalitytherapy for rectal cancer. Clin Colorectal Cancer 7(2):99-104, 2008.Newstead, Gillian MB, ChB* Jansen SA, Fan X, Karczmar GS, Abe H, Schmidt RA, Newstead GM.Differentiation between benign and malignant breast lesions detected by.Magn Reson Med 59(4):747-54, 2008.UCCRC SCIENTIFIC REPORT 200995
* Jansen SA, Fan X, Karczmar GS, Abe H, Schmidt RA, Giger M, NewsteadGM. DCEMRI of breast lesions: is kinetic analysis equally effective for bothmass and nonmass-like enhancement?. Med Phys 35(7):3102-9, 2008.* # Jansen SA, Conzen SD, Fan X, Krausz T, Zamora M, Foxley S, RiverJ, Newstead GM, Karczmar GS. Detection of in situ mammary cancer ina transgenic mouse model: in vitro and in vivo MRI studies demonstratehistopathologic correlation. Phys Med Biol 53(19):5481-93, 2008.* Abe H, Schmidt RA, Kulkarni K, Sennett CA, Mueller JS, Newstead GM.Axillary Lymph Nodes Suspicious for Breast Cancer Metastasis: Sampling withUS-guided 14-Gauge Core-Needle Biopsy--Clinical Experience in 100 Patients.Radiology 250(1):41-9, 2009.* # Al-Hallaq HA, Mell LK, Bradley JA, Chen LF, Ali AN, Weichselbaum RR,Newstead GM, Chmura SJ. Magnetic resonance imaging identifies multifocaland multicentric disease in breast cancer patients who are eligible for partialbreast irradiation. Cancer 113(9):2408-14, 2008.Nishikawa, Robert PhDReiser I, Nishikawa RM, Edwards AV, Kopans DB, Schmidt RA, PapaioannouJ, Moore RH. Automated detection of microcalcification clusters for digitalbreast tomosynthesis using projection data only: a preliminary study. Med Phys35(4):1486-93, 2008.Nishikawa RM, Acharyya S, Gatsonis C, Pisano ED, Cole EB, MarquesHS, D’Orsi CJ, Farria DM, Kanal KM, Mahoney MC, Rebner M, StaigerMJ. Comparison of soft-copy and hard-copy reading for full-field digitalmammography. Radiology 251(1):41-9, 2009.Oto, Aytekin MD* # Yang C, Karczmar GS, Medved M, Oto A, Zamora M, Stadler WM.Reproducibility assessment of a multiple reference tissue method forquantitative dynamic contrast enhanced-MRI analysis. Magn Reson Med61(4):851-9, 2009.* Oto A, Zhu F, Kulkarni K, Karczmar GS, Turner JR, Rubin D. Evaluation ofdiffusion-weighted MR imaging for detection of bowel inflammation in patientswith Crohn’s disease. Acad Radiol 16(5):597-603, 2009.Lewis JR, Te HS, Gehlbach B, Oto A, Chennat J, Mohanty SR. A case ofbiliopleural fistula in a patient with hepatocellular carcinoma. Nat RevGastroenterol Hepatol 6(4):248-51, 2009.Oto A, Ernst R, Ghulmiyyah L, Hughes D, Saade G, Chaljub G. The role of MRcholangiopancreatography in the evaluation of pregnant patients with acutepancreaticobiliary disease. Br J Radiol 82(976):279-85, 2009.Pelizzari, Charles PhD* Cho S, Xia D, Pelizzari CA, Pan X. Exact reconstruction of volumetric imagesin reverse helical cone-beam CT. Med Phys 35(7):3030-40, 2008.* Elas M, Bell R, Hleihel D, Barth ED, McFaul C, Haney CR, Bielanska J,Pustelny K, Ahn KH, Pelizzari CA, Kocherginsky M, Halpern HJ. Electronparamagnetic resonance oxygen image hypoxic fraction plus radiation dosestrongly correlates with tumor cure in FSa fibrosarcomas. Int J Radiat OncolBiol Phys 71(2):542-9, 2008.Aristophanous M, Penney BC, Pelizzari CA. The development and testingof a digital PET phantom for the evaluation of tumor volume segmentationtechniques. Med Phys 35(7):3331-42, 2008.# Altman MB, Vesper BJ, Smith BD, Stinauer MA, Pelizzari CA, Aydogan B,Reft CS, Radosevich JA, Chmura SJ, Roeske JC. Characterization of a novelphantom for three-dimensional in vitro cell experiments. Phys Med Biol54(5):N75-82, 2009.Sennett, Charlene MD* Abe H, Schmidt RA, Kulkarni K, Sennett CA, Mueller JS, Newstead GM.Axillary Lymph Nodes Suspicious for Breast Cancer Metastasis: Sampling withUS-guided 14-Gauge Core-Needle Biopsy--Clinical Experience in 100 Patients.Radiology 250(1):41-9, 2009.* Drukker K, Gruszauskas NP, Sennett CA, Giger ML. Breast US computeraideddiagnosis workstation: performance with a large clinical diagnosticpopulation. Radiology 248(2):392-7, 2008.* Gruszauskas NP, Drukker K, Giger ML, Sennett CA, Pesce LL. Performanceof breast ultrasound computer-aided diagnosis: dependence on image selection.Acad Radiol 15(10):1234-45, 2008.* Li H, Giger ML, Yuan Y, Chen W, Horsch K, Lan L, Jamieson AR, Sennett CA,Jansen SA. Evaluation of computer-aided diagnosis on a large clinical full-fielddigital mammographic dataset. Acad Radiol 15(11):1437-45, 2008.* Yuan Y, Giger ML, Li H, Sennett C. Correlative feature analysis on FFDM.Med Phys 35(12):5490-500, 2008.Suzuki, Kenji PhD* Suzuki K, Yoshida H, Nappi J, Armato SG 3rd, Dachman AH. Mixture ofexpert 3D massive-training ANNs for reduction of multiple types of falsepositives in CAD for detection of polyps in CT colonography. Med Phys35(2):694-703, 2008.Pan, Xiaochun PhD* Cho S, Xia D, Pelizzari CA, Pan X. Exact reconstruction of volumetric imagesin reverse helical cone-beam CT. Med Phys 35(7):3030-40, 2008.Sidky EY, Pan X. Image reconstruction in circular cone-beam computedtomography by constrained, total-variation minimization. Phys Med Biol53(17):4777-807, 2008.LaRoque SJ, Sidky EY, Pan X. Accurate image reconstruction from few-viewand limited-angle data in diffraction tomography. J Opt Soc Am A Opt ImageSci Vis 25(7):1772-82, 2008.Cho S, Pearson E, Pelizzari CA, Pan X. Region-of-interest image reconstructionwith intensity weighting in circular cone-beam CT for image-guided radiationtherapy. Med Phys 36(4):1184-92, 2009.96UCCRC SCIENTIFIC REPORT 2009
Selected Major Grants and AwardsThe Advanced Imaging Program has a funding base of $8,320,181 in annual total costs (current as of July 2009). This sum includes$3,311,886 in NCI funding and $3,320,764 in other NIH funding. Due to space constraints, only new awards presented sinceJanuary 1, 2008 with funding of $100,000 or more in annual total costs are listed here.Investigator Title Start DateHalpern, HowardGiger, MaryellenJiang, YuleiLa Riviere, PatrickChen, Chin-TuKao, Chien-MinKarczmar, GregoryGiger, MaryellenLa Riviere, PatrickKarczmar, GregoryVery Low Frequency EPR Imaging forin Vivo PhysiologyOptimization of Computer-AidedDiagnosis (CAD) Output in BreastImagingComputer-Aided Diagnosis of BreastLesions in MammogramsTailored Algorithms for Non-ContrastComputed Tomography UsingSinogram RestorationHybrid MicroSPECT/MicroCT forQuantitative ImagingMaximal Information Utilizing inTOF-PET for Reducing ScatterHigh Spectral, Spatial, TemporalResolution MRIIntergrated Multi Modality ImageBased Markers of Breast Density andStructure in Assessing Breast CancerRisk at the University of ChicagoMolecular Probes and Techniques forOptoacoustic Imaging of ProteasesPre-Clincal Development of MRI\Guided HIFU Marking for LesionVisualizationEndDateAnnualTotal CostClass8/1/2008 5/31/2013 $1,333,707 P41Funding AgencyNational Institute ofBiological Imaging andBioengineering6/15/2006 5/31/2011 $407,744 R21 National Cancer Institute7/11/2008 6/30/2009 $302,891 R56 National Cancer Institute9/24/2008 7/31/2013 $270,049 R01 National Cancer Institute3/1/2008 2/28/2010 $250,000 S10National Center forResearch Resources3/1/2009 2/28/2011 $192,445 R21 National Cancer Institute10/1/2008 9/30/2009 $192,000 N/ANorth American PhilipsCorporation8/1/2008 7/31/2011 $191,000 FG02 Department of Energy7/1/2008 6/30/2012 $175,000 08 American Cancer Society9/30/2008 9/29/2009 $141,000 N/ANorth American PhilipsCorporationAdvancedImagingOto, Aytekin Optimization of Prostate MRI 4/1/2008 4/1/2009 $101,000 N/A Philips Medical SystemsUCCRC SCIENTIFIC REPORT 200997
Program 6Cancer Risk and PreventionHuman fibroblasts expressing two different forms of the BLM helicase. One cell line (top two panels) expresses the normal protein (BLM+)and the other cell line (bottom two panels) expresses a form of BLM (SM-BLM) mutated at two sumoylation sites important for its regulation.These cell lines were stained with antibodies to the single-stranded DNA binding protein RPA (blue stain) and the RAD51 recombinase (red stain).BLM is identified by green fluorescence. All three proteins are important in DNA repair. After treatment of cells with the DNA damaging agenthydroxyurea, “repair foci” form that contain concentrations of DNA repair proteins. In BLM+ cells, there are many foci that contain all three proteins(BLM, RPA, and RAD51); however, in SM-BLM cells, although there are many foci that contain both BLM and RPA, the repair foci do not containRAD51 recombinase. Consequently, the regulatory mutations in BLM impair the movement to or retention of RAD51 in repair foci.(Image by N. Ellis and K. Ouyang)
Research is focused on high-risk individuals defined bygenetics, exposure, and/or other vulnerabilities or disparitiesbased on race/ethnicity or access to health care.Overview & GoalsThe overall objectives of the Cancer Risk andPrevention Program are to understand thegenetic, psychological, behavioral, and socioenvironmentalbasis of cancer and to translateand disseminate these cancer control researchefforts in our community. The program consistsof 40 members from 12 departments and twoUniversity Divisions (Biological Sciences,Social Sciences). Research is focused on highriskindividuals defined by genetics, exposure(behavior, environmental), and/or othervulnerabilities (e.g., older age) or disparitiesbased on race/ethnicity or access to health care.The primary scientific goals of the Program are(1) to elucidate the genetic and environmentalbasis, as well as the mechanisms of progression,for common cancers (breast, ovarian, colorectal,prostate, lung, skin, and blood), and to translatethis new knowledge into clinical and publichealth practices; (2) to develop animal modelsfor chemoprevention studies and developbiomarkers for early detection of cancer; (3) toidentify genetic, physiological, and bio-behavioralbases of cancer risk and prevention; and (4) tosolidify an organized outreach research effort inthe Southside Chicago neighborhoods to enhanceparticipation and utilization of University ofChicago research, education, and clinical services,thereby reducing the disparities in cancer andother health outcomes and their modifiabledeterminants in the community.Program Leaders:Brian Chiu, PhDCancer Risk& PreventionAndrea King, PhDUCCRC SCIENTIFIC REPORT 200999
MembersInvestigator*Habibul Ahsan MDAnirban Basu PhDMarc Bissonnette MDEugene Chang MDBrian Chiu PhDRena Conti PhDNancy Cox PhDWilliam Dale MD,PhDSoma Das PhDHarriet de Wit PhDAnna Di Rienzo PhDJames Dignam PhDNathan Ellis PhDSarah Gehlert PhDDavid Grdina PhDWilliam Green PhDTara Henderson MD,MPHSusan Hong MD,MPHDezheng Huo MD, PhDNora Jaskowiak MDKaren Kim MDAndrea King PhDRick Kittles PhDSonia Kupfer MDDiane Lauderdale PhDYan Chun Li PhDStacy Lindau MDChristopher Masi MD, PhDMartha McClintock PhDDaniel McGeHee PhDDavid Meltzer MD, PhDEneida Mendonca MD, PhDOlufunmilayo Olopade MBBSBlase Polite MDDavid Rubin MDLisa Sanchez-Johnsen PhDLisa Shah MD, MAMarion Verp MDPaul Vezina PhDIrving Waxman MDRankProfessorAssistant ProfessorAssociate ProfessorProfessorAssociate ProfessorInstructorProfessorAssistant ProfessorAssociate ProfessorProfessorProfessorAssociate ProfessorAssociate ProfessorProfessorProfessorAssociate ProfessorAssistant ProfessorAssistant ProfessorAssistant ProfessorAssistant ProfessorAssociate ProfessorAssociate ProfessorAssociate ProfessorInstructorAssociate ProfessorAssociate ProfessorAssistant ProfessorAssistant ProfessorProfessorAssociate ProfessorAssociate ProfessorAssociate ProfessorProfessorAssistant ProfessorAssociate ProfessorAssistant ProfessorInstructorAssociate ProfessorProfessorProfessorDepartmentHealth StudiesMedicineMedicineMedicineHealth StudiesPediatricsMedicineMedicineHuman GeneticsPsychiatryHuman GeneticsHealth StudiesMedicinePsychologyRadiation and Cellular OncologyNeurobiologyPediatricsMedicineHealth StudiesSurgeryMedicinePsychiatryMedicineMedicineHealth StudiesMedicineOB/GYNMedicinePyschologyAnesthesia/Critical CareMedicinePediatricsMedicineMedicineMedicinePsychiatryMedicineOB/GYNPsychiatryMedicine100UCCRC SCIENTIFIC REPORT 2009* Reflects all Program membership during 2008-2009
Featured Faculty Research Summaries †The Cancer Risk and Prevention Program conducts a broad scope ofresearch that encompasses basic studies of carcinogenesis, preclinical andclinical translational research, behavioral and epidemiological studies,as well as population-based genetic research. Investigators focus theirwork on research themes that reflect the scientific goals of the Program ashighlighted below.Theme: Genetic and Environmental Basis for CancerOlufunmilayo Olopade, MBBSProfessor of MedicineDr. Olopade’s multidisciplinary research team is workingto advance research on the prevention, early detection,and treatment of breast cancer, specifically focusing on theinterplay of genes and environment in the developmentof triple-negative breast cancer, which tends to be moreaggressive, less responsive to treatment, and more likelyto strike young women and those of African ancestry. Theteam is working to identify and characterize genes relevantDr. Olufunmilayo Olopadeto tumor progression, determine their role in inheritedsusceptibility, and perform genetic epidemiologic analysestranslatable to clinical practice. The laboratory is also focused on understanding epigenetic mechanisms underlyingabnormal gene expression, including aberrant CpG-island-promoter methylation of specific tumor suppressorgenes, global changes in genomic DNA methylation, and alterations in histone modification (deacetylation andmethylation).The ultimate goal of Dr. Olopade’s research is to develop more effective and less harmful methods to prevent, screen,and treat breast cancer in all women. The specific aims are to 1) identify and elucidate the genetic and environmentalfactors that influence breast cancer progression; 2) improve tools used for breast cancer diagnosis; and 3) developnew personalized therapies that specifically target tumors.Cancer Risk& PreventionRecent findings in the laboratory have revealed differences in tumor biology, with Africans and African Americanshaving poorly-differentiated tumors that lack estrogen receptor expression and present in advanced stages. Thesebiological differences lead to cancers that are more difficult to diagnose and treat, leading to poorer health outcomes.Thus, the findings suggest that disparities in cancer epidemiology are in part due to genetic differences among racial/ethnic populations.Rick Kittles, PhDAssociate Professor of MedicineDr. Kittles’ overall research focus is to formally evaluate genetic mechanisms involved in complex diseases. Hiswork entails understanding how genetic variation is structured across human populations and how that variationcontributes to inter-individual variation in disease susceptibility. His interests also include biological and socioculturalissues related to “Race” and health disparities.Recent findings in Dr. Kittles’ laboratory indicate that chromosome band 8q24.1 harbors four independent regionsof susceptibility to prostate cancer (Pca). These regions on 8q24 span over 2 million base pairs (Mb) and constitute agene desert, containing only four known transcription units and no apparent microRNA genes. Three of the regionscluster in a distal 8q24.1 region from 128.15 Mb to 128.65 Mb, which is itself 200 kb proximal to the MYC gene. Thelaboratory is currently trying to decipher the specific functional changes that occur in this region of DNA that lead† Note: Due to space constraints, only a small representative sample of Program members is presented here.UCCRC SCIENTIFIC REPORT 2009101
to prostate cancer. The work has major implications given that this region will likely be a target for drug development or riskassessment.The Kittles laboratory has been at the forefront of the development of ancestry-informative genetic markers, admixture mappingtheory, and applications for disease gene mapping in admixed populations, such as African Americans and Hispanics. Recently,Dr. Kittles’ laboratory and collaborators at Wayne State University completed an admixture mapping study for prostate cancersusceptibility genes in AAs. The team found significant evidence of association with Pca on chromosomes 5q35 and 7q31 andconfirmed the previous ancestry linkages on 8q24.1. Fine mapping with greater ancestry informative marker density in theseregions is needed to narrow the defined locus and better target candidate gene.Dr. Kittles firmly believes that genetics will play a major role in early detection and risk assessment for Pca, especially for AAmen given their higher risk compared to European Americans (EAs). High-risk men have been found to have Pca detected atlow PSA values, even 80%) may have a biopsy recommendation at a PSA of 3.0versus another AA man with a similar PSA value but lower WA ancestry (
on these new leads, Dr. Chiu and colleagues are developing a large bio-repository of blood and tissue samples from patientswith lymphoma and multiple myeloma at the University of Chicago that will be annotated not only with treatment andoutcome information, but also with molecular characteristics and extensive epidemiologic data. A strong emphasis will beplaced on the detection of factors for racial/ethnic disparities in hematopoietic cancers.Because NHL includes more than 20 histologic and clinicopathologic subtypes, a long period of time is required to conductstudies at a single institution with enough patients to yield the statistical power necessary to identify factors associated withrisk for rare subtypes of NHL. To address this issue, Dr. Chiu is collaborating with researchers around the world to pooldata across studies, including the International Lymphoma Epidemiology Consortium (InterLymph) and the InternationalMultiple Myeloma Consortium. For example, in a recent pooled analysis of 29,423 participants in the United States, Europe,and Australia, the InterLymph Consortium reported that Sjögren syndrome and Systemic lupus erythematosus are associatedwith a higher risk of marginal zone lymphoma and diffuse large B-cell lymphoma, whereas celiac disease and psoriasisare associated with a higher risk of T-cell lymphoma. As part of another worldwide collaboration, Dr. Chiu and colleaguesare developing a new consortium that will collect data from several Eastern Asian cities and countries. He will specificallyoversee the work at the Taiwan study site. This new consortium will provide a great opportunity to investigate environmentaland genetic risk factors for lymphoma in different populations.Theme: Models for Chemoprevention and Biomarker IdentificationHabibul Ahsan, MDProfessor of Health Studies, Medicine, and Human GeneticsDr. Ahsan’s research interests focus on studying the interrelationshipsbetween environmental and genomic factors incancer and exploiting information on these relationships ata population level for developing and evaluating preventioninterventions in humans. The research integrates environmental,nutritional, and life-style factors with measures of host factorsand molecular genomics (involving DNA, RNA and proteinvariations) to understand the etiology, pathogenesis, prognosis,and prevention of cancer and other disorders of national andinternational public health significance.Pathology image analysis in the UCCRC’s Human TissueResource Center.Ongoing NIH-funded major research projects include: 1) agenome-wide association study of early-onset breast canceramong 6,000 cases and controls; 2) a prospective cohort study of 20,000 men and women in Bangladesh to investigate thecancer risk from arsenic exposure; 3) genetic susceptibility to arsenic-related skin tumors among 3,000 cases and controls;and 4) a randomized trial of vitamin E and selenium among 6,000 arsenic-exposed patients for the prevention of cancers anddeaths.Cancer Risk& PreventionDr. Ahsan conducted a series of observational, pilot randomized chemoprevention trials (RCTs) and molecular studies,which led to a large skin tumor chemoprevention RCT for antioxidants. His team showed that arsenic is positively associatedwith oxidative stress biomarkers, including urinary 8-OHdG and F2-isoprostane, and plasma protein carbonyl, sICAM andsVCAM. His group was also the first to develop and validate a food frequency questionnaire (FFQ) for assessing the dietof South Asian populations, which revealed that dietary intakes of antioxidants reduce risk of arsenical skin tumors. Themeasurement of blood selenium levels indicated a strong, protective effect of selenium on risk of premalignant skin lesions. Ina parallel RCT, Dr. Ahsan’s team showed a clear enhancement of urinary arsenic excretion after selenium supplementation.The beneficial effects of selenium were further supported by molecular studies, in which the team demonstrated that arsenicexposure leads to aberrant expression of specific oxidative stress- and inflammation-related genes. In an independent study,UCCRC SCIENTIFIC REPORT 2009103
