

Chapter 86

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Management of the Neonate:<br />
Anesthetic Considerations<br />
Per-Arne Lönnqvist<br />
<strong>86</strong><br />
CHAPTER<br />
INTRODUCTION<br />
Safe and effective anesthesia for the neonate undergoing surgery<br />
is one of the most challenging tasks presented to the anesthesio -<br />
logist. Great manual skills and continuous practice are required<br />
to perform successfully such essential tasks as vascular line place -<br />
ments and tracheal intubation. Additionally, to provide successful<br />
pediatric anesthesia, extensive knowledge of the neonate’s unique<br />
physiology is required. Neonatal anesthesia demands a wellplanned<br />
technique, based on a good understanding of pathophy -<br />
siologic conditions and surgical needs. In the past, both major<br />
surgery (e.g., thoracotomy for ductus arteriosus ligation) as well as<br />
minor operations (e.g., circumcision) were performed without<br />
analgesia. 1,2 This inhumane management can result in a measur -<br />
able and detrimental stress response associated with serious<br />
morbidity. 3 Furthermore, scientific evidence has suggested that<br />
the neonate’s nervous system could retain long-term pain memory<br />
with the consequences of causing modification of the response to<br />
future painful stimulation. 4 It is also well recognized that a com -<br />
petent nociceptive system already exists in the fetal period, 5 which<br />
confirms that a nonanalgesic practice is no longer acceptable.<br />
Anesthesia-related morbidity and mortality is higher in<br />
infants, 6,7 particularly in the neonate, compared to older children<br />
and adults. These increased risks are significantly reduced with<br />
proper training in pediatric anesthesia and regular exposure to<br />
pediatric anesthesia practice necessary to maintain skills 8,9 in<br />
neonatal care. These epidemiologic data have initiated an impor -<br />
tant debate and the regulation authorities of Great Britain cur -<br />
rently recommend transfer of all children ≤3 years of age requiring<br />
emergency surgical procedure to larger centers with adequate<br />
pediatric anesthesia staffing and facilities. 10<br />
Effects of Anesthetic Agents on the<br />
Premature and Neonatal Brain<br />
Although adequate anesthesia is to be considered mandatory for<br />
premature infants and neonates, recent studies have also provided<br />
evidence that being subjected to anesthesia at this early age may<br />
not be without important consequences to the child.<br />
The seminal publications by Ikonomidou 11 and Jevtovic-<br />
Todorovic, 12 showing a significant increase of apoptotic cell death<br />
by various anesthetic agents in the young rat, has sparked a vivid<br />
debate whether anesthesia in early life can be detrimental to the<br />
developing central nervous system. The increased apoptosis seen<br />
following the use of certain anaesthetics in rodents have also been<br />
linked to later developmental and cognitive deficits in the animals,<br />
showing that the increase in the normal apoptotic sequence of the<br />
neonate can have significant negative long-term effects.<br />
The main agents that have been targeted are N-methyl-Daspartic<br />
acid (NMDA) antagonists (e.g., ketamine) and -amino -<br />
butyric acid (GABA)-mimetic compounds (e.g., benzodiazepines,<br />
barbiturates, volatile agents), but nitrous oxide also has a potential<br />
for increased apoptosis if combined with other agents. It is clear<br />
that combinations of these drugs appear more potent with regards<br />
to the ability to induce apoptotic cell death than use of a single<br />
agent. The period of risk is associated with what is generally called<br />
the period of synaptogenesis or “brain-growth spurt.” Thus,<br />
interference by anesthetic drugs during this delicate developmen -<br />
tal period may lead to altered and maybe dysfunctional synaptic<br />
“hard wiring” of the maturing brain.<br />
Although the findings in animal studies are striking, there are<br />
a large number of problems with trying to translate this to the<br />
human preterm or neonate (e.g., doses, duration of exposure,<br />
species differences, nutritional issues). Another major issue in this<br />
context is the fact that neonatal surgery most often cannot be<br />
delayed until the child is out of the potential risk period without<br />
adding other risks and that previous research has clearly shown<br />
that insufficient anaesthesia and analgesia in neonates and prema -<br />
ture infants is associated with substantial harm, including negative<br />
long-term effects.<br />
The exposure to different anaesthetics during neonatal anaes -<br />
thesia is usually limited to a few hours and it is difficult to judge<br />
to what extent such limited exposure time may affect apoptotic<br />
cell death in the human neonate. Although the risks associated<br />
with neonatal anaesthesia should not be neglected due to this time<br />
limitation, it may possibly be seen as slightly less important<br />
compared to the prolonged exposure to very similar combinations<br />
of sedative and analgesic agents during the sometimes prolonged<br />
postoperative neonatal intensive care unit (NICU) stay (days–<br />
weeks).<br />
Despite the accumulating animal data, it is not currently pos -<br />
sible to know if one anaesthetic is better or worse than another<br />
and, thus, no recommendations have so far been issued. However,<br />
as stated above, there is absolute consensus that premature and<br />
neonatal infants always should receive adequate anaesthesia and<br />
postoperative analgesia. An approach based on opioids, regional<br />
anaesthesia, and a low concentration of volatile agent (e.g., 1%<br />
sevoflurane in oxygen-air) to counteract potential awareness does,<br />
in the author’s opinion, appear as a reasonable strategy, but<br />
adequate data to support this concept are currently lacking.<br />
Significant scientific effort is currently put into this field of<br />
research, both from individual research groups as well as from
1438 PART 5 ■ Anesthetic, Surgical, and Interventional Procedures: Considerations<br />
national bodies, for example, the U.S. Food and Drug Administra -<br />
tion (FDA), and more information will most likely be available<br />
within the next 5 to 10 years. For more in-depth information re -<br />
garding these issues the reader is referred to the reviews by<br />
Mellon 13 and Anand. 14<br />
This chapter aims at providing a comprehensive review of the<br />
theoretical aspects of neonatal anesthesia and at giving practical<br />
guidelines for the most frequently performed surgical interven -<br />
tions during the neonatal period.<br />
PHYSIOLOGIC PARTICULARITIES<br />
PRONE TO INFLUENCE<br />
ANESTHESIA MANAGEMENT<br />
Development of the Nociceptive<br />
System and Stress Response<br />
All structural components of the nociceptive system are already<br />
developed at the end of the second trimester, 15 as described in<br />
<strong>Chapter</strong> 4. In a pivotal study, Giannakoulopoulos and coworkers<br />
verified a competent stress reaction as well as behavioral<br />
signs indicative of a fully functional nociceptive system even in<br />
the fetus. 16 Two different groups of subjects were studied during<br />
fetal exchange transfusion due to fetomaternal blood group<br />
incom patibility. To achieve fetal venous access, the umbilical<br />
vein is usually punctured close to the insertion of the umbilical<br />
cord in the placenta under ultrasonographic guidance. Since the<br />
umbilical cord is uninnervated, such a procedure should not be<br />
associated with any pain or stress reaction. However, due to<br />
anatomic factors, this approach for fetal venous access is not<br />
always feasible, and in such cases the venous system of the fetus<br />
has to be accessed by puncture of the intrahepatic vein. This<br />
method, thus, involves perforation of the skin, muscle, and liver<br />
capsule, and if the fetus does have functionally intact stress and<br />
nociceptive systems, such a puncture would be associated with<br />
measurable signs of a neuro endocrine stress reaction as well as<br />
behavioral signs indicative of a pain reaction. As could be<br />
expected, puncture and exchange transfusion performed via<br />
the umbilical cord was not associated with any measurable<br />
stress reaction or behavioral signs of pain. However, in fetuses<br />
undergoing intrahepatic vein cannulation and transfusion, a<br />
distinct stress reaction could be observed (increase in cortisol and<br />
-endorphin). The stress response was also found to correlate with<br />
the duration of the needling and transfusion procedure in these<br />
fetuses. Moreover, during puncture of the abdominal wall and the<br />
liver capsule, the babies were found to start breathing rapidly<br />
(as well as starting to move the extremities vigorously). No<br />
such behavioral reactions were noted during puncture of the<br />
umbilical cord and the transfusion process itself did not induce<br />
any stress response.<br />
Neonatal pain is capable of producing a “pain memory,” either<br />
as a result of plasticity changes within the nervous system itself or<br />
due to a psychological process. A number of studies performed in<br />
neonatal rodents have investigated the maturational changes of<br />
the opioid system and the descending pain inhibitory control<br />
pathways. The main differences between the neonatal and adult<br />
rodent are summarized in Table <strong>86</strong>–1. Although the current<br />
knowledge is almost exclusively based on the neonatal rodent<br />
studies, it is reasonable to assume the conditions may be similar in<br />
the human neonate.<br />
TABLE <strong>86</strong>-1. Developmental Changes in the Nociceptive<br />
System of the Fetal and Newborn Rat<br />
1. High density of -receptors both in superficial and deeper<br />
layers of the gray matter in the spinal cord. A more adult<br />
localization of -receptors to the superficial layers of the<br />
dorsal horn are not achieved until postnatal day 14–28<br />
(P14–28) (approximately equal to a human toddler). 28<br />
2. Nociceptive A-fiber input predominates over C-fiber input<br />
in the neonatal period. 29<br />
3. Descending inhibitory control pathways from the brainstem<br />
to the spinal cord are not functional in neonates or during<br />
early infancy. 30<br />
4. Predominance of enkephalin over endorphin in the initial<br />
perinatal period. 31<br />
5. Enhanced intracellular calcium-release in response to<br />
NMDA (N-methyl-D-aspartate) stimulation compared to<br />
adults. 32<br />
6. A 40-fold increase in efficacy of morphine from P3<br />
(approx. human preterm baby) to P14 (approximately<br />
late infancy). 33<br />
Very interesting new knowledge currently exists regarding the<br />
growth factor effects of endogenous opioids in relation to normal<br />
neuronal development during the neonatal period. In rat models,<br />
endogenous opioids have, through a receptor mediated process,<br />
been found to have an inhibitory influence on dendrite and spine<br />
elaboration in 10-day-old rodents. 17 Suppression of astrocyte<br />
growth has also been shown in vitro following met-enkephalin<br />
administration. 18 Furthermore, morphine administration has been<br />
found to cause inhibition of DNA synthesis in the neonatal rat<br />
brain but not in older animals. This effect could be blocked by<br />
pretreatment with naloxone once again indicating receptor me -<br />
diated mechanisms. 19<br />
Despite the apparently normal development of most neonates<br />
following neonatal surgery, including significant postoperative<br />
administration of morphine or other opioids, further knowledge<br />
is required to delineate the potential problem of interference with<br />
normal neuronal development of the neonate if exposed to high<br />
doses of exogenous opioids. 20 A number of studies in preterm and<br />
term human babies reported the presence of a fully competent<br />
neuroendocrine stress reaction in response to surgical stimula -<br />
tion. 21,22 The neuroendocrine stress response has been found to be<br />
correlated with degree of surgical trauma 23 and can be beneficially<br />
modified by adequate anesthesia and analgesia. 24 The attenuation<br />
of the neuroendocrine stress response in both preterm and<br />
neonates by proper analgesia has been found to reduce morbidity.<br />
In the specific setting of neonatal cardiac surgery, high-dose<br />
sufentanil anesthesia and postoperative analgesia (n 30) have<br />
been shown to reduce the incidence of sepsis/necrotizing entero -<br />
colitis, disseminated intravascular coagulation, and metabolic<br />
acidosis by 20 to 25 percent 24 compared with a halothanemor<br />
phine based anesthetic technique (n 15). This study was<br />
also prematurely ended because of apparently lower mortality<br />
figures in the sufentanil group (0%) compared to the previous<br />
halothane-morphine based anesthetic technique (27%). 24 The<br />
reader should bear the small number of patients enrolled in this<br />
study in mind, but these results clearly point to a more favorable<br />
outcome for sick children if adequate intra- and postoperative<br />
analgesia is provided.
CHAPTER <strong>86</strong> ■ Management of the Neonate: Anesthetic Considerations 1439<br />
Cardiovascular System<br />
The physiology and main developmental stages of the cardiovas -<br />
cular systems are discussed in <strong>Chapter</strong> 3.<br />
Transitional Circulatory Adaptation<br />
Following birth, the circulation changes from a fetal parallel<br />
pattern characterized by both ventricle pumping the majority of<br />
their output into the systemic circulation (pulmonary blood flow<br />
10% of combined ventricular output 25 ) to an extrauterine series<br />
pattern with the right and left ventricles assuming responsibility<br />
for the pulmonary and the systemic circulations, respectively (see<br />
<strong>Chapter</strong> 3). The three embryological shunts close during the<br />
immediate postnatal period. The placenta circulation and the flow<br />
through the ductus venosus cease when the umbilical cord is<br />
clamped at birth. The foramen ovale will close within 1 to 2 hours<br />
after delivery, as the pressure in the left atrium will surpass that of<br />
the right atrium due to the rapid decrease in pulmonary pressures<br />
associated with initiation of breathing and the subsequent aeration<br />
of the lung. The foramen ovale will remain patent during the<br />
neonatal period and anatomic closure will often not take place<br />
until 1 year of age. Anatomic closure will not take place in all<br />
individuals and a patent foramen ovale can be present in up to 10<br />
to 20% of the adult population. The ductus arteriosus will start to<br />
close approximately 10 to 15 hours following delivery and is<br />
usually physiologically closed by the 2nd day of life. However,<br />
permanent anatomic closure with formation of the ligamentum<br />
arteriosus is not completed until about 3 weeks postnatally. During<br />
this period the ductus arteriosus might reopen if exposed to<br />
unfavorable neuroendocrine mediators or increasing pulmonary<br />
pressures. The main factors that modulate pulmonary vascular<br />
resistance and neonatal pulmonary resistance at birth and during<br />
the first days of life are summarized in Table <strong>86</strong>–2.<br />
During certain circumstances in the early neonatal period, a<br />
relapse into the fetal circulatory pattern most often occurs due to<br />
pulmonary vasospasm with resulting pulmonary hypertension but<br />
can also be a consequence of, e.g., severe hypoxia or hypercarbia.<br />
Pulmonary vasospasm resulting in persistent pulmonary hyper -<br />
tension of the newborn (PPHN) is characterized by profound<br />
hypoxia due to right-to-left shunting through the fetal extrapul -<br />
monary shunts combined with right ventricular strain and<br />
circulatory compromise. A number of different neonatal condi -<br />
tions predispose to the development of PPHN, for example, con -<br />
genital diaphragmatic hernia, meconium aspiration syndrome,<br />
asphyxia, hypoxia and sepsis, all of which can coincide with the<br />
need for neonatal surgical intervention (Table <strong>86</strong>–3). Thus, the<br />
neonatal anesthesiologist needs to be familiar with the pathophy -<br />
siology of PPHN, its diagnosis, and treatment. Conventional<br />
treatment consists of tracheal intubation and mechanical ven -<br />
tilation, induction of alkalosis by attempted hyperventilation, and<br />
acidosis correction, analgosedation, muscle paralysis, volume<br />
replacement, and inotropic/pressor support (dopamine, norepine<br />
phrine). 26<br />
More recent treatments include selective pulmonary vasodila<br />
tation by means of inhaled nitric oxide (iNO) or inhalation of<br />
nebulized prostacyclin and the use of high-frequency oscillatory<br />
ventilation. 27 Regarding iNO, the effective dose range appears to be<br />
within the 1 to 30 ppm dose range, although doses up to 80 ppm<br />
might be attempted in severe cases for brief periods of time. 28 Side<br />
effects of the treatment are few and mainly limited to the risk of<br />
methemoglobin formation and minor prolongation of bleeding<br />
time. The most dangerous complication of iNO treatment is severe<br />
rebound pulmonary hypertension in association with abrupt<br />
discontinuation of the iNO therapy either accidentally or during<br />
deliberate weaning. The risk of severe rebound necessitates the<br />
immediate option to reinstate therapy and to be able to handle an<br />
accidental delivery device malfunction situation; a back-up system<br />
needs to be available at the bedside. Since NO and especially<br />
concomitant and unavoidable nitrogen dioxide (NO 2<br />
) exposure at<br />
higher concentrations (100 ppm and 2 ppm, respectively) can<br />
be toxic it is imperative to use an approved delivery device and<br />
also to measure continuously the NO and NO 2<br />
levels in the in -<br />
spired gases. The anesthesiologist must be prepared to conduct<br />
the anesthetic without interrupting these new and effective treat -<br />
ments. If the anesthesiologist is not comfortable in this situation,<br />
help should be sought from an experienced neonatologist.<br />
TABLE <strong>86</strong>-2. Factors That Modulate Pulmonary Vascular Resistance in the Near-Term and Term Transitional and<br />
Neonatal Pulmonary Circulation<br />
Endogenous mediators<br />
and mechanisms<br />
Mechanical factors<br />
Lowers Pulmonary Vascular Resistance<br />
Oxygen, nitric oxide<br />
PGI2, E2, D2<br />
Adenosine, ATP, magnesium<br />
Bradykinin, atrial natriuretic factor<br />
Alkalosis, K channel activation<br />
Histamine, acetylcholine<br />
Vagal nerve stimulation<br />
b-Adrenergic stimulation<br />
Lung inflation<br />
Vascular cell structural changes<br />
Interstitial fluid and pressure changes<br />
Shear stress<br />
PGI2, E2, D2 prostaglandins I2, E2, D2; ATP adenosine triphosphate; PGF2a prostaglandin F2a.<br />
Increases Pulmonary Vascular Resistance<br />
Hypoxia, acidosis<br />
Endothelin-1, leukotrienes, thromboxanes<br />
Platelet activating factor<br />
Ca channel activation<br />
a-Adrenergic stimulation<br />
PGF2a<br />
Overinflation or underinflation<br />
Excessive muscularization, vascular remodeling<br />
Altered mechanical properties of smooth muscle<br />
Pulmonary hypoplasia, pulmonary thromboemboli<br />
Alveolar capillary dysplasia<br />
Main pulmonary artery distention<br />
Ventricular dysfunction, venous hypertension
1440 PART 5 ■ Anesthetic, Surgical, and Interventional Procedures: Considerations<br />
TABLE <strong>86</strong>-3. Disorders Frequently Associated With Persistent Neonatal Pulmonary Hypertension<br />
Diagnosis Symptoms and Signs Investigations Treatment<br />
Congenital diaphragmatic<br />
hernia<br />
Meconium aspiration<br />
syndrome<br />
Birth asphyxia<br />
Septicemia<br />
Respiratory distress<br />
Displaced cardiac sounds, usually<br />
shifted to the right<br />
No breath sounds over one<br />
hemithorax, usually left side<br />
Scaphoid abdomen<br />
“Honeymoon” period<br />
History of intrauterine fetal<br />
distress<br />
Meconium stained amniotic fluid<br />
Meconium in pharynx and<br />
trachea<br />
Respiratory distress<br />
Chest wall retractions<br />
History of intrauterine fetal<br />
distress or difficult delivery<br />
Low APGAR scores<br />
Hyper- or hypotonicity<br />
Seizures<br />
Cardiovascular compromise<br />
Poor peripheral circulation<br />
Poor urine output<br />
Respiratory distress not always<br />
present<br />
Hypo- or hyperthermia<br />
Hypotonicity<br />
Cardiovascular compromise with<br />
poor peripheral circulation<br />
Poor urine output<br />
Respiratory distress not always<br />
present initially<br />
Chest x-ray diagnostic<br />
Meconium present at tracheobronchial<br />
suctioning<br />
Chest X-ray shows pachy<br />
bilateral infiltrates<br />
Cardiac and cerebral<br />
ultrasonography<br />
Cerebral function monitoring<br />
Elevation of liver enzymes<br />
Computed tomography on day<br />
3 for prognostic reasons<br />
C-reactive protein<br />
White blood cell count<br />
Bacterial cultures<br />
Chest x-ray may show fine<br />
granular infiltrates<br />
iNO inhaled nitrous oxide; HFOV high frequency oscillatory ventilation; ECMO extracorporeal membrane oxygenation.<br />
In more severe cases:<br />
Intubation<br />
Mechanical ventilation<br />
Analgo-sedation<br />
Vigorous acid-base correction<br />
Surfactant replacement<br />
iNO, HFOV, ECMO<br />
No emergency surgery!<br />
If possible thorough tracheobron -<br />
chial suctioning<br />
Possible indication for partial liquid<br />
ventilation<br />
(For further treatment please see<br />
Congenital diaphragmatic hernia)<br />
Endotracheal intubation<br />
Mechanical ventilation<br />
Inotropic support<br />
Diuretics<br />
Acid-base correction<br />
Pharmacologic seizure control<br />
Avoidance of hyperglycemia<br />
Adequate antibiotics<br />
Respiratory support as needed<br />
Volume replacement Inotropic<br />
support<br />
Diuretics<br />
Myocardial Function<br />
The neonatal cardiac myocyte contains more noncontractile ele -<br />
ments, has a disorganized intracellular arrangement of the con -<br />
tractile proteins, and its shape is less elongated than in the adult. 29<br />
This leads to a reduced capability of the neonatal myocardium to<br />
generate force. 30 The sarcoplasmatic reticulum and the T-tubular<br />
system are also immature, which leads to an increased dependence<br />
on extracellular calcium for contraction. 31 Developmental changes<br />
both in the cytoskeleton and the extracellular matrix make the<br />
neonatal myocardium less compliant, and both early diastolic<br />
relaxation and late diastolic filling are reduced compared to the<br />
adult. 32,33 While the overall number of ventricular myocytes is still<br />
increasing (hyperplasia) during the neonatal period, after that<br />
period further increase in ventricular mass depends only on<br />
physiologic hypertrophy. 34 Compared to adults, the neonatal<br />
myocardium is metabolically less effective in handling fatty acids,<br />
which makes carbohydrates and lactate its primary energy<br />
substrates. 35 It is also more resistant to hypoxia, 36 which might be<br />
explained by increased myocardial glycogen stores and higher rates<br />
of anaerobic glycolysis in the neonatal myocardium com pared to<br />
the adult. Better myocardial performance is also observed following<br />
an ischemic insult in the immature heart, 37 something which might<br />
be explained by less pronounced increase in resting tension during<br />
the ischemic insult compared to the adult myocar dium, thus,<br />
resulting in better preservation of myocardial energy stores.<br />
The parasympathetic innervation of the neonatal heart is<br />
considered to be more mature compared to the sympathetic<br />
system 38 and the expression of cholinergic receptors is maximal at<br />
birth and remains high during the neonatal period. 39 The time<br />
course for the maturation of the sympathetic nervous system is<br />
associated with great interindividual variability. At 3 months of<br />
age, the sympathetic nervous system can often be regarded as<br />
functionally developed but final maturation can be delayed until<br />
1 year of age in certain individuals. The adrenergic plexus system<br />
is less developed, 40 which might explain the pronounced response<br />
to norepinephrine simulating denervation supersensitivity. 41<br />
Circulating catecholamines are, thus, relatively more important<br />
for inotropic and chronotropic function in the neonate. The b-<br />
adrenergic receptors and the adenylate cyclase system are well<br />
developed in the neonate 38 but the coupling between the two<br />
might be reduced since direct activation of adenylate cyclase will<br />
produce a larger increase in inotropic response compared to<br />
b-receptor stimulation. 42 Birth is associated with very high levels<br />
of circulating catecholamine levels, 43 which most likely results in
CHAPTER <strong>86</strong> ■ Management of the Neonate: Anesthetic Considerations 1441<br />
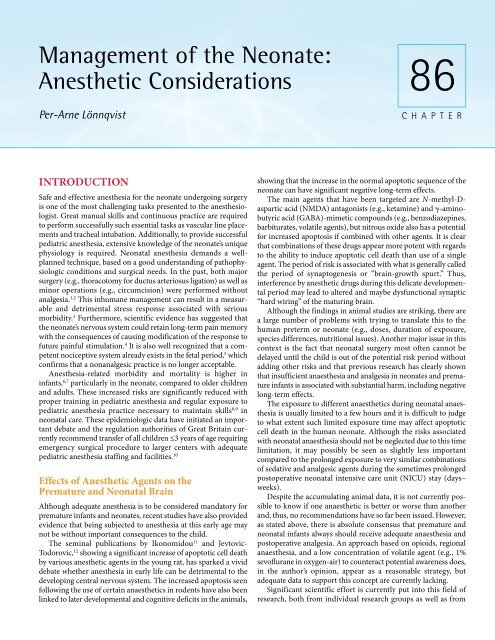
Figure <strong>86</strong>-1. Progressive reduction in cardiac output during<br />
the first days of life. LVO (n 16), SV(n 16), and ICBFV<br />
(a .20) in the first 72 h after birth in healthy term infants. Mean<br />
and 1 SD. Reproduced from Winberg 61 with permission.<br />
near maximal adrenergic stimulation of the myocardium imme -<br />
diately after parturition. During this time, the functional reserve<br />
of the myocardium is limited and the myocardium responds<br />
poorly to further increases in demand. 44 During the first days of<br />
life, there is a progressive reduction in cardiac output (Figure<br />
<strong>86</strong>–1) leading to an increase in functional reserve and an increased<br />
response to inotropic stimulation. 45<br />
Reactions to Changes in Preload, Afterload,<br />
Inotropy, and Heart Rate<br />
Recent scientific evidence has demonstrated that cardiac output<br />
is not unaffected by changes in preload. 46–48 A direct relationship<br />
between neonatal stroke volume and cardiac output exists already<br />
immediately following birth, whereas changes in heart rate does<br />
not appear to have the major influence on cardiac output in this<br />
setting as previously believed (Figure <strong>86</strong>–2). 46 The increase in<br />
stroke volume in response to volume loading exists already<br />
immediately after birth but will be more prominent towards the<br />
end of the neonatal period. 45 The inflection point of the Frank–<br />
Starling relationship might be at a lower filling pressure (8 mmHg)<br />
compared to adults (12–15 mmHg). Because of the limited ability<br />
to generate force by the neonatal myocardium and the reduced<br />
compliance the neonatal heart tolerates increases in afterload<br />
poorly 46,49 (Figure <strong>86</strong>–3). This is most pronounced regarding the<br />
right ventricle but applies to the left ventricle as well. Right<br />
ventricular strain often cause leftward interventricular septal shift,<br />
which can limit the filling of the left ventricle. 50 With the possible<br />
exception of the immediate period following parturition, the<br />
neonatal myocardium responds to inotropic stimulation with an<br />
increase in cardiac output. However, the response is usually less<br />
pronounced compared to adults. The choice of the optimum<br />
inotrope can be debated but, according to clinical experience,<br />
dopamine, dobutamine, epinephrine, isoproterenol, and norepine -<br />
phrine all increase cardiac output. Choosing agents with less<br />
effects on afterload might have a theoretical advantage since the<br />
neonatal myocardium tolerates increases in afterload poorly. Heart<br />
rate has previously been perceived as the major factor affecting<br />
cardiac output in the neonate. This is, as described above, only<br />
Figure <strong>86</strong>-2. Left ventricular stroke volume (SV) versus left<br />
ventricular output (LVO) in 16 term infants during the first 72 h<br />
after birth.<br />
partially true. 46 Relative bradycardia obviously reduces cardiac<br />
output, but increases in heart rate above approximately 180 to 190<br />
bpm do not cause an increase in output, since higher rates limit<br />
diastolic filling time; hence, the stroke volume is reduced. Even at<br />
heart rates below 180 bpm, the supposed tight relationship<br />
between heart rate and cardiac output can be questioned in the<br />
early neonatal period (Figure <strong>86</strong>–4). The optimal heart rate with<br />
regard to optimizing the hemodynamic situation will of course<br />
Figure <strong>86</strong>-3. Left ventricular stroke volume (SV) versus systemic<br />
vascular resistance (SVR) in 16 term infants during the<br />
first 72 h after birth.
1442 PART 5 ■ Anesthetic, Surgical, and Interventional Procedures: Considerations<br />
Figure <strong>86</strong>-4. Heart rate (HR) versus left ventricular output<br />
(LVO) in 16 term infants during the first 72 hours after birth.<br />
vary between patients. After correcting and optimizing filling<br />
pressures, heart rates in the range of 120 to 180 bpm should be<br />
aimed for as a general rule.<br />
Changes in Heart Rate and Blood Pressure<br />
During the Neonatal Period<br />
The heart rate decreases and the blood pressure increases both in<br />
term neonates 47 and preterm infants 48 during the first 3 postnatal<br />
days (Figure <strong>86</strong>–5). Adequate knowledge regarding the normal<br />
levels for these crucial parameters must be known to enable the<br />
pediatric anesthesiologist to adjust properly the depth of anesthesia<br />
in the neonate. 51 The main features of the neonatal circulation and<br />
myocardial functions are summarized in Table <strong>86</strong>–4.<br />
Ventilatory Function and Control<br />
Control of Breathing<br />
During the neonatal period, control of breathing differs in some<br />
important aspects from what is normally seen in the older child or<br />
the adult. Neonates respond to hypercapnia (combined with hy -<br />
poxia) with an increase in ventilation but less than older subjects,<br />
as evidenced by a less steep CO 2<br />
response curve. 52 The ventilatory<br />
response to hypercapnia gradually matures both in relation to<br />
increasing gestational age and postnatal age. 52 In adults, hypoxia<br />
causes an increase in ventilation, whereas in the neonate hypoxia<br />
only briefly increases ventilation. This initial increase in ventila -<br />
tion is later followed by a sustained depression of ventilation. 53 A<br />
periodic breathing pattern is present in both preterm and term<br />
babies with an inverse relationship to gestational age. This ten -<br />
dency for periodic breathing decreases markedly following 44<br />
weeks postconceptual age but can be seen up to 1 year of age. 54<br />
The respiratory drive of the neonate is a complex interplay be -<br />
tween a number of various factors. Furthermore, the relative im -<br />
portance of different stimuli changes during the neonatal period.<br />
Thus, suprapontine drive dominates immediately after birth,<br />
together with the mechanosensory driving mechanism. The impor -<br />
tance of these systems, however, diminishes later on and the<br />
Figure <strong>86</strong>-5. Mean (SD) left ventricular output, stroke volume,<br />
heart rate, and arterial blood pressure during postnatal circulatory<br />
adaptation in 16 healthy infants born at full term.<br />
chemoreceptor drive takes over as the most important system for<br />
maintaining the respiratory drive (Figure <strong>86</strong>–6). 55<br />
Anesthetic Effects on Control of Breathing<br />
Apart from the well-known depressing effects of most anesthetics<br />
on respiration in both neonates and older subjects a specific<br />
situation exists in newborns and especially in ex-premature infants.<br />
General anesthesia increases the risk for postoperative apnea<br />
in this patient category until the age of 44 to 60 post concept-<br />
TABLE <strong>86</strong>-4. Main Characteristics of the Neonatal<br />
Circulation and Myocardial Functions<br />
1. Myocardium less able to generate force.<br />
2. Myocardium relatively noncompliant.<br />
3. Myocardium more dependent on extracellular calcium.<br />
4. Myocardium more resistant to hypoxia and ischemia, at<br />
least immediately following birth.<br />
5. Limited functional reserve early in the neonatal period.<br />
6. Balance in favor of the parasympathetic nervous system.<br />
7. Changes in preload will significantly affect stroke volume<br />
and cardiac output.<br />
8. Tolerates increases in afterload poorly.<br />
9. Responds to inotropic support although less than the adult.<br />
10. Cardiac output less heart rate dependent than previously<br />
believed.
