

Chapter 129

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Training and Education in<br />
Pediatric Anesthesia<br />
Paul J. Samuels, Jon Tomasson, and Charles D. Kurth<br />
<strong>129</strong><br />
CHAPTER<br />
INTRODUCTION<br />
The practice of medicine is rapidly evolving as powerful forces<br />
impact health care in the 21st century. The expanding body of<br />
biomedical knowledge, the explosive development of information<br />
technology, and a renewed focus on patient safety are profoundly<br />
altering the professional activities of physicians. This is especially<br />
true of pediatric anesthesiology. Both the way specialists in our<br />
discipline care for patients and the technology with which care is<br />
provided are undergoing tremendous change.<br />
Although progress and innovation have significant potential to<br />
advance health care quality, it is only through education that these<br />
developments can be successfully incorporated into medical<br />
practice. The challenge of contemporary medical education was<br />
articulated in a report from the Institute of Medicine’s Committee<br />
on the Roles of Academic Health Centers in the 21st Century 1 :<br />
“Among all of the academic health center roles, education will<br />
require the greatest changes in the coming decade. We regard<br />
education as one of the primary mechanisms for initiating a<br />
cultural shift toward an emphasis on the needs of patients and<br />
populations and a focus on improving health, using the best of<br />
science and the best of caring.” This chapter will discuss how the<br />
tectonic shifts shaping health care are altering training in pediatric<br />
anesthesiology, and how these changes will influence the practice<br />
of our specialty in the future.<br />
Changes in Medical Education<br />
The same forces impacting health care are also transforming<br />
medical education. The dictum “see one, do one, teach one” so<br />
common a generation ago, is now an educational anachronism. In<br />
the past, it was assumed that students learned merely as a result of<br />
participation in clinical activities. Metrics for successful education<br />
were primarily knowledge based, with little attention paid to<br />
patient outcome or practitioner technical skill. Students commonly<br />
“learned by doing,” even when their educational activities put<br />
patients at risk. This approach to medical education is no longer<br />
acceptable socially, professionally, or politically. 2<br />
Educators in recent years have adopted a model that focuses<br />
on the end product of training—the competent physician—rather<br />
than on the educational process itself. This is referred to as<br />
“outcome-based education,” an approach to learning in which<br />
educational outcomes are specified, which in turn determines<br />
curricular content, teaching methods, and assessment tools. 3 This<br />
shift in educational philosophy has dramatically changed the<br />
nature and structure of training programs in our field, providing<br />
an impetus for the development of new methods of teaching,<br />
learning, and assessment.<br />
New Models in Teacher Development<br />
The first step in creating organized educational programs that<br />
produce physicians responsive to the demands of contemporary<br />
medicine is to develop highly capable teachers. In recent years,<br />
educational activities have become more complex and now<br />
demand expertise in new teaching methodologies, including<br />
problem based learning, simulation, and e-learning. As teaching<br />
has evolved, so too has the recognition that the skills required<br />
of the outstanding instructor that may differ from those of the<br />
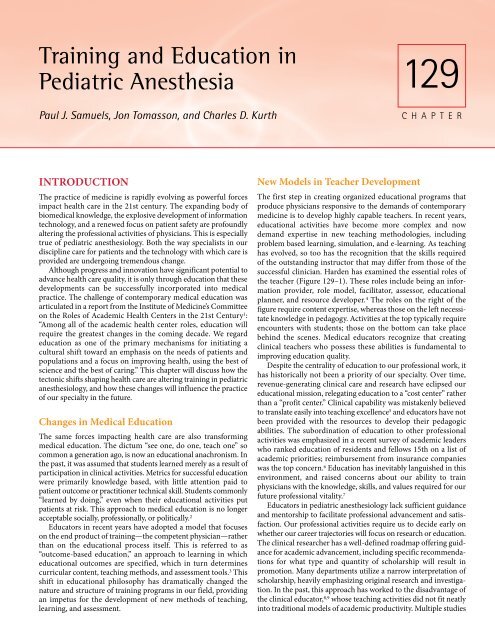
successful clinician. Harden has examined the essential roles of<br />
the teacher (Figure <strong>129</strong>–1). These roles include being an information<br />
provider, role model, facilitator, assessor, educational<br />
planner, and resource developer. 4 The roles on the right of the<br />
figure require content expertise, whereas those on the left necessitate<br />
knowledge in pedagogy. Activities at the top typically require<br />
encounters with students; those on the bottom can take place<br />
behind the scenes. Medical educators recognize that creating<br />
clinical teachers who possess these abilities is fundamental to<br />
improving education quality.<br />
Despite the centrality of education to our professional work, it<br />
has historically not been a priority of our specialty. Over time,<br />
revenue-generating clinical care and research have eclipsed our<br />
educational mission, relegating education to a “cost center” rather<br />
than a “profit center.” Clinical capability was mistakenly believed<br />
to translate easily into teaching excellence 5 and educators have not<br />
been provided with the resources to develop their pedagogic<br />
abilities. The subordination of education to other professional<br />
activities was emphasized in a recent survey of academic leaders<br />
who ranked education of residents and fellows 15th on a list of<br />
academic priorities; reimbursement from insurance companies<br />
was the top concern. 6 Education has inevitably languished in this<br />
environment, and raised concerns about our ability to train<br />
physicians with the knowledge, skills, and values required for our<br />
future professional vitality. 7<br />
Educators in pediatric anesthesiology lack sufficient guidance<br />
and mentorship to facilitate professional advancement and satisfaction.<br />
Our professional activities require us to decide early on<br />
whether our career trajectories will focus on research or education.<br />
The clinical researcher has a well-defined roadmap offering guidance<br />
for academic advancement, including specific recommendations<br />
for what type and quantity of scholarship will result in<br />
promotion. Many departments utilize a narrow interpretation of<br />
scholarship, heavily emphasizing original research and investigation.<br />
In the past, this approach has worked to the disadvantage of<br />
the clinical educator, 8,9 whose teaching activities did not fit neatly<br />
into traditional models of academic productivity. Multiple studies
2120 PART 6 ■ Specific Considerations<br />
Figure <strong>129</strong>-1. Twelve roles of<br />
the medical educator. With<br />
permission from Harden<br />
(reference 4).<br />
have demonstrated that promotion for the clinician-educator is<br />
slower when compared to the clinician-researcher, 10 resulting in<br />
the perception that academic medicine values education less<br />
than investigation. We would argue that scholarship can be framed<br />
more productively and with greater relevance. Recent work by<br />
Boyer, 11 Glassick, 12 and Fleming 10 define scholarship more broadly,<br />
and suggest definitions of educational scholarship that will have<br />
more meaning to promotion committees. Fleming’s approach can<br />
be found in Table <strong>129</strong>–1. Hutchings amplifies these themes and<br />
denotes a difference between excellent teaching and “scholarship<br />
of teaching” that require activities to (1) be made public, (2) be<br />
TABLE <strong>129</strong>-1. Promotion Criteria for Clinical Educators<br />
Teaching<br />
Volume<br />
Awards<br />
Innovations<br />
Continuing Education<br />
Quality<br />
Mentoring and Supervision<br />
Student Advising<br />
Research<br />
Supervision<br />
Mentoring<br />
Thesis/dissertation committees<br />
Educational Administration/Service<br />
Education Committees<br />
Accreditation committees<br />
Leadership positions<br />
Curriculum development<br />
Scholarship of Teaching<br />
Peer-reviewed publications<br />
Books/chapters<br />
Editorial services<br />
Recognition by peers<br />
Invited/keynote presentations<br />
Grants and contracts<br />
Reproduced with permission from Fleming 14<br />
open to peer review and critique, and (3) be useable by members<br />
of the teaching community. 13 Delineating and quantifying the<br />
activities that are important to the clinician-educator offers career<br />
development guidance, and encourages departments to create<br />
promotion criteria consistent with the work of an educator. The<br />
future of medical education depends on instilling confidence in<br />
clinical teachers that their contribution to medicine is as highly<br />
valued as that of a researcher.<br />
CONTINUITY OF EDUCATION<br />
IN ANESTHESIOLOGY<br />
The main goals of education in pediatric anesthesiology are (1) to<br />
prepare physicians with the broad range of abilities to provide<br />
exceptional care to the patient and community, (2) to cultivate<br />
practitioners with commitment to performance improvement and<br />
lifelong learning, (3) to train leaders capable of advancing the<br />
knowledge base of our specialty, and (4) to facilitate innovation.<br />
This process begins in medical school and continues throughout<br />
one’s professional career. Given the environment in which most<br />
of us work, achieving the goal of excellence and consistency in<br />
education presents ongoing challenges. Our opportunities for<br />
continuing education are disrupted by the dynamics of our<br />
profession, including practitioners more commonly seeking subspecialization,<br />
and competition for resources between education,<br />
clinical care, and research. 14 In addition, there is discontinuity<br />
between the different phases of medical education as one progresses<br />
from medical school to residency, fellowship, and following<br />
graduation. This fragmentation is due to the lack of coordination<br />
between the organizations responsible for the implementation,<br />
regulation, and funding of education. 15<br />
In response to these issues, educators have begun to adopt more<br />
continuous approaches to education that attempt to bridge the<br />
discrete chapters in one’s development as a physician. With regard<br />
to education, in each epoch of the pediatric anesthesiologist’s<br />
career we are observing an evolution in who we are teaching, what<br />
content is important to our specialty, how that content is transmitted,<br />
and how we assess the success of our pedagogic efforts.<br />