Dr. Ahsan’s team showed that selenium supplementation can revert these specific gene expressions and that arsenic causesglobal DNA hypermethylation, whereas in the same individuals, selenium leads to DNA hypomethylation.Based on these studies, a large chemoprevention RCT was established to evaluate the effects selenium and vitamin Esupplementation on prevention of skin tumorigenesis among 6000 study participants. While this 10-year trial is currentlyunderway, findings are likely to demonstrate important data on cancer chemoprevention. Dr. Ahsan is also involved in a seriesof observational, molecular, and short-term RCTs to establish folate as an effective agent in promoting excretion of arsenic fromthe body. However, unlike selenium and vitamin E, folate is unlikely to offer any long-term chemoprevention effect for canceronce arsenic exposure is removed and, thus, may not be suitable as a long-term chemoprevention modality.In addition, Dr. Ahsan and colleagues are studying genetic and other host determinants of cancer risk and survival, especiallyfor breast cancer. In a recent study, they showed that women carrying certain hormone-related genes are at higher risk of breastcancer and found that placental genetic profile is predictive of post-pregnancy breast cancer risk, suggesting that offspring’s andmating partner’s genotypes are predictive of risk. Dr. Ahsan’s team has also examined genomic losses and gains in breast cancerand identified novel loci. Currently, they are extending these investigations to understand genome level sequence variations aswell as loss or gain of genes in 3,000 women with early-onset breast cancer and in an equal number of age-matched controls.These findings will be followed by investigations of the same set of genomic determinants in relation to breast cancer survival.Marc Bissonnette, MDAssociate Professor of MedicineEpidermal growth factor receptors (EGFR) and their ligands are overexpressed in colon cancer. Dr. Bissonnette’s team hasshown that EGFR blockade inhibits experimental colonic carcinogenesis, and clinical studies have demonstrated efficacy of antiEGFR antibodies in combination with cytotoxic chemotherapy for metastatic human colon cancer. The overall objective of theBissonnette laboratory is to understand the roles of EGFR in colonic carcinogenesis and develop chemopreventive strategies.Azoxymethane (AOM) and azoxymethane/dextran sulfate sodium (AOM/DSS) carcinogen models are employed using micewith up- or down-regulated EGFR signaling cascades to elucidate growth factor pathways in sporadic and inflammatory humancolon cancer. In the AOM and AOM/DSS models, the laboratory demonstrated that EGFR and its ligands are up-regulated indysplastic aberrant crypt foci, the earliest detectable premalignant lesion in colonic carcinogenesis. Furthermore, EGFR signalsare required for later stages of tumor progression.Environmental factors, especially dietary constituents, contribute substantially to the risk of sporadic human colon cancer.Recent studies in the laboratory indicated that tumor promotion by Western style dietary fat also requires EGFR signals. Thiseffect appears to involve increases in cyclooxygenase-2 (Cox-2) in the tumor stroma. Cox-2 is the rate-limiting enzyme inbiosynthesis of prostanoids that drive proliferation, angiogenesis, and cell survival. The Bissonnette group is currently dissectingthe roles of stromal fibroblast and epithelial EGFR to understand their contributions to Cox-2 regulation in tumorigenesis. Incontrast to tumor promoting effects of Western style dietary fat, other naturally-occurring dietary constituents, such as greentea, curcumin and vitamin D3, exhibit chemopreventive activity against colon cancer. These substances also inhibit EGFRsignals, but the role of EGFR inhibition in their anti-cancer effects has not been elucidated. This previously unknown interactionof EGFR and diet could potentially be exploited using such naturally occurring agents to reduce the diet-associated colon cancerrisk for insulin-dependent diabetes and obesity. Furthermore, development of more effective chemopreventive analogues, basedperhaps upon their EGFR inhibitory profile, might provide improved strategies to prevent this often-fatal disease.Specific aims in the laboratory include 1) dissection of the roles of epithelial cell and fibroblast EGFR in colonic neoplastictransformation; 2) identification of targets regulated by miR-143 and miR-145 in colonic tumorigenesis; 3) studies to uncoverthe connections between diet and EGFR in colonic tumor promotion; 4) elucidation of the roles of EGFR in tumor invasion andmetastasis, as the laboratory showed that loss of EGFR in stromal cells greatly attenuated colon cancer tumor xenograft growth;and 5) deciphering vitamin D-VDR pathways that inhibit diet-induced inflammation and colon cancer development.104The laboratory has also recently discovered a novel and potentially important role for EGFR in regulating microRNA in colonictumorigenesis. These small non-coding RNA regulate messenger RNA stability or translation and are involved in a wide rangeUCCRC SCIENTIFIC REPORT 2009
of normal and malignant processes. Putative tumor suppressors, such as miR-143 and miR-145, are down-regulated in coloncancer. In the AOM/DSS model, this down-regulation requires EGFR. Consistent with these findings, the laboratory showedthat EGFR negatively regulates these miRNA in cell culture. Conversely, when miR-143 and miR-145 were transfected intocolon cancer cells, these miRNA inhibited EGFR-induced proliferation. Thus, tumor-promoting effects of EGFR appear to bemediated at least in part by down-regulating miR-143 and miR-145. Studies are in progress to understand how EGFR regulatesthese miRNA and what targets mediate their effects.Nathan Ellis, PhDAssociate Professor of MedicineThe overall research focus of the Ellis laboratory is the study of genomic instability and its relationship to colorectal cancer(CRC) susceptibility. Germline mutations and somatic genetic changes in DNA repair genes are causally linked to hereditaryCRC cancer syndromes and carcinogenesis, respectively, demonstrating that the maintenance of genomic integrity plays acrucial role in cancer susceptibility. The laboratory employs candidate gene and genome-wide association studies to identifycancer risk genes and carries out DNA sequencing studies to pinpoint and analyze culprit mutations. These genetic analysesare combined with functional analyses to determine how genetic alterations alter repair function and cause increased cancersusceptibility.A particular strength of Dr. Ellis’s laboratory is the capacity to perform comparative genetic studies in different humanpopulations to assess the impact on cancer risk. The patient base at The University of Chicago includes a large contingentof African Americans (AA), which offers a more genetically diverse perspective than other populations and results in anincreased power to localize genetic risk factors to smaller regions. In addition, heterogeneity in genetic risk factors hasproven useful in elucidating risk factor functions, especially those of low frequency. The Ellis laboratory also examinesAA-specific factors in CRC incidence to shed light on the causes of health disparities in this population. A consortium ofCRC investigators at major Chicago hospitals, who are pooling biological specimens, clinical data, and research expertise toenhance these comparative studies, has been established.The Ellis laboratory studies genetic risk factors in CRC through the identification of high-interest DNA repair genes frompublished genome-wide association and other biological studies. By searching HapMap and public sequence databases, singlenucleotide polymorphisms (SNPs) in the high-interest genes are analyzed, identifying tagging SNPs so that a systematicanalysis of all genetic variation can be conducted. Next, the frequencies of these genetic polymorphisms are compared incases versus controls in a large cohort from the University of Chicago to identify associations that potentially increase CRCrisk. Putative risk factors are replicated in additional case-control cohorts, and regions that contain putative risk factorsare subjected to deep sequence analysis. Further genotype analysis is performed to pinpoint candidate causal sequencealterations. The causal sequence alterations in cell culture systems are then studied to determine their effects on DNA repairfunction and genomic integrity.Cancer Risk& PreventionThe laboratory performed a systematic SNP analysis of genes in the base excision repair (BER) pathway, which removesoxidative and other damages from DNA, and found a strong association between a pair of contiguous SNPs in XRCC1 and AACRC cases. The same SNPs were not associated with CRC in European Americans, nor were previously studied amino acidsubstitutions in XRCC1 found to be associated with CRC in either population. Bioinformatic analysis has identified importantregulatory sequences in the region containing these two SNPs, which is now the focus of deep sequence analysis.In multiple genome-wide association studies, a series of small regions in a two million base pair segment of chromosome8q24.1 have been associated with prostate, colorectal, breast, and ovarian cancer. In collaboration with Dr. Rick Kittles, thelaboratory has linked SNPs in a DNA repair gene called MMS21 with CRC, which intersects with functional studies of theBLM gene involved in homologous recombination repair. The Ellis laboratory is currently sequencing the MMS21 region tofully explore alterations that are associated with genetic risk, develop cell culture models for studying the role of MMS21 inhomologous recombination repair, and assay BLM functions. These models will eventually be used to dissect culprit sequencealterations and elucidate the molecular mechanisms by which they confer increased genetic risk.UCCRC SCIENTIFIC REPORT 2009105
Theme: Psychological and Bio-Behavioral Basis of Cancer Risk and PreventionMartha McClintock, PhDProfessor of PyschologyDr. McClintock studies the reciprocal interactions between socialbehavior and psychological states. Because behavior and biologicalmechanisms are reciprocally linked, Dr. McClintock’s researchcenters on the behavioral control of endocrinology, immunologyand disease, in addition to the hormonal and neuroendocrinemechanisms of behavior. Current interests in the laboratory focuson breast cancer, working with both animal and parallel clinicalprocesses in humans.Development of a fingerstick blood spot technique,a minimally invasive method for obtaining biologicalIn collaboration with Dr. Suzanne Conzen (Cell Signaling and Geneinformation in population-based cancer risk research.Regulation Program), the laboratory discovered that social isolation(Image by S. Lindau)increases the risk of malignant mammary tumors, acceleratesaging and shortens the lifespan in both rat and transgenic mousemodels. These results demonstrate that social isolation regulates gene expression. Through additional work with the Centerfor Interdisciplinary Health Disparities Research, Dr. McClintock is applying this basic research to understand the dramatichealth disparity in mortality between African-American women and women of Northern European ancestry with breast cancer.In addition, Dr. McClintock collaborates with Center colleagues, Drs. Gehlert and Olopade, in conducting translational healthdisparities research among African-American women, in the communities surrounding the University of Chicago, who havebreast cancer and are at greater risk for high mortality. The goal of this research is to identify social and psychological factorsthat underlie the dramatic health disparity in Chicago, utilizing the insights gained to reduce risk in all women.In a life span study, the McClintock laboratory examined how the social environment regulates spontaneous mammary tumordevelopment and malignancy in genetically-prone Sprague-Dawley rats by randomly assigning animals to live either alone orin groups of five female rats. Mammary tumor burden among social isolates increased to eighty-four times that of age-matchedcontrols, as did tumor malignancy. Specifically, social isolates showed a 3.3 relative risk for observed ductal carcinoma insitu and invasive ductal carcinoma, the most common early breast cancers in women. Importantly, isolation did not extendovarian function in late middle age; in fact, isolated animals were exposed to lower levels of estrogen and progesterone in themiddle-age period of mammary tumor growth while tumor estrogen and progesterone receptor status remained unchanged.Isolates, however, did develop significant dysregulation of corticosterone responses to everyday stressors manifest before tumordevelopment in early adulthood, and enduring across the lifespan. Among isolates, corticosterone recovery from an acutestressor was highly attenuated and associated with increased progression of mammary tumors. In addition to being stress andtumor prone, an array of behavioral measures demonstrated that socially isolated females possess an anxious, fearful, andvigilant phenotype.This animal model of spontaneous breast cancer provides a framework for studying the interaction of social neglect with geneticrisk to identify mechanisms whereby psychosocial stressors increase malignancy and growth of breast cancer. Specifically, aspart of the National Social Life Health and Aging Project (NSHAP), Dr. McClintock is examining psychosocial mechanismsof malignant disease, reconceptualizing health during aging to include mental health and social context. In a sample of 3,000people between the ages of 57 and 85, selected to be demographically representative of the United States, reproductive cancersare the second most prevalent cancers, with skin cancer being the most common. In a nude mouse model of skin cancer, socialisolation in the face of recurring stressors accelerated the progression of skin cancers following UV radiation. The social andpsychological risk factors of both reproductive and skin cancers will be further studied in the second wave of the NSHAP, inwhich the sample will be expanded to 4,500 by including partners of the original participants. Genetic and stress measures willbe obtained, in addition to the original biomeasures, including medical histories, psychological profiles and social structures.106UCCRC SCIENTIFIC REPORT 2009
Harriet de Wit, PhDProfessor of PsychiatryThe Human Behavioral Pharmacology Laboratory (HBPL), directed by Dr. de Wit, studies the causes and consequences ofrecreational drug use, including cancer-related drugs such as tobacco and alcohol. Causes of drug use include factors suchas personality, genetics, stress, and behavioral dimensions, such as sensitivity to reward or insensitivity to punishment. Thelaboratory studies these risk factors as predictors of individuals’ responses to low doses of a drug, which, in turn, can predictrisk for future use. Drugs of abuse have complex effects on behavior, including effects on mood states, decision-making,and cognition that can lead to repeated, or hazardous, use of the drugs. These drug effects are studied under controlledconditions to identify risk factors for repeated or hazardous use.One important aim of the research is to identify brain mechanisms that mediate the behavioral effects of drugs. Incollaboration with Dr. Abe Palmer of the Department of Human Genetics, the laboratory is studying variations in thegenes that encode proteins involved in neurotransmitter functions, in relation to the behavioral responses to acute drugadministration. For example, the deWit team has shown that polymorphisms in genes encoding aspects of dopaminereceptor function are associated with variations in the behavioral effects of d-amphetamine. That is, some of the interindividualdifferences in acute responses to a stimulant drug can be explained by variation in the targets of the drug’s action.These variations may also affect future risk for using the drug in a hazardous or excessive manner.Another aim of the research is to study the relationships between stress and drug use. Stress is thought to increase therisk for drug use, and drug use, in turn, may affect an individual’s responses to stress. In collaboration with Drs. AndreaKing, Ajna Hamidovic and Emma Childs, of the Department of Psychiatry and Behavioral Neuroscience, the laboratory isstudying stress responses in young adults as predictors of cigarette smoking. In one study that was supported by the UCCRC,the team is testing whether behavioral and physiological responses to an acute social stressor (a public speaking task)predicts progression from occasional smoking to regular smoking over a 6 month period. In other studies, the laboratory isinvestigating the effects of acute stress on responses to drugs, and the effects of drugs on responses to acute stress. Takentogether, these studies will improve the current understanding of complex interactions between stress and drug use, and howstress may increase risk for future drug use.Cancer Risk& PreventionIn a further study, the de Wit laboratory is studying factors involved in relapse to smoking. Drug users, including smokers,remain at risk for relapse long after the drug’s effects have subsided, and most drug users who are able to quit ultimatelyrelapse. Relapse is thought to be related to conditioned, drug-related cues, but it is not known how reactions to these cueschange with time. Recent studies with animal models of relapse suggest that cues become more, rather than less, effectivewith longer periods of abstinence. In collaboration with researchers at the National Institute on Drug Abuse IntramuralResearch Program, the laboratory is studying craving elicited by smoking-related cues in smokers who abstain for 7, 14 or 35days to study the time course of cue-induced cravings. This study will provide important information about how drug-relatedcravings change over the course of extended periods of abstinence from smoking.UCCRC SCIENTIFIC REPORT 2009107
Daniel McGehee, PhDAssociate Professor of Anesthesia/Critical CareThe primary goal of the research in Dr. McGehee’s laboratory is understanding the cellular mechanisms underlying nicotineaddiction. Nicotine is the principal neuroactive component of tobacco, and addiction to tobacco products is one of the maincauses of preventable illness and premature death in this country. Tobacco use is associated with remarkably high prevalence ofmultiple forms of cancer.Using electrophysiological recording methods in rat brain slices, the laboratory is testing synaptic transmission and plasticitywithin brain reward circuitry. The brain areas being investigated include the midbrain dopamine system, its afferent inputs,and efferent projection sites. The aims of Dr. McGehee’s research are to assess the impact of both acute and long-term nicotineexposure on synaptic strength in the ventral tegmental area, nucleus accumbens, and brainstem cholinergic centers. Withsupport from the UCCRC, the laboratory has recently begun to investigate the impact of co-administration of nicotine andethanol, as these drugs are the most commonly abused substances in our society with a high degree of co-morbidity. In thisregard, the McGehee team is testing the interaction of ethanol with nicotinic receptors in these brain areas. Preliminaryresults indicate profound enhancement of nicotinic responses in VTA, but significant suppression in the brainstem cholinergiccenters. This line of research may lead to novel treatments for both nicotine and ethanol abuse.The most recently published work investigated the impact of nicotine and opiate drugs on dopamine release in the nucleusaccumbens and dorsal striatum. A profound overlap of the effects of these two classes of addictive drugs was observed ondopamine release dynamics. The data suggest a common mechanism in rewarding effects of these drugs, again suggestingpossible treatment strategies.Theme: Community Outreach to Reduce Health DisparitiesKaren Kim, MDAssociate Professor of MedicineDr. Kim is nationally recognized as an advocate for reducinghealth disparities and equal access to health care for AsianAmericans and is the cofounder of the Asian CancerPrevention Organization. Specifically, Dr. Kim’s researchinterest focuses on community based interventions directed atimproving access to cancer screening in minority populations.Research is focused on two specific cancers, hepatocellularcarcinoma and colorectal cancer. Her interest in hepatitis BDr. Rick Kittlesinduced liver cancer is part of a recently Centers for DiseaseControl-funded program which addresses awareness andcultural competent messaging to improve hepatitis B screening in Asian Americans. Asian Americans have the highest rates ofhepatocellular cancer worldwide as a direct result of chronic infection with hepatitis B. Dr. Kim’s research utilizes a lay healtheducator model in several Chicago Asian communities, including Chinese, Korean, Vietnamese, Laotian, and Cambodianimmigrant communities to improve awareness and screening for hepatitis B to decrease the liver cancer burden in these highrisk and underserved communities. Prevalence rates for chronic hepatitis B infection vary significantly between ethnic specificcommunities with rates as high as 13.5% in Chinese communities, and as low as 4.6% in Korean communities. These efforts haveresulted in increased funding to address the need to disaggregate the Asian American community health data to understandthe health disparities better in minority communities. Dr. Kim is part of a community-wide research program to collect localhealth indices for cancer screening in order to inform policy and public health leaders about the need for programs directedtoward these culturally- and linguistically-isolated communities.108UCCRC SCIENTIFIC REPORT 2009