CHAPTER <strong>86</strong> ■ Management of the Neonate: Anesthetic Considerations 1443<br />
Figure <strong>86</strong>-6. Schematic representation of the relative importance<br />
of different respiratory drive mechanisms after birth.<br />
Cooling of the skin and the increased arousal induced by labor<br />
and delivery are important for initiation of breathing at birth.<br />
Mechanosensory information constitutes a major drive to sustain<br />
regular and efficient breathing during the first few weeks of<br />
life. The importance of the peripheral chemoreceptor drive, as<br />
well as of the integration and modulation of various respiratory<br />
and nonrespiratory stimuli, increases after the newborn period.<br />
(Figure based on an original concept of P. Johnson, Oxford<br />
University, 1984.)<br />
ual weeks. 56,57 Anemia further increases this risk (Hct 30%) 57<br />
(Figure <strong>86</strong>–7). Even after 56 postconceptual weeks, the risk for<br />
postoperative apnea can still be approximately 1%. 80 Since the risk<br />
for this potentially life-threatening event is above what is usually<br />
accepted in anesthetic practice (rates for significant morbidity and<br />
mortality in the range of 1/10.000 to 1/100.000) 58 these patients<br />
should be monitored in hospital for at least 12 to 24 hours after<br />
surgery in an environment with adequate staffing and resuscitation<br />
skills (i.e., recovery room, high dependency unit, neonatal ICU or<br />
step down unit). The minimum monitoring re quirements would<br />
be either an apnea monitor or preferably pulse oximetry.<br />
Figure <strong>86</strong>-7. Predicted probability of apnea by weeks postconceptual<br />
age for all three models: model I (solid line) all infants; model 2<br />
(irregular line) all nonanemic infants; and model 3 (broken line)<br />
~ patients who were not anemic and did not experience apnea in recovery<br />
room. The risk for apnea decreases markedly when patients with<br />
anemia (model 2) are eliminated, and the risk diminishes further if<br />
patients with apnea in recovery room (model 3) also are eliminated.<br />
Reproduced from Coté et al 83 with permission.<br />
Anesthetic Effects on Respiratory Mechanics<br />
General anesthesia will impair the function of almost all muscular<br />
components of the respiratory system. The genioglossus muscle,<br />
which is very important for airway patency, is disproportionally<br />
sensitive to the depressant effects of anesthetics leading to an<br />
increased risk for airway obstruction. 59 Reduced tonus of the<br />
intercostal muscles will reduce the stability of the thoracic wall,<br />
increasing the risk for thoracoabdominal asynchrony resulting in<br />
less effective ventilation. 60 Although the diaphragm is more resis -<br />
tant to anesthetics compared to the genioglossus and intercostal<br />
muscle some interference with normal function still occurs. 61 The<br />
above-mentioned actions of anesthetics on the respiratory mus -<br />
cles, together with some other factors, will substantially increase<br />
the risk for detrimental reductions of functional residual capacity<br />
(FRC). Application of positive end-expiratory pressure (5–6 cm<br />
H 2<br />
O) will prevent the adverse effects on FRC and compliance in<br />
neonates and infants. 62 The main particularities of the respiratory<br />
control and respiratory mechanics in the neonate are summarized<br />
in Table <strong>86</strong>–5.<br />
Hepatic Function<br />
The maturation process of the liver is a very complex interplay<br />
between different enzyme pathways, isoenzyme patterns,<br />
avail ability of cofactors, hepatic blood flow, and extraction<br />
characteris tics of the hepatocyte (see <strong>Chapter</strong> 7). During fetal life<br />
TABLE <strong>86</strong>-5. Main Particularities of Neonatal Respiratory<br />
Control and Respiratory Mechanics<br />
1. Hypercarbia results in stimulation of respiration but to a<br />
lesser extent than in the adult.<br />
2. Hypoxia causes a transient increase in ventilation followed<br />
by a sustained respiratory depression.<br />
3. Neonates, and especially ex-premature infants, have a<br />
tendency for periodic breathing which is accentuated by<br />
anesthetics. Thus, these infants are at increased risk of<br />
postoperative apnea until approximately 60 weeks<br />
postconceptual age.<br />
4. The respiratory driving mechanisms are multifactorial<br />
during the neonatal period.<br />
5. Different types of afferent input and reflexes from the lung<br />
are important in respiratory control of the neonate.<br />
6. Newborns have higher oxygen consumption compared to<br />
older subjects. Tidal volume is relatively similar per kilo<br />
body weight but respiratory rates are higher.<br />
7. Lung compliance is lower whereas the chest wall<br />
compliance is higher compared to adults.<br />
8. The neonate is at increased risk of reduction of FRC and<br />
development of atelectasis. This can be counteracted by<br />
application of a modest PEEP.<br />
9. Anesthesia will negatively affect all respiratory muscles in<br />
the neonate, particularly the genioglossus and intercostal<br />
muscles. This leads to increased risk of airway obstruction<br />
and thoracoabdominal asynchrony.<br />
10. The diaphragm of the neonate is the dominating respiratory<br />
muscle. However, due to the relatively lower content of<br />
oxidative type I fibers the diaphragm of the neonate is<br />
susceptible to fatigue if subjected to increased ventilatory<br />
demands.
1444 PART 5 ■ Anesthetic, Surgical, and Interventional Procedures: Considerations<br />
TABLE <strong>86</strong>-6. Sulfation and Glucuronidation of<br />
Acetaminophen (AA) in Human Neonates and Adults<br />
(Formation Rate Constants, HR-1)<br />
Age Range AA-Sulfate AA-Glucuronide Sulfate/Glucuronide<br />
Neonates 0.099 0.025 4<br />
Adults 0.075 0.170 0.4<br />
Adapted from Levy et al. 96<br />
the liver is exposed to a very high blood flow due to the placenta<br />
circulation, which causes hepatic accumulation of anesthetic<br />
drugs. Addition ally, maternal metabolism is largely responsible<br />
for biotransfor mation and elimination of drugs, a pathway no<br />
longer available after birth. Elimination of many drugs such as<br />
diazepam is con siderably prolonged in the neonate. 63 The different<br />
metabolic pathways of the neonate mature at different rates.<br />
Conjugation by sulfation and acetylation are relatively mature,<br />
whereas glucuroni dation and conjugation with glutathione and<br />
glycine are less well developed. Whereas acetaminophen mainly<br />
undergoes glucuroni dation in the adult, it mainly undergoes<br />
sulfation in the neonate 64 (Table <strong>86</strong>–6).<br />
A number of drugs display prolonged elimination half-lives in<br />
neonates compared to adults when they mainly undergo hepatic<br />
biotransformation (e.g., morphine). 65 Other factors responsible<br />
for the prolongation of elimination half-lives are the increased<br />
volume of distribution and the very limited, thus easily saturated,<br />
enzymatic capacity of the neonate. In the latter instance, elimina -<br />
tion may become virtually nil with increasing dosage. 66 On the<br />
other hand, certain drugs do not undergo prolonged elimination<br />
in neonates. The elimination rate of lidocaine does not signifi -<br />
cantly differ from that in adults because its clearance depends less<br />
on hepatic metabolism than on liver blood flow, which is fairly<br />
similar in neonates and adults. 67 The immature hepatic meta -<br />
bolism of certain drugs is to some extent ameliorated by a larger<br />
fraction of the drug being excreted unchanged. The urinary<br />
excretion of unchanged caffeine represents only 1% of the given<br />
dose in adults but may be as high as 85% in the neonate. 68<br />
The transition to extrauterine life as outlined above causes<br />
significant changes in hepatic function. With the cessation of the<br />
placental circulation the neonate’s liver faces a situation of reduced<br />
blood flow and oxygenation while becoming solely responsible for<br />
drug metabolism. However, parturition in itself might enhance<br />
the maturation of hepatic drug metabolism. Increased glucocorti -<br />
coid levels might beneficially affect different enzyme systems 69,70<br />
and the drastic decrease in plasma levels of the inhibitory maternal<br />
hormones (e.g., pregnenolone and progesterone 71 ) helps, increas -<br />
ing the biotransformation capacity of the liver. Glucocorticoid<br />
levels increase during late gestation and will influence the matura -<br />
tion of different hepatic enzyme systems. The normal increase in<br />
glucocorticoid levels during late gestation or treatment with<br />
steroids will affect the maturation of both the UDP-GT enzyme<br />
system 71 and certain P450-related activities. 72 Recent scientific<br />
evidence has suggested that exposure to drugs able to cause liver<br />
enzyme induction during the neonatal period could cause longlasting<br />
“imprinted” alteration of hepatic metabolism. 73 Short-term<br />
phenobarbital administration to neonatal rodents causes longterm<br />
enzymatic changes, still recognizable in adult rats compared<br />
to control animals. 74 Exposure to different drugs and other<br />
subs tances during the early neonatal period might influence<br />
the individual’s drug metabolic pattern later on in life. The<br />
implica tions of such neonatally induced hepatic changes in drug<br />
metabo lism or hepatic enzyme expression is unknown but raises<br />
both questions and concerns. Despite the lack of any obvious short<br />
term risks or side effects of medication administered in the<br />
neonatal period, further long-term follow-up studies are needed<br />
to show that this does not lead to unwanted consequences later on<br />
in adult life.<br />
Immature hepatic drug metabolism and elimination are likely<br />
to be responsible for the increased toxicity of a number of different<br />
drugs during early infancy. This is evidenced by lower LD 50<br />
values<br />
for many drugs in newly born versus adult animals. 75 This is not<br />
true, however, for some drugs such as acetaminophen, which<br />
undergoes reduced metabolism by the P-450 system with sub -<br />
sequent lower levels of the toxic reactive metabolite responsible<br />
for the hepatic toxicity; in this instance, neonates tolerate dosages<br />
of acetaminophen that would be hepatotoxic in adults. 76 The issue<br />
of the P-450 system in newborns is complex. Comparable total<br />
levels of the P-450 system are present before midgestation in<br />
human fetal liver 77 but the individual proportions of the various<br />
P-450 components differ considerably from adults and the<br />
maturation process differ between individual P-450 isoenzymes.<br />
Plasma protein binding of alkaline drugs, for example, synthetic<br />
opioids and local anesthetics, also differ substantially in neonates<br />
compared to adults. Higher free, unbound, and Pharmacologicly<br />
active fractions of these drugs will, thus be present in the neonate<br />
compared to adults. This in turn is due to much lower plasma levels<br />
of -1 acid glycoprotein, the protein mainly responsible for binding<br />
of such drugs, found in neonates. Alpha-1 acid glycoprotein levels<br />
will gradually increase during infancy and adult levels are reached<br />
at about 1 year of age. 78 Alpha-1 acid glycoprotein is one of the<br />
acute phase proteins and rapidly increasing levels of -1 acid gly -<br />
coprotein (0.1 g/L 24 h) will be seen in neonates following major<br />
activation of acute phase system (e.g., major surgery, sepsis or<br />
extracorporeal membrane oxygenation). The main issues of im -<br />
mature hepatic drug metabolism in the neonate is highly complex<br />
but have important clinical implications which are summarized in<br />
Table <strong>86</strong>–7.<br />
Renal Function<br />
Formation of new nephrons are completed about 34 to 35 weeks<br />
of gestation and further renal growth during late gestation,<br />
infancy, and adulthood is caused by enlargement of already<br />
existing structures 79 (see <strong>Chapter</strong> 5). Due to low systemic blood<br />
pressure and high renal vascular resistance, the kidneys only<br />
receive about 3% of the cardiac output during the last trimester, 80<br />
which sharply contrasts to the situation in adults where 25% of<br />
cardiac output passes through the kidneys. After birth, renal<br />
vascular resistance decreases (like pulmonary vascular resistance)<br />
and perfusion pressures increase resulting in a fairly rapid increase<br />
in renal blood flow. Effective renal plasma flow increase from<br />
83 mL/min/1.73 m 2 in the term neonate to 300 mL/min/1.73 m 2<br />
by 3 months of age. 81 In the neonate, the inner cortical and the<br />
medullary zones will receive relatively more of the renal blood<br />
flow compared to the mature kidney. Autoregulation of renal<br />
blood flow is functioning in the neonate but the lower shoulder<br />
of this pressure–flow relationship is set at a lower level (approxi -<br />
mately 50 mmHg). 82<br />
The glomerular filtration rate is low in the term infant, then<br />
double within the first 2 weeks of life 83 but does not reach adult<br />
levels until 2 years of age. 84 The tubular function is also reduced in
CHAPTER <strong>86</strong> ■ Management of the Neonate: Anesthetic Considerations 1445<br />
TABLE <strong>86</strong>-7. Clinical Implications of the Neonatal Immaturity of Hepatic and Renal Functions<br />
Hepatic Functions<br />
1. Dosing intervals and maintenance dosing needs to be<br />
adjusted.<br />
2. Administer small and repeated doses of intravenous drugs<br />
and titrate to effect in order not to cause an overdose or<br />
cause an unwanted prolongation of the effect of the drug.<br />
3. When possible monitor drug plasma levels (digoxin,<br />
antibiotics) to ensure effect and avoid overdose.<br />
4. Use drugs with a known neonatal pharmacokinetics<br />
(morphine, fentanyl, lidocaine, bupivacaine,<br />
acetaminophen) rather than new drugs which have not<br />
been evaluated properly in neonates.<br />
Renal Functions<br />
1. Neonates tolerate fluid restriction poorly. Keep fasting times<br />
to a minimum and start intravenous fluids early to avoid<br />
dehydration.<br />
2. Avoid excessive fluid administration.<br />
3. Restrict sodium administration in order not to cause<br />
hypernatremia.<br />
4. Outside the first 24 h after birth a urine output of less than<br />
1 mL/kg/h indicate hypovolemia or impeding renal failure.<br />
5. The neonate will respond to furosemide but larger doses<br />
compared to adults are needed in order to induce diuresis.<br />
6. Fluid requirements in a catabolic situation is substantially<br />
lower compared to a normal anabolic situation since the<br />
formation of new cells is very limited. A catabolic situation<br />
will also limit the neonate’s ability to excrete potassium and<br />
handle nitrogen waste products.<br />
7. The dosing of drugs which largely depend on renal excretion<br />
will have to be reduced and if possible the plasma<br />
concentrations should be closely checked in order to avoid<br />
accumulation and side effects<br />
the neonate with a decreased ability to concentrate the urine,<br />
which is the result of a relatively lower tonicity of the medullar<br />
interstitium. Fairly rapid maturation takes place during the<br />
neonatal period with an increased capacity of concentrating the<br />
urine from twice the osmolarity of plasma in the term baby to four<br />
times at 2 months of age. 85 The neonatal kidney has a welldeveloped<br />
system for sodium reabsorption <strong>86</strong> but a limited capacity<br />
for excreting a sodium load. 84 The neonate responds to furosemide<br />
administration with an increase in diuresis but larger doses<br />
(1 mg/kg) compared to adults are often needed.<br />
Urine output is low immediately after birth and the neonate<br />
might only void once during the first 24 hours. Diuresis then<br />
rapidly increases to a normal value of 1 to 2.5 mL/kg/h. Urine<br />
output less than 1 mL/kg/h indicate hypovolemia (most<br />
commonly) or impeding renal failure (usually due to asphyxia,<br />
hemorrhage, or septic shock). Growth, with the generation of new<br />
cells, reduces the excretory load on the renal system, since for -<br />
mation of new cells will require water, potassium and nitrogenmetabolites.<br />
The formation of new cells will take care of a<br />
considerable amount of the normal “waste products,” since water<br />
and potassium are sequestered to form new intracellular fluid and<br />
nitrogen metabolites are used to manufacture new membrane and<br />
intracellular proteins. Thus, growth has been termed “the third<br />
kidney” and will take care of a substantial part of the normal renal<br />
“waste load.” From a phylogenetic point of view it is also reason -<br />
able to assume that the neonates renal function is tailor-made to<br />
the normal requirements of the neonatal period and, thus, it would<br />
appear illogical if the newborn would be born with borderline<br />
renal failure. It should be remembered that the growth related<br />
unloading of the renal system will only be operational in an ana -<br />
bolic situation. In a catabolic situation, for example, the immediate<br />
postoperative period or during septicemia, no or very few new<br />
cells are being made, leaving the kidneys to handle the entire waste<br />
load. As a results of the above-mentioned renal considerations,<br />
the neonate cannot easily handle either fluid or sodium overload,<br />
and poorly tolerates fluid restriction since the concentration<br />
capacity is low. Meticulous attention must, thus, be focused on<br />
fluid and electrolyte balance during the neonatal period. The<br />
excretion of drugs too is affected, especially water soluble drugs<br />
which are dependent on renal excretion. The main clinical<br />
consequences of renal immaturity are summarized in Table <strong>86</strong>–7.<br />
Fluid and Electrolyte Balance, Caloric<br />
Requirement, and Blood Volume<br />
The total body water is substantially higher in the normal neonate<br />
(75%) compared to the adult (60%), and preterm babies have a<br />
still higher total body water content (see <strong>Chapter</strong> 5). Intra- and<br />
extracellular water represents 30 to 35% and 40 to 45% of the<br />
neonate’s total body weight, respectively. This considerable<br />
expansion of the extracellular fluid compartment is even more<br />
pronounced in the premature infant. 87 The blood volume of the<br />
normal neonate is approximately 85 mL/kg and up to 90 to 100<br />
mL/kg in preterm infants, with consistent interindividual vari -<br />
ability (60 to 130 mL/kg) due to possible placenta-to-neonate<br />
transfusion. Since plasma volume is relatively constant (50 mL/<br />
kg, 88 this variability depends mainly on hematocrit variability.<br />
Maintenance fluid requirements increase regularly during the first<br />
days (60, 80, 100, and 120 mL/kg/24h at day 1, 2, 3, and 4,<br />
respectively), then remain stable for the rest of the neonatal period<br />
(approximately 150 mL/kg/24 h). Caloric consumption is about<br />
100 to 120 kcal/kg/24h, half of which is required for basal<br />
metabolic needs and the remaining for growth. 89 Since caloric<br />
requirements are closely linked to fluid intake (it is virtually<br />
impossible to supply fluid with a caloric content of more than 1<br />
calorie per milliliter), pathological conditions where cell growth is<br />
halted (severe sepsis, postoperative period following major<br />
surgery), are at risk of metabolic overload as well as fluid retention<br />
if fluid and caloric supply are not adjusted. Daily electrolyte<br />
requirements for maintenance of electrolyte balance in the neonate<br />
are 2.5 mmol/kg, 2.0 mmol/kg, and 0.5 mmol/kg for sodium,<br />
potassium, and calcium, respectively. It should be remembered<br />
that a negative sodium balance negatively affects the growth of the<br />
neonate and can also affect growth later in life. 90 In most cases a
1446 PART 5 ■ Anesthetic, Surgical, and Interventional Procedures: Considerations<br />
maintenance infusion of 10% glucose containing 20 mmol/L<br />
sodium and 20 mmol/L potassium is usually satisfactory for the<br />
first 48 postnatal hours. If enteral feeding has not been established<br />
at this time, total parenteral nutrition should be started to ensure<br />
adequate nutrition of the baby.<br />
Temperature Control<br />
Thermoregulation in the neonate displays significant particulari -<br />
ties (see <strong>Chapter</strong> 10). Heat loss is favored by the comparatively<br />
larger body surface–to–body weight relationship, the poorly<br />
developed insulating subcutaneous fat layer, and the inability to<br />
use shivering thermogenesis. These limitations are partially<br />
compensated for by the unique thermal capacity for nonshivering<br />
thermogenesis (NST), which takes place in the neonate’s brown<br />
adipose tissue (see <strong>Chapter</strong> 10). Brown fat is mainly located be -<br />
tween the scapulae, around the blood vessels of the neck, in the<br />
axillae, in the mediastinum, and around the adrenal glands and<br />
kidneys. However, nonshivering thermogenesis is negatively<br />
influenced by the administration of volatile anesthetics. 91 Halo -<br />
thane, enflurane and isoflurane appear to cause an equipotent<br />
inhibition of thermogenesis. Concentrations of volatile anesthetics<br />
as low as 0.7% result in a 50% inhibition of the maximal thermal<br />
response 92 (Figure <strong>86</strong>–8). Recent data also indicate that a fentanylpropofol–based<br />
anesthetic will interfere with NST. 93 Inadvertent<br />
intraoperative hypothermia has been found to cause a number of<br />
negative effects in adults, such as impaired immunologic function,<br />
increased rate of wound infections, negative influences on hepatic<br />
and renal function, and reduced drug metabolism. 94 Although no<br />
corresponding data are currently available in children, it is reason -<br />
Figure <strong>86</strong>-8. The effects of halothane, isoflurane, and enflurane<br />
on the maximal norepinephrine-induced oxygen consumption<br />
in isolated brown adipocytes. The cells were preincubated with<br />
the indicated concentrations of the anesthetic agent, immediately<br />
transferred to an airtight oxygen electrode chamber, and<br />
then stimulated with successive additions of norepinephrine. In<br />
each of the control experiments, the maximal rate of oxygen<br />
consumption was defined. The highest rate of oxygen consumption<br />
that was reached for each concentration of each anesthetic,<br />
expressed as percent inhibition of the maximal rate of oxygen<br />
consumption, are the values shown. The results are the averages<br />
from two series of experiments. The values obtained were for<br />
cells treated with halothane: I max<br />
89 2%, IC 50<br />
0.7 <br />
0.04%, r 0.997; with enflurane: I max<br />
79 4%, IC 50<br />
0.7<br />
0.07%, r 0.994; and with isoflurane: I max<br />
69 3%, IC 50<br />
0.6 0.06%, r 0.993.<br />
able to assume that these negative effects will occur also in the<br />
neonate, maybe at an ever greater degree, and hypothermia must<br />
be prevented during anesthesia and surgery in the neonate at all<br />
times (see “Prevention of Heat Loss” ). This fact is further under -<br />
scored by convincing evidence from adults pointing out that a<br />
reduction of as little as 2C will predispose to a number of post -<br />
operative complications and will also affect outcome. 95<br />
PREOPERATIVE INVESTIGATIONS<br />
Medical History and Physical Examination<br />
Hydration Status<br />
The anesthesiologist should screen every neonate for clinical signs<br />
of dehydration, for example, reduced fontanel tension, decreased<br />
skin perfusion, reduced skin turgor, and unexplained tachycardia<br />
(see <strong>Chapter</strong> 27). Special attention should be paid to any patho -<br />
logic fluid losses, most often occurring from the gastrointestinal<br />
tract. Also signs of hypovolemia (diaphoresis, tachycardia, hypo -<br />
tension, reduced capillary refill, oliguria) must be sought. All<br />
degrees of dehydration and/or hypovolemia will have to be fully<br />
corrected before going to the operating theater, the only exception<br />
being airway obstruction and other super-emergency conditions<br />
(e.g., threatening intestinal gangrene due to malrotation volvulus).<br />
Failure to correct a negative fluid balance or to miss pre-existing<br />
hypovolemia can cause severe problems during the course of the<br />
anesthetic.<br />
Respiratory Function<br />
The presence of any respiratory symptoms must be noted. Stridor<br />
is not infrequently mistaken as expiratory stridor. Since airway<br />
obstruction is very rare unless the neonate is infected with res -<br />
piratory syncytial virus, until proven otherwise, stridor is essen -<br />
tially inspiratory in nature and represents a symptom of upper<br />
airway obstruction. Its presence should lead to further investiga -<br />
tions and consultation with an otolaryngologist. Tachypnea,<br />
grunting, jugular and costal retractions, reduced peripheral oxy -<br />
gen saturation on room air, oxygen dependence or frank cyanosis<br />
are all signs of respiratory distress. Neonatal respiratory distress can<br />
be caused by a number of different pathologies and merits<br />
consultation with a neonatologist before anesthesia.<br />
Cardiovascular Function<br />
Cardiovascular abnormalities are usually known in neonates<br />
scheduled for surgery. However, the anesthesiologist should always<br />
check for the presence of any signs and symptoms indicative of<br />
cardiovascular problems, for example, poor or excessive weight<br />
gain, failure-to-thrive problems, hepatomegaly, tachypnea, cyano -<br />
sis, heart murmur, or weak or absent femoral pulses. If such symp -<br />
toms or signs of cardiovascular abnormalities are present further<br />
consultation with the pediatric cardiologist, including an echo -<br />
cardiographic examination, is mandatory before anesthesia and<br />
surgery. A liberal attitude towards pediatric cardiology consulta -<br />
tion should be the rule in order not to miss any significant<br />
cardiovascular abnormality. Neonates undergoing correction of<br />
any congenital malformation are at increased risk of having some<br />
associated syndrome. The anesthesiologist can not be expected<br />
to be knowledgeable regarding all rare congenital syndromes but<br />
signs suggestive of Down syndrome should always be sought. The
CHAPTER <strong>86</strong> ■ Management of the Neonate: Anesthetic Considerations 1447<br />
Pierre–Robin syndrome has anesthesiological implications and<br />
signs of micrognathia should be identified before going into the<br />
operating theater.<br />
Coagulation Disorders<br />
Coagulopathy is rare in neonates. However, since coagulation dis -<br />
orders can cause life-threatening bleeding intra- and postopera -<br />
tively, the anesthesiologist has to search for symptoms and signs<br />
(e.g., prolonged bleeding from skin puncture sites, spontaneous<br />
bleeding from the nasal or oral mucosa, presence of more signifi cant<br />
amount of blood during tracheal suctioning in already ventilated<br />
patients). The skin surface should also be inspected in order to<br />
identify any petechiae indicating a possible low platelet count. If the<br />
patient is suffering from uncontrolled sepsis, a coagulopathy should<br />
be suspected until proven otherwise. If coagulation problems are<br />
suspected, appropriate laboratory tests must be performed (see<br />
“Coagulation”). If these tests are not within the normal range,<br />
consultation with a coagulationist should be under taken.<br />
Laboratory Screening<br />
Hemoglobin, Blood Typing,<br />
and Compatibility Screening<br />
Neonatal hemoglobin values are considerably higher (150 to 240<br />
g/L) than in adults (see <strong>Chapter</strong> 9). It consists mainly of fetal<br />
hemoglobin (HbF) which has a higher oxygen binding capacity<br />
(P 50<br />
19.5 mmHg) than normal adult hemoglobin (HbA) (P 50<br />
<br />
27 mmHg); thus, the HbF oxygen dissociation curve is displaced<br />
to the left. Due to its higher oxygen binding capacity, HbF has a<br />
decreased potential for oxygen release to the tissues. In a situation<br />
where oxygen demand is high or oxygen transport is marginal<br />
(e.g., sepsis, hypoxemia, hypovolemia, and intraoperative<br />
hemorrhage), transfusion of HbA will be beneficial. Polycythemia<br />
(normal hemoglobin range in the newborn: 150–240 g/L) can be<br />
present in certain neonates (incidence approximately 4%) and<br />
hematocrit values above 65% increase blood viscosity, which<br />
negatively influences tissue blood flow. In such a situation,<br />
exchange transfusion (20–30 mL/kg of blood exchanged for the<br />
same amount of plasma) can be discussed before surgical<br />
intervention in order to optimize the conditions for the patient. A<br />
preoperative hemoglobin and hematocrit value should be taken<br />
in all neonates scheduled for surgery, with the exception of<br />
diagnostic or very minor procedures (e.g., inguinal hernia repair).<br />
If surgery is more extensive or if there is even a small risk of<br />
significant bleeding, blood typing and compatibility screening<br />
should be performed. Blood and plasma should be ordered<br />
according to the potential needs and should be readily available<br />
before induction of anesthesia. Indications for the ordering of<br />
plasma are mainly the anticipation of major blood loss where<br />
plasma will be needed to boost coagulation or in situations where<br />
substantial third space losses are likely (e.g., gastroschisis repair).<br />
In the neonate, blood typing and compatibility screening requires<br />
determination of the neonates blood type as well as blood typing<br />
and screening of the mother. The type and screen of the mother is<br />
acceptable if the baby is less than 6 weeks old. If irregular<br />
antibodies are found in the mother, cross-matching has to be<br />
performed. Screening tests do not need to be performed in the<br />
neonate, since the neonatal immune system is not capable of<br />
producing antibodies until 3 months of age. Thus, the antibodies<br />
present in the neonate only originate from placental transfer from<br />
the mother.<br />
Electrolytes and Acid-Base Balance<br />
If the patient is scheduled for more extensive surgery the patient’s<br />
electrolyte and acid-base status must be checked before induction<br />
of anesthesia. A standard screen should include sodium, potas -<br />
sium, chloride, calcium, pH, and base excess/standard bicarbonate<br />
levels. Any significant deviation from normal values should be<br />
corrected before anesthesia and surgery. It is worth remembering<br />
that the neonatal reference values for potassium are higher than in<br />
older children and adults (day 1–2: 4.5–7.0 mmol/L; 3rd postnatal<br />
day–3 months: 4.0–6.2 mmol/L). Values outside of the normal<br />
values might be associated with the same risk for cardiac<br />
arrhythmias as in older patients.<br />
Coagulation<br />
Coagulation parameters are quite different in neonates and pre -<br />
mature babies compared to adults (Table <strong>86</strong>–8) and can be<br />
mistaken for a coagulopathy with an increased bleeding tendency,<br />
especially regarding activated partial thromboplastin time 96<br />
whereas neonates most often have an increased tendency for blood<br />
clotting. The theoretical background for this is still not entirely<br />
clear but can be a result of lower inhibitor levels. Thus, surgery<br />
does not have to be postponed or action taken merely on the<br />
grounds of coagulation tests outside normal adult limits. However,<br />
if coagulation parameters are outside the normal values for<br />
premature or term babies, especially also if clinical signs of coa -<br />
gulopathy are present, consultation with a coagulation expert<br />
should be undertaken.<br />
Platelet counts are similar to normal adult values in term<br />
neonates (250–300 10 9 /L) but are frequently lower in premature<br />
children (50–150 ( 10 9 /L). The function of the platelets are<br />
generally normal. The existence of thrombocytopenia should raise<br />
concern since this is often one of the initial signs of sepsis in<br />
neonates and a neonatologist should be consulted regarding the<br />
cause of a low platelet count. No specific knowledge is available<br />
for the lowest acceptable platelet count in association with<br />
neonatal surgery, but levels of at least 50 to 65 10 9 /L should most<br />
probably be required. Platelet transfusion of 5 mL/kg will increase<br />
the total platelet count by about 40 10 9 /L. In major surgery,<br />
intraoperative platelet transfusion is usually not needed until the<br />
patient has bled approximately two blood volumes, if the patient<br />
had a normal platelet count preoperatively. Due to limited reserves<br />
and a generally insufficient supply of vitamin K by breast feeding,<br />
neonates should receive supplemental vitamin K either by the oral<br />
or, preferably, by the intramuscular route (1 mg) immediately<br />
following birth. This will safeguard against the development of<br />
coagulopathy during the neonatal period. In emergent delivery<br />
situation or as a result of early transfer of the baby between<br />
hospitals, vitamin K administration can easily be forgotten. Before<br />
neonatal anesthesia and surgery it is prudent to check the patient’s<br />
notes to ensure that vitamin K has been administered. If not,<br />
coagulation parameters should be checked and vitamin K given<br />
(1 mg I.M. or I.V.). Intramuscular administration of vitamin K is<br />
preferable since I.V. administration is associated with an increased<br />
risk of side effects (mainly severe hemodynamic reactions). The<br />
effect of vitamin K is delayed (hours) and in an emergent situation<br />
transfusion of fresh frozen plasma will provide enough<br />
coagula tion factors to allow the start of the surgical intervention.