The following sections address how educators in our specialty are
CHAPTER <strong>129</strong> ■ Training and Education in Pediatric Anesthesia 2121<br />
reorganizing the definitions of educational success in each phase<br />
of a physician’s career.<br />
Anesthesiology Education in Medical School<br />
Students are variably exposed to the field of anesthesiology during<br />
the 4 years of medical school. Our inconsistent involvement in the<br />
curriculum makes it difficult to demonstrate our relevance to<br />
medical education and creates obstacles to recruitment. Medical<br />
school is a time of building knowledge and skills in the biomedical<br />
sciences, internalizing the values of the medical profession, and<br />
exploration of potential opportunities for postgraduate study.<br />
Most students struggle to make their specialty decisions by the<br />
end of the third year of medical school, and need guidance, role<br />
models, and mentorship.<br />
A long-held tenet of our specialty is that the study of anesthesiology<br />
should be a postgraduate activity. Aitkenhead 16 disagrees<br />
with this assumption, and appropriately argues that our<br />
specialty is integral to many areas of medicine and must be<br />
defended as an important element of the general medical curriculum.<br />
For some, the study of anesthesiology allows the student to<br />
confirm or reject their specialty interest. To all, the clerkship<br />
demonstrates that our practice includes many patient care activities<br />
other than providing general anesthesia, including widely<br />
applicable subjects such as pediatric resuscitation, pain management,<br />
respiratory care, pediatric physiology and pharmacology,<br />
emergency procedures, and intensive care.<br />
Exposure to our specialty is undermined by the increasing<br />
complexity of the undergraduate medical curriculum. Medical<br />
school has traditionally focused on knowledge acquisition in the<br />
basic sciences such as biochemistry, physiology, and pharmacology,<br />
and on the core clinical disciplines including medicine,<br />
surgery, pediatrics, obstetrics-gynecology, and psychiatry. The<br />
curriculum has been expanded during the past decade in response<br />
to criticism that its limited scope does not adequately prepare the<br />
physician for contemporary practice. 17 Many medical schools have<br />
recently expanded upon the traditional core disciplines with the<br />
addition of emerging fields, 18 including health economics, 19 health<br />
law, 20 medical informatics 21 and palliative care. 22 Anesthesiology<br />
education competes with these subjects for time in the curriculum,<br />
and has been diminished as students become increasingly occupied<br />
with other educational activities.<br />
It is imperative that we develop interesting and innovative<br />
programs for students in order to effectively educate them in<br />
widely applicable anesthesia concepts. Medical simulation appears<br />
to be one of these exciting possibilities, as demonstrated by work<br />
from the University of Toronto in which anesthesiologists in the<br />
simulation lab guide undergraduate students through basic lifesaving<br />
skills such as maintenance of the airway, breathing, and<br />
circulatory support as part of their general medical studies. 23<br />
Simulation-based training represents an engaging and relevant<br />
addition to medical education and, appropriately developed, could<br />
become an indispensable part of the undergraduate curriculum. 24<br />
Medical educators, recognizing that medical specialties create<br />
academic “silos” which inhibit cross-talk between clinicians in<br />
other fields, seek avenues to better integrate medical knowledge.<br />
The fundamental interdisciplinary nature of our specialty provides<br />
a unique opportunity to incorporate anesthesiology into the<br />
medical school curriculum as a model of a clinical science demanding<br />
teamwork, highly functional working relationships, and use<br />
of sophisticated technology. These essential qualities of anesthesiology<br />
mesh well with principles of modern medical education<br />
and, when recognized, may enhance our value to medical school<br />
studies.<br />
Postgraduate Medical Education<br />
Postgraduate medical education, known in the United States as<br />
residency, prepares the physician for the practice of general anesthesiology<br />
or for further subspecialty training following graduation.<br />
U.S. programs train approximately 1500 residents annually. 25<br />
Residency consists of 1 year of medicine, surgery, or pediatrics<br />
followed by 3 years of clinical training in general anesthesiology<br />
and the subspecialties. In the past decade, anesthesiology has<br />
undergone a resurgence in popularity, with medical students<br />
entering the field increasing from 0.3% in 1996 to 3.6% in 2008. 26<br />
The American Board of Anesthesiology requires residents to<br />
spend between 2 and 6 months training in pediatrics, training that<br />
typically occurs during the latter 2 years of residency. Residents<br />
require close supervision when beginning their pediatric anesthesiology<br />
training, with the goal of greater autonomy as they gain<br />
experience and confidence. Education objectives should focus<br />
on pediatric anatomy, physiology, pharmacology, and pediatric<br />
diseases of importance to the anesthesiologist, including exposure<br />
to healthy children and to children with more complex medical<br />
needs. Exposure to a heterogeneous group of pediatric cases will<br />
augment the student’s understanding of our specialty as well as<br />
develop the resident’s appreciation for when a child can be cared<br />
for in a general setting, or when safety dictates that care should be<br />
provided in a more specialized environment.<br />
U.S. and European graduate medical education requirements<br />
for the pediatric component of postgraduate anesthesiology<br />
training include a review of defined didactic material and fulfillment<br />
of specific case log expectations. In the United States,<br />
minimum pediatric case requirements include 100 anesthetics in<br />
children younger than 12 years of age, 20 in children younger than<br />
3 years old, and 5 in children younger than 3 months of age. 27<br />
European standards are more flexible and are suggested to include<br />
30 children younger than 5 years of age and 10 children younger<br />
than 12 months of age during the 5-year training period. 28<br />
Providing quantitative guidelines for residency training is an<br />
important contribution to consistent education. It is increasingly<br />
clear that although these quantitative methods represent an<br />
improvement in pedagogy, additional assessment tools will be<br />
required in the future.<br />
The demographics of students entering our field, as well as their<br />
professional motivations, are evolving. Recent medical school<br />
graduates are choosing specialty training for postgraduate study<br />
more commonly than primary care, 29 fueled by the perception of<br />
greater job security in the specialties, the widening reimbursement<br />
gap between primary care and specialists, and a trend toward<br />
selecting a career with a “controllable lifestyle.” 30 This trend has<br />
dramatically increased the popularity of anesthesiology in recent<br />
years. Other demographic changes include a progressive growth in<br />
the number of women entering medical school. Almost half of U.S.<br />
medical students are female, 31 and it is projected that by the year<br />
2020 women may represent as many as 57% of medical school<br />
applicants. 32 These changes have resulted in greater competition<br />
for training positions in our specialty and an increased number of<br />
female anesthesiology residents. Our specialty will have to adjust
2122 PART 6 ■ Specific Considerations<br />
to the changing professional and personal requirements of young<br />
physicians entering medical practice. Issues such as work-life<br />
balance and childcare flexibility will require particular vision and<br />
sensitivity as educators strive to maintain intellectually vigorous<br />
and desirable training programs.<br />
Postgraduate program directors will have to determine how to<br />
incorporate medical education into a health care environment<br />
shaped by a public that demands highly specialized care. Children<br />
who require complex management are increasingly centralized in<br />
pediatric institutions, diminishing opportunities for residents in<br />
community hospitals to gain pediatric experience. Duty hour<br />
restrictions have also created training obstacles. Although the goal<br />
of postgraduate education is the transmission of the knowledge,<br />
skills, values, and judgment required of an anesthesiologist, there<br />
are few studies to determine what the content of training should<br />
be or how long training should last. Training programs remain<br />
calendrically organized, with the underlying assumption that<br />
sufficient time spent in clinical activities achieves specific educational<br />
objectives. Without evidence to either support or refute this<br />
assumption, educators must develop additional specific qualitative<br />
and quantitative approaches to competency measurement that<br />
enable us to better determine when a physician is capable of safe,<br />
independent practice.<br />
Measurement of Competency<br />
Leading the transformation of medical education is a growing<br />
interest in ascertaining how well physicians perform their professional<br />
duties. Medical schools, training programs, and certifying<br />
bodies require assessment to determine competency to<br />
practice, to discriminate among candidates for future training<br />
opportunities, to provide learning feedback, and to measure the<br />
quality of training programs. 33 Despite the importance of assessing<br />
the knowledge and skills of physicians, the multidimensional<br />
demands of medical practice (Table <strong>129</strong>–2) pose challenges to<br />
performance measurement. In the past, efforts to determine<br />
competency focused on examination results and the presence of<br />
board certification and other training credentials. These measurements<br />