Dr. Kim’s second area of research interest addresses disparities in colorectal cancer in African Americans. Despite thehigher incidence of colorectal cancer in African Americans, studies addressing interventions specifically targeting cancerprevention are lacking. Low Vitamin D levels have been hypothesized to be associated with increased mortality fromcolorectal cancer, and epidemiological studies show that African Americans are at greatest risk for reduced vitamin D levels.Therefore, chemoprevention trials using vitamin D may have a greater impact on African Americans than other populations.Unfortunately, national clinical trials using vitamin D have low African American enrollment. Dr. Kim’s research, fundedby the American Cancer Society and the UCCRC, studies the feasibility of vitamin D chemoprevention on polyp preventionin African Americans. Preliminary results have shown recruitment rates of 80% with 35% enrollment. Ongoing work tounderstand barriers to minority enrollment in clinical trials continue to be a priority. Dr. Kim hopes to expand this workinto a multi-center study in the near future.Lisa Sanchez-Johnsen, PhDAssistant Professor of PsychiatryDr. Lisa Sánchez-Johnsen is the Director of both the Multicultural Health Research Program and the Latino HealthResearch Program in the Department of Psychiatry & Behavioral Neuroscience. She has extensive experience in communityparticipatory research and has served as the chair of several community advisory boards for Latino health in Illinois andHawaii. As part of Dr. Sánchez’s research studies, she has active involvement in Hispanic/Latino Health CommunityAdvisory Boards, which are instrumental in developing and implementing those studies. Her areas of interest includeconducting cancer prevention research with underserved ethnic minority groups, such as Latinos, African Americans, andAsians. She is currently conducting clinic and community-based and culturally competent cancer risk reduction assessmentsand interventions in the areas of obesity, physical activity, body image, and smoking.As part of Dr. Sánchez’s K01 award and her U of C Health Disparities Research grant, she is pilot-testing a communitybasedobesity and secondhand smoke education intervention with 40 Latina women. The specific aims of her K01 study areto: 1) test the acceptability and feasibility of a 6-week culturally-proficient diet, physical activity, body image, and tobaccointervention in 40 overweight Latinas using a community-based participatory framework; 2) estimate the effectiveness ofthis intervention on weight loss, healthy body image, healthy eating, physical activity; and secondhand smoke education; and3) develop and adapt measures of diet, physical activity, body image, and tobacco use to be culturally proficient for Latinas,and compare their reliability and validity. In the first phase, she completed quantitative and qualitative interviews with 20women to test the acceptability of the questionnaires and to guide the development of the intervention. In the second phase,she is conducting a culture-based diet, physical activity, body image, and tobacco intervention for overweight Latina females,using a community-based participatory research framework.Cancer Risk& PreventionDr. Sánchez’s early research revealed that Blacks consumed more calories and percent calories from fat than Latinas, whereasLatinas consumed more fiber and calories from carbohydrates and protein than Blacks. Latinas also preferred a thinnerbody and had a greater body image discrepancy than Blacks. Blacks were also more sedentary than Latinas. These findingshighlighted the need to explore cultural variables underlying ethnicity, as it relates to diet, physical activity, and body image,so that culture-based community obesity interventions can be developed. To address this need, Dr. Sánchez is conductingan NCI R21 study (to explore the role of four cultural variables (acculturation, acculturative stress, ethnic identity, andcultural values) that may help to explain the ethnic disparities in correlates of overweight/obesity (diet, physical activity,and body image) among Mexican and Puerto Rican women. The research will also identify logistical/practical and culturalconsiderations regarding the development of diet, physical activity, and body image interventions for overweight Mexican andPuerto Rican women. Results will be used to develop tailored and targeted interventions that address diet, physical activity,and body image in overweight Mexican and Puerto Rican women of various acculturation levels.UCCRC SCIENTIFIC REPORT 2009109
Sarah Gehlert, PhDProfessor of the School for Social Service AdministrationDr. Sarah Gehlert is the Principal Investigator of the Center for Interdisciplinary Health Disparities Research (CIHDR), fundedby an initiative of the National Cancer Institute, National Institute of Environmental Health Sciences, Office of Social andBehavioral Research, and National Institute of Aging. The CIHDR aims to 1) bring together scientists from inside and outsidethe University and members of the community to inform the CIHDR’s scientific agenda; 2) increase interest in populationhealth and health disparities among scientists and students from various disciplines and from community members; and 3)disseminate findings to as wide an audience as possible, including members of vulnerable populations, community-basedorganizations and agencies, and scientific investigators inside and outside the University.Dr. Gehlert also leads one of CIHDR’s four interdependent and mutually-informative research projects entitled “Socialenvironment, stress, and health.” In its first year of operation, the project conducted 49 community-based participatory focusgroups in South Side Chicago neighborhood areas to understand how residents conceptualize breast cancer and its treatmentand how accurately psychosocial constructs and measures used in other CIHDR projects captured residents’ life experiences.Dr. Gehlert contributed towards two publications that resulted from focus group activities, involving community epidemiologyof breast cancer risk and perceptions of breast cancer and its treatment among African-American women and men.The project shares a central research question with CIHDR projects by Drs. Fumni Olopade, Martha McClintock, and SuzanneConzen (Cell Signaling and Gene Regulation Program), namely how factors in women’s social environments contribute to theAfrican American and white disparity in breast cancer mortality in the United States. Informed by the focus group data andexperiences, the Gehlert laboratory staff worked with African American women newly diagnosed with breast cancer living onChicago’s South Side to address two additional specific aims: 1) to utilize the informed and modified instruments along withbiological/genetic- and neighborhood/community-level variables to understand the relationships between social, behavioral,and biological factors in the etiology of breast cancer among African-American women (compared to white women); and 2)to develop recommendations to inform health care policy, practice, and education around breast cancer. Women are followedfor 1.5 years, and data is collected inside the home (perceived discrimination, social network living arrangements, depression)and in a four-block area around each woman’s home to assess built environment and publically-available data on crime,socioeconomic status, etc. geo-coded to each woman’s address. As a result, the team outlined a multi-level model of breastcancer, and in collaboration with the Principal Investigators of the other eight centers funded by the same initiative, outlinedtheir shared model of how disparities develop.110UCCRC SCIENTIFIC REPORT 2009
Additional Program Highlights*Research••Community-Based Smoking Cessation to Reduce African American Health Disparities. Andrea King, PhD, LisaSánchez-Johnsen, PhD, and colleagues developed an intensive group-based smoking cessation intervention program andprovided transdermal nicotine patches to urban low- and middle income African American smokers to reduce healthdisparities in access and comfort with tobacco interventions. Results showed the majority of participants completed theintervention, adhered to patch and approximately one-third had quit smoking by the end of treatment. Predictors of successin treatment included patch adherence, utilization of the cognitive-behavioral skills in the program, and lower negativeeffect. The research team concluded that more studies are warranted to examine targeted treatment elements and individualdifference factors to enhance cessation outcomes in African American smokers (King et al., Journal National Med Assoc100:208-217, 2008).••Prediction of BRCA Mutations Using the BRCAPRO Model in Clinic-Based African American, Hispanic, and OtherMinority Families in the United States. BRCAPRO, a BRCA1/BRCA2 mutation carrier prediction model, was developed onthe basis of studies in individuals of Ashkenazi Jewish and European ancestry. Olufunmilayo Olopade, MBBS, and DezhengHuo, MD, PhD evaluated the performance of the BRCAPRO model among clinic-based minority families and assessed theclinical utility of mutation status of probands (the first individual tested in a family) in the recommendation of BRCA1/BRCA2 mutation testing for other at-risk family members. The findings support the use of BRCAPRO in pretest BRCA1/BRCA2 mutation prediction among minority families in clinical settings, but there is room for improvement in ethnicgroups other than Hispanics. Knowledge of the mutation status of the proband provides additional predictive value, whichmay guide genetic counselors in recommending BRCA1/BRCA2 testing of additional relatives when a proband has testednegative (Huo et al., J Clin Oncol 10;27(8):1184-1190, 2009).••Racial differences in clinical outcomes from metastatic breast cancer. Blaise Polite, MD, and his colleagues examinedracial differences in clinical outcomes in the setting of two large cooperative group randomized clinical trials. The studycohort consisted of 787 white and 195 African American patients with metastatic breast cancer enrolled in two successiveCancer and Leukemia Group B (CALGB) trials using taxanes in the metastatic setting. African Americans with metastaticbreast cancer have an increased hazard of death compared with whites despite the receipt of similar per-protocol treatment,but experience no differences in time to treatment failure or overall response to therapy. More direct and robust measuresof comorbidities, and perhaps other factors, such as receipt of subsequent therapy could help further explain the observedsurvival difference (Polite et al., J Clin Oncol 26(16):2659-2665, 2008).Cancer Risk& Prevention••Population Specific GSTM1 Copy Number Variation. As one of the majorglutathione conjugation enzymes, GSTM1 detoxifies a number of drugs andxenobiotics. Through a genome-wide association study, Nancy Cox, PhD,Soma Das, PhD, and M. Eileen Dolan, PhD (Clinical and ExperimentalTherapuetics Program) identified a significant association between HapMapSNP rs366631 and GSTM1 expression. HapMap rs366631 is a pseudo-SNPthat can be used as a GSTM1 deletion marker. Both the pseudo-SNP allelefrequency and GSTM1 upstream region copy number variation showpopulation-specific patterns between Caucasian and African samples(Huang et al., Hum Mol Genet 18(2):366-372, 2009).Dr. Tara Henderson* Due to space constraints, only a small representative sample of Program highlights is presented here.UCCRC SCIENTIFIC REPORT 2009111
Selected New Funding•• Lisa Sanchez-Johnsen, PhD, was the recipient of a National Cancer Institute R21 award to examine the role of fourcultural variables (acculturation, acculturative stress, ethnic identity, and cultural values) that may help to explain theethnic disparities in levels of obesity within the Hispanic/Latino community. The findings from this study will aid inassessing the role of ethnicity and culture in obesity-related variables, and identify some of the cultural factors that shouldbe accounted for when developing obesity interventions for Mexicans and Puerto Ricans.••••••••Harriet Dewit, PhD, in collaboration with Cecilia Hillard, MD, Professor at the Medical College of Wisconsin, was therecipient of a National Institutes for Health R21 award to test the theory that gender differences in the effects of stress onendocannabinoid (eCB) signaling contribute to the gender differences in susceptibility to certain psychiatric disorders.Data from this study will help to clarify the differential vulnerabilities of women and men to certain disorders, substanceabuse in particular.Tara Henderson, MD, MPH, and her colleagues, with funding from a National Cancer Institute K07 award, are examiningthe long-term health of childhood cancer survivors, a high risk group for both early deaths and subsequent illnesses dueto second cancers. Dr. Henderson is developing a four-year training program to examine the long-term trends that affectthis group, and also research methods for examining the clinical outcomes, health beliefs and behaviors of a targetedgroup of women who developed breast cancer following chest radiation for a pediatric cancer.Andrea King, PhD, was awarded an R01 grant from the National Institutes of Health to study the factors associated withalcohol stimulation and sedation in binge drinkers. Data from this study will determine the relative contributions ofsensitivity to stimulant-like alcohol effects, tolerance to sedative-like effects, and objective responses to future drinkingpatterns over time. Such information may have an important impact on the early identification of at-risk drinkers and thefactors underlying hazardous drinking practices to improve prevention, education, and early intervention efforts.Eugene Chang, MD, was the recipient of an R21 award from the National Center for Human Genome Research to developtechnologies for the discovery of novel human colonic mucosal-associated microbes. Current methods are likely to diluteand distort sampling of the enteric microbiome, and are likely to miss underrepresented species that may have directbearing on human health and disease. This study is anticipated to produce new and improved non-cultivation-basedtechnologies that will facilitate genomic sequencing and metagenomic analysis of previously uncharacterized members ofthe human enteric microbiome.•• Dezheng Huo, MD, PhD, received R03 funding from the National Cancer Institute to characterize breast cancersubtypes using an integrative genetic and epidemiologic approach. The study aims to determine the pattern of loss ofheterozygosity and copy number alterations between subtypes and to examine germline determinants. The resultswill improve the prevention and treatment of breast cancer by identifying genetic variants predisposing individuals todifferent subtypes of the disease.112UCCRC SCIENTIFIC REPORT 2009
New Faculty Recruitments and UCCRC MembersBrian Chiu, PhD is a cancer epidemiologist whose research focuses on integrating advanced molecular techniques withtraditional epidemiologic methods to examine host and environmental factors that influence the etiology of hematopoieticcancers. Dr. Chiu’s research includes the examination of lifestyle, environmental, and genetic factors that contribute to thepathogenesis of non-Hodgkin lymphoma to identify potential prevention strategies.Susan Hong, MD, MPH, is an internist with an interest in cancer survivorship. Dr. Hong has developed a women’s healthcurriculum for the internal medicine residents, which has been integrated into the residency program. Dr. Hong has establisheda Cancer Survivorship Clinic with an initial focus on breast cancer survivors. In addition to providing clinical services, thisclinic provides the structure for the expansion of survivorship research.Dezheng Huo, MD, PhD is a statistician and cancer epidemiologist with broad biostatistical research interests including theetiology and prevention of cancer in underserved and under-studied populations. Dr. Huo is currently studying polymorphismsand reproductive factors in breast cancer risk among Africans; the incidence of breast cancer subtypes across ethnic groups inthe U.S.; and genetic, environmental, and lifestyle factors that influence the risk for breast cancer subtypes.Sonia Kupfer, MD was recruited as an Instructor in the Department of Medicine. Dr. Kupfer performs genetic associationstudies in colorectal cancer with a special focus on African Americans.Eneida Mendonca, MD, PhD is a member of the Computation Institute of the University of Chicago and Argonne NationalLaboratory. Dr. Mendonca uses mining and retrieval technologies to improve the diagnosis and treatment of pediatric cancer.Her current interests focus on using computational methods and informatics to analyze biomedical data in order to build aninfrastructure to support pediatric oncology research. Dr. Mendonca is also interested in exploring long-term health issues andelucidating decision-making processes associated with pediatric cancer treatment and survivorship.Lisa Shah, MD, MA is an Instructor in the Department of Medicine whose interests include hospital-based smoking cessationinterventions, preventive health care, and quality improvement.Cancer Risk& PreventionUCCRC SCIENTIFIC REPORT 2009113
