Pressure Support Ventilation - A New Triggered Venilation Mode for Neonates
Booklet about pressure support ventilation written by Jean Christophe Roze and Thomas Krueger.
Booklet about pressure support ventilation written by Jean Christophe Roze and Thomas Krueger.

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
PRESSURE SUPPORT VENTILATION |<br />
PRESSURE SUPPORT VENTILATION IN PRACTICE<br />
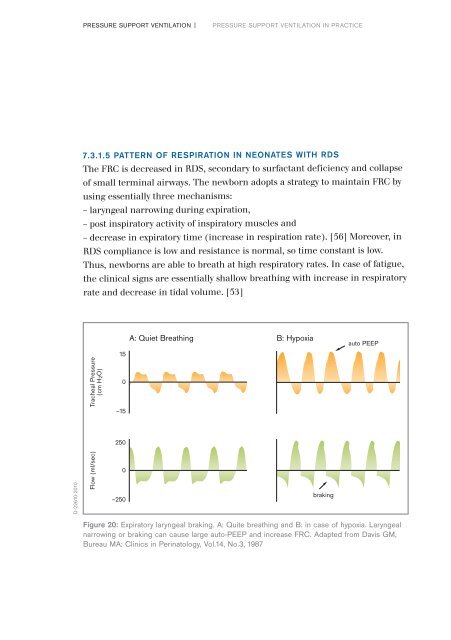
7.3.1.5 PATTERN OF RESPIRATION IN NEONATES WITH RDS<br />
The FRC is decreased in RDS, secondary to surfactant deficiency and collapse<br />
of small terminal airways. The newborn adopts a strategy to maintain FRC by<br />
using essentially three mechanisms:<br />
– laryngeal narrowing during expiration,<br />
– post inspiratory activity of inspiratory muscles and<br />
– decrease in expiratory time (increase in respiration rate). [56] Moreover, in<br />
RDS compliance is low and resistance is normal, so time constant is low.<br />
Thus, newborns are able to breath at high respiratory rates. In case of fatigue,<br />
the clinical signs are essentially shallow breathing with increase in respiratory<br />
rate and decrease in tidal volume. [53]<br />
Tracheal <strong>Pressure</strong><br />
(cm H2O)<br />
A: Quiet Breathing B: Hypoxia<br />
15<br />
0<br />
–15<br />
auto PEEP<br />
250<br />
D-22610-2010<br />
Flow (ml/sec)<br />
0<br />
–250<br />
braking<br />
Figure 20: Expiratory laryngeal braking. A: Quite breathing and B: in case of hypoxia. Laryngeal<br />
narrowing or braking can cause large auto-PEEP and increase FRC. Adapted from Davis GM,<br />
Bureau MA: Clinics in Perinatology, Vol.14, No.3, 1987