are now understood as an incomplete metric of physician<br />
ability, as contemporary assessment expands to include not only<br />
what physicians know, but what they do. 34 Competence to practice<br />
medicine is now broadly interpreted as “the habitual and judicious<br />
use of communication, knowledge, technical skills, clinical<br />
reasoning, emotions, values, and reflection in daily practice for<br />
the benefit of the individuals and communities being served”. 33<br />
Professional assessment now recognizes that competence develops<br />
as a physician matures, rather than occurring discretely, such as<br />
when one achieves board certification. 35 Anesthesiology educators<br />
are working to develop tools that adequately capture these complex<br />
dimensions of competence utilizing reliable and quantitative<br />
tools. Readers can find a detailed description of anesthesiology<br />
competency measurement in Tetzlaff. 36<br />
Assessment is described as either formative or summative.<br />
Consider the example of learning to drive. Early lessons focus on<br />
skill development, with debriefing providing an opportunity to<br />
discuss the student’s strengths and weaknesses as improved<br />
driving ability develops. This feedback represents formative assessment,<br />
providing student reassurance and an opportunity for<br />
reflection on how improvement may occur. Ultimately, the student<br />
will require testing for licensure, for which summative assessment<br />
is used. Summative assessment, by contrast, is comprehensive in<br />
TABLE <strong>129</strong>-2. Dimensions of Professional Competence<br />
Cognitive<br />
Core knowledge<br />
Basic communication skills<br />
Information management<br />
Applying knowledge to real-world situations<br />
Using tacit knowledge and personal experience<br />
Abstract problem-solving<br />
Self-directed acquisition of new knowledge<br />
Recognizing gaps in knowledge<br />
Generating questions<br />
Using resources (eg, published evidence, colleagues)<br />
Learning from experience<br />
Technical<br />
Physical examination skills<br />
Surgical/procedural skills<br />
Integrative<br />
Incorporating scientific, clinical, and humanistic judgment<br />
Using clinical reasoning strategies appropriately (hypotheticodeductive,<br />
pattern-recognition, elaborated knowledge)<br />
Linking basic and clinical knowledge across disciplines<br />
Managing uncertainty<br />
Context<br />
Clinical setting<br />
Use of time<br />
Relationship<br />
Communication skills<br />
Handling conflict<br />
Teamwork<br />
Teaching others (eg, patients, students, and colleagues)<br />
Affective/Moral<br />
Tolerance of ambiguity and anxiety<br />
Emotional intelligence<br />
Respect for patients<br />
Responsiveness to patients and society<br />
Caring<br />
Habits of Mind<br />
Observations of one’s own thinking, emotions, and techniques<br />
Attentiveness<br />
Critical curiosity<br />
Recognition of and response to cognitive and emotional<br />
biases<br />
Willingness to acknowledge and correct errors<br />
Reproduced with permission from Epstein 41<br />
nature, providing an overall judgment about competence, fitness<br />
to practice, or the creation of a benchmark to measure qualification<br />
for advancement. This distinction is critical, as high-stakes<br />
decisions including board certification or medical licensure must<br />
be based on rigorous assessment methodologies.<br />
For both formative and summative assessment in anesthesiology,<br />
commonly used methods include standardized test<br />
performance, one-on-one evaluation of knowledge and skill by<br />
supervising clinicians, oral examinations, simulation, and fulfillment<br />
of case volume expectations. The nature of anesthesiology<br />
training, including the close observation by faculty of clinical care<br />
performed by students, provides a rich environment from which<br />
performance assessment can be made. However, each traditional<br />
method of assessment has relative strengths and weaknesses that
TABLE <strong>129</strong>-3. Assessment Methods in Anesthesiology<br />
CHAPTER <strong>129</strong> ■ Training and Education in Pediatric Anesthesia 2123<br />
Method Domain Type of Use Limitations Strengths<br />
Multiple choice<br />
questions<br />
Global ratings<br />
with comments<br />
at end of rotation<br />
Oral examinations<br />
High-fidelity<br />
simulations<br />
Standardized patients<br />
and objective<br />
structured clinical<br />
examinations<br />
Knowledge, ability to<br />
solve problems<br />
Clinical skills, communication,<br />
teamwork,<br />
presentation<br />
skills, organization,<br />
work habits<br />
Knowledge, clinical<br />
reasoning<br />
Procedural skills,<br />
teamwork, simulated<br />
clinical<br />
dilemmas<br />
Some clinical skills,<br />
interpersonal<br />
behavior, communication<br />
skills<br />
Summative assessment<br />
within<br />
courses or clerkships,<br />
national inservice,<br />
licensing,<br />
and certification<br />
examinations<br />
Global summative and<br />
sometimes formative<br />
assessment<br />
in clinical rotations<br />
Commonly used in<br />
residency and<br />
fellowship programs<br />
and for<br />
board certification<br />
Formative and some<br />
summative assessment<br />
Formative and summative<br />
assessments<br />
in courses, clerkships,<br />
medical<br />
schools, national<br />
licensure examinations,<br />
board<br />
certification in<br />
Canada<br />
Difficult to write,<br />
especially in certain<br />
content areas; can<br />
result in cueing; can<br />
seem artificial and<br />
removed from real<br />
situations<br />
Often based on secondhand<br />
reports and<br />
case presentations<br />
rather than direct<br />
observation; subjective<br />
Subjective, sex and race<br />
bias has been<br />
reported, time consuming,<br />
requires<br />
training of examiners,<br />
summative<br />
assessments need two<br />
or more examiners<br />
Timing and setting may<br />
seem artificial,<br />
expensive<br />
Timing and setting may<br />
seem artificial,<br />
require suspension<br />
of disbelief, checklists<br />
may penalize<br />
examinees who use<br />
shortcuts, expensive<br />
Can assess many<br />
content areas in<br />
relatively little time,<br />
has high reliability,<br />
can be graded by<br />
computer<br />
Use by multiple independent<br />
raters can<br />
overcome some<br />
variability due to<br />
subjectivity<br />
Feedback provided<br />
by credible experts<br />
Tailored to educational<br />
goals, can be<br />
observed by faculty,<br />
often realistic and<br />
credible<br />
Tailored to educational<br />
goals, reliable,<br />
consistent case<br />
presentations and<br />
rating, can be<br />
observed by faculty<br />
or standardized<br />
patients, realistic<br />
Reproduced with permission from Epstein (reference 45).<br />
limit its utility (Table <strong>129</strong>–3). Some of the flaws associated with<br />
any single assessment technique can be overcome with the simultaneous<br />
use of multiple methods. 37 Balancing the strengths and<br />
weaknesses of various assessment methods must be taken into<br />
serious consideration when determining which combination of<br />
tools best measures specific knowledge and skills.<br />
The achievement of board certification, a common goal<br />
measuring individual competency and training program effectiveness,<br />
represents a valuable standard of cognitive and decision<br />
making skills as seen by physicians, insurance companies, and the<br />
public. 38 But because certification only evaluates cognitive areas it<br />
cannot sufficiently assess the performance skills required of an<br />
anesthesiologist. The measurement of technical skill is critically<br />
important in our specialty. This is especially true during training,<br />
when resident education must be weighed against patient safety.<br />
Recent investigation has evaluated whether there is a minimum<br />
number of times a procedure should be performed to confer<br />
competence. Mulcaster 39 examined the competency of the novice<br />
to perform laryngoscopic intubation, and found that there was a<br />
90% probability of success after 47 attempts. Konrad 40 describes a<br />
90% intubation success rate, defined as the student not requiring<br />
assistance from a supervisor, after 57 attempts. However, 18% of<br />
students still required assistance up until 80 intubation attempts.<br />
The cumulative sum method has also been used as a statistical<br />
approach to evaluate learning curves for anesthesia skills including<br />
intubation, peripheral venous cannulation, and epidural catheter<br />
placement. 41<br />
The Outcome Project<br />
In the U.S., assessment of medical students, residents, and fellows<br />
has shifted to utilize a model established in 1999 by the Accreditation<br />
Council for Graduate Medical Education (ACGME) as<br />
the “Outcome Project,” which defines six general competencies<br />
common to all physicians regardless of specialty. The six core<br />
competencies are listed in Table <strong>129</strong>–4. The Outcome Project is<br />
specifically designed to enhance the educator’s ability to offer<br />
formative assessment and requires that training programs<br />
introduce tools providing evidence that specific educational<br />
objectives are being met. All U.S. anesthesiology residencies must
2124 PART 6 ■ Specific Considerations<br />
TABLE <strong>129</strong>-4. Accreditation Council for Graduate<br />
Medical Education Core Competencies<br />
1. Patient care that is compassionate, appropriate, and effective<br />
2. Medical knowledge, including understanding of established<br />
and evolving biomedical, clinical, and cognate (e.g., epidemiology<br />
and social-behavioral) science.<br />
3. Professionalism, including a commitment to fulfilling professional<br />
responsibilities, a high sense of ethics, and an awareness<br />
of patient diversity<br />
4. Systems-based practice—an awareness of the overall health<br />
care system and the ability to utilize resources to provide<br />
optimal care<br />
5. Practice-based learning and improvement, providing opportunities<br />
for investigation and evaluation of health care<br />