Selected Publications* : Intraprogrammatic Collaboration# : Interprogrammatic CollaborationAhsan, Habibul MD* Argos M, Kibriya MG, Jasmine F, Olopade OI, Su T, Hibshoosh H, Ahsan H.Genomewide scan for loss of heterozygosity and chromosomal amplification inbreast carcinoma using single-nucleotide polymorphism arrays. Cancer GenetCytogenet 182(2):69-74, 2008.* Huo D, Adebamowo CA, Ogundiran TO, Akang EE, Campbell O,Adenipekun A, Cummings S, Fackenthal J, Ademuyiwa F, Ahsan H, OlopadeOI. Parity and breastfeeding are protective against breast cancer in Nigerianwomen. Br J Cancer 98(5):992-6, 2008.Kaklamani VG, Wisinski KB, Sadim M, Gulden C, Do A, Offit K, Baron JA,Ahsan H, Mantzoros C, Pasche B. Variants of the adiponectin (ADIPOQ) andadiponectin receptor 1 (ADIPOR1) genes and colorectal cancer risk. JAMA300(13):1523-31, 2008.Jasmine F, Ahsan H, Andrulis IL, John EM, Chang-Claude J, Kibriya MG.Whole-genome amplification enables accurate genotyping for microarraybasedhigh-density single nucleotide polymorphism array. Cancer EpidemiolBiomarkers Prev 17(12):3499-508, 2008.Pierce BL, Ahsan H. Case-only genome-wide interaction study of disease risk,prognosis and treatment. Genet Epidemiol, 2009.Heck JE, Nieves JW, Chen Y, Parvez F, Brandt-Rauf PW, Graziano JH,Slavkovich V, Howe GR, Ahsan H. Dietary intake of methionine, cysteine, andprotein and urinary arsenic excretion in Bangladesh. Environ Health Perspect117(1):99-104, 2009.Chen Y, Kibriya MG, Jasmine F, Santella RM, Senie RT, Ahsan H. Do placentalgenes affect maternal breast cancer? Association between offspring’s CGB5 andCSH1 gene variants and maternal breast cancer risk. Cancer Res 68(23):9729-34, 2008.Basu, Anirban PhD* Yin W, Basu A, Zhang JX, Rabbani A, Meltzer DO, Alexander GC. Theeffect of the Medicare Part D prescription benefit on drug utilization andexpenditures. Ann Intern Med 148(3):169-77, 2008.* Dale W, Basu A, Elstein A, Meltzer D. Predicting utility ratings for jointhealth States from single health States in prostate cancer: empirical testing of 3alternative theories. Med Decis Making 28(1):102-12, 2008.* Basu A, Dale W, Elstein A, Meltzer D. A linear index for predicting jointhealth-states utilities from single health-states utilities. Health Econ 18(4):403-19, 2009.Alexander GC, Zhang J, Basu A. Characteristics of patients receivingpharmaceutical samples and association between sample receipt and out-ofpocketprescription costs. Med Care 46(4):394-402, 2008.Bissonnette, Marc MD# Dougherty U, Sehdev A, Cerda S, Mustafi R, Little N, Yuan W, JagadeeswaranS, Chumsangsri A, Delgado J, Tretiakova M, Joseph L, Hart J, Cohen EE, AluriL, Fichera A, Bissonnette M. Epidermal growth factor receptor controls flatdysplastic aberrant crypt foci development and colon cancer progression in therat azoxymethane model. Clin Cancer Res 14(8):2253-62, 2008.# Khare S, Mustafi R, Cerda S, Yuan W, Jagadeeswaran S, Dougherty U,Tretiakova M, Samarel A, Cohen G, Wang J, Moore C, Wali R, Holgren C,Joseph L, Fichera A, Li YC, Bissonnette M. Ursodeoxycholic acid suppressesCox-2 expression in colon cancer: roles of Ras, p38, and CCAAT/enhancerbindingprotein. Nutr Cancer 60(3):389-400, 2008.Sun J, Mustafi R, Cerda S, Chumsangsri A, Xia YR, Li YC, Bissonnette M.Lithocholic acid down-regulation of NF-kappaB activity through vitamin Dreceptor in colonic cancer cells. J Steroid Biochem Mol Biol 111(1-2):37-40,2008.Wali RK, Kunte DP, Koetsier JL, Bissonnette M, Roy HK. Polyethylene glycolmediatedcolorectal cancer chemoprevention: roles of epidermal growth factorreceptor and Snail. Mol Cancer Ther 7(9):3103-11, 2008.# Keswani RN, Chumsangsri A, Mustafi R, Delgado J, Cohen EE, BissonnetteM. Sorafenib inhibits MAPK-mediated proliferation in a Barrett’s esophagealadenocarcinoma cell line. Dis Esophagus 21(6):514-21, 2008.* # Tao Y, Hart J, Lichtenstein L, Joseph L, Ciancio M, Hu S, Chang EB,Bissonnette M. Inducible Heat Shock Protein70 Prevents Multifocal FlatDysplastic Lesions and Invasive Tumors in an Inflammatory Model of ColonCancer. Carcinogenesis 30(1):175-82, 2009.* Hu S, Zhu X, Triggs JR, Tao Y, Wang Y, Lichtenstein L, Bissonnette M,Musch MW, Chang EB. Inflammation-induced, 3’UTR-dependent translationalinhibition of Hsp70 mRNA impairs intestinal homeostasis. Am J PhysiolGastrointest Liver Physiol 296(5):G1003-11, 2009.Chang, Eugene MD* # Tao Y, Hart J, Lichtenstein L, Joseph L, Ciancio M, Hu S, Chang EB,Bissonnette M. Inducible Heat Shock Protein70 Prevents Multifocal FlatDysplastic Lesions and Invasive Tumors in an Inflammatory Model of ColonCancer. Carcinogenesis 30(1):175-82, 2009.* Hu S, Zhu X, Triggs JR, Tao Y, Wang Y, Lichtenstein L, Bissonnette M,Musch MW, Chang EB. Inflammation-induced, 3’UTR-dependent translationalinhibition of Hsp70 mRNA impairs intestinal homeostasis. Am J PhysiolGastrointest Liver Physiol 296(5):G1003-11. Epub, 2009.Sakiyama T, Musch MW, Ropeleski MJ, Tsubouchi H, Chang EB. Glutamineincreases autophagy under Basal and stressed conditions in intestinal epithelialcells. Gastroenterology 136(3):924-32, 2009.Musch MW, Arvans DL, Wu GD, Chang EB. Functional coupling of thedownregulated in adenoma Cl-/base exchanger DRA and the apical Na+/H+ exchangers NHE2 and NHE3. Am J Physiol Gastrointest Liver Physiol296(2):G202-10, 2009.Chiu, Brian PhDChiu BC, Blair A. Pesticides, chromosomal aberrations, and non-Hodgkin’slymphoma. J Agromedicine 14(2):250-5, 2009.Colangelo LA, Chiu B, Kopp P, Liu K, Gapstur SM. Serum IGF-I and C-reactiveprotein in healthy black and white young men: The CARDIA male hormonestudy. Growth Horm IGF Res, 2009.Brock KE, Gridley G, Chiu BC, Ershow AG, Lynch CF, Cantor KP. Dietary fatand risk of renal cell carcinoma in the USA: a case-control study. Br J Nutr101(8):1228-38, 2009.Conti, Rena PhD* # Conti RM, Meltzer DO, Ratain MJ. Nonprofit biomedical companies. ClinPharmacol Ther 84(2):194-7, 2008.Conti RM. The societal benefit of nonprofit biotechnology companies. Clin AdvHematol Oncol 6(5):366-7, 386, 2008.Qato DM, Alexander GC, Conti RM, Johnson M, Schumm P, Lindau ST. Use ofprescription and over-the-counter medications and dietary supplements amongolder adults in the United States. JAMA 300(24):2867-78, 2008.Cox, Nancy PhD* # Huang RS, Chen P, Wisel S, Duan S, Zhang W, Cook EH, Das S, Cox NJ,Dolan ME. Population Specific GSTM1 Copy Number Variation. Hum MolGenet 18(2):366-72, 2009.* # Perera MA, Thirumaran RK, Cox NJ, Hanauer S, Das S, Brimer-Cline C,Lamba V, Schuetz EG, Ratain MJ, Di Rienzo A. Prediction of CYP3A4 enzymeactivity using haplotype tag SNPs in African Americans. Pharmacogenomics J9(1):49-60, 2009.* Huo D, Kim HJ, Adebamowo CA, Ogundiran TO, Akang EE, Campbell O,Adenipekun A, Niu Q, Sveen L, Fackenthal JD, Fackenthal DL, Das S, CoxN, Rienzo AD, Olopade OI. Genetic polymorphisms in uridine diphosphoglucuronosyltransferase1A1 and breast cancer risk in Africans. Breast CancerRes Treat 110(2):367-76, 2008.# Duan S, Zhang W, Bleibel WK, Cox NJ, Dolan ME. SNPinProbe_1.0: Adatabase for filtering out probes in the Affymetrix GeneChip(R) Human Exon1.0 ST array potentially affected by SNPs. Bioinformation 2(10):469-70, 2008.# Huang RS, Duan S, Kistner EO, Zhang W, Bleibel WK, Cox NJ, Dolan ME.Identification of genetic variants and gene expression relationships associatedwith pharmacogenes in humans. Pharmacogenet Genomics 18(6):545-9, 2008.# Duan S, Huang RS, Zhang W, Bleibel WK, Roe CA, Clark TA, ChenTX, Schweitzer AC, Blume JE, Cox NJ, Dolan ME. Genetic architecture oftranscript-level variation in humans. Am J Hum Genet 82(5):1101-13, 2008.114UCCRC SCIENTIFIC REPORT 2009
# Zhang W, Duan S, Kistner EO, Bleibel WK, Huang RS, Clark TA, Chen TX,Schweitzer AC, Blume JE, Cox NJ, Dolan ME. Evaluation of genetic variationcontributing to differences in gene expression between populations. Am J HumGenet 82(3):631-40, 2008.Dale, William MD, PhD* Dale W, Basu A, Elstein A, Meltzer D. Predicting utility ratings for jointhealth States from single health States in prostate cancer: empirical testing of 3alternative theories. Med Decis Making 28(1):102-12, 2008.* Basu A, Dale W, Elstein A, Meltzer D. A linear index for predicting jointhealth-states utilities from single health-states utilities. Health Econ 18(4):403-19, 2009.# Bylow K, Dale W, Mustian K, Stadler WM, Rodin M, Hall W, Lachs M,Mohile SG. Falls and physical performance deficits in older patients withprostate cancer undergoing androgen deprivation therapy. Urology 72(2):422-7,2008.# Dale W, Hemmerich J, Bylow K, Mohile S, Mullaney M, Stadler WM. Patientanxiety about prostate cancer independently predicts early initiation ofandrogen deprivation therapy for biochemical cancer recurrence in older men:a prospective cohort study. J Clin Oncol 27(10):1557-63, 2009.Mohile SG, Lachs M, Dale W. Management of prostate cancer in the older man.Semin Oncol 35(6):597-617, 2008.Mohile SG, Mustian K, Bylow K, Hall W, Dale W. Management ofcomplications of androgen deprivation therapy in the older man. Crit RevOncol Hematol 70(3):235-55, 2009.Das, Soma PhD* # Huang RS, Chen P, Wisel S, Duan S, Zhang W, Cook EH, Das S, Cox NJ,Dolan ME. Population Specific GSTM1 Copy Number Variation. Hum MolGenet 18(2):366-72, 2009.* # Perera MA, Thirumaran RK, Cox NJ, Hanauer S, Das S, Brimer-Cline C,Lamba V, Schuetz EG, Ratain MJ, Di Rienzo A. Prediction of CYP3A4 enzymeactivity using haplotype tag SNPs in African Americans. Pharmacogenomics J9(1):49-60, 2009.# Innocenti F, Liu W, Fackenthal D, Ramirez J, Chen P, Ye X, Wu X,Zhang W, Mirkov S, Das S, Cook E Jr, Ratain MJ. Single nucleotidepolymorphism discovery and functional assessment of variation in the UDPglucuronosyltransferase2B7 gene. Pharmacogenet Genomics 18(8):683-97,2008.# Huang RS, Duan S, Kistner EO, Bleibel WK, Delaney SM, Fackenthal DL,Das S, Dolan ME. Genetic variants contributing to daunorubicin-inducedcytotoxicity. Cancer Res 68(9):3161-8, 2008.* Huo D, Kim HJ, Adebamowo CA, Ogundiran TO, Akang EE, Campbell O,Adenipekun A, Niu Q, Sveen L, Fackenthal JD, Fackenthal DL, Das S, CoxN, Rienzo AD, Olopade OI. Genetic polymorphisms in uridine diphosphoglucuronosyltransferase1A1 and breast cancer risk in Africans. Breast CancerRes Treat 110(2):367-76, 2008.# Innocenti F, Kroetz DL, Schuetz E, Dolan ME, Ramirez J, Relling M, ChenP, Das S, Rosner GL, Ratain MJ. Comprehensive Pharmacogenetic Analysis ofIrinotecan Neutropenia and Pharmacokinetics. J Clin Oncol 27(16):2604-14,2009.de Wit, Harriet PhDChilds E, de Wit H. Hormonal, cardiovascular, and subjective responses toacute stress in smokers. Psychopharmacology (Berl) 203(1):1-12, 2009.de Wit H. Impulsivity as a determinant and consequence of drug use: a reviewof underlying processes. Addict Biol 14(1):22-31, 2009.Acheson A, de Wit H. Bupropion improves attention but does not affectimpulsive behavior in healthy young adults. Exp Clin Psychopharmacol16(2):113-23, 2008.Hamidovic A, de Wit H. Sleep deprivation increases cigarette smoking.Pharmacol Biochem Behav 93(3):263-9, 2009.Di Rienzo, Anna PhD* # Perera MA, Thirumaran RK, Cox NJ, Hanauer S, Das S, Brimer-Cline C,Lamba V, Schuetz EG, Ratain MJ, Di Rienzo A. Prediction of CYP3A4 enzymeactivity using haplotype tag SNPs in African Americans. Pharmacogenomics J9(1):49-60, 2009.Hancock AM, Witonsky DB, Gordon AS, Eshel G, Pritchard JK, CoopG, Di Rienzo A. Adaptations to climate in candidate genes for commonmetabolic disorders. PLoS Genet 4(2):e32, 2008.Pemberton TJ, Mehta NU, Witonsky D, Di Rienzo A, Allayee H, ContiDV, Patel PI. Prevalence of common disease-associated variants in AsianIndians. BMC Genet 9:13, 2008.Luca F, Kashyap S, Southard C, Zou M, Witonsky D, Di Rienzo A, ConzenSD. Adaptive Variation Regulates the Expression of the Human SGK1Gene in Response to Stress. PLoS Genet 5(5):e1000489, 2009.Sun C, Southard C, Di Rienzo A. Characterization of a novel splicingvariant in the RAPTOR gene. Mutat Res 662(1-2):88-92, 2009.Sun C, Di Rienzo A. UGT2B7 is not expressed in normal breast. BreastCancer Res Treat 117(1):225-6, 2009.Dignam, James PhD* Bradbury AR, Ibe CN, Dignam JJ, Cummings SA, Verp M, WhiteMA, Artioli G, Dudlicek L, Olopade OI. Uptake and timing of bilateralprophylactic salpingo-oophorectomy among BRCA1 and BRCA2mutation carriers. Genet Med 10(3):161-6, 2008.* Hall MJ, Dignam JJ, Olopade OI. Family history of pancreatic cancer ina high-risk cancer clinic: implications for risk assessment. J Genet Couns17(4):365-72, 2008.Dignam JJ, Dukic V, Anderson SJ, Mamounas EP, Wickerham DL,Wolmark N. Hazard of recurrence and adjuvant treatment effects overtime in lymph node-negative breast cancer. Breast Cancer Res Treat116(3):595-602, 2009.Dignam JJ, Kocherginsky MN. Choice and interpretation of statisticaltests used when competing risks are present. J Clin Oncol 26(24):4027-34, 2008.* # Wei M, Xu J, Dignam J, Nanda R, Sveen L, Fackenthal J, GrushkoTA, Olopade OI. Estrogen receptor alpha, BRCA1, and FANCF promotermethylation occur in distinct subsets of sporadic breast cancers. BreastCancer Res Treat 111(1):113-20, 2008.Dignam JJ, Dukic VM. Comments on: Yin W, Di G, Zhou L, Lu J, LiuG, Wu J, Shen K, Han Q, Shen Z, Shao Z. Time-varying pattern ofrecurrence risk for Chinese breast cancer patients. Breast Cancer ResTreat 114(3):527-35, 2009.Anderson SJ, Wapnir I, Dignam JJ, Fisher B, Mamounas EP, Jeong JH,Geyer CE Jr, Wickerham DL, Costantino JP, Wolmark N. Prognosis AfterIpsilateral Breast Tumor Recurrence and Locoregional Recurrences inPatients Treated by Breast-Conserving Therapy in Five National SurgicalAdjuvant Breast and Bowel Project Protocols of Node-Negative BreastCancer. J Clin Oncol 27(15):2466-73, 2009.Ellis, Nathan PhD* # Ellis NA, Huo D, Yildiz O, Worrillow LJ, Banerjee M, Le Beau MM,Larson RA, Allan JM, Onel K. MDM2 SNP309 and TP53 Arg72Prointeract to alter therapy-related acute myeloid leukemia susceptibility.Blood 112(3):741-9, 2008.Ouyang KJ, Woo LL, Ellis NA. Homologous recombination andmaintenance of genome integrity: cancer and aging through the prism ofhuman RecQ helicases. Mech Ageing Dev 129(7-8):425-40, 2008.Gold B, Kirchhoff T, Stefanov S, Lautenberger J, Viale A, Garber J,Friedman E, Narod S, Olshen AB, Gregersen P, Kosarin K, Olsh A,Bergeron J, Ellis NA, Klein RJ, Clark AG, Norton L, Dean M, Boyd J, OffitK. Genome-wide association study provides evidence for a breast cancerrisk locus at 6q22.33. Proc Natl Acad Sci U S A 105(11):4340-5, 2008.Olshen AB, Gold B, Lohmueller KE, Struewing JP, Satagopan J, StefanovSA, Eskin E, Kirchhoff T, Lautenberger JA, Klein RJ, Friedman E,Norton L, Ellis NA, Viale A, Lee CS, Borgen PI, Clark AG, Offit K, BoydJ. Analysis of genetic variation in Ashkenazi Jews by high density SNPgenotyping. BMC Genet 9:14, 2008.Zhu J, Zhu S, Guzzo CM, Ellis NA, Sung KS, Choi CY, Matunis MJ. SmallUbiquitin-related Modifier (SUMO) Binding Determines SubstrateRecognition and Paralog-selective SUMO Modification. J Biol Chem283(43):29405-15, 2008.Ellis NA, Sander M, Harris CC, Bohr VA. Bloom’s syndrome workshopfocuses on the functional specificities of RecQ helicases. Mech AgeingDev 129(11):681-91, 2008.Cancer Risk& PreventionUCCRC SCIENTIFIC REPORT 2009115
Gehlert, Sarah PhD* Gehlert S, Sohmer D, Sacks T, Mininger C, McClintock M, Olopade O.Targeting health disparities: a model linking upstream determinants todownstream interventions. Health Aff (Millwood) 27(2):339-49, 2008.Salant T, Gehlert S. Collective memory, candidacy, and victimisation:community epidemiologies of breast cancer risk. Sociol Health Illn 30(4):599-615, 2008.Warnecke RB, Oh A, Breen N, Gehlert S, Paskett E, Tucker KL, Lurie N,Rebbeck T, Goodwin J, Flack J, Srinivasan S, Kerner J, Heurtin-Roberts S,Abeles R, Tyson FL, Patmios G, Hiatt RA. Approaching health disparitiesfrom a population perspective: the National Institutes of Health Centers forPopulation Health and Health Disparities. Am J Public Health 98(9):1608-15,2008.Holmes JH, Lehman A, Hade E, Ferketich AK, Gehlert S, Rauscher GH,Abrams J, Bird CE. Challenges for multilevel health disparities research in atransdisciplinary environment. Am J Prev Med 35(2 Suppl):S182-92, 2008.Paskett ED, Reeves KW, McLaughlin JM, Katz ML, McAlearney AS, RuffinMT, Halbert CH, Merete C, Davis F, Gehlert S. Recruitment of minority andunderserved populations in the United States: the Centers for PopulationHealth and Health Disparities experience. Contemp Clin Trials 29(6):847-61,2008.Gehlert S, Mininger C, Sohmer D, Berg K. (Not so) gently down the stream:choosing targets to ameliorate health disparities. Health Soc Work 33(3):163-7,2008.* Masi CM, Gehlert S. Perceptions of breast cancer treatment among African-American women and men: implications for interventions. J Gen Intern Med24(3):408-14, 2009.Grdina, David PhDFu P, Birukova AA, Xing J, Sammani S, Murley JS, Garcia JG, Grdina DJ,Birukov KG. Amifostine reduces lung vascular permeability via suppression ofinflammatory signaling. Eur Respir J 33(3):612-24, 2009.Dziegielewski J, Baulch JE, Goetz W, Coleman MC, Spitz DR, Murley JS,Grdina DJ, Morgan WF. WR-1065, the active metabolite of amifostine,mitigates radiation-induced delayed genomic instability. Free Radic Biol Med45(12):1674-81, 2008.Paunesku D, Paunesku T, Wahl A, Kataoka Y, Murley J, Grdina DJ, WoloschakGE. Incidence of tissue toxicities in gamma ray and fission neutron-exposedmice treated with Amifostine. Int J Radiat Biol 84(8):623-34, 2008.Murley JS, Nantajit D, Baker KL, Kataoka Y, Li JJ, Grdina DJ. Maintenance ofmanganese superoxide dismutase (SOD2)-mediated delayed radioprotectioninduced by repeated administration of the free thiol form of amifostine. RadiatRes 169(5):495-505, 2008.Ahmed KM, Nantajit D, Fan M, Murley JS, Grdina DJ, Li JJ. Coactivationof ATM/ERK/NF-kappaB in the low-dose radiation-induced radioadaptiveresponse in human skin keratinocytes. Free Radic Biol Med 46(11):1543-50,2009.Grdina DJ, Murley JS, Kataoka Y, Baker KL, Kunnavakkam R, Coleman MC,Spitz DR. Amifostine induces antioxidant enzymatic activities in normaltissues and a transplantable tumor that can affect radiation response. Int JRadiat Oncol Biol Phys 73(3):886-96, 2009.Green, William PhDDrisdel RC, Sharp D, Henderson T, Hales TG, Green WN. High affinity bindingof epibatidine to serotonin type 3 receptors. J Biol Chem 283(15):9659-65, 2008.Liu Y, Padgett D, Takahashi M, Li H, Sayeed A, Teichert RW, Olivera BM,McArdle JJ, Green WN, Lin W. Essential roles of the acetylcholine receptorgamma-subunit in neuromuscular synaptic patterning. Development135(11):1957-67, 2008.Walsh H, Govind AP, Mastro R, Hoda JC, Bertrand D, Vallejo Y, Green WN.Up-regulation of nicotinic receptors by nicotine varies with receptor subtype. JBiol Chem 283(10):6022-32, 2008.Waites CL, Specht CG, Hartel K, Leal-Ortiz S, Genoux D, Li D, Drisdel RC,Jeyifous O, Cheyne JE, Green WN, Montgomery JM, Garner CC. SynapticSAP97 isoforms regulate AMPA receptor dynamics and access to presynapticglutamate. J Neurosci 29(14):4332-45, 2009.Kang R, Wan J, Arstikaitis P, Takahashi H, Huang K, Bailey AO, Thompson JX,Roth AF, Drisdel RC, Mastro R, Green WN, Yates JR 3rd, Davis NG, El-HusseiniA. Neural palmitoyl-proteomics reveals dynamic synaptic palmitoylation.Nature 456(7224):904-9, 2008.Cheng H, Vetrivel KS, Drisdel RC, Meckler X, Gong P, Leem JY, Li T, Carter M,Chen Y, Nguyen P, Iwatsubo T, Tomita T, Wong PC, Green WN, Kounnas MZ,Thinakaran G. S-palmitoylation of gamma-secretase subunits nicastrin andAPH-1. J Biol Chem 284(3):1373-84, 2009.Henderson, Tara MD, MPHNathan PC, Ford JS, Henderson TO, Hudson MM, Emmons KM, CasillasJN, Lown EA, Ness KK, Oeffinger KC. Health behaviors, medical care, andinterventions to promote healthy living in the Childhood Cancer SurvivorStudy cohort. J Clin Oncol 27(14):2363-73, 2009.Oeffinger KC, Ford JS, Moskowitz CS, Diller LR, Hudson MM, Chou JF, SmithSM, Mertens AC, Henderson TO, Friedman DL, Leisenring WM, Robison LL.Breast cancer surveillance practices among women previously treated withchest radiation for a childhood cancer. JAMA 301(4):404-14, 2009.Huo, Dezheng MD, PhD* # Ellis NA, Huo D, Yildiz O, Worrillow LJ, Banerjee M, Le Beau MM, LarsonRA, Allan JM, Onel K. MDM2 SNP309 and TP53 Arg72Pro interact to altertherapy-related acute myeloid leukemia susceptibility. Blood 112(3):741-9, 2008.* Garner CP, Ding YC, John EM, Ingles SA, Olopade OI, Huo D, AdebamowoC, Ogundiran T, Neuhausen SL. Genetic variation in IGFBP2 and IGFBP5 isassociated with breast cancer in populations of African descent. Hum Genet123(3):247-55, 2008.* Calderwood AH, Huo D, Rubin DT. Association between colorectal cancerand urologic cancers. Arch Intern Med 168(9):1003-9, 2008.# Odenike OM, Alkan S, Sher D, Godwin JE, Huo D, Brandt SJ, Green M, Xie J,Zhang Y, Vesole DH, Stiff P, Wright J, Larson RA, Stock W. Histone deacetylaseinhibitor romidepsin has differential activity in core binding factor acutemyeloid leukemia. Clin Cancer Res 14(21):7095-101, 2008.# Cohen EE, Baru J, Huo D, Haraf DJ, Crowley M, Witt ME, Blair EA,Weichselbaum RR, Rosen F, Vokes EE, Stenson K. Efficacy and safety of treatingT4 oral cavity tumors with primary chemoradiotherapy. Head Neck 31(8):1013-21, 2009.* Huo D, Senie RT, Daly M, Buys SS, Cummings S, Ogutha J, Hope K, OlopadeOI. Prediction of BRCA Mutations Using the BRCAPRO Model in Clinic-BasedAfrican American, Hispanic, and Other Minority Families in the United States.J Clin Oncol 27(8):1184-90, 2009.* # Olopade OI, Grushko TA, Nanda R, Huo D. Advances in breast cancer:pathways to personalized medicine. Clin Cancer Res 14(24):7988-99, 2008.Kim, Karen MDVela MB, Kim KE, Tang H, Chin MH. Innovative health care disparitiescurriculum for incoming medical students. J Gen Intern Med 23(7):1028-32,2008.King, Andrea PhDKing A, Epstein A, Conrad M, McNamara P, Cao D. Sex differences in therelationship between alcohol-associated smoking urge and behavior: a pilotstudy. Am J Addict 17(5):347-53, 2008.* King A, Sanchez-Johnsen L, Van Orman S, Cao D, Matthews A. A pilotcommunity-based intensive smoking cessation intervention in AfricanAmericans: feasibility, acceptability and early outcome indicators. J Natl MedAssoc 100(2):208-17, 2008.King A, Cao D, Vanier C, Wilcox T. Naltrexone decreases heavy drinking ratesin smoking cessation treatment: an exploratory study. Alcohol Clin Exp Res33(6):1044-50, 2009.Kittles, Rick PhDAldrich MC, Selvin S, Hansen HM, Barcellos LF, Wrensch MR, Sison JD,Quesenberry CP, Kittles RA, Silva G, Buffler PA, Seldin MF, Wiencke JK.Comparison of Statistical Methods for Estimating Genetic Admixture ina Lung Cancer Study of African Americans and Latinos. Am J Epidemiol168(9):1035-46, 2008.Robbins CM, Hernandez W, Ahaghotu C, Bennett J, Hoke G, Mason T,Pettaway CA, Vijayakumar S, Weinrich S, Furbert-Harris P, Dunston G, PowellIJ, Carpten JD, Kittles RA. Association of HPC2/ELAC2 and RNASEL nonsynonymousvariants with prostate cancer risk in African American familialand sporadic cases. Prostate 68(16):1790-7, 2008.116UCCRC SCIENTIFIC REPORT 2009