1448 PART 5 ■ Anesthetic, Surgical, and Interventional Procedures: Considerations<br />
TABLE <strong>86</strong>-8. Reference Values (Mean [Boundary]) for Coagulation Tests in Term and Premature (30–36 g.w.) Babies<br />
Coagulation test Day 1 Day 5 Day 30 Adult<br />
Premature infants<br />
PT (sec) 13.0 (10.6–16.2) 12.5 (10.0–15.3) 11.8 (10.0–13.6) 12.4 (10.8–13.9)<br />
APTT (sec) 53.6 (27.5–79.4) 50.5 (26.9–74.1) 44.7 (26.9–62.5) 33.5 (26.6–40.3)<br />
TCT (sec) 24.8 (19.2–30.4) 24.1 (18.8–29.4) 24.4 (18.8–29.9) 25.0 (19.7–30.3)<br />
Fibrinogen (g/L) 2.43 (1.50–3.73) 2.80 (1.60–4.18) 2.54 (1.50–4.14) 2.78 (1.56–4.00)<br />
Coagulation inhibitors<br />
AT III (U/mL) 0.38 (0.14–0.62) 0.56 (0.30–0.82) 0.59 (0.37–0.81) 1.05 (0.79–1.31)<br />
Protein C (U/mL) 0.28 (0.12–0.44) 0.31 (0.11–0.51) 0.37 (0.15–0.59) 0.96 (0.64–1.28)<br />
Term infants<br />
PT (sec) 13.0 (10.1–15.9) 12.4 (10.0–15.3) 11.8 (10.0–14.3) 12.4 (10.8–13.9)<br />
APTT (sec) 42.9 (31.3–54.5) 42.6 (25.4–59.8) 40.4 (32.0–55.2) 33.5 (26.6–40.3)<br />
TCT (sec) 23.5 (19.0–28.3) 23.1 (18.0–29.2) 24.3 (19.4–29.2) 25.0 (19.7–30.3)<br />
Fibrinogen (g/L) 2.83 (1.67–3.99) 3.12 (1.62–4.62) 2.70 (1.62–3.78) 2.78 (1.56–4.00)<br />
Coagulation inhibitors<br />
AT III (U/mL) 0.63 (0.39–0.87) 0.67 (0.41–0.93) 0.78 (0.48–1.08) 1.05 (0.79–1.31)<br />
Protein C (U/mL) 0.35 (0.17–0.53) 0.50 (0.22–0.78) 0.63 (0.33–0.93) 0.96 (0.64–1.28)<br />
PT prothrombin time; APTT activated partial thromboplastin time; TCT thrombin clotting time; AT III antithrombin III.<br />
Adapted from Andrew et al. 144<br />
When major surgery is planned a preoperative coagulation screen<br />
consisting of prothrombin time, activated partial thromboplastin<br />
time, and platelet count should be performed before surgery.<br />
The use of thromboelastography has recently been described<br />
also in neonates and infants. Using this technique, children with<br />
complex congenital heart disease have been found to have a<br />
functionally intact coagulation-fibrinolytic system working at a<br />
lower level than in healthy infants, indicating a reduction in the<br />
hemostatic potential with less reserve. 97 Using the same techno -<br />
logy, the effects of various colloid alternatives were analyzed in<br />
infants (3–15 kg). 98 In this investigation, the use of gelatins as an<br />
alternative to albumin was suggested since the use of hydroxyethyl<br />
starch affected the overall coagulation process the most.<br />
Diagnostic Investigations<br />
Special investigations can be required after taking the medical<br />
history and obtaining results from the laboratory testing. The most<br />
common preoperative investigations are chest radiography,<br />
echocardiography and ultrasonic head scans.<br />
Chest X-Rays<br />
Chest radiographs should be obtained in all patients with cardio -<br />
respiratory symptoms. Not only will this investigation provide the<br />
anesthesiologist with information regarding the severity of various<br />
conditions but it can also provide information if further treatment<br />
might optimize the patients condition before anesthesia and<br />
surgery. Thus, based on the chest radiograph, surgery might be<br />
postponed in order to re-expand atelectatic lung tissue or to<br />
reduce interstitial edema by intensifying diuretic treatment.<br />
Ultrasonographic Examinations<br />
Echocardiography should be performed liberally not only to search<br />
for associated congenital heart disease but also to more precisely<br />
estimate the intravascular volume status. Echocardiography is also<br />
useful in order to determine if the ductus arteriosus still remains<br />
open and to determine the possible presence of pulmonary<br />
hypertension and right-to-left shunting.<br />
Due to the existence of an open fontanel ultrasonic head scans<br />
provide the unique opportunity for investigating the intracranial<br />
contents of the neonate (for the vein of Galen for instance). In<br />
term neonates, this investigation rarely provides crucial infor -<br />
mation since intracranial hemorrhage is unusual in this group.<br />
However, premature infants have an increased risk for such<br />
hemorrhages with the highest risk seen in the most prematurely<br />
born babies. Before performing anesthesia in such premature<br />
infants, it might be wise to perform an ultrasonic head scan in<br />
order to document any pre-existing problem and, thus, escape the<br />
responsibility for any hemorrhages which have already occurred<br />
prior to the involvement of the anesthesiologist. 99<br />
PREANESTHETIC MANAGEMENT<br />
Premedication<br />
If the neonate is judged to be in pain preoperatively, low and<br />
titrated doses of morphine are appropriate. The response to<br />
morphine in this age group is variable and doses of 10 to 20 g/kg<br />
should be administered intravenously until adequate pain relief is<br />
achieved. In case of difficult venous access where an inhalational<br />
induction is planned, subcutaneous or intramuscular atropine<br />
(10–20 g/kg; minimum 100 g) is often useful to counteract<br />
parasympathetic reflexes before the placement of a reliable venous<br />
line. In case of intravenous induction, atropine can be given<br />
intravenously (10 g/kg; minimum 100 g) just before the start of<br />
the anesthetic. Apart from these specific situations, no preme -<br />
dication is usually required in the neonatal period.<br />
Parental Presence During Induction<br />
In older patients, parental presence can be helpful, although cer -<br />
tain practitioners still find this practice questionable. 100,101<br />
However, the neonate is not yet mentally capable of psychologic -
CHAPTER <strong>86</strong> ■ Management of the Neonate: Anesthetic Considerations 1449<br />
ally benefiting from parental presence, and contrary to the<br />
standard case in older children, where the children in most<br />
circumstances are otherwise healthy and the anesthetic and the<br />
surgical procedure are not expected to be hazardous, neonatal<br />
parents are often very anxious and scared for obvious reasons.<br />
Thus, parental presence does not provide any significant benefits<br />
to the neonate, may cause unnecessary stress on the parents, and<br />
can cause problems to the anesthetic team. The decision to allow<br />
or abstain from parental presence during induction of anesthesia<br />
can only be made on a case-by-case evaluation.<br />
Monitoring Requirements<br />
Overview<br />
Because of the small size of neonatal patients a number of<br />
advanced continuous monitoring options frequently used in adult<br />
patients undergoing major surgery or who are hemodynamically<br />
unstable (e.g., pulmonary artery catheterization, transesophageal<br />
echocardiography) cannot be used in the neonatal setting.<br />
However, the need for adequate and reliable monitoring is<br />
especially important in neonates since the patient will become<br />
more or less inaccessible to the anesthesiologist following surgical<br />
draping of the patient. The minimal monitoring required for<br />
neonatal anesthesia consists of the following: pulse oximetry,<br />
capnography, noninvasive blood pressure monitoring, electrocar -<br />
diogram, and body temperature measurement. The use of a<br />
precordial or an esophageal stethoscope is viewed as essential by<br />
some practitioners and is compulsory for medical–legal reasons<br />
in certain countries. Monitoring of anesthetic gases can obviously<br />
be incorporated into standard monitoring but the anesthesiologist<br />
must be aware of the caveats with the currently available<br />
systems resulting in problems with the interpretation of the<br />
generated data.<br />
If the patient is scheduled for more extensive surgery where<br />
substantial bleeding may occur or if the patient is unstable for any<br />
reason more invasive monitoring is required. Intra-arterial blood<br />
pressure monitoring should be performed liberally under these<br />
circumstances not only since it allows accurate and on-line<br />
measurement of the blood pressure even at very low blood<br />
pressure levels but also since it permits excellent monitoring of<br />
the intravascular volume status. Hypovolemia usually causes<br />
undulations of the blood pressure tracing synchronous with<br />
ventilation due to the variability in venous return caused by<br />
ventilation. Hypovolemia also causes a change in the up-stroke of<br />
the blood pressure curve due to inadequate filling of the heart.<br />
Compared to monitoring of central venous pressure intra-arterial<br />
blood pressure monitoring is superior in the setting of judging<br />
changes in filling pressures in the neonate. Intra-arterial access<br />
also allows repeated arterial blood gas sampling and other labo -<br />
ratory analyses (e.g., hematocrit, blood glucose, sodium, potas -<br />
sium, and ionized calcium).<br />
Insertion of a single lumen or multilumen central venous<br />
catheter might be a good option to get secure venous access and<br />
allow infusions of inotropic and vasoactive drugs. In any situation<br />
at risk of air embolism, precordial Doppler monitoring, together<br />
with an esophageal stethoscope, should be used to rapidly detect<br />
and treat this complication. Continuous measurement of urine<br />
output is obviously of great importance for the monitoring of the<br />
neonate undergoing major surgery. Urine output less than 1.0 mL/<br />
kg/h is indicative of hypovolemia. However, sudden decreases in<br />
output should be viewed with suspicion and the catheter system<br />
should immediately be check for blockage or kinking before any<br />
therapeutic measures are taken.<br />
Specific Considerations Concerning<br />
Common Monitoring Options<br />
PULSE OXIMETRY: Neonatal probes should only be used since<br />
adult probes are not reliable when peripheral vascular perfusion is<br />
poor. It is preferable to place the probe on the hand so that its<br />
access is facilitated when it has to be checked or moved to a new<br />
location in order to obtain a good tracing again. The probe and<br />
cable should be protected from interference caused by electric<br />
cautery. Use of a pulse oximeter displaying the plethysmogram<br />
and indicating changes in skin perfusion is recommended since<br />
significant additional information regarding the cause of malfunc -<br />
tion and the development of peripheral vasoconstriction due to<br />
hypovolemia or hypothermia is provided. Pulse oximetry will not<br />
provide reliable readings in the presence of either pronounced<br />
polycythemia or methemoglobinemia.<br />
CAPNOGRAPHY: Mainstream analysis will give more reliable<br />
readings that sidestream analysis for rapid ventilatory rates. At<br />
ventilatory rates above 50/min, the accuracy of both types of<br />
analyzers is substantially affected. However, it is usually possible to<br />
decrease the ventilatory rate intermittently briefly to 15 to 20/min<br />
to obtain a more reliable reading. The probe of mainstream<br />
analyzers will generate heat, thus, care must be taken to avoid<br />
contact of the probe with the skin. The advantages with main -<br />
stream analysis will, however, to a substantial extent be offset by<br />
the problems of mixture and dilution of the expired gases by the<br />
fresh gas flow. 102 A major issue in this respect is that it is impossible<br />
to use a measuring point distal to the tracheal tube connector with<br />
mainstream analysis. To obtain more reliable readings, sidestream<br />
analysis with a sampling point distal to the elbow connector<br />
should be used, with the ideal point being distal to the point where<br />
the tube connector narrows to the diameter of the tracheal tube 103<br />
(Figure <strong>86</strong>–9). In summary, very useful trend information can be<br />
generated both by mainstream and sidestream analyzers but the<br />
clinician must be aware of the limitations of the techniques and,<br />
when clinically indicated, control the end-tidal readings against<br />
conventional blood gas analysis.<br />
NONINVASIVE BLOOD PRESSURE MONITORING: The cuff must<br />
be appropriately sized and the arterial indicator arrow has to be<br />
in the correct place. Measurement intervals shorter than every<br />
third minute should not be routinely used, since this can cause<br />
venous stasis and petechial formation, especially in preterm<br />
babies. The calf can be used instead of the arm, depending on the<br />
circumstances. Noninvasive blood pressure monitoring provides<br />
sufficiently accurate readings in most cases and at least allows for<br />
trend observations.<br />
ELECTROCARDIOGRAPHIC TRACINGS: Cleaning the skin with an<br />
alcohol solution improves the quality of skin contact with electro -<br />
des and provides a high quality signal throughout the operation.<br />
The derivation providing the best P-wave tracing should be<br />
preferred, as it makes easier the diagnostic of nodal arrhythmia<br />
which is frequent in pediatric anesthesia. Electrocardiogram pads<br />
must be carefully removed especially in preterm infants, to avoid<br />
skin damage.
1450 PART 5 ■ Anesthetic, Surgical, and Interventional Procedures: Considerations<br />
Figure <strong>86</strong>-9. The site of mixing of fresh gas flow and expired<br />
gas is always proximal to the endotracheal tube connector. At<br />
an expired gas flow of 500 mL/min-1, the influence of fresh<br />
gas flow rate on the site of mixing and the degree of dilution<br />
is significantly greater.<br />
ANESTHETIC GAS ANALYSIS: Most available monitors aspirate gas<br />
volumes of approximately 150-200 mL/min which is con siderable<br />
if compared to the tidal volume of the neonatal child. The gas is<br />
also most frequently sampled close to the Y-piece of the ventilatory<br />
tubing. This invariably causes mixing of inspired and expired gases<br />
and also distorts the end-tidal CO2 tracing. The values derived in<br />
this setting are, thus, not accurate but trend changes are still<br />
detectable.<br />
INTRA-ARTERIAL BLOOD PRESSURE MONITORING: Maintenance<br />
of functional arterial lines throughout the operation is not an easy<br />
task during neonatal surgery. Pre-existing arterial lines must be<br />
checked before draping or a new line should be estab lished. The<br />
wrist should be splinted when using a radial approach. The<br />
insertion site should be protected from electrical interference<br />
(electrical cautery). Extension lines should be long enough when<br />
a femoral approach is planned, otherwise there is a risk that the<br />
catheter kinks or becomes dislodged (small gauge central venous<br />
lines are good options in this setting). The arterial line must be<br />
continuously flushed with a dilute heparin solution (1 U/mL) to<br />
prevent clotting. If flushing the system is necessary, it must be<br />
done over a short period of time to limit the injected volume; the<br />
distance from the wrist to the aortic arc is short and even small<br />
saline boluses may cause systemic and cerebral embolism.<br />
NEAR-INFRARED SPECTROSCOPY: This relatively new method<br />
to continuously assess cerebral oxygenation, displayed as cerebral<br />
tissue oxygenation index (cTOI), has gained widespread use<br />
in pediatric cardiac anesthesia and is able to give a fast but<br />
unspecific warning of cerebral ischemia. A sensor, similar in size<br />
compared to the bispectral (BIS)-monitor, is put on one or both<br />
sides of the forehead of the child (unilateral monitoring is usually<br />
sufficient in most instances) and is then attached to a relatively<br />
small moni tor. 104 The cTOI value has also been shown to<br />
correlated to central venous oxygenation (SvO 2<br />
) in neonates and<br />
infants. 105 This new modality of monitoring will definitely gain<br />
widespread use both in adults and children and will in the future<br />
most likely be considered standard of care for all cases of major<br />
surgery in the neonate.<br />
ANESTHETIC DEPTH MONITORING: BISPECTRAL INDEX<br />
MONITORING (BIS), SPECTRAL ENTROPY AND AUDITORY<br />
EVOKED POTENTIALS (AEP): This electroencephalography<br />
(EEG)-derived monitoring device has gain popularity in adult<br />
anesthesia as an indicator of anesthetic depth and safeguard<br />
against awareness. However, there is widespread skepticism with<br />
regards to the fact that this monitor in fact has anything to do with<br />
anesthetic depth, although there is a clear covariation between the<br />
BIS value and anesthetic depth in adults. Due to the differences<br />
in EEG patterns between adults and neonates and small children,<br />
the BIS monitor cannot be recom mended in these age groups. 106<br />
A different concept of attempting to assess anesthetic depth is<br />
the so-called Spectral Entropy that is based on the EEG power<br />
spectrum. Although this method appears comparable to BIS in<br />
adults and older children spectral entropy has not been properly<br />
validated in neonates and small infants. 107<br />
A third monitoring system in this category is Auditory Evoked<br />
Potentials (AEP). Despite measuring the response to an active<br />
auditory stimulus this method does not appear to have any<br />
advantage over the other two systems described above. 108 Thus, at<br />
present the various option for anesthetic depth monitoring that<br />
are widely used in adults cannot be recommended in the context<br />
of neonatal anesthesia.<br />
ANESTHETIC MANAGEMENT<br />
Pharmacokinetic Data for<br />
Commonly Used Drugs<br />
Because of the lack of interest and incentive for drug companies to<br />
register drugs for use in neonates and small infants, there has been<br />
a substantial knowledge gap regarding fundamental pharmaco -<br />
kinetic data for a large number of analgesic and anaesthetic drugs<br />
that are frequently used in the context of neonatal anaesthesia.<br />
However, a significant scientific effort from various research<br />
groups during the last few years have provided valuable informa -<br />
tion regarding pharmacokinetic data in this field, often using the<br />
approach of population pharmacokinetics, nonlinear mixedeffects<br />
modelling (NONMEM) and allometric scaling ( 3 / 4<br />
power<br />
modeling). The provision of the new data provide a basis for more<br />
appropriate dosing as well as minimising the risk for accumulation<br />
and undesired side effects. A summary of pharmacokinetic data<br />
are given below in Table <strong>86</strong>–9.<br />
Preoxygenation<br />
The median time necessary to achieve an end-tidal oxygen<br />
concentration of at least 90% using a tight fitting mask and 6 L/<br />
min oxygen flow is 40 seconds (range: 20–50 sec) and a preoxy -<br />
genation period of 60 seconds is, thus, recommended up to 5 years<br />
of age. 115 However, even after a 2-minute period of preoxygenation<br />
by manual ventilation with 100% oxygen following anesthesia<br />
induction and muscle relaxation oxygen, desaturation (SpO 2<br />
90%) occurs after about 80 to 90 seconds of apnea in neonates. 116<br />
Induction Techniques<br />
Neonates undergoing surgery usually already have intravenous<br />
access with an infusion running. In this setting, intravenous<br />
induction obviously is the first option. Pharmacologic properties
CHAPTER <strong>86</strong> ■ Management of the Neonate: Anesthetic Considerations 1451<br />
TABLE <strong>86</strong>-9. Pharmacokinetic Values for Some Analgesic and Anesthetic Drugs Commonly Used in Neonates and Infants<br />
Drug Clearance Volumes of Distributions Volumes of Distributions PK Model Used/Age Groups<br />
Ketorolac 109 Central volume Peripheral volume Two compartment/Infants<br />
R()isomer 7.5 mL min-1 1.2 L 0.83 L 6–18 mo<br />
S() isomer 45.3 mL min-1 3.2 L 0.22 L<br />
Midazolam 110 157 mL min-1 Central volume 3.8 L Peripheral volume Two compartment/<br />
30.2 L Infants 3–24 mo<br />
Morphine 111 71 L h-1 (70 kg)-1 Volume of distribution One compartment/<br />
136 L (70 kg)-1 0–3 yr<br />
Proparacetamol 112 55 L h-1 (70 kg)-1 Central volume Peripheral volume Three compartment/<br />
24 L (70 kg)-1 30 L (70 kg)-1 Premature babies–14 yr<br />
Propofol 113 442 mL min-1 Apparent volume of distribution Three comparment/<br />
(70 kg)-1 at steady state 259 L (70 kg)-1 Neonates<br />
Tramadol 114 17.5 L h-1 Central volume 228 L (70 kg)-1 Peripheral volume Two compartment/<br />
(70 kg)-1 0.6 L kg-1 0–6 yr<br />
of intravenous agents are fully evaluated in <strong>Chapter</strong> 14. Thiopental<br />
has withstood the test of time and is a good routine induction<br />
agent in hemodynamically stable patients. It should, however, be<br />
remembered that the terminal half-life of thiopental is very long<br />
in premature and newborn babies 117 and can result in prolonged<br />
emergence from anesthesia as well as an increased tendency for<br />
the development of postoperative apnea. Recently, the pharmaco -<br />
kinetic profile of propofol has been outlined in small children and<br />
infants 118 ; propofol might prove to be a useful alternative to<br />
thiopental also in the neonate. Based on clinical experience larger<br />
doses than normally recommended are often required to induce<br />
anesthesia with thiopental (4–8 mg/kg) or propofol (3.0–3.5<br />
mg/kg) in neonates compared to adults. In hemodynamically<br />
unstable patients ketamine (1.5–3 mg/kg) is the drug of choice for<br />
intravenous induction.<br />
In patients with a compromised airway or if intravenous access<br />
appears difficult, an inhalational induction should be used. The<br />
newer volatile agent sevoflurane tends to replace halothane as the<br />
induction agent of choice in these situations due to its relative lack<br />
of hemodynamic depression. 119 In the setting of inhalational<br />
induction with sevoflurane the anesthesiologist should be aware of<br />
one unique characteristic of sevoflurane compared to the other<br />
volatile anesthetics. Contrary to the other volatile agents, the<br />
minimum alveolar concentration (MAC) value of sevoflurane is<br />
not reduced in preterm and newborn babies compared to older<br />
children (see <strong>Chapter</strong> 13). Thus, the MAC for sevoflurane in the<br />
neonate is approximately 3.2%, which is similar to the MAC values<br />
for 1 to 6 months old infants 119 (Figure <strong>86</strong>–10). A drawback with<br />
sevoflurane is the slightly more pronounced depression of<br />
ventilation compared to halothane above 1.4 MAC, 120 but this is<br />
not believed to be of clinical importance. 121<br />
Airway Management<br />
General Considerations<br />
Preservation and protection of a patent airway is fundamental to<br />
the practice of neonatal anesthesia. Due to practical problems and<br />
the vulnerability of the newborn infant, tracheal intubation should<br />
be used liberally to avoid unnecessary ventilatory problems. This<br />
is particularly true if the anesthesiologist in charge has a limited<br />
experience with neonates. A face mask anesthetic can be consi -<br />
dered for very brief procedures. However, even during short<br />
procedures ventilation should at least be assisted, since most<br />
anesthetics will cause a significant degree of respiratory depression<br />
in the neonate. If, despite a good mask seal, the anesthesiologist is<br />
experiencing difficulties with keeping a clear airway, the use of an<br />
oropharyngeal airway or the application of 3 to 4 cm H 2<br />
O of<br />
continuous positive airway pressure are often helpful. If the<br />
situation is still not satisfactory at this point, the use of a laryngeal<br />
mask airway (LMA) can be used even in very small neonates. 122<br />
Should problems still persist, tracheal intubation must be<br />
performed without any further delay.<br />
Laryngeal Mask Airway<br />
The number 1 size LMA can be used successfully even down to<br />
approximately 1.0 kg. 122,123 To have a good LMA fit in such small<br />
patients, injection of a muscle relaxant is helpful to allow adequate<br />
relaxation of the pharyngeal muscles during the insertion<br />
procedure. Due to the relatively large dead space of the LMA often<br />
associated with high end-tidal CO 2<br />
concentrations, ventilation<br />
should at least intermittently be assisted in order to avoid hyper -<br />
capnea and atelectasis formation. To avoid gastric overdistension,<br />
Figure <strong>86</strong>-10. The mean ( standard deviation) end-tidal concentration<br />
of sevoflurane in oxygen for each of the six age<br />
groups from neonates to older children up to 12 y of age. The<br />
data for MAC at 30 y of age were obtained from reference 9.
1452 PART 5 ■ Anesthetic, Surgical, and Interventional Procedures: Considerations<br />
a nasogastric tube should be inserted before placement of the<br />
LMA and left open to vent the stomach. Use of the LMA allows the<br />
anesthesiologist to avoid unnecessary tracheal intubation in expremature<br />
babies with bronchopulmonary dysplasia where<br />
extubation has just recently been achieved with great difficulty.<br />
The LMA with preserved spontaneous ventilation can be used for<br />
selected cases with an anticipated anesthetic duration of less than<br />
30 to 45 minutes. If longer interventions are planned, tracheal<br />
intubation should be performed.<br />
The LMA has also been advocated in the resuscitation situation<br />
immediately after delivery in asphyxiated term babies. If an<br />
experienced anesthesiologist performs the placement of the LMA<br />
in this situation, successful placement of the LMA is virtually<br />
always achieved at the first attempt. 124 If the position of the LMA<br />
is checked by fiberscopy, the epiglottis is visible in about 50% of<br />
cases. The clinical relevance of this finding is still open to question<br />
since only 2% of the children had complete airway obstruction. 125<br />
The clinician should also be aware that end-tidal CO 2<br />
readings<br />
will underestimate the PaCO 2<br />
by as much as about 10% of the<br />
correct arterial value if the child is allowed to breath sponta -<br />
neously. 126 However, if ventilation is controlled, end-tidal CO 2<br />
values are as accurate as if a tracheal tube were used. 127 This,<br />
together with the high prevalence of hypercapnea associated with<br />
the use of the LMA in spontaneously breathing neonates and<br />
infants, further underscores the necessity of at least intermittently<br />
assisting the ventilation manually.<br />
Tracheal Intubation<br />
As discussed above, tracheal intubation should be considered the<br />
standard method for airway management in the neonate. A<br />
number of points deserve attention:<br />
1. Awake tracheal intubation has previously been recommended<br />
in neonates as a safe and practical method. Currently, this<br />
practice is no longer acceptable since tracheal intubation is a<br />
very stressful and painful stimulus which can definitely cause<br />
harm to the patient both in the short and long-term pers -<br />
pective. Additionally, the technique is also very stressful for the<br />
anesthetic team since the intubation conditions are far from<br />
optimal compared to the situation following a controlled<br />
anesthetic induction. 128<br />
2. Different measures exist to achieve the appropriate degree of<br />
muscle relaxation to allow easy intubation. Succinylcholine<br />
should mainly be reserved for rapid sequence intubation and<br />
nondepolarizing muscle relaxants should be preferred under<br />
more ordinary circumstances. However, the use of nonde -<br />
polarizing muscle relaxants will cause a reduction in FRC<br />
associated with decrease dventilatory homogeneity. This can<br />
be counteracted by the use of 3 cm H 2<br />
O of positive endexpiratory<br />
pressure (PEEP) and, thus, the use of this level of<br />
PEEP is recommended in anesthetized and paralyzed<br />
neonates. 129<br />
Sufficient muscle relaxation can be achieved also by deeper<br />
inhalational anesthesia, but, due to the increased risks for<br />
cardiopulmonary complications, this will require quite exten -<br />
sive neonatal anesthesia experience. Since sevoflurane causes<br />
substantially less cardiovascular depression compared to<br />
halothane, sevoflurane is preferable when available. However,<br />
the slightly more pronounced respiratory depression caused by<br />
sevoflurane compared to halothane should be borne in mind.<br />
When intubation is performed during deeper inhalational<br />
anesthesia only, the use of muscle relaxants might also be<br />
completely avoided in most cases of neonatal surgery. Inspira -<br />
tory concentrations of sevoflurane and halothane necessary to<br />
achieve good intubating conditions will, however, cause a<br />
certain degree of hypotension and great caution should be<br />
observed in the unstable neonate regarding the use of deeper<br />
levels of inhalational anesthesia. However, in more stable<br />
neonates intubation during sevoflurane inhalation was found<br />
to achieve more stable hemodynamics compared to the<br />
outdated technique of awake intubation. 130<br />
3. Since the neonatal larynx is located more anteriorly and more<br />
cephalad, with the epiglottis tending to be much floppier and<br />
to drop down over the laryngeal entrance like a theater curtain,<br />
use of a straight laryngoscope blade is recommended to gain<br />
good visualization of the vocal cords in neonates (see <strong>Chapter</strong><br />
38). The tip of the blade should not be placed in the vallecula as<br />
in older subjects but should lift the epiglottis. This is most easily<br />
achieved by first inserting the laryngoscope so that the tip of<br />
the laryngoscope is in the entrance the esophagus and then<br />
gently withdraw the laryngoscope until the laryngeal entrance<br />
“pops” in view. Visibility is regularly enhanced by gentle external<br />
pressure on the larynx which can be accom plished either by the<br />
anesthesiologist’s own little finger or by an assistant.<br />
4. Several equations are available to help determine the optimal<br />
depth to which the tracheal tube should be inserted in order<br />
to avoid unintentional dislodgment of the tube or intubation of<br />
one of the mainstem bronchi (term neonate; oral intubation:<br />
9 cm at teeth; nasal intubation: 11 cm at nose). Although<br />
helpful, such equations and guidelines are not completely<br />
reliable and the anesthesiologist must still carefully look how<br />
much of the tube is inserted during the intubation procedure<br />
and then confirm equal breath sounds and chest wall move -<br />
ments bilaterally as well as adequate end-tidal CO 2<br />
readings<br />
before being satisfied with the positioning of the tracheal tube.<br />
5. Due to the very compliant chest wall and the slightly stiffer<br />
lung, the neonate is prone to develop atelectasis following<br />
intubation or other situation involving muscle relaxation and<br />
cessation of manual or mechanical ventilation. In order to reexpand<br />
the atelectatic lung, a vital capacity maneuver should be<br />
performed. Based on animal experiments, a vital capacity<br />
maneuver (VCM; inflation pressure 40 cm H 2<br />
O for 15 sec) 131<br />
or a timed re-expansion inspiratory maneuver (TRIM; inflation<br />
pressure 30 H 2<br />
O for 10 sec) 132 has been suggested.<br />
6. Adequate fixation of the tracheal tube is of course very<br />
important. Since nasal intubation provides better opportunities<br />
to accomplish reliable fixation, nasal intubation should be<br />
performed in all situations with limited access to the head or if<br />
the patient is in the lateral or prone position.<br />
7. By tradition, uncuffed tracheal tubes are used in neonates and<br />
infants and an air leak should be present at an airway pressure<br />
of approximately 20 cm H 2<br />
O to prevent laryngotracheal<br />
trauma. With the introduction of newer materials and designs<br />
of the tracheal tubes, this traditional view is now questioned. 133<br />
However, more data are necessary before changing the classical<br />
recommendation of using uncuffed tracheal tubes in neonates.<br />
8. Use of an atraumatic technique and appropriate size of the<br />
tracheal tube is of paramount importance since the risk of<br />
laryngeal damage with long-term sequelae otherwise is high. 134<br />
9. A number of diseases and syndromes are associated with<br />
difficult intubation in the neonate too (see companion<br />
textbook, Bissonnette B, Luginbuehl I, Marciniak B, editors.