practices, appraisal and assimilation of scientific evidence,<br />
resulting in improvement of health care practices<br />
6. Interpersonal and communication skills that result in<br />
effective exchange of information and teamwork<br />
From the Accreditation Council for Graduate Medical Education Web site<br />
(http://www.acgme.org/acWebsite/home/home.asp).<br />
demonstrate that students develop these competencies during<br />
training, and that measurement tools are available to provide<br />
feedback to both the trainee and training program. The ACGME<br />
is implementing this agenda in three stages over a 10-year period<br />
and the program will be fully phased in by 2011.<br />
One of the goals of the Outcome project is to develop measurement<br />
tools appropriate to assess the knowledge and skills specific<br />
to each medical specialty. The ACGME, with assistance from the<br />
American Board of Medical Specialties (ABMS) has identified a<br />
broad range of tools potentially useful to all training programs<br />
known as the Assessment Toolbox. The toolbox provides a<br />
description of many evaluative methods and references, and can<br />
be downloaded from the ACGME Web site at www.acgme.org/<br />
outcome/assess/toolbox.asp. Many of these tools are untested, and<br />
educators in anesthesiology must identify which will provide the<br />
most relevant individual and programmatic feedback given our<br />
unique professional requirements.<br />
Challenges of the Anesthesiology Training<br />
Students face unique challenges during their training due to the<br />
combination of high work demands, inexperience, and lack of<br />
support. These issues can be exacerbated during pediatric subspecialty<br />
training, when long periods of time separating rotations<br />
can make it difficult to become reoriented to the equipment,<br />
diseases, and special needs of children and their families. In<br />
addition, residents can be saddled with responsibilities that have<br />
only marginal educational value. 42 All these factors contribute to<br />
student stress 43 and require close monitoring by all teaching<br />
faculty. Residents must feel that their educational needs are of<br />
primary departmental importance or they will come to believe<br />
that they are thought of as service providers rather than students.<br />
To effectively manage residents there should be an individual<br />
whose primary responsibility is to champion their educational<br />
needs, and represent them departmentally. Residents should have<br />
a specific educational plan providing graded complexity and<br />
independence as the resident matures, and a mechanism should<br />
exist to monitor successful fulfillment of pediatric case distribution<br />
requirements.<br />
TABLE <strong>129</strong>-5. Accreditation Council for Graduate<br />
Medical Education Duty-Hour Guidelines<br />
1. Duty hours are limited to 80 hours per week, inclusive of<br />
all in-house call.<br />
2. Between daily duty periods and after in-house call, there<br />
should be a 10-hour time period for rest and personal<br />
activities. There should be 1 day off per week free from<br />
responsibilities.<br />
3. In-house call is no more frequent than every third night.<br />
Continuous on-site duty should not exceed 24 hours but an<br />
additional 6 hours are allowed for transfer of patient care,<br />
conductance of outpatient clinics or didactic activities.<br />
4. At-home call is not subject to the 24+6 hour rule or everythird-night<br />
rule as listed in paragraph 4, but residents must<br />
adhere to the 80-hour limit in-house rule and 1 day off per<br />
week.<br />
5. Moonlighting should be included in the 80-hour weekly<br />
work limit and may not interfere with resident educational<br />
goals.<br />
Teaching facilities are confronting the need to balance the<br />
adequacy of resident training with the provision of a healthy and<br />
safe health care environment. To achieve these goals, the ACGME<br />
created duty hour limits in 2003, which can be seen in Table<br />
<strong>129</strong>–5. European residency duty hours are even more restrictive<br />
than those in the U.S. For example, in France, residents are limited<br />
to a 52.5-hour workweek, reflecting the European Working Time<br />
Directive. 44 Duty hour restrictions have been controversial,<br />
received enthusiastically by some trainees and with concern by<br />
faculty and program directors. 45 Although duty hour restrictions<br />
in some high-hour training programs such as surgery have created<br />
a more reasonable work-life balance, their implementation has<br />
created a number of deleterious educational effects. Restrictions<br />
have increased patient handoffs and disrupted continuity of care,<br />
and it is unknown whether they have improved patient safety or<br />
the overall educational experience. Some program directors in<br />
family medicine, concerned with the diminished educational<br />
opportunities secondary to duty hour restrictions, have suggested<br />
that shorter working hours should result in a compensatory<br />
lengthening of residency. 46 Departments of anesthesiology have<br />
also have struggled with implementing these restrictions, and<br />
adequate supervision of clinical work has required the reorganization<br />
of both trainees and faculty. The ACGME will continue to<br />
monitor the effects of duty hour restrictions, and further limitations<br />
may be mandated in the future.<br />
Subspecialty Training in<br />
Pediatric Anesthesiology<br />
Subspecialty or fellowship training in pediatric anesthesiology<br />
should prepare the physician to care for the most complex<br />
pediatric patients, to contribute to our specialty’s knowledge base<br />
through discovery and innovation, to create leaders in research,<br />
and to develop teachers capable of training the next generation of<br />
general and pediatric anesthesiologists. In 2008, there were 45<br />
ACGME-approved pediatric anesthesiology fellowships in the<br />
U.S., training 172 fellows. 47<br />
In 1997, pediatric anesthesiology fellowships in the U.S.<br />
became accredited by the ACGME, creating a series of didactic,
CHAPTER <strong>129</strong> ■ Training and Education in Pediatric Anesthesia 2125<br />
TABLE <strong>129</strong>-6. Didactic Components of an Accreditation<br />
Council for Graduate Medical Education Accredited<br />
Pediatric Anesthesiology Fellowship<br />
The didactic curriculum, provided through lectures and<br />
reading, should include the following areas, with emphasis on<br />
developmental and maturational aspects as they pertain to<br />
anesthesia and life support for pediatric patients:<br />
1. Cardiopulmonary resuscitation<br />
2. Pharmacokinetics and pharmacodynamics and mechanisms<br />
of drug delivery<br />
3. Cardiovascular, respiratory, renal, hepatic, and central<br />
nervous system physiology, pathophysiology, and therapy<br />
4. Metabolic and endocrine effects of surgery and critical<br />
illness<br />
5. Infectious disease pathophysiology and therapy<br />
6. Coagulation abnormalities and therapy<br />
7. Normal and abnormal physical and psychological<br />
development<br />
8. Trauma, including burn, management<br />
9. Congenital anomalies and developmental delay<br />
10. Medical and surgical problems common in children<br />
11. Use and toxicity of local and general anesthetic agents<br />
12. Airway problems common in children<br />
13. Pain management in pediatric patients of all ages<br />
14. Ethical and legal aspects of care<br />
15. Transport of critically ill patients<br />
16. Organ transplantation in children<br />
17. All pediatric anesthesiology residents should be certified as<br />
providers of advanced life support for children.<br />
TABLE <strong>129</strong>-7. Recommended Minimal Case Numbers<br />
for Pediatric Anesthesiology Fellowship Program<br />
Case type<br />
Total cases 250<br />
Cardiac cases 10 to 15<br />
Craniotomies 5<br />
Total cases
2126 PART 6 ■ Specific Considerations<br />
in certification in pediatric anesthesiology is fueled by a number<br />
of issues facing our specialty. These include the expansion of<br />
knowledge in our field, the desire to improve medical care for<br />
children, increased scrutiny being applied to the qualifications of<br />
a pediatric subspecialist, and pressure for improvement and innovation<br />
in our specialty. The application by the SPA acknowledges<br />
that the majority of routine pediatric anesthesiology can and<br />
should be provided by board-certified generalist anesthesiologists,<br />
but suggests that an individual with subspecialty training can best<br />
provide complex pediatric care. Many in our specialty believe<br />
certification provides powerful advocacy for pediatric health care<br />
and will improve teaching quality. 50 Certification would require<br />
that specific standards of knowledge and skill within our specialty<br />
be met, as well as the creation of assessment tools to confirm that<br />
physicians have fulfilled these expectations. Assessment in turn<br />
offers valuable feedback to individual practitioners and to training<br />
programs, thus improving overall pediatric care.<br />
The need for effective assessment methodologies discussed<br />
in the previous section on residency intensifies at the fellowship<br />
level. One meaningful measurement of training success we have<br />
developed is a tool evaluating clinical skills, teamwork, and professionalism<br />
following fellowship completion as judged by<br />
supervisors of new graduates. The effectiveness of graduates in<br />
the “real world” and their ability to perform the many roles of a<br />
pediatric anesthesiologist represent critical benchmarks for how<br />
well training programs prepare the physician to fulfill the demands<br />
of the profession once formal training is completed. We solicit<br />
feedback 12 months following graduation, utilizing the survey in<br />
Table <strong>129</strong>–9, and have found that it provides a powerful metric in<br />
support of our educational mission.<br />
Over the years, clinical training in anesthesiology has eclipsed<br />
the development of research skills in our students. As a result, we<br />
have been successful in training highly competent clinical<br />