Chang JS, Wrensch MR, Hansen HM, Sison JD, Aldrich MC, Quesenberry CPJr, Seldin MF, Kelsey KT, Kittles RA, Silva G, Wiencke JK. Nucleotide excisionrepair genes and risk of lung cancer among San Francisco Bay Area Latinos andAfrican Americans. Int J Cancer 123(9):2095-104, 2008.Caulfield T, Fullerton SM, Ali-Khan SE, Arbour L, Burchard EG, CooperRS, Hardy BJ, Harry S, Hyde-Lay R, Kahn J, Kittles R, Koenig BA, Lee SS,Malinowski M, Ravitsky V, Sankar P, Scherer SW, Seguin B, Shickle D, Suarez-Kurtz G, Daar AS. Race and ancestry in biomedical research: exploring thechallenges. Genome Med 1(1):8, 2009.King G, Yerger VB, Whembolua GL, Bendel RB, Kittles R, Moolchan ET. Linkbetween facultative melanin and tobacco use among African Americans.Pharmacol Biochem Behav 92(4):589-96, 2009.Giri VN, Egleston B, Ruth K, Uzzo RG, Chen DY, Buyyounouski M, Raysor S,Hooker S, Torres JB, Ramike T, Mastalski K, Kim TY, Kittles R. Race, geneticWest African ancestry, and prostate cancer prediction by prostate-specificantigen in prospectively screened high-risk men. Cancer Prev Res (Phila Pa)2(3):244-50, 2009.Lauderdale, Diane PhDLauderdale DS, Huo D. Cancer death rates for older Asian-Americans:classification by race versus ethnicity. Cancer Causes Control 19(2):135-46,2008.Kandula NR, Wen M, Jacobs EA, Lauderdale DS. Association betweenneighborhood context and smoking prevalence among Asian Americans. Am JPublic Health 99(5):885-92, 2009.Li, Yan Chun PhD* Kong J, Zhang Z, Musch MW, Ning G, Sun J, Hart J, Bissonnette M, LiYC. Novel role of the vitamin D receptor in maintaining the integrity ofthe intestinal mucosal barrier. Am J Physiol Gastrointest Liver Physiol294(1):G208-16, 2008.Wang Q, Li YC, Wang J, Kong J, Qi Y, Quigg RJ, Li X. miR-17-92 clusteraccelerates adipocyte differentiation by negatively regulating tumor-suppressorRb2/p130. Proc Natl Acad Sci U S A 105(8):2889-94, 2008.Musch MW, Li YC, Chang EB. Angiotensin II directly regulates intestinalepithelial NHE3 in Caco2BBE cells. BMC Physiol 9:5, 2009.Lindau, Stacy MDCurlin FA, Dinner SN, Lindau ST. Of more than one mind: obstetriciangynecologists’approaches to morally controversial decisions in sexual andreproductive healthcare. J Clin Ethics 19(1):11-21, discussion 22-3, 2008.Lindau ST, Tetteh AS, Kasza K, Gilliam M. What schools teach our patientsabout sex: content, quality, and influences on sex education. Obstet Gynecol111(2 Pt 1):256-66, 2008.* Lindau ST, Hoffmann JN, Lundeen K, Jaszczak A, McClintock MK, JordanJA. Vaginal Self-Swab Specimen Collection in a Home-Based Survey of OlderWomen: Methods and Applications. J Gerontol B Psychol Sci Soc Sci, 2009.Lindau ST, Drum ML, Gaumer E, Surawska H, Jordan JA. Prevalence of highriskhuman papillomavirus among older women. Obstet Gynecol 112(5):979-89,2008.Masi, Christopher MD, PhD* Masi CM, Gehlert S. Perceptions of breast cancer treatment among African-American women and men: implications for interventions. J Gen Intern Med24(3):408-14, 2009.McClintock, Martha PhD* Gehlert S, Sohmer D, Sacks T, Mininger C, McClintock M, Olopade O.Targeting health disparities: a model linking upstream determinants todownstream interventions. Health Aff (Millwood) 27(2):339-49, 2008.Yee JR, Cavigelli SA, Delgado B, McClintock MK. Reciprocal Affiliation AmongAdolescent Rats During a Mild Group Stressor Predicts Mammary Tumors andLifespan. Psychosom Med 70(9):1050-9, 2008.Hermes GL, McClintock MK. Isolation and the timing of mammary glanddevelopment, gonadarche, and ovarian senescence: implications for mammarytumor burden. Dev Psychobiol 50(4):353-60, 2008.* Lindau ST, Hoffmann JN, Lundeen K, Jaszczak A, McClintock MK,Jordan JA. Vaginal Self-Swab Specimen Collection in a Home-BasedSurvey of Older Women: Methods and Applications. J Gerontol B PsycholSci Soc Sci, 2009.Pyter LM, Pineros V, Galang JA, McClintock MK, Prendergast BJ.Peripheral tumors induce depressive-like behaviors and cytokineproduction and alter hypothalamic-pituitary-adrenal axis regulation.Proc Natl Acad Sci U S A 106(22):9069-74, 2009.McClintock MK. Human aromas, pheromones and vasanas: effects onfertility, sexuality and emotions. Aroma Research 10: 72-77, 2009.Gehlert S, Murray A, Sohmer D, McClintock MK, Conzen SD, andOlopade F. The importance of transdisciplinary collaborations forunderstanding and resolving health disparities. Journal of Health andSocial Policy, 2009 (in press).Hermes GL, Delgado B, Tsakalis M, Tretiakova M, Cavigelli SA, Krausz T,Conzen SD, and McClintock MK. Social Isolation dysregulates endocrineand behavioral stress responses while increasing the malignant burdenof spontaneous mammary tumors. Proc Natl Acad Sci U S A, 2009 (inpress).McClintock MK, Gehlert S, Conzen SD, Olopade F, and Krausz T.Overcoming Health Disparities: The Power of a TransdisciplinaryApproach to Environmental Regulation of Gene Expression. RoyalSociety of Canada, 2009 (in press).McGeHee, Daniel PhDBritt JP, McGehee DS. Presynaptic opioid and nicotinic receptormodulation of dopamine overflow in the nucleus accumbens. J Neurosci28(7):1672-81, 2008.Campioni M, Xu M, McGehee DS. Stress-Induced Changes in NucleusAccumbens Glutamate Synaptic Plasticity. J Neurophysiol 101(6):3192-8,2009.Meltzer, David MD, PhDMeltzer D. Response to “Future costs and the future of cost-effectivenessanalysis”. J Health Econ 27(4):822-5, 2008.* # Conti RM, Meltzer DO, Ratain MJ. Nonprofit biomedical companies.Clin Pharmacol Ther 84(2):194-7, 2008.Abbo ED, Sobotka S, Meltzer DO. Patient preferences in instructionaladvance directives. J Palliat Med 11(4):555-62, 2008.Braithwaite RS, Meltzer DO, King JT Jr, Leslie D, Roberts MS. What doesthe value of modern medicine say about the $50,000 per quality-adjustedlife-year decision rule?. Med Care 46(4):349-56, 2008.Howard DH, Meltzer D, Kollman C, Maiers M, Logan B, Gragert L,Setterholm M, Horowitz MM. Use of cost-effectiveness analysis todetermine inventory size for a national cord blood bank. Med DecisMaking 28(2):243-53, 2008.* Yin W, Basu A, Zhang JX, Rabbani A, Meltzer DO, Alexander GC. Theeffect of the Medicare Part D prescription benefit on drug utilization andexpenditures. Ann Intern Med 148(3):169-77, 2008.* Dale W, Basu A, Elstein A, Meltzer D. Predicting utility ratings forjoint health States from single health States in prostate cancer: empiricaltesting of 3 alternative theories. Med Decis Making 28(1):102-12, 2008.* Basu A, Dale W, Elstein A, Meltzer D. A linear index for predictingjoint health-states utilities from single health-states utilities. Health Econ18(4):403-19, 2009.Walton SM, Schumock GT, Lee KV, Alexander GC, Meltzer D, StaffordRS. Prioritizing Future Research on Off-Label Prescribing: Results of aQuantitative Evaluation. Pharmacotherapy 28(12):1443-1452, 2008.Mendonca, Eneida MD, PhD# Sam LT, Mendonca EA, Li J, Blake J, Friedman C, Lussier YA.PhenoGO: an integrated resource for the multiscale mining of clinicaland biological data. BMC Bioinformatics 10 Suppl 2:S8, 2009.Cancer Risk& PreventionUCCRC SCIENTIFIC REPORT 2009117
Olopade, Olufunmilayo MBBS* Bradbury AR, Ibe CN, Dignam JJ, Cummings SA, Verp M, White MA,Artioli G, Dudlicek L, Olopade OI. Uptake and timing of bilateral prophylacticsalpingo-oophorectomy among BRCA1 and BRCA2 mutation carriers. GenetMed 10(3):161-6, 2008.* Huo D, Kim HJ, Adebamowo CA, Ogundiran TO, Akang EE, Campbell O,Adenipekun A, Niu Q, Sveen L, Fackenthal JD, Fackenthal DL, Das S, CoxN, Rienzo AD, Olopade OI. Genetic polymorphisms in uridine diphosphoglucuronosyltransferase1A1 and breast cancer risk in Africans. Breast CancerRes Treat 110(2):367-76, 2008.* Huo D, Adebamowo CA, Ogundiran TO, Akang EE, Campbell O,Adenipekun A, Cummings S, Fackenthal J, Ademuyiwa F, Ahsan H, OlopadeOI. Parity and breastfeeding are protective against breast cancer in Nigerianwomen. Br J Cancer 98(5):992-6, 2008.* Garner CP, Ding YC, John EM, Ingles SA, Olopade OI, Huo D, AdebamowoC, Ogundiran T, Neuhausen SL. Genetic variation in IGFBP2 and IGFBP5 isassociated with breast cancer in populations of African descent. Hum Genet123(3):247-55, 2008.* Huo D, Senie RT, Daly M, Buys SS, Cummings S, Ogutha J, Hope K, OlopadeOI. Prediction of BRCA Mutations Using the BRCAPRO Model in Clinic-BasedAfrican American, Hispanic, and Other Minority Families in the United States.J Clin Oncol 27(8):1184-90, 2009.* # Olopade OI, Grushko TA, Nanda R, Huo D. Advances in breast cancer:pathways to personalized medicine. Clin Cancer Res 14(24):7988-99, 2008.Xu J, Huo D, Chen Y, Nwachukwu C, Collins C, Rowell J, Slamon DJ, OlopadeOI. CpG island methylation affects accessibility of the proximal BRCA1promoter to transcription factors. Breast Cancer Res Treat, 2009.Polite, Blase MD# Polite BN, Cirrincione C, Fleming GF, Berry DA, Seidman A, Muss H, NortonL, Shapiro C, Bakri K, Marcom K, Lake D, Schwartz JH, Hudis C, Winer EP.Racial differences in clinical outcomes from metastatic breast cancer: a pooledanalysis of CALGB 9342 and 9840--Cancer and Leukemia Group B. J ClinOncol 26(16):2659-65, 2008.Sanchez-Johnsen, Lisa PhD* King A, Sanchez-Johnsen L, Van Orman S, Cao D, Matthews A. A pilotcommunity-based intensive smoking cessation intervention in AfricanAmericans: feasibility, acceptability and early outcome indicators. J Natl MedAssoc 100(2):208-17, 2008.Sanchez-Johnsen LA, Hogan K, Wilkens LR, Fitzgibbon ML. Correlates ofproblematic eating behaviors in less acculturated Latinas. Eat Behav 9(2):181-9,2008.Verp, Marion MD* Bradbury AR, Ibe CN, Dignam JJ, Cummings SA, Verp M, White MA,Artioli G, Dudlicek L, Olopade OI. Uptake and timing of bilateral prophylacticsalpingo-oophorectomy among BRCA1 and BRCA2 mutation carriers. GenetMed 10(3):161-6, 2008.Vezina, Paul PhDVezina P, Leyton M. Conditioned cues and the expression of sensitization inanimals and humans. Neuropharmacology 56: 160-168, 2009Waxman, Irving MD# Konda VJ, Ross AS, Ferguson MK, Hart JA, Lin S, Naylor K, Noffsinger A,Posner MC, Dye C, Cislo B, Stearns L, Waxman I. Is the risk of concomitantinvasive esophageal cancer in high-grade dysplasia in Barrett’s esophagusoverestimated?. Clin Gastroenterol Hepatol 6(2):159-64, 2008.de Tejada AH, Chennat J, Miller F, Stricker T, Matthews J, Waxman I.Endoscopic and EUS features of groove pancreatitis masquerading as apancreatic neoplasm. Gastrointest Endosc 68(4):796-8, 2008.Ross A, Mehdizadeh S, Tokar J, Leighton JA, Kamal A, Chen A, Schembre D,Chen G, Binmoeller K, Kozarek R, Waxman I, Dye C, Gerson L, Harrison ME,Haluszka O, Lo S, Semrad C. Double balloon enteroscopy detects small bowelmass lesions missed by capsule endoscopy. Dig Dis Sci 53(8):2140-3, 2008.Rubin, David MD# Nathanson JW, Yadron NE, Farnan J, Kinnear S, Hart J, Rubin DT. p53mutations are associated with dysplasia and progression of dysplasia in patientswith Crohn’s disease. Dig Dis Sci 53(2):474-80, 2008.Rubin DT. An Updated Approach to Dysplasia in IBD. J Gastrointest Surg12(12):2153-6, 2008.Nathanson JW, Zisman TL, Julian C, McCaffrey S, Rubin DT. Identificationof patients at increased risk for colorectal cancer in an open access endoscopycenter. J Clin Gastroenterol 42(9):1025-31, 2008.# Weber CR, Nalle SC, Tretiakova M, Rubin DT, Turner JR. Claudin-1 andclaudin-2 expression is elevated in inflammatory bowel disease and maycontribute to early neoplastic transformation. Lab Invest 88(10):1110-20, 2008.* Calderwood AH, Huo D, Rubin DT. Association between colorectal cancerand urologic cancers. Arch Intern Med 168(9):1003-9, 2008.Zisman TL, Rubin DT. Colorectal cancer and dysplasia in inflammatory boweldisease. World J Gastroenterol 14(17):2662-9, 2008.Rubin DT, Cruz-Correa MR, Gasche C, Jass JR, Lichtenstein GR,Montgomery EA, Riddell RH, Rutter MD, Ullman TA, Velayos FS, ItzkowitzS. Colorectal cancer prevention in inflammatory bowel disease and the roleof 5-aminosalicylic acid: a clinical review and update. Inflamm Bowel Dis14(2):265-74, 2008.118UCCRC SCIENTIFIC REPORT 2009
Selected Major Grants and AwardsThe Cancer Risk and Prevention Program has a funding base of $17,841,935 in annual total costs (current as of July 2009). This sumincludes $4,221,965 in NCI funding and $8,082,978 in other NIH funding. Due to space constraints, only new awards presented sinceJanuary 1, 2008 with funding of $100,000 or more in annual total costs are listed here.Investigator Title Start DateKing, AndreaBasu, AnirbanOlopade,OlufunmilayoChang, EugeneGreen, WilliamOlopade,OlufunmilayoOlopade,OlufunmilayoOlopade,OlufunmilayoPolite, BlaseChang, EugeneMendonca, EneidaChang, EugeneMeltzer, DavidSanchez-Johnsen,LisaHenderson, TaraShah, LisaDale, WilliamLi, Yan ChunKim, KarenPolite, BlaseAlcohol Stimulation and Sedation inBinge DrinkersA Comprehensive Probabilistic-Micro-Simulation Model to Assess Cost-EffectivenessDr. Ralph and Marian Falk Center forClinical Cancer GeneticsCytoprotective Role of Heat ShockProteins in IBDThe Neuronal Alpha-BungarotoxinBinding SiteDeveloping an Infrastructure toConduct Clinical Breast Cancer Trialsin Resource Poor Nations such asNigeriaTargeting the Fanconi Anemia-BRCA1Pathway in Breast CancerNational Women's Cancer ResearchAlliance (NWCRA)A Phase III Randomized DoubleBlind STudy of Sunitinib Vs Placeboin Patients w/Progressive Advanced/Metastatic Well DifferentiatedPancreatic Islet Cell TumorsTechnologies for the <strong>Discover</strong>y ofNovel Human Colonic Mucosal-Associated MicrobesAnswering Information Needs inWorkflowShort Term Training: HealthProfessional StudentsResearch and Mentoring in Cost-Effectiveness and Hospital-Based ElderCareEndDateAnnualTotal CostClassFunding Agency1/1/2009 12/31/2013 $671,587 R01 National Institutes of Health9/23/2008 5/31/2013 $568,535 R01National Institute of MentalHealth1/1/2008 12/31/2010 $500,000 N/A Falk Foundation4/1/2008 1/31/2013 $310,838 R378/1/2008 7/31/2009 $307,646 R5610/1/2008 9/30/2009 $250,000 N/A10/1/2008 9/30/2009 $250,000 N/A5/1/2008 4/30/2009 $250,000 N/A9/8/2008 9/7/2010 $193,465 N/A Pfizer, Inc.9/26/2008 7/31/2010 $187,640 R21Nat. Inst. of Diabetes &Digestive & Kidney DiseasesNational Inst. ofNeurological Disorders andStrokeBreast Cancer ResearchFoundationBreast Cancer ResearchFoundationThe Entertainment IndustryFoundationNational Center For HumanGenome Research4/1/2008 3/31/2010 $182,739 R01 National Institutes of Health5/1/2008 4/30/2013 $181,129 T35 National Institutes of Health6/1/2008 $174,352 K24 National Institute on AgingLatinos, Culture, and Obesity 7/21/2008 6/30/2010 $173,250 R21 National Cancer InstituteHealth Beliefs and Behavior:Cohort Studies in Pediatric CancerSurvivorshipA Missed Opportunity: ExploringBarriers to Quit in HospitalizedSmokersDecision Making in Older MenStarting Androgen Ablation forProstate CancerCardiovascular Effects ofDoxercalciferolVitamin D Intervention in PolypRecurrence in African Americans - APilot StudyUnderstanding Racial Disparities inChemotherapy Receipt9/17/2008 8/31/2012 $129,600 K07 National Cancer Institute8/15/2008 8/14/2010 $125,000 N/A9/1/2008 8/31/2010 $123,484 N/AAmerican Cancer Society,IllinoisAmerican Cancer Society,Illinois2/3/2009 2/2/2010 $121,800 N/A Genzyme Corporation7/1/2008 6/30/2009 $100,000 N/A7/1/2008 6/30/2010 $100,000 N/AAmerican Cancer Society,IllinoisAmerican Society of ClinicalOncologyCancer Risk& PreventionUCCRC SCIENTIFIC REPORT 2009119
Clinical Trials ActivityDr. Alessandro Fichera with a patient
The UCCRC has sustained a vigorous clinical researchprogram for many years, and has long been recognizedfor its strength in basic and clinical research.Clinical Trials ActivityMost recently, these activities are been expandedto population research including epidemiologyand prevention trials. The tight and dynamiclinkages connecting our basic scientists withour enhanced team of translational and clinicalresearchers have led to major contributions toearly-phase clinical trials and drug development.The integration of population researchersis taking these trials to the population andcommunity level.and translational endpoints, sequencing ofmultidisciplinary treatment, transplantation,organ preservation, and treatment intensificationas strategies to increase cure rates and response.Within the past few years, there has been aremarkable increase in tangible benchmarks, suchas multi-investigator, multi-disciplinary grants, aswell as investigator-initiated clinical trials.UCCRC therapeutic clinical trials areconceived and conducted by multidisciplinaryteams, each comprised of a group of clinicalinvestigators representing Medical Oncology,Radiation Oncology, Pathology, Biostatistics,and appropriate surgical specialties. All of ourresearch programs conduct clinical research.These clinical efforts focus on studies of newdrugs (cytotoxic or cytostatic) with clinicalClincal TrialsActivityUCCRC SCIENTIFIC REPORT 2009121
The clinical trials activity of the UCCRC is managed through the Cancer Clinical Trials Office (CCTO). The CCTOprovides oversight and quality control for these studies through the provision of policies and procedures, by centralizingregulatory and reporting functions, supervision of staff, auditing, and tracking of these activities with a centralized database.The overall objective of the CCTO is to provide the infrastructure to support successful cancer clinical research acrossdepartments within the University, as well as through national cooperative groups. CCTO services and areas of operationcan be divided into four distinct but somewhat overlapping areas: (1) regulatory affairs; (2) affiliate institution coordinationand oversight; (3) protocol tracking and management; and (4) quality control.Our drug development program is unique in the Chicago metropolitan area, and among the largest in the United States.Patients travel from throughout the world to be evaluated for enrollment in Phase I and Phase II trials of novel anticanceragents. Annually, between 12001400 patients are enrolled on clinical trials, with 800-1000 entered on therapeutic trials.Clinical trials span the gamut from preclinical development to investigator-initiated Phase I clinical trials to Phase II trialsin the regional Phase II network to Phase III studies within CALGB. Many trials also incorporate correlative laboratorystudies which include pharmacokinetic studies, genotyping studies, population pharmacology and pharmacogenetics, andmeasurement of biomarker endpoints. In 2008, clinical trials enrollment included 1005 patients to 200 therapeutic protocols;548 patients were treated on 101 Phase II protocols, and 180 patients were treated on 26 Phase I studies.In 2008, regulatory managers in the CCTO opened 98 new protocols and were responsible for ongoing regulatory activitiesof an additional 351studies already open to enrollment, as well as the regulatory activities (e.g., IRB continuing renewals,amendments, safety reports) for 357 studies closed to enrollment, but not terminated with the IRB. These trials representover 50 principal investigators from multiple departments (Medicine, Radiology, Radiation and Cellular Oncology, Surgery,Pediatrics, and Obstetrics and Gynecology122UCCRC SCIENTIFIC REPORT 2009
Number of therapeutic protocols (N=344*) and patient accrual (N=1005 by sponsor in 2008)Study SponsorTotal No. TrialsNo. InvestigatorInitiatedNo. of PtsEnrolledInstitutional 36 (11%) 27 307 (31%)NCI 45 (13%) 19 229 (22%)Cooperative Group 122 (35%) 2 139 (14%)Industry 141 (41%) 6 330 (33%)Total 344 54 (16%) 1005*Note that of the 344 trials open to accrual in 2008, approximately 16% were investigator-initiated. In addition, more than 50% of our accrual totherapeutic protocols is to NCI and institutional studies that are largely investigator-initiated.The UCCRC and CCTO have been instrumental in the success of several major grants and contracts including the Phase IGrant: Phase I Clinical Trials of Anticancer Agents, the Phase II Contract: Novel Therapeutics, the CALGB grant, and the BreastCancer SPORE, which was awarded in the fall of 2006. The most recent Phase II contract (2006) added the Medical Universityof South Carolina as an academic partner; approximately 200 patients are enrolled on Phase II contract studies annually. TheCCTO continues to support the clinical trials activity associated with these programs.Clincal TrialsActivityUCCRC SCIENTIFIC REPORT 2009123
Shared ResourcesDr. Vytas Bindokas imaging tumor cell nuclear morphology, using thelive-cell optimized Olympus DSU spinning disk confocal system with ahigh-sensitivity EM-CCD camera, in the UCCRC’s Integrated Microscopy Facility.