CHAPTER <strong>86</strong> ■ Management of the Neonate: Anesthetic Considerations 1453<br />
Syndromes: Rapid Recognition and Perioperative Implications.<br />
New York: McGraw-Hill; 2006.). In such a situation an<br />
individualized preinduction strategy should be formed to deal<br />
with this potential problem. 135<br />
Use of Muscle Relaxants for Intubation<br />
The dose necessary to achieve adequate muscle relaxation with<br />
succinylcholine is substantially larger in neonates compared to<br />
older children and adults 136 (see <strong>Chapter</strong> 16). The most likely<br />
explanation for this larger dose requirement in neonates is the<br />
larger extracellular fluid volume (responsible for a larger volume<br />
of distribution) present in the newborn. Thus, an effective intubat -<br />
ing dose of succinylcholine in the neonate will be approximately<br />
3 mg/kg. 136<br />
Neonates have increased sensitivity to nondepolarizing muscle<br />
relaxants due to their reduced capacity for release of acetylcholine<br />
at the motor end-plate in neonates. 137 This increased sensitivity 138<br />
(Figure <strong>86</strong>–11) is, however, offset by the increase in extracellular<br />
fluid volume. Thus, the actual dose requirements per kg body<br />
weight is similar to the doses used in adults. 138 Neonates also<br />
display a faster onset time and a prolonged duration of action of<br />
these agents. 139 At present neonatal pharmacokinetic data only<br />
exists for atracurium, 138 vecuronium 140 and pancuronium, 141 mak -<br />
ing these drugs the first line choices. Of these agents only atra -<br />
curium is of intermediate duration since both vecuronium 142 and<br />
pancuronium cause long-acting muscular relaxation in neonates.<br />
Further data are necessary before the routine use of rocuronium<br />
or mivacurium can be recommended in the neonatal population.<br />
With the variable duration of the nondepolarizing muscle<br />
relaxants in neonates monitoring of neuromuscular transmission<br />
is clearly advisable. However, such monitoring is not easily<br />
accomplished in this age group. Adequate reversal of muscle<br />
relaxation should, therefore, be the rule in all neonates. In this<br />
respect it can be discussed whether nondepolarizing muscle re -<br />
laxants should be used routinely since the judicious use of halo -<br />
genated agents and regional anesthetic techniques can produce<br />
adequate muscle relaxation in most clinical situations without the<br />
concomitant use of nondepolarizing muscle relaxants.<br />
Ventilation<br />
Ventilation should almost constantly be controlled in neonates,<br />
either by manual ventilation or with the aid of a ventilator. 143 A<br />
number of pediatric anesthesia breathing circuits have been<br />
described 144 (see <strong>Chapter</strong> 23) and one of the most commonly used<br />
intraoperatively is still the Jackson–Rees modification of the Ayres<br />
T-piece system. Although very versatile, this traditional system<br />
does have certain disadvantages compared to circle absorber<br />
systems. The use of low-flow (600 mL/min) semiclosed circle<br />
ventilation has been found possible also in neonates using modern<br />
anesthesia machines. 145<br />
A number of patients undergoing neonatal surgery have various<br />
degrees of pulmonary problems, and during surgery the need for<br />
more advanced means of mechanical ventilation might become<br />
necessary. Thus, the ventilator used during the anesthetic must be<br />
as sophisticated as the ventilator in the NICU and, at the same time,<br />
be able to deliver anesthetic gases. With the latest developments<br />
within neonatal intensive care, the neonatal anes thesiologist<br />
must also be prepared and equipped to perform anesthesia and<br />
surgery during administration of inhaled nitric oxide and/or high<br />
frequency oscillatory ventilation (HFOV). These new demands will<br />
place a great deal of responsibility on the anesthesiologist and the<br />
operation unit to learn and acquire new and sophisticated<br />
ventilators in order to meet the needs of the sick neonate.<br />
The mode of ventilation differs slightly depending on the age<br />
of the neonate and the type of surgery. Generally, pressure con -<br />
trolled ventilation is preferred in premature infants, in newborns<br />
with respiratory distress or any other pre-existing pulmonary<br />
pathology, and also during the first days of extrauterine life. Out -<br />
side the above mentioned patient categories, volume controlled<br />
ventilation can be used successfully and is especially useful in<br />
situations where surgical manipulations will interfere with<br />
intraoperative ventilation. Due to high compliance of the thoracic<br />
cage, lower compliance of the lung and higher closing volume,<br />
neonates are particularly prone to develop atelectasis during sur -<br />
gery. 146 In order to counteract this tendency for regional lung<br />
collapse, a positive-end expiratory pressure of 3 to 5 cm H 2<br />
O<br />
should routinely be used in this setting. For shorter procedures,<br />
manual ventilation is an option. A false sense of security might be<br />
associated with this mode of ventilation, since even experienced<br />
practitioners cannot reliably sense a change in compliance only by<br />
the tactile feel of the bag. 147<br />
Figure <strong>86</strong>-11. Log dose-probit response regression lines for<br />
neonates (N), infants (I) and children (C). The points along the<br />
lines represent mean responses from subgroups of five patients.<br />
Maintenance of Anesthesia<br />
Volatile Agents<br />
In babies given a regional block as part of the anesthetic plan, or<br />
who are otherwise stable and not subjected to major or very<br />
painful procedures, a volatile agent is often a good choice for<br />
maintenance. Three different volatile anesthetics are commonly<br />
used: sevoflurane, isoflurane, and halothane. All of these agents<br />
negatively affect the baroreceptor reflex with halothane having the<br />
most pronounced effect. 148 The drop in blood pressure is similar<br />
for all three agents but the mechanism for this differs for halothane<br />
compared to isoflurane and sevoflurane. Halothane depresses<br />
myocardial contractility to a greater extent than isoflurane and
1454 PART 5 ■ Anesthetic, Surgical, and Interventional Procedures: Considerations<br />
sevoflurane, and is also associated with a decrease in heart rate.<br />
With isoflurane and sevoflurane, a reduction of peripheral<br />
vascular resistance is the main cause of the reduced blood pressure<br />
and the heart rate will be maintained or even slightly increased. 149<br />
Most often, the degree of hypotension caused by the inhalational<br />
agents can be tolerated. However, if treatment is deemed necessary,<br />
a bolus administration of 5 to 10 mL/kg of crystalloid in the case<br />
of sevoflurane and isoflurane, 119,148 or administration of atropine if<br />
halothane is used, often suffices to correct the situation. 150 The<br />
concomitant administration of N 2<br />
O has different effects on<br />
the MAC requirements for the three volatile anesthetics<br />
mentioned above. The addition of 60% N 2<br />
O decreases the MAC<br />
values by 60%, 40%, and 25% for halothane, 151 isoflurane, 152 and<br />
sevoflurane, 119 respectively. To use N 2<br />
O together with halothane<br />
in an attempt to minimize the negative cardiovascular effects of<br />
halothane appears reasonable. However, whether supplemental<br />
use of N 2<br />
O is of significant value when isoflurane or sevoflurane<br />
is used can be debated.<br />
The preconditioning effect of sevoflurane is currently an area<br />
of great interest, and recent data has shown a myocardial pre -<br />
conditioning effect of sevoflurane in a neonatal rodent model. The<br />
mechanism behind this preconditioning effect of sevoflurane<br />
appeared to be a blockage of mitochondrial K ATP<br />
channels. 153<br />
The effect of inhalational agents on cerebral autoregulation is<br />
also an important topic in the context of neonatal anesthesia.<br />
Recent data suggest that cerebral autoregulation is preserved up<br />
to 1.5 MAC sevoflurane as assessed by the transient hyperemic<br />
response measured by transcranial Doppler. 154<br />
Opioids<br />
The use of moderate to high doses of opioids for maintenance of<br />
anesthesia is associated with a high degree of hemodynamic<br />
stability. This is especially useful in unstable patients or in the case<br />
of major surgery in the neonate. The use of fentanyl (10–50 g/kg)<br />
or sufentanil (35 g/kg) has been found capable of attenuating the<br />
neuroendocrine stress response and reducing morbidity; a reduc -<br />
tion in mortality has even been suggested in neonates undergoing<br />
corrective surgery for congenital heart defects. 15,24 Synthetic<br />
opioids are high clearance drugs and the metabolism is not so<br />
dependent on the maturation of the hepatic biotransformation<br />
system 155 (see <strong>Chapter</strong> 15). The terminal half-lives of fentanyl and<br />
sufentanil in the neonate are approximately 5 and 13 hours,<br />
respectively. 156 Because these drugs have a high clearance, their<br />
elimination is substantially prolonged in situations of compro -<br />
mised liver blood flow, for example, high abdominal pressure<br />
following closure of an omphalocele or gastroschisis. In this<br />
situation the terminal half-life of fentanyl has been reported to<br />
increase to 1.5 to 3 times the normal average value. 155<br />
When a regional anesthesia has not been performed for<br />
intraoperative analgesia, the repeat injection of small boluses of<br />
fentanyl (1–2 g/kg) can be used together with a volatile agent as a<br />
balanced anesthesia technique. 157 Some caution is recommended<br />
regarding the intraoperative doses of opioids in patients having<br />
received a regional anesthetic block. If there is intraoperative need<br />
to increase the depth of anesthesia, this should preferentially be<br />
accomplished by temporarily increasing the dose of volatile agent.<br />
Otherwise the patient will be exposed to the risk of a prolonged<br />
emergence with respiratory depression, possibly necessitating<br />
postoperative ventilation, since at the time of emergence the patient<br />
will have good analgesia from the regional block and, thus, will have<br />
no stimulatory effects of any pain. Such a situation can be overcome<br />
by the administration of naloxone, but the staff in the recovery<br />
room or NICU should be aware of the risks of renarcotization if a<br />
prolonged infusion of naloxone has not been started.<br />
5.6. Use of Regional Anesthesia<br />
Techniques<br />
The modern concept of a combination of a light general volatile<br />
anesthetic and a central or peripheral nerve block has proved to be<br />
of great benefit in neonatal surgery. 157,158 Apart from offering<br />
excellent intra- and postoperative analgesia, frequently making<br />
the perioperative administration of opioids unnecessary, regional<br />
anesthetic techniques provide muscle relaxation, making unnecessary<br />
the use of muscle relaxants except to facilitate tracheal<br />
intubation. A regional block also attenuates the magnitude of the<br />
surgically induced stress response 159 which is highly likely to be<br />
beneficial to the recovery of the patient. Retrospective data also<br />
indicate that a thoracic epidural block reduces the need for posto -<br />
perative ventilation compared to children receiving more tradi -<br />
tional postoperative analgesia with opioids. 157 A further advantage<br />
may also be earlier return of peristalsis following abdominal<br />
surgery in premature babies and neonates. 160 The use of epidural<br />
blocks has been found adequately safe in children, as shown in a<br />
large prospective audit (10,000 children), including more than<br />
500 epidurals performed in neonates. 161<br />
Although regional blocks offer considerable benefits in neo -<br />
nates compared to more traditional techniques, care must be taken<br />
regarding the dosing of local anesthetics in order to avoid toxi -<br />
city. 162 Generally accepted guidelines restrict a maximum bolus<br />
injection of bupivacaine to 1.5 (up to 2.0) mg/kg and a subsequent<br />
continuous infusion to maximum 0.2 mg/kg/h 163 and these dosage<br />
recommendation have recently been found to result in safe plasma<br />
levels in neonates, at least up to 48 hours postoperatively. 158<br />
Bupivacaine plasma levels of 2 to 4 g/L are generally believed to<br />
represent the threshold for CNS toxicity in children, but signi -<br />
ficantly lower plasma levels are associated with pretoxic symptoms<br />
in awake ex-premature infants receiving a caudal block. 164 Since<br />
the metabolism of lidocaine is relatively mature in neonates this<br />
local anesthetic might be an even better option than bupivacaine<br />
in neonates if a continuous infusion technique is con sidered.<br />
Determinations of plasma levels of lidocaine are usually readily<br />
available at most laboratories, making monitoring of the treatment<br />
possible and steady state conditions following conti nuous infusion<br />
will be reached within approximately 12 hours. 165 This provides a<br />
sharp contrast to bupivacaine infusion, where plasma concentra -<br />
tions of bupivacaine are still increasing in a significant portion of<br />
neonates following 48 hours of infusion. 158 Neonates receiving<br />
continuous regional blockades postoperatively should be cared for<br />
in the NICU or in a high dependence environ ment with appro -<br />
priate monitoring, for example, ECG, pulse oxi metry, respiratory<br />
rate, pain scoring, and general behavior of the neonate.<br />
Prevention of Heat Loss/Maintenance<br />
of Normal Body Temperature<br />
Every possible effort must be made to prevent perioperative<br />
hypothermia in the neonate (see <strong>Chapter</strong> 10). This can be<br />
accomplished by combining a number of different measures (Table<br />
<strong>86</strong>–10). If hypothermia still occurs despite precautions, attempts
CHAPTER <strong>86</strong> ■ Management of the Neonate: Anesthetic Considerations 1455<br />
TABLE <strong>86</strong>-10. Measures to Prevent Neonatal<br />
Perioperative Hypothermia<br />
1. Avoid unnecessary exposure of the patient. Cover the baby<br />
as much as possible during anesthesia induction and line<br />
placement.<br />
2. Use warm preparation solutions and the smallest amount<br />
necessary<br />
3. Keep the incubator plugged in and warm during the<br />
operation.<br />
4. Increase the operating room temperature to at least 25–26C.<br />
5. Use an active humidifier or a heat-moisture exchanger to<br />
prevent heat and water losses from the exhaled air.<br />
6. Active heating blanket with a prewarmed gel mattress<br />
7. Forced convective air heating system. Do not use the<br />
highest temperature setting to avoid hyperthermia and/or<br />
skin burns.<br />
8. Open bed incubator with overhead radiant heaters.<br />
Preferably use servocontrol mode with skin temperature<br />
probe.<br />
9. Warm intravenous fluids. Coaxial devices are more efficient<br />
to warm fluids.<br />
10. If intraoperative irrigation is necessary in the surgical<br />
wound, warm solutions should be used.<br />
to normalize body temperature should be undertaken as soon as<br />
possible. In order to be in control of temperature homeostasis, it<br />
is crucial to measure body temperature in all neonatal patients as<br />
part of routine monitoring. The best site for measurement of true<br />
core temperature during normal clinical conditions can be debated<br />
but convenient sites are the axilla, esophagus, rectum, and naso -<br />
pharynx. To gain further information any of the above monitoring<br />
sites can be complemented by measurement of the skin tem -<br />
perature in order to determine the degree of difference between<br />
the peripheral and the core temperature.<br />
With regards to the operating room temperature, it has recently<br />
been reported that using a room temperature of more than 23C<br />
is beneficial but will not prevent hypothermia in neonates as a<br />
single measure. 166<br />
Intraoperative Fluid Requirements and<br />
Volume Replacement During Anesthesia<br />
Caloric, Fluid, and Electrolyte Requirements<br />
Caloric, fluid, sodium, and potassium requirements have been<br />
defined during minor surgery performed under halothane<br />
anesthesia (Table <strong>86</strong>–11). 167 These requirements are close to those<br />
associated with the basal metabolic rate. 168 Depending on the<br />
degree of surgical trauma basal infusion rates during neonatal<br />
surgery can be set as follows:<br />
TABLE <strong>86</strong>-11. Intraoperative Energy and Fluid<br />
Requirements 167<br />
Intraoperative Requirements<br />
Caloric<br />
Fluid<br />
Sodium<br />
Potassium<br />
Calculated Maintenance Value<br />
1.5 kg 5 kcal/h<br />
2.5 kg 10 mL/h<br />
0.045 kg 0.16 mmol/h<br />
0.03 kg 0.10 mmol/h<br />
1. minor surgery (e.g., inguinal hernia repair): 5 mL/kg/h;<br />
2. moderate surgery (e.g., duodenal atresia repair): 7.5 mL/kg/h;<br />
3. major surgery (e.g., gastroschisis repair): 10 mL/kg/h.<br />
These infusion rates will cover fluid losses due to evaporation<br />
from the wound and “third spacing” losses. These infusion rates<br />
should be viewed as guidelines only; individual adjustments will<br />
have to be made in each separate case.<br />
Glucose Administration<br />
To include or abstain from intraoperative glucose administration<br />
has been a highly debated topic during recent years. In the majo -<br />
rity of neonates it is possible to use only Ringer solutions during<br />
the operation without risking the development of hypoglycemia. 169<br />
However, in newborns less than 48 hours ols, in babies born to<br />
diabetic mothers, following interruption of a continuous glucose<br />
infusion, and in premature or small-for-date babies, there is a<br />
definite risk of intraoperative hypoglycemia. Since the risks<br />
associated with intraoperative glucose administration are small<br />
(excluding cardiac and neurosurgical anesthesia) most practitio -<br />
ners include some amounts of glucose in the intraoperative<br />
infusion in order to safeguard against intraoperative hypoglyce -<br />
mia. Frequent intraoperative measurements of blood glucose are,<br />
however, of value regardless of infusion strategy in order to<br />
monitor glucose levels.<br />
Fluid Replacement and Suitable Solutions<br />
The composition of the intraoperative infusion fluid varies greatly<br />
between centers. A solution containing 2.5% glucose with sodium<br />
70 mmol/L represents an acceptable standard solution for most<br />
cases. Volume replacement will mainly be governed by clinical<br />
signs such as blood pressure, urine output, and time for capillary<br />
refill, since attempts at measuring carefully the amount of<br />
intraoperative blood loss in neonates are associated with great<br />
difficulties. Neonates tolerate hypovolemia poorly and substitution<br />
with crystalloids and colloids (Ringer solution 3 mL/mL of blood<br />
loss; 5% albumin 1 mL/mL of blood loss) should be started very<br />
early to compensate for ongoing losses due to oozing from the<br />
wound edges and transudation. Substitution with packed red cells<br />
and plasma (aliquots of 5–10 mL/kg of packed red cells or plasma<br />
are given according to the estimated blood loss and the blood<br />
pressure response) should also be started early and if the child is<br />
not polycythemic at the outset of surgery, the author suggests that<br />
transfusion should be started when the blood loss exceeds 10% of<br />
the estimated blood volume.<br />
Administration of a 4 to 5% albumin solution has traditionally<br />
been the colloid of choice in the neonatal setting to treat hypo -<br />
volemia, whereas it has been strongly questioned in adults. 170<br />
Albumin solutions contain quite large amounts of sodium. After<br />
significant administration of albumin the occurrence of hyper -<br />
natremia is exceedingly rare in the authors experience, even if<br />
surgery is performed immediately postpartum. Successful use of<br />
gelatin solutions (maximum dose of Haemaccel 40 mL/kg) in<br />
neonatal surgery has recently been reported. 171 Currently, albumin<br />
is still the colloid of choice for use in neonatal surgery until further<br />
data are available.<br />
Major hemorrhage, fortunately, is a rare event during neonatal<br />
surgery due to the meticulous hemostasis technique practiced by<br />
most pediatric surgeons. If confronted with major bleeding, rapid<br />
transfusion can most often be accomplished by rapid injection
1456 PART 5 ■ Anesthetic, Surgical, and Interventional Procedures: Considerations<br />
with a normal syringe attached to the infusion line. If very<br />
substantial blood loss is anticipated preoperatively, the use of a<br />
rapid transfusion device might be indicated. 172 If transfusion is<br />
given, it is necessary to make sure that the infused components<br />
are warmed. Supplementary intravenous calcium administration<br />
might also be needed in the setting of larger transfusions of packed<br />
red cells (calcium chloride 10 mg/kg (0.05 mmol/kg) I.V., might<br />
need to be repeated. Rule of thumb: 1 mg calcium chloride/<br />
transfused mL of packed red cells or plasma). 173<br />
Intraoperative Complications<br />
The most frequently encountered intraoperative complications are<br />
listed in Table <strong>86</strong>–12. Whatever the presenting symptom, airway<br />
problems should always be ruled out first, even including rein -<br />
tubation of the patient. Tachycardia and hypotension are usually<br />
indicative of hypovolemia. Bradycardia and hypotension can<br />
either be caused by anesthetic overdose, especially if halothane is<br />
used, or represent a late and very ominous sign of an unobserved<br />
complication about to escalate. However, if a thoracic epidural<br />
block has been performed, relative bradycardia and modest<br />
hypotension can be caused by blockade of the sympathetic cardio -<br />
accelerator fibers. Bradycardia and hypertension is rarely seen<br />
except in the case of an abrupt increase in afterload, as can be seen<br />
during aortic clamping/compression or following the ligation of a<br />
large patent ductus arteriosus, but in neurosurgical patients can<br />
also be a sign of increasing intracranial pressure. In this setting, the<br />
hemodynamic response is caused by a partially operative baro -<br />
receptor reflex. Tachycardia and hypertension in the absence of<br />
catecholamine producing tumors most frequently indicate<br />
insufficient levels of anesthesia (Table <strong>86</strong>–13).<br />
Venous air embolism is always a risk in neonatal anesthesia and<br />
utmost care must be observed not to allow injection of small air<br />
bubbles or to cause air entrainment at three-way stopcocks. It must<br />
be remembered that the fetal extrapulmonary shunts might still<br />
be open or can reopen during the course of the anesthetic. Inter -<br />
mittent increases in pulmonary artery pressure due to intense<br />
surgical stimulation combined with insufficiently light anesthesia<br />
can set the stage for devastating systemic embolization due to<br />
right-to-left shunting of air bubbles through the oval foramen or<br />
the ductus arteriosus.<br />
Low urine output is a frequent problem during lengthy pro -<br />
cedures. Most commonly this is due to prerenal causes which can<br />
easily be corrected by fluid and/or volume replacement. If this<br />
does not return the urine output to an acceptable level, then a renal<br />
cause for the problem might be present. Although the neonatal<br />
TABLE <strong>86</strong>-12. Intraoperative Complications<br />
Ventilatory<br />
Circulatory<br />
Complications Complications Miscellaneous<br />
1. Dislodgment of 1. Hypotension 1. Hypothermia<br />
tracheal tube<br />
2. Tracheal tube 2. Bradycardia 2. Low urine output<br />
obstruction<br />
3. Bronchial intubation 3. Tachycardia 3. Coagulopathy<br />
4. Pneumothorax 4. Hypertension<br />
5. Failure of the 5. Venous air<br />
anesthetic equipment embolism<br />
TABLE <strong>86</strong>-13. Differential Diagnosis of Intraoperative<br />
Hemodynamic Events<br />
Any Major Hemodynamic<br />
Event<br />
Tachycardia <br />
hypotension<br />
Bradycardia <br />
hypotension<br />
Tachycardia <br />
hypertension<br />
Bradycardia <br />
hypertension<br />
First Exclude Any Problems Related<br />
to Hypoxia or the Airway:<br />
1. Ventilator circuit<br />
2. Tracheal tube kinked or blocked by<br />
secretions<br />
3. Dislodgment of the tracheal tube<br />
4. Intubation of a main stem bronchus<br />
5. Unilateral or bilateral pneumothorax<br />
Hypovolemia<br />
Reduced venous return due to surgical<br />
manipulations<br />
Overdose of volatile anesthetic<br />
Late ominous sign—collapse imminent<br />
Insufficient level of anesthesia<br />
Hypercapnea<br />
Clamping or compression of the aorta<br />
Ligation of a large ductus arteriosus<br />
Increasing intracranial pressure<br />
kidney is far from mature (see “Renal Function”) it is still capable<br />
of responding to stress induced increases of antidiuretic hormone<br />
and aldosterone. If fluid and volume replacement is believed to be<br />
accurate, then a small dose of furosemide (0.25–0.5 mg/kg) is<br />
indicated to try to enhance renal urine production. Probably the<br />
most common cause for insufficient urine output is postrenal in<br />
nature and is caused by obstruction or kinking of the Foley<br />
catheter. In this case, urine output often completely ceases or the<br />
urine production is very variable over time. Checking the patency<br />
of the Foley catheter should, thus, be the first action taken if urine<br />
output is less than anticipated.<br />
Termination of Anesthesia—Emergence<br />
Reversal of Muscle Relaxation<br />
Although adequate time is believed to have elapsed since the last<br />
dose of intermediate acting nondepolarizing muscle relaxant,<br />
all neonates should be subjected to the administration of<br />
neostigmine (50 g/kg) and glycopyrrolate (10 g/kg) in order to<br />
reverse any residual muscle relaxation. Because of inherent<br />
problems with neonatal application of nerve stimulators (e.g., type<br />
and placement of the stimulating electrodes, size of the stimulating<br />
current) monitoring of train-of-four does often not provide<br />
reliably infor mation regarding the status of the neuromuscular<br />
blockade, since almost all such monitors will not function<br />
optimally in the neonate. However, if the neonate displays any type<br />
of spontaneous muscular response, reversal can be performed<br />
without risk.<br />
Should the Trachea Be Extubated or<br />
Kept Intubated?<br />
The answer to this question is complex and should be decided<br />
individually for each patient. However, if the neonate has stable<br />
vital signs, is normothermic without any major residual effects of<br />
the anesthetic, and has good quality pain relief without any<br />
concomitant respiratory depression, tracheal extubation can often<br />
be successfully performed if the patient fulfills certain criteria:
CHAPTER <strong>86</strong> ■ Management of the Neonate: Anesthetic Considerations 1457<br />
1. regular spontaneous breathing<br />
2. vigorous movements of the limbs<br />
3. gagging<br />
4. eye opening or pronounced grimacing<br />
5. stable hemodynamics, good oxygen saturation<br />
6. Absence of significant hypothermia<br />
In any other case, the patients should be ventilated in the NICU<br />
at least overnight before extubation is attempted. However, one<br />
should remember that controlled mechanical ventilation is not<br />
without significant risks for the patient and these risks must be<br />
carefully weighed against the risk for respiratory depression/<br />
insufficiency after attempted early extubation.<br />
Anesthetic Aspects Associated With<br />
Laparoscopic and Thoracoscopic Surgery<br />
Still, a traditional surgical technique is most often used, but lapa -<br />
roscopic surgery is becoming increasingly popular 174 and may<br />
soon be the method of choice in many institutions. If a laparosco -<br />
pic approach is used, the anesthesiologist must pay special<br />
attention to the various issues associated with the use of pneumo -<br />
peritoneum.<br />
Pneumoperitoneum<br />
Laparoscopic techniques or robotic surgery require the use of gas<br />
insufflation into the abdominal cavity. The insufflation will lead to<br />
physiologic alterations, especially if the abdominal pressure is<br />
allowed to be more than marginally increased. The choice of<br />
insufflation gas may also influence these physiologic changes, as<br />
will the choice of body positioning necessary for surgical access<br />
(e.g., extreme head-up or head-down positions). 175,176<br />
Carbon dioxide is the most frequently used gas, since if<br />
inadvertently insufflated into the blood vessels it will be rapidly<br />
absorbed, and thus the risk of serious pulmonary gas embolism is<br />
minimized. A certain amount of the CO 2<br />
will be absorbed via the<br />
peritoneum itself and this will cause an increased CO 2<br />
load for the<br />
patient. By using advanced mass spectrometry, it has been shown<br />
that 10 to 20% of exhaled CO 2<br />
after 10 minutes of pneumoperi -<br />
toneum is derived from exogenous CO 2<br />
. 177 An increase in alveolar<br />
minute ventilation by approximately 25 to 30% is needed during<br />
normal circumstances in order to counteract the increased CO 2<br />
load. 175 Further adjustment of minute ventilation may be needed<br />
due to cranial displacement and splinting of the diaphragm if<br />
abdominal pressures are unduly raised and/or if the patient is<br />
placed in a head-down position. Thus, in some patients the preser -<br />
vation of adequate ventilation during laparoscopic surgery can be<br />
quite challenging.<br />
Increased abdominal pressure and cranial displacement of the<br />
diaphragm will also increase the risk for atelectasis formation. To<br />
prevent undue atelectasis formation the use of volume controlled<br />
ventilation and a slightly elevated PEEP is recommended.<br />
Endotracheal intubation represents standard airway manage -<br />
ment in children undergoing laparoscopic procedures. The<br />
combined use of pneumoperitoneum and a head-down tilt will,<br />
however, produce a downward movement of the tip of the endo -<br />
tracheal tube that may result in endobronchial intubation. De -<br />
pending on the size of the child the shift of the tip can range<br />
between 1.2 to 2.7 cm. 178<br />
Pneumoperitoneum can also cause hemodynamic instability,<br />
but if intra-abdominal pressures are maintained in the lower range<br />
(10 mmHg) the impact on hemodynamics is usually minor. In<br />
this situation, venous return will be enhanced due to displacement<br />
of blood from the splanchnic bed as well as an overall increase in<br />
systemic vascular resistance. 175 However, if intra-abdominal pres -<br />
sures are allowed to increase to about 12 mmHg, then cardiac<br />
function will be directly affected as evidenced by septal dyskine -<br />
sia 179 and furthermore preload will be reduced due to compression<br />
of the inferior vena cava. 175<br />
Since the hemodynamic consequences of pneumoperitoneum<br />
is so closely related to the intra-abdominal pressure, it is absolutely<br />
essential to monitor the intra-abdominal pressure during the<br />
surgical procedure. The maximum tolerable intra-abdominal<br />
pressure level during laparoscopic surgery should be 6 to 8 mm<br />
Hg. 180 If greater pressures occur or are necessary for surgical access<br />
one may have to abandon the procedure and instead convert to an<br />
open approach due to safety concerns for the child.<br />
Both volatile and total intravenous anesthesia can be used for<br />
laparoscopic surgery. However, the use of nitrous oxide is sub -<br />
optimal based on the fact that nitrous oxide will easily diffuse into<br />
gas filled spaces and thereby increase the volume and/or pressure<br />
of trapped gas (cf. pneumothorax and intracranial air). Further -<br />
more, the use of nitrous oxide can both obscure the visibility for<br />
the surgeon due to expansion of the bowel as well as causing<br />
unwanted increases of the intra-abdominal pressure.<br />
All the problems listed above will obviously be more prominent<br />
in neonates and infants compared to older children.<br />
Thoracoscopy<br />
There is currently a surgical trend at certain major centres to<br />
perform tetralogy of Fallot (TOF) repair as a thoracoscopic pro -<br />
cedure. This is of cause associated with very specific anaesthetic<br />
considerations. A number of issues are similar to the situation of<br />
pneumoperitoneum but there are also some specific issues asso -<br />
ciated with thoracoscopy in neonates. 181<br />
CONSIDERATIONS REGARDING ENDOTRACHEAL INTUBATION:<br />
Although endotracheal intubation following an inhalational in -<br />
duction with preserved spontaneous ventilation is preferred by<br />
many clinicians (in order to avoid the risk of potential gastric<br />
distension) an intravenous induction can also be used safely in<br />
most cases.<br />
It is important to place the tip of the endotracheal tube distal<br />
to the fistula, but even more important is that the tip has a<br />
reasonable safety margin to the carina. The latter is paramount<br />
since intuba tion of the right mainstem bronchus, either during<br />
intubation or secondary to movement during the positioning of<br />
the patient, will make ventilation impossible once gas has been<br />
insufflated into the right pleural cavity causing right lung collapse.<br />
It is therefore necessary to confirm the position of the tube<br />
tip both following intubation as well as after placing the patient<br />
in the final position with the right side slightly elevated for<br />
surgical access.<br />
ONE-LUNG VENTILATION (OLV): Insufflation of CO 2<br />
into the<br />
right pleural cavity will cause the right lung to collapse, even when<br />
using the recommended insufflation pressure of 5 to 6 mmHg.<br />
This will in turn result in an increase in pulmonary vascular<br />
resistance secondary to hypoxic vasoconstriction in the right lung.<br />
The positive pressure in the right hemithorax will also cause a<br />
decrease in venous return by compression of the vena cava and<br />
may also cause direct compression of the right ventricle. Thus,
1458 PART 5 ■ Anesthetic, Surgical, and Interventional Procedures: Considerations<br />