anesthesiologists, but have lagged in the creation of physicianscientists.<br />
As can be seen in Figure 2, our field has fallen well<br />
behind other medical specialties with respect to National Institute<br />
of Health funding. 51 Subspecialty training in anesthesiology<br />
should provide a mechanism to create physician-scientists as well<br />
as clinicians. This task is not possible given the present duration<br />
of fellowship training. Other pediatric subspecialty training<br />
programs, such as pediatric critical care or hematology/oncology,<br />
are 36 months in duration, of which many months are dedicated<br />
to the development of research skills. The 12 months of training in<br />
pediatric anesthesiology does not, and cannot, offer this degree of<br />
depth in clinical and research education. In order to reverse<br />
this trend fellowship programs must consider how to best<br />
develop appropriate educational pathways for physician-scientists,<br />
including the creation of specific research fellowships in pediatric<br />
anesthesiology. Unless this is done, our field will be perceived as<br />
not contributing to important areas of biomedical research, and<br />
innovation and discovery in our field will suffer.<br />
Continuing Professional<br />
Development of Faculty<br />
Following residency and fellowship, anesthesiologists require<br />
continuing education to maintain and develop clinical and<br />
teaching skills, to keep abreast of biomedical and technological<br />
developments, and to comply with certification, credentialing, and<br />
licensure requirements. Continuing medical education (CME)<br />
occurs in many forms, including structured participation in<br />
courses, meetings, grand rounds, continuous quality improvement,<br />
or professional development through medical journals and<br />
Web-based material. CME is frequently mandated by licensing<br />
bodies and, in the United Kingdom, is linked to reimbursement<br />
and weekly scheduling. Physicians report spending an average of<br />
50 hours annually in CME activities. 52 Despite the time commitment<br />
in CME and the development of robust business activities<br />
surrounding these educational enterprises, it is unclear whether<br />
this activity successfully improves physician performance. 53 Some<br />
evidence supports improved effectiveness of educational activities<br />
that include an interactive format including case discussion<br />
and hands-on sessions rather than participation in traditional<br />
lectures. 54 This in turn is consistent with adult learning theory,<br />
which supports the model of effective education being learnercentered,<br />
active, and relevant to the participants’ practice. 55<br />
It can be difficult for attending physicians to develop and fulfill<br />
specific educational needs once formal training is completed. This<br />
can be due to lack of appropriate mentorship, financial and time<br />
constraints, and the disorganization of educational resources<br />
discussed earlier. There is a movement transforming postgraduate<br />
medical education from the traditional graduate medical educa -<br />
tion model in which the primary assumption is that knowledge<br />
and skill acquisition is simply a function of hours spent in didactic<br />
experiences. The emerging model is known as continuing<br />
professional development (CPD). Although there is no sharp<br />
demarcation between CME and CPD, the latter recognizes the<br />
multidisciplinary context of patient care, 56 and offers an approach<br />
to medical education that is self-directed, clinically oriented, and<br />
suggestive of a trajectory which continues to rise during one’s<br />
TABLE <strong>129</strong>-9. Recent Graduate Employer Evaluation Tool<br />
1. Relative to other new graduate pediatric anesthesiologists, how would you rate the clinical skill of this graduate?<br />
1 2 3 4 5<br />
bottom 10% 10–25% 25–75% 75–90% top 10%<br />
2. Relative to other new graduate pediatric anesthesiologists, how would you rate teamwork of this graduate?<br />
1 2 3 4 5<br />
bottom 10% 10–25% 25–75% 75–90% top 10%<br />
3. Relative to other new graduate pediatric anesthesiologists, how would you rate the leadership ability of this graduate?<br />
1 2 3 4 5<br />
bottom 10% 10–25% 25–75% 75–90% top 10%<br />
4. If applicable, relative to other new graduate pediatric anesthesiologists, how would you rate academic activity of this graduate?<br />
1 2 3 4 5<br />
bottom 10% 10–25% 25–75% 75–90% top 10%
CHAPTER <strong>129</strong> ■ Training and Education in Pediatric Anesthesia 2127<br />
Figure <strong>129</strong>-2. 2005 National Institutes of Health Awards per Faculty (in thousands). With permission<br />
from Reves (reference 57).<br />
TABLE <strong>129</strong>-10. Comparison of Continuing Medical<br />
Education with Continuing Professional Development<br />
Continuing Medical<br />
Education<br />
Specialized knowledge<br />
Directed at individual<br />
specialist<br />
Deficit view of knowledge<br />
Content determined by experts<br />
Emphasis on theory out<br />
of context<br />
Internal or external<br />
Discrete learning<br />
Reproduced with permission from Turner (reference 63).<br />
Continuing Professional<br />
Development<br />
Generalized knowledge<br />
Associated with groups/care<br />
teams<br />
Knowledge from professionals<br />
practice<br />
Active, self-directed learning<br />
Theory grounded in practice<br />
Usually in the workplace<br />
Continuous learning<br />
professional lifetime. CPD expands upon acquisition of knowledge<br />
and incorporates further development in practice management,<br />
teamwork exercises, communication, information technology, and<br />
education. 57 A comparison of CME and CPD can be seen in Table<br />
<strong>129</strong>–10.<br />
INNOVATIONS IN EDUCATIONAL<br />
TECHNOLOGY: WEB-BASED<br />
LEARNING AND HIGH-FIDELITY<br />
SIMULATION<br />
As the content of medical education is reorganized by demands<br />
of accreditation and technological advances, it also faces the<br />
challenges of incorporating innovative teaching tools into<br />
physician training. Access to the Internet is changing the nature of<br />
anesthesiology education, as physicians find an increasing number<br />
of valuable resources available to them via computer. Medical<br />
students, residents, fellows, and practicing physicians will soon<br />
have access to podcast lectures covering the most current medical<br />
knowledge, eliminating the temporal and geographic constraints<br />
on lecture attendance. Other Internet material is increasingly<br />
accepted as having significant educational value, and Web-based<br />
social networking is creating new opportunities for physicians<br />
at every level of training. In this section, we want to outline some<br />
of these technological developments as they relate to training in<br />
our field.<br />
High-Fidelity Simulation<br />
One innovation we find particularly invigorating has been<br />
increasing use of simulation in healthcare. Medicine has rapidly<br />
embraced high-fidelity medical simulation—similar to that used<br />
in other high-risk organizations such as aviation and the nuclear<br />
power industry—in order to achieve its educational goals.<br />
Physicians widely recognize that patients can be left vulnerable to<br />
morbidity from medical error as students make the transition to<br />
expert clinician. This is especially true at the beginning of a<br />
medical career when experience is limited, and when rare, lifethreatening<br />
events require management. The landmark study by<br />
the Institute of Medicine entitled “To Err is Human” 1 highlighted<br />
this issue by estimating that medical error kills between 44,000<br />
and 98,000 patients annually. As a response to this challenge,<br />
simulation shows tremendous promise as a technique to enhance<br />
teaching of technical and nontechnical skills, as a research tool,<br />
and to assist in performance assessment.<br />
Simulation offers a number of unique training benefits<br />
important to physician development. The ability to create a wide<br />
variety of clinical scenarios provides a valuable opportunity to<br />
review uncommon interventions in an environment without
2128 PART 6 ■ Specific Considerations<br />
patient risk. Scenarios can be flexibly constructed, with a range of<br />
difficulty appropriate for both the novice and expert clinician.<br />
Participants can see the results of their decisions and actions<br />
immediately, and errors can be allowed to occur and reach their<br />
conclusion. High-fidelity simulation frequently takes place in a<br />
realistic environment with actual medical equipment, exposing<br />
technical problems and systemic failures that diminish the<br />
effectiveness of patient care. Simulation can explore interpersonal<br />
interactions and offers training opportunities in teamwork,<br />
leadership and communication. In addition, all simulated sessions<br />
can be recorded without concern for patient confidentiality and<br />
stored for later evaluation.<br />
Several studies have demonstrated practice improvement<br />
following participation in simulation training. Rosenthal showed<br />
that significant improvement in basic airway management after<br />
simulation persisted 6 weeks after initial training and with<br />
subsequent patient encounters. 58 When medical students were<br />
randomized to either simulation-based training or problem based<br />
learning in management of critical respiratory events, Steadman<br />
demonstrated that clinical performance was enhanced in the<br />
simulation group. 59 In teams previously trained in ACLS, DeVita<br />
described how simulation training improved team performance,<br />
which dramatically increased the likelihood of successful resuscitation.<br />
60<br />
Early career development in high-risk fields such as medicine<br />
emphasizes the acquisition of “technical” ability, in which simulation<br />
can play an important role. After achieving appropriate skill<br />
levels, training shifts to include more “nontechnical” aspects of<br />
patient care, including teamwork, situational awareness, and<br />
decision-making. The concept of teamwork training is thoroughly<br />