Multiple levels of scientific and administrative oversightensure the continued delivery of optimal state-of-the-arttechnologies to meet the needs of the research community.OverviewThe University of Chicago Biological SciencesDivision (BSD) provides shared technologiesthrough 23 Core Facilities, which aim tosupport research and serve as educationalresources for the University of Chicago. TheCore Facilities serve as centralized centersof expertise and provide UCCRC researchersaccess to a comprehensive set of technicalresources, which offer advanced services tosupport vital translational research, and facilitatethe interaction of researchers and cliniciansfrom different disciplines. Multiple levels ofscientific and administrative oversight ensurethe continued delivery of optimal state-ofthe-arttechnologies to meet the needs of theresearch community. Thirteen of these sharedfacilities are supported by the UCCRC. Thesefacilities are integrated with the other CoreFacilities and include the Biostatistics CoreFacility, Cancer Clinical Trials Office, FrankW. Fitch Monoclonal Antibody Facility, FlowCytometry Facility, Genomics Core Facility,Human Immunologic Monitoring Core, HumanTissue Resource Center, Integrated MicroscopyFacility, Immunohistochemistry Facility,Magnetic Resonance Imaging and SpectroscopyFacility, Pharmacology Core Facility, ScientificImage Reconstruction and Analysis Facility, andTransgenic Mouse and Embryonic Stem CellFacility.SharedResourcesUCCRC SCIENTIFIC REPORT 2009125
Biostatistics Core FacilityScientific Director: Ronald Thisted, PhDTechnical Director: Theodore Karrison, PhDWebsite: http://health.bsd.uchicago.edu/Page.aspx?Page=BiostatLabThe Biostatistics Core Facility provides collaborative statistical support to investigators for the design, conduct, and analysisof clinical trials, observational and population-based studies, and basic science research projects.The services provided include:••••••••••••••Collaboration with investigators in the formulation of study design and dataanalysis plans, including sample-size and power calculations;Assistance in the development, execution, and statistical analyses of investigator-initiatedphase I, phase II, and phase III clinical trials and correlative/translational studies;Collaboration in the design and analysis of prospective and retrospective observationalstudies, basic science research projects, and animal experiments;Collaboration with investigators on the preparation of manuscripts for publication;Assistance in new grant submissions, including U01, P01, R01, R21, and SPORE grants;Participation in the review of clinical protocols through membership on the Clinical Trials Review Committee; andParticipation in the teaching and training of investigators in fundamentalstatistical concepts, study design, and clinical trials methodology.Cancer Clinical Trials OfficeScientific Director: Marcy A. List, PhDTechnical Director: Connie Skosey, RN, CCRPWebsite: http://uccrc.uchicago.edu/researchers/core_ccto.htmlThe Cancer Clinical Trials Office (CCTO) provides oversight and quality control for clinical trials activity at the UCCRCby centralizing regulatory and reporting functions. The overall objective of the CCTO is to provide the infrastructure tosupport successful clinical research across departments.The services provided are categorized under the following key functions:•• Regulatory Affairs: Provide centralized regulatory management for the conduct of all cancer clinical trials at theUniversity of Chicago regardless of sponsor, department, or type of study, including the completion of requiredforms and submission to the Clinical Trials Review Committee (CTRC), the Institutional Review Board (IRB),and other required committees (e.g., Institutional Biosafety Committee); annual renewals to the IRB and theScientific and Accrual Monitoring Committee of the UCCRC; and investigational new drug submissions.••Affiliate Institution Coordination and Oversight: Provide infrastructure for the participation ofaffiliate institutions enrolling patients on trials at the UCCRC (including CALGB affiliate institutions,Phase II NCI contract affiliate institutions, and additional ad hoc affiliates participating in selectedstudies); coordinate all study-related communications; serve as the point of patient registrationfor some programs; and review operations to ensure compliance with federal regulations.•• Protocol Tracking, Management: Provide a centralized location and database (Velos eResearch) fortracking protocol-specific data (including study teams, protocol status, and patient registration);provide web-based direct access (e.g., in clinics) to current consent forms, protocols, and investigationalbrochures; and report generation with respect to both clinical data and study status information.•• Quality Control: Provide training of regulatory managers across departments; support continuing education;train nurses, data managers, faculty and fellows in the use of Velos eResearch; oversee designated data andsafety monitoring activities (e.g., severe adverse event tracking, coordination of High-Risk Protocol ConferenceHRPC); coordinate the audit program; and develop and implement Standard Operating Procedures.126UCCRC SCIENTIFIC REPORT 2009
Frank W. Fitch Monoclonal Antibody FacilityScientific Director: Anne Sperling, PhDTechnical Director: Carol McShanWebsite: http://fitchantibodies.bsd.uchicago.eduThe Frank W. Fitch Monoclonal Antibody Facility provides a wide range of services focusing on the generation and productionof monoclonal antibodies. The overall objective of the Facility is to provide investigators with comprehensive hybridoma andprotein production services.The services provided include:••••••••••••Production of novel monoclonal antibodies, including complete immunization, fusion, and ELISA screening services;Custom and routine culturing of antibody producing cell lines, including thawing ofcryopreserved cell lines, subcloning, routine culture, and cryopreservation;Customized ELISA services, including performance of standard assays and development of custom assays;Antibody purification, conjugation, and isotype determination;Ascites fluid production and large-scale protein production using Hollow Fiber Bioreactor (HFB) technology; andSupply of commonly used antibodies.Flow Cytometry FacilityScientific Director: Anne Sperling, PhDTechnical Director: Ryan DugganWebsite: http://ucflow.bsd.uchicago.eduThe Flow Cytometry Facility provides access to state-of-the-art technology and quantitative analytical approaches to measuremolecular and cellular function. The Facility is designed to meet the wide-spread needs for specialized cytologic analysisby providing instrumentation for cell sorting and bench-top analysis of subcellular components using multiparametricfluorescence detection technology.The services provided include:•• Bench-top analyses ranging from simple protein expression assays usingfluorescent reporters to highly complex 9-color functional assay;•• Cell sorting at bulk rates of 30,000 cells per second or in microtiter format;•• Development of novel fluorescence-based detection assays and applications;•• Data analysis; and•• Education and training in use and application of all instrumentation and software analysis programs within the Facility.Genomics Core FacilityScientific Director: T. Conrad Gilliam, PhD.Technical Directors: William J. Buikema, PhD, Rafael Gama, PhD, and Barry Allen, PhDWebsites: http://cancer-seqbase.uchicago.edu; http://fgf.bsd.uchicago.edu; http://brdfhelp.uchicago.eduThe Genomics Core Facility provides, via its three Subcores (DNA Sequencing andGenotyping, Functional Genomics Facility, and Biomedical Research DevelopmentFacility), state-of-the-art microarray, DNA sequencing, and genotyping platformswith specialized databases for storing, managing, and manipulating both clinicalinformation and diverse types of genetic and genomic data. The Facility is aimedtowards both biomedical researchers who are generally unfamiliar with whole genomeand bioinformatics approaches, as well as experts seeking sophisticated hardware,software, programming, or database solutions, or seeking to facilitate interdisciplinarySharedResourcesUCCRC SCIENTIFIC REPORT 2009127
collaborations. The Facility maintains the latest copies of all major genomic databases, thus allowing investigators to performall genomic and bioinformatics analyses at the highest possible speeds.The services provided include:••••••••••••••••••Plasmid preparation, DNA sequencing, and genotyping analysis;Fragment assembly and primer walking;Archival data storage and technical consultations for DNA preparation and interpretation of results;Genome-scale gene expression profiling and screening of protein-DNA interactions, DNA copy numbervariations, chromosomal deletions, splicing variants, and novel transcribed sequences;Validation of differential gene/miRNA expression;Antibody protein array profiling and protein-protein interaction array hybridizations;Customized services include slide scanning, RNA extraction, RNA quality evaluation, and RNA/DNA quantification;Software tutorials and microarray data analysis; andComprehensive mirrored genomic databases, bioinformatic software applications, and custom genomic database design.Human Immunologic Monitoring FacilityScientific Director: Thomas F. Gajewski, MD, PhDTechnical Director: Yuanyuan Zha, PhDWeb Site: http://him.bsd.uchicago.eduThe Human Immunologic Monitoring (HIM) Facility provides service to clinical cancerinvestigators to measure immunologic endpoints and other pharmacodynamic parametersin subjects participating in clinical trials. The Facility serves as a specialized laboratoryto perform scientific analyses that include: 1) Evaluating changes in immune responseparameters in response to immunotherapeutic interventions; 2) Monitoring biologic effectsof other pharmacologic agents using lymphocytes or other hematopoietic cell subsets as asurrogate tissue; and 3) Interfacing with the cGMP Facility to carry out the preparation ofclinical-grade products, such as cancer vaccines, for administration to patients.The services provided include:••••••••••••Preparation of peptide-based cancer vaccines;IFN-γ ELISPOT and peptide/tetramer analysis;Flow cytometry for specific T cell subsets and activation markers;mRNA isolation and analysis of gene expression profiling data in the tumor microenvironment;ELISA assays for angiogenesis factors; andWestern blot analysis for specific signal transduction intermediates.128Human Tissue Resource CenterScientific Director: Mark Lingen, DDS, PhDTechnical Director: Leslie MartinWebsite: http://pathcore.bsd.uchicago.eduThe Human Tissue Resource Center (HTRC) provides investigators a centralizedinfrastructure to optimize the efficiency and costs related to research involving humanbiospecimens. The HTRC is comprised of three integrated components: BiospecimenBank (BSB), Laser Capture Microdissection (LCM), and Pathology Image Analysis(PIA). Currently, the HTRC provides services for the collection of clinically-annotatedhuman tissues and provides collaborative support and services for procuring, processing,dispersing, and assessing all types of biospecimens.UCCRC SCIENTIFIC REPORT 2009
The Services provided include:•• Centralized tissue banking for organ, saliva, urine, blood, plasma, serum, and other tissue derivatives;•• Pathological verification and analysis of tissue samples;•• Consultation and technical support in the construction and analyses of custom tissue microarrays;•• Histological services including routine tissue formalin fixation, processing, paraffinembedding, microtomy, H&E staining, and immunostaining;•• Identification, localization, and microdissection of targeted cell populations (from human and animal tissue sources);•• Extraction of DNA and/or RNA from dissected tissues; and•• Quantitative image analysis of immunohistochemistry on conventional and tissue microarraysections, including tissue scoring, rare event detection, microvascular density counting,ploidy analysis, integrated optical density analysis, and tissue microarray scoring.Integrated Microscopy FacilityScientific Director: Benjamin Glick, PhDTechnical Directors: Shirley Bond, MA, Christine Labno, PhD, and Vytas Bindokas, PhDWeb Site: http://digital.bsd.uchicago.eduThe Integrated Microscopy Facility functions as a supervised, user-based core by providingstate-of-the-art microscopy imaging capabilities to investigators through microscopyinstrumentation, image analysis tools, and expert training and assistance. The Facilitystrives to provide high-quality optics and equipment that most labs do not possess, includingconfocal and state-of-the-art two-photon spectral microscopes. Available techniquesprovided by the Facility include classic color histological stain imaging, contrast generationin unstained cells, and fluorescence technologies that allow for applications ranging fromlocalization of multiple targets to readouts of biochemical or physiologic parameters in eitherfixed or living preparations.The services provided include:••••••••••••••Light microscopes with brightfield and fluorescence optics, including high-end objectives and technologies (color,phase contrast, DIC, multi-parameter fluorescence including multi-ratio imaging and laser-based TIRFM);Digital image capture: high-resolution B/W and color CCD cameras, high-sensitivity CCDs, and high-speed EMCCD;Confocal microscopy including two-photon spectral systems (highresolution,high- sensitivity, and high-speed image capture);Support for live sample maintenance and imaging;New product demonstrations and user training on microscopes and software;Data analysis, storage, back-up, oversight, and maintenance; andAssistance with technique/technology development.SharedResourcesImmunohistochemistry FacilityScientific Director: Anthony Montag, MDTechnical Director: Terry Shihong Li, MDWebsite: http://ihccf.uchicago.edu/index.htmThe Immunohistochemistry Facility provides support for basic research in cellular structure/function, as well astranslational research in clinical applications and molecular medicine. The Facility aims to provide routine histologic andimmunohistochemical services in a timely manner using cutting-edge technology and expertise, evaluate and develop newtechniques and stains for development, and educate investigators.UCCRC SCIENTIFIC REPORT 2009129
The services provided include:•• Routine histological services including tissue preparation,processing, sectioning, and H&E staining;•• Specialized tissue sectioning (preparation of 20 serial sections on a single slide);•• Immunohistochemical services including enzymatic amplification methodsand detection systems using conventional and fluorescence microscopy;•• Development of staining methods for novel antibodies, including theidentification of appropriate post-sectioning fixatives, antigen retrievalmethods, buffers, enzymatic pretreatment, and antibody titration;•• Repository of control tissue for investigator use;••Development of in situ hybridization assays; and•• Technical support for protocols on all aspects of tissue antigen detection.Magnetic Resonance Imaging and Spectroscopy FacilityScientific Director: Brian Roman, PhD and Greg Karczmar, PhDTechnical Director: Xiaobing Fan, PhDWeb Site: http://mris.bsd.uchicago.eduThe Magnetic Resonance Imaging and Spectroscopy (MRIS) Facility provides magnetic resonanceimaging for studies of both animal models of cancer and clinical research involving humansubjects. The measurements provided include very high resolution anatomic images, imagesof hemodynamic parameters such as perfusion rate and capillary permeability, imaging tumoroxygenation and changes in oxygenation. In addition, the scanners can provide metabolicmeasurements with MR spectroscopy and MR spectroscopic imaging.The services provided include:•• Scans of tissues, cells, animal models of cancer, and patients to provide informationon, for example, detailed 3D anatomy, blood volume, energy metabolism, changes intumor oxygenation during therapy, calcium dynamics, and pancreatic function;•• fMRI measurements of brain activation;•• Development and testing of new contrast agents and imaging methods;•• Data analysis and consultation; and•• Veterinary services, including the preparation of animals for MRI experiments, anesthesia andrespiration, physiological monitoring, catheter implantation, and tumor implantation.Pharmacology Core FacilityScientific Director: M. Eileen Dolan, PhDTechnical Directors: Jacqueline Ramirez, MS and Shannon Delaney, MSWeb Site: http://pharmacology.bsd.uchicago.eduThe Pharmacology Core Facility evaluates pharmacokinetic, pharmacodynamic, andpharmacogenetic parameters in conjunction with clinical trials. The Facility is comprised of anAnalytical Core and a Biochemical Core. The Analytical Core is responsible for assays of variouspharmacological targets, the development of pharmacological assays of anti-cancer agents andtheir metabolites, and the analysis of drug and metabolite concentrations in biological fluids. TheBiochemical Core is responsible for the assessment of markers for drug resistance and measurementof drug-metabolizing enzyme activity in human tissue.130UCCRC SCIENTIFIC REPORT 2009
The services provided include:••••••••••Analysis of drug levels in biological fluids (whole blood, plasma, urine);Sample transportation and storage;Plasma and lymphocyte isolation from whole blood;DNA and RNA Isolation; andAssessment of markers for drug resistance.Scientific Image Reconstruction and Analysis FacilityScientific Director: Robert M. Nishikawa, PhDTechnical Director: Chun Wei Chan, MSWebsite: http://osrf.bsd.uchicago.edu/facilities/svif.htmlThe Scientific Image Reconstruction and Analysis Facility (SIRAF) provides three essentialservices for medical imaging, including a high performance computer cluster, direct archivalcapabilities, and software to facilitate the development of databases. The SIRAF allowsresearchers to have free access to all computers and services and supports image acquisition,construction of databases, reconstruction techniques, image analysis (including computeraideddiagnosis), and technology assessment. The Facility supports basic research involvingmodeling and simulations, applied research involving the development of new imageanalysis methods, research that requires patient information by aiding in the collection ofanonymized data, and the development of grid-based technologies.The services provided include:••••••••Free-access to a high speed computer system and specialized software packages;Centralized archiving for storage of large databases;HIPAA-compliant access to patient images and associated medical records storedin the Picture Archive and Communication System (PACS); andAccess to grid computing.Transgenic Mouse and Embryonic Stem Cell FacilityScientific Director: Kathleen Millen, PhDTechnical Director: Linda DegensteinWebsite: http://transgenic.bsd.uchicago.eduThe Transgenic Mouse and Embryonic Stem Cell Facility provides investigators with genetically-manipulated mice throughtransgenic technology or embryonic stem cell manipulation. The Facility provides a comprehensive set of technical services, hasa fully operational gene targeting service and offers an annual course in Mouse Handling and Breeding. In addition, the Facilityis in the process of establishing gene construction services.SharedResourcesThe services provided include:•• Transgenic mouse production from founder through F1 Stage;•• ES cell technology mouse production (e.g., knockouts, knockins, conditional knockouts);•• ES cell line development and gene targeting and culturing;•• Mouse embryonic fibroblast (MEF) cell production and embryo rederivation;•• Various breeding services and genetically engineered mouse model line maintenance; and•• DNA preparation from ES cell lines for the construction of gene targeting constructs.UCCRC SCIENTIFIC REPORT 2009131
Other Resources and Centers
Patient and Community ResourcesThe UCCRC has developed a broad range of resources to provide cancerinformation to the public. These include the UCCRC website, printpublications, the Cancer Resource Center, the Cancer Risk Clinic, theUpper Aerodigestive Malignancies Clinic, and the Community EngagementCentering on Solutions program. Through education, the UCCRC aimsto save lives through the prevention and control of cancer, and enhance itsclinical trials program through increased public awareness.Website and Print PublicationsThe UCCRC website (http://uccrc.uchicago.edu) features a “For Patients” section thatprovides general cancer information. Thepublic can access numerous links to onlineresources concerning general and specificcancer information, cancer publications,patient resources and support groups, andcancer survivorship. In addition, the UCCRCwebsite provides a cancer glossary, a calendarof events for patients and their families, acurrent listing of active UCCRC clinical trials,and designated contacts for patient referrals.The site is integrated with the University ofChicago Medical Center website, which providesinformation on clinical services, appointmentservices, and a searchable directory of physicians(http://www.uchospitals.edu). The UCCRChas completely rewritten the website and haslaunched a total redesign to make it moreuser-friendly. The new design will include anexpansive section on UCCRC programs for thecommunity and the general public.The UCCRC also informs the public aboutadvances in cancer diagnosis and treatmentthrough media outreach and the distribution ofvarious publications. A quarterly newsletter andan annual report are circulated to approximately5,000 patients and friends of the UCCRC. Thesepublications provide readers with updated UCCRCinformation on new research developments,patient care services, and active clinical trials.The UCCRC also sends email publications thathighlight related media articles to UCCRCmembers, staff, and donors approximately every2 weeks. In addition, a monthly e-mail newsletterinforms UCCRC members about its latestdevelopments and activities.The UCCRC also works closely with the UCMC’sOffice of Media Affairs to discuss news of interestto the media and general public, help respond tomedia inquiries, and ultimately inform the publicof cancer-related activities. This close workingrelationship has led to an increased focus oncancer-related issues in the media. Approximately32% of all press releases distributed by the MedicalCenter in 2008 were directly related to cancer. Forthe first five months of 2009, 33% of press releaseswere related to cancer.Other Resources& CentersUCCRC SCIENTIFIC REPORT 2009133
Cancer Resource CenterThe UCCRC offers a unique resource to patients and their families to facilitate their access to counseling and reliable cancerrelatedinformation. The Cancer Resource Center, in existence since 1997, operates in partnership with the American CancerSociety and is currently located in the main lobby of the Duchossois Center for Advanced Medicine outpatient facility. TheCenter is staffed by a certified health education specialist and a licensed clinical social worker who help patients and theirfamilies obtain comprehensive cancer information, including facts about specific types of cancer, education on treatment andpain management, and information about innovative clinical trials and how they can participate. The Center offers supportgroups for caregivers and patients with breast, head and neck, oral, and lung cancer. A new partnership with Gilda’s ClubChicago also offers patients on-site access to a wide variety of activities, including additional support/networking groups,healing arts and movement workshops, and various educational programs. The Center also offers assistance with financialgrant applications and medical insurance, referrals for social and support services (housekeeping, home healthcare, childcare, medical equipment, and other support services), and patient navigation services, including transportation to and fromcancer-related appointments (travel vouchers, discounted lodging, etc). Outreach activities include meeting with patients inthe clinic, coordinating weekly volunteer opportunities, and supplying monthly cancer awareness literature.Outreach and delivery of these special services to cancer patients has increased dramatically over the past several years. In2008, Cancer Resource Center staff had face-to-face informational meetings with approximately 2,100 patients and providedspecial services to an additional 2,633 patients (815 new patients, 1,818 return patients). The Center provided transportationassistance for more than 1,000 Chicago Transit Authority rides, gas covering 35,000 miles of travel, and 2,500 hospitalparking passes. Additionally, the Center facilitated financial assistance with medications for pain and nausea, nutritionsupplies, and home healthcare items.Cancer Risk ClinicThe Cancer Risk Clinic, established in 1992 with an initial seed grant from the UCCRC, is a comprehensive cancer riskassessment and prevention program dedicated to helping individuals with a high risk of cancer. The Clinic is directed byDr. Funmi Olopade, MBBS, and staffed by a team of genetic counselors, a research nurse, a clinical psychologist, a medicalgeneticist, and a medical oncologist who work with these individuals to provide genetic counseling, education about cancerrisk and prevention, and personalized risk reduction strategies. These strategies include systematic monitoring or screeningfor early detection, implementation of life-style changes including diet and exercise, and the use of cancer preventionprocedures or drugs. The clinic records annual visits of more than 450 new patients and has a database of more than 4,000individuals who were evaluated for inherited susceptibility to different cancers. The clinic also has an active communityoutreach program, which has led to an increase in the number and diversity of patients evaluated for cancer risk, and thusavailable for research studies. Resources in the Cancer Risk Clinic have been invaluable to the translational research efforts ofinvestigators both at the University and other collaborating institutions.134UCCRC SCIENTIFIC REPORT 2009