reductions in cardiac output and blood pressure are likely to occur<br />
during the case.<br />
Ventilation during surgery can be achieved either by mechani -<br />
cal ventilation or by hand ventilation by the anesthesiologist. Even<br />
if mechanical ventilation is used, periods of manual ventilation<br />
are often necessary.<br />
PROBLEMS WITH GAS EXCHANGE: Insufflation of CO 2<br />
com bined<br />
with a limited possibility to maintain adequate alveolar ventilation<br />
will result in serious CO 2<br />
retention combined with pronounced<br />
respiratory acidosis (pH 7.0). This situation is further<br />
compounded by the fact that the measurement of end-tidal-CO 2<br />
is notoriously unreliable and the CO 2<br />
tracing may even become<br />
absent during parts of the procedure. A well-functioning arterial<br />
line is, thus, a prerequisite in this situation. Desaturation episodes<br />
can be considered the rule, and to counteract this as much as<br />
possible ventilation with 100% oxygen is recommended during<br />
the period of OLV.<br />
The combination of hypoxia, hypercapnea and acidosis will of<br />
cause add to the increase in pulmonary vascular resistance caused<br />
by the atelectasis of the right lung. Due to the substantial altera -<br />
tions that take place both regarding hemodynamics and gas<br />
exchange it is very useful to use cerebral near-infrared spectros -<br />
copy (Invos) to monitor cerebral oxygenation throughout the<br />
procedure. 182<br />
Requirements for monitoring and vascular access are:<br />
1. normal noninvasive monitoring<br />
2. arterial line for repeated blood gas analysis and invasive blood<br />
pressure monitoring<br />
3. at least two peripheral venous lines or if deemed necessary a<br />
femoral or central venous catheter<br />
4. cerebral near-infrared spectroscopy (Invos)<br />
Even if it is clearly possible to perform TOF repair as a thora -<br />
coscopic procedure, the combination of neonatal anesthesia with<br />
periods of hypoxia, pronounced hypercarbia, and substantial<br />
acidosis may raise concern regarding the risk for brain cell<br />
apoptosis with potential long-term cognitive and behavioral<br />
problems (see “Effects of Anesthetic Agents on the Premature and<br />
Neonatal Brain” above). Despite this, there are case reports where<br />
this technique at least initially has been used successfully, even in<br />
TOF cases with significant concomitant congenital heart disease<br />
(e.g., pulmonary atresia with single ventricle physiology). 182<br />
POSTOPERATIVE CARE<br />
Pain Scoring<br />
The use of appropriate pain scales for monitoring of postoperative<br />
pain is fundamental to the provision of optimal pain relief.<br />
Im plementation of regular pain assessment has a number of<br />
advan tages:<br />
1. regular pain assessment and charting of the results increases<br />
the awareness of the care providers regarding the problem of<br />
postoperative pain in neonates and children<br />
2. assessment performed before and after an intervention aimed<br />
at reducing pain will provide the care providers with feedback<br />
regarding the efficacy of the intervention<br />
3. pain assessment will provide a tool for evaluation of different<br />
analgesic techniques and allows for a more structured and<br />
scientific analysis of the treatment of postoperative pain<br />
The problem with pain assessment in the neonatal period is<br />
that existing pain scales are only designed and validated for shortterm<br />
procedural pain (e.g., heel lancing). Frequently used pain<br />
scales which has been developed and validated for ongoing<br />
postoperative pain in neonates and infants are the CHIPPS scale 183<br />
and the CRIES score. 184 An advantage with the CHIPPS scale is<br />
that the intention with this scale is not only to assess pain but also<br />
to identify a score which will predict the need for administration<br />
of supplemental analgesia. However, a recently published com -<br />
parison of neonatal pain scores did find that the neonatal infant<br />
pain scale may be a preferable pain evaluation tool in the setting<br />
of neonatal surgery. 185<br />
Analgesia<br />
A plan for treatment of postoperative pain should be available in<br />
all neonates. The metabolism of paracetamol (acetaminophen) is<br />
reason ably well developed in the neonate and, thus, this drug<br />
should be regularly administered. Rectal dosages of 20 to 40 mg/kg<br />
have been reported to result in safe plasma concentrations in the<br />
preterm and term baby. 1<strong>86</strong>,187 Whenever possible, regional anesthe -<br />
tic techniques should also be utilized due to the excellent quality<br />
of pain relief combined with the low risk for unwanted side<br />
effects. 188 If regional techniques are not applicable or are insuf -<br />
ficient, continuous low-dose infusions of opioids are often helpful<br />
(e.g., morphine 10–20 g/kg/h) 189 and with careful titration of the<br />
infusion the risk for respiratory depression is very small. However,<br />
more complicated analgesic regimens should be carried out under<br />
closed supervision in the NICU or high dependency unit.<br />
Fluid Balance/Nutrition<br />
If the neonate has been subjected to anything but a minor proce -<br />
dure or pure diagnostic examination, there will be a postsurgical<br />
stress reaction inducing a state of catabolism and fluid retention.<br />
Although the period of catabolism and fluid retention is shorter in<br />
newborns and infants it is not possible to resume full nutrition or<br />
normal fluid volumes immediately following surgery. Ignoring the<br />
effects of the postsurgical stress reaction will lead to unnecessary<br />
strain on the neonates metabolism and cardiorespiratory system<br />
and will also lead to unwanted fluid retention and edema. Thus,<br />
during the first 12 to 24 hours postoperatively it is generally wise<br />
to restrict the fluid volume to approximately 80 to 100 mL/kg <br />
24 h and give only a glucose solution, for example, 10% glucose<br />
with sodium 40 mmol/L and potassium 20 mmol/L. Early<br />
supplementation with lipid emulsions can, however, be used in<br />
neonates requiring additional caloric support. 190<br />
This traditional approach has recently been challenged by data<br />
showing that neonates undergoing major gastroschisis surgery are<br />
able to achieve a positive protein balance if given parenteral amino<br />
acids (2.5 g kg-1 24 h-1) immediately postoperatively without<br />
signs of protein intolerance. 191 However, further prospective<br />
randomized trials including the full variety of neonatal surgical<br />
procedures are needed before changing the more traditional<br />
approach described above.<br />
Antibiotics<br />
Although mainly a surgical concern the anesthesiologist should<br />
check that appropriate antibiotic coverage has been order for
CHAPTER <strong>86</strong> ■ Management of the Neonate: Anesthetic Considerations 1459<br />
the patient. If not, or if any doubts exist regarding the need for or<br />
the choice of antibiotic, the anesthesiologist should contact the<br />
surgeon to discuss this matter.<br />
Radiographic Examinations<br />
A postoperative chest radiograph is frequently performed follow -<br />
ing a number of interventions in order to check for adequate line<br />
and tube placing and to rule out pneumothorax. Radiographic<br />
control of the location of epidural catheters should also be<br />
performed if the catheters have been threaded via the caudal or<br />
lumbar epidural route to a more cephalad position. The suspicion<br />
of partial intravenous injection through the epidural catheter also<br />
warrants postoperative radiographic control. The necessity for<br />
other investigations will have to be individualized and is most of<br />
the times the responsibility of the surgeon.<br />
Postoperative Complications<br />
Complications during the immediate postoperative period in<br />
neonates is dominated by ventilatory problems. The most<br />
common problems encountered are the following: opioid-induced<br />
hypoventilation, postoperative apnea in the ex-premature, residual<br />
muscle relaxation, postextubation stridor, inadequate ventilation<br />
due to insufficient pain relief, and upper airway obstruction. The<br />
frequency of these potentially life-threatening events merits close<br />
supervision of the neonate for at least 24 hours postoperatively<br />
before being returned to an ordinary ward.<br />
The anesthesiologist is often confronted with questions regard -<br />
ing postoperative diuresis. In this situation, it is important to<br />
remember that the normal newborn child does not always pass<br />
urine until 12 to 24 hours after birth and that the surgically<br />
induced stress response leads to water conservation and reduced<br />
diuresis. It is, thus, not reasonable to expect a hourly urine output<br />
in excess of about 1 mL/kg/h in the immediate postoperative<br />
phase. If the patient is believed to be truly oliguric, the anes -<br />
thesiologist has to decide whether this is due to hypovolemia or if<br />
diuresis should be enhanced by the administration of loop<br />
diuretics. It should be remembered that patients can be hypovole -<br />
mic despite showing signs of peripheral edema, for example,<br />
on the dorsum of the hand and feet and eye lids. Although<br />
postoperative hemorrhage is unusual following neonatal surgery,<br />
additional volume replacement is frequently necessary following<br />
major operations due to ongoing losses through drains or due to<br />
developing tissue edema and “third spacing.” If postoperative<br />
hemorrhage or hypovolemia of other causes do occur the clinical<br />
signs will be usual: diaphoresis, reduced peripheral circulation,<br />
prolonged capillary refill, tachycardia, oliguria, and hypotension.<br />
SPECIFIC NEONATAL CONDITIONS<br />
REQUIRING SURGICAL<br />
INTERVENTION<br />
Airway Obstruction<br />
Stridor<br />
A variety of different conditions can cause the presence of inspi -<br />
ratory stridor with jugular and intercostal/subcostal retractions in<br />
the neonate: 192 (1) bilateral choanal atresia, (2) Pierre–Robin<br />
syndrome, (3) cystic hygroma, (4) laryngomalacia, (5) laryngeal<br />
web or adhesion of the vocal cords, (6) vocal cord paralysis, (7)<br />
subglottic hemangiomas, (8) tracheomalacia. It should be<br />
remembered that in a significant number of neonates outside the<br />
immediate newborn, period the cause for the stridor can be ac -<br />
quired and, thus, a sequelae of previous intubation. 193 If the<br />
inspiratory stridor is more severe in nature or if it tends to be<br />
progressive causing respiratory distress the cause of the obstruc -<br />
tion needs to be clarified. In the case of bilateral choanal atresia,<br />
the diagnosis is made by trying to pass a suction catheter through<br />
each of the nostrils (see <strong>Chapter</strong> 63). In more severe cases of cystic<br />
hygroma, the condition will be obvious from observing the<br />
swelling in the neck. Apart from these conditions, a diagnostic<br />
bronchoscopy will have to be performed to identify the cause of<br />
the problem as well as determining the degree of obstruction.<br />
Depending on the finding made during the bronchoscopy further<br />
action may need to be undertaken (e.g., tracheal intubation or<br />
tracheotomy). How to approach this problem will obviously<br />
depend on the severity of the condition. If the stridor is only slight<br />
or moderate, a preoperative workup can be performed in a normal<br />
fashion, whereas if the symptoms are judged to be life-threatening,<br />
immediate action needs to be taken. It is of vital importance<br />
both for the well-being of the patient and for diagnostic purposes<br />
that spontaneous ventilation is preserved during the anesthetic.<br />
The main steps of anesthetic management are summarized in<br />
Table <strong>86</strong>–14.<br />
Cleft Lip Repair<br />
Neonatal surgical intervention in these conditions is now perfor -<br />
med in certain centers in order to improve the cosmetic and<br />
functional outcome. 194 Cleft lip/palate can be associated with other<br />
malformations, but frequently patients are otherwise healthy and<br />
normal. The main steps of anesthetic management are sum -<br />
marized in Table <strong>86</strong>–15.<br />
Thoracic Surgery<br />
Esophageal Atresia With<br />
Tracheoesophageal Fistula<br />
The incidence of the malformation is approximately 1/3000. The<br />
lesion is classified I to V depending on the anatomic configuration<br />
of the tracheoesophageal fistula. In the majority of cases the upper<br />
esophageal segment ends in a blind pouch with the lower esopha -<br />
geal segment connecting to the trachea close to the carina via a<br />
fistula. This abnormality makes the neonate unable to swallow its<br />
own pharyngeal secretions and the baby will cough or even choke<br />
when breastfed. More serious aspiration into the airways can also<br />
occur through the fistula, which is in direct continuum with the<br />
stomach. Acid aspiration of gastric secretions can cause significant<br />
chemical pneumonitis. In order to minimize the risks of pulmo -<br />
nary aspiration, surgery should be performed without undue<br />
delay. Surgery can be deferred until the next morning and since<br />
available expertise and infrastructure is usually superior during<br />
daytime this is often preferable compared to the on-call nighttime<br />
setting. The main steps of anesthetic management are summarized<br />
in Table <strong>86</strong>–16.<br />
Tracheoesophageal Cleft<br />
Tracheoesophageal cleft is a very rare syndrome with an estimated<br />
incidence of approximately 1/100,000. The extent of the cleft
1460 PART 5 ■ Anesthetic, Surgical, and Interventional Procedures: Considerations<br />
TABLE <strong>86</strong>-14. Typical Anesthetic Management of a Neonate Presenting With Stridor<br />
Symptoms<br />
Preoperative investigations<br />
(if time allows)<br />
Monitoring<br />
Suggested anesthetic and<br />
recommendations<br />
Recommended Examinations and Management<br />
Inspiratory stridor, jugular and intercostal/subcostal retractions, cyanosis<br />
1. Arterial blood gas, routine laboratory<br />
2. Chest radiograph<br />
3. Transthoracic echocardiography (can help to diagnose vascular ring abnormality)<br />
Routine monitoring only<br />
1. No premedication<br />
2. Establish I.V. access before induction, preferably in the neonatal intensive care unit<br />
3. I.V. atropine (10 g/kg), preoxygenation<br />
4. Inhalational induction sevoflurane or halothane in oxygen<br />
5. Deep anesthesia needed to avoid laryngospasm, coughing or breath-holding. The more severe the<br />
obstruction the longer the time necessary to reach the appropriate level of anesthesia<br />
6. Apply a continuous positive airway pressure (3–5 cm H 2<br />
O). This helps distending the airways and<br />
prevent laryngospasm<br />
7. Depending on the ear-nose-throat technique used, continuous supply of O 2<br />
and volatile agent is<br />
provided through a bronchoscope attachment or holding the fresh gas tubing within the mouth; jet<br />
ventilation can be used (delivery of volatile agent usually not possible)<br />
8. If the airway is left unintubated and tracheotomy is not performed, administration of I.V.<br />
hydrocortisone (1–2 mg/kg) may help counteracting postoperative airway edema (postoperative<br />
inhalation of epinephrine might be useful in this regard too)<br />
9. Even if the airway obstruction is judged to be only minor to moderate, e.g., with a number of<br />
patients suffering from laryngotracheomalacia, the patient should be cared for in an NICU or high<br />
dependency area for the first postoperative 12–24 hours<br />
varies. In less severe cases there is only a cleft present in<br />
the posterior parts of the larynx with no involvement of the<br />
trachea and the esophagus. However, in the most extensive cases<br />
(Type IV) the cleft extends from the larynx to the carina. The<br />
existence of the cleft creates the possibility for regurgitation and<br />
aspiration of both saliva and stomach contents with repeated<br />
cyanotic episodes and pneumonias. Occasionally the diagnosis<br />
is suspected following repeated tracheal tube dislodgment. The<br />
final diagnosis is made at bronchoscopy. The anesthetic plan for<br />
later closure of the defect has to be individualized since the<br />
TABLE <strong>86</strong>-15. Typical Anesthetic Management of a Neonate Undergoing Cleft Lip/Palate Repair<br />
Symptoms<br />
Preoperative investigations<br />
Monitoring<br />
Suggested anesthetic and<br />
recommendations<br />
Recommended Examinations and Management<br />
Usually apparent on inspection. Isolated palate lesion requires palpation of the palate<br />
1. Search for other malformations<br />
2. Echocardiography to search for associated cardiac anomalies<br />
3. Blood type and compatibility tests<br />
4. Order 1 unit blood<br />
Routine monitoring<br />
1. No premedication<br />
2. I.V. atropine (10 g/kg)<br />
3. Preoxygenation<br />
4. Induction technique according to the preference of the anesthesiologist<br />
5. Tracheal intubation can be difficult (blade of the laryngoscope sliding into the cleft); packing the<br />
cleft with a small wet sponge will circumvent this problem<br />
6. RAE tubes are useful. Careful that the distance from the tip of the tube to the preformed “knee”<br />
may be wrong and lead to bronchial intubation. If too long, cut appropriately before intubation or<br />
fixe the “knee” lower on the mandible<br />
7. Throat packing is recommended to protect airway from blood and secretions; the end of the pack<br />
should be left outside the mouth to remind to remove it at the end.<br />
8. Local anesthetic block of the infraorbital nerves will provide excellent intra- and immediate<br />
postoperative analgesia<br />
9. Extubation should only be performed after the removal of the throat pack and following careful<br />
suctioning of the mouth and pharynx. Because of blood oozing following surgical reconstruction,<br />
extubation in the lateral position is preferable and when fully awake. If edema or bleeding and<br />
concern regarding the airway, the patient should be returned to NICU until safe extubation can be<br />
achieved
CHAPTER <strong>86</strong> ■ Management of the Neonate: Anesthetic Considerations 1461<br />
TABLE <strong>86</strong>-16. Typical Management of a Neonate Presenting With Tracheoesophageal Fistula<br />
Symptoms<br />
Preoperative investigations<br />
Monitoring<br />
Suggested anesthetic and<br />
recommendations<br />
Recommended Examinations and Management<br />
Coughing or choking when swallowing. Drooling. Can’t pass a nasogastric tube into the stomach<br />
1. Chest radiograph with radio-opaque catheter or nasogastric tube inserted into the upper<br />
esophageal segment. Avoid use of radio-opaque dye to prevent aspiration<br />
2. Echocardiography to search for associated cardiac anomalies<br />
3. Routine laboratory and arterial blood gas<br />
4. Blood type and compatibility tests<br />
5. Order 1 unit blood and 1 unit plasma<br />
1. Routine monitoring<br />
2. Invasive blood pressure monitoring<br />
3. Foley catheterization<br />
1. No premedication<br />
2. Establish venous access before induction of anesthesia if not yet in place<br />
3. I.V. atropine (10–20 g/kg)<br />
4. Evacuate any secretions from the upper esophageal pouch by aspirating the catheter<br />
5. Preoxygenation<br />
6. Rapid sequence induction with succinylcholine (1–2 mg/kg) for relaxation. Cricoid pressure is not<br />
meaningful since aspiration can still occur through the fistula<br />
7. Avoid gastric distention. Gas insufflation of the stomach is greater in patients with decreased lung<br />
compliance. Bronchoscopy prior to tracheal intubation is occasionally used to identify the fistula<br />
and seal it with a small balloon tipped catheter. If severe gastric distention, rapid decompression<br />
(needle aspiration gastrostomy) is requested<br />
8. Maintenance depends on the condition of the neonate and the postoperative ventilatory strategy.<br />
In the unstable neonate an opioid anesthetic (fentanyl 10–25 g/kg) is often preferable. Stable<br />
term neonates will benefit of inhalational agents. Low dose volatile agents is also a good choice if<br />
analgesia is provided by an epidural technique. Certain surgeons require that the patient be kept<br />
sedated, paralyzed and ventilated in the early postoperative period to “protect” the anastomosis, a<br />
high-dose opioid anesthetic is most indicated<br />
9. Insertion of an arterial catheter for the unstable neonate<br />
10. Placement of a continuous thoracic epidural regional block, either via the caudal approach or<br />
directly (by experienced anesthesiologists only)<br />
11. During surgery, the lung, the trachea and the large veins will be compressed leading to<br />
desaturation, reduction of venous return and cardiac output. The surgeon must be alerted when<br />
this happens but must be given reasonable time to perform the different stages of the procedure.<br />
Brief periods of desaturation or blood pressure changes must be accepted without alarming the<br />
surgeon<br />
12. Manipulation and ligation of the fistula leads to minor bleeding and secretions. Repeated<br />
suctioning of the tracheal tube might be needed to avoid partial or complete obstruction<br />
13. Before the closure of the thoracic wound the lung should be carefully re-expanded in order to<br />
avoid unnecessary postoperative atelectasis<br />
procedure is a significant surgical and anesthetic ordeal. 195,196<br />
Below are only some guidelines for the initial bronchoscopy.<br />
The main steps of anesthetic management are summarized in<br />
Table <strong>86</strong>–17.<br />
Congenital Lobar Emphysema<br />
This congenital malformation consists of pathologic enlargement<br />
of one of the lung lobes, which can be caused by bronchomalacia,<br />
a vascular anomaly, or an intrabronchial obstruction. Depending<br />
on the size of the lesion, it can compress healthy lung tissue and<br />
also create an intrathoracic volume lesion with mediastinal shift<br />
and impeded venous return. Such patients will present with<br />
a combination of respiratory distress and cyanosis. Surgical<br />
intervention due to this condition will be undertaken either on a<br />
semiemergent basis or as an elective procedure. The condition<br />
is also frequently (35%) associated with congenital heart disease.<br />
The main steps of anesthetic management are summarized in<br />
Table <strong>86</strong>–18.<br />
Patent Ductus Arteriosus<br />
In the neonatal period this is almost exclusively a disease of the<br />
premature baby. The presence of a patent ductus arteriosus (PDA)<br />
causes a left-to-right shunt across the ductus resulting in two<br />
different unfavorable situations. First, the resulting pulmonary<br />
overcirculation puts significant volume strain on the left side of<br />
the heart and causes enlargement of the left atrium and ventricle<br />
and causes high-output cardiac failure. Second, in severe cases<br />
the left-to-right shunting may become so pronounced that there<br />
can be reversal of the diastolic aortic blood flow in the descending<br />
aorta. In this situation, the blood supply to the lower body<br />
is jeopardized and patients with PDA are at increased risk of<br />
developing necrotizing enterocolitis as a result of splanchnic
1462 PART 5 ■ Anesthetic, Surgical, and Interventional Procedures: Considerations<br />
TABLE <strong>86</strong>-17. Typical Management of a Neonate Presenting With Tracheoesophageal Cleft<br />
Symptoms<br />
Preoperative investigations<br />
Monitoring<br />
Suggested anesthetic and<br />
recommendations<br />
Recommended Examinations and Management<br />
Recurrent episodes of cyanosis, frequently associated with feeding. Repeated tracheal tube<br />
dislodgment<br />
1. Nasogastric tube for continuous suction. Can be very difficult. Check x-ray for position<br />
2. Chest radiograph<br />
3. Echocardiography<br />
4. Routine laboratory<br />
5. Blood type and compatibility test<br />
6. Order 1 unit blood and 1 unit plasma<br />
1. Routine monitoring<br />
2. Invasive blood pressure monitoring<br />
1. No premedication, I.V. atropine (10 g/kg), preoxygenation<br />
2. Inhalation induction and spontaneous ventilation. Keep the nasogastric tube on suction<br />
3. If symptoms are mild and complete cleft unlikely, bronchoscopy can be handled as usual. In severe<br />
cases, ventilation and oxygenation may be difficult due to reduced lung compliance and repeated<br />
aspiration. This is accentuated if positive pressure ventilation is attempted<br />
4. If cleft is complete (down to the carina), securing the airway with a tracheal tube is not possible.<br />
Selective bronchial intubation might become the only option available. If necessary, use a normal<br />
tracheal tube for each main bronchus and two separate ventilation circuits for each tube. This will<br />
avoid many problems<br />
hypoperfusion. Pharmacologic closure of the PDA (I.V. indo -<br />
methacin) is often successful but if this treatment has failed, in<br />
longstanding cases or if the size of the PDA is judged to be very<br />
large, surgical ligation of the PDA is required. The anesthesiologist<br />
should be aware that one of the cornerstones of the conservative<br />
treatment of a PDA is fluid restriction and the use of diuretics<br />
(usually furosemide). Thus, these patients are regularly on the<br />
border of hypovolemia and can also have significant potassium<br />
deficits, two conditions that have serious implications for the safe<br />
administration of anesthesia. Even if unsuccessful in accomplish -<br />
ing closure of the PDA, I.V. indomethacin will regularly cause<br />
transient renal dysfunction with a reduction in urine output and<br />
a fall in platelet number and activity due to the effects of indo -<br />
methacin on prostanoid synthesis in the kidney and the platelet.<br />
Thus, it is wise to wait until urine output has normalized and there<br />
is no clinical or laboratory signs of platelet dysfunction before<br />
accepting the neonate for surgery. The main steps of anesthetic<br />
management are summarized in Table <strong>86</strong>–19.<br />
TABLE <strong>86</strong>-18. Typical Management of a Neonate With Congenital Lobar Emphysema<br />
Symptoms<br />
Preoperative investigations<br />
Monitoring<br />
Suggested anesthetic and<br />
recommendations<br />
Recommended Examinations and Management<br />
Tachypnea. Moderate to severe respiratory distress. Tachycardia and/or hypotension. Cyanosis.<br />
Lateral shift of cardiac sounds. Accidental finding on chest radiograph<br />
1. Chest radiograph<br />
2. Echocardiography<br />
3. Routine laboratory, arterial blood gas, blood type and compatibility test<br />
4. Order 1 unit blood and 1 unit plasma<br />
1. Routine monitoring<br />
2. Invasive blood pressure monitoring<br />
3. Foley catheterization<br />
1. No premedication, I.V. atropine (10 g/kg), preoxygenation<br />
2. Inhalational induction, maintain spontaneous ventilation to limit enlargement of the lobar<br />
emphysema by positive pressure ventilation while securing the airway. If the patient is in<br />
distress ketamine is preferred to thiopental to prevent hemodynamic deterioration<br />
3. Selective bronchial intubation might be necessary if positive pressure ventilation needed. 100%<br />
O 2<br />
helps reduce the size of the emphysema (resorption of the nitrogen)<br />
4. Maintenance depends on severity. Total intravenous anesthesia or volatile techniques are<br />
suitable<br />
5. Inotropic support may be needed and a dopamine infusion should be at hand<br />
6. Re-expand the lungs before thoracic closure to limit postoperative atelectasis<br />
7. If possible, the trachea should be extubated at the end of procedure. Spontaneous breathing<br />
reduces the strain on the bronchial stump and decrease the risk for significant air leak or<br />
development of a bronchopleural fistula. Regional anesthetic techniques are very helpful (e.g.,<br />
continuous paravertebral or thoracic epidural blockade)
TABLE <strong>86</strong>-19. Typical Management of a Neonate With Patent Ductus Arteriosus<br />
Symptoms<br />
Preoperative investigations<br />
Monitoring<br />
Suggested anesthetic and<br />
recommendations<br />
CHAPTER <strong>86</strong> ■ Management of the Neonate: Anesthetic Considerations 1463<br />
Recommended Examinations and Management<br />
Cardiac failure with fluid retention, poor weight gain, tachypnea, ventilator dependence.<br />
Bouncing femoral pulses or wide pulse pressure due to the left-to-right shunting (cf. aortic<br />
insufficiency). Echocardiography will give final diagnosis<br />
1. Chest radiograph<br />
2. Echocardiography (ask for signs of hypovolemia and degree of cardiac failure)<br />
3. Ultrasonic head scan to document any pre-existing intracranial pathology<br />
4. Routine laboratory including potassium<br />
5. Blood type and compatibility test. Platelet count<br />
7. Order 1 unit blood and 1 unit plasma<br />
8. Check last 24 h urine output and diuretic use to judge body fluid status<br />
Routine monitoring; invasive blood pressure monitoring if patient is unstable<br />
1. No premedication, IV atropine (10 g/kg), preoxygenation<br />
2. Induction of anesthesia depends on the degree of cardiac failure. If moderate (failure to wean the<br />
patient from the ventilator), standard IV induction and maintenance with low dose sevoflurane<br />
(less myocardial depression than halothane); if severe (poor contractility on preoperative<br />
echocardiography or digitalization), opioid anesthetic and small doses of midazolam or a very low<br />
dose of sevoflurane<br />
3. Nasal intubation is preferred to reduce the risk of dislodgment of the tube due to limited access to<br />
the patient, right lateral positioning and low weight<br />
4. During surgery, lung compression is inevitable; periods of desaturation must be tolerated to allow<br />
progress of the surgery. If bradycardia develops, immediate re-expansion is needed<br />
5. Hypotension occurs frequently; if not due to surgical impairment of venous return, this requires<br />
lightening anesthesia first, then give plasma expander (most patients are hypovolemic). If<br />
moderate expansion (10–15 mL/kg of 5% albumin solution) fails to restore the blood pressure,<br />
inotropic support is necessary (dopamine 5–10 g/kg/min)<br />
6. Before closing the wound the surgeon should be encouraged to place either a multilevel intercostal<br />
block or a paravertebral block under direct vision<br />
7. Weaning from the ventilator may requires several days despite the correction of the pathology due<br />
to edema and atelectasis of the right lung, necessity to administer fluids to stabilize<br />
hemodynamics and improve cardiac function<br />
Abdominal Surgery<br />
Congenital Diaphragmatic Hernia<br />
The incidence of congenital diaphragmatic hernia (CDH) is<br />
approximately 1/5000 live births. Most often it is left-sided, but<br />
right-sided cases do occur. The severity of the malformation<br />
depends on the amount of herniation of the abdominal contents<br />
that as occurred during fetal life. In minor herniation, the patient<br />
can be asymptomatic at birth and is only diagnosed by a chest<br />
radiograph often performed for other reasons. In severe cases, the<br />
baby has immediate symptoms of severe respiratory distress and<br />
hypoxic respiratory failure combined with life-threatening pulmo -<br />
nary hypertension. The ventilatory problems are not due solely to<br />
an intrathoracic mass lesion, as previously believed, but are instead<br />
also due to the associated pulmonary hypoplasia and pulmonary<br />
hypertension. Thus, there is no need for immediate reduction<br />
of the abdominal viscera as previously practiced. This can in fact<br />
be regarded as absolutely contraindicated and should be preceded<br />
by preoperative stabilization. In the case of more pro nounced<br />
intrauterine herniation not only will the ipsilateral lung be<br />
hypoplastic but the contralateral lung is also affected to some<br />
degree by hypoplasia. 197 Most of the children with CDH are term<br />
infants and normally developed regarding most organ systems<br />
except for the lungs. Not only are both lungs affected by varying<br />
degrees of hypoplasia depending on the severity of the intrauterine<br />
herniation, but they are also immature.<br />
Recent research has found CDH lungs in more severe cases to<br />
be surfactant deficient 198 and surfactant replacement has been<br />
reported to be successful in certain cases. 199 Thus, the CDH patient<br />
can be described as being term with the lungs of a premature. The<br />
associated pulmonary hypertension is due both to a reduction in<br />
the number of pulmonary vessels and also due to an exaggerated<br />
pulmonary vasoreactivity capable of causing life-threatening<br />
episodes of pulmonary vasospasm leading to profound extrapul<br />
monary right-to-left shunting. The vasoreactivity in CDH<br />
will occasionally produce what has been termed a “honeymoon<br />
period.” In these cases, the patient will have a period of acceptable<br />
gas exchange immediately after birth without the use of any<br />
more extreme ventilatory settings or adjuvant treatments. This<br />
is later followed by very severe pulmonary hypertension associated<br />
with profound hypoxic respiratory failure. Conventional<br />
treatment for the treatment of this situation has been prophylaxis<br />
consisting of deep analgo-sedation, inotropic support, moderate<br />
hyperventila tion if possible, and meticulous control of the<br />
patient’s acid-base status. Previous attempts to treat this situation<br />
with intravenous vasodilators has been abandoned due to the<br />
risk of hypotension, since systemic hypotension can be lifethreatening<br />
in this setting. More modern treatment consists of<br />
surfactant replacement, high frequency oscillatory ventilation,<br />
inhaled nitric oxide, and extracorporeal membrane oxygenation.<br />
The neonatal anesthesio logist might, thus, be faced with<br />
the situation of administering anesthesia to patients either on
1464 PART 5 ■ Anesthetic, Surgical, and Interventional Procedures: Considerations<br />
inhaled nitric oxide 199 or extra corporeal membrane oxygenation<br />
(ECMO). 200<br />
Improved outcome has been reported following preoperative<br />
stabilization of the patient and treatment of pulmonary hyperten -<br />
sion. 201 An interesting phenomenon with the pulmonary hyper -<br />
tension experienced by CDH patients (and some other neonatal<br />
disorders as well, e.g., meconium aspiration syndrome and<br />