integrated into the aviation industry, where it is known as crew<br />
resource management (CRM). When the aviation industry discovered<br />
that 70% of aircraft accidents were due to pilot error, 61 it<br />
modified its safety training to include a focus on effective flight<br />
deck team performance and communication. As anesthesiologists,<br />
despite our daily teamwork with nurses, surgeons, and other<br />
health care professionals, our training historically has focused on<br />
individual rather than team performance. Many authors have<br />
recognized that teamwork training should be incorporated into<br />
anesthesia practice, including Gaba, who pioneered the adoption of<br />
CRM concepts into anesthesiology. His Anesthesia Crisis Resource<br />
Management course serves as a model for multidisciplinary team<br />
training in simulated operating rooms. Because effective teamwork<br />
training has led to improved safety in aviation, we believe that it<br />
will enhance patient outcomes in medicine as well.<br />
Despite simulation’s tremendous potential to improve physician<br />
performance, there is reluctance to use it as an assessment tool. 62<br />
Concerns include its expense, its lack of “fidelity,” the threatening<br />
nature of the simulation environment, and the lack of evidence of<br />
its assessment validity. Utilizing medical simulation for physician<br />
assessment will require the development of validated methodologies<br />
that demonstrate the effectiveness of simulation training,<br />
including the identification of key behaviors that result in suboptimal<br />
outcomes. One such tool has been investigated by Fletcher<br />
and Flin, 63 whose Anaesthetists’ Non-Technical Skills system<br />
describes an approach to performance measurement that is highly<br />
relevant to our practice 64 (Table <strong>129</strong>–11). This assessment methodology<br />
is limited by its complexity and labor intensity.<br />
In some countries, simulation is in its early stages of being used<br />
as a credentialing tool in anesthesiology. In New Zealand, board<br />
certification requires the participation in one of two simulation<br />
TABLE <strong>129</strong>-11. Anaesthesia Non-Technical Skills<br />
(ANTS) System: Categories, Elements, and Rating Scale<br />
1) Task management: Skills for organizing resources and<br />
required activities to achieve goals be they individual case<br />
plans or longer term scheduling issues.<br />
a) Planning and preparing.<br />
b) Prioritizing.<br />
c) Providing and maintaining standards.<br />
d) Identifying and utilizing resources.<br />
2) Team-working: Skills for working in a group context, in any<br />
role, to ensure effective joint task completion and team<br />
member satisfaction; the focus is particularly on the team<br />
rather than the task.<br />
a) Coordinating activities with team members.<br />
b) Exchanging information.<br />
c) Using authority and assertiveness.<br />
d) Assessing capabilities.<br />
d) Supporting others.<br />
3) Situational awareness: Skills for developing and maintaining<br />
an overall awareness of the work setting based on observing<br />
all relevant aspects of the theatre environment (patient, team,<br />
time, displays, equipment); understanding what they mean,<br />
and thinking ahead about what could happen next.<br />
a) Gathering information.<br />
b) Recognizing and understanding.<br />
c) Anticipating.<br />
4) Decision-making: Skills for reaching a judgment to select a<br />
course of action or make a diagnosis about a situation, in<br />
both normal conditions and in time-pressured crisis<br />
situations.<br />
a) Identifying options.<br />
b) Balancing risks and selecting options.<br />
c) Reevaluating.<br />
Rating:<br />
4 - Good Performance was of a consistently high<br />
standard, enhancing patient safety. It could be<br />
used as a positive example for others.<br />
3 - Acceptable Performance was of a satisfactory standard<br />
but could be improved.<br />
2 - Marginal Performance indicated cause for concern.<br />
Considerable improvement is needed.<br />
1 - Poor Performance endangered or potentially<br />
endangered patient safety. Serious<br />
remediation is required.<br />
Not observed Skill could not be observed in this scenario.<br />
Reproduced with permission from Flin (reference 72).<br />
courses: Effective Management of Anesthetic Crises (EMAC) or<br />
Early Management of Severe Trauma (EMST). 65 Simulation is also<br />
a prerequisite for Israeli oral board examination. 66 In the U.S., the<br />
American Board of Anesthesiology is developing its simulation<br />
infrastructure and will incorporate simulation-based learning into<br />
its recertification programs. 67<br />
Simulation in Pediatric Anesthesiology<br />
High-fidelity simulation is also becoming an important educational<br />
tool in pediatric anesthesiology. Expert care of the pediatric<br />
patient in the operating room, intensive care unit or emergency
CHAPTER <strong>129</strong> ■ Training and Education in Pediatric Anesthesia 2<strong>129</strong><br />
department is a high-risk endeavor, especially when treating<br />
our youngest patients. Children are at increased risk due to<br />
their limited tolerance of error, the infrequency of pediatric lifethreatening<br />
events, and because they require the care of an anesthesiologist<br />
less frequently than adults. A high level of competency<br />
can be difficult to develop and maintain, especially in a nonpediatric<br />
hospital. Limited duty hours have also reduced exposure<br />
to pediatric patients, creating additional obstacles to gaining<br />
clinical experience. Studies looking at pediatric resident performance<br />
of life-saving skills such as resuscitation or tracheal<br />
intubation confirm clear objective deficiencies, 68–72 including<br />
senior residents who, despite a high level of knowledge, had never<br />
led a code or performed some emergency procedures. Simulation<br />
has grown to fill this important gap by offering a training method<br />
that amplifies critical pediatric learning experiences.<br />
Recent innovations in simulator technology have resulted in the<br />
production of pediatric manikins including the child size METI<br />
PediaSIMTM (Medical Education Technologies Inc, Sarasota, FL)<br />
in 1999 and the infant-sized Laerdal SimBabyTM (Laerdal Medical,<br />
Stavanger, Norway) and METI BabySIMTM in 2005. 73 Like their<br />
adult counterparts, pediatric simulation manikins are capable of<br />
speaking, breathing, and generating realistic physiologic responses<br />
to physical and pharmacologic interventions. Anesthesiologists<br />
and other pediatric specialists are utilizing simulators develop<br />
the cognitive, procedural, communication, and teamwork skills<br />
required of pediatric patient care.<br />
Simulation has been incorporated into many areas of pediatric<br />
training, including pediatric advanced life support, 74 pediatric<br />
trauma, 75 and neonatal resuscitation. 76 Institutions are investing<br />
heavily in pediatric simulation, as exemplified by the Boston<br />
Children’s Hospital, which has constructed an on-site simulation<br />
center replicating their intensive care unit. 77 This facility will offer<br />
continuous multidisciplinary medical, surgical, and trauma training.<br />
Pediatric simulation is also being used to evaluate systems<br />
providing pediatric care. Hunt and colleagues employed pediatric<br />
simulators to study the effectiveness of trauma management in a<br />
series of pediatric emergency rooms responsible for advanced<br />
cardiopulmonary and trauma life support. 78 Others authors have<br />
focused simulation efforts on improving technical and nontechnical<br />
performance of residents 79 and fellows 80,81 managing critically<br />
ill children.<br />
Anesthesiologists and other pediatric healthcare providers<br />
struggle to maintain and develop skills for safe and effective<br />
medical care. High-fidelity simulation has tremendous potential to<br />
bridge the gap between knowledge and action in an environment<br />
that is realistic, reproducible, and poses no threat to patient safety.<br />
Simulation-based training should be thought of as a complement<br />
to patient care, rather than a substitute for it. 82 Although currently<br />
there is no evidence that simulation training improves patient<br />
outcomes, educators are confident that pediatric simulation will<br />
emerge as a powerful tool for medical education and practitioner<br />
and healthcare system assessment.<br />
Web-Based Education Tools<br />
A variety of excellent Web-based pediatric anesthesiology education<br />
sites are now available, including the wide availability<br />
of journal articles online, as well as other content and social<br />
networking sites. Websites important to our specialty include the<br />
Children’s Hospital of Toronto Pediatric Anesthesia Forum (at:<br />
http://forums.ccb.sickkids.ca/paf) providing a forum for the open<br />
exchange ideas of interest to our specialty. The New York State<br />
Society of Regional Anesthesia (at: http://www.nysora.com) is an<br />
outstanding example of excellent content designed for the general<br />
anesthesiologist with an interest in regional techniques, with<br />
detailed descriptions of procedures, high quality graphics, and<br />
comprehensive equipment lists and references. Medical journals<br />
are creating novel approaches to sharing material through the use<br />
of multimedia. An example includes The Journal of the American<br />
Medical Association, which instituted a monthly program known<br />
as “Author in the room” in which a moderator discusses the<br />
findings of an important recent article with its writer, summarizing<br />
the research and providing an almost instantaneous method<br />
for translating new medical knowledge into practice. Anesthesiology<br />
should look closely at some of these models and embrace the<br />
creation of similar content of value to our specialty. Although<br />
educational material on the Internet is disorganized and varies<br />
in quality, and it is unclear how these resources should best<br />
be utilized, 83 the ability to provide content and networking<br />
