

Airway Assessment
2cKbSEQ
2cKbSEQ

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
INCIDENCE OF IMPOSSIBLE MASK VENTILATION<br />
Impossible or grade 4 mask ventilation is a rare occurrence with the incidence reported<br />
between 0.07 per cent and 1.4 per cent 10,12,13 . Kheterpal and colleagues reported an incidence<br />
of 0.15 per cent (one in 690 patients) 11 . This included 77 cases of impossible mask ventilation<br />
in 53,041 patients. They identified five independent predictors of impossible mask ventilation<br />
(Table 10).<br />
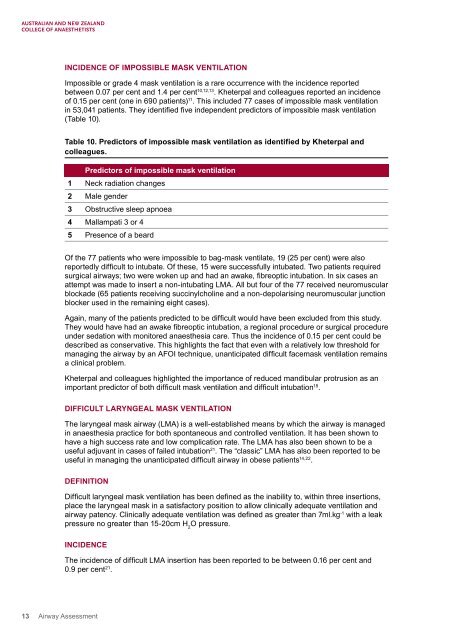
Table 10. Predictors of impossible mask ventilation as identified by Kheterpal and<br />
colleagues.<br />
Predictors of impossible mask ventilation<br />
1 Neck radiation changes<br />
2 Male gender<br />
3 Obstructive sleep apnoea<br />
4 Mallampati 3 or 4<br />
5 Presence of a beard<br />
Of the 77 patients who were impossible to bag-mask ventilate, 19 (25 per cent) were also<br />
reportedly difficult to intubate. Of these, 15 were successfully intubated. Two patients required<br />
surgical airways; two were woken up and had an awake, fibreoptic intubation. In six cases an<br />
attempt was made to insert a non-intubating LMA. All but four of the 77 received neuromuscular<br />
blockade (65 patients receiving succinylcholine and a non-depolarising neuromuscular junction<br />
blocker used in the remaining eight cases).<br />
Again, many of the patients predicted to be difficult would have been excluded from this study.<br />
They would have had an awake fibreoptic intubation, a regional procedure or surgical procedure<br />
under sedation with monitored anaesthesia care. Thus the incidence of 0.15 per cent could be<br />
described as conservative. This highlights the fact that even with a relatively low threshold for<br />
managing the airway by an AFOI technique, unanticipated difficult facemask ventilation remains<br />
a clinical problem.<br />
Kheterpal and colleagues highlighted the importance of reduced mandibular protrusion as an<br />
important predictor of both difficult mask ventilation and difficult intubation 18 .<br />
DIFFICULT LARYNGEAL MASK VENTILATION<br />
The laryngeal mask airway (LMA) is a well-established means by which the airway is managed<br />
in anaesthesia practice for both spontaneous and controlled ventilation. It has been shown to<br />
have a high success rate and low complication rate. The LMA has also been shown to be a<br />
useful adjuvant in cases of failed intubation 21 . The “classic” LMA has also been reported to be<br />
useful in managing the unanticipated difficult airway in obese patients 14,22 .<br />
DEFINITION<br />
Difficult laryngeal mask ventilation has been defined as the inability to, within three insertions,<br />
place the laryngeal mask in a satisfactory position to allow clinically adequate ventilation and<br />
airway patency. Clinically adequate ventilation was defined as greater than 7ml.kg -1 with a leak<br />
pressure no greater than 15-20cm H 2<br />
O pressure.<br />
INCIDENCE<br />
The incidence of difficult LMA insertion has been reported to be between 0.16 per cent and<br />
0.9 per cent 21 .<br />
13 <strong>Airway</strong> <strong>Assessment</strong>