idiopathic persistent pulmonary hypertension of the newborn) is<br />
that the tendency to react with severe vasospasm appears to be<br />
time limited and once the patient is through this period pulmo -<br />
nary hypertension will not reappear for the rest of the patient’s life.<br />
However, some patients with pronounced pulmonary hypoplasia<br />
will never come through this period and will develop chronic<br />
pulmonary hypertension as a result. Before this period has passed<br />
the patient can respond with vasospasm to almost any kind of<br />
stressful stimulus and it is readily apparent that emergency surgery<br />
with the release of cytokines and other neuroendocrine stress<br />
factors is not helpful. If on the other hand the patient is stabilized<br />
and has been so for “a hundred hours” without signs of deterio -<br />
ration or episodes of pulmonary vasospasm surgery can be<br />
performed without a stormy intra- and postoperative period. 201<br />
Most patients will eventually fulfill these modern criteria but a<br />
small subsegment will not and will have to be operated on despite<br />
the lack of full stabilization. Such patients are often on advanced<br />
adjuvant treatments (e.g., high-frequency oscillatory ventilation,<br />
inhaled nitric oxide or ECMO), which put very specific demands<br />
on the surgical and anesthetic teams.<br />
One key issue in the treatment of CDH patients is to try to<br />
predict which patients have enough lung tissue to survive with<br />
maximum medical treatment and which patients have pulmonary<br />
hypoplasia of such severity that extrauterine life is not possible.<br />
No specific tests or observations can yet define this with<br />
satisfactory sensitivity and specificity but some indications can be<br />
achieved from the immediate postpartum situation and also<br />
examination of the patient’s red blood cells. If the baby presents<br />
with immediate symptoms and has never shown an acceptable<br />
blood-gas analysis as an indicator of sufficient amount of lung<br />
tissue to sustain gas exchange (lack of “honeymoon period”), this<br />
is a strong indicator of poor prognosis. In severe cases of intrau -<br />
terine herniation, cardiac output will be compromised, leading to<br />
a compensatory erythropoesis. This will cause the occurrence of<br />
significant amounts of immature nucleated erythrocytes at birth.<br />
If the CDH patient displays ≥2.0 10 9 /L of nucleated red blood<br />
cells in the blood stream, this is an significant indicator of a poor<br />
prognosis, and if ≥0.5 10 9 /L ECMO is frequently needed. 202 The<br />
main steps of anesthetic management are listed in Table <strong>86</strong>–20.<br />
Omphalocele<br />
The incidence of the malformation is 1/5000. This abdominal wall<br />
defect can range from minute to very significant with herniation of<br />
parts of the intestine, spleen and the liver. Contrary to gas troschisis,<br />
the herniated viscera will be covered by a hernia sac or mem -<br />
brane. 203 If this membrane has ruptured, the situation might look<br />
very similar to gastroschisis, but a closer inspection of the abdo -<br />
minal wall will disclose the true nature of the condition. Although<br />
they present similar appearances, omphalocele is quite different<br />
from gastroschisis from an embryologic standpoint. Omphalocele<br />
is also much more often associated with other malformations<br />
(mainly cardiac) than gastroschisis, which only represents a<br />
midline fusion failure. Small omphaloceles can be closed without<br />
any problems, whereas larger herniation can cause significant<br />
problems. This is mainly due to the increase in intra-abdominal<br />
pressure resulting from forcing the herniated viscera into an abdo -<br />
minal cavity which is too small. This increase in intra-abdominal<br />
pressure will cause a cephalad shift of the diaphragm, interfering<br />
with ventilation, and will also affect organ blood flow. 204,205 In this<br />
situation, both renal and hepatic function will be impaired. Due to<br />
a reduction in renal perfusion transient oliguria or even anuria tend<br />
to occur and reductions in liver blood flow will reduce the capacity<br />
for hepatic drug clearance. In this situation the terminal half-life<br />
of both renal and hepatic dependent drugs can be significantly<br />
prolonged (e.g., fentanyl, local anesthetics). Forceful closure of the<br />
abdominal defect will also cause significant tension of the skin and<br />
the abdominal wall and necrosis with secondary infection are<br />
frequent complications. To avoid the above the surgeons on<br />
occasion will opt to create a “tent” by artificial material and suspend<br />
this contraption in order to allow gravity to reduce the herniated<br />
viscera gradually by distending the abdominal cavity over a period<br />
of 4 to 7 days. During this period, the tent will be reduced slowly<br />
in the same manner as rolling the end of a tube of tooth paste. The<br />
omphalocele can then usually be closed without any major pro -<br />
blems. Drawbacks with this approach are the risk for infection and<br />
the risk of suture disruption at the wound edges.<br />
Although not an absolute emergency, surgery should be per -<br />
formed as soon as convenient. Proper preoperative stabilization<br />
and investigation must take precedence, but surgery should not<br />
be postponed until the next working day due to the risk of<br />
infection and fluid balance problems. To avoid fluid loss and<br />
evaporative heat loss, the omphalocele should be covered by wet<br />
sponges and a plastic wrap during the preoperative period. Despite<br />
this, close attention has to be paid to preserving body temperature<br />
and an optimal volume and electrolyte status. The main steps of<br />
anesthetic management are summarized in Table <strong>86</strong>–21.<br />
Gastroschisis<br />
The incidence of gastroschisis is 1/10,000. In this condition, the<br />
abdominal wall defect is located in the midline between the<br />
umbilicus and the xiphoid process. Most parts of the gut will<br />
usually be herniated and not covered by any membrane. The gut<br />
does not appear entirely normal but will instead be edematous and<br />
partly covered by fibrin. This malformation is rarely associated<br />
with any other congenital birth defects but a routine search for<br />
mainly cardiac malformations should nevertheless be undertaken.<br />
The diagnosis of this condition is obvious from inspecting the<br />
patient. An intact umbilicus, the location of the herniation and<br />
the lack of any covering membrane/hernia sac distinguishes this<br />
lesion from omphalocele. Clinical handling of this condition will<br />
not in any major way differ from the handling of patients with<br />
more pronounced forms of omphalocele. Thus, for guidelines<br />
please see Table <strong>86</strong>–21.<br />
Intestinal Obstruction<br />
The gastrointestinal tract can be affected by mechanical obstruc -<br />
tion at any location between the pylorus and the anus. The<br />
handling of the more frequent of these disorders will be discussed.<br />
Pyloric Stenosis<br />
This lesion is caused by pathologic hypertrophy of the pyloric<br />
smooth muscle. Neonates rarely display any symptoms of this<br />
condition since the very characteristic forceful projectile type of<br />
vomiting will usually not occur until 4 to 6 weeks of age. 206
CHAPTER <strong>86</strong> ■ Management of the Neonate: Anesthetic Considerations 1465<br />
TABLE <strong>86</strong>-20. Typical Management of a Neonate With Congenital Diaphragmatic Hernia<br />
Symptoms<br />
Preoperative investigations<br />
Monitoring<br />
Suggested anesthetic and<br />
recommendations<br />
ECMO extracorporeal membrane oxygenation.<br />
Recommended Examinations and Management<br />
Tachypnea, various degrees of respiratory distress and cyanosis, absent breath sounds over one<br />
hemithorax, lateral displacement of cardiac sounds, scaphoid abdomen<br />
1. Check that the patient fulfills the golden criterion of 100 hours of stability before surgery,<br />
otherwise request that surgery be postponed until completion of this delay<br />
2. Check the presence of a nasogastric tube allowing decompression of the stomach (prevention of<br />
further respiratory distress caused by a distended intrathoracic stomach)<br />
3. Chest radiograph and echocardiography<br />
4. Routine laboratory, including test for the presence of nucleated erythrocytes<br />
5. Blood type and compatibility test; order 1 unit blood and 1 unit plasma<br />
1. Routine monitoring, invasive blood pressure monitoring in most severe cases<br />
2. Foley catheterization<br />
3. Monitor SpO 2<br />
simultaneously on the right hand and one foot to estimate the severity of<br />
extrapulmonary right-to-left shunting<br />
4. Place a multilumen central venous line (administration of inotropes, sampling of venous blood<br />
gases and for volume infusion)<br />
1. No premedication, I.V. atropine (10 g/kg), preoxygenation<br />
2. Tracheal intubation should be performed after induction if not yet done. Keep spontaneous<br />
ventilation (positive pressure ventilation yields gastric distention and respiratory distress).<br />
3. Inhalational anesthetic is suitable for very stable patients. In unstable patients, opioid anesthetic<br />
(fentanyl 25–50 g/kg) is most appropriate.<br />
4. To optimize analgesia intra- and postoperatively, a continuous regional block is often indicated. If<br />
an epidural technique is used the tip of the catheter must be closed to the dermatome of the skin<br />
incision. If the epidural puncture is not performed at the appropriate thoracic level but threaded<br />
from a caudal or lumbar approach the location of the tip needs to be confirmed by fluoroscopy.<br />
Since the incision is usually a left-sided subcostal incision an ipsilateral T 6–7 continuous thoracic<br />
paravertebral block is an excellent alternative<br />
5. Surgical repair is usually uneventful; hypotension may be due to venous return impairment, if so<br />
give a volume bolus or increase inotropic support. If pneumothorax on the contralateral side,<br />
must be drained. Finally, consider acute episode of pulmonary hypertension with right ventricular<br />
strain and impeded venous return (left heart) and right-sided septal shift (reducing diastolic<br />
volume of left ventricle). Increasing gap between the SpO 2<br />
of the right hand and the foot (increase<br />
in extrapulmonary right-to-left shunt). In this event, give additional bolus of opioid to deepens<br />
anesthesia, increase ventilation and FiO 2<br />
(to improve oxygenation and reduce pCO 2<br />
) and check<br />
acid-base status (correct any acidosis). If this fails, consider administering inhaled nitric oxide.<br />
After reduction of the hernia and closure of the diaphragm, ventilation may be affected (probably<br />
due to changes in anatomic geometry of the diaphragm and lack of space for the content). Ventilation<br />
must be maintained and surgeons informed<br />
6. If the patient is judged to be at risk of sustained pulmonary hypertension, use a ventilator allowing<br />
nitrous oxide administration; however, these ventilators do not allow delivery of volatile agents.<br />
Total intravenous anesthesia is an excellent option. With patient on ECMO, problems with<br />
bleeding will be important due to anticoagulation with heparin<br />
7. Occasionally extubation is possible at the end; most often, ventilation will be needed<br />
Although rare, some patients will present during the late neonatal<br />
period. If the diagnosis has been delayed the patient will become<br />
dehydrated and will also have a combined electrolyte/acid base<br />
disorder. Due to the loss of primarily hydrogen, chloride, and<br />
potassium ions with protracted vomiting the patient will develop<br />
a hypochloremic, hypokalemic alkalosis. Before these patients are<br />
accepted for anesthesia and surgery, they must be rehydrated and<br />
have normal electrolytes and acid-base parameters. Providing<br />
intravenous access and starting the correction of the fluid balance<br />
has a very high priority in these patients. Thus, surgery can and<br />
must wait until the fluid balance has been corrected and can be<br />
delayed without any problems and should be performed during<br />
normal day time. The main steps of anesthetic management are<br />
summarized in Table <strong>86</strong>–22.<br />
Duodenal Obstruction<br />
This is most often caused by duodenal atresia. Depending on<br />
the exact location of the atresia, the vomiting or the drainage<br />
from the nasogastric tube will be discolored by bile. Duodenal<br />
atresia is frequently associated with Down syndrome and the<br />
patient should be checked for physical stigmata associated<br />
with this syndrome. Cardiac malformations are also often<br />
associated with this condi tion, most commonly as part of a Down<br />
syndrome. Other causes of duodenal obstruction are annular<br />
pancreas and choledochal cysts. Due to the nature of the con -<br />
dition, diagnosis is usually made at an early stage and patients<br />
will, thus, not be allowed to develop fluid or electrolyte distur -<br />
bances. The main steps of anesthetic management are listed in<br />
Table <strong>86</strong>–23.
1466 PART 5 ■ Anesthetic, Surgical, and Interventional Procedures: Considerations<br />
TABLE <strong>86</strong>-21. Typical Management of a Neonate Presenting With Omphalocele<br />
Symptoms<br />
Preoperative investigations<br />
Monitoring<br />
Suggested anesthetic and<br />
recommendations<br />
Recommended Examinations and Management<br />
30–40% have congenital heart defects. Midline defects<br />
1. Nearly all patients have paralytic ileus. Nasogastric tube allows decompression of stomach<br />
2. Chest radiograph and echocardiography<br />
3. Routine laboratory with special attention regarding electrolyte status<br />
4. Make sure the patient is not hypovolemic<br />
5. Blood type and compatibility test; Order 1 unit blood and 1 unit plasma<br />
1. Routine monitoring healthy neonates<br />
2. Invasive blood pressure monitoring and Foley catheterization<br />
3. If available, monitor stomach or bladder pressure if primary closure of the defect is expected.<br />
Pressures 20 mmHg significantly reduce cardiac output and hepatic blood flow 205<br />
1. No premedication, I.V. atropine (10 g/kg), preoxygenation<br />
2. Aspirate nasogastric tube and perform a rapid sequence induction<br />
3. Closure of a minor defect and creating a “tent” are usually uneventful; primary closure of a larger<br />
defect is accompanied by a number of problems<br />
4. Maintenance depends on hemodynamic stability. Inhalational or opioid technique indicated. Pain<br />
relief can be provided with epidural which also provide abdominal wall muscle relaxation.<br />
Remember that high intra-abdominal pressure reduces clearance of local anesthetics. Lidocaine<br />
provides better muscle relaxation than bupivacaine and plasma levels are easier to monitor<br />
5. Large insensible water loss (often in excess of 10 mL/kg/h). Volume replacement with albumin or<br />
plasma. Fluids must be warmed. Overhead or convective warming are needed<br />
6. Despite adequate volume replacement hypotension may persists and dopamine infusion is often<br />
needed to achieve normal blood pressure and urine output (severe presentation)<br />
7. Overenthusiastic attempts by the surgeon to close the defect inevitably cause a decrease in blood<br />
pressure and cardiac output and may interfere with ventilation. The surgeon must be alerted and<br />
use an alternative approach (Gortex patch, Silastic tent)<br />
8. Postoperative ventilation support might be needed in the more severe presentation<br />
Intestinal Obstruction<br />
This is most commonly caused by single or multiple atresia of the<br />
small intestine. The symptoms present somewhat later than<br />
duodenal obstruction and an abdominal radiograph will show<br />
classic signs of mechanical ileus. If diagnosed properly patients<br />
rarely deteriorate regarding fluid and electrolyte balance to any<br />
significant degree. The main steps of anesthetic management are<br />
summarized in Table <strong>86</strong>–24.<br />
Malrotation of the Gut<br />
In this condition, the mesentery of the gut has failed to develop in<br />
a normal way. Instead of attaining the normal broad base of the<br />
mesenterium, reaching from the ligament of Treiz to the right iliac<br />
fossa, rotation of the gut will be incomplete, leaving the gut sus -<br />
pended in a mesenterial base which is very narrow at the root of the<br />
superior mesenteric vessels. This sets the stage for the possibility of<br />
rotation of the gut around its own base with concomitant strangula -<br />
TABLE <strong>86</strong>-22. Typical Management of a Neonate Presenting With Pyloric Stenosis<br />
Symptoms<br />
Preoperative investigations<br />
Monitoring<br />
Suggested anesthetic and<br />
recommendations<br />
Recommended Examinations and Management<br />
Forceful projectile vomiting after feeding. Look for signs of dehydration. Palpable olive-like<br />
resistance to the right in the epigastrium. Ultrasonographic examination will usually provide the<br />
final diagnosis<br />
1. A nasogastric tube should be passed at the same time the diagnosis is made<br />
2. Make sure signs of dehydration are not present. Check or inquire about urine output during the<br />
last couple of hours. Inspect the diaper<br />
3. Routine laboratory with special attention regarding electrolyte and acid-base status. Sodium,<br />
potassium, and chloride values should be normal. Do not accept base excess values above 2<br />
Routine monitoring<br />
1. No premedication, I.V. atropine (10 g/kg), preoxygenation<br />
2. Reduce stomach volume and content by aspirating the nasogastric tube<br />
3. Rapid sequence induction. Maintenance with volatile agents. Relaxation indicated during<br />
pyloromyotomy to avoid duodenal tears<br />
4. Infiltration of the wound edges with a long acting local anesthetic (bupivacaine or ropivacaine)<br />
will ensure high quality pain relief in the immediate postoperative period. Narcotics should not<br />
be used for risk of postoperative hypoventilation or apnea
TABLE <strong>86</strong>-23. Typical Management of a Neonate Presenting With Duodenal Atresia<br />
Symptoms<br />
Preoperative investigations<br />
Monitoring<br />
Suggested anesthetic and<br />
recommendations<br />
CHAPTER <strong>86</strong> ■ Management of the Neonate: Anesthetic Considerations 1467<br />
Recommended Examinations and Management<br />
Classic signs of intestinal obstruction. An abdominal radiograph is usually diagnostic due<br />
to the presence of the “double bubble” signs, which consists of two large air-filled structures<br />
(stomach and proximal duodenum separated by the pylorus) in the epigastric region<br />
1. Check the presence of a nasogastric tube<br />
2. Make sure signs of dehydration are not present<br />
3. Routine laboratory (electrolyte and acid-base status)<br />
4. Blood type and compatibility test and order 1 unit blood<br />
1. Routine monitoring<br />
2. Invasive blood pressure monitoring<br />
1. No premedication, I.V. atropine (10 g/kg), preoxygenation<br />
2. Try to empty the stomach by aspirating the nasogastric tube<br />
3. Rapid sequence induction<br />
4. Since the patient will be subjected to fairly extensive upper abdominal surgery a continuous<br />
epidural block supplemented by a light volatile agent maintenance anesthetic is often a good<br />
choice<br />
5. Central venous catheter placement might be mandatory, not for anesthetic purposes but for<br />
postoperative total parenteral nutrition since enteral nutrition will usually be delayed<br />
tion of the mesenteric vessels. This will lead to an ischemic<br />
paralysis of the gut which does not have to have any mechanical<br />
obstructive component associated. If prolonged the gut ischemia<br />
will cause a combined situation of ileus, hypovole mia, and sepsis/<br />
endotoxemia from translocation of intestinal bacteria. Thus, these<br />
patients will often present in an unstable state. However, this<br />
represents one of the very few real emergen cies within neonatal<br />
surgery, since failure to treat this condition rapidly can cause severe<br />
harm to the patient. Either necrosis of almost the entire small<br />
intestine will occur and leave the patient and the family with the<br />
lifelong problems associated with the short bowel syndrome or the<br />
condition might become fatal or require a very long period of<br />
intensive care due to overwhelming sepsis/endotoxemia. The<br />
emergency nature of this condition cannot be overemphasized and<br />
stabilization of the circulation, correction of fluid and electrolyte<br />
deficits and other necessary measures needs to be performed<br />
simultaneously with starting and maintainin the anesthetic! The<br />
main steps of anesthetic management are listed in Table <strong>86</strong>–25.<br />
Anal Atresia<br />
This malformation should be identified as part of the routine<br />
examination of each newborn baby. The atresia can be classified as<br />
low, intermediate, or high. If an adequate fistula (most often<br />
rectovaginal fistula in females) is not present the baby will need<br />
some surgical intervention to allow reasonable drainage of the<br />
gastrointestinal tract. In the case of a low, membranous atresia<br />
definitive correction is possible but in the case of a higher atresia<br />
final repair will be deferred until later, and drainage will be<br />
accomplished by the formation of a colostomy. Since diagnosis is<br />
usually made early, the neonate will almost always be in good<br />
clinical condition for the anesthesia.<br />
TABLE <strong>86</strong>-24. Typical Management of a Neonate Presenting With Intestinal Obstruction<br />
Symptoms<br />
Preoperative investigations<br />
Monitoring<br />
Suggested anesthetic and<br />
recommendations<br />
Recommended Examinations and Management<br />
Classic signs of intestinal obstruction. An abdominal radiograph is usually diagnostic showing<br />
traditional signs of mechanical obstruction<br />
1. Check the presence of a nasogastric tube<br />
2. Make sure signs of dehydration are not present<br />
3. Routine laboratory with special attention regarding electrolyte and acid-base status<br />
4. Blood type and compatibility test and order 1 unit blood<br />
1. Routine monitoring. Invasive blood pressure monitoring when indicated<br />
1. No premedication, I.V. atropine (10 g/kg), preoxygenation<br />
2. Try to empty the stomach by aspirating the nasogastric tube<br />
3. Rapid sequence induction<br />
4. Since the patient will be subjected to extensive upper abdominal surgery a continuous<br />
epidural block supplemented by a light volatile agent maintenance anesthetic is a good<br />
choice<br />
5. Contrary to duodenal atresia the surgical procedure will most often involve resection of the<br />
bowel. Due to third spacing within the mesenterium volume replacement with 5% albumin<br />
or plasma is usually required to maintain adequate intravascular volume<br />
6. As with duodenal atresia, a central venous catheter might be mandatory for postoperative<br />
nutritional purposes (parenteral nutrition)
1468 PART 5 ■ Anesthetic, Surgical, and Interventional Procedures: Considerations<br />
TABLE <strong>86</strong>-25. Typical Management of a Neonate Presenting With Malrotation of the Gut<br />
Symptoms<br />
Preoperative investigations<br />
Monitoring<br />
Suggested anesthetic and<br />
recommendations<br />
Recommended Examinations and Management<br />
Sicker aspect than “ordinary” intestinal obstruction: dehydration, frank hypovolemia and sepsis.<br />
Pain and discomfort is more intense than in other neonatal occlusion due to bowel ischemia.<br />
X-rays will often not show any signs of mechanical obstruction but instead a picture of<br />
paralytic ileus<br />
1. Check the presence of a nasogastric tube<br />
2. Electrolyte and acid-base status. Coagulation profile is needed since coagulopathy is not<br />
infrequent. Do not wait for the results before going to the operating theater<br />
3. Blood type and compatibility test<br />
4. Order 2 units of blood and 2 units of fresh frozen plasma<br />
5. Check that adequate antibiotic prophylaxis/treatment is started immediately<br />
1. Routine monitoring<br />
2. Invasive blood pressure monitoring in severe presentations<br />
3. Foley catheterization with hourly urine output measurements<br />
1. No premedication, I.V. atropine (10 g/kg), preoxygenation<br />
2. Try to empty the stomach by aspirating the nasogastric tube<br />
3. Rapid sequence induction. Maintenance depends on patient’s hemodynamic status and clinical<br />
presentation. Opioid and/or inhalational anesthesia techniques appropriate<br />
4. In presence of coagulopathy, epidural anesthesia should be denied or postponed until the end of<br />
the surgery<br />
5. Two large bore venous access. A central venous line might be useful<br />
6. Administer syringe boluses (5% albumin, plasma or packed red cells) according to blood pressure.<br />
If hypotension persists consider dopamine infusion<br />
7. Check regularly blood glucose, hematocrit, electrolytes and ionized calcium, arterial blood gas<br />
analysis and coagulation parameters<br />
8. Untwisting of the gut release vasoactive substances and lactic acid into the circulation yielding<br />
hypotension. Volume, inotropic support and correction of acid-base status<br />
9. Most patients will require postoperative ventilatory support in the NICU<br />
Inguinal Hernia Repair<br />
Repair of a inguinal hernia is most often delayed until the baby is<br />
passed the neonatal period. (see <strong>Chapter</strong> 54) However, if the size<br />
is very significant and give raise to pain or intermittent episodes<br />
of incarceration surgery might be necessary in the first few weeks<br />
of life (for inguinal hernia repair in the ex-premature baby please<br />
see below).<br />
Necrotizing Enterocolitis<br />
This is a severe complication seen almost exclusively in premature<br />
children. The cause of this complication is most likely<br />
multifactorial, but intestinal ischemia with secondary bacterial<br />
overgrowth appears as a key factor. The premature baby will<br />
present with abdominal distention, increasing gastric aspirates and<br />
micro- or macroscopic gastrointestinal bleeding. Signs of general<br />
sepsis are also frequently present. Withholding enteral feeding and<br />
starting parenteral nutrition and antibiotic treatment will usually<br />
handle the situation, but in severe cases perforation of the gut<br />
might supervene, which necessitates surgical intervention.<br />
However, patients with an intestinal perforation are generally very<br />
sick and unstable and will present the anesthesiologist with a<br />
significant challenge. Crucial to success is preoperative circulatory<br />
support by volume replacement and inotropic agents as well as<br />
appropriate antibiotic treatment. The current surgical trend is to<br />
insert only one or more abdominal drainage tubes and refrain<br />
from performing acute intestinal resections and enterostomies.<br />
This is a significant advantage from an anesthetic perspective and<br />
is likely to increase the baby’s chances of surviving. Further<br />
surgery can be performed at a later stage when the patient has<br />
recovered. The main steps of anesthetic management are<br />
summarized in Table <strong>86</strong>–26.<br />
Bladder Exstrophy<br />
In this malformation, there is a defect midline fusion of the uri -<br />
nary bladder, the symphysis, and the urethra. The interior of the<br />
bladder will be exposed and the mucosa and the ureteral orifices<br />
can be observed. Care should be taken to cover the area with wet<br />
sponges in order not to cause secondary injury and infection due<br />
to drying of the mucosa. Prophylactic antibiotics should be started<br />
and the patient should be scheduled for operative repair as soon<br />
as possible during normal working hours. The surgery is often<br />
associated with moderate blood loss and transfusion is almost<br />
always necessary in these patients. In order to close the symphysis,<br />
a inferior pubic ramus osteotomy is frequently required. Posto -<br />
peratively the legs are often suspended, similar to patients with<br />
bilateral femoral fractures, in order not to cause undue stress on<br />
the symphysis. A specific concern in these patients is the risk for<br />
the subsequent development of latex allergy. Care should be taken<br />
not to expose these babies to latex (e.g., surgical gloves, tapes, face<br />
masks) 207 (see <strong>Chapter</strong> 45). The main steps of anesthetic manage -<br />
ment are summarized in Table <strong>86</strong>–27.<br />
Myelomeningocele 208,209<br />
Myelomeningocele (MMC) is associated with an incomplete<br />
closure of the neural tube (see <strong>Chapter</strong> 58). This will obviously be
TABLE <strong>86</strong>-26. Typical Management of a Neonate With Necrotizing Enterocolitis<br />
Symptoms<br />
Preoperative investigations<br />
Monitoring<br />
Suggested anesthetic and<br />
recommendations<br />
CHAPTER <strong>86</strong> ■ Management of the Neonate: Anesthetic Considerations 1469<br />
Recommended Examinations and Management<br />
1. Abdominal distention, feeding problems associated with increased gastric aspirates, micro- or<br />
macroscopic gastrointestinal bleeding<br />
2. Hypovolemic/septic appearance. Laboratory signs of infection/sepsis<br />
3. Abdominal x-rays: paralytic ileus with gas in the intestinal wall and, in severe cases, the portal vein.<br />
If perforation has occurred, free intra-abdominal gas is present<br />
1. Check the presence of a nasogastric tube<br />
2. Routine laboratory panel including C-reactive protein and white cell count<br />
3. Coagulation parameters, arterial blood gas analysis. Correct any degree of acidosis<br />
4. Determine degree of dehydration and hypovolemia and correct accordingly<br />
5. Echocardiography (look for signs of hypovolemia and decreased myocardial contractility). Check<br />
for signs of pulmonary hypertension<br />
6. Chest radiograph. Look for signs of acute respiratory distress syndrome and bronchopulmonary<br />
dysplasia<br />
1. Routine monitoring<br />
2. Invasive blood pressure monitoring<br />
3. Foley catheterization with measurement of hourly urine output<br />
1. No premedication, I.V. atropine (10 g/kg), preoxygenation<br />
2. Most babies are already intubated and mechanically ventilated in the NICU. If not, rapid sequence<br />
induction should be performed. If the baby is severely septic or hemodynamically unstable,<br />
ketamine should be used as induction agent. Opioid maintenance anesthetic is often preferred in<br />
order to maintain hemodynamic stability<br />
3. Dopamine or dopexamine infusion will be used to improve cardiac output and splanchnic<br />
perfusion before anesthesia and surgery. If not, it should be readily available. High infusion rate<br />
should be used (10–15 mL/kg/h) and volume supported with 5% albumin, fresh frozen plasma and<br />
packed red cells. Epinephrine infusion might be needed to support cardiac output and systemic<br />
blood pressure<br />
4. If urine output remains low despite volume loading and a low-dose dopamine infusion, administer<br />
iteratively small doses of furosemide (0.5 mg/kg)<br />
5. Due to the risk of coagulopathy, avoid epidural techniques despite potential benefits. Postoperative<br />
analgesia can be achieved by continuous morphine infusion<br />
associated with a varying degree of neural dysfunction below the<br />
level of the MMC and will also predispose to early infection<br />
unless rapid surgical closure is undertaken and appropriate<br />
antibiotic coverage provided. This lesion is often associated with<br />
hydrocephalus and the later development of an Arnold–Chiari<br />
type II syndrome. Large MMCs or MMCs at a higher level are<br />
often more complex to handle. Due to the risk of secondary<br />
infection and to improve the handling of the patients surgical<br />
closure should be performed as soon as convenient. Before surgery<br />
the MMC should be covered by wet sponges to counteract drying<br />
of the tissues and an attempt at assessing the neurologic function<br />
below the lesion should be performed. Antibiotic coverage must<br />
be instituted at once. Special issues with these patients are how to<br />
position the patient during tracheal intubation in order not to put<br />
undue pressure on the MMC. These patients also are very likely to<br />
develop latex allergy. 207 The main steps of anesthetic management<br />
are summarized in Table <strong>86</strong>–28.<br />
Surgery on the NICU Graduate<br />
Overview<br />
These patients do most often belong to one of two groups. Either<br />
the neonatal period has been relatively uneventful despite the<br />
baby being born preterm, thus, leaving the child almost completely<br />
healthy or with only minor residual medical problems. In this<br />
case, anesthesia is relatively straightforward. On the other hand,<br />
the preterm baby might have been on ventilatory support for<br />
extended time periods, complicated by, e.g., repeated sepsis<br />
episodes, cerebral hemorrhage, patent ductus arteriosus, and/<br />
or necrotizing enterocolitis. Patients in the latter group will often<br />
be on multiple medications (e.g., diuretics, digoxin, antiepileptics,<br />
inhaled steroids, and b2-agonists). Such babies will frequently<br />
have developed a moderate to severe degree of bronchopulmonary<br />
dysplasia/chronic lung disease of the newborn and tracheal<br />
extubation has often been accomplished with great difficulty.<br />
Most of these ex-premature babies will still be on a continuous<br />
positive airway pressure device or will receive supplemental<br />
oxygen by nasal prongs. Postoperative apnea is a cause of concern<br />
in this patient category and the time period during which<br />
the infants are at risk will be significantly longer than 44 to<br />
60 postconceptual weeks (see “Ventilation Function and Control”)<br />
and often the risk for postoperative apnea is still present up to<br />
6 to 12 months of age. Since the neonatologists so often have<br />
had great difficulty in extubating these children, both the neona -<br />
tologists and the parents are reluctant to have the child reintubated<br />
if surgery and anesthesia becomes necessary. The anesthesiologist<br />
should try to respect these concerns and when ever possible<br />
try to use alternative but safe techniques in order to try to<br />
avoid tracheal intubation. Below the two most frequent situation<br />
where the anesthesiologist will meet the NICU graduate will be<br />
outlined.