opportunities represents an exciting avenue for development.<br />
Our professional societies should participate in consolidating<br />
educational material and consider the creation of standards for<br />
Web-based teaching.<br />
CONCLUSION<br />
There is growing recognition that education in pediatric<br />
anesthesiology must keep pace with innovation or the future of<br />
our specialty is at risk. In the past few years, many stakeholders in<br />
medicine, including medical schools, individual departments,<br />
organizations which provide medical education oversight, and the<br />
public, recognize that the future quality of patient care will depend<br />
on how well we respond to these challenges by reinvigorating our<br />
approach to education. In both North America and in Europe,<br />
government entities have created new demands for medical<br />
pedagogy. The ACGME, the Canadian Royal College of Physicians<br />
and Surgeons, and the British Postgraduate Medical Education<br />
and Training Board, have each taken steps to insure that medical<br />
training keeps abreast of biomedical advances and societal needs<br />
through the specification of educational goals and more robust<br />
evaluation of educational outcomes.<br />
In this chapter we have argued that the calendrical education<br />
paradigm, in which discrete periods of time are assumed to be<br />
adequate to the task of imparting necessary knowledge and skill,<br />
is changing to a more sophisticated vision of what education<br />
entails. We have sketched out the difficulties that pediatric anesthesiologists<br />
face in terms of organizing their educational needs<br />
and in convincing educational institutions that what we have to<br />
offer is valuable. We have discussed ways in which technology,<br />
including the use of simulation and the Internet, benefits the<br />
educational experience but also poses challenges to educators. We<br />
have described the ways in which these issues are inextricably<br />
linked to the search for adequate and meaningful measurement of<br />
physician competency, both quantitative and qualitative.<br />
The expectations and duties of our specialty are expanding as<br />
biomedical advances and educational technologies develop in<br />
parallel to a public that demands physician excellence and<br />
accountability. To effectively incorporate medical progress into<br />
our practice, and to fulfill our social responsibility as physicians,<br />
it is clear that medical education will have to change. Although<br />
there is consensus that education must evolve, the complexity of<br />
the healthcare environment and rapidity with which medicine is
2130 PART 6 ■ Specific Considerations<br />
changing creates difficulties in determining how to best proceed.<br />
Finding an appropriate balance between traditional medical<br />
studies and emerging fields will require leadership and vision. One<br />
area that will become increasingly important in the future is how<br />
healthcare will cover the cost of practitioner training. Education is<br />
time consuming and even teaching hospitals see it as marginal to<br />
the core mission of the institution because it does not generate<br />
revenue. Educational reform can only occur with the strong<br />
support of all anesthesiologists who recognize that commitment<br />
to education is commitment to our specialty and our profession.<br />
Today’s medical students, residents, and fellows represent<br />
tomorrow’s clinicians, researchers, educators, and leaders in pediatric<br />
anesthesiology. We must provide them with the resources<br />
needed to create a vibrant, innovative, and intellectually robust<br />
future. By weaving together these varied strands of clinical excellence,<br />
technological innovation, individual creativity, and institutional<br />
support, we will fulfill pediatric anesthesiology’s promise of<br />
“the best of science and the best of caring.”<br />
REFERENCES<br />
1. Kohn LT. Academic Health Centers: Leading Change in the 21st Century.<br />
Washington, DC: The National Academies Press, 2004.<br />
2. Bradley P. The history of simulation in medical education and possible<br />
future directions. Med Educ. 2006;40:254–262.<br />
3. Harden RM. Developments in outcome-based education. Med Teach.<br />
2002;24:117–120.<br />
4. Harden RM, Crosby J. AMEE Guide No 20: The good teacher is more<br />
than a lecturer - the twelve roles of the teacher. Med Teach. 2000;22:334–<br />
347.<br />
5. McLeod PJ, Steinert Y, Meagher T, McLeod A. The ABCs of pedagogy for<br />
clinical teachers. Med Educ. 2003;37:638–644.<br />
6. Davis EA, Escobar A, Ehrenwerth J, et al. Resident teaching versus the<br />
operating room schedule: an independent observer-based study of 1558<br />
cases. Anesth Analg. 2006;103:932–937.<br />
7. Cooke M, Irby DM, Sullivan W, Ludmerer KM. American medical education<br />
100 years after the Flexner report. N Engl J Med. 2006;355:1339–1344.<br />
8. Thomas PA, Diener-West M, Canto MI, et al. Results of an academic<br />
promotion and career path survey of faculty at the Johns Hopkins<br />
University School of Medicine. Acad Med. 2004;79:258–264.<br />
9. Buckley LM, Sanders K, Shih M, Hampton CL. Attitudes of clinical faculty<br />
about career progress, career success and recognition, and commitment<br />
to academic medicine. Results of a survey. Arch Intern Med. 2000;160:<br />
2625–2629.<br />
10. Fleming VM, Schindler N, Martin GJ, DaRosa DA. Separate and equitable<br />
promotion tracks for clinician-educators. JAMA. 2005;294:1101–1104.<br />
11. Boyer EL. Clinical practice as scholarship. Holist Nurs Pract. 1996;10:1–6.<br />
12. Glassick CE. Boyer’s expanded definitions of scholarship, the standards<br />
for assessing scholarship, and the elusiveness of the scholarship of<br />
teaching. Acad Med. 2000;75:877–880.<br />
13. Hutchings P, Shulman L. The scholarship of teaching: new elaborations,<br />
new developments. Change. 1999;31:10–15.<br />
14. Hirsh DA, Ogur B, Thibault GE, Cox M. “Continuity” as an organizing<br />
principle for clinical education reform. N Engl J Med. 2007;356:858–866.<br />
15. Harden RM. Trends and the future of postgraduate medical education.<br />
Emerg Med J. 2006;23:798–802.<br />
16. Aitkenhead AR. Undergraduate and postgraduate education. Best Pract<br />
Res Clin Anaesthesiol. 2002;16:375–389.<br />
17. Ludmerer KM. The development of American medical education from<br />
the turn of the century to the era of managed care. Clin Orthop Relat Res.<br />
2004:256–262.<br />
18. Barzansky B, Etzel SI. Educational programs in US medical schools, 2003–<br />
2004. JAMA. 2004;292:1025–1031.<br />
19. Conill AM, Hillman AL. The future catches up: a medical school curri -<br />
culum in health economics. Am J Med Sci. 2000;319:306–313.<br />
20. Felthous AR, Stanislaus A, Wolfson JK, et al. Health law and mental health<br />
law courses in US medical schools. Am Acad Psychiatr Law. 1987;15:319–<br />
327.<br />
21. Espino JU, Wagner M, Szczepaniak C, et al. An overview of the medical<br />
informatics curriculum in medical schools. Proc AMIA Symp. 1998:467–<br />
471.<br />
22. Fortin AH, Barnett KG. Medical school curricula in spirituality and<br />
medicine. JAMA. 2004;291:2883.<br />
23. Morgan PJ, Cleave-Hogg D, McIlroy J, Devitt JH. Simulation technology:<br />
a comparison of experiential and visual learning for undergraduate<br />
medical students. Anesthesiology. 2002;96:10–16.<br />
24. Parsons D. Curriculum development and the future of anesthesia training<br />
programs. Can J Anesth. 2006;53:855–857.<br />
25. Grogono A. Resident numbers and graduation rates from residencies,<br />
2006. ASA Newsletter. Available at: http://www.grogono.com/nrmp/2006/<br />
Residencies06.pdf. Accessed April 13, 2010.<br />
26. National Residency Matching Program. Results and Data: 2008 Main<br />
Residency Match. Available at: http://www.nrmp.org/data/resultsanddata<br />
2008.pdf. Accessed April 13, 2010.<br />
27. Anesthesiology APRfGMEi. ACGME Program Requirements for Graduate<br />
Medical Education in Anesthesiology Available at: http://www.<br />
acgme.org/acWebsite/downloads/RRC_progReq/040_anesthesiology_07<br />
012008_u03102008.pdf. Accessed April 13, 2010.<br />
28. Carlsson C, Keld D, van Gessel E, et al. Education and training in<br />
Anaesthesia—revised guidelines by the European Board of Anaesthesiology,<br />
Reanimation, and Intensive Care. Eur J Anaesthesiol. 2008;25:528–530.<br />
29. Newton DA, Grayson MS. Trends in career choice by US medical school<br />
graduates. JAMA. 2003;290:1179–1182.<br />
30. Dorsey ER, Jarjoura D, Rutecki GW. The influence of controllable lifestyle<br />
and sex on the specialty choices of graduating U.S. medical students,<br />
1996-2003. Acad Med. 2005;80:791–796.<br />
31. Association of American Medical Colleges. AAMC reports major increase<br />
in U.S. medical school enrollment [press release]. October 25, 2005.<br />
Available at http://www.aamc.org/newsroom/pressrel/2005/051025.htm.<br />
Accessed September 22, 2010.<br />
32. Cooper RA. Impact of trends in primary, secondary, and postsecondary<br />
education on applications to medical school. I: gender considerations.<br />
Acad Med. 2003;78:855–863.<br />
33. Epstein RM, Hundert EM. Defining and assessing professional competence.<br />
JAMA. 2002;287:226–235.<br />
34. Kimatian SJ. Postgraduate medical education: how do we know it’s<br />
working? Anesth Analg. 2006;102:209–212.<br />
35. Leach DC. Competence is a habit. JAMA. 2002;287:243–244.<br />
36. Tetzlaff JE. Assessment of competency in anesthesiology. Anesthesiology.<br />
2007;106:812–825.<br />
37. Epstein RM. Assessment in medical education. N Engl J Med. 2007;356:<br />
387–396.<br />
38. Brennan TA, Horwitz RI, Duffy FD, et al. The role of physician specialty board<br />
certification status in the quality movement. JAMA. 2004;292:1038–1043.<br />
39. Mulcaster JT, Mills J, Hung OR, et al. Laryngoscopic intubation: learning<br />
and performance. Anesthesiology. 2003;98:23–27.<br />
40. Konrad C, Schupfer G, Wietlisbach M, Gerber H. Learning manual skills<br />
in anesthesiology: Is there a recommended number of cases for anesthetic<br />
procedures? Anesth Analg. 1998;86:635–639.<br />
41. de Oliveira Filho GR. The construction of learning curves for basic skills<br />