Upper Aerodigestive Cancer Risk ClinicThe Upper Aerodigestive Cancer Risk Clinic opened in 2007 and is co-directed by Dr. Kyle Hogarth, MD, and Ravi Salgia,MD, PhD. The Clinic offers a multidisciplinary approach to prevent, diagnosis, and treat individuals at high risk for thedevelopment or recurrence of cancers of the upper aerodigestive tract, including lung cancer, esophageal cancer, head andneck cancer, mesothelioma, and other rare malignancies. An expert team comprised of specialists in cancer, pulmonarymedicine, psychiatry, and substance abuse, work collaboratively with patients to provide individualized care, including cancerscreening, early detection services, risk reduction and prevention plans, and comprehensive treatment. Treatments are aimedat preventing or ending high-risk behaviors. These may include counseling and medication to help patients overcome tobaccoaddiction, counseling and therapy for depression, stress management, and relapse prevention plans. Through the FrancesLederer Aerodigestive Cancer Research Program, researchers are investigating the use of earlier diagnosis methods, includingthe testing of family members of patients for genetic markers that may indicate high risk. The Clinic is aiming to eventuallycreate risk profiles that will facilitate the design of individualized prevention and improved screening plans for at-risk patients.Community Lectures.The UCCRC has developed an ongoing community lecture series to provide members, nurses, and social workers with forums toeducate the public and address concerns regarding lung cancer. Sponsored by the UCCRC, the Hematology/Oncology ThoracicOncology Research Program, and the Respiratory Health Association of Metropolitan Chicago, this lecture series has been heldannually every November since 2006. The lectures focus on lung cancer diagnosis, patient resources, treatments, and research.A new lung cancer networking group was established in response to the lecture series. The group meets once per month toenable lung cancer patients, as well as their family members and friends, to share their experiences and information.Community Engagement Centering on SolutionsThe Community Engagement Centering on Solutions (CECOS) Program was developed by the UCCRC in 2007 to expandits community outreach. The program represents a comprehensive effort to enhance public awareness of cancer prevention,early cancer detection and control, and the role of genetics in cancer. Led by Rick Kittles, PhD, the Associate Director forDiversity and Community Relations at the UCCRC, the program develops collaborative partnerships with the surroundingcommunity and its leaders to promote health and prevent disease. Specifically, CECOS develops sustained relationshipsbetween Chicago’s Southside community and the UCCRC to increase local awareness of the latest advances in cancer research,provide information related to cancer issues and treatment options, and communicate the benefits of participating in cancerclinical trials and other UCCRC research studies. The program seeks to increase the participation of underserved communitiesin these studies through education. To accomplish these goals, CECOS provides a central source of information for all UCCRCcommunity-focused programming, including health, educational, volunteerism, and service programming; engages faculty andstaff in conducting cancer research in the community; trains UCCRC members in the relevance of biomedical research andenables the development of skills required to disseminate this knowledge to the community; and helps community membersshare ideas about cancer and address fears pertaining to clinical trials. CECOS also organizes workshops and conferenceswithin the Southside community to disseminate information on cancer advances, clinical trials, research trends, and the valueof understanding family history in assessing cancer risk. These activities ensure a meaningful bidirectional exchange of ideasand perspectives between the community and the UCCRC that will translate into sound, culturally-appropriate, and relevantresearch.Other Resources& CentersUCCRC SCIENTIFIC REPORT 2009135
CECOS has successfully developed and delivered one successful healthcare initiative per quarter in the Southsidecommunity since its inception. Initiatives in 2008 included the Brother to Brother: Breaking the Barriers to GoodHealth workshop for discussing men’s health and related cancer issues, the Save Our Sister: Sharing Strategies forSurvival workshop for raising awareness of breast cancer rates among the African American community, the Lungsfor Life: Facing the Challenge of Lung Cancer Together workshop for disseminating information on lung cancer riskreduction, and the Annual Nutrition Knowledge Bowl, a competition involving students from six Chicago-area highschools designed to raise awareness of nutrition and its role in preventing cancer. A video on the Nutrition Bowl wasaired on CATV in June 2009. High-school participants in this program are continuing to help CECOS spread theword about the importance of healthy eating as Nutrition Bowl Ambassadors. In 2009, CECOS organized the OurDaughters, Our Duty: The Facts about HPV and Cancer, a town hall meeting to discuss how community members canprotect themselves and their families from cervical cancer. The program has also developed unique partnerships withChicago Public Schools, Kennedy-King College, and the other City Colleges of Chicago.In response to public demand, many of CECOS’s efforts focus on the relationship between cancer and poor nutrition.An example of these activities is the partnership with theBronzeville Farmers’ Market. Every Sunday throughout the summer of 2008, CECOS members staffed a tent at themarket to distribute informational material on cancer and nutrition. In the spring of 2009, CECOS launched a newinitiative to provide nutrition tours at local grocers. The team provided on-site nutritional information and led a tourthrough Farmers Best Market, the only African American-owned supermarket in Illinois. In May of 2009, CECOS helda focus group with school teachers involved in the Nutrition Bowl to facilitate the improved design and expansion offuture nutritional events, including the 2009 Nutrition Bowl (to be held in the winter).In addition to the activities offered by the Cancer Resource Center and CECOS, the UCCRC, UCMC Office ofCommunity Affairs, and the Center of Interdisciplinary Health Disparities Research (CIHDR; see Highlights – ResearchInitiatives for details) have built positive relationships with political leaders, churches, community organizations,support groups, and other hospitals in order to develop and participate in community events. Community outreachprograms and initiatives include the Smoking Cessation Program (C-STOP); a Community Fitness Program thataddresses various health topics; monthly educational sessions held downtown at the Whole Foods grocery store onvarious topics; community workshops and forums offering cancer risk assessments, osteoporosis screenings, self breastexam demonstrations, smoking cessation classes, and nutrition information; and public education and lecture series.136UCCRC SCIENTIFIC REPORT 2009
EducationUCCRC members participate in a variety of training programs and educational opportunities. Unique departmentalcommittees are responsible for graduate and post-graduate training in a variety of disciplines related cancer, including theCancer Biology; Clinical Pharmacology and Pharmacogenomics; Genetics, Genomics, & Systems Biology; Immunology;Molecular Biology; Medical Physics; and Molecular Metabolism and Nutrition Committees. Many UCCRC members areinvolved in one or more of these training programs, many of which are supported by NIH training grants. The UCCRC alsooffers fellowship training programs in Surgical Oncology, Radiation Oncology, and Pediatric Oncology. All UCCRC membersparticipate in a variety of seminar series, journal clubs, and program and departmental retreats, which are instrumental infostering a variety of inter- and intrapro grammatic research collaborations.Committee on Cancer BiologyThe Committee on Cancer Biology administers a multidisciplinary graduate training program to bestow a PhD in CancerBiology. The Committee is directed by Geoffrey Greene, PhD, and supported by a training grant from the NCI. The programhas a full curriculum and focuses on several areas of cancer biology, including apoptosis, cancer cytogenetics, cell cycle,chromosome damage/repair, drug resistance, hormone action, metastatic progression, cell signaling, and tumor biology/immunology. The Committee facilitates the exchange of information and ideas, and fosters interactions between basic,translational, and clinical researchers.Committee on Clinical Pharmacology and PharmacogenomicsThe Committee on Clinical Pharmacology and Pharmacogenomics administers a 2-year post-graduate training program,accredited by the American Board of Clinical Pharmacology and supported by an NIH training grant, for MDs, PhDs andPharmDs. The Committee is led by Dr. Mark Ratain and consists of faculty from various departments. The goal of the programis to train individuals in various subspecialties of clinical pharmacology, including principles of therapeutics, molecularpharmacology, and pharmacogenomics. The program offers training through various didactic exercises, seminars, and researchprojects.Committee on Medical PhysicsThe Committee on Medical Physics offers research training leading to a MS or PhD degree. The program, led by Dr. MaryellenGiger and supported by an interdisciplinary NIH training grant, applies the principles of the physical sciences to biomedicine.The Committee includes members of the UCCRC Advanced Imaging Program and faculty from the Departments of Radiology,and Radiation and Cellular Oncology. Areas of focus include, for example, diagnostic radiography, magnetic resonance imagingand spectroscopy, computer-aided diagnosis and quantitative image analysis, electron paramagnetic resonance imaging, nuclearmedicine imaging, and computer applications in radiation therapy.Committee on Genetics, Genomics, & Systems Biology (GGSB)The Committee on GGSB offers a PhD program that combines training in modern genetic analysis with genetic-based methodsfor investigating clinical and basic science questions in the context of physiological, developmental, and evolutionary systems.The program, under the leadership of Douglas Bishop, PhD, is supported by an NIH training grant and consists of faculty from16 different departments and represents a broad interdisciplinary approach to teaching and research. Strengths of the programinclude gene expression and developmental genetics, chromosome organization and behavior, population and evolutionarygenetics, and genetics of human disease with an emphasis on genetic alterations in cancer.Other Resources& CentersUCCRC SCIENTIFIC REPORT 2009137
Committee on ImmunologyThe Committee on Immunology provides multidisciplinary training towards a PhD degree in fundamental immunologyand approaches to understanding immunological diseases. The program has been continuously-funded by NIH traininggrants for over 30 years and represents one of the oldest and most prestigious immunology programs in the country. TheCommittee, under the direction of Harinder Singh, PhD, integrates the basic biological sciences with the clinical sciencesto effectively develop new approaches for the diagnosis and treatment of various immune diseases and cancer. Areas ofbasic and applied immunology research include autoimmunity; hematopoiesis, lymphoid and myeloid development; T-celldifferentiation; signal transduction in lymphoid development and activation; and tumor immunity.Committee on Molecular Metabolism and Nutrition (CMMN)The Committee on MMN is an interactive research program, supported by an NIH training grant, that offersinterdisciplinary doctoral training in the molecular basis of biological processes related to nutritional status, metabolichomeostasis, and human disease. Led by Chistopher Rhodes, PhD, the program focuses on metabolism and metabolicdiseases including, for example, diabetes and obesity, using biochemical, clinical, physiological, cell, and molecular biologicalapproaches. The Committee works closely with the Digestive Disease Research Core Center and Kovler Diabetes Center atthe University of Chicago.Department of Health StudiesThe Department of Health Studies, chaired by Ronald Thisted, PhD, is a cross-disciplinary program that studies theenvironmental and organizational factors that influence the health of human populations through biostatistics, epidemiology,and health services research. The Department offers a Masters of Science in Health Studies for Clinical Professionals(MSCP), and a certificate program, the Clinical Research Training Program (CRTP). The MSCP is a course of study designedfor the enhancement of doctoral-level individuals in the theory, methods, and concepts of biostatistics, epidemiology, andhealth services research needed to design and carry out clinical and epidemiologic research studies. The CRTP, a NIHsupportedprogram designed for clinicians or clinical researchers, offers formal training opportunities in areas relevant to thedesign, implementation, and analysis of clinical research. In addition, the Department offers a PhD program in biostatistics,epidemiology, and health services research based on a core curriculum in population-based health research.MacLean Center for Clinical Medical EthicsThe MacLean Center for Clinical Medical Ethics is recognized as a leading program in the country for research and trainingin medical ethics. The Center is directed by Mark Siegler, MD, and consists of several UCCRC members as well as facultyin medicine, law, business, public policy, and social sciences. Established in 1984 with support from the family of Dorothy J.MacLean, the Center offers both a 2-year Masters Degree and a one-year part-time fellowship program. The Masters Degreeprogram provides a health services research curriculum and is intended for physicians interested in pursuing an academiccareer with a focus on health policy and clinical medical ethics. The one-year, part-time fellowship program offers clinicians,not necessarily pursuing academic medicine, training in medical ethics.138UCCRC SCIENTIFIC REPORT 2009
Graham School of General StudiesThe University of Chicago Graham School of General Studies offers a Clinical Trials Management Certificate Program. Thispost-baccalaureate program provides comprehensive training required to initiate clinical research, apply effective monitoringmethods, prepare reports, and understand regulations and good clinical practices. All staff in the Cancer Clinical Trials Officehave completed this training program, which consists of courses in clinical practices, the drug development process, statisticalconcepts for clinical research, and clinical site management and monitoring.Training GrantsUCCRC members are principal investigators of 12 NIH T32 training programs in basic and clinical research that foster andenhance interdisciplinary interactions. These training programs cover diverse areas of cancer-related research, such as cancerbiology, immunology, molecular biology, genetics, medical oncology, clinical therapeutics, medical physics, and addictionsresearch.Cancer- Relevant Training GrantsPI Grant # TitleAlbert Bendelac 5-T32-AI07090 Interdisciplinary Training Program in ImmunologyEugene Chang 5-T32-DK07074 Research Training in Digestive Diseases and NutritionMaryellen L. Giger 5-T32-EB02103 Research Training in Medical PhysicsBenjamin Glick 5-T32-GM07183 Molecular and Cellular Biology Training GrantGeoffrey Greene 5-T32-CA09594 Graduate Training Program in Cancer BiologyElizabeth M. McNally 5-T32-HL07381 Cardiovascular Sciences Training GrantDavid Meltzer 5-T32-AG23496 MD/PhD Program in Medicine, Social Sciences, and AgingOlufunmilayo Olopade 5-T32-CA09566 Basic Medical Research Training in Medical OncologyMark J. Ratain 5-T32-GM07019 Clinical TherapeuticsNancy B. Schwartz 5-T32-HD07009 Graduate Training in Growth and DevelopmentJulian Solway 5-T32-HL07605 Research Training in Respiratory BiologyPaul Vezina 5-T32-DA07255 Neuropsychopharmacology Training in Drug Abuse ResearchOther Resources& CentersUCCRC SCIENTIFIC REPORT 2009139
The University of Chicago Medical CenterThe University of Chicago Medical Center has been at the forefront of medicine since 1927. The Medical Center occupies over 30buildings, which house all hospital and clinical areas of the campus as well as teaching and research space. The primary clinicalfacilities of the UCCRC include the Bernard A. Mitchell Hospital, the Comer Children’s Hospital, and the outpatient clinics inthe Duchossois Center for Advanced Medicine (DCAM).Bernard A. Mitchell HospitalThe Bernard A. Mitchell Hospital is the primary adult inpatient facility, which includes the emergency department and theArthur Rubloff Intensive Care Tower. More than 60 beds are dedicated to adult medical oncology. Patients who participatein clinical pharmacology studies and require hospitalization are placed in the GeneralClinical Research Center (GCRC), an NIH-funded facility with dedicated skilled nursingand research staff for clinical research. The facility provides more than 4,000 square feetof space for specialized research and patient care (8-bed inpatient and 3-bed outpatientunits). Additional GCRC resources include a dedicated metabolic kitchen, nutritionunit, and a core laboratory facility offering a variety of services such as rapid routineassays and sample processing.Comer Children’s HospitalThe Comer Children’s Hospital, which opened in 2005, is a tertiary care teaching facility dedicatedto treating childhood diseases through patient education, care, and research. The state-of-the-arefacility provides 242,000 sq ft of space with a capacity of more than 150 beds, 25% of which arededicated to the treatment of children and adolescents with cancer. The facility also includes oneof the country’s largest and most advanced pediatric intensive-care units equipped to treat childrenwith multiple traumas and complex medical problems.Duchossois Center for Advanced MedicineThe UCCRC’s outpatient facilities are located in the state-of-the-art DCAM facility,which brings together most of the Medical Center’s diagnostic and outpatient treatmentservices. The 550,000 sq ft facility houses outpatient clinics for medical oncology,gynecological oncology, and radiation oncology. Resources include modern radiationtherapy facilities, contemporary chemotherapy infusion suites, and an apheresis unit.The multidisciplinary Breast Center provides mammography services, examination andconsulting rooms, patient information, and cancer risk assessment in a single location toserve patients with breast cancer and their families.New Hospital PavilionThe UCMC has made significant commitments to replacing clinical care and clinicalresearch space with state-of-the art facilities. In addition to the opening of the ComerChildren’s Hospital and Center for Children and Specialty Care in 2005 and 2006,construction of the New Hospital Pavilion began in 2009. The Pavilion will be a400,000 sq ft, $700 million facility that will provide complex specialty care, witha focus on cancer and advanced surgery. Completion of the facility is planned for 2012.140UCCRC SCIENTIFIC REPORT 2009
Dedicated Research FacilitiesEllen and Melvin Gordon Center for Integrative Science (GCIS)The GCIS is a 430,000 sq ft building that houses 20 members of the UCCRC in stateof-the-artmodular laboratories. The seven-story building, which opened in 2005,represents one of the few collaborative research facilities in the nation that bridgesphysical and biological sciences under one roof. The GCIS houses the Ben MayDepartment for Cancer Research, the Howard Hughes Medical Institute, the Institutefor Biohpysical Dynamics, the Department of Biochemistry and Molecular Biology, andselect laboratories of the Physical Sciences Division.Gwen and Jules Knapp Center for Biomedical <strong>Discover</strong>yThe UCCRC is experiencing a significant expansion in facilities. Constructionof the Knapp Center for Biomedical <strong>Discover</strong>y (KCBD) has been completed withoccupancy occurring during June of 2009. The 12 story KCBD provides an additional330,000 sq ft of research space and houses ~50 UCCRC researchers. The facilityincludes a state-of-the-art vivarium; dedicated core facility space for the Genomics,Transgenic Mouse/ES Cell, and Integrated Microscopy Facilities; and will housesresearch programs from the Departments of Medicine (Section of Hematologyand Oncology) and Pediatrics (Section of Pediatric Hematology and Oncology), the UCCRC, the Ludwig Center for MetastasisResearch, and the Institute for Genomics and Systems Biology. The UCCRC has 22,000 sq ft, allowing for the recruitmentof up to 8 new faculty members. The KCBD is connected to the adjacent GCIS and Knapp Center for Molecular Medicine bypedestrian bridges. Upon full occupancy of the KCBD, over 75 UCCRC researchers (more than 80% of all UCCRC laboratoryresearchers) will be located in three inter-connected, state-of-the-art facilities. This configuration will foster more extensiveinteractions between researchers and enable the UCCRC to achieve strategic programmatic growth.Other Resources& CentersUCCRC SCIENTIFIC REPORT 2009141
HighlightsThe Gwen and Jules Knapp Center forBiomedical <strong>Discover</strong>y, a new UCCRC research facility.
Research InitiativesBreast Cancer Specialized Program of Research Excellence (SPORE)The Breast Cancer SPORE program brings together a multidisciplinary team of basic, clinical, and population scienceinvestigators to perform innovative research using a global strategy to reduce the pain and suffering from breast cancer.Awarded by the National Cancer Institute, the program is one of only 11 Breast SPOREs in the the United States. Theinvestigators represent three UCCRC Programs, including the the Cancer Risk and Prevention, Advanced Imaging, and Clinicaland Experimental Therapeutics Programs. The Breast Cancer SPORE is an integrated program that translates recent advancesin genetics to benefit women who are at risk of developing an aggressive form of breast cancer, which disproportionately affectsAfrican American women at a young age.The Breast Cancer SPORE is led by Dr. Fumni Olopade (Cancer Risk and Prevention Program), along with co-leaders Drs. GiniFleming (Clinical and Experimental Therapeutics Program), and Maryellen Giger (Advanced Imaging Program), and involvesresearchers in genetics, bioinformatics, molecular biology, biophysics, and structural biology. The UCCRC integrates theseresearchers with those in clinical disciplines, including epidemiology, medical oncology, surgical oncology, and radiationoncology, to facilitate the translation of scientific advances to patients.The SPORE consists of four translational research projects, each co-led by basic and applied investigators from the UCCRC.Project 1 aims to develop mammography and MRI image-based markers, to assess breast density, for use alone or incombination with other biomarkers to quantify breast cancer risk and monitor therapeutic response. In Project 2, researchersare examining whether MR imaging with improved spectral, temporal, and spatial sampling leads to improved detection ofearly breast cancer. Project 3 aims to determine whether variations in genes involved in hormone and xenobiotic metabolisminfluence breast cancer risk. Finally, Project 4 aims to identify population-specific genetic variants that influence toxicityto breast cancer chemotherapy. These projects are supported by an Analytic and Informatics Core; Biospecimen, Pathologyand Genotyping Core; and an Administration Core. These Core Facilities were built on the unique strengths of the existingUCCRCsupported Cores.Breast Cancer SPORE Projects and LeadersProject Basic Scientist Applied Scientist(s)1) Imaging-based determination ofbreast cancer riskMaryellen Giger(Advanced Imaging Program)Gillian Newstead,(Advanced Imaging Program)2) Specificity of MRI with optimaltemporal, spatial, and spectralsampling in early breast cancerGregory Karczmar(Advanced Imaging Program)Gillian Newstead(Advanced Imaging Program)Nora Jaskowiak(Cancer Risk and Prevention Program)3) Variation in hormone andxenobiotic metabolizing enzymegenes and breast cancerAnna Di Rienzo(Cancer Risk and Prevention Program)Olufunmilayo Olopade (Cancer Riskand Prevention Program)4) Identifying population specificvariants important in toxicity tobreast cancer therapyM. Eileen Dolan(Clinical and ExperimentalTherapeutics Program)Mark Ratain (Clinical andExperimental Therapeutics Program)HighlightsUCCRC SCIENTIFIC REPORT 2009143
Leukemia and Lymphoma Society Specialized Center of Research Grant (SCOR)The SCOR focuses on the development of peptides and small molecules therapeutics for hematological malignancies.Awarded by the Leukemia and Lymphoma Society, this initiative specifically aims to develop a comprehensivemultidisciplinary program that will provide a platform for the identification and testing of novel cell-permeable peptidesand small molecules for the treatment of hematological malignancies. Development of the SCOR grant was supported byPilot Project funding from the UCCRC. The SCOR represents a collaboration among three institutions and is led by MichaelThirman, MD (Molecular Genetics and Hematopoiesis Program).The central theme of the SCOR program is a common therapeutic strategy based on the targeting of protein-proteininteractions in leukemia and lymphoma, rather than focusing on a single disease entity. The program brings together alarge group of scientists to form a highly interactive group of chemists, molecular biologists, and clinicians who might nototherwise have the opportunity to work together in a translational research program in leukemia and lymphoma. Specifically,the program encompasses a collaborative effort involving eleven University of Chicago senior researchers as well as twoproject leaders from two other NCI-designated Cancer Centers. Each project within the SCOR incorporates the use ofcell permeable peptides and small molecules as part of an integrated program to develop and optimize a novel therapeuticplatform for hematologic malignancies. The associated cores have formed an integral part of the SCOR and have providedvaluable reagents and expertise for each of the projects.SCOR Projects and LeadersProject1) Targeting Transducible Anticancer PeptideTherapeutics to Kill Tumor Cells In Vivo2) Peptide and Small Molecule Therapeutics forMLL-Associated Leukemia3) Specific Anti-BCL-6 Targeted TranscriptionTherapy for B-Cell LymphomasLeaderSteven Dowdy(University of California-San Diego)Michael Thirman(UCCRC - Molecular Genetics and Hematopoiesis Program)Ari Melnick(Cornell University)CoreLeader(s)A) Peptide Therapeutics Steve Kron and Piers Nash(UCCRC - Cell Signaling and Gene Regulation Program)Steven Dowdy(University of California-San Diego)B) Small Molecule Therapeutics Geoffrey Greene and Milan Mrksich(UCCRC - Cell Signaling and Gene Regulation Program)C) Patient Demographics and Cell Bank Michelle Le Beau and Richard Larson(Molecular Genetics and Hematopoiesis Program)D) Hematopathology John Anastasi(Molecular Genetics and Hematopoiesis Program)E) Clinical Trials and Minimal Residual DiseaseMonitoringWendy Stock(Molecular Genetics and Hematopoiesis Program)F) Stem Cell Processing and Purging Koen van Besien and Amittha Wickrema(Molecular Genetics and Hematopoiesis Program)144UCCRC SCIENTIFIC REPORT 2009