1470 PART 5 ■ Anesthetic, Surgical, and Interventional Procedures: Considerations<br />
TABLE <strong>86</strong>-27. Typical Anesthetic Management of a Neonate Presenting With Bladder Exstrophy<br />
Symptoms<br />
Preoperative investigations<br />
Monitoring<br />
Suggested anesthetic and<br />
recommendations<br />
Recommended Examinations and Management<br />
Obvious from looking at the baby<br />
1. Routine laboratory panel<br />
2. Cardiac echocardiography<br />
3. Blood type and screen<br />
4. Order 1 unit blood and 1 unit plasma<br />
5. Check that adequate antibiotic prophylaxis/treatment is started immediately and that the defect is<br />
covered by wet sponges<br />
1. Routine monitoring<br />
2. Invasive blood pressure monitoring<br />
1. Make sure the patient is not exposed to latex<br />
2. No premedication, I.V. atropine (10 g/kg), preoxygenation<br />
3. Intravenous or inhalational induction appropriate. Tracheal intubation is indicated due to<br />
prolong surgery. No special requirement for maintenance.<br />
4. Due to extensive surgical reconstruction and postoperative need for some immobility of the<br />
lower limbs, a lumbar epidural block should be considered.<br />
5. Hemodynamically stable and normothermic patients can be extubated following emergence from<br />
anesthesia.<br />
Retinopathy of the Premature (ROP)<br />
The cause for this condition was previously believed to be hypero -<br />
xia secondary to overenthusiastic administration of oxygen during<br />
the early neonatal period. Increasing degrees of prematurity and<br />
repeated sepsis episodes are currently seen as more fundamental<br />
predisposing factors for the development of ROP than hyperoxia.<br />
Briefer episodes of hyperoxia, as often happens during anesthesia<br />
of these infants, is currently not believed to be so dangerous in<br />
this regard. The retinal lesions will be treated with a laser or with<br />
a cryothermic probe (or a combination). The ophthalmologists<br />
will need free access to the patients eyes and will, thus, interfere<br />
with the anesthesiologists possibilities to handle the airway. Thus,<br />
face mask ventilation is usually not practical since the anesthe -<br />
siologists hands need to be out of the operating field. Despite the<br />
often small size of these infants (1–2 kg body weight) the use of the<br />
laryngeal mask airway will often avert the need for tracheal<br />
intubation. 122 Crucial for the successful return to the previous level<br />
of respiratory support prior to the anesthetic, is to expose the<br />
patient to as few medications as possible and to use only drugs<br />
with a very short effect duration. 122 The use for example of<br />
thiopental should be considered contraindicated since the halflife<br />
is excessively long in these babies. 117<br />
Inguinal Hernia Repair<br />
Awake caudal or spinal anesthesia can successfully be performed<br />
in the ex-premature infant 210–212 and will circumvent the problem<br />
of general anesthesia and tracheal intubation. The risk for<br />
postoperative apnea will also be reduced with these methods<br />
compared to general anesthesia. However, supplementation of<br />
these blocks by any sedative drugs, including ketamine, 213 will<br />
TABLE <strong>86</strong>-28. Typical Anesthetic Management of a Neonate Presenting With Myelomeningocele<br />
Symptoms<br />
Preoperative investigations<br />
Monitoring<br />
Suggested anesthetic<br />
and recommendations<br />
Recommended examinations and management<br />
Obvious from routine inspection of the patient<br />
1. Routine laboratory panel.<br />
2. Blood type and screen. Order 1 units of blood and 1 units of plasma.<br />
3. Check that adequate antibiotic prophylaxis/treatment is started immediately and that the<br />
defect is covered by wet sponges<br />
1. Routine monitoring<br />
2. If large undermining of the skin needed for closure, invasive blood pressure monitoring<br />
might be indicated.<br />
1. Make sure the patient is not exposed to latex<br />
2. No premedication, IV atropine (10 g/kg) and preoxygenation<br />
3. Intravenous or inhalational induction and maintenance per choice<br />
4. If general anesthesia is used tracheal intubation is mandatory because of the duration of<br />
surgery and the prone position. To minimize the risk for accidental dislodgment of the<br />
tracheal tube nasal intubation is recommended. To avoid pressure damage of the nervous<br />
structures within the MMC, tracheal intubation can be performed in the lateral position.<br />
Custom made support pads with a hole cut for the MMC can also be used for tracheal<br />
intubation in the supine position.<br />
5. Most patient will be extubated at the end of the procedure.
CHAPTER <strong>86</strong> ■ Management of the Neonate: Anesthetic Considerations 1471<br />
increase the risk for the development of apnea in the postoperative<br />
period. Although the risk for apnea will be reduced by an awake<br />
regional technique these patients should still be closely supervised<br />
overnight. 214 The limited duration of both caudal and especially<br />
spinal blocks in this age group will make it difficult to perform<br />
bilateral inguinal hernia repairs with these techniques without<br />
intravenous or volatile supplementation at the end of the<br />
procedure. Clonidine will significantly prolong the duration of<br />
caudal blocks 215 and co-administration of 1 g/kg of clonidine<br />
together with bupivacaine will usually prolong the duration in expremature<br />
babies sufficiently to allow bilateral repair. In the<br />
author’s experience the use of adjuvant clonidine administration<br />
in this setting has not been associated with any noticeable increase<br />
of postoperative apneic episodes although this still needs to<br />
be verified scientifically. Although awake caudal anesthesia is<br />
advantageous compared to general anesthesia in this patient<br />
category it should be remembered that the bolus dose of<br />
bupivacaine needed to provide an adequate block might produce<br />
signs of early central nervous system toxicity due to systemic<br />
absorption of the local anesthetic. 164 In this respect an awake spinal<br />
block might be preferable, since a lesser amount of local anesthetic<br />
is needed to accomplish an adequate block with this technique. If<br />
by some reason awake regional techniques are not appropriate the<br />
same method described above (see “Retinopathy of the Prema -<br />
ture”), complemented by either a caudal or ilioinguinal block for<br />
intra- and postoperative analgesia, should be considered in an<br />
attempt to avoid tracheal intubation.<br />
Circumcision<br />
Circumcision is often performed in the neonatal period due to<br />
religious beliefs or parental preference. Adequate anesthesia or<br />
regional anesthesia is obviously an obligatory part of this minor<br />
procedure. Failure to do so in not only inhumane and represents<br />
unacceptable clinical practice but will also cause long-term altera -<br />
tions in pain perception. 4 A brief face-mask volatile anesthetic or<br />
a penile block are acceptable options. A eutectic mixture of local<br />
anesthetics (EMLA cream) is used by some practitioners in this<br />
setting but this method does not provide sufficient analgesia in<br />
most cases.<br />
CONCLUSION<br />
In the current era of changing demographics, with a rapidly in -<br />
creasing number of older and sicker patients, the anesthesio logist<br />
might occasionally question the ethical and moral value of the<br />
medical work at hand. In this situation, pediatric anesthesia in<br />
general, and neonatal anesthesia in particular, will provide the<br />
anesthesiologist with an unique opportunity to make a true<br />
difference in patients with their entire life span ahead of them.<br />
However, this is an endeavor that should not be undertaken lightly<br />
but instead with the utmost care and professionalism. The<br />
successful performance of neonatal anesthesia will depend on a<br />
combination of a thorough understanding of the specific charac -<br />
teristics of perinatal physiology and pharmacology, adequate basic<br />
training and maintenance of manual skills as well as the availability<br />
of proper equipment and perioperative facilities. If lacking in any<br />
of the above aspects necessary for the safe and successful conduct<br />
of neonatal anesthesia the practitioner should not hesitate to<br />
consult more experienced colleagues or transfer the patient to a<br />
center better equipped to take care of small babies.<br />
REFERENCES<br />
1. Shearer MH. Surgery on paralyzed, unanesthetized newborn. Birth<br />
19<strong>86</strong>;13:79.<br />
2. Berry FA, Gregory GA. Do premature infants require anesthesia for<br />
surgery? Anesthesiology 1987;67:291–293.<br />
3. Anand KJS, Sippel WG, Aynsley-Green A. Randomized trial of fentanyl<br />
anesthesia in preterm neonates undergoing surgery: Effects on stress<br />
response. Lancet 1987;i:243–248.<br />
4. Taddio A, Goldbach M, Ipp M, et al. Effect of neonatal circumcision on<br />
pain responses during vaccination in boys. Lancet 1994;344:291–292.<br />
5. Anand KJS, Carr DB. The neuroanatomy, neurophysiology, and<br />
neurochemistry of pain, stress, and analgesia in newborns and children.<br />
Pediatr Clin North Am 1989;36:795–822.<br />
6. Cohen MM, Cameron CB, Duncan PG. Pediatric Anesthesia morbidity<br />
and mortality in the perioperative period. Anesth Analg 1990;70:160–167.<br />
7. Morray JP, Geiduschek JM, Ramamoorthy C, et al. Anesthesia-related<br />
cardiac arrest in children: initial findings of the Pediatric Perioperative<br />
Cardiac Arrest (POCA) Registry. Anesthesiology. 2000;93:6–14.<br />
8. Keenan RL, Sharpiro JH, Kane FR, et al. Bradycardia during anesthesia in<br />
infants: An epidemiologic study. Anesthesiology 1994;80:976–982.<br />
9. Lunn JN. Implications of the national confidential enquiry into perio -<br />
perative deaths for paediatric anaesthesia. Paediatr Anaesth 1992;2:<br />
69–72.<br />
10. The report of the joint working group. The transfer of infants and children<br />
for surgery. London, UK: British Paediatric Association; 1993.<br />
11. Ikonomidou C, Bosch F, Miksa M, Bittigau P, Vöckler J, Dikranian K,<br />
Tenkova TI, Stefovska V, Turski L, Olney JW. Blockade of NMDA<br />
receptors and apoptotic neurodegeneration in the developing brain.<br />
Science 1999;283(5398):70–4.<br />
12. Jevtovic-Todorovic V, Hartman RE, Izumi Y, Benshoff ND, Dikranian K,<br />
Zorumski CF, Olney JW, Wozniak DF. Early exposure to common anes -<br />
thetic agents causes widespread neurodegeneration in the developing<br />
rat brain and persistent learning deficits. J Neurosci 2003 Feb 1;23(3):<br />
876–82.<br />
13. Mellon RD, Simone AF, Rappaport BA Use of anesthetic agents in<br />
neonates and young children. Anesth Analg 2007;104(3):509–20.<br />
14. Anand KJ, Soriano SG. Anesthetic agents and the immature brain: are<br />
these toxic or therapeutic? Anesthesiology 2004;101(2):527–30.<br />
15. Anand KJS, Phil D, Hickey PR. Pain and its effects in the human neonate<br />
and fetus. N Eng J Med 1987;317:1321–1329.<br />
16. Giannakoulopoulos X, Sepulveda W, Kourtis P, et al. Fetal plasma cortisol<br />
and -endorphin response to intrauterine needling. Lancet 1994;344:<br />
77–81.<br />
17. Hauser KF, McLaughin PJ, Zagon IS. Endogenous opioids regulate<br />
dendritic growth and spine formation in developing rat brain. Brain Res<br />
1987;416:157–161.<br />
18. Stiene-Martin A, Hauser KF. Opioid-dependent growth of glial cultures:<br />
suppression of astrocyte DNA synthesis by met-enkephalin. Life Sciences<br />
1990;46:91–98.<br />
19. Kornblum HI, Loughlin SE, Leslie FM. Effects of morphine on DNA<br />
synthesis in neonatal rat brain. Develop Brain Res 1987;31:45–52.<br />
20. Aynsley-Green A. Pain and stress in infancy and childhood—where to<br />
now? Paediat Anaesth 1996;6:167–172.<br />
21. Anand KJS, Brown MJ, Causon RC, et al. Can the human neonate mount<br />
an endocrine and metabolic response to surgery? J Pediatr Surg<br />
1985;20:41–48.<br />
22. Anand KJS, Phil D, Hansen DD, et al. Hormonal-metabolic stress res -<br />
ponses in neonates undergoing cardiac surgery. Anesthesiology 1990;73:<br />
661–670.<br />
23. Anand KJS, Aynsley-Green A. Measuring the severity of surgical stress<br />
in neonates. J Pediatr Surg 1988;23:297–305.<br />
24. Anand KJS, Phil D, Hickey PR. Halothane-morphine compared with<br />
high-dose sufentanil for anesthesia and postoperative analgesia in<br />
neonatal surgery. N Eng J Medicine 1992;326:1–9<br />
25. Rudolph AM, Heymann MA. Circulatory changes during growth in the<br />
fetal lamb. Circul Res 1970;26:289–299.<br />
26. Clarke WR. The transitional circulation: Physiology and anesthetic<br />
implications. J Clin Anesth 1990;2:192–211.<br />
27. Kinsella JP, Abman SH. Recent developments in the pathophysiology and<br />
treatment of persistent pulmonary hypertension of the newborn. J Pediatr<br />
1995;126:853–<strong>86</strong>4.<br />
28. Lönnqvist PA and the ENPNOSG. Inhaled nitric oxide in newborn and<br />
paediatric patients with pulmonary hypertension and moderate to severe
1472 PART 5 ■ Anesthetic, Surgical, and Interventional Procedures: Considerations<br />
impaired oxygenation: effects of doses of 3-100 parts per million. Intens<br />
Care Med 1997;23:773–779.<br />
29. Nassar R, Reedy MC, Anderson PA. Developmental changes in the<br />
ultrastructure and sarcomere shortening of the isolated rabbit ventricular<br />
myocyte. Circul Res 1987;61:465–483.<br />
30. St John Sutton MG, Raichlen JS, Reichek N, et al. Quantitative assessment<br />
of growth and function of the cardiac chambers in the normal human<br />
fetus: A prospective longitudinal echocardiographic study. Circulation<br />
1984;69:645–654.<br />
31. Jarmakani JM, Nakanishi T, George BL, et al. Effects of extracellular<br />
calcium on myocardial mechanical function in the neonatal rabbit.<br />
Develop Pharmacol Ther 1982;5:1–13.<br />
32. Kaufman TM, Horton JW, White DJ, et al. Age-related changes in myo -<br />
cardial relaxation and sarcoplasmatic reticulum. Am J Physiol 1990;259:<br />
H309–316.<br />
33. Palmisano BW, Mehner RW, Stowe DF, et al. Direct myocardial effects of<br />
halothane and isoflurane: Comparison between adult and infant rabbits.<br />
Anesthesiology 1994;81:718–729.<br />
34. Anversa P, Olivetti G, Loud AV. Morphometric study of early postnatal<br />
development in the left and right ventricular myocardium of the rat. I.<br />
Hypertrophy, hyperplasia, and binucleation of myocytes. Circul Res<br />
1980;46:495–502.<br />
35. Fisher DJ, Heymann MA, Rudolph AM. Myocardial consumption of<br />
oxygen and carbohydrates in newborn sheep. Pediatr Res 1981;15:<br />
843–846.<br />
36. Fisher DJ. Left ventricular oxygen consumption and function in hypoxe -<br />
mia in conscious lambs. Am J Physiol 1983;244:H664.<br />
37. Mask WK, Abd-Elfattah AS, Jessen M, et al. Embryonic versus adult<br />
myocardium: adenine nucleotide degradation during ischemia. Ann Thor<br />
Surg. 1989;48:109–112.<br />
38. Papp JG. Autonomic responses and neurohumeral control in the early<br />
antenatal heart. Basic Res Cardio 1988;83:2–9.<br />
39. Kojima M, Ishima T, Taniguchi N, et al. Developmental changes in betaadrenoreceptors,<br />
muscarinic cholinoceptors and Ca 2 channels in rat<br />
ventricular muscles. Br J Pharmacol 1990;99:334–339.<br />
40. Ursell PC, Ren CL, Danilo P Jr. Anatomic distribution of autonomic<br />
neural tissue in the developing dog heart: I. Sympathetic innervation.<br />
Anatomic Record 1990;226:71–80.<br />
41. Rockson SG, Homey CJ, Quinn P, et al. Cellular mechanisms of impaired<br />
adrenergic responsiveness in neonatal dogs. J Clin Invest 1981;67:319–327.<br />
42. Artman M, Kithas PA, Wike JS, et al. Inotropic responses during postnatal<br />
maturation in rabbit. Am J Physiol 1988;255:H335–342.<br />
43. Lagercrantz H, Slotkin TA.The stress of being born. Scientific American<br />
19<strong>86</strong>;254:92–102.<br />
44. Teitel DF, Klautz R, Steendijk P, et al. The end-systolic pressure-volume<br />
relationship in the newborn lamb: Effects of loading and inotropic<br />
interventions. Pediatr Res 1991;29:473–482.<br />
45. Klopfenstein HS, Rudolph AM. Postnatal changes in the circulation and<br />
responses to volume loading in sheep. Circul Res 1978;42:839–845.<br />
46. Winberg P, Lundell BPW. Left ventricular stroke volume and output in<br />
healthy term infants. Am J Perinatol 1990;7:223–226.<br />
47. Winberg P, Jansson M, Marions L, et al. Left ventricular output during<br />
postnatal circulatory adaptation in healthy infants born at term. Arch Dis<br />
Child 1989;64:1374–1378.<br />
48. Winberg P, Ergander U. Relationship between changes in heart rate, left<br />
ventricular output and stroke volume in preterm infants during<br />
fluctuation in heart rate. Pediatr Res 1992;31:117.<br />
49. Gilbert RD. Effects of afterload and baroreceptors on cardiac function in<br />
fetal sheep. J Develop Physiol 1982;4:299–309.<br />
50. Teitel DF, Iwamoto HS, Rudolph AM. Effects of birth-related events on<br />
central blood flow patterns. Pediatr Res 1987;23:557–566.<br />
51. Baum VC, Palmisano BW. The immature heart and anesthesia. Anes -<br />
thesiology 1997;87:1529–1548.<br />
52. Rigatto H. Maturation of breathing control in the fetus and newborn<br />
infant. In: Beckerman RC, Brouillette RT, Hunt CE, editors. Respiratory<br />
Disorders in Infants and Children. Baltimore: Williams & Wilkins; 1992.<br />
pp. 352–370.<br />
53. Rigatto H, Kalapesi Z, Leahy FN, et al. Ventilatory response to 100% and<br />
15% oxygen during wakefulness and sleep in preterm infants. Early<br />
Human Development 1982;7:1–10.<br />
54. Kelly DH, Stellwagen LM, Kaitz E, et al. Apnea and periodic breathing in<br />
normal full-term infants during the first twelve months. Pediatr Pul -<br />
monology 1985;1:215–219.<br />
55. Lagercrantz H, Milerad J, Walker DW. Control of ventilation of the<br />
neonate. In: Crystal RG, West JP, editors. The Lung: Scientific Founda -<br />
tions. 2nd ed. Philadelphia: Lippincott-Raven Publishers; 1997.<br />
pp. 1463–1473.<br />
56. Steward DJ. Preterm infants are more prone to complications following<br />
minor surgery than are term infants. Anesthesiology 1982;56:304–306.<br />
57. Coté CJ, Zaslavsky A, Downes JJ, et al. Postoperative apnea in former<br />
preterm infants after inguinal herniorrhaphy: a combined analysis.<br />
Anesthesiology 1995;82:809–822.<br />
58. Fisher DM. When is the ex-premature infant no longer at risk for apnea?<br />
Anesthesiology 1995;82:807–808.<br />
59. Ochiai R, Gothrie K, Motoyama EK. Differential sensitivity of halothane<br />
anesthesia on genioglossus, intercostals, and diaphragm in kittens. Anesth<br />
Analg 1992;74:338–344.<br />
60. Benameur M, Goldman MD, Ecoffey C, et al. Ventilation and thoraco -<br />
abdominal asynchrony during halothane anesthesia in infants. J Applied<br />
Physiol 1993;74:1591–1596.<br />
61. Ochiai R, Gothrie K, Motoyama EK. Effects of varying concentrations of<br />
halothane on the activity of the genioglossus, intercostals, and diaphragm<br />
in cats: an electromyographic study. Anesthesiology 1989;70:812–816.<br />
62. Motoyama EK. Respiratory physiology in infants and children. In:<br />
Motoyama EK, editor. Smith's Anesthesia for Infants and Children. 5th ed.<br />
St. Louis: CV Mosby Company; 1990. pp. 11–76.<br />
63. Cree JE, Meyer J, Hailey DM. Diazepam in labour: its metabolism and<br />
effect on the clinical condition and thermogenesis of the newborn. Brit<br />
Med J 1973;4:251–255.<br />
64. Miller RP, Roberts RJ, Fisher LJ. Acetaminophen elimination kinetics in<br />
neonates, children and adults. Clinical Pharmacology Therapeutics 1976;<br />
19:284–294.<br />
65. Lynn AM, Slattery JT. Morphine pharmacokinetics in early infancy.<br />
Anesthesiology 1987;66:136–139.<br />
66. Bartels H. Drug therapy in childhood: What has been done and what has<br />
to be done. Pediatr Pharmacology 1983;3:131–143.<br />
67. Morselli PL, Franco-Morselli R, Bossi L. Clinical pharmacokinetics in<br />
newborns and infants. Clinical Pharmacokinetics 1980;5:485–527.<br />
68. Aranda JV. Methylxanthine metabolism in the newborn infant. In: Soyka<br />
LF, Redmond, editors. Drug Metabolism in the Immature Human. New<br />
York: Raven Press; 1981. pp. 183–193.<br />
69. Leakey JE, Althaus ZR, Bailey JR, et al. Dexamethasone increases UDPglucuronyl<br />
transferase activity towards bilirubin, oestradiol and<br />
testosterone in foetal liver from rhesus monkey during late gestation.<br />
Biochem J 1985;225:183–188.<br />
70. Leakey JEA, Althaus ZR, Bailey JR, et al. Dexamethasone induces hepatic<br />
cytochrome P-450 content and increases certain monooxygenase acti -<br />
vities in rhesus monkey fetuses. Biochem Pharmacol 19<strong>86</strong>;35:1389–1391.<br />
71. Kardish R, Feuer G. Relationship between maternal progesterone and<br />
the delayed drug metabolism in the neonate. Biol Neonate 1972;20:<br />
58–67.<br />
72. Wishart GJ. Functional heterogenicity of UDP-glucuronyltransferase as<br />
indicated by its differential development and inducibility by gluco -<br />
corticoids: Biochem J 1978;174:485.<br />
73. Leaky JEA, et al. Dexamethasone induces hepatic cytochome P-450<br />
content and increases certain monooxygenase activities in rhesus monkey<br />
fetuses. Biochem Pharmacol 19<strong>86</strong>;35:1389.<br />
74. Simpson VJ, Chung LWK. Programming of rat hepatic arylhydrocarbon<br />
hydroxylase activity during late neonatal period. Proc West Pharmacol Soc<br />
1982;25:257–261.<br />
75. Goldenthal EI. A compilation of LD50 values in newborn and adult<br />
animals. Toxicol Appl Pharmacol 1971;18:185–207.<br />
76. Green MD, Shires TK, Fisher LJ. Hepatotoxicity of acetaminophen in<br />
neonatal and young rats. I. Age-related changes in hepatotoxicity. Toxicol<br />
Appl Pharmacol 1984;74:116–124.<br />
77. Crestiel T, et al. Drug-metabolizing enzymes in human foetal liver: Partial<br />
resolution of multiple cytochromes P450. Pediatr Pharmacology<br />
1982;2:199.<br />
78. Lerman J, Strong HA, LeDez KM, et al. Effects of age on the serum<br />
concentration of 1-acidglycoprotein and the binding of lidocaine in<br />
pediatric patients. Clin Pharmacol Ther 1989;46:219–225.<br />
79. Avner ED. Embryogenesis and anatomic development of the kidney. In:<br />
Polin RP, Fox WW, editors. Fetal and Neonatal Physiology. Philadelphia:<br />
WB Saunders Company; 1992. pp. 1181–1187.<br />
80. Seikaly MG, Arant BS. Development of renal hemodynamics: Glomerular<br />
filtration and renal blood flow. Clinical Perinatology 1992;19:1–13.