in anesthetic procedures: an application for the cumulative sum method.<br />
Anesth Analg. 2002;95:411–416, table of contents.<br />
42. Boex JR, Leahy PJ. Understanding residents’ work: moving beyond counting<br />
hours to assessing educational value. Acad Med. 2003;78:939–944.<br />
43. Larsson J RU, Holmstrom I. Being a young and inexperienced trainee<br />
anesthetist: a phenomenological study on tough working conditions. Acta<br />
Anaesthesiol Scand. 2006;50:653–658.<br />
44. Woodrow SI, Segouin C, Armbruster J, et al. Duty hours reforms in the<br />
United States, France, and Canada: is it time to refocus our attention on<br />
education? Acad Med. 2006;81:1045–1051.<br />
45. Brunworth JD, Sindwani R. Impact of duty hour restrictions on otolaryngology<br />
training: divergent resident and faculty perspectives. Laryngoscope.<br />
2006;116:1127–1130.<br />
46. Peterson LE, Johnson H, Pugno PA, et al. Training on the clock: family<br />
medicine residency directors’ responses to resident duty hours reform.<br />
Acad Med. 2006;81:1032–1037.<br />
47. American College of Graduate Medical Education. Main Page. Available<br />
at: http://acgme.org/adspublic. Accessed April 13, 2010.<br />
48. Bannister C. Pediatric anesthesiology: update on pediatric anesthesiology<br />
training programs. ASA Newsletter. 2003;67:31–23.<br />
49. Guidry OF. Report from the president. ABA News. 2007;20.
CHAPTER <strong>129</strong> ■ Training and Education in Pediatric Anesthesia 2131<br />
50. Clark RM. Subspecialty certification in advanced pediatric anesthesiology.<br />
Pediatr Anesth Newsletter. Spring, 2008:11.<br />
51. Reves J. We are what we make: transforming research in anesthesiology.<br />
Anesthesiology. 2007;106:826–835.<br />
52. Goulet F, Gagnon RJ, Desrosiers G, et al. Participation in CME activities.<br />
Can Fam Phys. 1998;44:541–548.<br />
53. Davis DA, Thomson MA, Oxman AD, Haynes RB. Changing physician<br />
performance. A systematic review of the effect of continuing medical<br />
education strategies. JAMA. 1995;274:700–705.<br />
54. Clark NM, Gong M, Schork MA, et al. Impact of education for physicians<br />
on patient outcomes. Pediatrics. 1998;101:831–836.<br />
55. Davis D, O’Brien MA, Freemantle N, et al. Impact of formal continuing<br />
medical education: do conferences, workshops, rounds, and other<br />
traditional continuing education activities change physician behavior or<br />
health care outcomes? JAMA. 1999;282:867–874.<br />
56. Peck C, McCall M, McLaren B, Rotem T. Continuing medical education<br />
and continuing professional development: international comparisons.<br />
BMJ. 2000;320:432–435.<br />
57. Turner NM. Continuing medical education in pediatric anesthesia—a<br />
theoretical overview. Paediatr Anaesth. 2008;18:697–701.<br />
58. Rosenthal ME, Adachi M, Ribaudo V, et al. Achieving housestaff competence<br />
in emergency airway management using scenario based simulation<br />
training: comparison of attending vs housestaff trainers. Chest.<br />
2006;<strong>129</strong>:1453–1458.<br />
59. Steadman RH, Coates WC, Huang YM, et al. Simulation-based training<br />
is superior to problem-based learning for the acquisition of critical<br />
assessment and management skills. Crit Care Med. 2006;34:151–157.<br />
60. DeVita MA, Schaefer J, Lutz J, Wang H, Dongilli T. Improving medical<br />
emergency team (MET) performance using a novel curriculum and a computerized<br />
human patient simulator. Qual Saf Health Care. 2005;14:326–331.<br />
61. Weiner E, Kanki BG, Helmreich RL. Cockpit Resource Management. San<br />
Diego, CA: Academic Press, 1995.<br />
62. Byrne AJ, Greaves JD. Assessment instruments used during anaesthetic<br />
simulation: review of published studies. Br J Anaesth. 2001;86:445–450.<br />
63. Fletcher G, Flin R, McGeorge P, Glavin R, et al. Anaesthetists’ Non-<br />
Technical Skills (ANTS): evaluation of a behavioural marker system. Br J<br />
Anaesth. 2003;90:580–588.<br />
64. Fletcher GCL, McGeorge P, Flin RH, et al. The role of non-technical skills<br />
in anaesthesia: a review of current literature. Br J Anaesth. 2002;88:<br />
418–429.<br />
65. Australian and New Zealand College of Anaesthetists. EMAC and EMST<br />
courses. Available at: http://www.anzca.edu.au/trainees/courses/emacand-emst-courses.<br />
Accessed April 13, 2010.<br />
66. Berkenstadt H, Ziv A, Gafni N, Sidi A. Incorporating simulation-based<br />
objective structured clinical examination into the Israeli National Board<br />
Examination in Anesthesiology. Anesth Analg. 2006;102:853–858.<br />
67. Steadman RH. The American Society of Anesthesiologists’ national<br />
endorsement program for simulation centers. J Crit Care. 2008;23:203–206.<br />
68. Schoenfeld PS, Baker MD. Management of cardiopulmonary and trauma<br />
resuscitation in the pediatric emergency department. Pediatrics. 1993;91:<br />
726–729.<br />
69. White JR, Shugerman R, Brownlee C, Quan L. Performance of advanced<br />
resuscitation skills by pediatric housestaff. Arch Pediatr Adolesc Med.<br />
1998;152:1232–1235.<br />
70. Nadel FM, Lavelle JM, Fein JA, et al. Assessing pediatric senior residents’<br />
training in resuscitation: fund of knowledge, technical skills, and<br />
perception of confidence. Pediatr Emerg Care. 2000;16:73–76.<br />
71. Falck AJ, Escobedo MB, Baillargeon JG, et al. Proficiency of pediatric<br />
residents in performing neonatal endotracheal intubation. Pediatrics.<br />
2003;112:1242–1247.<br />
72. O’Donnell CP, Kamlin CO, Davis PG, Morley CJ. Endotracheal intubation<br />
attempts during neonatal resuscitation: success rates, duration, and<br />
adverse effects. Pediatrics. 2006;117:e16–21.<br />
73. Eich C, McFadzean J, Timmermann A, et al. Simulator-based training in<br />
paediatric anaesthesia and emergency medicine—Thrills, skills and<br />
attitudes. Br J Anaesth. 2007;98:417–419.<br />
74. Burlacu CL, Chin C. Effect of pediatric simulation training on candidate’s<br />
confidence. Paediatr Anaesth. 2008;18:566–567.<br />
75. Falcone RA Jr, Daugherty M, Schweer L, et al. Multidisciplinary pediatric<br />
trauma team training using high-fidelity trauma simulation. J Pediatr<br />
Surg. 2008;43:1065–1071.<br />
76. Halamek LP, Kaegi DM, Gaba DM, et al. Time for a new paradigm in<br />
pediatric medical education: teaching neonatal resuscitation in a<br />
simulated delivery room environment. Pediatrics. 2000;106:E45.<br />
77. Weinstock PH, Kappus LJ, Kleinman ME, et al. Toward a new paradigm<br />
in hospital-based pediatric education: the development of an onsite<br />
simulator program. Pediatr Crit Care Med. 2005;6:635–641.<br />
78. Hunt EA, Hohenhaus SM, Luo X, Frush KS. Simulation of pediatric<br />
trauma stabilization in 35 North Carolina emergency departments: identification<br />
of targets for performance improvement. Pediatrics. 2006;117:<br />
641–648.<br />
79. McGee W, Mailloux P, Fernandez G, Langlois G. A pilot simulation<br />
program training residents in critical care medicine-qualitative analysis<br />
[abstract]. Crit Care Med. 2006:A121.<br />
80. Nishisaki A, Keren R, Nadkarni V. Does simulation improve patient<br />
safety? Self-efficacy, competence, operational performance, and patient<br />
safety. Anesthesiol Clin. 2007;25:225–236.<br />
81. Nishisaki A, Jarrah R, Hales R, et al. Multi-institutional high fidelity<br />
simulation “boot camp” orientation and training program for pediatric<br />
critical care fellows. Crit Care Med. 2006;34:A121.<br />
82. Issenberg SB, McGaghie WC, Petrusa ER, et al. Features and uses of highfidelity<br />
medical simulations that lead to effective learning: a BEME<br />
systematic review. Med Teach. 2005;27:10–28.<br />
83. Vozenilek J, Huff JS, Reznek M, Gordon JA. See one, do one, teach one:<br />
advanced technology in medical education. Acad Emerg Med. 2004;11:<br />
1149–1154.