Center for Interdisciplinary Health Disparities Research (CIHDR)In 2003, the UCCRC was awarded one of eight Center grants by the National Institutes of Health/National Cancer Instituteto study health disparities. The CIDHR, based at the University of Chicago’s Institute for Mind and Biology, was establishedto understand population health and health disparities to eliminate group differences in health using a multi-level approach.Over the past five years, the CIHDR has focused its efforts on understanding population differences in the incidence andnature of breast cancer among Black and White women. Black women in the United States and West Africa develop breastcancers that occur at a younger age and are more aggressive and lethal than those experienced by White women of NorthernEuropean ancestry. In conjunction with these studies, the Center is also examining the occurrence of breast cancer in Nigerianwomen through research conducted at the University of Ibadan. The overall goal is to increase our understanding of the social,behavioral, and biological factors that influence health disparities so that appropriate measures may be taken to eliminate suchdisparities.The CIHDR is directed by Sarah Gehlert, PhD, the Associate Dean for Research in the School of Social Service Administration,and co-directed by Martha McClintock, PhD, the David Lee Shillinglaw Distinguised Service Professor in Psychology (bothmembers of the Cancer Risk and Prevention Program). The Center draws on the diverse talents of social workers, psychologists,physicians, and molecular geneticists to explore the causes of breast cancer in African-American women by examining bothmedical and environmental factors.The specific aims of the Center are to bring together scientists and community members who are vulnerable to adverse healthconditions to inform them of the Center’s agenda, which are to 1.) foster health disparities research from multiple levels ofanalysis through shared conceptual frameworks that integrate discipline-specific theories and methods; 2.) increase interest inhealth disparities among scientists, students, and community members; 3.) develop appropriate methods for the comprehensiveanalysis of environmental, psychological, and genetic factors among vulnerable populations; 4.) increase existing knowledge onsocial, behavioral, and biological factors that influence health disparities; and finally, 5.) disseminate these findings to vulnerablepopulations, community organizations, and scientific researchers. The Center is supported by the Human Tissue ResourceCenter Core, and is conducting research in four separate projects to achieve these aims.CIHDR Projects and LeadersProject1) Comparison of gene regulation in mammary tumors and ovarianfunction between socially isolated and group-living rats2) Molecular characterization of primary breast tumors fromNigerian and Chicago Southside women to determine ifalterations in BRCA1 contribute to breast cancer in youngerBlack women; exploration of McClintock’s model in primarytumors3) Examination of culture-specific views of breast cancer andtreatment; testing of McClintock’s model in communityvolunteers (using community, living, social, behavioral,biological, and health outcomes factors)LeaderMartha McClintock(Cancer Risk and Prevention Program)Olufunmilayo Olopade(Cancer Risk and Prevention Program)Sarah Gehlert(Cancer Risk and Prevention Program)4) Examination of mammary tumor growth rate, response tochemotherapy, and chemoprevention in animal modelsSuzanne Conzen(Cell Signaling and Gene Regulation Program)HighlightsUCCRC SCIENTIFIC REPORT 2009145
Institute for Genomics and Systems Biology (IGSB)The IGSB was established to further the advancement of technology development for genome analysis and accelerate thetransition of basic discoveries in genome science into translational and clinical research. The Institute, which reflectsthe collaborative nature between the University of Chicago and Argonne National Laboratory, focuses on genomics andsystems biology approaches to understand genome function evolution, uncover new diagnostic and therapeutic targets, anddiscover new strategies for complex human diseases with a major focus on cancer. The IGSB is organized into ten areas ofinvestigation, including proteomics and structural genomics, computational biology and informatics, microbial systemsbiology, evolutionary genomics and systems, biological engineering and technology development, cellular and genomicnetworks, chemical genomics, cancer, population genomics and complex diseases, and clinical genomics.The Institute is directed by Kevin White, PhD, (Cell Signaling and Gene Regulation Program) and draws on the expertiseof investigators from Argonne National Laboratory and more than twenty different departments in the Biological Sciencesand Physical Sciences Divisions at the University of Chicago. More than 70 researchers, many of which are members of theUCCRC, are performing research on complex biological systems from a wide variety of experimental, computational, andtheoretical approaches. Current research initiatives include breast cancer, metabolic diseases and diabetes, and inflammatorybowel disease. The IGSB has established two core facilities to support its research, including the Cellular Screening Center(CSC), for high-throughput RNAi and chemical genetic screening, and the High-Throughput Genome Analysis Core (HGAC),which features resources for ultra-high-throughput sequencing and microarray processing. The IGSB is also establishing aProteomics Core for high-throughput cloning and protein production facilities for antibody generation.IGSB Initiatives and LeadersInitiative1) Breast Cancer – Assessment of the role of specific genes in breastcancer; rapid identification of novel drug targets; screening of chemicallibraries to develop improved, targeted therapies2) Metabolic Diseases and Diabetes – <strong>Discover</strong>y of genomic variation andexpression patterns for evaluating potential outcomes of drug therapy;drug and genome screening of insulin-secreting cells for identifyingtherapies that promote insulin production3) Inflammatory Bowel Disease – Determination of the relationshipbetween specific bacteria and inflammatory bowel diseaseLeaderKevin White(Cell Signaling and Gene Regulation Program)and Ruby DharMark Ratain(Clinical and Experimental TherapeuticsProgram)Eugene Chang(Cancer Risk and Prevention Program)146UCCRC SCIENTIFIC REPORT 2009
Ludwig Center for Metastasis ResearchThe Ludwig Center for Metastasis Research, which is affiliated with the UCCRC, aims to further our understanding ofmetastasis and translate laboratory concepts into novel therapeutics for the prevention and treatment of metastasis. Establishedin 2006 by an endowment from the Ludwig Fund (providing $2.5 million per year), the Center will be housed in the Gwen andJules Knapp Center for Biomedical <strong>Discover</strong>y. The Center is led by Ralph Weichselbaum, MD, the Chairman of the Departmentof Radiation & Cellular Oncology (Clinical and Experimental Therapeutics Program) and Geoffrey Greene, PhD, the Vice Chairof The Ben May Department for Cancer Research and the Associate Director Basic Sciences for the UCCRC (Cell Signalingand Gene Regulation Program). Researchers from various disciplines, including molecular and cell biology, bioinformatics,chemistry, genetics, imaging, and medicine collaborate to dissect the basic mechanisms of metastasis using sophisticated, stateof-the-artapproaches. The Center is pursuing three specific research aims, initially targeting metastasis of breast and prostatecancers.Ludwig Center AimsAims1) Development of radiolabeled steroidreceptor modulators2) Development of novel receptortargetednanoparticle reagents3) Identification and development ofnovel small moleculesDescriptionFor imaging and killing tumor cells expressing the estrogen or androgenreceptor (targeted against cancers of the breast, prostate, ovary, and lung)For selective and precise imaging and delivery of therapeutics to tumor cellsexpressing the estrogen or androgen receptor (targeted against a wide array ofcancers)For the sensitization of tumors, independent of hormone receptor status, toionizing radiation or chemotherapy (targeted against cancers of the breast, headand neck, lung, ovary, and prostate)HighlightsUCCRC SCIENTIFIC REPORT 2009147
Systems Biology Approach for the Study of Therapy-Related Acute Myeloid Leukemia (t-AML)In early 2009, the Cancer Research Foundation (CRF) provided the University of Chicago with generous funding to catalyzea multidisciplinary systems biology and genomics approach to study t-AML. An interdisciplinary team of scientists hasbeen assembled to use a comprehensive approach to identify individuals at risk for developing t-AML, identify geneticsusceptibility factors that are involved, and design effective prevention and treatment strategies for this disease. Therapyrelatedacute myeloid leukemia is a direct result of mutational events that are induced by chemotherapy or radiotherapyused in the treatment of primary malignancies, such as breast and colon cancer. Approximately 8-10% of all patients treatedfor cancer will develop the disease, an average of 5 years after receiving treatment, and have a median survival of 8 months.Patients who have received immunosuppressive agents for organ transplantation and the elderly are also at risk for developingt-AML and AML.Members of the interactive team, led by Michelle Le Beau, PhD, Director of the UCCRC and Cancer Cytogenetics Laboratory,represent the UCCRC and the IGSB. The team has extensive research expertise in clinical oncology, hematopathology,genetics, genomics, systems biology, computational modeling of molecular networks, and hematopoiesis. Using a systemsapproach, these investigators will integrate six research projects involving high-throughput screening, stem cell biology,pharmacogenetics, clinical trial design, and computation to understand the basic biology of t-AML. Taken together, theseprojects will help researchers identify the molecular basis of the disease and lead to improved therapies, earlier detection, andprevention strategies.t-AML Projects and LeadersProject1) Identifying the genetic signature of therapy-relatedleukemiasTeamKen Onel, Michelle Le Beau, and Richard Larson (MolecularGenetics and Hematopoiesis Program); Kevin White (CellSignaling and Gene Regulation Program); Yves Lussier (Clinicaland Experimental Therapeutics Program)2) Understanding the leukemia stem cell John Cunningham, Michelle Le Beau, and Harinder Singh(Molecular Genetics and Hematopoiesis Program); Kevin White;Yves Lussier3) Pharmacogenetics – predicting response to therapy Ken Onel and Sandeep Gurbuxani (Molecular Genetics andHematopoiesis Program); M. Eileen Dolan (Clinical andExperimental Therapeutics Program); Yves Lussier4) Using the leukemia stem cell to model disease Harinder Singh, John Cunningham, Michelle Le Beau, YvesLussier5) Targeted clinical trials Richard Larson, Lucy Godley, Wendy Stock, and OlatoyosiOdenike (Molecular Genetics and Hematopoiesis Program); M.Eileen Dolan; Rong Huang6) Computational biology – creating an atlas oftherapiesYves Lussier with all team members148UCCRC SCIENTIFIC REPORT 2009
Selected Awards and HonorsCell Signaling and Gene Regulation ProgramEdwin Ferguson, PhD, Associate Professor of Molecular Genetics and Cell Biology, was the recipient of the University ofChicago 2009 Llewellyn John and Harriet Manchester Quantrell Award for Excellence in Undergraduate Teaching.Hue Luu, MD, Assistant Professor of Surgery, was the recipient of the 2009 Career Development Fellowship Award from theOrthopaedic Research Society.Elizabeth McNally, MD, PhD, Professor of Medicine, was elected Vice President of the American Society for ClinicalInvestigation (ASCI) in 2009.Kevin White, PhD, Professor of Human Genetics, was named by Crain’s Chicago Business as one of its “40 Under 40” in 2008,which recognizes the area’s up-and-comers. Dr. White was the only recipient from an academic setting.Molecular Genetics and Hematopoiesis ProgramKenneth Cohen, MD, Assistant Professor of Medicine, was the recipient of the 2009 Cancer Research Foundation YoungInvestigator Award.Barbara Kee, PhD, Associate Professor of Pathology, was the co-editor with Dr. Amittha Wickrema of the book entitled,Molecular Basis of Hematopoiesis (2009).Richard Larson, MD, Professor of Medicine, served as a Councilor for the 2009 American Society of Hematology ExecutiveCommittee. Dr. Larson was also the Co-Chair of the 2009 Organizing Committee for Global Opinion Leader Summit onCML in Paris, France and a member of the 2009 Organizing Committee for Benzene (Health Effects and Mechanisms of BoneMarrow Toxicity) at the Technical University of Munich, Germany.Michelle Le Beau, PhD, Professor of Medicine, was elected to the Board of Directors of the American Association of CancerInstitutes and received the American Cancer Society Distinguished Service Award in 2008. Dr. Le Beau was also selected togive the 2008 Distinguished Lectureship for the Lurie Comprehensive Cancer Center of Northwestern University.Olatoyosi Odenike, MD, Assistant Professor of Medicine, is a member of the International Working Group for MyelofibrosisResearch and Treatment. Dr. Odenike is also a 2009 member of the American Society of Clinical Oncology (ASCO) ScientificProgram Committee for the Leukemia, Myelodysplasia, and Transplantation Track and will serve as the Track Leader in 2010.Janet Rowley, MD, Professor of Medicine has received many of the nation’s most prestigious awards, and 2009 was anextraordinary year for awards. President Barack Obama awarded her with the Presidential Medal of Freedom, the nation’shighest civilian honor. (In 1998, President Bill Clinton presented the National Medal of Science, the nation’s highest scientifichonor, to Dr. Rowley.) She also received the 2009 Genetic Prize of the Peter and Patricia Gruber Foundation and the 2009Association of American Cancer Institute’s distinguished Scientist Award. She was one of only six research scientists invited byPresident Barack Obama to the signing of the executive order to lift the ban on embryonic stem cell research in 2009.Amittha Wickrema, PhD, Associate Professor of Medicine, was the co-editor with Dr. Barbara Kee of Molecular Basis ofHematopoiesis (2009).HighlightsUCCRC SCIENTIFIC REPORT 2009149
Immunology and Cancer ProgramMaria-Luisa Alegre, MD, PhD, Associate Professor of Medicine, received the Leif B. Sorenson Faculty Research Award fromthe University of Chicago Department of Medicine in 2008. Dr. Alegre was also elected to the Board of Directors for theAutumn Immunology Conference as a Liaison to Academia and member of the Basic Science Advisory Committee for theAmerican Society of Transplantation in 2009.Albert Bendelac, MD, PhD, Professor of Pathology, was named the University of Chicago A.N. Pritzker Professor inPathologyin 2008.Thomas Gajewski, MD, PhD, Associate Professor of Pathology, was elected the incoming President (2010-2012) of theInternational Society for the Biologic Therapy of Cancer (iSBTc), the major translational cancer immunotherapy society.Vu Nguyen, MD, Assistant Professor of Medicine, received the Cancer Research Foundation Young Investigator Awardin 2008, and was the recipient of the Damon Runyon Clinical Investigator Award and the American Society for Blood andMarrow Society New Investigator Award in 2009.Jian Zhang, MD, Assistant Professor of Medicine, was the recipient of the Career Investigator Award from the AmericanLung Association in 2008.Clinical and Experimental Therapeutics ProgramEzra Cohen, MD, Assistant Professor of Medicine, was a member of the Scientific Committee for the 7 th InternationalConference on Head and Neck Cancer. He is also a member of the Investigational Drug Steering Committee PI3K/Akt/mTOR (PAM) Task Force (2008), International Thyroid Oncology Group (2009), and American Society of Clinical OncologyScientific Program Committee (2009). Dr. Cohen also served as a panelist at the 2009 Workshop on Oral Cancer Screening,hosted by the American Dental Association’s Council on Scientific Affairs.Mark Ferguson, MD, Professor of Surgery, was elected President of the International Society of Diseases of the Esophagus in2008 and appointed to the Board of Directors for the Cardiothoracic Surgery Network (CTSNet) in 2009.Alessandro Fichera, MD, Assistant Professor of Surgery, was nominated President of the Chicago Society of Colon andRectal Surgeons in 2008 and elected into the Society of University Surgeons in 2009.Philip Hoffman, MD, Professor of Medicine, was named the 2009 Faculty Honoree by the University of Chicago PritzkerSchool of Medicine class of 2009.Edwin Kaplan, MD, Professor of Surgery, received the Oliver Cope Meritorious Achievement Award in 2009 from theAmerican Association of Endocrine Surgeons (AAES) for his contributions in the field of endocrine surgery as an investigator,teacher, and clinical surgeon. This honor has only been awarded five prior times in the 30-year history of the AAES.Theodore Karrison, PhD, Associate Professor of Health Studies, was inducted as a Fellow of the American StatisticalAssociation (ASA) in 2009 for his outstanding contributions to statistical methodology, collaborative research, and leadershipin the field of statistical science. The ASA Fellow designation is among the most distinctive honors in the field of statistics.Hedy Kindler, MD, Associate Professor of Medicine, was elected President of the International Mesothelioma InterestGroup. She was also elected a member of the Board of Directors and Cadre Leader (Pancreatic Cancer) of the Cancer andLeukemia Group B (CALGB).150UCCRC SCIENTIFIC REPORT 2009
Bruce Minsky, MD, Professor of Radiation and Cellular Oncology, was the recipient of the 2008 Distinguished Alumni Awardfrom the Memorial Sloan Kettering Cancer Center. In 2008, he was a Visiting Professor in the Department of RadiationOncology at the Medical College of Wisconsin and at the Mofitt Cancer Center in Tampa, FL. He was also a Visiting Professorat Oregon Health and Sciences University in Portland, OR and at Sirio-Lebanese Hospital in Sao Paulo, Brazil in 2009.Mitchell Posner, MD, Professor of Surgery, is a member of the Surgical Oncology Advisory Council of the American Board ofSurgery (2009) and was nominated President-Elect of the Society of Surgical Oncology in 2009.Kevin Roggin, MD, Assistant Professor of Surgery, was elected to the Gold Humanism Honors Society (2008) and was therecipient of the 2008 Leonard Tow Humanism in Medicine Award. Dr. Roggin was also nominated Outstanding FacultyMember and elected as a fellow of the Academy of Distinguished Medical Educators of the Pritzker School of Medicine in 2008.He was listed as one of “America’s Top Surgeons” by the Consumers’ Research Council of America (2008-2009) and received the2009 MDx Medical Patient’s Choice Award.Richard Schilsky, MD, Professor of Medicine, was elected the President of the American Society of Clinical Oncology in 2008.David Song, MD, Associate Professor of Surgery, was the 2008 recipient of the Arthur G. Michel Award, in recognition of beingan outstanding clinician, from the Breast Cancer Network of Strength.Walter Stadler, MD, Professor of Medicine, was listed as one of “America’s Top Doctors” in medical oncology by CastleConnolly in 2008.Gary Steinberg, MD, Professor of Surgery, was appointed the Chairperson of the Scientific Advisory Board of the BladderCancer Advocacy Network in 2009. He was also selected Program Chairman for the 2009 Fourth Annual Bladder Cancer ThinkTank Meeting focused on “Novel Therapeutics for Advanced Urothelial Cancer of the Bladder”.Everett Vokes, MD, Professor of Medicine, was appointed Chairman of Medicine at the University of Chicago Medical Centerin 2009. Dr. Vokes has been recognized several times on America’s best doctor lists, including America’s Top Doctors byCastle Connolly (most recently 2008), Best Doctors in America, and Chicago Magazine’s Top Doctors. He was also one of tworecipients of the 2008 Translational Research Professorship from the American Society of Clinical Oncology. Dr. Vokes hasserved as Chair of the Cancer and Leukemia Group B (CALGB) Respiratory Committee since 2004.Advanced Imaging ProgramStephen Archer, MD, Professor of Medicine, is the Chair of the Cardiopulmonary Critical Care Council of the American HeartAssociation and was elected member of the Association of Professors of Cardiology in 2008.Samuel Armato, PhD, Associate Professor of Radiology, was the Raine Visiting Professor at the University of Western Australiain Perth (2009).Richard Baron, MD, Professor of Radiology, was appointed to the Radiological Society of North America (RSNA) Board ofDirectors in 2008.Maryellen Giger, PhD, Professor of Radiology, was named President-Elect (2008), President (2009), and Chairman of the Board(2010) for the American Association of Physicists in Medicine.Charles Metz, PhD, Professor of Radiology, received the 2008 Kurt Rossmann Award for Excellence in Teaching from studentsin the University of Chicago Graduate Programs in Medical Physics, offered jointly by the Departments of Radiology andRadiation and Cellular Oncology.HighlightsUCCRC SCIENTIFIC REPORT 2009151
Cancer Risk and Prevention ProgramAnirban Basu, PhD, Assistant Professor of Medicine, was a recipient of the 2009 Bernie J. O’Brien New Investigator Awardfrom the International Society of Pharmacoeconomics and Outcomes Research (ISPOR). He was also chosen as the LabelleLecturer in Health Services Research at McMaster University, Canada, and was the winner of the Society for MedicalDecision Making (SMDM) Comparative Effectiveness Research Essay Contest in 2009.Brian Chiu, PhD, Associate Professor of Health Studies, was inducted to the Delta Omega Honorary Society in PublicHealth, Alpha Phi Chapter, in 2009.Harriet De Wit, PhD, Professor of Psychiatry, was the 2009 recipient of the Marian W. Fischman Lectureship Award fromthe College on Problems of Drug Dependence. The award recognizes the contributions of an outstanding woman scientist indrug abuse research.James Dignam, PhD, Associate Professor of Health Studies, will assume the position of Group Statistician and SeniorScientific Director, Statistics and Data Management Center for the Radiation Therapy Oncology Group (RTOG) in 2009.Founded in 1968, the RTOG is an NCI-sponsored multi-institutional international Clinical Trials Cooperative Group. Whilethe RTOG headquarters are located at the American College of Radiology in Philadelphia, Dr. Dignam will coordinate thisactivity from the University of Chicago.David Grdina, PhD, Professor of Radiation and Cellular Oncology, was appointed as a member of the NASA Space RadiationStanding Review Panel and the National Council on Radiation Protection and Measurements PAC1 in 2009.Sarah Gehlert, PhD, Professor of the School of Social Service Administration, was named to the Helen Ross Professorship in2008.Stacy Lindau, MD, Assistant Professor of Obstetrics and Gynecology, is the Director of the University of Chicago Program inIntegrative Sexual Medicine for Women and Girls with Cancer (2008). Dr. Lindau received the Best Poster Award in Biology atthe International Society for the Study of Women’s Sexual Health 2009 Annual Meeting. She is also a member of the NationalAcademy of Sciences Committee on Population, which is organizing a workshop on Collecting, Storing, Accessing, andProtecting Social Survey Data Containing Biological Measures in 2009.David Meltzer, MD, PhD, Associate Professor of Medicine, was elected a member of the American Society for ClinicalInvestigation (ASCI) in 2008.Olufunmilayo Olopade, MBBS, Professor of Medicine, was elected to the Institute of Medicine of the National Academies in2008. Dr. Olopade also received the Nigerian Lawyers Association Annual Merit Award, National Medical Association Scrollof Merit Award, and YWCA Racial Justice Award in 2008. She was named Honorary Canon by the Saint James Cathedral ofChicago, Illinois in 2008 and received an Honorary Degree of Doctor of Science from Bowdoin College in Brunswick, Maine in2009.David Rubin, MD, Associate Professor of Medicine, received a fellowship in the American Gastroenterological Association andwas elected to the Nominating Committee for the American Gastroenterological Association in 2009.Dr. Lisa Sanchez-Johnsen PhD, Assistant Professor of Psychiatry, recently received the “Distinguished Early CareerProfessional” award from the National Latino Psychological Association due to her research, service, and clinical workaddressing health disparities and community based research. She also received the “Latino Leadership Citation PresidentialAward” from the American Psychological Association based on her “innovative research in developing culturally-tailoredbehavioral interventions to reduce cancer related outcomes”. For the past 6 years, she has been a Health Disparities ResearchScholar with the NIH-National Center for Minority Health and Health Disparities.152UCCRC SCIENTIFIC REPORT 2009
FinancialsThe University of Chicago Cancer Research CenterReporting Date: 3/31/09Funding AgencySum of Direct CostsSum of Total Costs(Direct + Indirect)Total Numberof ProjectsACS $1,124,165 $1,325,000 8NCI $24,431,918 $34,658,783 106NSF $341,157 $502,424 6Other NIH $40,943,439 $55,650,976 159Other Peer $4,930,558 $6,296,547 32Subtotal of Peer Reviewed $71,771,237 $98,433,730 311Industry $10,604,635 $13,444,055 215Other Non Peer $10,579,303 $11,343,429 132Subtotal of Non Peer Reviewed $21,183,938 $24,787,484 347Grand Total (All Projects) $92,955,175 $122,529,210 658*CALGB projects ($11,306,870 Total Cost) are not included above.HighlightsUCCRC SCIENTIFIC REPORT 2009153
www.uccrc.uchicago.eduEditor: Hoyee Leong, PhDCover Design: Words & PicturesInterior Design and Printing: Pixel Print Graphics