CHAPTER <strong>86</strong> ■ Management of the Neonate: Anesthetic Considerations 1473<br />
81. Rubin MI. Maturation of renal function in childhood: Clearance studies.<br />
Journal of Clinical Investigation 1949;28:1144.<br />
82. Jose PA, Slotkoff LM, Montgomery S, et al. Autoregulation of renal blood<br />
flow in the puppy. Am J Physiol 1975;229:983–988.<br />
83. Guignard JP, Torrado A, Da Cunha O, et al. Glomerular filtration rate<br />
during the first three weeks of life. J Pediatr 1975;87:268–272.<br />
84. Aperia A, Broberger O, Thodenius K, et al. Development of the renal<br />
control of salt and fluid homeostasis during the first year of life. Acta<br />
Paed Scand 1975;64:393–398.<br />
85. Engle WD. Development of fetal and neonatal renal function. Seminars<br />
in Perinatology 19<strong>86</strong>;10:113–124.<br />
<strong>86</strong>. Siegel S, Oh W. Renal function as a marker of human fetal maturation.<br />
Acta Paed Scand 1976;65:481–485.<br />
87. Friis-Hansen B. Body water compartments in children: changes during<br />
growth and related changes in body composition. Pediatrics 1961;<br />
28:169.<br />
88. Bennett EJ, Bowyer DE. Fluid and electrolyte balance. In: Sumner E,<br />
Hatch DJ, editors. Textbook of Paediatric Anaesthetic Practice. London:<br />
Baillière Tindall; 1989. pp. 179–211.<br />
89. Siker D. Pediatric fluids, electrolytes, and nutrition. In: Polin RP, Fox<br />
WW, editors. Fetal and Neonatal Physiology. Philadelphia: WB Saunders<br />
Com pany; 1992. pp. 83–117.<br />
90. Wassner SJ. Altered growth and protein turnover in rats fed sodiumdeficient<br />
diets. Pediatr Res 1989;26:608–613<br />
91. Dicker A, Ohlsson KBE, Johnson L, et al. Halothane selectively inhibits<br />
nonshivering thermogenesis: Possible implications for thermoregulation<br />
during anesthesia of infants. Anesthesiology 1995;82:491–501.<br />
92. Ohlsson KBE, Mohell N, Cannon B, et al. Thermogenesis in brown<br />
adipocytes is inhibited by volatile anesthetic agents: A factor contributing<br />
to hypothermia in infants? Anesthesiology 1994;81:176–183.<br />
93. Plattner O, Semsroth M, Dessler DI, et al. Lack of nonshivering thermo -<br />
genesis in infants anethetized with fentanyl and propofol. Anesthesiology<br />
1997;<strong>86</strong>:758–759.<br />
94. Sessler DI. Temperature regulation. In: Gregory GA, editor. Pediatric<br />
Anesthesia. 3rd ed. New York: Churchill Livingstone; 1994. pp. 47–81.<br />
95. Sessler DI. Perioperative thermoregulation and heat balance. Ann NY<br />
Acad Sci 1997;813:757–777.<br />
96. Andrew M, Paes B, Johnston M. Development of the hemostatic system<br />
in the neonate and young infant. Am J Pediatr Hematol/Oncol<br />
1990;12:95–104.<br />
97. Haizinger B, Gombotz H, Rehak P, et al. Activated thrombelastogram<br />
in neonates and infants with complex congenital heart disease in<br />
comparison with healthy children. Br J Anaesth. 2006;97(4):545–52.<br />
98. Haas T, Preinreich A, Oswald E, et al. Effects of albumin 5% and artificial<br />
colloids on clot formation in small infants. Anaesthesia. 2007;62(10):<br />
1000–7.<br />
99. Charlton AJ, Davies JM, Rimmer S. Anaesthesia and brain damage in<br />
the newborn. Anaesthesia 1989;44:641–643.<br />
100. Kain ZN. Parental presence during induction of anaesthesia. Paediatr<br />
Anaesth 1995;5:209–212.<br />
101. Kain ZN, Ferris CA, Mayes LC, et al. Parental presence during induction<br />
of anaesthesia: practice differences between United States and Great<br />
Britain. Paediatr Anaesth 1996;6:187.<br />
102. Campell FA, McLeod ME, Bissonnette B, Swartz JS. End-tidal carbon<br />
dioxide measurement in infants and children during and after general<br />
anaesthesia. Can J Anaesth 1994;41:107–110.<br />
103. Halpern L, Bissonnette B. The most proximal and accurate site for<br />
sampling end-tidal CO 2<br />
in infants. Can J Anaesth 1994;41:984–990.<br />
104. Dullenkopf A, Kolarova A, Schulz G, et al. Reproducibility of cerebral<br />
oxygenation measurement in neonates and infants in the clinical<br />
setting using the NIRO 300 oximeter. Pediatr Crit Care Med. 2005;6(3):<br />
344–7.<br />
105. Weiss M, Dullenkopf A, Kolarova A, et al. Near-infrared spectroscopic<br />
cerebral oxygenation reading in neonates and infants is associated with<br />
central venous oxygen saturation. Paediatr Anaesth. 2005;15(2):102–9.<br />
106. Davidson AJ. Measuring anesthesia in children using the EEG. Paediatr<br />
Anaesth. 2006;16(4):374–87.<br />
107. Klockars JG, Hiller A, Ranta S, et al. Spectral entropy as a measure of<br />
hypnosis in children. Anesthesiology. 2006;104(4):708–17.<br />
108. Ironfield CM, Davidson AJ. AEP-monitor/2 derived, composite auditory<br />
evoked potential index (AAI-1.6) and bispectral index as predictors<br />
of sevoflurane concentration in children. Paediatr Anaesth. 2007;17(5):<br />
452–9.<br />
109. Lynn AM, Bradford H, Kantor ED, et al. Postoperative ketorolac<br />
tromethamine use in infants aged 6–18 months: the effect on morphine<br />
usage, safety assessment, and stereo-specific pharmacokinetics. Anesth<br />
Analg. 2007;104(5):1040–51.<br />
110. Peeters MY, Prins SA, Knibbe CA, et al. Propofol pharmacokinetics and<br />
pharmacodynamics for depth of sedation in nonventilated infants after<br />
major craniofacial surgery. Anesthesiology. 2006;104(3):466–74.<br />
111. Bouwmeester NJ, Anderson BJ, Tibboel D, et al. Developmental<br />
pharmacokinetics of morphine and its metabolites in neonates, infants<br />
and young children. Br J Anaesth. 2004;92(2):208–17.<br />
112. Anderson BJ, Pons G, Autret-Leca E, et al. Pediatric intravenous<br />
paracetamol (propacetamol) pharmacokinetics: a population analysis.<br />
Paediatr Anaesth. 2005;15(4):282–92.<br />
113. Allegaert K, de Hoon J, Verbesselt R, et al. Maturational pharmaco -<br />
kinetics of single intravenous bolus of propofol. Paediatr Anaesth.<br />
2007;17(11):1028–34.<br />
114. Allegaert K, Anderson BJ, Verbesselt R, et al. Tramadol disposition in<br />
the very young: an attempt to assess in vivo cytochrome P-450 2D6<br />
activity. Br J Anaesth. 2005;95(2):231–9<br />
115. Morrison JE Jr, Collier E, Friesen RH, et al. Preoxygenation before<br />
laryngoscopy in children: how long is enough? Paediatr Anaesth 1998;<br />
8:293–298.<br />
116. Patel R, Lenscyk M, Hannalah RS, et al. Age and onset of desaturation<br />
in apnoeic children. Can J Anaesth 1994;41:771–774.<br />
117. Kingston HG, Kendrick A, Sommer KM, et al. Binding of thiopental in<br />
neonatal serum. Anesthesiology 1990;72:428–431.<br />
118. Martin PH, Murthy BVS, Petros AJ. Metabolic, biochemical and<br />
haemodynamic effects of infusion of propofol for long-term sedation of<br />
children undergoing intensive care. Br J Anaesth 1997;79:276–279.<br />
119. Lerman J, Sikich N, Kleinman S, et al. The pharmacology of sevoflurane<br />
in infants and children. Anesthesiology 1994;80:814–824.<br />
120. Doi M, Ikeda K. Respiratory effects of sevoflurane. Anesthesia and<br />
Analgesia 1987;66:241–244.<br />
121. Brown K, Aun C, Stocks J, et al. A comparison of the respiratory effects<br />
of sevoflurane and halothane in infants and young children. Anesthesio -<br />
logy 1998;89:<strong>86</strong>–92.<br />
122. Lönnqvist PA. Successful use of laryngeal mask airway in low-weight<br />
ex-premature infants undergoing cryotherapy for retinopathy of the<br />
premature. Anesthesiology 1995;83:422<br />
123. Brimacombe J. Use of laryngeal mask airway in very small neonates.<br />
Anesthesiology 1994;81:1302.<br />
124. Paterson SJ, Byrne PJ, Molesky MG, et al. Neonatal resuscitation using<br />
the laryngeal mask airway. Anesthesiology 1994;80:1248–1253.<br />
125. Rowbottom SJ, Simpson DL, Grubb D. The laryngeal mask in children:<br />
A fibreoptic assessment of positioning. Anaesthesia 1991;46:489–491.<br />
126. Spahr-Schopfer IA, Bissonnette B, Hartley EJ. Capnography and the<br />
paediatric laryngeal mask airway. Can J Anaesth 1993;40:1038–1043.<br />
127. Chibber AK, Fickling K, Kolano JW, et al. Comparison of end-tidal and<br />
arterial carbon dioxide in infants using laryngeal mask airway and<br />
endotracheal tube. Anesth Analg 1997;84:51–53.<br />
128. Cook-Sather SD, Tulloch HV, Canan A, et al. A comparison of awake<br />
versus paralyzed tracheal intubation for infants with pyloric stenosis.<br />
Anesth Analg 1998;<strong>86</strong>:945–951.<br />
129. von Ungern-Sternberg BS, Hammer J, Schibler A, et al. Decrease of<br />
functional residual capacity and ventilation homogeneity after<br />
neuromuscular blockade in anesthetized young infants and preschool<br />
children. Anesthesiology. 2006;105(4):670–5.<br />
130. Hassid S, Nicaise C, Michel F, et al. Randomized controlled trial of<br />
sevoflurane for intubation in neonates. Paediatr Anaesth. 2007;17(11):<br />
1053–8.<br />
131. Magnusson L, Zemgulis V, Tenling A, et al. Use of a vital capacity<br />
maneuver to prevent atelectasis after cardiopulmonary bypass: an<br />
experimental study. Anesthesiology 1998;8:134<br />
132. McDonald PF, Van Der Walt JH, Parnis SJ. A timed reexpansion inspi -<br />
ratory manoeuvre (TRIM) for treating oxyhaemoglobin desaturation in<br />
children following a period of apnoea- studies in an animal model.<br />
Paediatr Anaesth 1998;8:409–412.<br />
133. Deakers TW, Reynolds G, Stretton M, et al. Cuffed endotracheal tubes<br />
in pediatric intensive care. J Pediatr 1994;125:57–62.<br />
134. Holzki J. Laryngeal damage from tracheal intubation. Paediatr Anaesth<br />
1997;7:435–437.<br />
135. Frei FJ, Ummenhofer W. Difficult intubation in paeditrics. Paediatr<br />
Anaesth 1996;6:251.
1474 PART 5 ■ Anesthetic, Surgical, and Interventional Procedures: Considerations<br />
136. Meakin G, McKiernan EP, Morris P, et al. Dose-response curves for<br />
suxamethonium in neonates, infants and children. Br J Anaesth<br />
1989;62:655–658.<br />
137. Meakin G, Morton RH, Wareham AC. Age-dependent variation in<br />
response to tubocurarine in the isolated rat diaphragm. Br J Anaesth<br />
1992;68:161–163.<br />
138. Meakin G, Shaw EA, Baker RD, et al. Comparison of atracuriuminduced<br />
neuromuscular blockade in neonates, infants and children. Br<br />
J Anaesth 1988;60:171–175.<br />
139. Meretoja OA. Neuromuscular blocking agents in paediatric patients:<br />
influence of age on the response. Anaesth Intens Care 1990;18:440–448.<br />
140. Meretoja OA, Wirtavuori K, Neuvonen PJ. Age-dependence of the doseresponse<br />
curve of vecuronium in pediatric patients during balanced<br />
anesthesia. Anesth Analg 1988;67:21–26.<br />
141. Meretoja OA, Luosto T. Dose-response characteristics of pancuronium<br />
in neonates, infants and children. Anaesth Intens Care 1990;18:455–459.<br />
142. Meretoja OA. Is vecuronium a long-acting neuromuscular blocking<br />
agent in neonates and infants? Br J Anaesth 1989;62:184–187.<br />
143. Marrarro G. Intraoperative ventilation. Paediatr Anaesth 1998;8:<br />
373–382.<br />
144. Lin YC, Brock-Utne JG. Paediatric anaesthetic breathing systems.<br />
Paediatr Anaesth 1996;6:1–5.<br />
145. Peters JWB, Bezstarosti-Van Eeden J, Erdmann W, et al. Safety and<br />
efficacy of semiclosed circle ventilation in small infants. Paediatr Anaesth<br />
1998;8:299–304.<br />
146. Nilsson K. Respiratory physiology in pediatric anesthesia. Curr Opin<br />
Anaesth 1990;3:335–338.<br />
147. Tan SSW, Sury MRJ, Hatch DJ. The “educated hand” in Paediatric<br />
Anaesthesia does it exist? Paediatr Anaesth 1993;3:291–295.<br />
148. Murat I, Lapeyere G, Saint-Maurice C. Isoflurane attenuates baroreflex<br />
control of heart rate in human neonates. Anesthesiology 1989;70:<br />
395–400.<br />
149. Murray D, Vandewalker G, Matherne P, et al. Pulsed Doppler and twodimensional<br />
echocardiography: comparison of halothane and isoflurane<br />
on cardiac function in infants and children. Anesthesiology 1987;67:<br />
211–217.<br />
150. Barash PG, Glanz S, Katz JD, et al. Ventricular function in children<br />
during halothane anesthetic: an echocardiographic evaluation. Anes -<br />
thesiology 1978;49:79–85.<br />
151. Murray D, Metha MP, Forbes R, et al. Additive contribution of nitrous<br />
oxide to halothane MAC in infants and children. Anesth Analg 1990;71:<br />
120–124.<br />
152. Murray D, Metha MP, Forbes R. Additive contribution of nitrous<br />
oxide to isoflurane MAC in infants and children. Anesthesiology 1991;75:<br />
1<strong>86</strong>–190.<br />
153. Liu H, Wang L, Eaton M, Schaefer S. Sevoflurane preconditioning limits<br />
intracellular/mitochondrial Ca2 in ischemic newborn myocardium.<br />
Anesth Analg. 2005;101(2):349–55.<br />
154. Wong GT, Luginbuehl I, Karsli C, Bissonnette B. The effect of<br />
sevoflurane on cerebral autoregulation in young children as assessed by<br />
the transient hyperemic response. Anesth Analg. 2006;102(4):1051–5.<br />
155. Koehntop DE, Rodman JH, Brundage DM, et al. Pharmacokinetics of<br />
fentanyl in neonates. Anesth Analg 19<strong>86</strong>;65:227–232.<br />
156. Greely WJ, de Bruijn NP, Davis DP. Sufentanil pharmacokinetics in<br />
pediatric cardiovascular patients. Anesth Analg 1987;66:1067–1072.<br />
157. Bösenberg AT, Hadley GP, Wiersma R. Oesophageal atresia: caudothoracic<br />
epidural anaesthesia reduces the need for postoperative<br />
ventilatory support. Pediatr Surgery International 1992;7:289–291.<br />
158. Larsson BA, Lönnqvist PA, Olsson GL. Total and free plasma concentra -<br />
tions of bupivacaine associated with continuous lumbar epidural<br />
infusion in neonates. Anesth Analg 1997;84:501–505.<br />
159. Wolf AR, Doyle E, Thomas E. Modifying infant stress responses to major<br />
surgery: spinal vs extradural vs opioid analgesia. Paediatr Anaesth<br />
1998;8:305–311.<br />
160. Hoehn T, Jetzek-Zader M, Blohm M, et al. Early peristalsis following<br />
epidural analgesia during abdominal surgery in an extremely low birth<br />
weight infant. Paediatr Anaesth. 2007;17(2):176–9.<br />
161. Llewellyn N, Moriarty A. The national pediatric epidural audit. Paediatr<br />
Anaesth. 2007;17(6):520–33.<br />
162. Larsson BA, Olsson GL, Lönnqvist PA. Plasma concentrations of<br />
bupivacaine in young infants after continuous epidural infusion.<br />
Paediatr Anaesth 1994;4:159–162.<br />
163. Berde CB. Toxicity of local anesthetics in infants and children. J Pediatr<br />
1993;122:S14.<br />
164. Breschan C, Hellstrand E, Likar R, et al. Early signs of toxicity and<br />
“subtoxic” conditions in infant monitoring: bupivacaine plasma levels<br />
following caudal anesthesia. Der Anaesthesist 1998;47:290–294.<br />
165. Lönnqvist PA. Plasma levels of lignocaine after thoracic paravertebral<br />
blockade in infants and children. Anaesthesia 1993;48:958–960.<br />
166. Tander B, Baris S, Karakaya D, et al. Risk factors influencing inadvertent<br />
hypothermia in infants and neonates during anesthesia. Paediatr<br />
Anaesth. 2005;15(7):574–9.<br />
167. Lindahl S. Energy expenditure and fluid and electrolyte requirements<br />
in anesthetized infants and children. Anesthesiology 1988;69:377–382.<br />
168. Holliday MA, Segar WE. Maintenance need for water in parenteral fluid<br />
therapy. Pediatrics 1957;19:823.<br />
169. Larsson LE, Nilsson K, Niklasson A, et al. Influence of fluid regimens<br />
on perioperative blood-glucose concentrations in neonates. Br J Anaesth<br />
1990;64:419–424.<br />
170. Human albumin administration in critically ill patients: systematic<br />
review of randomised controlled trials. Cochrane Injuries Group<br />
Albumin Reviewers. Br Med J 1998;317:235–240.<br />
171. Stoddart PA, Rich P, Sury MRJ. A comparison of 4.5% human albumin<br />
solution and Haemacel in neonates undergoing major surgery. Paediatr<br />
Anaesth 1996;6:103–106.<br />
172. Beebe DS, Beck D, Belani KG. Clinical management of infants and<br />
newborn babies undergoing major surgery utilizing a rapid infusion<br />
device. Paediatr Anaesth 1994;4:115–121.<br />
173. Jonmarker C, Werner O. Blod och blodersättning. Jonmarker C, Werner<br />
O (eds), Barnanestesi, Studentlitteratur, Lund, Sweden, 1990.<br />
174. Leclair MD, Plattner V, Mirallie E, et al. Laparoscopic pyloromyotomy<br />
for hypertrophic pyloric stenosis: a prospective, randomized controlled<br />
trial. J Pediatr Surg. 2007;42(4):692–8.<br />
175. Tobias JD. Anaesthesia for minimally invasive surgery in children. Best<br />
Pract Res Clin Anaesth 2002;16:115–130.<br />
176. Veyckemans F. Celioscopic surgery in infants and children: the<br />
anesthesiologist’s point of view. Paediatr Anaesth. 2004;14(5):424–32.<br />
177. Pacilli M, Pierro A, Kingsley C, et al. Absorption of carbon dioxide dur -<br />
ing laparoscopy in children measured using a novel mass spectrometric<br />
technique. Br J Anaesth 2006;97:215–219.<br />
178. Böttcher-Haberzeth S, Dullenkopf A, Gitzelmann CA, et al. Tracheal<br />
tube displacement during laparoscopy in children. Anaesthesia<br />
2007;62:131–134.<br />
179. Huettemann E, Sakka SG, Petrat G, et al. Left ventricular regional wall<br />
motion abnormalities during pneumoperitoneum in children. Br J<br />
Anaesth 2003;90:733–736.<br />
180. Terrier G. Anaesthesia for laparoscopic procedures in infants and<br />
children: indications, intra- and postoperative management and<br />
treatment of complications. Curr Opin Anaesthesiol 1999;12:311–314.<br />
181. Krosnar S, Baxter A. Thoracoscopic repair of esophageal atresia with<br />
tracheoesophagealfistula: anesthetic and intensive care management of<br />
a series of eight neonates. Paediatr Anaesth. 2005;15(7):541–6.<br />
182. Mariano ER, Chu LF, Albanese CT, et al. Successful thoracoscopic repair<br />
of esophageal atresia with tracheoesophageal fistula in a newborn with<br />
single ventricle physiology. Anesth Analg. 2005;101(4):1000–2.<br />
183. Büttner W, Finke W, Hilleke M, et al. Entwicklung eines Fremdbeoba -<br />
chtungsbogens zur Beurteilung des postoperativen Schmerzes bei<br />
Säuglingen. Anästh Intensiv Notfall Schmerz 1998;33:353–361.<br />
184. Krechel SW, Bildner J. CRIES: a new neonatal postoperative pain<br />
measurement score. Initial testing of validity and reliability. Paediatr<br />
Anaesth 1995;5:53–61.<br />
185. Suraseranivongse S, Kaosaard R, Intakong P, et al. A comparison of<br />
postoperative pain scales in neonates. Br J Anaesth. 2006;97(4):540–4.<br />
1<strong>86</strong>. Lin YC, Sussman HH, Benitz WE. Plasma concentrations after rectal<br />
administration of acitaminophen in preterm neonates. Paediatr Anaesth<br />
1997;7:457–459.<br />
187. Anderson BJ, Holford NHG, Wollard GA. Paracetamol kinetics in<br />
neonates. Anaesth Intens Care 1997;25:721–722.<br />
188. Giaufré E, Dalens B, Gombert A. Epidemiology and morbidity of regio -<br />
nal anesthesia in children: a one year prospective survey of the French-<br />
Language Society of Pediatric Anesthesiologists. Anesth Analg 1996;<br />
83:897–900.<br />
189. Kart T, Christrup LL, Rasmussen M. Recommended use of morphine in<br />
neonates, infants and children based on a literature review: part<br />
2-clinical use. Paediatr Anaesth 1997;7:93–101.<br />
190. Sandström K, Nilsson K, Andreasson S, et al. Early postoperative<br />
lipid administration after neonatal surgery. Acta Paed Scand 1994;83:<br />
249–254.
CHAPTER <strong>86</strong> ■ Management of the Neonate: Anesthetic Considerations 1475<br />
191. Reynolds RM, Bass KD, Thureen PJ. Achieving positive protein balance<br />
in the immediate postoperative period in neonates undergoing<br />
abdominal surgery. J Pediatr. 2008;152(1):63–7.<br />
192. Badgwell JM, McLeod ME, Friedberg J. Airway obstruction in infants<br />
and children. Can J Anaesth 1987;34:90–98.<br />
193. Holzki J, Laschat M, Stratmann C. Stridor in the neonate and infant.<br />
Implications for the paediatric anaesthetist. Prospective description of<br />
155 patients with congenital and acquired stridor in early infancy.<br />
Paediatr Anaesth 1998;8:221–227.<br />
194. Stephens P, Saunders P, Bingham R. Neonatal cleft lip repair: a retrospec -<br />
tive review of anaesthetic complications. Paediatr Anaesth 1997;7:<br />
33–36.<br />
195. Low J, Robinson SJ, Brown TCK. Type IV laryngotracheoesophageal<br />
cleft in a neonate. Paediatr Anaesth 1992;2:73–76.<br />
196. Lim SK, Fadhilah T, Ibitsan I. Type IV laryngotracheo-oesophageal cleftmanagement<br />
of a difficult airway. Paediatr Anaesth 1998;8:337–340.<br />
197. George DK, Cooney TP, Chu BK, et al. Hypoplasia and immaturity of the<br />
terminal lung unit (acinus) in congenital diaphragmatic hernia. Am Rev<br />
Resp Dis 1987;136:947–950.<br />
198. Wilcox DT, Glick PL, Karamanoukian HL, et al. Contributions by<br />
individual lungs to the surfactant status in congenital diaphragmatic<br />
hernia. Pediatr Res 1997;41:6<strong>86</strong>–691.<br />
199. Glick PL, Leach CL, Besner GE, et al. Pathophysiology of congenital<br />
diaphragmatic hernia III: exogenous surfactant therapy for the high-risk<br />
neonate with CDH. J Pediatr Surg 1992;27:<strong>86</strong>6–<strong>86</strong>9.<br />
200. Wilson JM, Bowler LK, Lund DP. Evolution of the technique of con -<br />
genital diaphragmatic hernia repair on ECMO. J Pediatr Surg 1994;29:<br />
1109–1112.<br />
201. Charlton AJ, Bruce J, Davenport M. Timing of surgery in congenital<br />
diaphragmatic hernia: low mortality after preoperative stabilisation.<br />
Anaesthesia 1991;46:820–823.<br />
202. Green DW, Lyon J, Ackerman NB et al. Nucleated erythrocyte count in<br />
newborn infants with left-sided congenital diaphragmatic hernia:<br />
relationship with the need for extracorporeal membrane oxygenation<br />
and survival. J Pediatr 1995;127:131–133.<br />
203. Langer JC. Gastroschisis and omphalocele. Semin Pediatr Surg 1996;5:<br />
124–128.<br />
204. Masey SA, Buck JR, Koehler RC, et al. Effects of increased intraabdominal<br />
pressure on regional blood flow in newborn lambs.<br />
Anesthesiology 1983;59:A425.<br />
205. Wesley JR, Drongowski R, Coran AG. Intragastric pressure measure -<br />
ment: a guide for reduction and closure of the silastic chimney in<br />
omphalocele and gastroschisis, J Pediatr Surg 1981;16:264–270.<br />
206. MacDonald NJ, Fitzpatrick GJ, Moore KP, et al. Anaesthesia for con -<br />
genital hypertrophic pyloric stenosis. Br J Anaesth 1987;59:672–677.<br />
207. Porri F, Pradal M, Lemière C, et al. Association between latex sensitiza -<br />
tion and repeated latex exposure in children. Anesthesiology 1997;<strong>86</strong>:<br />
599–602.<br />
208. Delgado JMS, Soto RH, Martin MJV, et al. Anaesthetic considerations for<br />
myelomeningocele in neonates. Paediatr Anaesth 1998;8:363–364.<br />
209. Viscomi CM, Abajian JC, Wald SL, et al. Spinal anesthesia for repair of<br />
myleomeningocele in neonates. Anesth Analg 1995;81:492–495.<br />
210. Spear RM, Deshpande JK, Maxwell LG. Caudal anesthesia in the awake,<br />
high-risk infant. Anesthesiology 1988;69:407–409.<br />
211. Gunter JB, Watcha MF, Forestner JE, et al. Caudal epidural anesthesia in<br />
conscious premature and high-risk infants. J Pediatr Surg 1991;26:9–14.<br />
212. Welborn LG, Rice LJ, Hannallah RS, et al. Postoperative apnea in former<br />
preterm infants: prospective comparison of spinal and general anes -<br />
thesia. Anesthesiology 1990;72:838–842.<br />
213. Tashiro C, Matsui Y, Nakano S, et al. Respiratory outcome in extremely<br />
premature infants following ketamine anaesthesia. Can J Anaesth 1991;<br />
38:287–291.<br />
214. Cox GC, Goresky GV. Life-threatening apnea following spinal anesthesia<br />
in former premature infants. Anesthesiology 1990;73:345–347.<br />
215. Jamali S, Monin S, Begon C, et al. Clonidine in pediatric caudal anes -<br />
thesia. Anesth Analg 1994;78:663–666.













